Embed Size (px)
Citation preview

Maximizing the Prospective Payment System
in the Long-Term Acute Care Hospital
Maria Wooldridge, MA, RRTKindred Hospital - New Orleans, LA
Objectives
Review the impact of LOS Outliers and weighted distribution
of DRGs under PPS for LTACs Strategies to maximize
reimbursement.

History of PPS Medicare 1965 Tax Equity & Fiscal Responsibility Act
(TEFRA) 1982 Prospective Payment System 1983 Resource-Based Relative Value Scale 1992 Balance Budget Act 1997 SNF PPS 1998 LTAC PPS 2002 Purpose and motivation for the
development of DRG’s was to serve as the basis for utilization review and quality assurance in hospitals by providing a clear definition of a hospital product (Fetter 1985).

LTAC Payment Categories
Short stay outliers - LOS up to 5/6 of LTAC DRG geometric mean LOS
Normal payment - DRG specific weight times payment rate
Normal payment with high cost outlier - high cost outliers exceed a DRG specific threshold
Interrupted stay

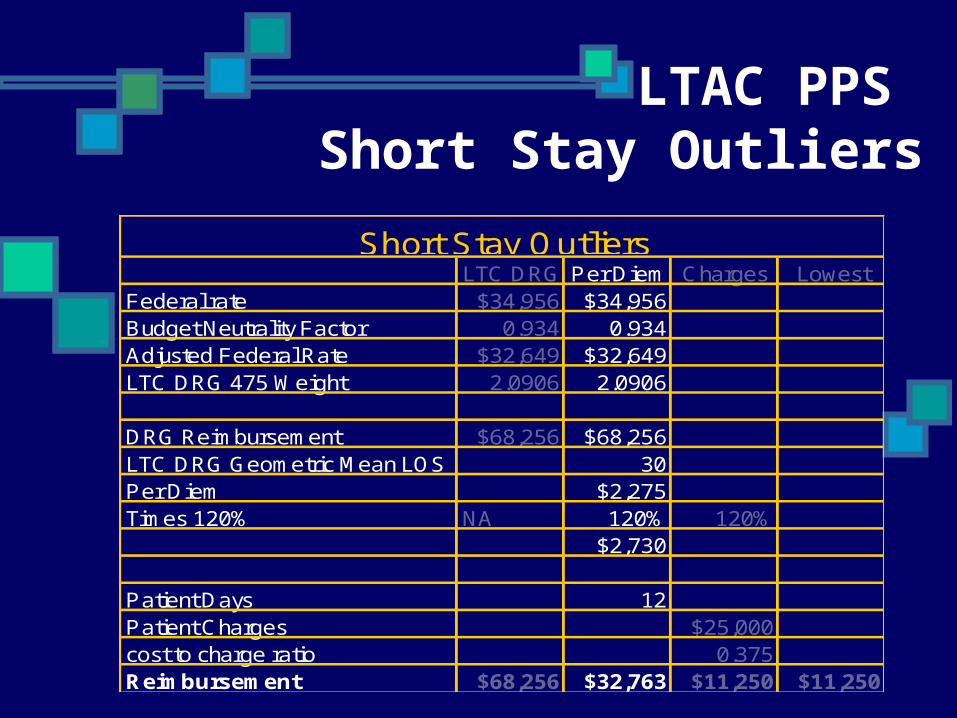
Short Stay Outliers
Short stay outliers - LOS up to five/sixths of geometric mean DRG LOS.
Payment based on least of three calculations Normal DRG payment Per diem based on DRG payment times
120 percent Cost of patient care (patient charges time
cost to charge ratio times 120 percent).

