Embed Size (px)
Citation preview


C O N T E N T S
214 A Team Approach to Address Antiretroviral Therapy Adherence Barriers ina Managed Care OrganizationSunshine D. Sommers, Daniel J. Kent, Beth Beam, Myde Boles, and DianaAntoniskis
219 An Employee Influenza Immunization Initiative in a Large University Managed Care SettingJeri J. Sias, Stephanie Cook, Thomas Wolfe, Gavin Baumgardner, and PamSalsberry
224 A Cost Analysis of Four Benefit Strategies for Managing a Cox II InhibitorGregory Tucker, Andrea Moore, Deborah Avant, and Merlyn Monteiro
228 Who Bears Responsibility for Glucocorticoid-Exposed Patients in a LargeHealth Maintenance Organization?
D E P A R T M E N T S
175 Cover ImpressionsPortrait of Frau Rieder, theApothecary’s Wife (1893),Wilhelm Leibl
179 PerspectivesPrescription Pharmaceutical Market Goes Global for Consumers
180 Caveats Patient Confidentiality in the 21st Century
182 SpotlightManaged Pharmaceutical Care
Within a Criminal Justice System
185 CampusOregon State University Partnerswith Medicaid and a ManagedCare Organization
233 Continuing EducationRear Window: Actuaries andPharmacists—Toward a NewCompetencyCarol J. McCall
238 CE Exam
240 Author’s Guidelines
EDITORIAL MISSION
JMCP is dedicated to providing managed care pharmacists, associates, and students with the toolsto excel in their daily practices by focusing on:Policy: Providing a forum for in-depth discussion of
issues of topical and long-term importance.Practice: Presenting information of interest and
educational value to the membership.Research: Publishing research that increases the
quality of research standards used in managedcare pharmacy practice and helps apply thatresearch to improve the practice of managed carepharmacy.
EDITORIAL STAFF
Editor-In-ChiefCraig S. Stern, R.Ph., M.B.A., Pharm.D., ProPharma
Pharmaceutical Consultants, Inc., Northridge, CAPublisherJudith A. Cahill, Executive Director • AMCP
HeadquartersContributing EditorsTracy S. Hunter, Ph.D.—AcademicsPerry Cohen, Pharm.D.—FeaturesShane Desselle, Ph.D.—CampusLinda Norton, Pharm.D.—Continuing EducationRenwyck Elder, R.Ph., M.B.A.—SpotlightJ. Warren Salmon, R.Ph., M.B.A.—InternationalDiane B. Ginsburg, M.S., R.Ph., F.A.S.H.P.—CaveatsCeleste d’Elliott—Cover ImpressionsJennifer F. Bloom, M.S.W. —AMCProgressEditorsí Review PanelCraig S. Stern, R.Ph., M.B.A., Pharm.D.Tracy S. Hunter, Ph.D.Diane B. Ginsburg, R.Ph., M.S., F.A.S.H.P.Editorial Advisory BoardRobert J. Anderson, Pharm.D., Mercer University,
Marietta, GAJean Brown, Ph.D., AdvancePCS, Fountain Hills, AZJoan Deady, Sutter Health, Sacramento, CAShane Desselle, Ph.D., Duquesne University,
Pittsburgh, PAColonel George J. Dydek, Pharm.D., U.S. Army,
Aberdeen Proving Ground, MDLeslie Fish, Pharm.D., Fallon Healthcare System,
Worcester, MARichard E. Geller, R.Ph., CIGNA HealthCare,
Glendale, CADiane B. Ginsburg, R.Ph., M.S., F.A.S.H.P., University of
Texas at Austin, College of Pharmacy, Austin, TXAlan Heaton, Pharm.D., Prime Therapeutics, Eagan, MNTracy S. Hunter, Ph.D., Nova Southeastern University,
Fort Lauderdale, FLEric G. Klein, Pharm.D., Eli Lilly & Co.,
Indianapolis, INNeil MacKinnon, Ph.D., Dalhousie University, College
of Pharmacy, Halifax, Nova Scotia, Canada Daniel C. Malone, College of Pharmacy, University of
Arizona, Tucson, AZDarlene Mednick, R.Ph., Merck-Medco Managed
Care, LLC, Franklin Lakes, NJMichael J. Sax, Pharm.D., The Pharmacy Group,
LLC, East Glastonbury, CTFounding EditorLouise J. Sargent, M.S., R.Ph.
Journal of Managed Care Pharmacy(ISSN 1083–4087) is peer-reviewed and publishedbimonthly by the Academy of Managed CarePharmacy, 100 North Pitt Street, Suite 400, Alexandria,VA 22314; 703-683-8416; 800/TAP-AMCP; 703-683-8417 (fax). Periodicals postage pending at Alexandria,VA, and additional mailing offices. Postmaster: Sendaddress changes to 100 North Pitt Street, Suite 400,Alexandria VA 22314.
n FEATURES
189 Employer-Sponsored Health Care ServicesMichael J. Dillon
193 Designing a Framework for Pharmacy Practice:A Look at Consumer Reactions and Expectations Lisa Lopez and Albert I. Wertheimer
201 Resources for Researching Managed Care Pharmacy on the InternetSwu-Jane Lin and J. Warren Salmon
Volume 7, No. 3
172 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3

n uncompromising gaze accom-panied by a lascivious yet pen-sive manner are the hallmarks
of Wilhelm Leibl’s Portrait of Frau Rieder,the Apothecary’s Wife. With an angularpose and an imposing look of expectancy,Leibl captures the piercing posture of thisfashionable and elegant woman. Thepainting emphasizes Leibl’s strong foot-hold in 19th century Realism.
Leibl’s credibility as an artist is evi-dent in his pivotal role within the Leibl-Kreis (Leibl circle). The circle consisted oftalented artists from Germany andAustria who preferred freedom of expres-sion over the mandates prevalent in aca-demic institutions. Leibl’s intense will-power made him the chosen leader of thegroup, which included Johann Sperl,Rudolf Hirth du Frênes, and Karl Haider.Though this exclusive club did not lastlong (1871–1873), Leibl benefited greatlyfrom the artistic association and remainedappreciative of the friendships it fostered.
Leibl’s commitment to detail can berecognized in Frau Rieder’s haute cou-ture. The pale coat is stylishly accentedwith a black collar and gold pin. Theblack hat is placed at a dashing, jauntyangle, suggesting Frau Rieder’s sophisti-cation. In capturing the wispy hair thatinnocently disappears into the back-ground, Leibl literally brushed in FrauRieder’s ambiguity.
Wilhelm Leibl was born in 1844 inCologne, Germany. Twenty years later, hewent to Munich to study at the Academyof Art. After a period in Paris, he returnedto Munich, where he became over-whelmed with artistic demands thatdrove him to seek a quieter lifestyle.Leibl’s life and his art flourished thereafterin the privacy and simplicity of Bavarianvillages. His later paintings recorded theuncomplicated life he loved rather thanthe historical style he was taught inMunich.
In 1870, one of his paintings won a
gold medal; however, it was not until the1890s that he became viewed as the lead-ing German Realist. During the 1870sLeibl’s art demonstrated a strong attach-ment to the German Renaissance; later,his works appear to have been influencedby French Impressionism.
Although Leibl never consideredhimself an expert at female portraits, ourcover art contradicts his opinion. Leibldied in 1900. Although we are a centuryaway from his lifetime, there remainsmuch to appreciate in his art.
Celeste d’Elliott,JMCP Contributing Editor
Cover CreditWilhelm Leibl (1844–1900). Portrait of Frau Rieder,the Apothecary’s Wife, oil on wood. 1893.Provenance: acquired in 1929 on the Munich artmarket, with funds from the Dr. Engel Foundation,permanent collection of the Museum of Fine Arts,Leipzig, Germany.
SourcesQuick M, Ruhmer E. Munich & American realismin the 19th century. Sacramento: EB. Crocker ArtGallery, 1978.
Aurisch H et al., Romantics, realists, revolutionaries.Masterpieces of 19th Century German paintingfrom the Museum of Fine Arts, Leipzig. New York:Prestel, 2000.
C O V E RI M P R E S S I O N S
Portrait of Frau Rieder, the Apothecary’s Wife (1893) n Wilhelm Leibl
A
AMCP HEADQUARTERS100 North Pitt Street, Suite 400 Alexandria, VA 22314Tel: 703-683-8416Fax: 703-683-8417AMCP Staff Editor and Liaison:Jennifer F. Bloom, M.S.W., ext. 308
BOARD OF DIRECTORSPresident: Cynthia J. Pigg, R.Ph., M.H.A.,
CIGNA HealthCare, Richmond, VAPresident-Elect: C.E. (Gene) Reeder, R.Ph.,
Ph.D., University of South Carolina,Columbia, SC
Past President: John D. Jones, R.Ph., J.D.,Prescription Solutions, Costa Mesa, CA
Treasurer: Peter M. Penna, Pharm.D., P.M.Penna, LLC, Farmington, CT
Director: Michael E. Bailey, R.Ph., MedImpactHealthcare Systems, San Diego, CA
Director: James R. (Rusty) Hailey, M.B.A.,Coventry Health Care, Inc., Franklin, TN
Director: Dianne Kane Parker, Pharm.D.,Pharmacia Inc., Irvine, CA
Director: Debbie Stern, R.Ph., Rxperts, Irvine,CA
ADVERTISINGAdvertising for Journal of Managed CarePharmacy is accepted in accordance with theadvertising policy of the Academy of ManagedCare Pharmacy.
For advertising information, contact:Professional Media Group, Inc., P.O. Box 18940 N. Woodbury Road, Pitman, NJ 08071Tel: 800-486-5454 or 856-589-5454; Fax: 856-582-7611
EDITORIAL
Correspondence related to editorial contentshould be mailed to:
Mitchell Petersen, Inc., 1775 Jamieson Avenue,Suite 210, Alexandria, VA 22314Tel: 703-518-4700; Fax: 703-518-8495 Managing Editor, Jeanne BurkeProduction Manager, Laura Mahoney
SUBSCRIPTIONS
Annual Subscription Rates: USA, individuals,institutions–$60; other countries–$80. Singlecopies cost $10. Missing issues replaced free ofcharge only up to six months after date ofissue. Send requests to AMCP headquarters.
REPRINTS
For article reprints, contact Tricia Rudis,Reprint Management Services, 717-560-2001,x49. Microfilm and microfiche editions ofJournal of Managed Care Pharmacy are avail-able from University Microfilms, 300 N. ZeebRoad, Ann Arbor, MI 48106.
All articles published represent the opinions of theauthors and do not reflect the official policy of theAcademy of Managed Care Pharmacy or theauthors’ institutions unless so specified.
Copyright© 2001 Academy of Managed CarePharmacy, Inc. All rights reserved. No part of thispublication may be reproduced or transmitted inany form or by any means, electronic or mechan-ical, without written permission from theAcademy of Managed Care Pharmacy.
A b o u t o u r c o v e r a r t i s t
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 175

C A M P U SR e s e a r c h a n d i n n o v a t i v e m a n a g e d c a r e c u r r i c u l a a t s c h o o l s o f p h a r m a c y
Oregon State University Partners with Medicaid and a Managed Care Organization
he Oregon State UniversityCollege of Pharmacy has con-tracted to provide faculty expert-ise to support the pharmacy pro-
grams of the Oregon Medicaid Programand a Medicaid managed care organization,CareOregon. These relationships helpadvance the service mission of the collegeby promoting safe, efficacious, and cost-effective pharmacotherapy in Oregon. Theactivities funded under the agreements alsooffer opportunities for research and studenteducation, promoting the college’s educa-tional mission.
nnBackgroundIn 1995, the traditional fee-for-service stateMedicaid program was transformed intothe Oregon Health Plan (OHP). The OHPwas designed to increase the covered popu-lation while controlling costs, primarily byusing a prioritized list of diagnosis andtreatment pairs. Coverage was initially lim-ited to diagnoses above a certain cut-off linethat depended on enrollment and funding.However, the Health Care FinancingAdministration (HCFA) limited this flexibil-ity by disallowing further movement of theline in response to funding shortfalls.HCFA also requires most patients to enrollin a managed care plan and OHP mandatesmanaged care enrollment when possible.For patients enrolled, the plan manages thepharmacy benefit. The exception is mentalhealth drugs, which are covered entirely byfee-for-service Medicaid.
Shortly after the OHP began, about85% of Medicaid clients were enrolled inmanaged care plans. This number has sincedecreased to about 70% as commercialplans have withdrawn from the OHP.Currently, about 125,000 Medicaid patientsare covered for drugs in fee-for-service.
CareOregon is a managed care plan inthe OHP that primarily serves Medicaidrecipients. Its providers and clinics arecommunity health centers, clinics basedat the Oregon Health Science University,and independent physician groups.
Currently, CareOregon serves approxi-mately 60,000 members and is expectedto reach 100,000 by July 2001, aspatients transfer from commercial plansleaving the OHP.
nn Medicaid Program ActivitiesIn 1994, the college entered into a contractwith the state Office of Medical AssistancePrograms (OMAP), the agency that admin-isters the OHP. The contract has benefitedboth parties and has expanded over theyears to currently fund approximately sixfull-time-equivalent (FTE) clinical pharma-cists whose responsibilities are: (1) adminis-trative support of the Oregon Drug UseReview (DUR) Board, (2) drug policy analy-sis and consultation, (3) educating Medi-caid providers, and (4) providing drug ther-apy consultation and information to Medi-caid providers.
One primary responsibility of the col-lege is to administer the DUR Board.College faculty analyze drug utilization,evaluate new drug therapies, and formulateeducational or policy strategies for the DURBoard and OMAP to consider. The facultythen facilitate and implement board recom-mendations through collaborations withOMAP, contracted managed care plans, orthe contracted pharmacy benefit manager(PBM). The OMAP agreement requires thatthe faculty evaluate and report on the effectof any intervention that is implemented.
OMAP often asks for opinions and eval-uation of a variety of drug policy proposals.For example, faculty were asked to evaluatean internal agency proposal to use incen-tives to increase generic prescribing. Thefaculty analyzed the feasibility of the pro-gram and its potential financial impactunder different scenarios.
The agency also regularly requests drug-claim-data reporting and analysis and drug-information and policy research reports. Arecent claim analysis reviewed the providerspecialties that prescribed mental healthdrugs. A recent drug information requestasked for an evaluation of new drugs used
to treat influenza. A recent policy analysisrequest was to report on federal law andpolicies in other states regarding drug co-payments for Medicaid recipients.
Several provider educational programsare already underway or being designed.The college faculty produce a peer-reviewed quarterly newsletter targeted toprimary care clinicians so as to promotehigh-quality, cost-effective prescribing.Articles primarily review therapeutic top-ics and new drugs; occasionally newsbriefs cover important breaking druginformation. Hard copies are mailed to allproviders and pharmacies in the state.Copies are also posted on the college’sWeb site at http://pharmacy.orst.edu/dur/dur_news.htm.
The faculty are now writing an evi-dence-based prescribing guide in collabora-tion with OMAP, commercial managed careplans, and professional medical and phar-macy organizations. The guide is designedas a tool for primary care clinicians. It willcontain concise prescribing recommenda-tions for common conditions treated by pri-mary care providers, cost information, dos-ing information, and formulary and priorauthorization information from major man-aged care plans in Oregon.
Faculty members offer monthly sem-inars to primary care providers at variousclinics that primarily care for Medicaidpatients. In addition, clinical faculty con-sult on drug therapies and respond todrug information requests from Medicaidproviders.
Finally, programs are being created toprovide academic detailing and drug pre-scribing feedback for Medicaid providers.These programs are on schedule to beimplemented in spring and summer 2001;they will be the primary focus of our activ-ities this year.
nnCareOregon ActivitiesThe college faculty contracted with Care-Oregon to manage its pharmacy benefitprogram. The college prepared a form-
T
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 185

Campus
ulary that was implemented in fall 2000.The college coordinates the Pharmacy andTherapeutics Committee, manages therelationship with CareOregon’s contractedPBM, writes reports and recommenda-tions for the Utilization ReviewCommittee, published a prescribing guidesimilar to the one being published forOMAP, and offers educational programsfor contracted primary care providers.
nn Teaching and ResearchOpportunities
Pharmacy clerkship students are integratedinto all these activities. Students taking theDrug Information/Drug Policy clerkshiprespond to drug-information requests,write new drug evaluations, write newslet-ter articles, and formulate policy recom-mendations. Students research requestsand present reports to the DUR Board,OMAP staff, and CareOregon staff.
Clerkship students must complete aproject during their rotation. This is usu-ally a drug-use evaluation in an ambula-tory care clinic or using drug claim infor-mation. The college also offers a PrimaryCare/Managed Care Specialty residencythat provides opportunities to gain expe-
rience in all of the activities described. There is considerable opportunity for
research as a result of these arrange-ments. College faculty provide pharmacypolicy and drug-use review services toapproximately 225,000 covered lives intotal, or 67% of the Oregon Medicaidpopulation. Because both OMAP andCareOregon allow access to pharmacyand medical claim data, several projectsusing Medicaid claims data are underway.
nnSummaryThe collaborations between the OSUCollege of Pharmacy, OMAP, and Care-Oregon have been beneficial for all par-ties. There is synergy because both organ-izations serve Medicaid populations andtherefore their goals and patient demo-graphics are similar. The current agree-ments provide a service to the state ofOregon, a rich learning environment forstudents, and many opportunities forresearch.
Kathy L. Ketchum, R.Ph., M.P.A., H.A., isCoordinator of Medicaid Programs at OregonState University College of Pharmacy inPortland, OR. Dean G. Haxby, Pharm.D., is
Director of Medicaid Programs and AssociateProfessor of Pharmacy Practice, Departmentof Pharmacy Practice, Oregon State Univer-sity College of Pharmacy. Dr. Haxby is alsoAdjunct Associate Professor of FamilyMedicine, Oregon Health Sciences Universityand Pharmacy Director at CareOregon.
Readers are invited to submit
ideas and articles to Campus.
Contact Shane Desselle, Ph.D., Duquesne
University, Mylan School of Pharmacy,
Pittsburgh, PA 15282;
Tel: 412-396-6363; Fax: 412-396-5130;
E-mail: [email protected].
The current agreements provide a service to
the state of Oregon, a rich learning environ-
ment for students, and many opportunities
for research.
186 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 243
he Academy of Managed CarePharmacy (AMCP)announced its newly electedBoard of Directors and com-mittee leadership at the 13th
Annual Meeting in Tampa, Florida, lastmonth.
Cynthia J. Pigg, R.Ph, M.H.A., willserve as AMCP President for 2001– 2002.Pigg, Assistant Vice President for CIGNAHealthCare of Richmond, Virginia, is acharter member of the Academy, hasserved as chair of the Professional RelationsCommittee, a member of the FinanceCommittee, AMCP’s representative on theVirginia Task Force on TherapeuticSwitching, and AMCP delegate to thePharmacy in the 21st Century Conference.Pigg has served as President-elect since2000.
Pigg replaces John Jones, AMCPPresident for 2000–2001, who becomesImmediate Past President. Jones serves asDirector for Pharmacy Networks andLegal Affairs for Prescription Solutions,Costa Mesa, California. A member of theAcademy since 1992, Jones led theLegislative and Legislative and RegulatoryAction Committees; he now becomeschair of the Corporate Member Councilas well as president of the Foundation forManaged Care Pharmacy.
C. E. (Gene) Reeder, Ph.D., has beennamed President-elect. Reeder, AssociateDean of the University of South CarolinaSchool of Pharmacy, has served on theBoard of Directors since 1998, and hasbeen a member of the Professional PracticeCommittee, the Special Projects Commi-ttee, and the Strategic Development andMarketing Committee. Reeder has alsoserved on the Board of Directors of theFoundation for Managed Care Pharmacy(FMCP), and on the Editorial AdvisoryBoard for the Journal of Managed CarePharmacy. Dr. Reeder will move into theoffice of the presidency for 2002–2003.
Peter M. Penna, Pharm.D., will serveas Treasurer of AMCP for the term2001–2003. Penna, president of P.M.
Penna, LLC, Farmington, Connecticut,helped to found AMCP in 1988–1989.Penna was President of AMCP during1990–1991 and President of the FMCPin 1991–1992. He received the FMCP’sLeadership Award in 1995.
Incoming directors are James R.(Rusty) Hailey, M.B.A., and Debbie Stern,R.Ph. Hailey is Vice President, SpecialtyMarkets, for Coventry Health Care, Inc.,Franklin, Tennessee. A member of AMCPsince 1990, he served on the MembershipCommittee last year and chaired thePharmaceutical Industry RelationsCommittee. Stern, Vice President, Rxperts,Irvine, California, has been an AMCP mem-ber since 1990; she has served on thePublic Relations Committee and on theProgram Planning and DevelopmentCommittee, which she chaired in2000–2001.
Continuing as AMCP Directors for2001–2002 are Michael Bailey,MedImpact Healthcare Systems, andDianne Kane Parker, Pharmacia.
nnCommittee Chairs for 2001–2002 • Educational Affairs: Marv Shepherd,
University of Texas at Austin School ofPharmacy
• Journal of Managed Care PharmacyEditorial Advisory Board: Craig S.Stern, ProPharma PharmaceuticalConsultants, Inc.
• Legislative: Steven W. Gray, KaiserPermanente Medical Care Program
• Legislative & Regulatory Affairs:Cindy Bradish, Humana, Inc.
• Membership: Virginia Sweeter,Professional Meeting Consultant
• Organizational Affairs: DennisLyons, Pharmaceutical Strategies
• Professional Practice: James Utt, JohnDeere Health, Inc.
• Program Planning & Development:Beth Brusig, Sentara Health Care—Optima Health Plan
• Schools of Pharmacy Relations: PallavRaval, Walgreens Health Initiatives
• Special Projects: Renee Rizzo Fleming,HealthNow New York
• Finance: Peter Penna, P.M. Penna, LLC• Nominations Committee: Carey
Cotterell, Kaiser Permanente MedicalCare Program
• Ad Hoc Committee on AMCP’s Frame-work for Drug Therapy Management:Dianne Kane Parker, Pharmacia
nnCorporate Member Council
To give corporate members of AMCP aforum for exchanging ideas with the leader-ship, the Board of Directors has created theCorporate Member Council.
The Council replaces the PharmaceuticalIndustry Relations Committee, which in-cluded both corporate and noncorporatemembers. The Council is a deliberative bodyworking to identify potential ways throughwhich individual and corporate memberscan collaborate to fulfill the mission andobjectives of AMCP, evaluate their feasibility,and offer recommendations to the Board.
“The Pharmaceutical Industry RelationsCommittee played an important role,” saidJohn Jones, Past President of AMCP and thechairman of the new Council. “However,AMCP has more than 50 corporate mem-bers, so the former committee simply couldnot provide all those members with anappropriate forum for expressing their ideasand participating in collaboration withother AMCP members. The new Counciloffers that opportunity.”
The Corporate Member Council consistsof AMCP Corporate Members; eachCorporate Member designates a representa-tive—typically the Corporate Contact fromthe member organization—to the Councilon an annual basis. The immediate Past-President of AMCP serves as the Chair of theCouncil. AMCP’s Executive Director andMembership Director also have seats on theCouncil.
“I believe AMCP’s Corporate Memberswill welcome the chance to participate inthe Corporate Member Council,” saidJohn Roney, Associate Director of Health
A M C P r o g r e s sN e w s a n d i n f o r m a t i o n t h e A c a d e m y
AMCP’s New Leaders
T

244 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
Systems Affairs for Procter & GambleHealth Care. “This new forum will giveall Corporate Members a role in a delib-erative body that will provide importantinput to the AMCP Board as it sets policyand direction for the Academy.” The firstmeeting of the Corporate MemberCouncil took place at the 13th AnnualMeeting and Showcase in Tampa.
For more information, please contactMembership Director Kevin Alder at 800-827-2627.
nnBylaws Amendments
Active members of AMCP have approvedten amendments to the Bylaws governingthe Academy.
An amendment to Section 3.3,Categories of Membership, creates a newmembership category of Allied Member,which is now being designed by theMembership Committee.
The amendment was proposed toallow participation in AMCP by nonphar-macist employees of managed care organi-zations who help administer the pharmacybenefit. AMCP has recognized that thesenonpharmacist colleagues, whose respon-sibilities range from patient assistance tonetwork administration to quality assur-ance to client support, are critical to thedelivery of the pharmacy benefit. Theseemployees often do not qualify foremployer payment of pharmacy organiza-tion dues and therefore do not now partic-ipate in AMCP activities. The Boardbelieves that these individuals would ben-efit from AMCP’s services and thereforeproposed a new category of membershipspecifically tailored to attract this impor-tant cadre of nonpharmacist professionals.
A second amendment to Categories ofMembership separated the currentStudent/Resident membership categoryinto one Student category for undergrad-uate students and one category forGraduate/Residency/Fellow members.
An amendment to Section 4.1, AnnualMeeting, changes the name of this sectionto “Annual Business Meeting.” The changein wording was proposed to distinguishthe Annual Business Meeting of Members
from the Academy’s Spring continuingeducation meeting, entitled “the AnnualMeeting.”
The format and purpose of theAnnual Business Meeting will be definedin the organization’s Policies andProcedures Manual, to include membercommunication for Board considerationat a later date, an open forum for infor-mational purposes, a State of Affairsreport by the President, presentation ofawards, and installation of directors andofficers. The Committee recommendedthat the Annual Business Meeting shouldnot include action items for vote.
Section 4.2, Special Meetings, wasamended to require 25% of active mem-bers to pre-register in order to hold aSpecial Meeting. The change also allowsthe Board to act upon a petition prior toa Special Meeting, and requires that allvotes at Special Meetings be taken bywritten ballot. This amendment alsoeliminates Section 4.8, Quorum forMeetings of Members, and Section 4.9,Vote Required at Meetings of Members,and incorporates these sections intoSection 4.2.
An amendment to Section 4.5, Voting,adds the language, “Voting for dissolutionshall be by written ballot mailed to mem-bers. Voting at Special Meetings shall beby written ballot.
An amendment to Section 5.1, Boardof Directors, removes language regardingcompensation of Board members, andadds that Board members are reimbursedfor expenses incurred in connection withperformance of AMCP business. The newlanguage clarifies that Board members arenot paid for service, but are reimbursed forexpenses in connection with the perfor-mance of AMCP business.
Section 5.3, Election of Directors andOfficers, was amended to include newlanguage: “Candidates receiving the high-est number of votes for each vacancy tobe filled shall be elected. There shall beno cumulative voting. A tie shall bedecided by lot.”
Section 5.9, Policy Making Powers,was amended to specify that a copy of an
annual report by Directors shall be madeavailable to all members, rather thanmailed to each member, as the earlier lan-guage required. The report will be mailedto any member who requests it.
By amending Article XIII, Dissolution,the Academy clarified the distribution ofremaining assets of the Corporation upondissolution to state that members are nolonger eligible payees. The Bylaws hadrequired, in the event of liquidation or dis-solution of the Corporation, that after pay-ment of all liabilities the Board “shall dis-tribute to each then current member of thecorporation, pro rata, the remaining assetsof the Corporation, up to and not exceed-ing the total amount of each such members’previous payments to the Corporation byway of dues and assessments.”
The Academy does not have a historicdatabase that would allow implementa-tion of that language. Therefore, the newlanguage stipulates that “no member,trustee, or officer of the corporation orany private individual shall be entitled toshare in the distribution of any of the cor-porate assets upon dissolution of theCorporation.” The balance of corporatefunds will be distributed by the Boardaccording to the Bylaws, which requirethat the Board shall distribute remainingassets to organizations primarily engagedin promoting the interests of the pharma-ceutical professional, which are organizedand operated exclusively for charitable,educational, or scientific purposes.
A number of other conformingchanges were made to the Bylaws, which,in the opinion of the Board, did notrequire individual votes. Members mayrequest a copy of the document by callingDan Fishkin at 703-683-8416, ext. 317(e-mail: [email protected]).
AMCProgress

