-
1 3
Med Biol Eng Comput (2014) 52:885894DOI
10.1007/s11517-014-1184-4
ORIGINAL ARTICLE
Using a lowamplitude RF pulse at echo time (LARFET) for device
localization in MRI
Murat Tmer Baykal Sarioglu Senol Mutlu Yekta Ulgen Arda
Yalcinkaya Cengizhan Ozturk
Received: 30 December 2013 / Accepted: 13 August 2014 /
Published online: 31 August 2014 International Federation for
Medical and Biological Engineering 2014
1 Introduction
MRI as a real-time imaging modality for use during
inter-ventional procedures is an active research area. Although the
spatial resolution with MRI is not close to that of X-ray methods,
more anatomical detail can be visualized because of increased
soft-tissue contrast without exposure to ion-izing radiation.
Temporal resolution in MRI is also lower than that of X-ray
techniques but demonstrably sufficient to guide catheterization in
humans [32]. MRI is also attractive for flexible slice positioning
and its ability to display differ-ent tissue contrasts, motion, and
flow. Techniques for cath-eter tracking in MRI can be grouped into
three main cate-gories: passive, semi-active, and active methods
[10]. Most interventions rely on tracking the interventional
devices tip (tip tracking) either in real-time images or in the
coor-dinate system of the MR scanner [2, 3, 9, 22]. Beyond,
defining the device tip, visualization of the interventional
devices shaft [19, 29] may be critical in many clinical sce-narios,
especially when flexible devices, such as catheters, are navigated.
But even with shaft visibility, tracking of tip is crucial for most
clinical procedures.
Passive tracking involves the use of contrast agents or
paramagnetic materials to enhance the contrast between the catheter
and the surrounding anatomy [25, 36]. Despite their simplicity in
implementation, the passive methods pri-marily suffer from low
contrast-to-noise ratios, and some-times the appearance of the
marker is indistinguishable from image artifacts [31].
Additionally, the catheter must be manipulated within the imaging
plane since no posi-tional coordinates are generated for automatic
scan plane prescription.
Semi-active techniques are based on local resonant cir-cuits
without external connections. Through inductive cou-pling to the
transmit coil, these resonant circuits provide
Abstract We describe a new method for frequency down-conversion
of MR signals acquired with the radio-fre-quency projections method
for device localization. A low-amplitude, off-center RF pulse
applied simultaneously with the echo signal is utilized as the
reference for frequency down-conversion. Because of the
low-amplitude and large offset from the Larmor frequency, the RF
pulse minimally interfered with magnetic resonance of protons. We
con-ducted an experiment with the coil placed at different
posi-tions to verify this concept. The down-converted signal was
transformed into optical signal and transmitted via fiber-optic
cable to a receiver unit placed outside the scanner room. The
position of the coil could then be determined by the frequency
analysis of this down-converted signal and superimposed on
previously acquired MR images for com-parison. Because of minimal
positional errors (0.8 mm), this new device localization method may
be adequate for most interventional MRI applications.
Keywords Interventional MRI Device localization Catheter
tracking Frequency down-conversion Self-mixing
M. Tmer (*) Y. Ulgen C. Ozturk Institute of Biomedical
Engineering, Bogazii University, Istanbul, Turkeye-mail:
[email protected]
B. Sarioglu Department of Electrical and Electronic Engineering,
Bilgi University, Istanbul, Turkey
S. Mutlu A. Yalcinkaya Department of Electrical and Electronic
Engineering, Bogazii University, Istanbul, Turkey
-
886 Med Biol Eng Comput (2014) 52:885894
1 3
flip angle amplification during RF transmission and signal
amplification during reception, resulting in local signal
enhancement [7, 8, 28, 29, 39]. In these techniques, the coil, and
consequently, the catheter tip can be localized by projecting the
volume onto orthogonal planes. The signal peak in the projections
corresponds to the location of the resonant coil.
In active catheter tracking, the microcoil is directly
con-nected to the MRI system and is positioned at the distal end of
the catheter for localization [12, 18, 21]. The peaks in the
frequency spectrum of the acquired MR signal cor-respond to the
physical location [11]. It is also useful for signals from device
channels to be displayed in color for better visualization [16,
26]. Since this technique provides the location directly, it can
also be used in automated cath-eter tracking, where the imaging
plane and imaging param-eters are adjusted by the tracking results
[5, 38]. Orienta-tion information can also be obtained using more
than one coil [17] or the shaft of the guidewire as a loopless
antenna [19].
The major problem with active techniques is RF heat-ing due to
long conducting wires [24, 41]. Different meth-ods have been
proposed to reduce heating [6, 37, 40] or for heating-controlled
operation [34] without avoiding the con-ducting wires.