LTAC PPS Short Stay Outliers
LTC DRG Per Diem Charges LowestFederal rate $34,956 $34,956Budget Neutrality Factor 0.934 0.934Adjusted Federal Rate $32,649 $32,649LTC DRG 475 Weight 2.0906 2.0906
DRG Reimbursement $68,256 $68,256LTC DRG Geometric Mean LOS 30Per Diem $2,275Times 120% NA 120% 120%
$2,730
Patient Days 12Patient Charges $25,000cost to charge ratio 0.375Reimbursement $68,256 $32,763 $11,250 $11,250
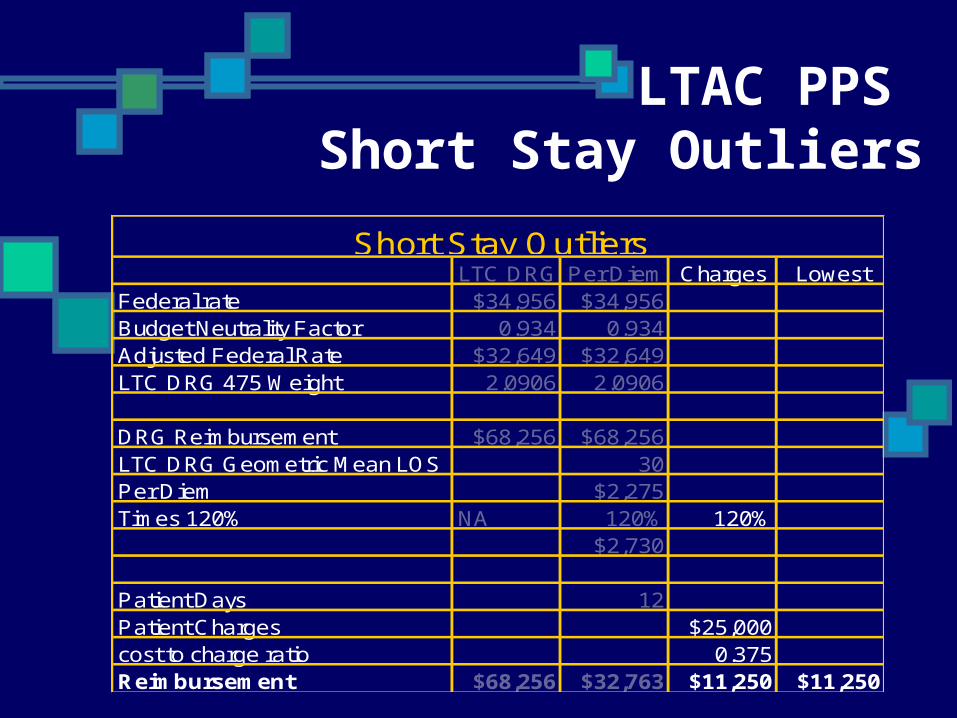
Short Stay Outliers
LTAC PPS Short Stay Outliers
LTC DRG Per Diem Charges LowestFederal rate $34,956 $34,956Budget Neutrality Factor 0.934 0.934Adjusted Federal Rate $32,649 $32,649LTC DRG 475 Weight 2.0906 2.0906
DRG Reimbursement $68,256 $68,256LTC DRG Geometric Mean LOS 30Per Diem $2,275Times 120% NA 120% 120%
$2,730
Patient Days 12Patient Charges $25,000cost to charge ratio 0.375Reimbursement $68,256 $32,763 $11,250 $11,250
Short Stay Outliers
LTAC PPS Short Stay Outliers
LTC DRG Per Diem Charges LowestFederal rate $34,956 $34,956Budget Neutrality Factor 0.934 0.934Adjusted Federal Rate $32,649 $32,649LTC DRG 475 Weight 2.0906 2.0906
DRG Reimbursement $68,256 $68,256LTC DRG Geometric Mean LOS 30Per Diem $2,275Times 120% NA 120% 120%
$2,730
Patient Days 12Patient Charges $25,000cost to charge ratio 0.375Reimbursement $68,256 $32,763 $11,250 $11,250
Short Stay Outliers
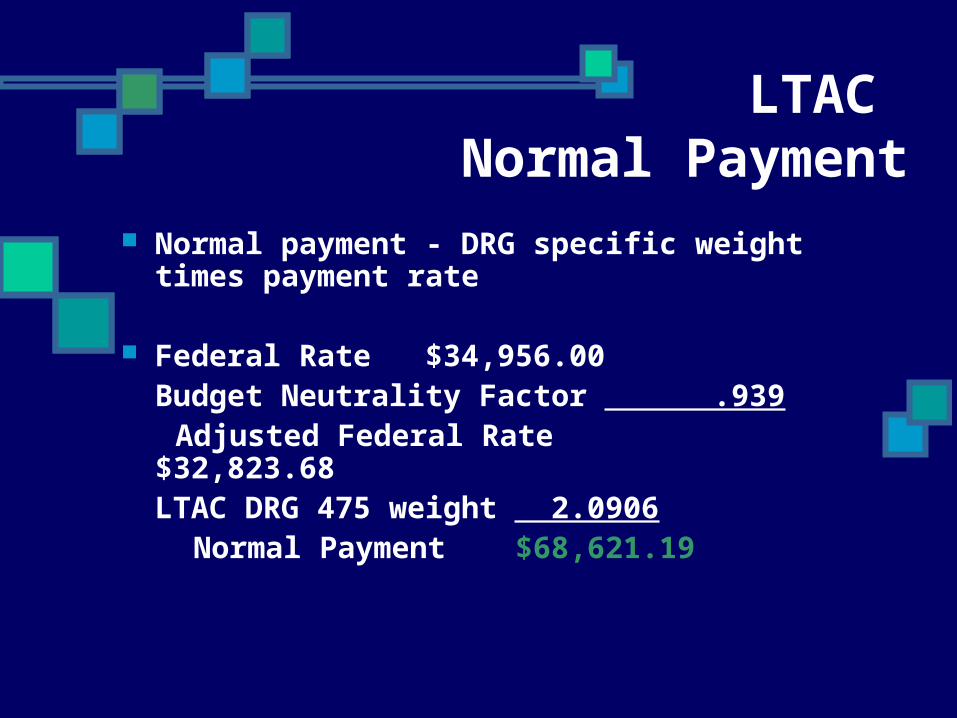
LTAC Normal Payment
Normal payment - DRG specific weight times payment rate
Federal Rate $34,956.00Budget Neutrality Factor .939
Adjusted Federal Rate $32,823.68LTAC DRG 475 weight 2.0906
Normal Payment $68,621.19

