Slide 1
Trauma, attachment & adoptionEmphasing individuals in
assessment & treatmentDr Matt WoolgarConsultant Clinical
PsychologistNational Adoption & Fostering ServiceSouth London
& Maudsley NHS Foundation TrustSenior Researcher, National
Academy for Parenting Research, Kings College London& Lecturer
Childrens & Young People's IAPT UCL/KCL
[email protected]
http://www.national.slam.nhs.uk/services/camhs/camhs-adoptionfostering/
Trauma & AttachmentBig constructs, but highly relevant for
adopted children
But can these big constructs become barriers to specifying what
exactly an adopted child & their family need?
Can they obscure the individuality & diversity that the
science tells comes from maltreatment?Trauma - Psychiatric
definitionsICD-10a stressful event or situation (of either brief or
long duration) of an exceptionally threatening or catastrophic
nature, which is likely to cause pervasive distress in almost
anyoneDSM-IVboth(a) loss of "physical integrity", or risk of
serious injury or death, to self or others, and (b) a response to
the event that involved intense fear, horror, or helplessness
Trauma vs. Maltreatment/NeglectIntense, usually single events, do
not capture the range of possible early experiences Low level,
chronic negative experience e.g., neglect Good science re. the
biological, psychological & social impact of maltreatment &
neglectConsequences quite different for different types of
maltreatment & neglectMore precision if we state the type,
frequency and timing of maltreatment?
Maltreatment & Neglect: Bio-psycho-social impact Emerging
neuroscience demonstrates that early maltreatment increases risks
for neurodevelopmental problemsBut the science is much more complex
than pictures of damaged brains might implyInvolves more domains
& in complex ways
Service planning for adopted children should be based on a
sophisticated understanding of the science and the
bio-psycho-social implications of maltreatmentMaltreatment impacts
upon bio-psycho-social adaption
EnvironmentBiologicalPsychologicalBehaviouralMaltreatment
impacts upon many levels within bio-psycho-social domains
Maltreatment, Neglect, Parenting, School,
PeersBrainGenesPhysiologyImmunologyEnvironmentBiologicalPsychologicalBehaviouralCognitionAttachmentMemoryMotivationAggressionCryingProsocialAvoidingMaltreatment
impacts upon many levels
Maltreatment, Neglect, Care, Parenting,
PeersBrainGenesPhysiologyImmunologyEnvironmentBiologicalPsychologicalBehaviouralCognitionAttachmentMemoryMotivationAggressionCryingProsocialAvoiding
Each child is uniqueSpaghetti complex and hard to trace or
specify each individual link / pathway Each plate is uniqueEach
adopted child also has a unique history & formulationCannot
lump all adopted children togetherBecause she is adopted she is
XTraumatisedBrain differentAttachment
problemsAnxiousShamefulWithout even seeing her, I can tell you she
needs Y
[cf. RM services]10Differential SusceptibilityPeople differ
[e.g., genetically] in how much they respond to both positive &
negative experiences
11Differential SusceptibilityPeople differ [e.g., genetically]
in how much they respond to both positive & negative
experiences
12Responses are IndividualA bigger dose of stress is worse on
average
But response to stress variesSusceptible child may show big
problems from only a small dose of maltreatmentResilient child may
be resistant to a larger doseBut response to treatment can also
varySusceptible child may respond well to small intervention if
precisely tailored to meet his/her needsResilient child may show
much smaller response13Differential susceptibility in siblingsBoy
is older & was exposed to significantly higher level of
maltreatment but doing okay nowGreat effort expended to address his
greater traumaNot bothered either way by treatment so far
Younger girl had less maltreatment, yet struggling in all
domains [except some peers]Challenging to family & system
[needy & volatile]Very keen for treatment sensitive, curious
& rewardingGreat potential, but how to help her?Dandelions
& OrchidsDandelions do okay in most environmentsOrchids will do
very badly in poor, BUT also in good but not quite right,
environmentsOrchids will flourish in exactly right, tailored or
personalised environmentsA good environment for the brother may
still not be precisely right for the sisterPuzzling when decent
parenting/school good enough for the more maltreated sibling but