Additionally, fully optical systems were pro-posed that replace
these conducting wires with inherently RF-safe optical fibers,
eliminating the risk of RF heating [13, 14]. In these systems, the
MR signal is transmitted with all amplitude and phase information,
allowing high-resolution imaging besides projection-based tip
tracking. In this case, the SNR suffers from the electro-optical
signal conversion distally (and opto-electrical conversion
proxi-mally) at this high frequency.
Amplifying [27] and frequency down-converting [1, 33] the MR
signal at the catheter tip could minimize sig-nal losses and thus
provide higher SNR. The mixing signal
could be provided from an outside generator, necessitating an
additional cable to transmit this signal to the catheter tip. This
would increase the complexity at the distal end. A second
alternative is an oscillator placed at the catheter tip next to the
low-noise amplifier (LNA), and mixer [1]. But for on-chip
oscillators a decrease in accuracy is expected over time due to
temperature or bias voltage variations.
In this work, we propose to provide the reference sig-nal for
frequency down-conversion from the MRI scanners own transmitter.
Since no frequency drift for the transmitter is expected over a
specific imaging sequence interval, it is a very reliable source of
signal. A low-amplitude RF pulse applied at echo time (LARFET) is
acquired by the antenna (microcoil) and used as the reliable and
precise reference to down-convert the echo signal. The frequency of
LARFET is defined as an offset with respect to the center frequency
of the scanner, making the technique immune to main field drifts.
Following down-conversion, the electrical signal is converted into
optical signal for MR-safe transmission. This is also critical to
protect the circuitry of the distal unit and receiver from currents
that would be induced on the outer surface of the cable.
2 Materials and methods
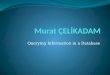
Three pieces of a CT dose index (CTDI) phantom were placed in
12.5 cm intervals as shown in Fig. 1. On each piece, there are 9
holes in a 3 3 placement with 10.61 cm grid interval, resulting in
a 21.22 21.22 25 cm3 FoV to investigate and twenty-seven positions
in 3-D coordinate system. A circuit consisting of an LNA, mixer,
and optical transmitter was connected on a 4.3 6.3 cm printed
cir-cuit board (PCB). The circuitry, which has a total current
consumption of 24 mA, was powered from an MR-compat-ible battery
(MP-174565, 4.8 Ah, Saft Batteries, Bagnolet,
Fig. 1 The locations for the experiment were selected from the
holes already existing on a CTDI phantom consisting of 3 equal
pieces. On each of these pieces, there are 9 holes which have a
diameter of 1.3 cm and are drilled in 10.61 cm intervals (1/2 of
the length of the 15 cm diagonal). They were numbered starting from
the lower left cor-ner (readers view). So the holes on the first,
second, and third pieces had the numbers 1119, 2129, and 3139,
respectively
5
Anterior
Posterior
LeftRight
1 2 3
4 6
97 8
1
2
3
Head
Foot
-
887Med Biol Eng Comput (2014) 52:885894
1 3
France). A microcoil ( = 2 mm, l = 3 mm, and N = 10 turn) was
used to acquire the signals. It was immersed in a saline-filled and
sealed glass tube (Fig. 2a), which fits into the holes very
tightly. The 3 3 grid was aligned parallel to the patient table
using a level, and plastic rods (Fig. 2b). For each spatial
location, an image was first acquired, in which the actual location
of the microcoil was detected as a hyper-intense spot, a result of
elevated RF flip angle at this location, i.e. using semi-active
tracking. Following this, the location was determined using the new
active method, which will be elaborated on in a subsequent section,
and compared to the semi-active localization.
The instrumentation consisted of two units intercon-nected by a
fiber-optic cable. The distal portion (Fig. 2a) was placed inside
the scanner (Siemens Trio, Erlangen,
Germany) to acquire the MR signals and the concurrent LARFET
signal. The output of this unit was an optical sig-nal and
transmitted to an external unit located outside the MR room. The
external unit reconverted the optical signal into electrical, which
was then digitized and analyzed.
2.1 Positional localization MRI pulse sequence
The applied pulse sequence is illustrated in Fig. 3. It starts
with a nonselective RF pulse applied by the body coil to excite all
the spins. The amplitude of the RF pulse is a bal-ance between
obtaining sufficient tracking SNR, which increases as one
approaches the Ernst angle for a given repeat time (TR), and the
desire for high tracking frame rate, which requires the use of
short TRs. An optimal bal-ance was found to be 5 for a TR of 8 ms.
After this nonse-lective RF pulse, a gradient echo is obtained by
applying a readout gradient along one axis.
The angular frequency f0 of the proton magnetic moment vector
that is exposed to a magnetic field B0 is given by
where is the gyromagnetic ratio whose value for 1H is 2.68 108
rad s1 T1 (/2 42.58 MHz/T). If, how-ever, a gradient G is applied
in addition to the static mag-netic field, the local frequency is
modified:
where x is the location of the protons with respect to the
isocenter. Since , G and B0 are all constants, the preces-sion
frequency of the spins is a linear function of their position x.