A n U p d a t e o n t h e L e g i s l a t i v e a n d R e g u l a t o r y I s s u e s F a c i n g P h a r m a c y P r a c t i c e
atient confidentiality. These twowords have been buzzwords inCongress since 1996, when Presi-dent Clinton and Congress passed
the Health Insurance Portability andAccount-ability Act (HIPAA) of 1996. Theact stipulated that Congress pass nationalmedical-record privacy legislation byAugust 21, 1999.
After much discussion and debate,Congress was unable to meet this deadline.Therefore, HIPAA requires that the U.S.Department of Health and HumanServices (DHHS) issue regulatory stan-dards. In November 1999, the Presidentand DHHS Secretary Donna E. Shalalareleased a proposal; an extensive commu-nication period ensued, with approximate-ly 55,000 public comments reported.
On December 20, 2000, PresidentClinton and DHHS released the final rule.Implementation of the final regulation is tocome into effect by April 2003 (2004 forentities with revenue under $5 million).Now, in the 21st century, there are mini-mum national standards regarding patientconfidentiality.
The final regulation includes healthplans, health care clearinghouses, andhealth care providers as covered entities.The provisions apply equally to public-and private-sector health plans andproviders. The final regulation applies toall types of personal health information,including oral communication, paperrecords, and electronic forms. It has thefollowing provisions: consumer control,boundaries on medical record use andrelease, security of personal health infor-mation, accountability for medical recordsuse and release, and protection for psy-chotherapy notes. These components areincluded because of careful considerationfrom the president and DHHS regardingconsumers’ comments. Below are briefdescriptions of the contents of the finalregulation. (For a pharmacy analysis, see:www.amcp.org/public/legislative/analy-sis/032701c.html).
How is a patient’s health information
used? Patients themselves control the useof the information. Providers are requiredto clearly post notifications of how theirinformation can and cannot be disclosed.Also, a history of disclosures must be madeavailable to patients. Patients must giveconsent before information is released.Patients have the right to file complaintsregarding violations of the provisions ofthis rule.
Health care providers, including phar-macists, are required under the law toobtain prior patient consent before use anddisclosure of patient-identifiable informa-tion for payment, treatment, and healthcare operations, including quality assur-ance and disease-management programs.Providers would be required to post a noti-fication of their privacy policies in clearsight. A health plan would not need toobtain consent for these purposes.However, given the complexities of therule, it is thought that most health planswould rather be safe than sorry, and obtainconsents from enrollees. In order to dis-close information for activities other thantreatment, payment, and health care oper-ations, the provider or other covered enti-ty would be required to obtain a specificwritten “authorization,” different from thegeneralized consent, detailing to whom theinformation would be disclosed and why.These types of activities would includemarketing programs and the sale of data.
Under the rule, each covered businessentity, including pharmacies, would berequired to adopt internal privacy proce-dures identifying those individuals withaccess to the information and for what use.The business would be required to hire aprivacy officer who must train and moni-
tor employees on the privacy proceduresof the organization. In most cases, thisrequirement would necessitate establish-ing a new position.
There are strict penalties for violatingthe privacy rules. While an individual hasno private right of action, DHHS can deemthat there has been a violation pursuant toa personal grievance filed by an individual,which can trigger criminal penalties forintentional disclosure.
The patient confidentiality rule doesnot preempt more stringent state laws onuse and disclosure of patient-identifiableinformation. Given this provision, multi-state covered entities will have to ascertainwhether federal or state laws govern in thelocations where they operate. The answermay well vary from jurisdiction to jurisdic-tion.
Many organizations, including AMCP,have analyzed the rule and recommend-ed changes to DHHS. Because of manyconcerns over the impact the final rulewill have on the delivery of care, DHHStook the extraordinary step of acceptingadditional comments on its already pub-lished final rule. Many in Congress arealready considering whether or not tointroduce legislation to fix what they seeas flaws in the regulation and the under-lying statute. Pharmacists must takeactive roles in attempting to perfect thisregulatory and legislative process toensure that they can continue to provideoptimal care for all patients.
Kali Spencer is a Pharm.D. candidate at theCollege of Pharmacy, University of Texas atAustin.
C A V E A T S
P
P o l i c y , l e g i s l a t i v e , a n d r e g u l a t o r y i s s u e s a n d t r e n d s
Patient Confidentiality in the 21st Century
180 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
Health care providers, including pharmacists,
are required under the law to obtain prior
patient consent before use and disclosure of
patient-identifiable information.

Employer-Sponsored Health Care Services
PRACTICEF E A T U R E
mployer-sponsored health care isa concept that may be unfamiliarto many managed care pharma-cists. It deserves close examina-
tion because it is an idea that has been wellreceived and effective. It was developed tohelp mid- to large-sized employers con-tract for primary care and pharmacy serv-ices in a manner that is cost-effective andconvenient for employees (both currentand retired) and often their dependents aswell. Its goal is to reduce costs whileimproving access and quality of care. Theoutcomes—reduced health care costs,improved quality of care, increased work-er productivity, and lower absenteeism—are well worth the investment.
nn The Options At first glance, employer-sponsored healthcare may seem like an attempt to circum-vent established managed care or pharma-cy benefit management (PBM) plans. It isnot. It does not replace the managed careplan, the PBM, or insurance. Instead, itaugments these services with additionalaccess points that are paid for via anothermechanism. The additional access pointsmay offer one or a combination of options:occupational health interventions, phar-macy benefits, primary care services, or cor-porate health services. Table 1, page 190,gives examples of each of these services.
According to Michael Hardies, M.D.,chief medical officer for CHD MeridianHealthcare, industry data reveal that per-sons who must leave the workplace toseek health care use 12–16 times as muchtime as those who can meet their health
care needs on the work site. This is apowerful motivator for employers to con-sider this creative alternative—it decreas-es cost, enhances quality, and improvesaccess to service.
All services described here are offeredat the employer’s work site (whether aheavy manufacturer or a corporate head-quarters) or nearby, thus providingemployees ready access to necessaryhealth care. Every employer-sponsoredhealth care program will be different; pro-grams are tailored to meet the employer’sand employees’ needs. For example, oneemployer may need only the pharmacybenefit (stand-alone or á la carte programselection), while another employer maychoose to implement modifications of allfour options (integrated programming).
The benefits of employer-sponsoredhealth care are easily elucidated with a lit-tle informed contemplation. Much of thisactivity recalls an earlier time when it wasnot unusual for health care to be deliveredat the work site. Until the early 1960s, itwas common for large employers to offerbasic on-site health care, with some largecompanies even operating company hos-pitals. The employee health clinic was animportant benefit in large factories orlabor sites, and offered services that bytoday’s standard seem rudimentary. Thefocus was often reactive or triage: injury oracute-illness treatment and referral. Withthe evolution of various types of insuranceand a push for patient choice, health caremoved out of the workplace and into theeconomy in the middle of the 20th century.
E
Author
MICHAEL J. DILLON, M.S., R.Ph., is Director of Pharmacy Services, CHD Meridian Healthcare, in Latham, NY.
AUTHOR CORRESPONDENCE: Michael J. Dillon, M.S., R.Ph., Director of Pharmacy Services, CHD Meridian Healthcare, 13 British American Blvd., Latham, NY12110; Tel: 518-782-4733; Fax: 518-782-4747; E-mail: [email protected].
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
B y M i c h a e l J . D i l l o n
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 189

Employer-Sponsored Health Care Services
190 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
nnWhat Was Old Is New AgainToday, employers are experiencing resur-gent interest in on-site health benefits fortheir employees. One major motivator is
cost. Employer-sponsored pharmacies thatoffer prescription services exclusively to acompany’s covered population can pur-chase pharmaceuticals directly at a fardeeper discount than that availablethrough managed care or PBM programs.Since pharmaceuticals are the fastest-growing health care cost today, this is a sig-nificant incentive for employers. The keyis provision of care to a defined popula-tion. Employer-sponsored pharmaciesleverage the employer’s size and prescrip-tion volume to purchase pharmaceuticalsdirectly within this “closed door” class oftrade. This defined population is the rea-son for both the pricing differential andthe restriction-to-care provision. A closed-door pharmacy can only dispense pre-scriptions to those who are clearly definedas beneficiaries of the client organization.Figure 1, below, describes this class oftrade with respect to other classes of tradein terms of their pharmaceutical costs.
Other savings are achieved by employer-sponsored pharmacies as well. Disease-state management and early-interventionprograms are fairly standard among sites,and they are especially successful if thepharmacy benefit is offered in conjunctionwith a primary care service. Table 2, page191, describes national and local-levelclinical efforts that are used by pharmaciesin the employer-sponsored model. Pharm-acists work as indispensable members ofthe health care team, and their interven-tions or suggestions may be offered as for-
mally as a structured chart review, or asinformally as a suggestion over coffee inthe employee cafeteria. The concept ofpharmaceutical care is easier to implementin employer-sponsored sites than it is inother locations. Pharmacists deal with oneplan and one plan only. There are no eligi-bility issues to resolve, and pharmacistsmust be familiar with only one benefitplan and design.
Employer-sponsored health care canalso help organizations achieve VoluntaryProtection Program (VPP) status with theOccupational Safety and Health Admini-stration (OSHA). OSHA’s VPP is designedto recognize and promote effective safetyand health management. In the VPP, man-agement, labor, and OSHA establish acooperative relationship at a workplacethat has implemented a strong programthat meets an established set of criteria.OSHA publicly recognizes the site’s exem-plary program, and removes the site fromroutine scheduled inspection lists (OSHAmay still investigate major accidents, validformal employee complaints, and chemi-cal spills). VPP participant sites generallyexperience 60%–80% fewer lost workdaysattributable to injuries than would beexpected of an “average” site of the samesize in their industries.
One health care administrator learnedthe value of employer-sponsored healthcare when his organization scaled backtheir services. “It was disastrous,” he said.He went on to say that administrators
Highest AWP Discounts Lowest AWP Discounts
FIGURE 1 Class-of-Trade Continuum
Gov’t Entities
AcuteHospitals
Employer-sponsored-pharmacy class of trade
Staff ModelPharmacies
Mail OrderPharmacies
Long-Term Care
Prisons
Home HealthProviders
Large RetailPharmacies
Independent
Notes: AWP is average wholesale price. Example is not necessarily to scale.
Type of Service Possible Features
Occupational or • Medical surveillancecorporate health • Injury treatmentservices • Travel medicine
• Return-to-work clearance
• Preventive care
Primary care • Health care tailored to unique population
• Screening and health maintenance care
• Cost-effective care provision
Pharmacy services • Drug dispensing• Drug-interaction,
adverse drugreaction, and allergy screening
• Drug-utilization review
• Preferred-drug management
• Vaccination• Drug information
TABLE 1 Employer-SponsoredHealth Care Services

Employer-Sponsored Health Care Services
believed that since they were already pay-ing for other types of insurance for theiremployees, savings could be reaped bysending employees out to their ownphysicians or health plans. “This was anill-conceived approach to managing cost.What little was saved up-front was imme-diately lost to increased absenteeism andincreased risk. Any organization that isserious about absence managementshould consider on-site employee healthservices a worthwhile investment.”
nn Earning Market Share Employer-sponsored health care’s successis contingent upon drawing customersfrom the client’s workforce. Employeeparticipation is voluntary. Employer-sponsored health care offers convenientlocations and hours of operation thataccommodate the workforce, a copay-ment differential, and some added bene-fits. These factors promote better compli-ance and improved utilization manage-ment. Convenience goes beyond place-ment of a pharmacy on the grounds ofthe employer’s factory or firm. Someorganizations place pharmacy drop-boxes throughout the plant, or staff adrive-through window. All emphasizecustomer service. Even in the largest oforganizations, a sense of community, loy-alty, and ownership is common; employ-ees come to know their health careproviders as members of their community,and welcome “their” health careproviders to their work teams. As themost accessible members of the healthteam, pharmacists hold a special place inthese patients’ esteem. A pharmacist whohas good communication and customer-service skills enhanced with underpin-nings of clinical expertise can cultivateloyalty and trust.
Some specific pharmacy care programshave been enormously successful at worksites. Several deserve mention:• Brown-bag programs encourage employ-
ees to empty their medicine cabinets intobrown bags and bring them to their phar-macist for review. Polypharmacy, noncom-pliance, and potential drug-interactionissues can be identified and rectified.
• Pharmacist-administered vaccinationsfor employees who travel overseas, oras simple preventions (influenza andtetanus), are gaining popularity instates where this practice is allowed.Many employees would go without aflu shot if they had to schedule anappointment or pay a copayment. On-site vaccination that is inexpensive orfree motivates good prevention.
• Coordination of hyperlipidemia andHelicobactor pylori screening programsthat educate high-risk patients withverbal and written information havebeen successful at many sites.
• A half-tablet program that takes advan-tage of pharmaceutical manufacturers’pricing strategies has reduced costs byup to 5% at some sites.
• Addition of over-the-counter (OTC) oralternative/complementary drugs hashelped increase the likelihood of posi-tive outcomes for patients who need orwant these items. Convenient availabili-ty of OTC items provides a lower-costtreatment strategy for some conditions.For example, patients may be more will-ing to accept that they have a viral infec-tion that does not require antibioticswhen they can obtain symptomatictreatment without leaving the clinic.
nnProof of SuccessPharmacy managers within employer-sponsored health care systems, like phar-
macy managers in many managed caresites, are heavily dependent on reliable,advanced information technology (IT). ITcan help managers share best practicesamong sites, identify geographic patternsof drug use, and broadcast policy, infor-mation, and educational materials topharmacists. Information managers mustconstantly look for ways to improve theorganization’s IT pharmacy applications,and apply them in ways that lead toimproved outcomes for patients anddecreased costs for the sponsor.
Currently the emphasis is on upgrad-ing IT systems so that the systems movetoward the ideal, paperless medicalrecord. Future systems will also incorpo-rate lab values and outcome measure-ments, better data retrieval, and patient-care modules.
Accreditation by an established groupconstitutes the highest form of publicrecognition, and stimulates continuousimprovement. Program quality should bevalidated by the Accreditation Associationof Ambulatory Healthcare (AAAHC) or asimilar group.
The ultimate measure of success is thecustomer-satisfaction survey. Employeeswho choose to use the sites generally rateservice well, and like the personalized carethey receive as well as the convenience.
nn Implications for Managed Care Pharmacists
Many large employers currently contract forhealth care services. Companies such asBethlehem Steel, General Electric, Goldman
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 191
National Level• Leverage buying power• Decrease suppliers• Cost-shift• Restrict/tighten benefits
Local Level• Educate prescribers• Perform disease management• Educate patients• Implement pharmaceutical-care programs
TABLE 2 ManagingPrescription Costs
ìAny organization that is serious about absence
management should consider on-site employee
health services a worthwhile investment.î

Employer-Sponsored Health Care Services
192 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
Sachs, International Paper, and ToyotaMotor Manufacturing currently use employ-er-sponsored health care services. Thedirect-contracting model works for them,and in the future, this type of program willgrow. It is mutually beneficial for theemployer, the employee, and care providers.
There is growing opportunity in thistype of setting for pharmacists who wish topractice in diverse locations and offer alevel of service unmatched in communitypractice. Patient access is unfettered andthe pharmacist’s role on the health careteam is valued. Consequently, pharmacistswho work in this type of environmentexperience high levels of satisfaction.
Total pharmacy savings for employerscan be 15%–25% or higher. While the effi-
cacy of each program depends on marketpenetration of total prescriptions, efficacyof pharmacy care programs, and impact ontotal health care costs, the day-to-day con-tributions of highly motivated pharmacyprofessionals are the most valuable driversat employer-sponsored pharmacies.
nnConclusion Employer-sponsored health care works.Its customers are identified on two levels:At the corporate and industrial level,employer-sponsored health care is wellreceived because health care costs arelowered and absenteeism is reduced.With these two issues creating tremen-dous concern across the nation, any
improvement is of great value. For theemployees who receive health care serv-ices at their work sites via employer-sponsored health care, this deliverymethod is welcomed as an efficient wayto improve quality of life. Small healthproblems are resolved before they devel-op into serious problems and healthmaintenance is convenient.
This old idea has been reinvented in away that is much improved. Employer-sponsored health care models define theircustomers differently than other models,emphasize accessible care, and reduce cost.This type of service is attractive to employ-ers, and will continue to grow. It is a distinctand growing opportunity in a unique mar-ket segment. This will continue to create

Designing a Framework for PharmacyPractice: A Look at Consumer Reactionsand Expectations
SPECIAL R E P O R T
he Academy of Managed CarePharmacy (AMCP) has had atask force at work since early1999 to design “Pharmacy’s
Framework for Drug TherapyManagement in the 21st Century.” Whilethere has been no shortage of studies andcommittees exploring the future of phar-macy, AMCP’s endeavor has one impor-tant feature that sets it apart from previ-ous efforts: It sought direct input frompharmacy’s customers—specifically, acade-micians, drug manufacturers, employers,government officials, health plan adminis-trators, patients, and physicians.
AMCP sees these individuals as key“consumers” in managed care pharmacy.And because AMCP values their health caredecision making, the organization felt it wascritical to include these groups’ voices increating a pharmacy framework thatresponds to their needs and expectations.
Toward this end, AMCP conducted atelephone survey of 20 individuals inSeptember and October 2000. Some of theresults were unexpected; others were com-pelling. In essence, it was felt that sharing
these insights could help stakeholderswork together to design a more sensitizedframework for pharmacy practice.
Respondents included two academi-cians, two representatives from drug man-ufacturers, four employers, two govern-ment representatives, five health planadministrators, two patient representatives,and three physicians. Each was askedabout seven key customer expectations. Ofthese seven expectations, five promptedthe most thought-provoking responsesamong the interviewees:• Drug-related problems will be identi-
fied, resolved, and prevented.• Care is coordinated. • There is value in the care that patients
receive and it is affordable.• The system is accessible and is looking
out for the patient’s best interest. • The system will provide adequate and
appropriate information and educationregarding appropriate drug use.
nn The Responses This section includes responses to the areasaddressed within these five expectations.
Asterisks (*) separate interviewees’ respons-es. A diamond (u) indicates that no differ-ing or compelling statement was made.
Drug-Related Problems Will BeIdentified, Resolved, and Prevented Many of the respondents noted that whilesociety generally expects that drug-relat-ed problems will be identified, resolved,and prevented, they say that: (1) suchefforts are not being carried out; and (2)computer systems that link certain drug-therapy data between physicians’ officesand pharmacies would help identifypotential adverse drug events.
(1) Drug-related identification, resolu-tion, and prevention efforts are notbeing carried out. Academicians (one of two respondentsagreed): “There are some good systems formonitoring and detecting drug-druginteractions using sophisticated software,but having the software and rating sys-tems currently in place can never over-come a reimbursement system that worksin the opposite direction.”
T
Authors
LISA LOPEZ is president of Chaac Communications, a health care editorial consulting practice in Athens, OH. ALBERT WERTHEIMER, Ph.D., M.B.A., is a professor atTemple University School of Pharmacy, in Philadelphia, PA.
AUTHOR CORRESPONDENCE: Albert I. Wertheimer, Ph.D., M.B.A., Professor, School of Pharmacy, Temple University, 3307 N. Broad St., Philadelphia, PA 19140; Tel: 215-707-1291; Fax: 215-707-8188; E-mail: [email protected].
ACKNOWLEDGMENT: This article reports on a professionally conducted series of telephone interviews with pharmacy stakeholders and consumers regarding theirexpectations and reactions to the provision of drug therapy management services. Responses are categorized by participant affiliation, and some of the more insightfulfindings are presented here. This endeavor is a component of the Academy of Managed Care Pharmacy project to develop a Framework for the Provision of DrugTherapy Management Services in the 21st Century, slated for completion in late 2001.
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
B y L i s a L o p e z a n d A l b e r t I . W e r t h e i m e r
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 193

Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
194 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
Drug manufacturers (two of two respon-dents agreed): Both respondents notedthat there are opportunities to improvecurrent efforts. “Managed care pharmacistsare actually in a pretty good position tomore closely mimic a hospital pharmacythan a retail pharmacy, with the added ben-efit that they can reach more peoplethrough sophisticated use of formulariesand availability of drugs, and a sophisticat-ed linkage with the medical partner of theirmanaged care organization in which theyview disease management as an objective.They may (target) diseases that cause mul-tiple visits to specialists and hospitals orthat require emergency room visits.”
Employer purchasers (three of fourrespondents agreed): “I think the systemsare in place—they are good and thehealth care offerings that the employershave do look closely at the drug compo-nent so that there’s adequate access, it’saffordable, and there’s some level of cost-sharing. However, in many cases employ-ers feel they are paying for a drug benefitand they’re not sure what outcomesthey’re getting from it.” *** “The largestinsurer here has 75% of the marketplaceand has a drug benefit program thatemployers buy as part of the benefit. Yetthere’s a feeling that employers have of,‘why am I spending all of this money ondrugs when you haven’t shown me any-thing?’ Even in [the insurer’s] disease-management program, drug is an after-thought with them. It’s not an integratedapproach. I haven’t seen anything thatshows an integrated model with good out-comes. [As an employee benefits consult-ing group], we’ve been able to show withsome of the health conditions that byappropriate medical and drug treatments,you can increase employee performance.One example is Heinz. During certaintimes of the year they do a lot of wellnesseducation on allergies and the use ofsedating versus nonsedating becauseHeinz has bought into the model that saysthat nonsedating antihistamines willincrease productivity and are a safety com-ponent. [The employer has] also pushedthis back to the health plan and asked that
the nonsedating antihistamines be placedin an appropriate therapeutic class ofbeing preferred because of the fact thatthey are a manufacturer.”
Government representatives (two oftwo respondents agreed): “Part of whatwe’re trying to do in this Congress isencourage research into what else can bedone with regard to medical errors. Thisis research into how we perceive andaddress the problem, in other words,comparing our medical system to othersystems, such as the airline industry, andhow they handle problems. It includesconducting some of the research that hasnot been done on drug-drug interactions.We don’t have hard research that we cantell doctors and pharmacists about cer-tain things.”
Health plan administrators (three offive respondents agreed): “There are no uni-versally applied effective systems in place.HEDIS [the Health Plan Employer Dataand Information Set] is not addressing thedrug therapy process—and should.” ***“I think the system is much more proac-tive and is working well. People are gettingin the system earlier because they are moreknowledgeable and more have health cov-erage than ever before.”
Patients (two of two respondents agreed):“Consumers, even advocates, don’t under-stand where health care decisions (muchless process decisions) are being made.That process is closed and there’s no wayfor consumers to really know what’s goingon. Nor do all consumers always have anadequate appeals process or independentreview. They should have that as well.Certainly decisions (about what drugs toinclude in a health plan) should be made,but how we do that is more difficult.”
Physicians (three of three respondentsdisagreed): “The current system is moder-ately effective at identifying and resolvingdrug errors and adverse events. I alwaysfound it kind of a joke that the FDA[Food and Drug Administration] sendsout the forms doctors are supposed to fillout when they identify adverse drug reac-tions. Now I don’t know any doctors thatfill those out. They may see an adverse
reaction—the side effects of something—and unless the pharmacist finds outabout it, which I think they’re better atidentifying and reporting, it’s overall amoderate effort. Certainly the more majorevents are likely to be reported, wheresomeone has been hospitalized.”
(2) Linked computer systems wouldhelp better identify potential adversedrug events.Academicians (two of two respondentsagreed): “Pharmacy-based informationsystems are rarely used, and if used,there’s no payor on the other end to rec-ognize the value of those services. Thesetype of programs are successful at reduc-ing total [health care] costs, but theyalways increase drug therapy costs.”
Drug manufacturers (two of two respon-dents agreed): “[This is also] a systems issue.There aren’t systems in place to do thingslike provide outcomes data. If in fact wehad a true physician/patient interactionsystem, something that captures electron-ically that interaction in the doctor’soffice and is put into a database, then youwould have real-time studies. We missthe opportunity as soon as that patientsits down with the physician. The infor-mation, including the prescription, getsput on a piece of paper and gets filedaway and is inaccessible to the rest of thehealth care scheme in most cases. That’swhy I think an electronic patient recordform in U.S. health care would changethe dynamics of health care delivery.”
Employer purchasers (four of fourrespondents agreed): “PBMs [pharmacy ben-efit management companies] have done anexcellent job with the messaging systemsin place—we don’t have that on the med-ical side. Pharmacy has been up to speedwith technology, but it’s a shame that wedon’t use it to get the pharmacist involvedin it up front. Especially with all thatpoint-of-care technology they talk abouttoday. A physician could just do the diag-nosing and this technology could help thedoctor prescribe the right drug based onthe plan’s formulary and other conditionsthe patient has.”

Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
Government representatives: (two oftwo respondents agreed) “As a health caresystem, we ought to move toward elec-tronic prescribing and record keeping.But the question is, ‘which sector absorbsthe cost?’ Electronic prescribing andrecord keeping lends itself to electronicpatient compliance as well. There aresome systems that monitor compliancethrough refills. Certainly the pharmacistcan’t be responsible for calling patientsevery four hours to make sure they’re tak-ing their medications. I hear about sys-tems that are in place in pharmacieswhere they flag drug-drug interactionsbefore they’re filled, so either the phar-macists are escaping right past the flag orare turning the system off because it’s anuisance, and because they are thin ontheir margins.”
Health plan administrators (five of fiverespondents agreed): Linked systems aregood, but certain efforts, like routine andpreventive care is “best carried out by non-MD types.” *** “The only time we see anyattempt at this [linking systems] is whenwe have money, but it usually falls by thewayside for other things. It happens everythree to five years. So we don’t get very farbecause it’s just too complex to try todevelop and link everything. Plus, withpeople moving in and out of plans, thatmakes it hard to do long-term studies. Ithink what will happen in the future isthat a SmithKline or a Merck will opentheir own disease-centric sites, such as adiabetes center, and have people get a fullarray of services for their conditions.”
Patients (two of two respondents agreed):“The resources that consumers are using toget information are the Internet; talking todoctors, pharmacists, friends, and relatives;and TV and radio.”
Physicians (three of three respondentsagreed): “Improved automation and theapplication of technology [are needed]where doctors don’t have to think abouttheir selection of drugs or scheduling offollow-up. Patients may change doctorsand health plans, so a common data-base—a linking of databases by sharing of
data electronically—would be very help-ful.” *** “There are emerging more andmore automated systems to try and catchpotential drug-drug interactions, identifyallergies, and these kinds of things beforedrugs are delivered. That will work bestwhere the patient gets all their medicationsat one pharmacy or one pharmacy chain.”
Care Is Coordinated All respondents believed that coordina-tion of drug therapy is particularly essen-tial when care is provided by multiplehealth care professionals. They also saidthat communication among suchproviders is important. However, whilemany providers are competent, mostrespondents said that: (1) Few pharma-cists are involved in collaborative, multi-disciplinary care; and (2) the drug thera-py process is still very much a paper-based, nonintegrated system that willrequire an investment in computer sys-tems to coordinate and integrate medicaland pharmacy information.
(1) Pharmacists are involved in multi-disciplinary care.Academicians (two of two respondents dis-agreed): “This is not often achieved. Insome areas, such as diabetes and asthma,pharmacists are involved, but there arecertain areas where they aren’t and wherecompliance is very important, such ashypertension.”
Drug manufacturers (two of two respon-dents disagreed): “So much of a pharma-cist’s job is regarded as physical dispens-ing: interpreting the prescription correct-ly, drawing it down from the inventory,counting out the requisite number oftablets, and then getting it to the patient,and increasingly, within the constraints ofwhatever health plan the patient is cov-ered by. There is a whole other aspect ofpharmacy, which is counseling and drug-utilization review, and even screening. Ina hospital setting where you have asalaried pharmacist, they probably prac-tice many of these broader disciplines.”
Employer purchasers (four of four
respondents disagreed): “In California, biggroup practices have—from what I’veheard—pharmacists on staff. I think that’sideal. Pharmacists should be working inthe outpatient arena, not just the drugstores, but for groups of physicians theyshould be consultants providing theirexpertise. Perhaps they’re reviewing aweek’s worth of cases that a doctor mightsee to see what drugs have been pre-scribed and what may or may not havebeen prescribed appropriately. If doctorsdon’t have time to go back and checkeverything about a patient, to know thatsomeone is monitoring them [is good].Basically now there is no accountability.There might be in the hospital, but thereisn’t on the outpatient side.”
Government representatives (two oftwo respondents disagreed): “Certainly thePBMs and managed care plans have beenoutspoken in demonstrating how theyhave the ability to operate effective dis-ease-management programs. But the phar-macist has to be an integral part of that.”
Health plan administrators: (four offive respondents disagreed): “Pharmacists areoften among the first to see things goingwrong with patient compliance becausepatients come in for refills more frequent-ly than they go for doctor visits—yet theyare out of the loop with other providers,”says one administrator. He continues,“There’s an opportunity for quality con-trol. They could reinforce preventive serv-ices—remind patients to get a mammo-gram or make sure the kids are immu-nized.”
Patients (two of two respondents dis-agreed): “I don’t know that people think oftheir pharmacists as a key player in the useof pharmaceuticals. When I ask pharma-cists a question, I feel like I’m botheringthem. In fact, when I go to pick up myprescription, I’m asked to sign a form,which automatically includes the sticker, ‘Ido not want consultation.’ When you sign,it looks like you’re signing for your drug.But there’s an assumption that you do notwant a consultation. It certainly doesn’tsuggest to someone that, ‘Oh, I can talk to
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 195

Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
196 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
my pharmacist about this.”Physicians (three of three respondents
disagreed): “The pharmacist shouldn’t justbe the lackey of the physician—‘do what-ever I say.’ A relationship between thephysician and clinical pharmacist [should]set some guidelines or norms as far as thatrelationship and making decisions. Also,clinical pharmacy management programsshould be monitoring and measuring theirresults and outcomes and have that betheir ‘truth in advertising.’ It would letthe referrers—the physicians—knowwhat results you get.”
There Is Value in the Care that PatientsReceive, and It Is Affordable All the respondents believe that drug ther-apy plays an important role in the qualityof care patients receive. However, theyvary in the degree to which they feel that:(1) the cost of drug therapy is an impor-tant consideration in the selection of drug-therapy options; (2) the value of drugtherapy is demonstrated in improvedhealth and higher employee productivity;and (3) the value of drug therapy is reflect-ed through lower drug benefit costs.
(1) Drug cost should be considered intherapy selection.Academicians (two of two respondentsagreed): “Drug formularies can get at drugcosts, but recommendations around use ofcertain drugs—evidence and supportinginformation—should be used.”
Drug manufacturers: (two of tworespondents agreed): “I do constantlyremind people that price increases are asmall portion of the total, and in fact, rel-ative to what the newer products do ver-sus the older products. We have to keepin mind is that we’re talking aboutimproved quality of life, the ability tokeep people out of the hospital; then theanswer is; there should be cost-benefitthere. But it is a very difficult argument toget people to focus on.”
Employer purchasers (four of fourrespondents agreed): “[The cost of drugs] isnot painful for most consumers, but it isif you don’t have coverage.”
Government representatives (bothrespondents both agreed and disagreed): “Insome cases cost is an important considera-tion. Nowadays with chronic illnesses, likeAlzheimer’s, the two drugs price-wise arethe same. If you focus too much on costsavings, you don’t get the full picture ofappropriate use. Health care is not like acontract with the defense departmentwhere you’re ordering parts.”
Health plan administrators (five offive respondents agreed): “Health plansshould be talking with the pharmacistsand vice versa regarding what the healthplan is doing regarding therapy deci-sions. On our part—and we should bedoing this and we’re not—health plansshould be educating the pharmacistsabout what the P&T [pharmacy and ther-apeutics] committee is doing and involvethem in our therapy decisions.” *** “Ifyou can determine that you have a drugthat has the same effect as another drugand is half the cost of that other drug, itwould be negligent to purchase one thatcosts twice as much.”
Patients (two of two respondents agreed):“A lot of Medicare beneficiaries havejoined HMOs, mostly because of the pre-scription drug coverage. But now thatthat’s being decreased quite a bit and thereare more expensive drugs, they have a lotof anxiety about how they’re going to con-tinue to pay for their drugs. There’s also aconcern [among consumers] about risinginsurance costs, and formularies and theirrestrictions. They feel, and appropriatelyso, that these decisions are made by man-aged care companies with only the cost inmind, and that the physicians have beenbrought into the process of rationalizingthe cost of drugs.”
Physicians (three of three respondentsagreed): “It would be inappropriate to notweigh in the cost. Cost to the individualmember, but overall cost to the healthplan, then the employer, and then thesociety—patients and doctors need tomake that link more often. Even thoughthe copayment may be only $5, and it’sone of the more expensive drugs, weought to be looking at alternatives
because there are limited resources outthere.” *** “Yes, cost should be consid-ered for multiple reasons: (1) manypatients still pay out of pocket for drugs;(2) as a societal issue, the more expensivedrugs are not always the better drugs (wecould talk for hours about the pressuresof direct-to-consumer advertising and thelack of balance of information about ther-apeutic options); and (3) most physiciansdon’t know what the cost of drugs is. Inour system, we frequently get little state-ments/reports from the pharmacy com-paring the cost of different drugs and it’seye-opening. It makes me questionwhether the drug that costs 10 timesmore than the other drug is better.”
(2) Drug therapy value reflects improvedhealth and higher employee productivity.Academicians (two of two respondents dis-agreed): There is significant lack ofaccountability in drug therapy, says oneacademician: For example, he says, “ahealth plan fragments the system when itturns the drug therapy benefit over to acompany like PCS, who in turn canrestrict the formulary and has carteblanche to do whatever they can to man-age the budget. The fact that they’re notmanaging hypertension patients with opti-mum drug therapy, for example, is irrele-vant. They’re reducing drug costs andthat’s what they’re paid to do.” *** “Theflaw in the current system is that it’s not inthe managed care organization’s benefit todo things that will prevent the disease intwo to five years because the patient maynot be covered by the plan for more thanone year. So there’s no incentive for themanaged care organization to work withpeople on smoking cessation and weightcontrol and exercise, because that’s notgoing to save money now.”
Drug manufacturers (two of tworespondents agreed): “I think you have tolook at the value of the pharmaceuticals,not the cost, and that we do that in every-thing we purchase. We trade off the costof what we’re going to pay versus thebenefits that we’ll receive.”
Employer purchasers (four of four

respondents disagreed): “Disease manage-ment is a positive step in the right direc-tion, but the danger is that the pharma-ceutical industry has jumped on thatbandwagon and gotten into that businessand in a very subtle way is trying to pro-mote the use of their drugs. They nevername the drug specifically, but they see itas a marketing strategy. [As an employer],I would not use those programs because Isee a conflict of interest. PBMs are suspect,too, because of their rebate incentives.”*** “Unlike larger employers, smallemployers lack the sophistication abouthealth care quality. It’s perhaps the less-mature managed care markets where thoseemployers lack that kind of sophisticationto get past costs. You’ve got to get past thatbecause if you can improve health out-comes, you will eventually improve costs.As an example, a lot of employers todaywon’t cover Zenecal for obesity, and theydon’t understand the kind of morbidityassociated with weight gain and [that] ifyou can reduce weight you can reducecholesterol and diabetes-related incidents.I think we’re at a point right now wherewe need to educate employers about totalhealth outcomes.”
Government representatives (two oftwo respondents disagreed): “The drug-uti-lization review system is how we identifyprescribing patterns [for Medicaid] and ithas been effective, but generally, systemsaren’t in place in our health care system todetermine if patients are getting the appro-priate therapy for their conditions.”
Health plan administrators (five offive respondents disagreed):u
Patients (two of two respondents dis-agreed): “I don’t know that people think oftheir pharmacist as a key player in the useof pharmaceuticals. I know when I askpharmacists a question, I feel like I’mbothering them. In fact, when I go to pickup my prescription, I’m asked to sign aform, which automatically includes thesticker, ‘I do not want consultation.’ Whenyou sign, it looks like you’re signing foryour drug. There’s an assumption that youdo not want a consultation. It certainlydoesn’t suggest to someone that, ‘Oh, I can
talk to my pharmacist about this.’”***“There’s really a lack of good data analyz-ing the value of drug therapy right now.And what I mean by value is the mosteffective drug. They’re not capturing thatdata—I’m not sure they’re asking the rightquestions.”
Physicians (three of three respondentsdisagreed): “Patients want to do the bestthey can, but they face a barrier in that ifthe cost is too high and even if that’s whatthey know that’s what they should take,they’re not going to be able to [afford it]. Amajor barrier [to good outcomes/compli-ance] is dosing: patients with one- or two-times-a-day medications will have bettercompliance than those who have three- orfour-times-a-day dosing requirements.”
(3) Drug therapy value is reflected inlower drug benefit costs.Academicians (two of two respondents dis-agreed): See #2.
Drug manufacturers (two of two agreed):“Employers have been asking health plansto carry [most of] the burden of the cost ofdrugs. The health plans are very mindful ofit. Because they are measured on thosebudgets, they have more or less the abilityto impact that depending on the amount ofthe control they have over being able todirect drug therapy to patients.”
Employer purchasers (four of fourrespondents disagreed): It is possible for thevalue of the drug therapy to be reflected inthe drug benefit, says one respondent. “Themanaged care and pharmaceutical indus-tries think that employers have tons ofresources that they can purchase these [dis-ease-management programs] when in reali-ty the HR [human resources] and benefitsbudgets are just squeezed like you wouldn’tbelieve. Take health-risk assessments[HRAs]. If a company were doing annualHRAs that loaded into a database, I thinkyou could really find a lot of potential,undiagnosed folks and recommend them toa primary care physician for screening orevaluation, but in reality, very few employ-ers do health-risk assessments. It would benice if some MCOs [managed care organi-zations] or PBMs could include that.”
Government representatives (two oftwo respondents disagreed):u
Health plan administrators (four offive respondents disagreed): Drug therapyvalue would be best reflected if “doctorswould diagnose the illness and the phar-macists would prescribe the medicine. Iwould like to see that happen because thepharmacist is more attuned to the med-ications than the doctors are.”
Patients (two of two respondents dis-agreed): “There’s concern [among con-sumers] about formularies and theirrestrictions. They feel, and appropriatelyso, that these decisions are made by man-aged care companies with only the cost inmind, and that the physicians have beenbrought into the process of rationalizingthe cost of drugs.”
Physicians (three of three respondentsdisagreed): “One of the concerns I have isthat because of the payment systems andthe at-risk systems and the preauthoriza-tion systems, it’s often putting the phar-macist in the uncomfortable position oftrying to broker what the health plan isdemanding—‘We won’t pay for thisdrug’—and what the physician wants toprescribe. That’s a very difficult andunreasonable position. It’s less a discus-sion around appropriate therapy optionsthan it is what will the health plan orinsurance company pay for.” *** “MCOscan and sometimes do change formula-ries frequently, which can change thepatient’s medication, so that’s been at theMCO’s request, not the physician’s or thepatient’s request. Trying to coordinate thedrug therapy of a patient who has differ-ent providers is difficult. Also, somepatients don’t understand why you needto treat hypertension for 5 to 10 years toget any benefit. They may think that ‘IfI’m not getting a benefit immediately,then I don’t need to stay on the medica-tion.’ I think we as society look for animmediate fix, an immediate cure, anddon’t look for the long term.”
The System Is Accessible and IsLooking Out for the Patient’s BestInterest
Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 197

In terms of this expectation, respondentsbelieved that: (1) most pharmacists donot have access to clinical and patientdata, but they disagree on whether theyshould; and (2) pharmacists must do abetter job coordinating drug therapyconcerns through coordination of carewith other providers or throughenhanced patient services.
(1) Give pharmacists access to patientdata.Academicians (two of two respondentsagreed): “The dispenser has almost noneof the clinical data to help assure appro-priate drug therapy—it obviously wouldhelp. Currently [the exchange of suchdata] is at a pretty low level.”
Drug manufacturers (two of two respon-dents agreed): “Managed care pharmacy isn’tinvolved in the physical act of dispensing,therefore they can be involved in the act ofthinking through how pharmacy careshould be delivered. They have access todata on individual patients and all patientsin the system. Access to those data, partic-ularly if it’s integrated with the medicaldiagnosis data—in other words, being ableto cross-integrate the diagnosis, treatment,and the outcomes—is a huge potentialadvantage for managed care pharmacy.”
Employer purchasers (four of fourrespondents agreed): “The model I’vealways tried to encourage people to thinkabout is a system where the pharmacist isa primary care provider, where the phar-macist gets involved at the prescribinglevel with the physician at the drug-selection process. Our system todaydoesn’t support that for a couple reasons:Physicians wouldn’t allow that to happenbecause it would mean lost revenue forthem, and pharmacists don’t have theadequate training or resources to makethat happen. Some chains are trying toimprove that with counseling centers.”
Government representatives (one oftwo respondents agreed): “There will alwaysbe a constant push and pull between thedoctors, and I’m not sure I want to weighin on that yet because I am a laypersonwhen it comes to these areas. But I think
that that is one place where the more inte-grated systems of health care delivery havean advantage, and to the extent to whichwe are moving away from integrated sys-tems is a disadvantage.”
Health plan administrators (four offive respondents agreed): “Pharmacistsshould have access to such data. It’s defi-nitely important for them to understandwhat’s being prescribed and are there anyother contraindications out there. It is nottheir place to question what the therapyoutlines are, but they should be able tohave access to all pertinent data. This is amajor quality part of the equation.” ***“Our clinical information system is set upso that our physicians and pharmacistscan see what drugs the patient is on. Ifeither party has questions about thepatient, they have the ability through thissystem to easily share information andconcerns. We have taken further stepswith additional programs to improve drugtherapy outcomes. We have an anti-coag-ulation clinic that just focuses on patientswho are on anti-coagulation drugs; theclinical pharmacists run that programwith the physicians’ input.”
Patients (two of two agreed): Whilerespondents agreed with this type of col-laboration, they also felt that physiciansshould decide what type of drug patientsget: “Ultimately patients should get thedrug that their physician says they shouldget and it should be the physician whodetermines whether the drug is effectiveor not, and if it is determined to be effec-tive, that the drug should be covered andcovered at the copayment of the [healthplan’s] preferred drug. So, for instance, ifthe plan only covers a certain drug for aparticular condition, but the physicianfeels another drug is more effective, theplan should [allow] the [patient to havethe same] copayment for the physician-recommended drug as its preferred drug.”
Physicians (two of three respondentsagreed): “I think pharmacists should havea moderate amount of patient clinicaldata, definitely allergy, and certainlyother medications. I’m not sure theyneed the full patient record from the doc-
tor visit, with the detail of medical histo-ry.” *** “Many pharmacies have put inmonitoring systems—do they haveaccess to all patient data, clinical labresults? No. Nor do pharmacists haveinformation about other drugs patientsmay be taking. I think good clinicalpharmacists are looking out for thepatients’ best interest but are handi-capped by the lack of patient informationand lack of reimbursements for efforts tobetter monitor and manage patients.”*** “Physicians have been recoiling, par-ticularly as their incomes have gonedown and they’re feeling hammered onby insurance companies and it makesthem disgruntled and makes them say, ‘Idon’t want my patient to be cared for bya pharmacist or by someone else; I don’twant to share information.’”
(2) Pharmacists must improve drug ther-apy coordination with other providers.Academicians (two of two respondentsagreed): u
Drug manufacturers (two of two respon-dents agreed): “Pharmacists need to collabo-rate with other providers in the system. Ithink the Internet will assist in this collabo-ration. I see a great role for pharmacists indemand-management programs where theyactually monitor and follow patients andproactively call them. I know that managedcare companies are looking at the role ofpharmacists doing this.”
Employer purchasers (four of fourrespondents agreed): u
Government representatives (two oftwo respondents agreed): “Right nowthere’s little teamwork going on in man-aged care—where, for example, a phar-macist has individuals referred to him.That’s what managed care should beabout—professionals working as a team.There needs to be a case manager ormedical social worker to work withpatients. We feel that pharmacists canwork with these individuals more close-ly; there’s a lot of potential for pharma-cists to take on this role. I think otherhealth professionals—nurses, dieticians,or exercise experts—could be a part of
Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
198 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3

Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
this. The pharmacist is the best person tobe there to counsel the patient for per-sons taking multiple drugs, especiallypeople with chronic conditions.”
Health plan administrators (five offive respondents agreed): “In our medicaloffices [group model HMO], we haveclinical pharmacists as well as operationpharmacists in each of those medicaloffices. So the interaction between thenurse practitioner, the pharmacist, thephysician, and the physician assistantoccurs very easily as a result of the factthat they work for the same organizationand have the same common goals.”
Patients (two of two respondents agreed):“I think now there’s a lot of turf battles. Ithink in a lot of other settings—hospitalsand some managed care settings—that’sstarting to change, with pharmacists andphysicians working together as teams withother providers, nurses, etc. It’s been foundthat when doctors and pharmacists worktogether and communicate on a regularbasis, that patient care is better, hospital-ization goes down, and that there are fewererrors, especially medication errors.”
Physicians (three of three respondentsagreed): “In the present setting, I thinkpharmacists could provide checks and bal-ances for doctors, watching for drug inter-actions, potential problems with allergies,giving a certain amount of added educationfor patients, perhaps advising other ancil-lary services or devices that may be usefulto the condition/patient. I would like to seean expanded role for the pharmacist inassistance in drug selection.” *** “As a soci-ety we’re better at reporting on Firestonetires that need to be recalled than to identi-fy patients who need to be on medicationswho aren’t. One obstacle is the feeling thatpharmacists, physicians, any provider thattouches the patient needs to spend less timewith that patient and see more patients inorder to generate an income. In general,patients tend to move around a lot more todoctors and pharmacies and it’s difficult toget the [providers] or their electronic sys-tems to talk to each other.”
The System Will Provide Adequate and
Appropriate Information and EducationRegarding Appropriate Drug Use The interviewees all agreed that informedpatients are the key to improving compli-ance with drug-therapy regimens and toimproving their health outcomes. Therespondents differed somewhat, however,in their perceptions about whetherpatients receive and understand drug ther-apy education, including the purpose fordrug intervention, and therapy optionsincluding lifestyle changes and self-care.
(1) Patients receive and understandtheir drug therapy.Academicians (one of two respondentsagreed): “Patients receive criminally negli-gent information about their drug thera-py. They also do not understand howpoorly their drug therapy is managed.Plus, their expectations are extremelylow.” *** “We’ve transitioned from a timewhere sick patients went to a doctor andtook the prescription and treatment, toone where we’re giving the patients infor-mation and choices about their treat-ment, and they’re making decisionsabout the diagnosis. I think that’s good;the baby boomers are approaching theirsenior years—throughout their lives theyhave demanded responsibility for theirwell-being and they’ll continue to dothat. But while individual physicians mayallow that, the system overall is not set upto do that because the people who pay forthe care may feel differently than the peo-ple who provide the care.”
Drug manufacturers (both agreed anddisagreed): “If you’re a college-educated45-year-old woman who insists on know-ing what your options are—‘What are thedifferent diagnostic tests I can take,’‘What are the different results,’ ‘How doyou interpret the results,’ ‘What’s the vari-ation of response typically with this test,’‘What are my treatment and prescriptionoptions?’—then you’ll generally get agreat deal more information [from thedoctor] and good advice. Someone lesswilling to ask all those questions and whois perhaps less well-educated, and older,may not get the same sort of breadth of dis-
cussion.” *** “AAFP [American Academyof Family Physicians] has encouragedpharmacists to be physician-extenders,which is a first step of what pharmacistscan do. Maybe something that AMCPcould do is look at how to bring thesegroups together to talk more about thesecollaborative things that need to be done.”
Employer purchasers (four of fourrespondents disagreed): “There aren’t a lot ofopportunities for pharmacists to provideclinical intervention/counseling at theretail level because time is not on theirside. Often they just want to give patientsthe prescription without having them waittoo long. Plus, retail pharmacists are oftenunderstaffed. That’s a challenge for anyPBM or that any pharmacy system has onthe retail side. Some PBMs are trying tofind innovative solutions to try to includethe retail pharmacists.” *** “I still see verylittle patient education going on, over thecounter and in terms of follow-up. Fromwhat I’ve seen not a whole lot has changedin maybe 20 years. The pharmacist is byand large busy filling prescriptions, takingcare of paperwork, and following up ontelephone calls.”
Government representatives (two oftwo respondents disagreed): “We hear sto-ries [from consumers] about counselingand compliance, that the counseling isnot being done as it’s intended to bedone. For the large part, I think the busy-ness of the pharmacy is to blame, so thequestion is, ‘How do we relieve the pres-sure on the pharmacist so the pharmacistcan fill in the role that policy makers wouldwant the pharmacist to do?’ Policymakersare clearly aware that we are facing a phar-macist shortage. The question is, are theresome things that can be done in a differentway—pulling pills off shelves, countingpills, utilizing more automated and pack-aging systems—to make it easier for phar-macists to do their job?”
Health plan administrators (three offive respondents agreed): “Less than halfthe diabetics in the United States areunder appropriate therapy. Even underwell-run diabetes-management pro-grams, there’s probably 70% who are
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 199

Designing a Framework for Pharmacy Practice: A Look at Consumer Reactions and Expectations
properly managed. Patients still have lit-tle understanding of their disease. Lessthan a third of patients conclude theircourse of antibiotics appropriately—something as simple as that. We’ve stillgot a long way to go.”
Patients (two of two respondents dis-agreed): While consumers often look todirect-to-consumer ads to get their infor-mation on drugs, “they feel those adsdon’t give them the full informationabout risks and side effects and safetyissues. What they’re doing is looking atthe ads and pulling up more information
on the Internet.”Physicians (three of three respondents
disagreed): “I think education of the patientoften gets short shrift. Patients often don’tget that unless they seek it themselves, askquestions or get it on the Internet. They’vetoo long relied on doctors to spoon-feedthem through the process.”
nnConclusion The AMCP Task Force is continuing itsdeliberations on these findings, and isexpected to have a framework ready forcomment in late 2001. In the meantime,
the project, funded by the Foundation forManaged Care Pharmacy (FMCP), ispreparing a list of critical functions indrug-therapy management, along with anexample of what a perfect score in thatfunction might look like, and a self-assess-ment instrument for pharmacists to deter-mine how well they are prepared to prac-tice at the level of the Framework. Thefinal product will be a generic documentand practice-site blind, but will includespecialty-specific assessments. n
200 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3