LTAC High Cost Outliers
Normal payment with high cost outlier - high cost outliers exceed a DRG specific threshold
Estimated patient cost (Patient charges times cost to charge ratio) 172,000DRG 475 specific outlier threshold 90,314Cost in excess of threshold
81,686Marginal cost factor
80%High cost outlier payment
$65,349Normal payment
$68,621Total
$133,970

Interrupted Stay (not a payment
category) Defined as a case in which an LTAC Patient is
discharged to an inpatient acute care hospital, an inpatient rehab facility (IRF) or a skilled nursing facility (SNF). for a period of time less than a threshold defined by CMS
Thresholds are: A. For 3 days or less
B. For acutes, 9 days or less C. For inpatient rehab facilities, 27 days or less
D. For SNF’s 45 days or less
Patient discharge & readmission will count as one
discharge and receive one DRG payment if threshold is not met.
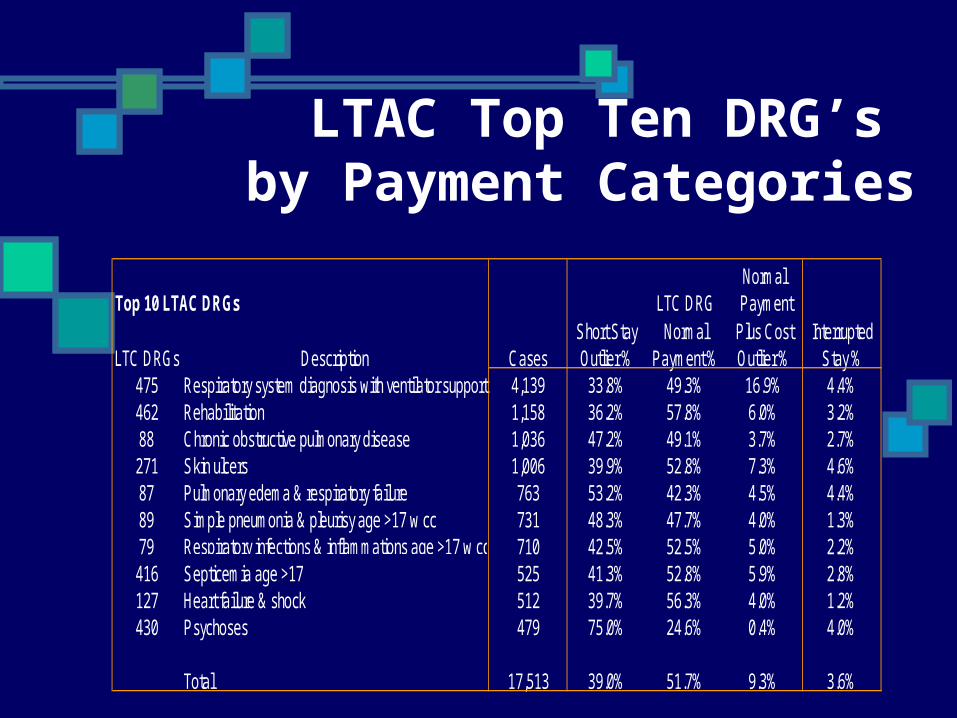
LTAC Top Ten DRG’s by Payment Categories
NormalTop 10 LTAC DRGs LTC DRG Payment
Short Stay Normal Plus Cost InterruptedLTC DRGs Description Cases Outlier % Payment % Outlier % Stay %
475 Respiratory system diagnosis with ventilator support 4,139 33.8% 49.3% 16.9% 4.4%462 Rehabilitation 1,158 36.2% 57.8% 6.0% 3.2%88 Chronic obstructive pulmonary disease 1,036 47.2% 49.1% 3.7% 2.7%271 Skin ulcers 1,006 39.9% 52.8% 7.3% 4.6%87 Pulmonary edema & respiratory failure 763 53.2% 42.3% 4.5% 4.4%89 Simple pneumonia & pleurisy age >17 w cc 731 48.3% 47.7% 4.0% 1.3%79 Respiratory infections & inflammations age >17 w cc 710 42.5% 52.5% 5.0% 2.2%416 Septicemia age >17 525 41.3% 52.8% 5.9% 2.8%127 Heart failure & shock 512 39.7% 56.3% 4.0% 1.2%430 Psychoses 479 75.0% 24.6% 0.4% 4.0%