Thus, for nonzero G, by measuring fMR, the fre-quency of the MR
signal and the location of the acquisition point can be determined.
Therefore, the frequency of the echo signal is a function of the
coils spatial location and the magnitude of the readout gradient;
hence, the location information is frequency encoded. The
difference between this sequence and the conventional
projection-based track-ing method (the Dumoulin method) was the
inclusion of an extra, low-amplitude RF pulse (LARFET), which was
applied by the body coil during signal acquisition. It served as
the reference signal for frequency down-conversion. Its frequency
was selected as f0 300 kHz, with a large off-set from the isocenter
and outside of the field of view for unambiguous localization. The
LARFET pulse amplitude was set to 0.3 V (corresponding to 2.6 dBm
transmission power and 0.1 flip angle), which was still detectable
by the microcoil inside the bore. The advantage of using the
low-amplitude and large frequency offset of the LARFET pulse was
the minimal perturbation of the MRI spins. Because of the large
offset, LARFET did not excite the spins.
(1)f0 = 2pi B0,
(2)fMR = f0 + 2pi G x,
Coax cableCoil
A
Fiber- optic cable
PCB
Saline filled tube
Plastic rods
MR-compatible
battery
Level
Circuit (mixer,
LNA, etc.)
SealWood blocks
B
Fig. 2 a The distal unit. The coil was immersed in a
saline-filled and sealed glass tube. It was connected to the PCB
via a 7-cm coax cable and an SMA connector. This configuration
helped keep the coil out-side the no-signal region shielded by the
ground plane of the PCB. All stages were connected from discrete
components, and at the last stage, the electrical signal was
converted to optical by the LED (HFBR-1518). b The part of the
experimental setup that was placed inside the scanner. Three pieces
that make up a CTDI phantom were fixed using a homemade wooden
framework such that the distance between them is 12.5 cm. A level
put on plastic rods which were inserted into holes ensured the
parallelism of the grid with respect to the patient table
-
888 Med Biol Eng Comput (2014) 52:885894
1 3
However, they were subject to BlochSiegert shift since an
off-resonance RF field was applied [4, 30]. The phase shift of a
spin can be calculated using the formula [30].
where all the frequencies are defined with respect to the
rota-tional frame. Therefore, by putting RF = 2 300 kHz and B1 =
0.1/3 s 0.58 rad/s into Eq. 3, one can obtain BS 1.54 107 rad/s or
fBS 2.5 108 Hz, which is negligible.
The measurements might be affected by some resonant offset
conditions. Magnetic field inhomogeneities and local susceptibility
gradients may also introduce similar errors. These errors are
corrected by obtaining two echoes with opposite polarity gradients
[11]. In this method, the loca-tion was the arithmetic mean of the
independently com-puted locations from the two echoes. This
procedure is repeated for each axis. Hence, four acquisitions are
neces-sary for 2-D and six for 3-D localization.
The duration of the nonselective RF pulse is 0.5 ms, and the
signal acquisition (readout) time is 3 ms. The readout gradient is
extended to 6 ms to dephase the spins and pre-pare them for the
next projection block; hence, one pro-jection block has an 8-ms
duration in total. As a result, the duration of one 3-D complete
projection block is approxi-mately 50 ms. This can also be reduced
to 32 ms using Had-amard encoding [11] instead of the 6 excitation
scheme.
2.2 Frequency encoding gradients
During the echo, together with LARFET, a frequency encoding
(readout) gradient with a bandwidth of 1 kHz/
(3)BS = ( B1)2
2RF,
cm is applied. The amplitude of the gradient is determined from
the following equation:
For BW = 1 kHz/cm, G is 2.349 mT/m. The opposite polarity
dephasing gradient pulse applied before the read-out was
rectangularly shaped with the highest possible slew rate to obtain
the shortest echo time and thus the optimal spatial
localization.
2.3 The distal unit
The block diagram of the distal unit is shown in Fig. 4. The
microcoil has a diameter of 2 mm with an air inductance of 130 nH.
It acts as an antenna to collect the MR signal together with the
LARFET reference signal. The frequencies carried in the signal are
labeled at each node in Fig. 4. Pas-sive detuning with crossed
Schottky diodes (BAS70-04W, Infineon, Neubiberg, Germany) protects
the input of the LNA from large induced voltages in the coil,
although the flip angle amplification effect is not completely
eliminated.
The composite signal is then fed into the LNA through a
noise-matching LC network. The LNA consists of two stages: the
first in common emitter (CE) configuration for low-noise operation
and the second in common emittercommon base (CE-CB) cascade
configuration, for its high stability. All stages use RF NPN
transistors (BFP540, Infineon, Neubiberg, Germany). The LNA has a
power gain of 56 dB with a noise figure of 0.9 dB at 123.2 MHz, the
center frequency of the scanner.