Researching Managed Care Pharmacy
PRACTICE F E A T U R E
ncreasingly, the explosion in scien-tific knowledge is overwhelmingboth researchers and practitionersin the health professions. The man-
aged care pharmacist today needs a con-stant and current sense of the basic phar-maceutical sciences, clinical pharmacy,pharmacy management systems, healthpolicy and ethics, new drug introductions,pharmacoeconomics, and pharmacoepi-demiology. Monitoring the ever-changingpharmaceutical industry is now more thana mere pastime.
Fortunately, there has been a correspon-ding growth in support available to thepharmacist manager, practitioner, andresearcher, in the form of free Internetresources and other proprietary databasesthat allow access to published materials,organizational contacts, and other resourcesfor informed decision making.
Evidenced-based clinical approaches,cost-effective care strategies, and programdescriptions and evaluations can all befound in databases described below.
Knowing how to navigate these infor-mation services is crucial to avoiding infor-mation overload. This article will firstdescribe some information retrieval data-bases that can be used to search for articlesrelevant to pharmacy administration. Itwill then outline search criteria to deter-mine the yield of each database anddemonstrate how to decide the relevanceof potential information sources. Werestricted the scope of this article to com-
puter-searchable and accessible databases.
nnBibliographic Databases
The bibliographic database is the most com-mon source for published articles. Most bib-liographic databases allow users to locatearticles by keyword, author, and title. Thesearch results usually yield title, authors,source, and an abstract of the article.
The abstract usually provides enoughinformation about the relevance of an arti-cle to support a decision about whether toobtain a full-text copy. Articles from corejournals can be found in a local library oruniversity library system and sometimesthough an interlibrary loan. Many infor-mation database providers will supply aphotocopy of articles or allow users todownload the article for a fee.
MEDLINEwww.nlm.nih.gov/databases/medline.htmlMEDLINE is the premier medical infor-mation source. Since June 26, 1997, theMEDLINE database has been accessible,free of charge.
MEDLINE covers medicine, nursing,dentistry, veterinary medicine, the healthcare system, and the preclinical sciences.It contains bibliographic informationfrom over 3,900 biomedical journals pub-lished in the United States and 70 foreigncountries, for a total or 9 million recordsdating back to 1966. The database isupdated every week; each month about33,000 new citations are added.
Using “pharmacy,” “pharmaceutical,” or“pharmacist” in keyword searches onMEDLINE produces 14 titles, includingthe American Journal of Health-SystemPharmacy, the Journal of Clinical Pharmacyand Therapeutics, and the Journal of theAmerican Pharmaceutical Association.
Many users find that modifying asearch term even slightly can bring verydifferent results. For example, using“asthma” as a keyword for a MEDLINEsubject search articles brought up 2,262articles.1 However, if “asthmatic” is used,the search produces only 707 articles.Because no mechanism has yet beenestablished to directly link two terms likethis, even a minor difference in phrasingmay mean missing an important article.
A remedy for this problem is to makeuse of NLM’s Medical Subject Headings(MeSH) thesaurus. MeSH indexes articlesin NLM databases using a hierarchical sys-tem to structure a set of terms or subjectheadings. You can choose to either broad-en or narrow the search terms according tothe “tree” structure of the thesaurus, orchoose related terms with which to linkthe tree’s branches. For example, thehierarchical structure of the MeSH term“drug utilization” is:
N. Health CareN4. Health Services Administration
Organization and AdministrationPharmacy Administration
Drug UtilizationDrug Utilization Review
Authors
SWU-JANE LIN, M.S, Ph.D., is Visiting Assistant Professor in Pharmacy Administration, and J. WARREN SALMON, Ph.D., is Professor of PharmacyAdministration, University of Illinois at Chicago, Chicago, IL.
AUTHOR CORRESPONDENCE: Swu-Jane Lin, M.S., Ph.D., University of Illinois at Chicago, 833 S. Wood St., M/C 871, Chicago, IL 60612-7229; Tel: 312-355-5666; Fax: 312-996-0868; E-mail: [email protected].
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
S w u - J a n e L i n a n d J . W a r r e n S a l m o n
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 201
I
Researching Managed Care Pharmacy Using Internet Searches
202 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
Clearly, using MeSH effectively canproduce a search result that is comprehen-sive and consistent. Consequently, theMeSH thesaurus system is now built intoall NLM-produced databases, includingMEDLINE; users simply input any key-word and then select “find MeSH/metaterms.” The system will respond with a listof suggested search terms. For example, ifyou type in “asthmatic” as a keyword, andthen select “find MeSH/meta terms,” theMeSH suggested list of search terms doesindeed include “asthma.”
The MeSH system also provides a“concept” list to help you map a querybetter. For example, using “disease statemanagement” as a keyword on MEDLINEwill return more than 2,000 articles (as ofFebruary 10, 1999), only a few directlyrelated to disease state management pro-grams. To tackle this problem one mustuse a concept as a second search termand once again select “find MeSH/metaterms.” The Internet Grateful Med (aninterface of MEDLINE) will provide a listof meta-thesaurus concepts which willinclude “managed care programs.” Usingthis phrase as a second search term pro-duces 20 fully relevant articles.
Because MEDLINE has a clinical orien-tation, false negatives (failure to retrieverelevant articles) and false positives(retrieval of irrelevant articles) could becommon in searches for articles related toadministration and management. A data-base such as HealthSTAR that is orientedto health service might be of more use.
HealthSTARwww.nlm.nih.gov/pubs/factsheets/online_databases.html#healthstarHealthSTAR is a bibliographic citation data-base created in 1996 by merging two NLMdatabases, HEALTH (Health Planning andAdministration) and HSTAR (HealthServices/Technology Assessment Research).
HealthSTAR contains three million cita-tions from 1975 to the present, both clini-cal (emphasizing the evaluation of patientoutcomes, the effectiveness of procedures,programs, products, services, and process-es) and nonclinical (emphasizing health
care administration, economics, planning,and policy).
IPA (International Pharmaceutical Abstracts)www.ovid.com/databases/index.cfmIPA is the bibliographic database mostspecific to pharmacy administration andpharmacy service research. Produced bythe American Society of Health-SystemPharmacists (ASHSP), it covers approxi-mately 600 titles (“subjects of drug ther-apy, toxicity, pharmacy practice, legisla-tion, regulation, technology, utilization,bio-pharmaceutics, information process-ing, education, economics, and ethics asrelated to pharmaceutical science andpractice”), and contains over 300,000records from 1970 to the present. JMCPis indexed in IPA.
IPA includes all abstracts from ASHSP-annual and midyear clinical and homecare meetings, as well as AmericanPharmaceutical Association (APhA) andAmerican Association of Colleges ofPharmacy (AACP) meetings; articles fromstate pharmacy journals, and articles thatoffer continuing education credit. IPA pro-vides numerous references on topics relat-ing to pharmacoeconomics and pharma-ceutical care. The paper version of thedatabase is updated semi-monthly, and theCD-ROM version is updated monthly.
CINAHL (Cumulative Index to Nursingand Allied Health Literature) www.cinahl.comCINAHL is an index database that coversjournal articles, dissertations, and otherpublications in nursing and allied healthfrom 1982 to the present. It indexes someresearch instruments and provides fulltext of selected others; a special feature isthe collection of nursing standards aswell as the state nursing journals.
The database, www.cinahl.com, pro-duced by CINAHL Information Systems,covers over 950 journals in cardiopul-monary technology, emergency services,health education, med/lab technology,medical assistance, medical records, occu-pational therapy, physical therapy, radio-
logical technology, respiratory therapy,social sciences, and surgical technology,with some attention to biomedicine, thebehavioral sciences, management, andeducation. Currently, the database containsover 250,000 records, is updated monthly,and is available in both CD-ROM andonline. CINAHL indexes 14 pharmacy andpharmacology-related journals.
EMBASE (Excerpta Medica Database)www.elsevier.com EMBASE, the Excerpta Medica databaseproduced by Elsevier Science, indexes liter-ature in biological science, biochemistry,clinical medicine, human medicine, forensicscience, pediatrics, pharmacy, pharmacolo-gy and drug therapy, pharmacoeconomics,psychiatry, public health, biomedical engi-neering and instrumentation, and environ-mental science. Its comprehensive treatmentof drug-related information makes EMBASEobviously useful for drug-related searches.
EMBASE covers over 3,800 journalsfrom approximately 70 countries; it cur-rently contains over 7 million records,adding more than 400,000 each year.Like the NLM databases, EMBASE uses athesaurus system, EMTREE, a hierarchi-cally structured, controlled-subjectvocabulary, to help users retrieve articles.EMTREE contains more than 39,800controlled vocabulary terms (21,240 drugterms and 18,630 medical terms) and120,000 synonyms. The company alsoproduces subsets of EMBASE for specificdisciplines. The EMBASE Pharmacoeco-nomics & Disease Management databaseis devoted to such research areas as healthcare costs, managed care, pharmacoeco-nomics, economic evaluation, healthinsurance, quality of life, treatment out-comes, resource management, hospitalcosts, and practice guidelines. It current-ly contains more than 138,000 abstractsand citations from the past eight years.
nn Tables of Content IndexesA bibliographic database is very usefulfor retrieving information addressing aspecific area of interest, for example,asthma disease management. However,

Researching Managed Care Pharmacy Using Internet Searches
there are times when one might wish tosurvey journals in a particular field towatch for potentially useful implications orapplications or simply in order to keep upwith research in that area. For example, auser interested in asthma disease manage-ment might want to see what is being pub-lished generally in Chest and the Journal ofAmerican Health-System Pharmacy.Databases that provide “tables of contents”can be searched by subject for a quick scanof the titles and authors of articles pub-lished in each issue of a relevant journal tosee which might warrant reading of theabstract or even the full article. Makinggood use of searchable databases for tablesof contents can save time and money.
Current Contents Life Scienceswww.isinet.com/prodserv/cc/ccprod.htmlCurrent Contents, published by the Institutefor Scientific Information, has seven week-ly editions in agriculture, the arts, and oth-ers; medical articles are indexed under LifeSciences. Complete bibliographic data forjournal articles, reviews, editorials, correc-tions, and conference proceedings areincluded, but the database does not provideabstracts. The database is provided in print,CD-ROM, and other media; the print andCD-ROM versions are updated weekly.
Current Contents indexes over 1,370journals. The keywords “pharmacy” or“pharmaceuticals” retrieved 14 pharmacy-related journals.
nn E-mail Service for Tables of ContentSome Web sites of academic associationsand publishers will e-mail tables of con-tents to subscribers, free of charge. Forexample, the American Medical Associa-tion, www.ama-assn.org will e-mail tables ofcontent for nearly a dozen journals, includ-ing JAMA, Archives of Family Medicine, andArchives of Internal Medicine.
The vast majority of journal publish-ers provide tables of contents and oftenabstracts online. Sometimes, one caneven find online the full text of articlesaddressing certain key issues.
nn Full-Text Articles
To accommodate the increasing demandfor remote access to documents, moreand more full-text databases are becom-ing available online. Several proprietarydatabases can be accessed both through alocal library or the Internet.
OVID www.ovid.com/products.cfmThe OVID Company provides six full-textdatabases: the Core Biomedical Collection(CBC), Biomedical Collections II (BC2), III(BC3), and IV (BC4), the Mental HealthCollection (MHC), and the NursingCollection (NURC). The CBC contains arti-cles from 1993 to the present, the othersarticles published after 1995.
The MHC covers 10 journals, each ofthe other five collections about 20 journals.The only journal that contains the wordpharmacy in its title is the American Journalof Health-System Pharmacy in the BC4 data-base. Interested readers should visit the Website for a complete list of included journalnames and some general information aboutthese full-text databases.
ABI/Inform www.oclc.org/oclc/man/6928fsdb/abi_inform.htmThis database compiled by the UMICompany contains citations from 1,805periodicals. Articles included relate to busi-ness and management and have been pub-lished in international professional publica-tions, academic journals, or trade maga-zines. Full text is available online for select-ed periodicals.
Using “health” as the keyword in a titlesearch returns some 29 publications withfull-text articles in the database. These peri-odicals include the Health Care FinancingReview, the Health Care Management Review,Health Services Research, Hospital & HealthNetworks, and the Journal of Health Politics,Policy & Law. Drug Topics and Pharmaceuti-cal Executive both provide full-text articles.Its business and management orientationand the full-text articles make this a partic-ularly convenient resource.
Medscape.com
www.medscape.comSome Web sites that provide information toboth consumers and health professionalsalso provide full-text articles. One isMedscape, which provides the full texts ofselected articles from about 60 medicaljournals and news periodicals, includingDrug Benefit Trends, U.S. Pharmacist, andJMCP. Keyword searching is available.
Again, many journal publishers providefull-text articles on their own sites. Forexample, two years worth of JMCP has beenposted on www.amcp.org, with older issuesbeing added as time permits.
nnCitation DatabaseThe Science Citation Index published bythe Institute for Scientific Informationindexes references (footnotes or bibli-ographies). What makes the SCI differentfrom other bibliographic databases is itsability to track not only references citedby an article, but also articles that havecited that article. The SCI can be used todiscover who is referencing what researchand to track the studies published byothers in a particular field of interest.
SCI thus allows researchers to trackthe history or methodology of an ideasince its first appearance. How often anarticle is cited suggests the impact of thatarticle on the field.
The SCI covers approximately 3,500journals in a broad range of disciplines; itcan be found at www.isinet.com/isi/prod-ucts/citation/sci/index.html. Using “pharma-cy” and “pharmaceutical” as keywordsretrieved 16 journal names, including theAmerican Journal of Health-System Pharmacy,the Journal of Clinical Pharmacy and Ther-apeutics, and Pharmacy World & Science.
nnNewspapers and Magazines
The UMI Company has compiled a data-base that abstracts reports from 32 news-papers, including the New York Times, theWall Street Journal, and the WashingtonPost. Though this is obviously useful, thelack of full-text articles is a disadvantage.
UMI also compiles ProQuest, which
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 203

Researching Managed Care Pharmacy Using Internet Searches
204 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
does provide the full text of articles from150 newspapers. This can be found atwww.umi.com/hp/Features/Papers/Selectable.
Online NewspapersMany newspapers provide free access tonews at their Web sites. As with any otherelectronic data, online articles are search-able and can be saved and categorized.Users who find themselves overwhelmedby the enormous number of news articlesavailable may like to try a filtering program.
A free program, PointCast, can be down-loaded from www.pointcast.com/?pcnidx.PointCast aggregates news and informationfrom over 700 sources and pushes it overthe Internet onto a viewer’s desktop. Thelong list of channels available includes avariety of sources of global and nationalnews, business and industrial news, federaland state government information, and
health care related information. One cantailor these channels to individual needsand interests, or choose to read only a par-ticular section of a single broadcastingchannel, for example, only health-relatedreports on CNN.
Of interest to pharmacists in managedcare will be the link to the F-D-C Reports; thesummary of current articles from more than20 journals provided by SilverPlatterInformation, Inc.; and the daily news releas-es from Johns Hopkins University andHealth System, the NIH, and Reuters HealthInformation Services. The program allowsaccess to AHRQ guidelines, and severalchannels devote themselves almost exclu-sively to managed care, pharmaceuticalindustry, legislative, and regulatory matters.
nnSpecial Purpose Databases
Many public and private organizations that
compile databases covering specific fields ofinterest put their work on the Internet forpublic use. The AHRQ (Agency forHealthcare Research and Quality) providessearchable and downloadable clinical prac-tice guidelines (www.ahrq.gov/data) and theCONQUEST database, which is a compila-tion of clinical performance indicators(www.ahrq.gov/qual/conquest.htm).
The research organization RAND pro-vides a bibliography of health-relatedresearch and a search engine for abstracts ofRAND publications (www.rand.org).
At the CDC Wonder site (wonder.cdc.gov) CDC has put together some 30 datasets, several of which are searchable biblio-graphic databases. CBA/CEA (cost bene-fit/cost effectiveness) provides 3,206 articlesretrieved from MEDLARS, CATLINE, andother sources of health policy, planning,and administration literature. CDP
TABLE 1 Pharmacy-Related Journals Covered and Articles Retrieved From Selected Databases, 1990 toFebruary 1999
MEDLINE HealthSTAR IPAc Science Citation Current Contents Index Expanded and Life Science
Social Science Citation Index
Total journals collected About 3,900 —b About 650 3,500 1,370
Journal titles with keywords pharmacy, 15 —b More than 216 16 14pharmacist, or pharmaceutical
Articles with keyword formulary 590 875 1,233 500 —
Articles with keywordsa 1,467 20,562 90 11 —d
disease state management
Articles with keywords economic 19 49 9 3 —d
evaluation and pharmaceuticals
Articles with keywords 46 59 27 2 —d
pharmacy network
Articles with keywords quality 394 245 22 0 —d
and pharmacy servicesaWhen more than one keyword is used as a search term, the retrieving logic looks to see if the keywords appear in a citation, but not necessarily in the order as inputted by theuser or as a specific phrase. Therefore, a user typing disease state management as keywords could retrieve an enormous number of irrelevant articles. Strategies to improvesearch results are explained in the text.bHealthSTAR collected articles from a variety of sources, and a detailed list of all information sources is not available.cThis is only the estimated number of journal listings due to the use of abbreviations; consequently, one may have failed to retrieve some journals in IPA.dCurrent Contents is a journal-based database, and keyword searches for articles are, therefore, not available.Note: MEDLINE has the most sophisticated searching mechanism, processing keywords through a set of Automatic Term Mapping functions and matching them against a MeSHtranslation table, a journals translation table, and a phrase list. Some proprietary databases may match keywords with words in titles, abstracts, or keyword listed in an article inorder to retrieve their search results.

(Chronic Disease Prevention) containsthree bibliographic databases. The HealthPromotion and Education database may be
Continued on page 213
of most interest to managed care pharma-cists, as it contains over 20,000 biblio-graphic citations and abstracts on diseaseprevention and health promotion. TheMMWR (Morbidity and Mortality WeeklyReport) data set contains articles publishedin MMWR since 1982. Queries can be per-formed at the CDC Wonder site to find cen-sus, morbidity, and mortality data for sub-groups of the U.S. population.
Toolbox for Health Managers and Ad-ministrators (www.pohly.com/about.shtml) isa Web site maintained by a managementconsulting firm that has a large number oflinks to health economics, medical andinsurance legislation, industry news, legalissues, regulatory, policy, and business plan-ning resources on the Internet.
The Center for Health Care Strategies isa nonprofit organization affiliated with theWoodrow Wilson School of Public andInternational Affairs at PrincetonUniversity. The Center carries out andfunds research on Medicaid managed-careprograms and on chronic illness. Its Website (www.chcs.org/chcsinfo.htm) summa-rizes research undertaken by the Centerand has an index of issues in Medicaidmanaged care and a list of relevant links.
nnGuide to SearchesTable 1 illustrates the differences betweensome of the databases discussed andshows how they can be used efficientlyacross a small sample of pharmacy admin-istration topics.
The problems arising when searchingthe information retrieval databases con-cern how to select both the appropriatedatabase and the appropriate search termor strategy. An inappropriate database willhave low relevance to the study topic. Forexample, using pharmaceutical care askeywords in a MEDLINE search for arti-cles published after 1990 will retrievemore than 1,700 articles, but most con-cern the biological or clinical study ofpharmaceuticals. This demonstrates that
searching a concept against databases thatare not designed to cover it will result in asignificant number of false positive hits.Moreover, inappropriate database selec-tion may cause a number of false negativesas well. For example, since the Journal ofHealth Economics is not indexed in MED-LINE, a MEDLINE search will fail to toretrieve any articles from it.
Until an automatic tool is available, itis probably best to use IPA as the startingpoint for searches relating to managedcare pharmacy. For a broader scope,HealthSTAR is also useful to search. SinceHealthSTAR allows users to includehealth articles indexed by MEDLINE inthe same query process, there is no needto repeat the query later in MEDLINEitself. Users may, however, sometimesneed to consult MEDLINE for back-ground articles, such as those addressingdisease biology, pharmacology, or theclinical effects of pharmaceuticals.
For users who need to address gener-al economic or managerial studies, data-bases include EcoLite, produced by theJournal of Economic Literature, and ABIINFORM. On the other hand, users witha narrower field of interest should look todatabases that claim to provide the spe-cific information. For example, EMBASEclaims to collect a large number of articleson pharmacoeconomics.
The phrasing of a query term and thesearch strategy employed can also affectthe hit and miss rate of a search. For exam-ple, some databases allow users to targetsearches by placing double quotationmarks around the search phrase. If phar-maceutical care is used as a query term inMEDLINE to search for articles publishedafter 1990, 1,760 citations are returned. If“pharmaceutical care” (with double quota-tion marks) is used, the result is a smallerbut markedly more relevant 298 articles.
The problem is worsened when differ-ent databases interpret the same query dif-ferently. In MEDLINE, the query term dis-ease state management will be interpretedas meaning any articles that have any ofthose three words appearing in any cita-tion field. As a result, thousands of cita-
tions, mostly irrelevant, will be retrieved.If the same term is used to conduct asearch on IPA, a much more modest num-ber of articles will be recovered, but theywill be much more relevant.
Three simple rules may make databasesearching more effective for researchers: • Spend a little time learning about the
scope and focus of any database youintend to search.
• Use “force mapping” (double quotesaround the phrase) for specific phraseswhenever possible.
• Use multiple search terms to refine yourquery; for example, by adding a conceptterm from the MeSH thesaurus.
Bearing these three rules in mind willgreatly enhance the quality of Internetsearch results.
nnConclusionThis article has delineated informationretrieval resources to benefit managedcare pharmacy and offered practical sug-gestions for their use.
Information about the health sciencesis continually altering and expanding,making it, as a body of knowledge, everharder to master. 2
In the future, intelligent informationfiltering systems will help users facedwith large volumes of information byautomatically retrieving and then filteringupdates of relevant new medical informa-tion.3 These filtering systems will recordthe online behavior of the user, creating aprofile of index terms contained in Webpages noted previously. In essence, infor-mation retrieval systems will take intoaccount the user’s dynamically changingcriteria of relevance.
References
1. Accessed November 5, 1998.
2. Hubbs PR et al. Medical information on theInternet. JAMA 1998; 280(15): 1363.
3. Quintana Y. Intelligent medical information fil-tering. International J of Medical Informatics 1998;51: 197–204.
Note
In just the last month (April 2001), the NationalLibrary of Medicine has integrated the MEDLINE
Researching Managed Care Pharmacy Using Internet Searches
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 213

214 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
OBJECTIVE: A pilot project was de-signed to utilize the knowledge andskills of pharmacists and social work-ers/mental health professionals to facil-itate readiness and informed decisionmaking to optimize antiretroviral thera-py adherence for HIV-positive patientsconsidering or beginning drug therapy.
SETTING: Group Health Cooperative incollaboration with Kaiser PermanenteNorthwest, both group-model healthmaintenance organizations (HMOs) inthe Pacific Northwest.
DESIGN: The Anti-RetroviralMedication Adherence Program(ARMAP) Team at each site consistedof one pharmacist and one socialworker or mental health therapist.Together, the team provided educationand psychosocial support to patientscontemplating, initiating, or reinitiatingantiretrovirals. The focus was onincreasing patient knowledge, identi-fying and addressing adherence barri-ers, and helping patients cope withlifestyle changes associated with inte-grating antiretroviral medications intotheir lives. Specific self-managementadherence behaviors and therapy
goals were designed individually.
MAIN OUTCOME MEASURES: Adherenceas measured by refill data and patientsatisfaction. Laboratory values for HIV-RNA viral load and CD4+ cell count,self-reported adherence, health status,and provider satisfaction were second-ary measures.
RESULTS: Pharmacy refill data andadherence questionnaires showedthree-month adherence rates of 83%and 91%, respectively. All patientrespondents indicated overall satisfac-tion with ARMAP. Ninety-two percentreported increased understanding ofantiretroviral medications. Ninety-twopercent of providers were satisfiedwith ARMAP.
CONCLUSION: Adherence to antiretro-virals was high for ARMAP partici-pants. Patients and providers weresatisfied with ARMAP and were able tobetter understand readiness to initiatetherapy.
KEYWORDS: HIV, antiretrovirals, adher-ence, patient satisfaction, multidisci-plinary team
A Team Approach to Address Antiretroviral TherapyAdherence Barriers in a Managed Care Organization
RESEARCH
SUNSHINE D. SOMMERS, M.S., is Pharmaceutical Outcomes Evaluator,Pharmacy Administration; DANIEL J. KENT, R.Ph., is Clinical InfectiousDisease Specialist/Co-Investigator, Pharmacy Administration; and BETH BEAM,M.S.W., C.S.W., is ARMAP Project Site Director/ Co-Investigator, Group HealthCooperative, Seattle, WA. MYDE BOLES, Ph.D., is Investigator, Center forHealth Research, and DIANA ANTONISKIS, M.D., is Director of ClinicalResearch, Immune Deficiency Clinic, Kaiser Permanente Northwest, Seattle, WA.
AUTHOR CORRESPONDENCE: Sunshine Sommers: 12400 E. Marginal WaySouth, Seattle WA, 98168; Tel: 206-901-4003; Fax: 206-901-4410; E-mail:[email protected]
ACKNOWLDEGMENT: We wish to acknowledge the contribution of ourAdherence Team members Stuart O’Brochta, R.Ph., John McManus, M.A.,Midge Levy, M.S.W., A.C.S.W., Jeri Thonstad, R.Ph., Phyllis Heims, M.S.W., andDean Clay, Ph.D., without whom our successful adherence intervention wouldnot have been possible. We also wish to express our gratitude to Ted Eytan,M.D., M.P.H., for his thoughtful input and to Heather Houston and Liz Follmerfor superb project management.
The project was supported by grant #101-9063 from the Garfield MemorialFund.
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
Authors
uboptimal medication adherence is one of the mostdifficult and complex problems that health careproviders and patients face. Nonadherence has beendescribed for almost every situation that requires med-ication therapy. 1–3 The National Pharmaceutical
Council’s Task Force for Compliance estimated the economicimpact of nonadherence in 1993 alone to be $100 billion dol-lars in health care and productivity costs.4
Many studies have attempted to identify predictors of non-adherence, particularly patient personality traits and sociodem-ographic factors.5, 6 This would allow health care providers totarget adherence-enhancement tools and programs to at-riskpatient populations. More recently, nonadherence has beenidentified as a problem that spans the population and is diffi-cult to predict, indicating that individualized treatment planstaking patients’ preferences, goals, concerns, and circum-stances into account may be a more effective approach toimproving adherence.7
Although personality traits and sociodemographic charac-teristics may not help clinicians predict adherence, characteris-tics of the medication regimen, the extent of patient involve-ment in treatment decisions, and the patient’s perception ofsupport from the health care team have been consistently asso-ciated with adherence and should be considered when creatingpatient care plans.8–10 Adherence to care plans and medicationsalso has been found to increase as patients gain knowledge.11
Treatment regimens for human immunodeficiency virus(HIV) are complex, usually involving at least three drugs and upto 25 pills daily. Many of the medications must be taken specifi-cally with food or in a fasting state, and at prescribed intervals.Side effects are common, and patients will likely take antiretro-virals for life, factors that have been linked to nonadherence.12, 13
Overcoming medication-adherence barriers is particularlycritical in HIV treatment. Sporadic use of protease inhibitors hasbeen associated with the emergence of drug-resistant strains ofHIV.14, 15 This has significant personal and public health implica-tions. Resistance to one drug may lead to cross-resistance toother drugs in the same class, limiting future treatment options.Multidrug-resistant strains also may be transmissible. 16
Some practitioners withhold triple-drug therapy in cases inwhich nonadherence is predicted.17 Critics of this approach saythat it unfairly penalizes patients based on race, mental healthstatus, or substance-abuse history, characteristics that are often
S
by Sunshine D. Sommers, Daniel J. Kent, Beth Beam, Myde Boles, and Diana Antoniskis