Total 17,513 39.0% 51.7% 9.3% 3.6%
OIG Guidance
Reasons for patient encounter History and Physical Progress Notes Treatment Plan Referrals and consultations Patient Education Recommend follow up care Documented rationale for services Documentation supporting medical necessary Test Results Relevant health risk factors Referrals and consultations Prescriptions
Basic Rules for Improving
Documentation The physician documentation is the key
element that supports accurate coding and timely submission of claims
Attending physician is the ultimate determining authority
Provide complete, clear and specific clinical documentation
Document the rationale behind their treatment decisions
Physicians should provide complete documentation
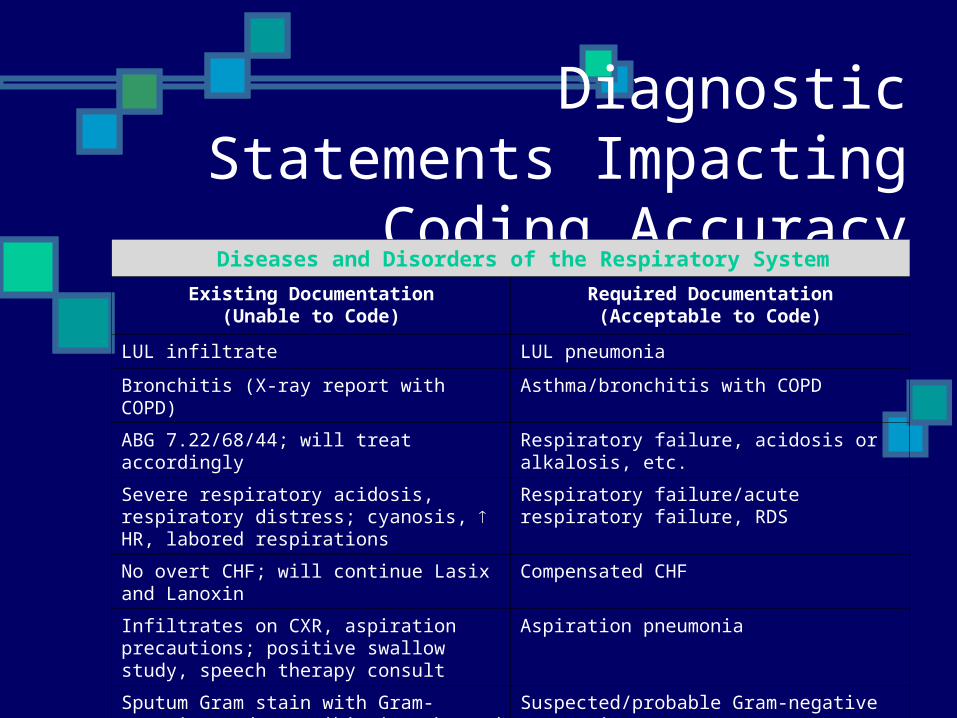
Diagnostic Statements Impacting Coding
AccuracyDiseases and Disorders of the Respiratory System
Existing Documentation(Unable to Code)
Required Documentation(Acceptable to Code)
LUL infiltrate LUL pneumonia
Bronchitis (X-ray report with COPD) Asthma/bronchitis with COPD
ABG 7.22/68/44; will treat accordingly Respiratory failure, acidosis or alkalosis, etc.
Severe respiratory acidosis, respiratory distress; cyanosis, HR, labored respirations
Respiratory failure/acute respiratory failure, RDS
No overt CHF; will continue Lasix and Lanoxin Compensated CHF
Infiltrates on CXR, aspiration precautions; positive swallow study, speech therapy consult
Aspiration pneumonia
Sputum Gram stain with Gram-negative rods; antibiotics changed to Fortaz/Gentamycin
Suspected/probable Gram-negative pneumonia
Bronchoscopy with biopsy Bx of lung or transbrochial lung Bx