The mixer is a Gilbert cell (HFA3101, Intersil, Milpitas, CA,
USA). The output of the LNA is connected to both
(4)G =2pi BW
RF
Gradient (X, Y, Z)
Acquire
LARFET LARFET
Fig. 3 The pulse sequence used to localize the coil. A frequency
encoding gradient is applied in the direction of localization with
a preceding rewinder gradient. LARFET is applied as soon as the
read-out gradient reaches its flattop and signal acquisition
starts. The verti-cal dotted line indicates the time point where
the area of the positive
polarity gradient equalized the negative part of the gradient
and cor-respondingly the echo time. To overcome the effect of the
resonant offset conditions, two echoes are acquired with opposed
polarity gra-dients
-
889Med Biol Eng Comput (2014) 52:885894
1 3
inputs in order to square the signal. Self-mixing is known to be
a problem occurring in direct conversion receivers when the strong
local oscillator signal leaks into the other input of the mixer.
When the DC offset at the mixer out-put is large, it might saturate
the mixer and corrupt the sig-nal. In the current application,
self-mixing was not an issue since it was deliberately used to
extract the necessary sig-nal fMR fLA from the two-tone input.
Mixer output is further amplified and band-pass filtered (fC1 =
10 kHz, fC2 = 1 MHz, and AV 1000) to separate out the component at
fMR fLA. Because of the high amplifica-tion in this stage, the
signal is saturated and a square wave is obtained at the output,
suitable for optical transmission. The signal is converted into
optical signal by the HFBR-1528 (Avago Technologies, San Jose, CA,
USA) and transmitted to the external unit outside the scanner
room.
2.4 The external unit
The block diagram of the external unit. The signal is
recon-verted into electrical form using an optical receiver
HFBR-2528, which is the counterpart of the HFBR-1528, and finally
captured using a digital oscilloscope (DPO4034B, Tektronix,
Beaverton, USA). The frequency analysis is per-formed offline on a
PC using Matlab (Mathworks, Natick, MA, USA) (Fig. 5).
2.5 Frequency analysis
Amplification of the weak MR signal at the catheter tip and
down-conversion before transmission were crucial for the
minimization of losses and ease of transmission. In our case, the
down-converting signal was the LARFET that is simultaneously
acquired with the frequency encoded MR signal. As shown in Fig. 4,
fMR fLA was carrying the fre-quency encoded location information
and separated out here for analysis.
The frequency analysis consisted of a fast Fourier trans-form
(FFT). The peak in the frequency spectrum was local-ized, and the
position of the coil was computed with the gradient amplitude taken
into account.
fLA in this study was f0 = 300 kHz. Combining fPeak = fMR fLA
with Eq. 2, the following was obtained:
where fPeak is the frequency of the down-converted signal. f0
was the frequency at the isocenter where B = B0. The exact value of
f0 could differ from the specification provided by the scanner
manufacturer. But experimental measurement of it was unnecessary
since f0 was canceled out from the above equation. The above
equation also shows the linear relation between fPeak and x. It can
be rewritten for x for position calculation:
where 2/G is BW, the bandwidth of the gradient (Eq. 4). It gives
f/x, the change in frequency of the received sig-nal with respect
to change in distance from the isocenter as discussed in Sect. 2.2.
As a result, the microcoil location was calculated using the
formula
fPeak + f0 300 kHz = f0 + 2pi G x
fPeak 300 kHz = 2pi G x
(5)(fPeak 300 kHz) 2pi G
= x,
Location =fPeak 300 kHz
BW
fiber optic cable
MR signal
fMR Matching Tuning
Ref. Signal
fLALoop Antenna
Band-Pass
fMR, fLA
fMR, fLA
2 fMR,2 fLA,
fMR+fLA,fMR fLA,
DCfMR, fLA fMR fLALNALED
A
fMR,fLA
fMR fLAPassive Detuning
fMR fLA
MIXER
Fig. 4 The block diagram of the distal unit. Two signals are
acquired by the loop antenna (tip coil). fMR is the frequency of
the MR signal acquired, and fLA is the frequency of LARFET applied
concurrently. After amplification, the signal is multiplied by
itself, and at the out-put of the mixer, combinations of initial
frequencies are generated.
Among them, fMR fLA is the location information carrying lower
frequency signal. It is extracted by the band-pass filter. The
amplifier at the last stage converts the signal into square waves
and drives the LED
Fig. 5 The block diagram of the external unit. The frequency of
the signal is the down-converted fMR fLA like at the output of the
distal unit
-
890 Med Biol Eng Comput (2014) 52:885894
1 3
To determine the peak frequency more precisely, the data was
lengthened in the time domain using zero pad-ding, resulting in
higher resolution in the frequency spectrum. Zero padding to a
power-of-two length also contributed to faster execution of FFT,
the popular DFT algorithm.