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 215
A Team Approach to Address Antiretroviral Therapy Adherence Barriers in a Managed Care Organization
viewed as predictive of nonadherence, despite the lack of con-sistent evidence in the literature.7 Preliminary evidence exists thateffective therapy is being withheld from certain populations.18
Readiness to change health behaviors has been described inthe literature and has been used to predict treatment success.19, 20
The asymptomatic HIV-positive population contemplating thelifestyle changes necessary to initiate antiretroviral therapy hasnot been well studied. The nonurgent nature of initiating drugtherapy in these patients has been described, allowing patientreadiness to become a crucial component of the decision to startantiretroviral drug therapy.21, 22 A major limitation of early aggres-sive HIV treatment without regard to readiness to adhere is thatpoor adherence leads to treatment failure. In a study of the linkbetween protease-inhibitor adherence and treatment success,researchers found that while 95% adherence correlated to an 80%success rate (defined as an undetectable plasma HIV RNA level),80% adherence was associated with a 50% success rate.23
Once an individual’s state of readiness to begin antiretroviraltherapy is understood, regimen-specific barriers to adherencemay be addressed. Programs that demonstrate success byenhancing adherence are complex, making it difficult to justifyoffering only one adherence-enhancement tool to patients andto determine the merits of an individual tool.24 Essential HIV-specific elements of a treatment plan have been proposed. Theseinclude the use of jellybean trials, viral load and T-cell counts,and medication diaries as patient-feedback tools.8 Other toolsthat have been used to support adherence include havingpatients associate pill taking with other activities, reminder tim-ing devices, social supports, and drug-information hotlines.25
nnProgram Description This report describes the Anti-Retroviral Medication AdherenceProgram (ARMAP) pilot project implemented at Group HealthCooperative (GHC) and Kaiser Permanente Northwest (KPNW).The program’s patient and provider acceptability and its associa-tion with adherence and disease regression are reported. The pro-gram was initiated in order to use the combined knowledge andskills of pharmacists and social workers/mental health profes-sionals to facilitate informed decision making, help patients setrealistic goals for adherence through better understanding of per-sonal barriers, and optimize antiretroviral therapy adherence byproviding regular follow-up for drug management.
The program was developed in response to issues raised in aconsumer focus group on HIV care. A general lack of awarenessof the importance of adherence and lack of knowledge aboutavailable adherence tools were identified in the focus group.
In preparation for ARMAP, the adherence team memberswere trained in interview and motivation techniques. A thor-ough review of adherence issues and current HIV treatment rec-ommendations was provided.
The pilot program was launched in October 1998, and enroll-ment occurred through February 1999. The ARMAP team at each
site consisted of one clinical pharmacist and one social worker (atGHC) or mental health therapist (at KPNW). At GHC, primarycare providers located throughout the service region manage HIV-positive patients, while at KPNW HIV-positive patients are treat-ed at a centrally located Immune Deficiency Clinic. Adult patientswere eligible for inclusion if they were candidates for antiretrovi-ral therapy and had not been on antiretrovirals in the previousthree months.
The ARMAP teams were established to address the education-al needs of the providers and patients in order to optimize adher-ence potential prior to the initiation of therapy. Troubleshootingonce therapy has been initiated is the more common approachdescribed in the literature but is less ideal because of the sub-stantial evidence that frequent missed doses, drug holidays, anddiscontinuation of antiretroviral therapy contribute to drug resist-ance and more rapid disease progression.14, 15, 26, 27
The initial patient consultations were scheduled for 90 minutes.Patients completed personal general information sheets, informedconsent forms, and MOS-HIV health status questionnaires, andprovided baseline adherence data using a questionnaire devel-oped by Chesney et al. at the University of California, SanFrancisco.28, 29 In the initial consultations, patients’ perceptions oftheir illness and therapy were elicited and clarified through dis-cussion that acknowledged patients’ feelings in a nonjudgmentalmanner. Adherence barriers and social supports were identifiedthrough direct or open-ended assessment questions about dailyroutine, employment, use of alcohol or drugs, emotional stabili-ty, relationships, living situation, and past experiences with med-ications. Patients were encouraged to build their social supportsystem, in some cases necessitating discussion of issues of HIV-status disclosure and privacy. Patient education was provided onHIV disease, available medications, side effects, combinationtherapy, drug resistance, and common adherence problems andstrategies. Patients were encouraged to ask questions and expressconcerns, and an effort was made to respond fully to each ofthem.
Patients who decided to proceed with antiretroviral therapyinitiation were offered a one- to two-week placebo (jellybean)trial that simulated the burden of their potential drug regimens.Other adherence tools were utilized depending on the needs ofthe individual patient. Motivational counseling was used insome cases, emphasizing the fact that taking antiretrovirals is away to maintain health rather than to treat illness. Medicationswere dispensed as one-month supplies to allow for closer mon-itoring and were cycled together to avoid multiple trips to thepharmacy within the month. Other available tools were HIVcalendar medication boxes, pagers, and alarm watches.
Shared decision making was employed to arrive at clinicallyappropriate, individualized treatment plans for patients whochose to initiate therapy. This process involved the providers,the ARMAP teams, and the patients.
Following initiation of drug therapy, the pharmacist made a

A Team Approach to Address Antiretroviral Therapy Adherence Barriers in a Managed Care Organization
216 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
phone call to the patient after three to four days to address prob-lems, concerns, or specific drug side effects. At two to threeweeks, the social worker called to provide additional support. A30-minute visit or phone consultation was scheduled at one andthree months to address further concerns and elements of thera-py effectiveness. Additional visits were arranged as needed.
To assess the impact of the ARMAP program, the Chesney et al.adherence questionnaire was administered at the one- and three-month visits and the MOS-HIV questionnaire was administered atthe three-month visit.18, 29 Patient and provider satisfaction ques-tionnaires were administered at the end of the study period.Adherence to antiretroviral medication was the primary outcomeof interest. Pharmacy refill data and self-reported adherence wereused as primary adherence measures. Laboratory values for HIV-RNA viral loads and CD4+ cell counts were collected as addition-al adherence indicators.
Multiple measures of adherence were collected to obtain amore complete picture than could be derived from a singlemeasure. Pharmacy dispensing records do not capture the tim-ing of doses or actual taking of medication; patient reports aresubject to inaccuracy because of patients’ inability to rememberor unwillingness to report failed drug dosing; HIV viral loadand CD4 count are influenced by many factors (e.g., drugabsorption, resistance of HIV strain) in addition to adherence.
nnPractice Innovation The two characteristics that made this program unique are itsfocus on determining patients’ readiness to integrate antiretro-viral therapy into their daily lives and the coupling of pharma-cists and social workers/mental health professionals as adjuncthealth care teams offering educational and psychosocial sup-port to patients contemplating, beginning, or restarting com-plex drug regimens.
The ARMAP program was rooted in the belief that waitingto treat is preferable to poor adherence to treatment, and thatpatients, if provided with adequate information and clarifica-tion of the issues associated with antiretroviral therapy, are bestable to identify their readiness to start medication. Although thepatient was encouraged to determine his or her readiness, dia-logue with the ARMAP team was an integral part of this deter-mination. Having a pharmacist and a social worker or mentalhealth professional help the patient with this decision removedthe pressure to treat the disease from the prescriber. Althoughdelaying antiretroviral therapy has not been shown to be detri-mental to future treatment success, the high visibility of the dis-ease and the political volatility surrounding it contribute to anenvironment in which physicians may not feel comfortablewaiting to treat an identified case of HIV.21
Traditionally, social workers and pharmacists have not beenpaired in the provision of health care, yet they have comple-mentary skills and knowledge to contribute to adherenceenhancement. Patients with HIV face unique challenges that
pharmacists and mental health professionals are able toaddress. Among these challenges are quickly changing knowl-edge about disease pathology and treatment options; the largeamount of conflicting information available through the mediaand other sources; social stigma; the psychological burden ofhaving a chronic and, most likely, terminal disease; the highcost of treatment; and the complexity of the currently preferredtreatment regimens.
nnResultsThirty-two participants (18 at KPNW and 14 at GHC) wereenrolled in the program’s pilot phase. The average age of pro-gram participants was 39 years, and the majority (31/32, 97%)was male. Five (16%) were nonwhite. Thirty-eight percent ofstudy participants were classified as having acquired immuno-deficiency syndrome (AIDS), using the Centers for DiseaseControl and Prevention classification. While 32 participantsentered the study, 26 patients (81%) were eligible for analysisat the one-month follow-up and 23 (72%) went on to completethe entire three-month pilot program, including all question-naires and medication refills.
Pharmacy refill data and self-administered questionnaireswere used as measures of adherence for patients who initiatedtherapy. Seventy-eight percent of participants were “very” or“extremely” sure that they would be able to take all or most of thestudy medication when asked at baseline. At one month, 26patients had initiated therapy and completed follow-up ques-tionnaires. Among the six not eligible for analysis at one month,three GHC and one KPNW participant chose not to start anti-retroviral therapy. Reasons patients decided not to start includedsubstance abuse, better understanding of disease status and ther-apy consequences, denial of disease status, and fear of diseasedisclosure. Two patients dropped out of the study before com-pleting the one-month questionnaire. Seventy-three percent ofpatients reported taking all their medications in the previous fourdays. Pharmacy refill data indicated that 88% had filled their pre-scriptions and had medication available on those four days.
At three months, 23 participants were available for analysis;two were lost to follow-up and one did not complete the self-assessment questionnaire. Ninety-one percent reported takingall of their medications in the previous four days; pharmacyrefill data indicated that 83% had medication available.
Almost all study subjects reported that they were able toadhere to their dosing schedules all or most of the time (96% atone month, 95% at three months). A significant proportion(100% at one month, 94% at three months) reported that theywere able to follow special instructions, such as “take withfood” or “take on an empty stomach.” When asked if theymissed any medications the previous weekend, 85% at onemonth and 90% at three months responded no. The most com-monly cited reasons for missing doses were “had a change inmy daily routine” and “busy with other things.”

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 217
A Team Approach to Address Antiretroviral Therapy Adherence Barriers in a Managed Care Organization
HIV-related lab values were used as additional measures ofadherence as well as an adherence encouragement tool. Theaverage baseline CD4+ count for ARMAP participants was 313cells/mm3. Twenty-three of 24 (96%) participants who begantherapy and had a repeat CD4+ count at three months showedan improvement over baseline. The average three-month CD4+count was 436 cells/mm.3 The baseline viral load for ARMAPparticipants ranged from 967–500,000 copies per milliliter (ml)(median 42,595 copies/ml). All patients initiating therapy expe-rienced a drop in viral load. At one month, three patientsachieved undetectable levels of the HIV virus (<50 copies/ml).Eight additional patients reached undetectable levels of virus atthree months. The percentage decrease in viral load at threemonths among patients who started antiretroviral medicationranged from 67% to over 99%, with the majority of patientsexperiencing a drop of at least 95% from baseline.
Patients participating in ARMAP were satisfied with the pro-gram. Table 1, right, shows the distribution of responses to twoparticipant-satisfaction-survey questions. Five-point Likert scaleswere used to assess both ARMAP’s perceived helpfulness and par-ticipants’ overall satisfaction with the program, with 1 correspon-ding to “very unsatisfied” or “very unhelpful” and 5 correspon-ding to “very satisfied” or “very helpful.” Although 23 patientscompleted all questionnaires, 78% of those initially enrolled com-pleted the satisfaction questionnaire. Eighty percent of partici-pants responding to the satisfaction survey reported that the pro-gram was “helpful” or “very helpful” for taking their medica-tions. All respondents indicated overall satisfaction withARMAP. The most widely reported benefit of ARMAP was anincreased understanding of antiretroviral medications (92%).Over 75% of respondents also believed that ARMAP benefitedthem by helping them to understand their readiness to begintaking medications, teaching them to identify challenges to tak-ing medications, and improving their ability to succeed withmedication taking (see Table 2, right).
Providers who had referred patients to the team also indi-cated overall satisfaction with ARMAP. Five-point Likert scaleswere used to assess its perceived usefulness or helpfulness, with1 being “not useful/helpful at all,” 3 being “neutral,” and 5 being“very useful/helpful.” The mean provider rating of the program’soverall usefulness was 4.42, with 92% (11/12) of providersindicating that ARMAP was “useful” or “very useful” to them.The program was most helpful, according to the mean response,with supporting patients on retroviral therapy (mean=4.64).The program was also deemed helpful by providers in reducingthe time they spent discussing medications and providingpatient education (4.33 and 4.17, respectively). The adherenceteam’s assessment of readiness to begin therapy and patient fol-low-up after starting therapy were identified as useful by mostproviders (mean response=4.42 and 4.58, respectively).
Preliminary analysis of health status via the HIV-MOSinstrument at baseline and 12 weeks showed no significant
change in health status after initiation of antiretroviral therapy,even after adjusting for adherence. These findings will bereported separately.
nnDiscussion
TABLE 1 Patient SatisfactionResponse Number %
Helpfulness of ARMAP in Medication Takinga (mean=4.4)
5: Very helpful 15 60%4 5 20%3: Somewhat helpful 3 12%2 1 4%1: Not at all helpful 0 0%
Overall Satisfaction with ARMAP (mean=4.9)
5: Very satisfied 22 88%4 3 12%3: Neutral 0 0%2 0 0%1: Very dissatisfied 0 0%
Note: N=25aOne KPNW survey respondent did not answer this question.
Yes No Not Applicable
Reported Benefit N (%) N (%) N (%)
Shared and compared experiences with others with similar problems 10 (40) 5 (20) 10 (40)
Increased my understanding of what antiretroviral medications are and how to take them 23 (92) 1 (4) 1 (4)
Helped me understand whether I was ready to start taking medications 20 (80) 3 (12) 2 (8)
Made specific changes to better manage my medications 16 (64) 6 (24) 3 (12)
Learned to identify challenges to taking my medications 21 (84) 3 (12) 1 (4)
Learned to avoid situations that interfere with taking my medications 17 (68) 4 (16) 4 (16)
Improved my ability to be successful with medication taking 22 (88) 2 (8) 1 (4)
Note: N=25.
TABLE 2 Patients’ Perceived Benefits of ARMAP Participation

A Team Approach to Address Antiretroviral Therapy Adherence Barriers in a Managed Care Organization
218 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
The major limitation of this pilot study was that no controlgroup was included, which makes us unable to attribute thehigh adherence rates solely to the teams’ interventions. Thehigh adherence rates may also be attributable to patient knowl-edge of adherence monitoring or to the fact that participantswere a self-selected group that may have been more likely toadhere and be receptive to the team’s interventions than thegeneral HIV-positive population would be. Adherence rates tomost medications also have been shown to decrease with dura-tion of therapy, so the adherence rates in this three-month pilotcannot be extrapolated.14
The reasons for the shift from higher patient-reported ratesof nonadherence compared to pharmacy refill data at onemonth to lower rates of patient-reported nonadherence at threemonths are unclear. Patients’ clearer understanding of the sur-vey instrument or less attention to missed doses over time mayhave played a role.
The project’s initial success has led to its extension in bothorganizations, and six- and nine-month data will soon be avail-able, allowing us to examine potential concurrent control groups.
nnConclusions The ARMAP pilot was well received by both patients andproviders and has proven successful in supporting adherence,contributing to an improved state of readiness to start medica-tions and positive clinical outcomes. Patient readiness to startantiretroviral medication was more clearly understood bypatients, physicians, and the ARMAP team as a result of thecloser collaboration. High adherence rates to newly initiatedantiretrovirals were documented, and no decline in health sta-tus was noted in these patients.
The successful collaboration between allied health profes-sionals and prescribers in this program may serve as a prototypefor future collaborations intended to improve clinical outcomesin ambulatory populations. As more time demands are placedon prescribers and conflicting health and drug information ismade available to the public, allied health professionals are in agood position to support prescribers by helping patients withchronic diseases to understand how medications and behaviorsmay affect their health.
References
1. Larrat EP, Taubman AH, Willey C. Compliance-related problems in theambulatory population. Amer Pharm 1990; NS30(2), 18–23.
2. Pablos-Mendez A et al. Nonadherence in tuberculosis treatment: predictorsand consequences in New York City. Am J Med 1997; 102: 64–70.
3. Diehl AK, Bauer RL, Sugarek NJ. Correlates of medication compliance innon-insulin-dependent diabetes mellitus. South Med Jour, 1987; 80(3): 332.
4. Dearing G. Improving patient compliance in the best interests of all.Managed Healthcare News, 1996; 12 (12), 1, 15–16.
5. Wainberg MA, Friedland G. Public health implications of antiretroviraltherapy and HIV drug resistance. JAMA 1998; 279: 1977–83.
6. Eraker SA, Kirscht JP, Becker MH. Understanding and improving patientcompliance. Ann Intern Med 1984; 100: 258–68.
7. Lerner BH, Gulick RM, Dubler NN. Rethinking nonadherence: historicalperspectives on triple-drug therapy for HIV disease. Ann Intern Med, 1October 1998; 129: 573–78.
8. Eldred LJ et al. Adherence to antiretroviral and pneumocycstis prophylaxisin HIV disease. J Acquir Immune Defic Syndr Hum Retrovirol 1998 Jun 1;18(2): 117–25.
9. Greenfield S et al. Patients’ participation in medical care: effects on bloodsugar control and quality of life in diabetes. J Gen Intern Med 1988; 3:448–57.
10. Powell-Cope GM et al. Perceived health care providers support and HIVadherence. Int Conf AIDS, 1998; 12: 592 (abstract no. 32354).
11. Woodward WC, Flores-Posadas M, Morrison CJ. Patient choice of highlyactive antiretroviral therapy (HAART): implications for adherence/compliance.Int Conf AIDS, 1998; 12: 592.
12. Deeks SG et al. HIV-1 protease inhibitors. A review for clinicians. JAMA(1997) 277: 145–53.
13. Chesney MA. New antiretroviral therapies: adherence challenges andstrategies. Evolving HIV treatments: Advances and the challenges of adher-ence. Paper presented at 37th ICAAC Symposium, Toronto, Canada; 1997.
14. Markowitz M et al. A preliminary study of ritonavir, an inhibitor of HIV-1protease, to treat HIV-1 infection. N Engl J Med 1995; 333: 1534–39.
15. Montouh L, Corbeil J, Richman DD. Recombination leads to the rapidemergence of HIV-1 dually resistant mutants under selective drug pressure.Proc Natl Acad Sci USA, 1996; 93: 6106–11.
16. Wainberg MA, Friedland G. Public health implications of antiretroviraltherapy and HIV drug resistance. JAMA (1998) 279: 1977–83.
17. Senak M. Predicting antiviral compliance: physicians’ responsibilities vs.patients’ rights. J International Association of Physicians in AIDS Care, 1997;3: 45–48.
18. Sorvillo F et al. Use of protease inhibitors among persons with AIDS in LosAngeles County. AIDS Care 1999; 11(2): 147–55.
19. Berger BA, Hudmon KS. Readiness for change: implications for patient care.J Am Pharm Assoc (Wash), 1997 May-Jun; NS37(3): 321–29.
20. Fowler ME. Recognizing the phenomenon of readiness: concept analysis andcase study. J Assoc Nurses AIDS Care, 1998 May-Jun; 9(3): 72–76.
21. Reedijk M et al. Initiation of antiretroviral treatment: decision-making ingeneral practice. Int Conf AIDS, 1998; 12: 1056 (abstract no. 60310).
22. Henry K. The case for more cautious patient-focused antiretroviral therapy.Ann Intern Med (2000) 132: 306–11.
23. Paterson D et al. How much adherence is enough? A prospective study ofadherence to protease inhibitor therapy using MEMS caps (Abstract). SixthConference on Retroviruses and Opportunistic Infections. 1999: 92.
24. Haynes RB, McKibbon KA, Kanani R. Systematic review of randomised trialsof interventions to assist patients to follow prescriptions for medications. Lancet(1996 Aug) 348: 383–86.
25. Rabkin JG, Chesney MA. Adhering to complex regimens for HIV. GMHCTreat Issues (1998 Apr) 12(4): 8–11.
26. Farnsworth A et al. Use of medication management tools to increase adher-ence in a controlled trial of quadruple-drug therapy in HIV+ female patients. IntConf AIDS (1998) 12: 594 (abstract no. 32364).
27. Byrd R et al. Support intervention to enhance medication adherence. IntConf AIDS (1998) 12: 591 (abstract no. 32349).
28. Wu AW et al. A health status questionnaire using 30 items from the MedicalOutcomes Study. Preliminary validation in persons with early HIV infection.Med Care (1991) 29(8): 786–98.
29. Chesney MA et al. Patient Care Committee & Adherence Working Group ofthe Outcomes Committee of the Adult AIDS Clinical Trials Group (AACTG).

