Embed Size (px)
Citation preview

iotttfgmn5
maletlata
0
d
SURGICAL ONCOLOGY AND RECONSTRUCTION
J Oral Maxillofac Surgxx:xxx, 2011
Maxillary Metastasis of a MedullaryThyroid Carcinoma in a 21-year-oldWoman 7 years After Thyroidectomy
Samira Basir Shabestari, DMD, MSc,* Iman Shirinbak, DMD,†
and Farzaneh Agha-Hosseini, DMD‡
cluc
Metastasis of the oral cavity is a rare phenomenon andrepresents approximately 1% of all oral malignanttumors.1 Tumor metastasis to the jaw most oftennvolves the posterior of the mandible. Metastases toral soft tissue sites represent less than 0.1% of oralumors.2,3 As noted by Zachariades, the mandible ishe site of involvement in 58.5% of metastatic tumorso the oral cavity and jaws, and the involvement rateor maxilla, oral soft tissues, and the major salivarylands is 11%, 25.8%, and 4.7%, respectively.4 Theaximal incidence for metastatic tumors of head and
eck occurs in the seventh decade ranging between5.2 and 64.5 years with a mean age of 60 years.3,5
The incidence of oral metastases is higher in malescompared with females (1.9 ratio).5 The most com-
on symptoms associated with metastases to the jawsre pain, paresthesia, tooth mobility, and gingival en-argement. Metastases to oral cavity soft tissue arextremely rare.2 The primary sites for metastasis tohe jaws and oral soft tissues are malignancies of theung, breast, prostate, gastrointestinal tract, kidney,nd liver.2,3 The prognosis of patients with metastasiso the oral cavity is poor with a median survival ofpproximately 6 months.3
Thyroid gland carcinoma is more common amongfemales with a female-to-male ratio of 8:3.6 Thyroid
*Assistant Professor, Department of Oral Medicine, Ayatollah
Mousavi Hospital, Zanjan University of Medical Sciences, Zanjan,
Iran.
†Assistant Professor, Department of Oral and Maxillofacial Sur-
gery, Ayatollah Mousavi Hospital, Zanjan University of Medical
Sciences, Zanjan, Iran.
‡Professor of Oral Medicine, Department of Oral Medicine, Den-
tal Research Center, School of Dentistry, Tehran University of
Medical Sciences, Tehran, Iran.
Address correspondence and reprint requests to Dr Shabestari:
Department of Oral Medicine, Zanjan University of Medical Sci-
ences, Zanjan, Iran; e-mail: [email protected]
© 2011 American Association of Oral and Maxillofacial Surgeons
278-2391/11/xx0x-0$36.00/0
oi:10.1016/j.joms.2011.04.005
1
gland carcinoma in people younger than 18 years israre and the 10-year survival rate for these patients isabout 40%.7 Three main histological types of thyroidancer have been described: differentiated, medul-ary, and anaplastic. Medullary carcinoma is the termsed to describe the type of thyroid gland malignancyomposed of parafollicular cells.1 The frequency of
medullary carcinoma is less than the differentiatedforms and it has a tendency to act aggressively.1,8
We report an unusual case of medullary thyroidcarcinoma (MTC) metastatic to the anterior maxilla 7years after a thyroidectomy in a 21-year-old woman.
Case Report
A healthy, 1-month postpartum 21-year-old woman com-plained of an expansile, painless swelling in the anterior leftmaxilla, which had progressed in size over the last 2months. The patient also complained of back pain, sweat-ing, chills, dysphagia, and loss of appetite during the pre-ceding 2 weeks. She had undergone vaginal delivery 3weeks previously. Her past medical history was significant
FIGURE 1. Extraoral view of patient: The patient was pale and thenasolabial fold was flattened.
Shabestari, Shirinbak, and Agha-Hosseini. Maxillary Metastasisof a Medullary Thyroid Carcinoma. J Oral Maxillofac Surg 2011.
for thyroidectomy 7 years before at age 15, for what she

nmc
T
mcps
sanpn
fgdhw
eTl
frHtTl
rtd
So
2 MAXILLARY METASTASIS OF A MEDULLARY THYROID CARCINOMA
thought was a goiter. Levothyroxine was subsequently pre-scribed, although the patient took the medication only for ashort time.
Facial examination showed that the mass extended frommidline of the maxilla to the left periorbital region. The oralswelling had caused disappearance of the left nasolabial folddue to fullness of the buccal vestibule and slight deviationof left nostril. Diminished sensation of the left upper part ofher nose, lip, and nasofrontal area was present (Fig 1).
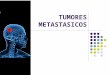
Intraoral examination noted a tender swelling of the leftpalate and mucobuccal fold with a variable consistencyranging from hard and firm to rubbery. The mass appeareddarker in color than that of normal oral mucous membrane(Fig 2A). The left maxillary second and third teeth (teeth
umber 10 and 11 according to the universal system) hadigrated and showed grade 2 mobility, with no evidence of
aries (Fig 2B).The neck showed a scar from prior thyroid surgery.