3 Results
The concept verification experiment was conducted at 27
different positions in a 3 3 3 grid as shown in Fig. 1.
Figure 6 shows the frequency spectrum of a sample signal
acquired from an off-center position. The spectrum is normalized to
its peak value whose location on the fre-quency axis was used to
determine the physical location of
the coil experimentally. For every position in the grid, six
similar graphs were obtained, namely, for all three axes and both
gradient polarities. For each axis, the physical coordi-nate is
considered to be the arithmetical mean of the inde-pendently
computed locations from opposite polarity gradi-ent signals.
In Fig. 7, the nine transversal MR images acquired for holes
3139 were added up and shown as one image. The computed locations
were superimposed as a green plus sign for comparison. A good
visual correlation was observed. Similar images can be obtained for
any coplanar nine holes in the 3-D grid.
For numerical comparison, a second set of locations was
extracted from the images by segmenting the bright spot regions and
determining their centers as shown in Fig. 8. For a more precise
localization, interpolation was per-formed within the region of
interest containing the bright spot.
The graphs in Fig. 9 show the errors of the proposed sys-tem
with the exact locations assumed to be the bright spot centers on
the MR images. They are all 0.8 mm.
4 Discussion
A low-amplitude RF pulse was successfully used as a pre-cisely
tuned down-converting signal in MRI device locali-zation. Since the
location information is encoded in fre-quency, the accuracy of the
localization is dependent on the frequency accuracy of the
down-converting signal. In this
260 270 280 290 300 310 320 330 3400
0.2
0.4
0.6
0.8
1X: 310053
Frequency (kHz)
Nor
mal
ized
spe
ctru
m (a
.u.)
Fig. 6 A sample frequency spectrum obtained during the
experi-ment. It has a sharp peak at 310,053 Hz corresponding to a
location 100.5 mm off-center. The last digit can be ignored because
it is below the precision of the system
Fig. 7 Left The nine transversal MR images acquired for
locations 3139 are added up and shown as one image. The computed
locations are also superimposed as green plus signs. Right Zoomed
images for better visualization
-
891Med Biol Eng Comput (2014) 52:885894
1 3
case, it is as reliable as the MR scanners RF transmission
system. In addition, it can be defined as an offset from the center
frequency f0. Therefore, no check for f0 is necessary at the start
or during the procedure to set the frequency of the LARFET.
There was a significant match with the bright spot region on the
MR images and the experimentally determined loca-tions. A numerical
comparison showed that the maximum
error of the system was around 0.8 mm, which corre-sponds to 1
pixel for a 512 512 image of 40 cm FoV. This is mainly due to the
fact that imaging experiences the same amount of distortion from
the magnetic field inho-mogeneities, as the proposed method. Taking
the size of the coil into account ( = 2 mm, l = 3 mm), an error of
0.8 mm (1 pixel) is acceptable. This is also far better than
required accuracies for many interventional procedures and
Fig. 8 Left Determination of the center of a sample bright spot.
The center is designated with a plus sign. Interpolation is used
for subpixel localization. Right 3-D plot of the region of
interest. It shows the bright spot as a hill and its boundary as a
contour line
Fig. 9 Absolute errors calcu-lated from the experimentally
determined coordinates and the positions of the coil determined
from the MR images. The numbers on the x axes give the hole
number
-
892 Med Biol Eng Comput (2014) 52:885894
1 3
comparable to error ranges of similar active tracking sys-tems
[15, 23]. Reducing the image resolution within the same FoV can
result in a broader spatial coverage of the center pixel, and the
location found by the system may fall in it rather than the
neighbor pixel, thus virtually increasing the accuracy of image
guidance. The accuracy with current configuration can also be
improved, when necessary, by repeating the measurements and
averaging at the expense of increased localization time. Since this
method is highly sensitive to magnetic field inhomogeneities, for
procedures like biopsy, where the absolute location would be
needed, this method should be applied carefully and only near the
isocenter, where the inhomogeneities and consecutively the
distortions are smallest.
The precision of the system depends on the spacing in the
discrete frequency domain data (f), which is the sam-pling
frequency divided by the number of samples:
where L is signal recording time. In the formula, it seems
possible to reduce the bin spacing in the frequency domain and
accordingly to increase the spatial resolu-tion by lengthening the
recording time L, namely, look-ing at more data at the expense of
increased localization time. Zero padding, however, as mentioned in
Sect. 2.5, can increase the data length N without really increasing
the recording time. Although it does not improve spectral
resolution, which is related to resolving closely spaced features
in the frequency domain, it can provide a more precise localization
of the peak frequency. With fS = 25 MS/s and L = 3 ms, 75 k data
points were obtained per projection. By zero padding and extending
this to 219 (512 k) points, a precision of approximately 50 Hz in
peak detection and consecutively 0.5 mm in localization could be
achieved with no increase in total localization time.