OBJECTIVE: To implement an employeeinfluenza-immunization initiative, assessemployee population characteristics, andestimate the cost savings to the universi-ty and its managed health care system.
DESIGN: An interdisciplinary team ofhealth care providers vaccinated em-ployees at mobile sites. A survey wasdistributed to assess population factorsand flu-vaccine status of employees. Aliterature-based economic analysis wasconducted to estimate savings.
SETTING: Large university campus witha major medical center.
MAIN OUTCOME MEASURES: Total num-ber of employees vaccinated comparedto prior years, employee populationcharacteristics, and estimated cost sav-ings (direct and indirect costs).
RESULTS: The immunization effortreach-ed 5,730 employees on the main
campus, an increase of more than 2,000employees from the previous year. Ofemployees completing an on-site sur-vey, nearly 30% were first-time influen-za vaccine recipients and 85.5% wereenrolled in one of the university healthplans. The direct cost for the initiativewas approximately $25,000 while theestimated cost savings approached$400,000.
CONCLUSION: The focused influenzaimmunization initiative increased num-bers of employees vaccinated on cam-pus. Survey results provided a descrip-tion of the employees vaccinated. Theemployer-driven program was predictedto provide cost savings.
KEYWORDS: Influenza, vaccination,immunization, managed care, pharma-cist, interdisciplinary
J Managed Care Pharm 2001: 219–23
An Employee Influenza Immunization Initiative in a Large University Managed Care Setting
REVIEW
JERI J. SIAS, Pharm.D., is Clinical Assistant Professor, University of Texas at El Paso and the University of Texas at Austin, Cooperative Pharmacy Program,El Paso, TX. STEPHANIE COOK, D.O., is Medical Director, University HealthConnections, Ohio State University Managed Health Care Systems, Inc,Columbus, OH. THOMAS WOLFE, Pharm.D., is Clinical EducationConsultant, Pfizer, Inc., Columbus, OH. GAVIN BAUMGARDNER, D.O.,M.H.A., Internal Medicine Resident, Doctors Hospital, Columbus, OH. PAMSALSBERRY, R.N., is Associate Professor, College of Nursing, Ohio StateUniversity.
AUTHOR CORRESPONDENCE: Jeri J. Sias, University of Texas/El Paso, 1100N. Stanton, Suite 301, El Paso, TX 79902; Tel: 915-747-8599; Fax: 915-747-8521; E-mail: [email protected].
ACKNOWLEDGMENTS: Evaluation: Scott Applegate, Mitch Medows, M.D.Implementation: Jill Bero, R.N., Marianne Robinson, Janet Sheppard, R.N.
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
Authors
nfluenza and pneumonia, combined, represent the sixthleading cause of death in the United States. Hosp-italizations attributable to influenza and pneumonia num-ber over 100,000 each year. Additionally, influenza
accounts for an average of 20,000 deaths annually. 1, 2 Influenzacan cause significant morbidity and mortality in elderly patientsand in persons of any age with chronic medical conditions. Inaddition to the impact of influenza in these high-risk groups, theaverage healthy working adult is also adversely affected sociallyand economically. Influenza outbreaks have far-reaching conse-quences. Communities as a whole can benefit from innovativeapproaches to decrease the prevalence of future outbreaks.
The National Vaccine Advisory Committee, recognizing theneed for improved rates of adult vaccination, has evaluatednontraditional settings for adult immunization, including theworkplace and pharmacies.3 While current influenza vaccina-tion recommendations target specific age and high-risk groups,the need and benefit for vaccination in healthy working adultsremains less clear. According to Nichol et al., influenza vacci-nation of healthy, working adults had positive health-relatedand economic outcomes.4 In their evaluation, the estimatedsick leave per year attributable to upper respiratory illness wasapproximately 1.22 days for nonvaccinated, healthy, workingadults, compared with 0.7 days for vaccinated adults (0.52 sickdays saved per employee per year). Additionally, their studyfocused on the potential economic benefits to employers byevaluating direct and indirect costs of vaccinating employees.
nnObjective This descriptive report outlines a worksite influenza-vaccina-tion initiative delivered by an interdisciplinary team. The majoremphasis of this initiative was to increase influenza-vaccinationrates among university employees by providing convenient andaccessible services. Characteristics and influenza-immuniza-tion history of the vaccinated population were assessed.Potential cost savings to the university and its managed healthcare system were evaluated by applying a literature-basedmodel.4
nnPractice Description/Setting The Ohio State University (OSU) has approximately 24,500employees. The OSU Managed Health Care System, Inc.(MHCS), the principal health care provider to employees in the
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 219
I
by Jeri J. Sias, Stephanie Cook, Thomas Wolfe, Gavin Baumgardner, and Pam Salsberry
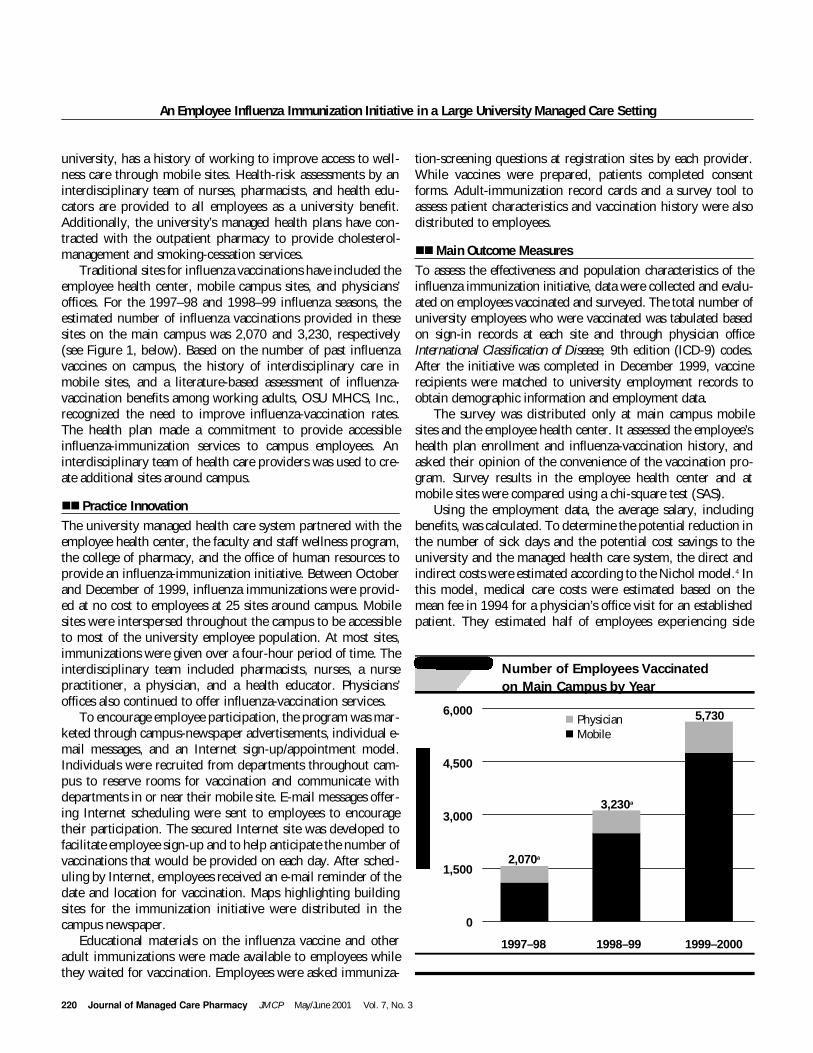
220 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
An Employee Influenza Immunization Initiative in a Large University Managed Care Setting
university, has a history of working to improve access to well-ness care through mobile sites. Health-risk assessments by aninterdisciplinary team of nurses, pharmacists, and health edu-cators are provided to all employees as a university benefit.Additionally, the university’s managed health plans have con-tracted with the outpatient pharmacy to provide cholesterol-management and smoking-cessation services.
Traditional sites for influenza vaccinations have included theemployee health center, mobile campus sites, and physicians’offices. For the 1997–98 and 1998–99 influenza seasons, theestimated number of influenza vaccinations provided in thesesites on the main campus was 2,070 and 3,230, respectively(see Figure 1, below). Based on the number of past influenzavaccines on campus, the history of interdisciplinary care inmobile sites, and a literature-based assessment of influenza-vaccination benefits among working adults, OSU MHCS, Inc.,recognized the need to improve influenza-vaccination rates.The health plan made a commitment to provide accessibleinfluenza-immunization services to campus employees. Aninterdisciplinary team of health care providers was used to cre-ate additional sites around campus.
nnPractice Innovation The university managed health care system partnered with theemployee health center, the faculty and staff wellness program,the college of pharmacy, and the office of human resources toprovide an influenza-immunization initiative. Between Octoberand December of 1999, influenza immunizations were provid-ed at no cost to employees at 25 sites around campus. Mobilesites were interspersed throughout the campus to be accessibleto most of the university employee population. At most sites,immunizations were given over a four-hour period of time. Theinterdisciplinary team included pharmacists, nurses, a nursepractitioner, a physician, and a health educator. Physicians’offices also continued to offer influenza-vaccination services.
To encourage employee participation, the program was mar-keted through campus-newspaper advertisements, individual e-mail messages, and an Internet sign-up/appointment model.Individuals were recruited from departments throughout cam-pus to reserve rooms for vaccination and communicate withdepartments in or near their mobile site. E-mail messages offer-ing Internet scheduling were sent to employees to encouragetheir participation. The secured Internet site was developed tofacilitate employee sign-up and to help anticipate the number ofvaccinations that would be provided on each day. After sched-uling by Internet, employees received an e-mail reminder of thedate and location for vaccination. Maps highlighting buildingsites for the immunization initiative were distributed in thecampus newspaper.
Educational materials on the influenza vaccine and otheradult immunizations were made available to employees whilethey waited for vaccination. Employees were asked immuniza-
tion-screening questions at registration sites by each provider.While vaccines were prepared, patients completed consentforms. Adult-immunization record cards and a survey tool toassess patient characteristics and vaccination history were alsodistributed to employees.
nnMain Outcome Measures To assess the effectiveness and population characteristics of theinfluenza immunization initiative, data were collected and evalu-ated on employees vaccinated and surveyed. The total number ofuniversity employees who were vaccinated was tabulated basedon sign-in records at each site and through physician officeInternational Classification of Disease, 9th edition (ICD-9) codes.After the initiative was completed in December 1999, vaccinerecipients were matched to university employment records toobtain demographic information and employment data.
The survey was distributed only at main campus mobilesites and the employee health center. It assessed the employee’shealth plan enrollment and influenza-vaccination history, andasked their opinion of the convenience of the vaccination pro-gram. Survey results in the employee health center and atmobile sites were compared using a chi-square test (SAS).
Using the employment data, the average salary, includingbenefits, was calculated. To determine the potential reduction inthe number of sick days and the potential cost savings to theuniversity and the managed health care system, the direct andindirect costs were estimated according to the Nichol model.4 Inthis model, medical care costs were estimated based on themean fee in 1994 for a physician’s office visit for an establishedpatient. They estimated half of employees experiencing side
6,000
4,500
3,000
1,500
0
1997–98 1998–99 1999–2000
5,730
3,230a
2,070a
n Physiciann Mobile
FIGURE 1 Number of Employees Vaccinated on Main Campus by Year

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 221
An Employee Influenza Immunization Initiative in a Large University Managed Care Setting
effects would see a physician and that an estimated two days ofwork were lost per 100 vaccines due to side effects. The num-bers of sick days (52 days/100 subjects) and physician officevisits (24 visits/100 subjects) avoided due to upper respiratoryillness were calculated as a difference in the rates betweenplacebo and vaccine group.
The direct costs for this university initiative included pro-gram costs (advertisement, Internet start-up costs, providers,and vaccine/supplies) and estimated direct costs (medical carefor side effects and medical care avoided). Indirect costs includ-ed the salary loss of one hour away from work for vaccinationin addition to estimates of work loss due to side effects and
work loss avoided as compared to nonvaccinated employees.
nnResultsIn the 1999–2000 influenza season, a total of 6,624 employeeswere documented as being vaccinated by university providers(employee health, mobile units, and physician offices) at themain campus and regional campus sites. Of those employees,5,730 were vaccinated on the main campus of the university(mobile sites/employee health: 5,081; physician offices: 649).This initiative increased vaccinations on the main campus bymore than 2,000 and 3,000 vaccines compared to the two priorvaccine seasons (see Figure 1, page 220).
Only the employees vaccinated in employee health(n=1,167) or at a mobile site (n=3,914) on the main campuswere analyzed (total n=5,081). Nearly 86% (4,358/5,081) ofvaccinated employees were matched to human-resource filesand had available demographic data (see Table 1, left). Whilethere were 24,554 employees during the initiative, 17,837 wereconsidered both benefits-eligible and worked on the main cam-pus. Of these benefits-eligible main campus employees, 24.4%(4,358/17,837) were vaccinated.
The total survey response rate was 60% (3,045/5,081).Ninety-eight percent of respondents reported having healthinsurance, with 85.5% indicating enrollment in one of the fouruniversity health plans. Employees who reported that this wastheir first influenza vaccination totaled 29.4%. Forty-six per-cent of the surveyed employees reported that they did not get aflu shot last year. Convenience was cited as influential in receiv-ing their vaccine in 93.2% of employees (see Table 2, left).
Survey return rates varied in the employee health center(22%: 257/1,167) compared with mobile sites (71.2%:2,788/3,914). First-time vaccine recipients seemed to be morelikely to use a mobile unit than the employee health center(mobile: 30.1%, employee health: 21.8%, p=0.005). Theseresults suggest that the convenience offered by mobile sitesenhanced immunization rates (mobile: 94.5%, employeehealth: 90.6%, p=0.011) (see Table 3, page 222).
An economic analysis was conducted using the modeldescribed by Nichol et al.4 The direct cost for the immunizationinitiative was $24,700. The average hourly wage plus benefitsfor participants was $25.61. When applying the Nichol modelto the vaccinated population (n=5,081), 2,242 sick days wereprojected to be saved for the year.4 The estimated total cost-savings of vaccinating employees was $393,371 (see Table 4,page 222). This amount suggests savings of $90.26 ($393,371/4,358) per employee vaccinated.
nnDiscussionThe findings from this project demonstrate benefits of a target-ed worksite vaccination program. A total of 5,730 patients werevaccinated during the 1999–2000 season on the main campus,reflecting an increase in immunizations over the two previous
TABLE 1 Employee Demographics
Characteristics Vaccinated Total UniversityPopulation Employeesn=4,358 a n=24,554
Mean Age 44.8 44
Female (%) 58.4 49.5
Job Classification
Administrative/ 2,055 (47.2) 12,601 (51.3)professional (%)
Classified civil 1,263 (29.0) 5,278 (21.5)service (%)
Faculty (%) 1,040 (23.9) 6,675 (27.2)aRepresents the number of patients who have demographic informationavailable through employment records.
TABLE 2 Survey Results (n=3,045)
Survey Question Response Numbera Percenta
Do you have health Yes 2,993 98.3insurance? No 44 1.4
Do you have university Yes 2,604 85.5health insurance? No 435 14.3
Is this your first time Yes 895 29.4receiving a flu vaccine? No 2,148 70.5
Did you get a flu vaccine Yes 1,634 53.7last year? No 1,403 46.1
Did convenience influence Yes 2,838 93.2you to get your flu shot at No 177 5.8this site?
aNumbers may not total 3,045 (100%) because of lack of response onsome surveys.

An Employee Influenza Immunization Initiative in a Large University Managed Care Setting
222 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
seasons. At the time of analysis, 4,358 of the 5,081 participantsin the mobile sites could be verified in the employer records.These matched records were later used to evaluate populationdemographics and to calculate potential cost-savings for theemployer.
The surveys (3,045) provided additional background infor-mation about the vaccinated employees that could not beobtained from employee or medical records alone. Almost half(46%) of employees completing a survey did not receive a vac-cination in the previous year, and 85.5% were enrolled in oneof the university health plans. Results demonstrated that nearly30% were first-time influenza vaccine recipients. Convenientaccess via mobile sites appeared to positively affect immuniza-tion rates.
The discrepancy observed in survey response rate betweenemployee health (21.9%) and the mobile sites (71.2%) may beattributed to inconsistencies in survey distribution. The demo-graphics and survey answers in employee health compared withmobile sites do suggest some differences and trends. It appearsthat more first-time flu vaccine recipients received their inocu-lations at mobile sites than in employee health centers.Employees receiving vaccines at mobile campus units reportedconvenience as a factor slightly more often than those who vis-ited employee health centers.
The Ohio State University is self-insured (i.e., funds its ownhealth plan). With 85.5% of surveyed participants enrolled inone of the university health plans, OSU MHCS, Inc., and theuniversity, as an employer, both benefit from high participationin the initiative. To determine potential cost savings, a litera-ture-based analysis by Nichol et al. was utilized.4 In this ran-domized, double-blind, placebo-controlled trial of influenzavaccination in 849 healthy, working adults in the Minneapolis–St. Paul region, an economic model of direct and indirect costswas developed.
In applying this model to this university’s findings, a directcost savings of $58,545 and an indirect cost savings of$334,826 were projected. The cost for medical care office visitsin the Nichol study was adjusted to the 1999 Consumer PriceIndex.5 To determine potential work lost, the average universi-ty employee salary including benefits was used. In this setting,a more conservative time (1 hour instead of 30 minutes) wasused to determine time away from work.
The Nichol study population (n=424) compares to this uni-versity’s vaccinated population (4,358) in the following ways:Average age in the university population was 44.8 years in con-trast to 39.2 years in the Nichol study. The proportion of femalerecipients was comparable between the university (58.4%) andthe Nichol study (60.2%). Thirty percent of the universityemployees completing surveys reported first-time influenzavaccination compared with 74% in the Nichol study. We usedthe Nichol economic analysis as a guide for the potential bene-fits in the university setting.
Variable Employee Mobile p valueHealth Unit
Female (%) 151 (63.4) 1,486 (58.0) 0.1n=238 n=2,546
First-time influenza 56 (21.8) 839 (30.1) 0.005vaccination (%) n=257 n=2,786
Convenience was a 230 (90.6) 2,608 (94.5) 0.011factor in getting flu n=254 n=2,761vaccination (%)
Note: Total Employee Health responses (n=257), Total Mobile UnitResponses (n=2,788)
TABLE 3 Comparison of Survey Responses ofPatients Receiving Flu Vaccine
TABLE 4 Economic Analysis
Variable Cost (Savings)n=4,358
Direct costs
Vaccination program costsa $24,700
Medical care for side effects (1 office $3,619visit per 100 subjects)b
Medical care avoided (24 office visits ($86,864)for upper respiratory illness per 100subjects)
Total direct costs ($58,545)
Indirect costs
Work time lost for vaccination $111,608(1 hour per vaccination)c
Work loss due to side effects (2 days $17,857per 100 subjects)
Work loss avoided (52 days for upper ($464,291)respiratory illness per 100 subjects)
Total indirect costs ($334,826)
Net costs ($393,371)
aIncluded costs for advertisement, personnel, vaccine/supplies, and Internetstart-up.bCost for physician visit derived from Nichol et al.4 ($69.51) and adjustedfor inflation ($83.05/visit).5cCost of work loss was determined by averaging the salaries (hourly wage+ benefits) based on job classification benefits ($25.61/hour, $204.88/eighthour day).

An Employee Influenza Immunization Initiative in a Large University Managed Care Setting
We believe that all of the estimated values reflect conserva-tive numbers and the potential savings are possibly greater thanthose reported. Further analysis of vaccinated employees inhigh-risk categories (e.g., persons with diabetes or asthma)compared with a control group should also be conducted.
nnConclusionThis interdisciplinary initiative was successful in increasinginfluenza immunizations during the 1999–2000 influenza sea-son. Approximately one-third of employees indicated that theyhad never before received a flu vaccine, and more than 90%cited convenience as influential in receiving a vaccine. It is pos-sible that access and convenience to vaccine services increasedvaccination rates.
Based on the literature, the potential cost savings to the univer-sity and managed health care systems was nearly $400,000, orapproximately $90 per employee. In addition, the university com-
munity was estimated to save more than 2,000 sick days. Theseinterdisciplinary immunization efforts could prove to be viablepartnerships in other settings as well. Such partnerships could ben-efit employees, employers, and the health care system, leading todecreased sick days and increased cost savings to the community.
References
1. Prevention and control of influenza: recommendations of the advisory com-mittee on immunization practices (ACIP). MMWR 1999; 48: 1–28.
2. Notice to readers: Update recommendations from the Advisory Committeeon Immunization Practices in response to delays in supply of influenza vac-cine for the 2000–01 Season. MMWR 2000; 49(39): 888–92.
3. Adult immunization programs in nontraditional settings: quality standardsand guidance for program evaluation. MMWR 2000; 49(RR-1): 1–13.
4. Nichol KL et al. The effectiveness of vaccination against influenza inhealthy, working adults. N Eng J Med 1995; 333: 889–93.
5. Bureau of Labor Statistics. Consumer Price Index—All Urban Consumers(Current Series). U.S. Medical Care. Base Period: 1982-84: 100. Series ID:
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 223


Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 225
A Cost Analysis of Four Benefit Strategies for Managing a Cox II Inhibitor
tried and failed before celecoxib was used; • a therapeutic buy-up program, in which a maximum allow-
able cost is implemented with the member paying the differ-ence; or
• a three-tiered copayment plan, in which celecoxib is placedin the highest tier with other nonformulary medications.
nnMethodsReports showing paid claims were run using the Apothequeryprescription data software, a patented API product. Thesereports, which contained data from four of API’s clients, showedeach claim processed, information about patient copayments,days supply, quantity dispensed, ingredient costs paid, the dateeach prescription was filled, and medication strength. For claimsthat were denied and never subsequently paid, requests weresubmitted to the information technology department for retrievalof these data. Claims that were submitted and subsequentlyreversed were “scrubbed” and discarded. Corresponding datareports were manipulated using Excel spreadsheet software whennecessary. The four clients examined varied in size, demograph-ics, and benefit design.
Data from a 36,000-member indemnity plan that uses athree-tiered copayment program were gathered and examined.The lowest tier, corresponding to generic drugs, requires a $7copayment. Preferred brand-name drugs, the second tier,require a $15 copayment. Celecoxib is placed on the third tier,nonpreferred brand-name drugs, which requires a $25 copay-ment. This type of program discourages use of nonpreferreddrugs, but allows the patient access to the medication if he orshe is willing to pay the price.
Using Excel software, all $25 copayments were changed to$15, thus showing a theoretical total copayment and a theoret-ical total amount paid had the third tier not been implemented.The difference between the theoretical amount paid and theactual amount paid was determined, and a percentage savingswas calculated. The three-tier copayment saves this plan 17.1%compared to the amount that would have been paid had thethird tier not been implemented.
Data from a 142,000-member group with a therapeutic buy-up plan were gathered and examined. In this type of plan, theinsurer selects a limited number of preferred products in a giventherapeutic class. The member pays the difference between thecost of the nonpreferred product and the preferred product, plusthe appropriate copayment. In order for a member to receive cele-coxib, a nonpreferred product, the member must pay a $20copayment plus the difference of the cost of the medication, usinggeneric naproxen as the comparison. Again, this discourages useof the drug, but allows access to patients willing to pay the price.Using Excel software, all copayments greater than $20 were nor-malized to $20, resulting in a theoretical total copayment and atheoretical total amount paid had the use of celecoxib not beenrestricted. The difference between the theoretical amount paid
and the actual amount paid was determined, and a percentage ofsavings was calculated. The therapeutic buy-up program savesthis plan 36.7% over what the plan would have paid if no restric-tions were implemented.
Claims data were examined from a 46,000-member groupthat uses a prior-authorization program to control the use of cele-coxib. In this type of program, pharmacists are trained in specif-ic disease states and their appropriate treatments. They areresponsible for determining whether celecoxib is being pre-scribed appropriately according to guidelines set by the plan, andapprove or deny submitted claims accordingly. 3 The prior-author-ization requirements do not specify a diagnosis; however, they dooutline specific screening criteria for patients who should not beon NSAIDs, based on factors such as increased age, risk of GIbleeding, use of anticoagulants, and previous intolerance to otherNSAIDs. Data for appeals were not available or tracked by API.
Under this plan, celecoxib may be used by patients who:• are older than 65;
5
4.5
4
3.5
3
2.5
2
1.5
1
0.5
0
Daily NSAID Therapy Costs

A Cost Analysis of Four Benefit Strategies for Managing a Cox II Inhibitor
226 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
• have prior documentation of GI ulcer;• are concurrently treated with corticosteroids or anticoagulants;• have used an H2 blocker or proton pump inhibitor;• are smokers or alcohol abusers; and/or • have tried and demonstrated intolerance of at least two other
NSAIDS.A comparison was made between celecoxib claims that were
paid and those claims that were submitted but denied payment.The cost per unit of therapy (capsule) was calculated by divid-ing the total amount paid by the plan by the total number ofcapsules dispensed. A listing of all celecoxib claims that wereultimately rejected was obtained, and the total number of cap-sules that were not dispensed was also calculated. Using thecost per capsule, cost savings were determined. The cost savingswere then compared with the potential total amount paid (paidclaims plus rejected claims). The total savings was 49.8%.
The final group studied is a plan with 13,000 lives that hasimplemented a step-therapy program. Step therapy is similar toprior authorization; predetermined requirements are establishedand the computer system will automatically pay the submittedclaim if, within the previous 90 days, the patient has used atleast one of the following for 30 days:• Cox II inhibitor or NSAID;• H2 antagonist, proton pump inhibitor, Cytotec (prostaglandin),
sucralfate;• anticoagulant/antiplatelet therapy; or• 10 days of combination ulcer treatment (i.e., PrevPac).
As with prior authorization, a comparison was madebetween all paid celecoxib claims and all celecoxib claims thatwere submitted but denied payment. A total for all submittedcelecoxib claims, regardless of final payment status, was deter-mined. The percentage of savings was calculated to be 74.1%.Step therapy is the program that realizes the largest percentagein cost savings of the plans examined (see Table 1, above).
nn Limitations Certain inherent limitations and assumptions must be addressedconcerning this analysis and the methods used. Ideally, data forsuch an analysis would be collected over a two-year period.Celecoxib was released during the first quarter of 1999; therefore,only several months’ (February–December 1999) worth of datacould be examined.
The software used to obtain claims data, Apothequery, hastwo main limitations that must be considered. First, integrationof the program with other software is difficult, and at the timethis article was written, the database was updated only every 30days. The software used to manipulate and examine the data islimited in the number of records it will hold at one time, lead-
Benefit Strategy ComparisonsCost- Amount Copayment Days Quantity Ingredient Cost of % Savingsa
Containment Paid Supply Cost Paid ApprovalsProgram Plus Denials
(Number of Claims)
Step therapy $7,661.14 $3,241.04 3,970 4,907 $10,285.45 $29,610.34 74.1(138)
Prior $64,922.61 $7,314.14 25,356 37,851 $69,745.51 $129,443.25 49.8authorization
(879)
Cost- Amount Copayment Days Quantity Ingredient New New % Savingsb
Containment Paid Supply Cost Paid Copayment PaidProgram
(Number of Claims)
Therapeutic $412,368.55 $385,887.39 296,883 415,421 $775,304.44 $145,813.75 $652,442.19 36.18buy-up (8,989)
Three-tier co- $23,019.98 $12,426.25 13,480 17,925 $34,301.91 $7,695.00 $27,751.23 17.10payment (505)
a% savings calculation: (Cost of approvals+denials)–amount paid
Cost of approvals+denials
b% savings calculation: New paid–amount paid
New paid

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 227
A Cost Analysis of Four Benefit Strategies for Managing a Cox II Inhibitor
ing to additional steps in the data-examination process. Suchpiecemeal examination of the data allows for an increased mar-gin of error in calculations. A fairly thorough knowledge of thesyntax of the software is necessary in order to perform the nec-essary statistical manipulations of the data. Assumptions weremade that the data received were accurate and correct, and thatcelecoxib was being prescribed correctly (i.e., for indicationsdiscussed previously, and not for chronic pain).
Administrative fees and transmission costs were not includ-ed due to their variability from plan to plan. Differences indemographics among patient populations were not considered.The focus of this study was to determine which benefit designwas the most cost-effective; however, because of the lack ofavailability of diagnostic information, cost differences betweendosages had to be omitted.
Certain biases must be addressed from the perspective of thePBM. These companies, like any other for-profit organizations,must make money in order to succeed. PBMs are faced with thechallenge of reducing drug costs for their clients while main-taining a high standard of care for their clients’ members. PBMsmust negotiate with pharmaceutical manufacturers to keepmedication costs as low as possible, while keeping the patient’sbest interest as their top priority.
Step therapy shows the biggest cost savings to a plan; how-
ever, the actual amount of this savings may be over-inflatedbecause of the small size of the plan used as an example.
nnConclusion Since its release in early 1999, celecoxib has become one of themost widely prescribed drugs for arthritis, and has since beenawarded the additional indication of familial adenomatouspolyposis. Celecoxib was the first member of the new class ofdrugs known as Cox II inhibitors, and was marketed as a drugthat would reduce GI effects that other NSAIDs cause.
Many PBMs and health benefit plans have addressed thehigh cost and potential for misuse of celecoxib and have placedrestrictions on its use by implementing various methods of con-trol. Despite the limitations mentioned, it can be concluded thatstep therapy provides a plan the greatest amount of cost avoid-ance because it is the most restrictive of the cost savings meas-ures examined.
References
1. Celebrex Package Insert, Pfizer, 1999.
2. 1999 Drug topics redbook, Feb. 2000 Update.
3. Wertheimer AI, Navarro RP. Managed care pharmacy principles and prac-tice. New York: Pharmaceutical Products Press, 1999, 303–04.