not enough for the less maltreated oneFocusing on the trauma or
shared experiences of siblings can obscure these crucial
differencesSubtle, complex & unique presentations(in which
common disorders still identifiable)???MoodTraumaLearning
disabilitySchoolproblemsSocial skills deficitsAnxiety1616The allure
of rare disorders in maltreated children (Haugaard, 2004)Although
more common diagnoses, such as ADHD, conduct disorder, PTSD, or
adjustment disorder, may be less exciting, they should be
considered as first line diagnoses before contemplating any rare
condition such as RAD or an unspecified attachment disorder Chaffin
et al, 2006 (APSAC)
When clinicians become seduced by this allure, they can stop
seeing the individual child & family
17What are the likely common disorders in adopted children?Poor
mental health data for UK adopted childrenA need for well designed
research
But UK adopted children largely from Looked After Children (LAC)
& have experienced maltreatment / neglectExcellent
epidemiological data for UK LAC From the Office of National
Statistics (ONS) study
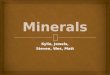
18Mental Health in UK LAC, Ford et al 2007Birth familyHigh
RiskONS LACAny disorder8.5%14.6%46%Anxiety
disorders3.6%5.5%11%PTSD0.1%0.5%2%Depression0.9%1.2%3%Behavioural
disorders4.3%9.7%39%ADHD1.1%1.3%9%Autism
[ASD]0.3%0.1%2.6%Neurodevelopmental3.3%4.5%12.8%Learning
disability1.5%1.5%10.7%Comparing ONS LAC data with Tier 4 Adoption
& Fostering Service (AFS)(Woolgar et al, 2013)ONS LACAFSCAMHS
ReferralsAny disorder46%66%31%Anxiety
disorders11%9%5%PTSD2%3%1%Depression3%4%1%Behavioural
disorders39%55%4%ADHD9%38%12%ASD2.6%4%4%Neurodevelopmental12.8%12%0%Learning
disability10.7%10%3%General CAMHS services for adoptionCAMHS
services under-identifyingBehavioural problemsNeurodevelopmental
problemsADHDGlobal learning disabilityNeurodevelopmental issues
(e.g., motor problems etc)Specific learning disability (e.g.,
dyslexia)
Anxiety, PTSD & depression (to lesser extent)
Summary of what we knowClear risk for common mental health
disorders for UK children adopted from care
Complex and pervasive bio-psycho-social presentations can emerge
from maltreatment/neglectSo much more than just a damaged brain
Unique and subtle presentations with individual responses to
extent [dose] of maltreatmentBiology responds to adversity with
diversity in presentationDandelions & orchids each have a role
to play
Cannot lump together all adopted childrens needsNeed a
personalised approach to service delivery22Complexity in practice:
9 year-old adopted boyhelp with school; they just dont get
himDomestic violence in utero & polysubstance misuse; 3 week
detox in SCBU; adopted by his first carerHistory of multiple NHS
CAMHS contactsSeries of Tier 3 assessments, discrepant diagnoses
each discounting the previous onesADHD, no autismAutism, no
ADHDADHD again, but no autismBehavioural problems & poor
parenting, but no ADHD or autismNot meeting high CAMHS thresholds
so no treatmentFamily bemused, angry & let down2323Tier 4
National & Specialist Adoption Specific AssessmentFew problems
at homeMother very clear & uses visual aids to help
understanding
School hate him [evidence of not liking him in their
report]Disagree that he has any mental health issues [he has
several]Blame mothers parenting [No, just her committed
advocacy]Low academic expectations [but normal IQ, so school
failing]
OutcomeComplex but subtle neurodevelopmental profileSeveral
common disorders, low severity but cumulative high needsRequires
substantial school support Liaison with school to explain profile
not a horrid childSupport School Action/Statementing processesWhat
is needed for assessment?Need for expert assessment and
differential diagnosis & adoption specific formulations / care
plans, based on current evidenceTreatment should be based on a
careful assessment conducted by a qualified mental health
professional with expertise in differential diagnosis and child
development (Chaffin et al, 2006, p87)
National commissioning for adoption assessments?NHS Tier 4
Specialist Adoption Service modelMulti disciplinary
assessmentPersonalised bio-psycho-social formulationPrioritise
common disorders, even if low thresholdDevelop personalised care
plan (& revisit)Liaise with network, especially schoolPrimary
therapeutic input is the Parents, but various evidence based
treatments can support them in this task by addressing
complexity.