Common Procedures & Impact on DRG
Assignment
No Impact PICC Lines Biopsy EGD PEG Swan Ganz PEJ
Impact Excisional
Debridement Vent Cholecystectomy Amputation Tracheostomy
Diseases and Disorders of the Respiratory
System DRG 76/77 - Other Resp System O.R. Procedures w/ CC &
W/O CC DRG 79/80 - Respiratory Infections & Inflammations Age
>17 w/CC (W/O CC) DRG 87 - Pulmonary Edema & Respiratory Failure DRG 88 - Chronic Obstructive Pulmonary Disease DRG 89/90 - Simple Pneumonia & Pleurisy Age >17 w/CC
(W/O CC) DRG 475 - Respiratory System Diagnosis With Ventilator
Support Eliminated)

DRG Progression Timelines for DRG Assignment
On registration Within 3 business days of admission Concurrently Within 6 days of discharge
The goals Timely and accurate DRG assignment Discharge DRG assigned match the final DRG
submitted on the claim How
Quality Documentation Timely Communication Accurate Coding and DRG Assignment
Review of Relevant Literature
Commentary on an examination of winners and losers under Medicare's PPS Qualitative study of 13 matched hospitals. Winners equaled
Strength of Leadership Ability to respond quickly to market / cost-
saving opportunities Productive Physician / administration
relationships Strategies to improve efficiency
PPS Success
Multi-factored approach You play a KEY role
Input - Front Door Management Throughout - Patient Management Output - Back Door Management

Input - Front Door Management
Effect on Referral Sources
Post Acute Referral Continuum
Prior adoption to PPS
Last hope
Educate the referral sources
Input - Front Door Management
Patient Selection What Role do you play in Review of
Patients for admission? Role of Clinical Liaisons (ACM’s)
Knowledge base? Expertise Review their intakes / thoroughness Conflicting motivators
Prevent short stay admissions! Develop quality review / questionnaire

Throughout – Patient Management
Complete drill-down as to why patients are being transferred out
Front door issues? Patient Management issues?
Review clinical capabilities. Advance the skill set of clinicians.

Throughout – Patient Management
Patient care conferences Frequency Attendees Knowledge of staff regarding short-term / long-
term goals / management Operational Silo’s?
Coordination of Care “Theory vs. Practice” Report
Outcome focus Documentation
Throughout – Patient Management
Focus on what is preventable Benchmark reports Nosocomial Infections - Back door Management
VRE C-Diff Pneumonia’s BSI MRSA Nosocomial Wounds

Throughout – Patient Management
Control of Costs (within your domain) Labor
Skill Mix Agency Patient placement and effect on HPPD
Supplies Rental Costs
Throughout – Patient Management
Influence on Physician practice patterns They currently practice in PPS
environments? Admission orders Patient management pathways / Best
Clinical practices Level of awareness of interdisciplinary
recommendations / communication
Output – Backdoor Management
Patient family discharge process Up-front family conference
Discharge planning Discharge options Medicaid application Explanation of benefits Healthcare Proxy Guardianship
Summary
Your Role is key Communicate and educate
“What we know and where we are going?”
Constant evolving process Network Thank You...