228 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
OBJECTIVE: High exposure to glucocorti-coid drugs is associated with anincreased risk of osteoporosis and frac-ture. To define the degree to which indi-vidual prescribers needed to adjust theirprescribing practices and thus to pre-vent glucocorticoid-induced osteoporo-sis among their patients, this researchsought to identify both the health planmembers who had high exposure to glu-cocorticoid drugs and the physicianswho prescribed these drugs.
DESIGN: Patient demographic charac-teristics, diagnoses, and medicationswere determined for members of theKaiser Foundation Health Plan ofNorthern California who received morethan two grams of prednisone (or itsequivalent) during any 12-month periodfrom 1998 through 1999.
RESULTS: High exposure to glucocorti-coid drugs was identified in 22,444health plan members, accounting forabout 1% of adult health plan members.High exposure to glucocorticoid drugsincreased sixfold from about 0.5% inmembers 20–30 years old to about 3%in members 70–79 years old; amongthese members, 3,788 physicians pre-scribed the glucocorticoid drugs that ledto high exposure. The highest numbersof highly exposed patients were seen
among rheumatologists and oncolo-gists. Nephrologists, pulmonologists,and gastroenterologists had an interme-diate number of highly exposedpatients. Internists had the lowest num-ber of highly exposed patients perphysician, yet prescribed glucocorticoiddrugs to the largest group (40%) of high-ly exposed patients in the study.
CONCLUSIONS: Using a pharmacy data-base system developed to identifypatients exposed to potentially harmfulamounts of glucocorticoid drugs, weidentified high glucocorticoid exposure in1%–3% of health plan members morethan 50 years old. In addition, groupingprescribing physicians by medical spe-cialty showed that the need to adjust pre-scribing practices to prevent glucocorti-coid-related complications was unevenlydistributed among specialty groups. Toimprove quality of care for patients inmanaged care organizations who havehigh exposure to glucocorticoid drugs,systems for preventive identification andintervention should be developed usingpharmacy databases, and should be tai-lored to physician specialty.
KEYWORDS: Glucocorticoids, menopause,osteoporosis
J Managed Care Pharm 2001: 228–32
Who Bears Responsibility for Glucocorticoid-ExposedPatients in a Large Health Maintenance Organization?
RESEARCH
Authors
rolonged exposure to high levels of glucocorticoiddrugs can cause bone loss, osteoporosis, and fracture. 1,
2 Fracture ultimately occurs in about half of patientswho take glucocorticoid drugs to control pulmonary,
rheumatologic, autoimmune, hematopoeitic, and gastrointesti-nal disease.1 About 18 million patients in the United Statesreceive treatment with exogenous steroid agents, and an esti-mated 0.4% of one U.S. health plan’s members are exposed toglucocorticoid drugs.3, 4
Intervention for persons with high exposure to glucocorti-coid drugs has been recommended by various medical special-ty groups, such as the American College of Rheumatology, theUnited Kingdom Task Force, and the British Society forGastroenterology. 5–7 In the recent past, approval of bisphospho-nates for prevention of glucocorticoid-induced bone loss hasspurred interest in this disorder. 8–10 However, the process ofidentifying persons with high exposure to glucocorticoid drugshas not been standardized, partly because glucocorticoid drugsare available in many formulations and doses and partlybecause the usual practice is to change dosage frequently or toprescribe intermittent use. Thus, only a few patients in U.S.health plans who are at risk for glucocorticoid-induced osteo-porosis receive drug prophylaxis to both prevent bone loss andreduce the risk of fracture.4, 11
At Kaiser Foundation Health Plan of Northern California, ahealth maintenance organization (HMO) caring for approxi-mately three million members, databases allow monitoring ofall prescriptions and clinic visits. Using these databases, weidentified and characterized members who had high exposureto glucocorticoid drugs to determine the care requirementsthey present to health care providers.
nnMethods The study protocol was approved by the Kaiser PermanenteNorthern California Institutional Review Board. Using thehealth plan’s computerized pharmacy database (PharmacyInformation Monitoring Service [PIMS]) for the years1998–1999, we identified prescriptions for 248 different drugitems (National Drug Codes) within the oral glucocorticoidtherapeutic class. Because glucocorticoid drugs are prescribedas physiologic replacement in patients diagnosed with adrenalor pituitary insufficiency, we excluded from the study 288 suchcases on the basis of their outpatient diagnostic codes.
We converted all glucocorticoid values to prednisone equiv-
Pby Bruce Ettinger, Alice Pressman, and Hema A. Shah
BRUCE ETTINGER, M.D., is Senior Investigator, Division of Research, KaiserPermanente Medical Care Program, Oakland, CA; ALICE PRESSMAN, M.S., isSenior Analyst, Division of Research, Kaiser Permanente Medical CareProgram; and HEMA A. SHAH, M.D., is Senior Medical Resident, Departmentof Internal Medicine, Kaiser Permanente Medical Center, San Francisco, CA.
AUTHOR CORRESPONDENCE: Bruce Ettinger, M.D., Division of Research,Kaiser Permanente Medical Care Program, 3505 Broadway, Oakland, CA94611-5463; Tel: 510-450-2131; Fax: 510-450-2097; E-mail:[email protected].
ACKNOWLEDGMENTS: This research was supported by a grant from Procter& Gamble Pharmaceuticals, Aventis Pharmaceuticals, and the Alliance forBetter Bone Health. The Medical Editing Department of Kaiser FoundationHospitals, Inc., provided editorial assistance.
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rights reserved.
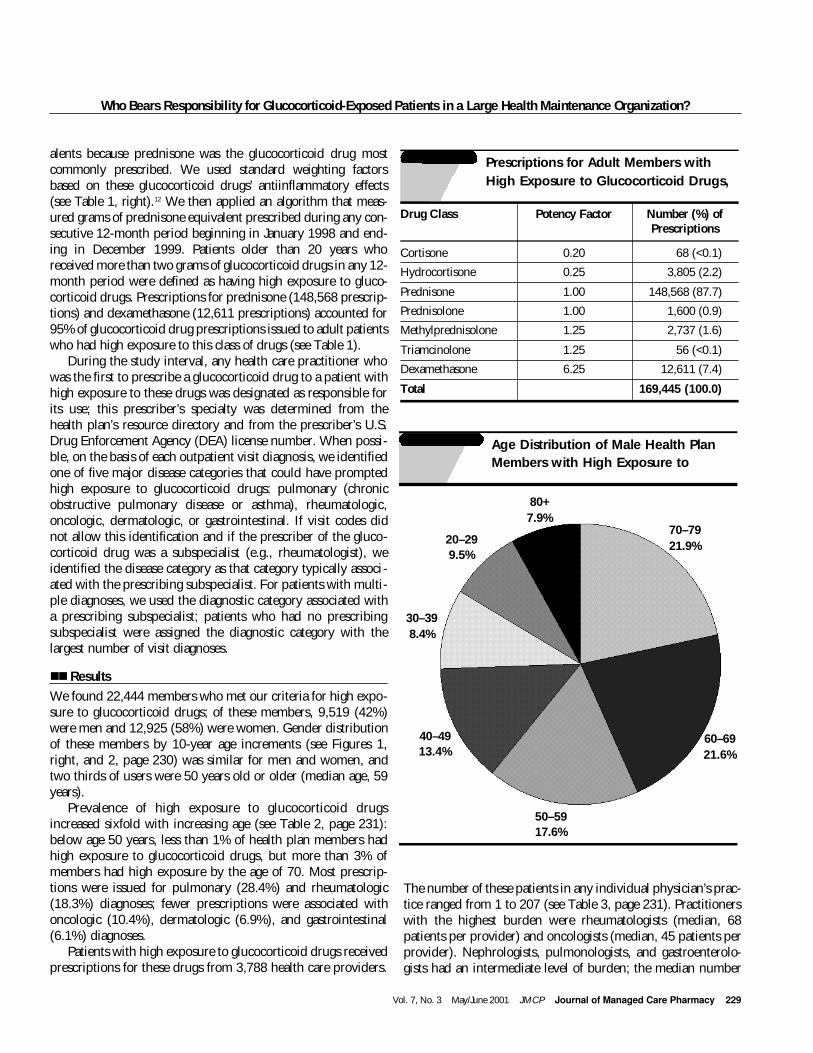
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 229
Who Bears Responsibility for Glucocorticoid-Exposed Patients in a Large Health Maintenance Organization?
alents because prednisone was the glucocorticoid drug mostcommonly prescribed. We used standard weighting factorsbased on these glucocorticoid drugs’ antiinflammatory effects(see Table 1, right).12 We then applied an algorithm that meas-ured grams of prednisone equivalent prescribed during any con-secutive 12-month period beginning in January 1998 and end-ing in December 1999. Patients older than 20 years whoreceived more than two grams of glucocorticoid drugs in any 12-month period were defined as having high exposure to gluco-corticoid drugs. Prescriptions for prednisone (148,568 prescrip-tions) and dexamethasone (12,611 prescriptions) accounted for95% of glucocorticoid drug prescriptions issued to adult patientswho had high exposure to this class of drugs (see Table 1).
During the study interval, any health care practitioner whowas the first to prescribe a glucocorticoid drug to a patient withhigh exposure to these drugs was designated as responsible forits use; this prescriber’s specialty was determined from thehealth plan’s resource directory and from the prescriber’s U.S.Drug Enforcement Agency (DEA) license number. When possi-ble, on the basis of each outpatient visit diagnosis, we identifiedone of five major disease categories that could have promptedhigh exposure to glucocorticoid drugs: pulmonary (chronicobstructive pulmonary disease or asthma), rheumatologic,oncologic, dermatologic, or gastrointestinal. If visit codes didnot allow this identification and if the prescriber of the gluco-corticoid drug was a subspecialist (e.g., rheumatologist), weidentified the disease category as that category typically associ-ated with the prescribing subspecialist. For patients with multi-ple diagnoses, we used the diagnostic category associated witha prescribing subspecialist; patients who had no prescribingsubspecialist were assigned the diagnostic category with thelargest number of visit diagnoses.
nnResults We found 22,444 members who met our criteria for high expo-sure to glucocorticoid drugs; of these members, 9,519 (42%)were men and 12,925 (58%) were women. Gender distributionof these members by 10-year age increments (see Figures 1,right, and 2, page 230) was similar for men and women, andtwo thirds of users were 50 years old or older (median age, 59years).
Prevalence of high exposure to glucocorticoid drugsincreased sixfold with increasing age (see Table 2, page 231):below age 50 years, less than 1% of health plan members hadhigh exposure to glucocorticoid drugs, but more than 3% ofmembers had high exposure by the age of 70. Most prescrip-tions were issued for pulmonary (28.4%) and rheumatologic(18.3%) diagnoses; fewer prescriptions were associated withoncologic (10.4%), dermatologic (6.9%), and gastrointestinal(6.1%) diagnoses.
Patients with high exposure to glucocorticoid drugs receivedprescriptions for these drugs from 3,788 health care providers.
The number of these patients in any individual physician’s prac-tice ranged from 1 to 207 (see Table 3, page 231). Practitionerswith the highest burden were rheumatologists (median, 68patients per provider) and oncologists (median, 45 patients perprovider). Nephrologists, pulmonologists, and gastroenterolo-gists had an intermediate level of burden; the median number
TABLE 1 Prescriptions for Adult Members withHigh Exposure to Glucocorticoid Drugs,
Drug Class Potency Factor Number (%) of Prescriptions
Cortisone 0.20 68 (<0.1)
Hydrocortisone 0.25 3,805 (2.2)
Prednisone 1.00 148,568 (87.7)
Prednisolone 1.00 1,600 (0.9)
Methylprednisolone 1.25 2,737 (1.6)
Triamcinolone 1.25 56 (<0.1)
Dexamethasone 6.25 12,611 (7.4)
Total 169,445 (100.0)
80+7.9%
30–398.4%
40–4913.4%
50–5917.6%
60–6921.6%
20–299.5%
70–7921.9%
FIGURE 1 Age Distribution of Male Health PlanMembers with High Exposure to

Who Bears Responsibility for Glucocorticoid-Exposed Patients in a Large Health Maintenance Organization?
230 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
of patients with high exposure to glucocorticoid drugs rangedfrom 11–18 per physician in these specialties. In contrast,internists had a median of three such patients per physician.However, internists were the largest specialty group of pre-scribers; three times as many patients with high exposure toglucocorticoid drugs received these drugs from internists asfrom rheumatologists, the next-highest prescribing group.
We repeated these analyses using two cutpoints of annualcumulative glucocorticoid exposure: more than 1 g prednisoneequivalent and more than 3 g prednisone equivalent. Comparedwith the results obtained using the more-than-two-gram cut-point, use of the more-than-one-gram cutpoint yielded 71%more patients with high exposure to glucocorticoid drugs, anduse of the more-than-three-gram cutpoint yielded 37% fewerpatients with high exposure to glucocorticoid drugs. Results ofusing each cutpoint did not change the distribution of patientsseen by each type of prescriber. For example, for any given cut-point, 40%–44% of patients with high exposure to glucocorti-coid drugs received prescriptions from internists, and 11%–13%of patients received prescriptions from rheumatologists.
nnDiscussionBy examining a computerized database of prescriptions issuedto adult health plan members, we found that approximately 1
in 100 persons in any given year was exposed to potentiallyharmful levels of glucocorticoid drugs. Our study showed thathigh exposure to glucocorticoid drugs increases sixfold withincreasing age and that rheumatic and pulmonary diseases werethe most common indications for prescribing these drugs; thesefindings are similar to those of other surveys.2, 4, 11, 13
Our study is the first large-scale examination of prescribersof high-dosage glucocorticoid drugs. Considerable attention hasbeen focused on the prescribing behavior of medical specialistssuch as rheumatologists and pulmonologists, in the belief thatthese specialists are the most frequent prescribers of glucocorti-coid drugs. Although we did find that these medical specialiststreat many patients who receive glucocorticoid drugs, we foundthat the larger group of generalists—not specialists—issue mostprescriptions for glucocorticoid drugs.
This finding is important because it bears on the interven-tion systems that managed care organizations may choose todevelop for reducing morbidity among patients exposed to highlevels of glucocorticoid drugs. For example, now that effectivedrugs are available for prevention of glucocorticoid-inducedosteoporosis, and with the impetus provided by new treatmentguidelines, managed care organizations are likely to place a highpriority on implementing interventions among these patients.5–9
Similarly, a rheumatologist—who typically cares for 60–70patients exposed to high levels of glucocorticoid drugs—is like-ly to give this condition quite different priority than would ageneralist, who typically has only a few such patients. Whereasthe generalist can manage treatment algorithms in the office, therheumatologist has a large burden of care that is best sharedwith a case manager—perhaps a pharmacist or specially trainednurse practitioner.
A strength of our study is the novel algorithm we developedfor calculating cumulative exposure to glucocorticoid drugsduring consecutive 12-month periods; this algorithm enables amultitude of glucocorticoid formulations and dosages to betranslated, first into standard prednisone equivalents, then intocumulative 12-month exposure, and ultimately into a “flag” thatalerts the practitioner to patients whose cumulative use of glu-cocorticoid drugs is more than two grams. This algorithm canbe easily adapted by managed care organizations equipped withaccess to a pharmacy database. (Data on specific programmingissues and prescription identification are available from theauthors.) By automating this system, a managed care organiza-tion can rapidly and accurately identify patients at risk and canrelay this information to clinicians responsible for initiatingprophylaxis against glucocorticoid-induced osteoporosis.Currently, only 5%–14% of patients receiving glucocorticoiddrugs in managed care settings receive bone-specific drugs forosteoporosis.4, 11, 14, 15 In some cases, clinicians may fail to provideprophylaxis because they are unaware of the extent of theirpatients’ exposure to glucocorticoid drugs; however, thesehealth care providers may also be unfamiliar with newer, more
80+7.7%
30–399.4%
40–4915.6%
50–5919.9%
60–6921.0%
20–296.7%
70–7919.8%
FIGURE 2 Age Distribution of Female Health PlanMembers with High Exposure to

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 231
Who Bears Responsibility for Glucocorticoid-Exposed Patients in a Large Health Maintenance Organization?
effective drugs for preventing and treating this form of osteo-porosis.16 Our proposed system would address both deficien-cies.
Some limitations of our study are worthy of mention. Ourmethod of flagging issuers and recipients of glucocorticoid pre-scriptions may not have identified the provider initially respon-sible for prescribing the glucocorticoid drugs. Whether the bur-den of preventing and managing glucocorticoid-related compli-cations rests on the clinician who diagnoses and manages thecase is arguable; another clinician may be prescribing thesedrugs in lieu of the responsible physician. More study is neededto identify and design systems that fairly and efficiently assignthis responsibility and track a health care system’s progress inincreasing the proportion of patients who receive appropriateintervention against glucocorticoid-induced osteoporosis.17
Another potential limitation of our study could be ourchoice of a 2 g prednisone cutpoint. Perhaps a more liberal alertsystem would be based on a 1 g prednisone cutpoint (equiva-
lent to 100 days of 10 mg prednisone/day). Our choice of the 2 gcutoff satisfied several criteria: It is the dose which, takenthroughout a five-year period, has been shown to cause adrenalsuppression; it is equivalent to a year’s exposure at 5.5 mg/day,a mean daily dosage associated with a statistically significantincrease in both hip and spine fracture risk; and it is close to thedosage (more than 7.5 mg of prednisone per day for more thansix months; equivalent to a cumulative total of more than 1.4grams) that the American College of Rheumatology and theUnited Kingdom Task Force have suggested as the cutpointindicating the need for active intervention.2, 5, 6, 18
In conclusion, we have developed a pharmacy database sys-tem that identifies patients exposed to potentially harmfulamounts of glucocorticoid drugs. Using this system, we foundthat approximately 1 in 100 adult health plan members has thislevel of exposure and that the percentage of patients with highexposure rises with age. Nearly half these patients receive theirglucocorticoid drug prescriptions from generalists who, on
TABLE 2 Number and Percentage of Patients with High Exposure to Glucocorticoid Drugs, by Sex and Age
Age 20–29 30–39 40–49 50–59 60–69 70–79 Ž80 All
Male 872 (0.5%) 803 (0.4%) 1,279 (0.6%) 1,675 (1.0%) 2,051 (1.9%) 208 (3.1%) 756 (3.3%) 9,519 (1.0%)
Female 867 (0.5%) 1,210 (0.5%) 2,016 (0.8%) 2,569 (1.4%) 2,713 (2.3%) 2,555 (3.1%) 995 (2.8%) 12,925 (1.2%)
Practice Type Number (%) Highly Exposed Patients per Prescribing PhysicianPhysicians Prescribing
Total (%) Median Range
Internal medicine 1,649 (43.5) 9,029 (40.2) 3 1–101
Rheumatology 37 (1.0) 2,851 (12.7) 68 1–207
Oncology 56 (1.5) 2,461 (11.0) 45 1–91
Pulmonology 44 (1.2) 936 (4.2) 13 1–66
Gastroenterology 74 (2.0) 909 (4.1) 11 1–39
Family practice 169 (4.5) 863 (3.8) 4 1–21
Pediatrics 338 (8.9) 732 (3.3) 1 1–11
Allergy/immunology 42 (1.1) 643 (2.9) 9 1–101
Neurology 76 (2.0) 549 (2.4) 6 1–23
Nephrology 22 (0.6) 459 (2.0) 18 3–41
Dermatology 94 (2.5) 351 (1.6) 3 1–15
Ophthalmology 84 (2.2) 305 (1.4) 2 1–48
Otorhinolaryngology 55 (1.5) 143 (0.6) 2 1–12
Other specialties 527 (13.9) 1,075 (4.8) 1 1–23
Nonstaff physicians 521 (13.8) 1,138 (5.1) 1 1–75
All 3,788 (100) 22,444 (1,000)
TABLE 3 Physicians Prescribing High-Exposure Glucocorticoid Drugs, by Practice Type

Who Bears Responsibility for Glucocorticoid-Exposed Patients in a Large Health Maintenance Organization?
232 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
average, care for only three such patients in their practice.Persons who are charged with developing managed care sys-tems to improve the quality of care for such patients shouldconsider identification and intervention systems built on phar-macy databases. Further, they should consider interventionstrategies based on the number of highly exposed patients ineach health care practitioner’s patient panel.
References
1. Reid IR, Heap SW. Determinants of vertebral mineral density in patientsreceiving long-term glucocorticoid therapy. Arch Intern Med 1990 (Dec);150(12): 2545–48.
2. Van Staa TP et al. Use of oral corticosteroids and risk of fractures. J BoneMiner Res 2000 (Jun); 15(6): 993–1000.
3. Silverman SL. Corticosteroid-induced osteoporosis: assessment, prevention,and treatment. J Musculoskel Med 1990 (July); 7(7): 14–27.
4. Mudano A et al. Glucocorticoid-induced osteoporosis: process of care andpatient outcomes in a managed care population [abstract]. Presented at theAmerican College of Rheumatology 63rd Annual Scientific Meeting, Boston,MA, November 13–17, 1999. Available at www.abstracts-on-line.com/scripts/abstracts/ACR/ACR.cfm/34860098 [Accessed on March 29,2000].
5. Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. American College of Rheumatology Task Force onOsteoporosis Guidelines. Arthritis Rheum 1996 (Nov); 39(11): 1791–801.
6. Eastell R et al. A UK Consensus Group on management of glucocorticoid-induced osteoporosis: an update. J Intern Med 1998 (Oct); 244(4): 271–92.
7. Scott EM, Gaywood I, Scott BB. Guidelines for osteoporosis in coeliac dis-ease and inflammatory bowel disease. British Society of Gastroenterology. Gut2000 (Jan); 46 Suppl 1: i1–8. [Based on review: Scott EM, Scott BB. A strategyfor osteoporosis in gastroenterology. Eur J Gastroenterol Hepatol 1998 (Aug);10(8): 689–96; discussion, 696–98.]
8. Saag KG et al. Alendronate for the prevention and treatment of glucocorti-coid-induced osteoporosis. Glucocorticoid-Induced Osteoporosis Intervention
Study Group. N Engl J Med 1998 (Jul) 30; 339(5): 292–99.
9. Cohen S et al. Risedronate therapy prevents corticosteroid-induced boneloss: a twelve-month, multicenter, randomized, double-blind, placebo-con-trolled, parallel-group study. Arthritis Rheum 1999 (Nov); 42(11): 2309–18.
10. Reid DM et al. Efficacy and safety of daily risedronate in the treatment ofcorticosteroid-induced osteoporosis in men and women: a randomized trial.European Corticosteroid-Induced Osteoporosis Treatment Study. J Bone MinerRes 2000 (Jun); 15(6): 1006–13.
11. Hill J et al. Management of patients at risk for glucocorticoid-inducedosteoporosis: predictors of treatment and surveillance in a managed care pop-ulation [abstract]. Presented at the American College of Rheumatology 63rdAnnual Scientific Meeting, Boston, MA, November 13–17, 1999. Available atwww.abstracts-on-line.com/scripts/abstracts/ACR/ACR.cfm/34860098[Accessed on March 29, 2000].
12. Schimmer BP, Parker KL. Adrenocorticotropic hormone; adrenocorticalsteroids and their synthetic analogs; inhibitors of the synthesis and actions ofadrenocortical hormones. In: Hardman JG et al., editors. Goodman &Gilman’s The pharmacologic basis of therapeutics. 9th ed. New York:McGraw-Hill, 1996: 1466.
13. Aagaard EM et al. Prevention of glucocorticoid-induced osteoporosis:provider practice in an urban county hospital. Am J Med 1999 (Nov); 107(5):456–60.
14. Buckley LM et al. Prevention of corticosteroid-induced osteoporosis:results of a patient survey. Arthritis Rheum 1999 (Aug);42(8): 1736–39.
15. Walsh LJ et al. Use of oral corticosteroids in the community and the pre-vention of secondary osteoporosis: a cross-sectional study. BMJ 1996 (Aug10): 313(7053): 344–46.
16. Buckley LM et al. Variations in physicians’ judgments about corticosteroidinduced osteoporosis by physician specialty. J Rheumatol 1998 (Nov); 25(11):2195–202.
17. Ettinger B, Chidambaran P, Pressman A. Prevalence and determinants ofosteoporosis drug prescriptions among patients with high exposure to gluco-corticoid drugs. Am J Manag Care. Forthcoming, June 2001.
18. Jasani MK et al. Corticosteroid-induced suppression of the hypothalamo-pituitary-adrenal axis: observations on patients given oral corticosteroids forrheumatoid arthritis. Q J Med 1967 (Jul);36 (143): 261–76.