The orientation of the coil with regard to the main mag-netic
field B0 can affect the signal quality and localization accuracy.
Theoretically, there should be a sinusoidal rela-tionship between
the signal intensity and the angle enclosed between B0 and the
coils main axis, where maximum sig-nal is expected at 90 and
minimum at 0. Erhart et al. [12] showed that this expectation is
true. Since in this work, only the idea of using the LARFET as the
reference signal for frequency down-conversion was tested, care was
taken to keep the angle large. If placed parallel to B0, solenoid
coils perform better than planar coils that are extensively
proposed for tip tracking because of their suitability for mass
production and parameter repeatability. Nevertheless, it is obvious
that there will be a reduction in signal qual-ity even with
solenoids. To overcome this undesired situa-tion, different coil
geometries can be applied to this system.
f = f0N=
1L
,
Nonplanar coils [8] or tilted and decoupled multiple coils [20]
are among the possible approaches.
Conventional active tracking systems achieve tempo-ral
resolution down to 20 ms and spatial accuracies in the order of
0.30.5 mm. In this sense, the technique proposed here performs at
least comparably well. The demonstrated performance together with
the absence of electrical con-nections, we believe, paves the way
for this technique to be directly applied to systems that are based
on the combined nearby placement of the tip coil and circuitry for
amplifi-cation and electro-optical signal conversion [1, 13, 14,
33, 35]. On the other hand, the frequency down-conversion not only
simplifies the design of the stages after the LNA but also
decreases the power necessary to drive the LED at the end, which is
basically the electro-optical signal converter. The low frequency
stage is designed to have a very high gain to saturate the signal
at the output and convert the sinusoidal signal into a square wave.
The loss of amplitude information is not important since in our
technique, only the frequency is relevant. Conversion into square
waves also simplified optical transmission of the signal since
square waves can turn the LED on and off. With its original
frequency, an unusual high gain LNA would be necessary to drive the
LED in the same manner, which is not prefer-able due to stability
concerns. A DC offset would be neces-sary to turn the LED on
increasing the power consumption together with the power necessary
to charge and discharge parasitic capacitances at the input of the
LED.
In its current form, namely, without miniaturizing the distal
unit and mounting it to the tip of a catheter, the sys-tem is fully
optically isolated, and while it does not ade-quately address the
RF heating issue, it is an excellent solu-tion to the challenges of
patient isolation in which leakage currents must be limited to a
total of 10 A. In this case, if fully charged, the battery can last
up to 200 h.
The advantages of the technique we propose are as fol-lows: (1)
potentially MR safe due to optical fiber, (2) pro-viding the device
localization coordinates directly, (3) potential high SNR due to
amplification at the source, (4) maintenance of high SNR during
electro-optical and opto-electrical signal conversion and
transmission due to frequency down-conversion. In addition, the
power neces-sary to drive the LED (electro-optical signal
converter) is reduced with the frequency down-conversion. Hence,
the limited power provided by the optical power supply (in future
IC-based designs) can be effectively used for signal
amplification.
5 Conclusion
The proposed LARFET technique is successfully demon-strated for
device localization in MRI. Down-conversion of
-
893Med Biol Eng Comput (2014) 52:885894
1 3
the MR signal right at the source reduced the complexity and
simplified the design of the later stages for signal trans-mission.
The accuracy and precision of the system are com-parable with other
active tracking methods. Reducing nec-essary power can enable the
miniaturization of this system, which could be mounted on catheter
tips, for safe tracking of endovascular devices.
Acknowledgments The authors thank Umut Cindemir and Berk Camli
for their efforts during experiments, Mr. Francis Payne and Dr. Can
Akgn for their valuable editorial support. The experiments were
conducted at National Magnetic Resonance Research Center (UMRAM) at
Bilkent University, Ankara and Acbadem Kozyatag Hospital, Istanbul.
This study was supported by The Scientific and Technological
Research Council Of Turkey (TUBITAK, Project 111E197) and Bogazii
University LifeSci Center (Ministry of Devel-opment, 2009K1200520),
and EU Marie Curie Actions IRSES Pro-ject 269300 (TAHITI, Improving
Therapy and Intervention through Imaging).