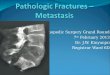
here was no cervical lymphadenopathy.A panoramic radiograph showed a relatively well-definedixed radiolucency of 2 � 3 cm. No evidence of dental
aries, retained roots, or sinus involvement was observed. Aoorly defined outline was seen around the upper leftecond and third teeth (Fig 3A). On computed tomographic
FIGURE 2. Intraoral view: A, Buccal vestibular swelling with dis-placement of teeth number 10 and 11. B, Left palatal swelling dueto the lesion.
Shabestari, Shirinbak, and Agha-Hosseini. Maxillary Metastasis
eof a Medullary Thyroid Carcinoma. J Oral Maxillofac Surg 2011.can assessment, a destructive mass in the left maxillarylveolar process was seen that projected into the subcuta-eous and cutaneous tissue. Neighboring teeth were dis-laced by the mass. The paranasal sinuses were otherwiseormal (Fig 3B).In addition to benign and malignant neoplasms, the dif-
erential diagnosis included an aggressive central giant cellranuloma, due to color and invasiveness of the lesion andisplacement of the teeth and pyogenic granuloma, due toer pregnancy within the last month. An incisional biopsyas performed.The histopathology consisted of hypercellular small pack-
ts of short spindle cells in an amyloid vascular background.he pathology report was “undifferentiated carcinoma with
eft maxillary bone invasion.”Immunohistochemistry analysis showed positive results
or pan-cytokeratin, calcitonin, and TTF-1, all as ready-to-useeagents from NovoCastra (Leica Microsystems, Germany).owever, the test was negative for thyroglobulin at concen-
ration 1:100 (Dako Cytomation, Denmark) in tumor cells.he overall findings were diagnostic for metastatic medul-
ary carcinoma of thyroid gland (Fig 4).Further information obtained regarding her prior thyroid-
FIGURE 3. Radiographic examination: A, Panoramic view: aelatively well-defined mixed radiolucency was seen. B, computedomographic scan view: left maxillary teeth were displaced byestructive mass.
habestari, Shirinbak, and Agha-Hosseini. Maxillary Metastasisf a Medullary Thyroid Carcinoma. J Oral Maxillofac Surg 2011.
ctomy informed us that she had been diagnosed with

rh
hmfdsrbvrd
arwa
S f a Me
SHABESTARI, SHIRINBAK, AND AGHA-HOSSEINI 3
medullary carcinoma of the thyroid. She had no familyhistory of thyroid disorders. She had undergone “centralnodal dissection, total thyroidectomy” surgery and had levo-thyroxine administration for 1 year. She had been under theimpression that an esthetic procedure had been performedfor a goiter.
Based on previous and recent pathology reports andalso consultation with an oncologist, a diagnosis of “met-astatic medullary thyroid carcinoma to left maxillary gin-gival with bone destruction” was confirmed. The patientwas referred to an oncologist for chemotherapy, but waslost to follow-up.
Discussion
Metastases to oral cavity are uncommon, but shouldnot be overlooked by clinicians. In about 20% ofcases, the oral metastasis is the first clinical sign of themalignancy.1 Metastatic tumors to the jaws originatefrom distant body sites, excluding lesions that are theresult of direct extension from neighboring sites orthose due to local recurrence.9 There are diverseoutes of metastasis to the jaws, including lymphatic,
FIGURE 4. Immunohistochemistry analysis: �400 (A), pa
habestari, Shirinbak, and Agha-Hosseini. Maxillary Metastasis o
ematogenous, and, rarely, iatrogenic reasons. The
ematogenous route is considered the most commonode for metastasis to jaw bones. The real incidence
or tumor metastasis to jaw bones is unknown. This isue to the fact prior to positron-emission tomographycanning, the jaws are not routinely involved in theadiographic metastatic search nor in autopsies. It haseen postulated that the incidence of jaw bone in-olvement to be less than other bones because theed marrow and blood vessels in the jaws tend toecrease with age.10 Based on several reports by dif-
ferent authors, approximately 1% of oral malignanciesare of metastatic origin.9 Metastases to the oral softtissues are much rarer, representing less than 0.1% oforal tumors.2 Common sources of metastases indicate
gender-associated variation. Breast, ovaries, and thy-oid are considered as common sources in females,hile lungs, prostate, kidney, and liver are more prev-
lent in males.10
Evidence for the presence of tumors may be pain,swelling, mobility of tooth, delay in healing of extrac-tion socket, and pathological fractures or paresthe-
eratin�, (B) calcitonin�, (C) TTF-1�, and (D) thyroglobulin.
dullary Thyroid Carcinoma. J Oral Maxillofac Surg 2011.