P E R S P E C T I V E SR e f l e c t s t h e e d i t o r ’ s v i e w p o i n t o n i m p o r t a n t i s s u e s i n m a n a g e d c a r e p h a r m a c y
t is no surprise that patients and pay-ors are comparison-shopping for bet-ter prescription prices. It is also nosurprise that they are looking to
Mexico and Canada for lower prescriptionprices, since they go across the border tovisit retail stores for lower prices on clothes,TVs, DVDs, food, and other consumergoods. Clearly, consumers benefit from thepurchasing power of the U.S. dollar andfrom lower competitive prices. However,aside from the cost of drugs, there is some-thing larger happening. The prescriptiondrug market is going global for consumers.
Mexico and Canada are obvious placesfor consumers to comparison shop for pre-scription medications. But how muchinformation is available to purchasers tomake decisions about comparative costs inCanada or Mexico? A few years ago a clientof mine requested a survey of the viabilityof sending employees to Canada or Mexicoto purchase prescription drugs. With thepermission of the client, I’d like to share thegeneral lessons from this survey regardingavailable prices, information, and possiblelimitations for decreasing prescriptionprices.
A market basket of commonly usedmedications was used for comparison pur-poses, and drug wholesalers in Mexico andCanada were contacted for pricing. Theconditions of the survey were that thesepharmaceuticals must be in dosagestrengths commonly used in the UnitedStates, that the drugs be made by ethicalU.S. manufacturers or manufacturers thatoperated plants that had been inspected bythe Food and Drug Administration (FDA),and that for comparison purposes the drugswere available in quantities of 100 units perbottle. The market basket consisted ofomeprazole, atorvastatin, simvastatin, lan-soprazole, celecoxib, amlodipine, fluoxe-tine, pravastatin, diltiazem, and loratadine.
nnThe Environment in MexicoNot surprisingly, drug manufacturers inMexico, some of which are owned by U.S.-branded manufacturers, make drugs for
consumption in Mexico only. In order forpharmaceuticals to be imported into theUnited States, the Mexican plants must beregistered with the FDA and each productmust be filed with the FDA under “A NewDrug Application” (ANDA). (Our requestfor a list of registered plants in Mexicorequired several months for a responsefrom the FDA.) Citizens of the United Statesmay have prescriptions filled in “any will-ing” retail pharmacy in Mexico, althoughthe pharmacies may not carry medicationsin the prescribed quantities. Based on theexchange rate at the time, the market basketsold at an 89% discount to its price in theUnited States.
nn The Environment in CanadaBranded pharmaceuticals sold in Canadamust be approved by the Canadian equiva-lent of the FDA, known as the HealthProducts and Food Branch (HPB). Pharma-ceuticals manufactured in Canada cannotbe shipped into the United States, but prod-ucts manufactured in the United States canbe shipped into Canada. Certain HPB regu-latory requirements, however, still prevail(e.g., all products must be labeled inEnglish and French). Pharmacists inCanada cannot legally dispense prescrip-tions written by a U.S. physician, unlessapproved by a Canadian physician. Thereare however, many anecdotes of pharma-cists and physicians who have sub rosafacilitated the prescribing and dispensing ofmedications in Canada for U.S. patients.Based on the exchange rates at the time themarket basket sold at a 59% discount to itsU.S. price.
nn The Global EnvironmentWhile Mexico and Canada are geographi-cally close to the United States, the Internetprovides a virtual world without borders.Drug distributors (e.g., GlobeXPharma.comand RxMarketplace.com) can supply phar-macies with medications. Internationaldrug manufacturers are increasingly visiblein copying U.S. patents for branded phar-maceuticals. For example, Far-Manguinhos,
a state-owned manufacturer in Brazil, isselling acquired immunodeficiency syn-drome (AIDS) drugs for half the pricecharged by U.S. manufacturers.
Patent laws differ in every country, andin spite of World Trade Organization inter-national patent protections, countries areplacing their internal health care interestsahead of the patent requirements. Forexample, Brazilian companies are allowedby their government to manufacture abranded medication if a U.S. manufactureris not making it in Brazil three years afterthe patent is issued.
The overwhelming issue is that localinterests are beating out commercial inter-ests not just in drugs, but also in software,movies, music, and other commodities.Manufacturing and distribution is global sothat international drug companies maysubcontract-manufacture or they may man-ufacture their own products as well. Theresult is an expanding international marketfor patented and off-patent products.1
Consumers can now embrace the inter-national market, because they have priceinformation and access to competitiveprices over the Internet. The next stepshould be a free flow of marketing informa-tion about individual medications andcomparative features and options of thera-peutically similar medications. Informationthat manufacturers have traditionallyoffered only to providers (e.g., indications,frequency of dosing) should soon be avail-able to consumers.
The global train has left the station.Between the free flow of information, con-sumerism, and globalism, the health careworld will never be the same.
Reference
1. Jordon M, Brazil may flout trade laws to keepAIDS drugs free for patients. Wall Street Journal,February 12, 2001, B1, B4.
IPrescription Pharmaceutical Market Goes Global for Consumers
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 179

182 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
re disease-management pro-grams in correctional facilitieseffective from the perspectivesof patient- care outcomes and
financial justification? This is the ques-tion faculty within the Office of ManagedHealth Care Pharmacy Services (MHCPS)at the Texas Tech University HealthSciences Center School of Pharmacy(TTUHSC-SOP) are trying to answer.
In 1995, Texas Tech University HealthSciences Center (TTUHSC), through itsOffice of Managed Correctional Health Care(MCHC), contracted with TTUHSC-SOP tobe the primary provider of pharmaceuticalcare to Texas Department of CriminalJustice (TDCJ) offenders in west Texas.Although TTUHSC had been providinghealth care to TDCJ offenders since 1989, itwas not until the 1993 Texas legislativesession that a managed health care net-work was authorized. This staff-modelHMO has been previously described.1-3 In1995, TTUHSC expanded its involvementin corrections by becoming the health ser-vices provider for youth offenders housedwithin Texas Youth Commission (TYC)facilities.
In 1995, the TTUHSC-SOP establishedthe MHCPS as a pharmacy business unit todesign and deliver services to the TDCJ andTYC populations.4 The primary mission ofthe MHCPS has been to provide a high-quality, cost-effective pharmacy benefitwhile integrating managed care practiceinto the academic programs of the school.At issue was whether disease-managementprograms could control the escalating costsof providing drug therapy to correctionalpopulations.
nn The Service Plan The leaders of the MHCPS chose early inthe program to outsource drug distributionto a single provider for all offenders. Thispermitted MHCPS staff to focus on theirprescription benefit management (PBM)activities while maintaining administrativeoversight for the quality of drug distribu-
tion. Staff quality-assurance activities includ-ed monthly facility-quality meetings andquarterly pharmacy-inspection audits.
As it is at most managed care organiza-tions, the early focus of MHCPS was popu-lation-based pharmaceutical care, such asformulary management, target drug pro-grams, and drug-usage evaluation. Theseprograms, although effective in managingoutliers in drug utilization, were not as suc-cessful in dealing with the patient-care andfinancial issues arising from newer psychi-atric treatments, chronic-care drug therapy,an aging population, and managing andtreating patients with HIV and hepatitis C.
nnDisease Management In September 1998, the Texas State Boardof Pharmacy and the Texas Board ofMedical Examiners jointly put into effectrules permitting delegated drug-therapymanagement under a collaborative practiceagreement. These rules provided the impe-tus for MHCPS leadership to propose a shiftin strategy away from solely population-based pharmaceutical care to a model thatalso included patient-focused care and out-comes measurement. MHCPS and MHCHstaffs began to meet regularly to plan howto implement pharmacist-initiated disease-management clinics for target medical con-ditions where data suggested possible drugcost savings. Once a pilot clinic plan wasapproved, the School of Pharmacy draftedstandard collaborative practice agreementsthat conformed to Board rules; these werealso reviewed by the health science center’sInstitutional Compliance Officer.
The standardized protocol can beapplied to all disease management per-formed by School of Pharmacy facultyregardless of practice site. It includes:• a definition of the drug therapy
authorized by the supervising physi-cian,• a description of the frequency of
reporting to the supervising physician,and
• an overview of the drug therapy evalua-
tion/diagnostic protocol and drug therapyplan/management, which we have chosen to organize using the SOAP (subjective, objective, assessment, plan) format.
Currently, MHCPS staff is engaged inasthma, chronic bronchitis and emphysema, diabetes, hypertension, anticoagulation, general psychiatric, and hyperlipidemia management programs. For each,we collect longitudinal outcome data forevaluation of patient-specific improvements and impacts on drug costs for thefacility and for specific formulary items.For many of these chronic diseases, onlynow do we have sufficient data to analyzetrends for reporting to the RegionalCorrectional Health Care Pharmacy andTherapeutics Committee.
In summary, the MHCPS staff has developed a pharmaceutical care model that hasboth population-based and patient-specificcomponents. We continue to collect data tosupport this type of practice in correctionalhealth and to support our continuedinvolvement in this contract.
Roland A. Patry, Dr. P.H., FASHP, Professor ofPharmacy Practice and Associate Dean forPatient Care Services, and Butch Habeger,M.B.A., FASHP, Assistant Professor of Phar-macy Practice and Chief, Managed HealthCare Pharmacy Services, Texas Tech Univer-sity Health Sciences Center, School of Pharm-acy, Amarillo, TX.
References
1. Seals TD, Keith MR. Influence of patient information leaflets on anticonvulsant drug compliancein prison. Am J Health Syst Pharm 1997; 54:2585–87.
2. Keith MR, Coffey EL. Clinical training programfor distributive pharmacists. Am J Health SystPharm 1997; 54: 674–77.
3. Keith MR. A diabetes disease management planin a correctional staff model HMO. PT 1999; 24:227–32, 235–37.
4. Patry RA, Habeger HA. Managed care pharmacypractice at the Texas Tech Health Sciences CenterSchool of Pharmacy. JMCP 1999(Nov/Dec); 5(6):556–57.
S P O T L I G H T
A
I n n o v a t i v e M a n a g e d C a r e P h a r m a c y P r a c t i c e
Managed Pharmaceutical Care Within a Criminal Justice System
Objectives: After completing this contin-uing education program, readers will beable to:1. understand the general problems
actuaries face in pricing health insur-ance,
2. explain how insurance is priced dif-ferently from other products,
3. describe the role of an actuary in pric-ing health insurance, and
4. discuss the contributions pharmacists
can make to that work.
KEYWORDS: Actuaries, insurance, pric-ing, modeling, pharmacy trends
J Managed Care Pharm 2001: 233–37
Rear Window: Actuaries and Pharmacists—Toward a New Competency
CAROL J. MCCALL, F.S.A., M.A.A.A., is Executive Vice President ofManaged Care and Informatics for Allscripts, Libertyville, IL.
AUTHOR CORRESPONDENCE: Carol McCall, F.S.A., M.A.A.A, AllscriptsHealthcare Solutions, 2401 Commerce Dr., Libertyville, IL 60048; Tel.: 800-654-0889, x594; Fax: 847-680-9887; E-mail: [email protected].
The Academy of Managed Care Pharmacy is approved by the American Council on Pharmaceutical Education as a provider of continuing pharmaceutical education. Individuals may obtainup to 1 contact hour of credit or 0.10 Continuing Education Unit
(CEU). The ACPE number is 233-000-01-003-H04. Certificates will be mailedwithin eight weeks to participants who successfully complete the CE exam andachieve a score of 70% or more and submit the exam to AMCP prior to June30, 2002. Learning objectives and test questions follow on page 238.
Copyright© 2001 Academy of Managed Care Pharmacy, Inc. All rightsreserved.
Author
CONTINUING EDUCATION
s almost everyone is aware, pharmacy costs in recentyears have risen faster than any other component ofhealth care costs, with rates in the mid-to-highteens. Given the estimates of utilization and new
pharmaceutical product development, the trend is unlikely toslow in the near future. In fact, as the impacts of biotechnolo-gy and genomics research begin to unfold, pharmaceuticals arelikely to make up more and more of the health care dollar.Accurately predicting the uptake and cost of new productscould emerge as one of the most important issues health plansface.
Pharmacists and actuaries have an opportunity to worktogether to help estimate the effects of these new therapies. Thegoal of this article is to lay a foundation for pharmacists tounderstand the general issues actuaries face in pricing healthinsurance and to describe the increasing role pharmacists canhave in that work.
nnWhat Is an Actuary? Webster’s dictionary defines an actuary as a person who “com-putes premium rates, dividends, etc., according to probabilitiesbased on statistical records.” I like this explanation of what theactuary does: “If an insurance company were a car, the presidenthas her hands on the wheel, the chief marketing officer has hisfoot on the gas, the chief financial officer has his foot on thebrake, and the actuary is looking out the back window givingdirections.” But perhaps most appropriate is the Society ofActuaries’ creed, which is that the work of actuaries is to “substi-tute facts for appearances and demonstrations for impressions.”
Actuaries put a price tag on future risks. They have beencalled financial architects and social mathematicians becausetheir analytical and business skills help solve a variety of finan-cial and social problems. Specifically, actuaries improve finan-cial decision making by creating models to evaluate the currentfinancial implications of uncertain future events.
Some examples: A life-insurance company sells a policy toa new customer. How much premium should the companycharge to offset the risk of insuring that customer? An autoinsurance company is thinking about giving a discount to cus-tomers with anti-lock brakes. How big should the discount beto reflect the different risks of cars that have anti-lock brakesand those that do not? The Environmental Protection Agency isconsidering a new regulation that will reduce harmful refineryemissions but will cost jobs. Is it worth the cost to reduce therisks to the health of people in the community? These are ques-
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 233
Aby Carol J. McCall

tions actuaries must answer every day. They must therefore beeducated in a variety of subjects. An experienced actuary is notonly an expert in applied mathematics and statistics but also hasa deep understanding of finance, economics, business law, andaccounting.
If you have never met an actuary, that’s not unusual. Theactuarial profession numbers about 19,000 people in NorthAmerica. But don’t let that small number fool you. Actuaries puttheir special problem-solving skills to work in many differentbusiness situations, and their work has influenced people’s livesfor more than a century. Common areas of actuarial practice arepensions, life insurance and annuities, health, property andcasualty insurance, and benefits consulting. While this articleconcentrates on health insurance, actuaries influence a widerange of businesses and decisions.
nnPricing Health InsuranceActuaries get involved in a variety of different areas withinhealth plans, among them product development, legislativeactivities, medical management, claims payment practices, salesinitiatives, and provider contracting. The reason is that all theseareas can affect the underlying cost of insurance. The actuary’sprimary goal is to understand and incorporate the impacts ofthese things into the price of the product. Failure to do so prop-erly can have serious consequences on the financial health of acompany.
Insurance, rather than being a traditional type of product, isactually a promise in this case to pay for medical expensesincurred over a specified period. This means that the actual costof the product can not be known until the period is overbecause the number of claims is not known at the outset. Inother businesses, the costs of a product are known before theproduct is ever sold.
This uncertainty is not terribly onerous as long as the totalcosts for a population during the period are easy to predict.Because probability and statistical theory lend themselves wellto estimating the total costs for large numbers of people whenthe probabilities are stable, actuaries can calculate premiumsbased on probable overall costs.
Complicating this situation for health insurance, however, isthe fact that both the number and frequency of medical claimsare moving targets at all times. Charges for medical procedureschange regularly, as do the types of services that are availableand the frequency with which they are performed. In fact, treat-ments may emerge that were not even contemplated when theoriginal prices were set.
Because health expenditures are so dynamic, prices forhealth insurance are constantly updated. They are typically setmonthly and guaranteed for a 12-month period. Thus, if youare an employer group buying insurance in April, the price (therate) for your group remains the same until April of the follow-
ing year. If you were buying in May rather than April, your ratemight be higher, but it would also be good for 12 months..
nnPredicting ClaimsThe methods that actuaries use to determine prices can get fair-ly complicated but they all boil down to one thing: The price isequal to the expected claims, adjusted for expenses.
Price = (Expected claims) ÷ (1 – Expense load)
We will ignore the expense component. They are important insetting price, but all of the difficulty lies in expected claims. Tocalculate Expected claims, you need three things: Experienceperiod claims, claims adjustments factors, and trend.
Expected Claims = (Experience Period Claims) x(Claims Cost Adjustments Factors) x (Trend)
nn Experience Period ClaimsThis is the actuary looking out the rearview mirror: Experienceperiod claims are historical claims for some defined populationover a period of time. It is important that the experience repre-sent or be able to form a solid basis, after adjustments for thecosts of the population for which you are setting the rate. Theexperience could be for a single employer group or an entireblock of business. If you are pricing for large employer groupswith credible experience, you can use their own experience forsetting rates.
More likely, though, you are setting rates for an entire block ofbusiness (i.e., a collection of groups or insureds with similarproducts or other characteristics, such as group size, underwrit-ing method, or geography). While specific groups within theblock may have purchased coverage at different times and be pay-ing different premiums, many of the factors used to calculate therates are the same for the entire block of business. For pharmacy,a block of business could be Medicare+Choice, for example. Itwould be difficult to use the experience from a commercial blockof business to model pharmacy claims for Medicare, since theunderlying populations and cost drivers are so different.
nnClaims Cost AdjustmentOnce the experience period is selected, the adjustment factorsare used to adjust the historical claims up or down for anychanges that will affect your costs. They are adjustments forchanges that have already occurred, or that you know will occurbut are not entirely reflected in the experience period. Theirpurpose is to restate the historical claims as though the impactof any changes were in place during the entire experience peri-od just as they will be during the rating period.
Some of the things for which adjustments to historical expe-
Rear Window: Actuaries and Pharmacists—Toward a New Competency
234 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3

Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 235
rience might need to be made may be tied to the demographicsof specific groups, while others apply to the broader popula-tion. When they are group or insured-specific, the rates for thegroup or person may be adjusted based on their demographics.If they cannot be applied differentially during rating, it isimportant not only that the factors be accurate but that you esti-mate correctly the mix of these individuals or groups within theentire block of business. For example, if you have factors thatreflect differences in cost by age but do not (or cannot, perhapsby law) set different rates for people based on age, you wouldneed to estimate the average age mix you will have. Even if yourfactors are correct, if you miscalculate the mix, the final rateswould be wrong.
Regardless of the type of adjustment, the goal is to estimatehow changes in the following areas will affect claims costs. Foreach area, there is often an impact to both cost and utilizationfor different types of health care expenses. Actuaries need toestimate both.• Covered Services: What if, for example, the definition of
covered services changed so that you began to cover OTCs(over the counter medicines)? What if a new drug like Viagrawas coming onto the market and your contract did not havespecific language dealing with this type of medication? If youcover it, how will it affect costs?
• Benefit Levels and Cost Sharing: These are the copay,deductible, and other cost-sharing provisions. Benefit levelsaffect not only the net cost of a service but also utilization, asis clear from changes in drug copays . Small increases incopays can reduce costs by more than the change in the copayamount would indicate. Changes in office visit copays canalso affect drug costs: If office visit copays go down, prescrip-tion utilization will increase.
• Geographic Area: Many costs differ by area, often due to dif-ferences in physician practice patterns. If your historical expe-rience has the majority of business in one area but your salesorganization has decided to target another area , what sort ofadjustments should you make?
• Age/Gender/Family Mix: Costs can differ dramatically by ageand gender. What if you discovered that recently you havehad a higher proportion of younger people than you have hadhistorically? If one of the rating factors you apply to individ-uals is based on age, would you make any adjustments ? Arethere any “side effects” of this shift for which you do not haveindividual rating factors that could affect your future experi-ence?
• Group Size and Underwriting Method: Within commercialbusiness, smaller groups may have been underwritten andtherefore represent a different risk (or estimated cost) thangroups that have not. Underwriting (the process of risk selec-tion and classification) can wear off: Groups that were initial-ly classified as representing a certain level of risk can havetheir classification change as they regress toward the mean. In
addition, any change in your underwriting methods canchange the risk you attract or retain. Assuming you currentlyunderwrite your business, what would you predict to happento costs if the sales force tells you it will bring in twice asmany groups next year as this year? Would your answerchange if they told you that, in order to do so, you needed tochange how you underwrite your groups?
• Medical Management Programs: There are a large number ofprograms designed to control the medical costs of insureds.They include case, disease, and pharmacy management pro-grams that are targeting specific diseases, situations, or condi-tions. What would happen to costs if you implemented anasthma program within your block of business? How wouldyou reflect this in your rates?
• Provider Contracts: Changes to contracts with hospitals,physicians, labs, pharmacies, etc. take place throughout theexperience period and you need to adjust your experience toreflect the most recent deals. These adjustments must alsoreflect adding or removing providers . Such changes can influ-ence your sales to or retention of certain types of risks, orchange the geographic distribution of business. How wouldyou adjust your experience to estimate what would happen ifyou lost the flagship hospital out of your network?
• Legislative Changes: Changes in the regulatory environ-mentcould be classified under another category (such as man-dating coverage of certain drugs), but others are broader.What happens, for example, when the government institutesa program for Medicare that includes pharmacy coverage? Ifyou are offering pharmacy coverage to your Medicare +Choice population, will you retain these members? If so, willthey have the same cost levels as your members have had inthe past? Perhaps your coverage is richer than the alternativechoices and those who stay are only those who need the high-er coverage. In that scenario, your average claims costs perretained-member would be higher than they had been .
There are other areas where you might need to make adjust-ments, but this gives you some idea of the scope and variety ofthings that can impact costs, and thus insurance pricing.
nn Trend–The Last FrontierMost of the adjustments you have just made to your experience,while very important, did not move the claims through time.Most of them adjusted the historical claims up or down based onnew business dynamics; they did not take into account that, allother things being equal, the cost and utilization of health caretends to go up over time.
Trend is the last adjustment, the magic factor that moves theseadjusted historical claims through time to the period for whichrates are being set. It is meant to take into account your best pre-dictions for what is going to happen in the future after you makeall the previous adjustments. This is where time is not on yourside; there is a large gap between when you are doing the work
Rear Window: Actuaries and Pharmacists—Toward a New Competency

Rear Window: Actuaries and Pharmacists—Toward a New Competency
236 Journal of Managed Care Pharmacy JMCP May/June 2001 Vol. 7, No. 3
needed to calculate the rates and when they will be used.
nn Through the Looking GlassImagine it is September 1, 2000, and you need to set rates forJanuary 1, 2001. You cannot wait any longer; legislative require-ments and your internal systems for calculating premiumsrequire that rates be available within two weeks. The usualexperience period used is often one year, which is large enoughto be credible and avoids seasonality issues, so you decide touse July 1, 1999 through June 30, 2000, with a midpoint for theperiod of January 1, 2000.
Why the two-month gap between the end of the experienceperiod and now? This is called the completion period. It takestime for all the claims to be submitted to the payer for reim-bursement and processed as a claim. For pharmacy claims, mostof which are adjudicated on-line, claims are paid very quickly.The information on claims data can be made available almostimmediately. For medical claims, which are not adjudicated on-line, the process can take anywhere from 6 to 12 months.
Actuaries have ways to estimate the final claim liabilities formonths where only a portion of all claims have been submitted.Collectively, amounts for “incurred but not reported” (IBNR)claims are called reserves. Actuaries use various methods to cal-culate reserves. A typical method uses historical data to calcu-late how long it takes for a month of claims to be completelypaid. When these calculations indicate that 65%–75% or moreof claims are likely to have been paid, actuaries will start usingthese “completion” estimates to increase the known, paidamounts in each month by the percent estimated to remain,thus calculating the final liability. For months with less than thispercentage, usually the most recent two to three months, thereis insufficient information to make credible completion esti-mates, so reserves are set using different methodologies. That iswhy the two most recent months are typically avoided for expe-rience studies.
The rate you are setting is for January 1, 2001, but the esti-mate you make must be for all medical expenses for the 12-month period from January 1, 2001 through December 31,2001, with a midpoint of July 1, 2001). In order to move youradjusted claims forward from its midpoint of January 1, 2000 tothe midpoint of the rating period, the trend adjustment must befor 18 months. Because the time lags are long, estimating trendis critical. If you are off even by a little, the difference is com-pounded because the period over which trend must be estimat-ed is so long.
nnMeasuring TrendTrend should represent the change in the underlying dynamicsof cost and utilization for health care, not changes in cost perse. Looking at your financial statements or reports, you may seea trend of, say, 8% for pharmacy. This represents the change incosts, period over period, but not the underlying secular trend.
The 8% change could be the result of some change in the pastthat may not be repeated (such as increasing copays or intro-ducing three-tier benefits). To measure secular trend, you needto remove or normalize everything so you can see the underly-ing patterns absent any of those changes.
Here again we have actuaries looking out the rearview mir-ror. Trend is supposed to be an estimate of the direction anddegree to which our future will differ from our past, yet the onlydata we have is our historical data. When looking at historicalexperience, you need to look at different types of trends (12month, 3 month, 1 month) and use external estimates in addi-tion to those based on company experience. It is important toknow not only the degree of trend but where it is headed. Is itgoing up? Going down? Will it change direction? Are there newtechnologies on the horizon that are not yet taken into account?Are formularies being outlawed or severely restricted? When?What will the impact be?
nnMissing TrendEstimating trend incorrectly can be painful. Suppose we thinksecular trend will be 7% between our experience period and thetime for which we are setting our rates. Compounding 7% over18 months gives us the amount by which we would increaseour adjusted historical claims:
(1.070)^(18/12) = 1.107. If trend were really 9%, the factor should have been (1.090)^(18/12) = 1.138, and our estimates—and rates—would be too low by almost 3% (the ratio of 1.138 and 1.107).
Pharmacy trends can be difficult to estimate. Characteristicslike patient demand, consumer advertising, physician detailing,and technological development combine to make the dynamicsof pharmacy costs different from other types of health care; phar-macy trends may be more volatile. If, for example, pharmacycosts are 15% of total costs, missing pharmacy trends by 5% (per-haps due to the unanticipated demand associated with a newbreakthrough drug) can mean missing overall trend by 0.75%.
The situation is magnified by the fact that, whatever the rea-son for your initial trend estimate, it will take time for you to findout that your estimate was wrong. If you continue to use the samenumbers until you see new information emerge in your experi-ence and trend calculations, it can have a dramatic financialimpact—enough that, if continued over time or if large enough,it can create serious financial consequences for a health plan.
nnAll the King’s HorsesThis is where pharmacists and actuaries need to work together.While vice president of pharmacy management for a largehealth plan, I became aware that a partnership of actuaries andpharmacists (and clinicians in general) can create a compellingvalue. Together, we created new knowledge and methods that

proved vital to managing and estimating drug costs, techniquesthat neither of us could have created without the other. In anyhealth plan, I would recommend that pharmacists:•Partner with actuaries to help estimate trends for pharmacy
costs, recognizing that of the three elements discussed (expe-rience periods, adjustment factors, and trend), estimatingtrend is the hardest.
•Keep actuaries informed about new drug launches. The timelags associated with setting rates make the situation even morecritical, especially with the pace of new drug development.
• Jointly create models for emerging therapies and work togeth-er to estimate their impact. In doing so, work with them to:
•Understand the models and the populations being used in the
experience.•Document assumptions and sensitivity-test models so you
know which assumptions are the most important.•Track these assumptions against emerging experience so you
can make any necessary adjustments quickly.• Involve the actuaries in the design of medical and pharmacy
management programs, so they know what business will beaffected, when, and by how much.
The need for this type of partnership will continue to grow.Pharmacy trends show no signs of slowing; pharmaceuticals con-tinue to make up more and more of the health care dollar. Givenall the new drug research and likely resultant products, accurate-ly predicting their timing, uptake, and cost will become critical to
Rear Window: Actuaries and Pharmacists—Toward a New Competency
Vol. 7, No. 3 May/June 2001 JMCP Journal of Managed Care Pharmacy 237