References
1. Anders J, Sangiorgio P, Deligianni X, Santini F, Scheer K,
Boero G (2012) Integrated active tracking detector for MRI-guided
interventions. Magn Reson Med 67(1):290
2. Bakker CJ, Hoogeveen RM, Weber J, van Vaals JJ, Viergever MA,
Mali WP (1996) Visualization of dedicated catheters using fast
scanning techniques with potential for MR-guided vascular
interventions. Magn Reson Med 36(6):816
3. Bakker CJ, Smits HF, Bos C, van der Weide R, Zuiderveld KJ,
van Vaals JJ, Hurtak WF, Viergever MA, Mali WP (1998) MR-guided
balloon angioplasty: in vitro demonstration of the poten-tial of
MRI for guiding, monitoring, and evaluating endovascular
interventions. J Magn Reson Imaging 8(1):245
4. Bloch F, Siegert A (1940) Magnetic resonance for nonrotating
fields. Phys Rev 57:522
5. Bock M, Volz S, Zuehlsdorff S, Umathum R, Fink C,
Hallsc-heidt P, Semmler W (2004) MR-guided intravascular
procedures: real-time parameter control and automated slice
positioning with active tracking coils. J Magn Reson Imaging
19(5):580
6. Bottomley PA, Kumar A, Edelstein WA, Allen JM, Karmarkar PV
(2010) Designing passive MRI-safe implantable conducting leads with
electrodes. Med Phys 37(7):3828
7. Burl M, Coutts GA, Young IR (2005) Tuned fiducial markers to
identify body locations with minimal perturbation of tissue
mag-netization. Magn Reson Med 36(3):491
8. Busse H, Thormer G, Garnov N, Haase J, Kahn T, Moche M (2010)
Technique for wireless position tracking of intravascular
catheters: Performance evaluation in a vessel phantom. Proc Intl
Soc Mag Reson Med 18:4163
9. Chung YC, Merkle EM, Lewin JS, Shonk JR, Duerk JL (1999) Fast
T(2)-weighted imaging by PSIF at 0.2 T for interventional MRI. Magn
Reson Med 42(2):335
10. Duerk JL, Wong EY, Lewin JS (2002) A brief review of
hardware for catheter tracking in magnetic resonance imaging. MAGMA
13(3):199
11. Dumoulin CL, Souza SP, Darrow RD (1993) Real-time position
monitoring of invasive devices using magnetic resonance. Magn Reson
Med 29(3):411
12. Erhart P, Ladd ME, Steiner P, Heske N, Dumoulin CL, Debatin
JF (1998) Tissue-independent MR tracking of invasive devices with
an internal signal source. Magn Reson Med 39(2):279
13. Fandrey S, Weiss S, Mller J (2012) A novel active MR probe
using a miniaturized optical link for a 1.5-T MRI scanner. Magn
Reson Med 67(1):148
14. Fandrey S, Weiss S, Muller J (2008) Development of an active
intravascular MR device with an optical transmission system. IEEE
Trans Med Imaging 27(12):1723
15. Fritz J, U-Thainual P, Ungi T, Flammang AJ, Cho NB,
Fichtinger G, Iordachita II, Carrino JA (2012) Augmented reality
visualiza-tion with image overlay for MRI-guided intervention:
accuracy for lumbar spinal procedures with a 1.5-T MRI system. Am J
Roentgenol 198(3):W266
16. Guttman MA, Ozturk C, Raval AN, Raman VK, Dick AJ, DeSilva
R, Karmarkar P, Lederman RJ, McVeigh ER (2007) Interventional
cardiovascular procedures guided by real-time MR imaging: an
interactive interface using multiple slices, adaptive projection
modes and live 3D renderings. J Magn Reson Imaging 26(6):1429
17. Hillenbrand CM, Elgort DR, Wong EY, Reykowski A, Wacker FK,
Lewin JS, Duerk JL (2004) Active device tracking and
high-resolution intravascular MRI using a novel catheterbased,
opposed-solenoid phased array coil. Magn Reson Med 51(4):668
18. Hurst GC, Hua J, Duerk JL, Cohen AM (1992) Intravascular
(catheter) NMR receiver probe: Preliminary design analysis and
application to canine iliofemoral imaging. Magn Reson Med
24(2):343
19. Kocaturk O, Saikus CE, Guttman MA, Faranesh AZ, Ratnayaka K,
Ozturk C, McVeigh ER, Lederman RJ (2009) Whole shaft vis-ibility
and mechanical performance for active MR catheters using
copper-nitinol braided polymer tubes. J Cardiovasc Magn Reson
11:29
20. Kuehne T, Fahrig R, Butts K (2003) Pair of resonant fiducial
markers for localization of endovascular catheters at all catheter
orientations. J Magn Reson Imaging 17(5):620
21. Ladd ME, Zimmermann GG, McKinnon GC, von Schulthess GK,
Dumoulin CL, Darrow RD, Hofmann E, Debatin JF (1998) Visualization
of vascular guidewires using MR tracking. J Magn Reson Imaging