n-cytok
sia.2,9,11 In the present case, swelling, migration, and

ccgmoi
4 MAXILLARY METASTASIS OF A MEDULLARY THYROID CARCINOMA
mobility of teeth and paresthesia of relatively largearea were seen. Metastatic tumors arising in or other-wise involving the oral soft tissues may frequently beconfused with pyogenic granuloma, peripheral giantgranuloma, peripheral fibroma, and periodontal ab-scesses,1,2 as these lesions are rarely ulcerated. Be-ause the patient had recently been pregnant, 1 of theonsiderations for differential diagnosis was pyogenicranuloma. Radiographic findings in metastatic tu-ors to the jaw structure may range from the absence
f any manifestation to a lytic or opaque lesion withll-defined margins.2,9 In our case, the radiolucencywas more well-defined.
There are 3 histologic categories of thyroid cancers:differentiated, medullary, and anaplastic. MTC has anintermediate prognosis between the relatively goodprognosis of most differentiated forms and the dismalprognosis of anaplastic thyroid carcinoma. MTC canbe sporadic or can occur as a hereditary form in up to25% of cases. The hereditary MTC syndromes, multi-ple endocrine neoplasia (MEN) type 2, affects approx-imately 1 in 30,000 individuals and consists of subcat-egories MEN 2A (Sipple’s syndrome), familial MTC,and MEN 2B.12 Hereditary forms can be diagnosedwith a positive family history and/or other manifesta-tion of MEN syndrome. Sporadic MTC, unlike hered-itary forms, is usually diagnosed late with regionalmetastasis. That is because of the difficulty in diagno-sis due to different morphologies.13
Systemic chemotherapy has limited success rate intreatment of the metastatic MTC cases. There aresome recommended chemotherapy regimens for thetreatment of MTC, including cyclophosphamide, dac-arbazine, and vincristine or dacarbazine, and fluorou-racil or bleomycin, doxorubicin, and cisplatin, whichhave produced some partial responses.14
New strategies to treat metastatic MTC cases areradioimmunotherapy and vaccine-based therapies.
Compounds have been introduced that block kinasesthat are involved in the pathogenesis or progressionof cancer. Recently, several kinase inhibitors havebeen under evaluation that may have important clin-ical advantages.15 However, it is important to con-sider the oral region as a metastatic source for thyroidgland malignancies.
Acknowledgment
Thanks to Dr Eric Dierks for help in putting this article intoproper English.
References1. Petteli A, Fioroni M, Rubini C: Gingival metastasis from a
medullary thyroid carcinoma: Case report. J Periodontal 71:112, 2000
2. Greenberg M, Glick M Burket’s Oral Medicine (ed 11). Phila-delphia, PA, Lippincott, 2008, pp 174
3. Vander R, Buter J, Vander I: Oral metastases: Report of 24cases. Br J Oral Maxillofac Surg 41:3, 2003
4. Zachariades N: Neoplasm metastatic to the mouth, jaws, andsurrounding tissues. J Craniomaxillofac Surg 17:283, 1989
5. Lucic M, Mandiovic M, Vukoje N: Metastatic carcinoma of theneck: [?] clinical analysis of our cases. Med Arch 43:9, 1989
6. Danese D, Gardini A, Farsetti A: Thyroid carcinoma in childrenand adolescents. Arch Payhol Lab Med 124(10);1, 440, 2000
7. Little W, Falace D: Dental Management of Medically Compro-mised Patients (ed 7). St. Louis, MO, Mosby, 2008, pp 261-263
8. Steven P, Hodak D, Kenneth D: Thyroid Carcinoma (ed ).Human Press, 2006, pp 497-508 [ISBN:59259-995-0 (online)]
9. Adebayo E, Ajike S: Report of six cases of metastatic jaw tumorsin Nigerians. Niger J Surg Res 6:30, 2004
10. Kaveri H, Punneya V, Tayor A: Metastatic thyroid carcinoma tothe mandible. J Oral Maxillofac Pathol 11:32, 2007
11. Anil S, Lal PM, Gill DS, et al: Metastasis of thyroid carcinoma tothe mandible. Case report. Aust Dent J 44:56, 1999
12. Mulligan LM, Kwok JB, Healey CS, et al: Germ-line mutations ofthe RET proto-oncogene in multiple endocrine neoplasia type2A. Nature 363:458, 1993
13. Moley JF, Fialkowski EA: Evidence-based approach to the man-agement of sporadic medullary thyroid carcinoma. WorldJ Surg 31:946, 2007
14. Lenhard RE, Osteen RT, Gansler T: Clinical Oncology (ed 3).Blackwell, 2000, pp 644
15. Cohen EE, Rosen LS, Vokes EE, et al: Axitinib is an activetreatment for all histologic subtypes of advanced thyroid can-
cer: Results from a phase II study. J Clin Oncol 26:4708, 2008