Development & recovery4 yr old boy in pre-adoptive
placement
4yrs: Reactive Attachment Disorder (RAD)Oppositional Defiant
Disorder (ODD)9yrsSpecific, but not secure, attachments to parents
evident, so no longer DAD or RADAutism Spectrum DisorderADHDNormal
IQ, but severe deficits in adaptive functioning &
literacyBreakdown Attachment Disorderwhats love got to do with
it..? A lot.Attachment disorder - RADASDADHDODDSubtle
neuro-psychologicalproblemsRADSocial
&AdaptivefunctioningRecovered[stability&
love]SpecialistassessmentParentingInterventionSchoolliaison
MedicationSocial skillsIf left undiagnosed & untreated? 17
year-old adopted girlPresented with Severe mood
swingsSelf-harmTheft, aggression; running away; threatening
behaviourAssociating with risky & inappropriate adultsEarly
& persistent school [& work] failure
Existing diagnosisAttachment disorder only (not a recognised
diagnosis)Previous treatmentNone, as no local CAMHS provision for
attachment disorder family left without any
supportAssessmentHistoryConduct problemsODD then CDADHDDepressed
moodSelf-harmAssessmentLow mood Low self-esteemLearning
disabilityReading disorderCharming & easily engaged
No attachment disorder now or ever any evidence for itMissed
opportunities for evidence-based interventionsODD/CD from 4
yearsADHDDepressed moodEducational support for reading / low IQ
Complex presentation & developmental course, with
accumulating risksAll obscured by general, impersonal &
incorrect diagnosis of attachment disorder which also allowed
services to avoid helping the family
Failure to see the individual child Brother done well & at
university differentially susceptible siblings same good adoptive
parentingOutcomeCelebrated 18th birthday by running away
Found 3 days later by police investigating another matter,
bleeding & agitated
Taken to A&E, admitted and assessed by adult services - in
the here and now
Went out as a child with attachment disorder, sent home as an
adult with a personality disorder diagnosisSummaryBig concepts such
as Trauma and Attachment are important for adoption formulationsBut
the science tells us thatAdversity breeds diversity not similarity,
so dont let big concepts obscure individual needsCommon, treatable
disorders are very common & treatable in looked after and
adopted childrenAdopted families require comprehensive assessments
and personalised treatment plans including evidence-based
interventions
ResourcesI have included some further rather technical
references nextThe excellent Chaffin et al article brings together
world leading attachment and maltreatment researchers and
clinicians to make recommendations about how to assess and treat
maltreated/ neglected children with attachment issues. Chaffin et
al, 2006 Child MaltreatmentReport of the APSAC Task Force on
Attachment Therapy, Reactive Attachment Disorder, and Attachment
Problems, Child Maltreatment, 2006AssessmentUse expert clinicians
Prioritise common disorders Assess neurodevelopmental factorsFamily
context not just the childConsider cultural issues; situations
& contexts; multiple time pointsAvoid extreme prognosis (e.g.,
psychopathy); pejorative terms (e.g., manipulative); distress as
mechanism of change; broad checklists
TreatmentUse evidence based approaches for 1st line common
disordersBrief, goal-directed interventions for increasing parental
sensitivity for children with attachment problemsUse parent
training techniques, e.g., Time Out etc. for behaviourInclude the
family & not just the child.Avoid attachment parenting
techniques using: holding, coercion; regression etc., as unproven
& harmfulReadingsChaffin, M., Hanson, R., Saunders, B. E.,
Nichols, T., Barnett, D., Zeanah, C., et al. (2006). Report of the
APSAC Task Force on Attachment Therapy, Reactive Attachment
Disorder, and Attachment Problems. Child Maltreatment, 11,
76-89.Ford, T., Vostanis, P., Meltzer, H., & Goodman, R.
(2007). Psychiatric disorder among British children looked after by
local authorities: Comparison with children living in private
households. British Journal of Psychiatry, 190, 319-325.
McCrory, E., De Brito, S., & Viding, E. (2010). Research
Review: The neurobiology and genetics of maltreatment and
adversity. Journal of Child Psychology & Psychiatry, 15,
1079-1095.Belsky, J. & Pluess, M. (2009). Beyond diathesis
stress: differential susceptibility to environmental influences.
Psychological Bulletin, 135, 885-908.Bakermans-Kranenburg, M. J.
& van IJzendoorn, M. H. (2007). Research Review: genetic
vulnerability or differential susceptibility in child development:
the case of attachment. Journal of Child Psychology &
Psychiatry, 48, 1160-1173.Woolgar, M. & Scott, S. (2013). The
negative consequences of over-diagnosing attachment disorders in
adopted children: the importance of comprehensive formulations.
Clinical Child Psychology & Psychiatry
doi:10.1177/1359104513478545 (April 2013 Online First).