8(1):251
22. Lardo aC, McVeigh ER, Jumrussirikul P, Berger RD, Calkins H,
Lima J, Halperin HR (2000) Visualization and temporal/spatial
characterization of cardiac radiofrequency ablation lesions using
magnetic resonance imaging. Circulation 102(6):698
23. Linte CA, Lang P, Rettmann ME, Cho DS, Holmes DR, Robb RA,
Peters TM (2012) Accuracy considerations in image-guided cardiac
interventions: experience and lessons learned. Int J Com-put Assist
Radiol Surg 7(1):13
24. Nitz WR, Oppelt A, Renz W, Manke C, Lenhart M, Link J (2001)
On the heating of linear conductive structures as guide wires and
catheters in interventional MRI. J Magn Reson Imaging 13(1):105
25. Omary RA, Unal O, Koscielski DS, Frayne R, Korosec FR,
Mis-tretta CA, Strother CM, Grist TM (2000) Real-Time MR
Imag-ing-guided Passive Catheter Tracking with Use of Gadolinium-
filled Catheters. J Vasc Interv Radiol 11(8):1079
26. Ozturk C, Guttman M, McVeigh E, Lederman RJ (2005) Mag-netic
resonance imaging guided vascular interventions. Top Magn Reson
Imaging 16(5):369
27. Pitsaer C, Umathum R, Homagk AK, Ozturk C, Bock M (2010)
Three concepts for tuning and matching intravascular catheter
coils. Proc Intl Soc Mag Reson Med 8:1852
28. Quick HH, Kuehl H, Kaiser G, Bosk S, Debatin JF, Ladd ME
(2002) Inductively coupled stent antennas in MRI. Magn Reson Med
48(5):781
29. Quick HH, Zenge MO, Kuehl H, Kaiser G, Aker S, Massing S,
Bosk S, Ladd ME (2005) Interventional magnetic resonance
angiography with no strings attached: wireless active catheter
visualization. Magn Reson Med 53(2):446
-
894 Med Biol Eng Comput (2014) 52:885894
1 3
30. Ramsey N (1955) Resonance transitions induced by
perturbations at two or more different frequencies. Phys Rev
100(4):1191
31. Ratnayaka K, Faranesh AZ, Guttman MA, Kocaturk O, Saikus CE,
Lederman RJ (2008) Interventional cardiovascular magnetic
resonance: still tantalizing. J Cardiovasc Magn Reson 10:62
32. Razavi R, Hill DLG, Keevil SF, Miquel ME, Muthurangu V,
Hegde S, Rhode K, Barnett M, van Vaals J, Hawkes DJ, Baker E (2003)
Cardiac catheterisation guided by MRI in children and adults with
congenital heart disease. Lancet 362(9399):1877
33. Sarioglu B, Aktan O, Oncu A, Mutlu S, Dundar G, Yalcinkaya
AD (2012) An optically powered CMOS receiver system for
intravascular magnetic resonance applications. IEEE J Emerg Sel
Topics Power Electron 2(4):683
34. Sonmez M, Saikus CE, Bell JA, Franson DN, Halabi M, Faranesh
AZ, Ozturk C, Lederman RJ, Kocaturk O (2012) MRI active guidewire
with an embedded temperature probe and providing a distinct tip
signal to enhance clinical safety. J Cardiovasc Magn Reson
14:38
35. Sun N, Liu Y, Lee H, Weissleder R, Ham D (2009) CMOS RF
Biosensor Utilizing Nuclear Magnetic Resonance. IEEE J Solid-State
Circ 44(5):1629
36. Unal O, Li J, Cheng W, Yu H, Strother CM (2006) MR-visible
coatings for endovascular device visualization. J Magn Reson
Imaging 23(5):763
37. Vernickel P, Schulz V, Weiss S, Gleich B (2005) A safe
transmis-sion line for MRI. IEEE Trans Biomed Eng 52(6):1094
38. Wacker FK, Elgort D, Hillenbrand CM, Duerk JL, Lewin JS
(2004) The catheter-driven MRI scanner: a new approach to
intra-vascular catheter tracking and imaging-parameter adjustment
for interventional MRI. Am J Roentgenol 183(2):391
39. Weiss S, Schaeffter T, Luedeke K, Leussler C, Holz D, Nehrke
K, Rasche V, Sinkus R (1999) Catheter localization using a resonant
fiducial marker during interactive MR fluoroscopy. Proc Intl Soc
Mag Reson Med 12:1954
40. Weiss S, Vernickel P, Schaeffter T, Schulz V, Gleich B
(2005) Transmission line for improved RF safety of interventional
devices. Magn Reson Med 54(1):182
41. Yeung CJ, Atalar E (2001) A Greens function approach to
local RF heating in interventional MRI. Med Phys 28(5):826
Using a low-amplitude RF pulse atecho time (LARFET) fordevice
localization inMRIAbstract 1 Introduction2 Materials andmethods2.1
Positional localization MRI pulse sequence2.2 Frequency encoding
gradients2.3 The distal unit2.4 The external unit2.5 Frequency
analysis
3 Results4 Discussion5 ConclusionAcknowledgments References