-
8/14/2019 Mass Event Zone Planning
1/9
Mass Event Coverage:Avoiding the EMS Quagmire
By:
William C. Butler II, NREMT-B, President;and
David E. Gesner, NREMT-P, MA., Director;
Marshall University Emergency Medical Services400 Hal Greer
Blvd.
Huntington, WV 25701.(304)696-2391/ 6652 / 6683
.. ./
/ .(
Emergency Medical Services organizations have for years
attempted to find new methods and protocols intheir effort to
minimize response time, scene time and total call time for
emergency medical responses.More often than not, their attempts are
fruitful and result in decreased patient morbidity and
mortality.Many problem areas remain, despite tireless effort on the
part of the providers and medical directors toresolve them. One
area of concern to many EMS organizations is the best method to
facilitate emergencymedical coverage to what we have called a Mass
Event. Simply, a mass event is any gathering of peoplewhere either
the numbers of people or the size of the response area taxes the
public safety resources of theresponsible agency or agencies. The
following discussion describes the problems and pitfalls common
tomass event coverage from a prehospltal point ofview, two fairly
common methods by which an EMS call ishandled in the mass event
situation, and the relatively new method by which Marshall
University EMSprovides emergency coverage in the mass event
situations common to this organization.
-
8/14/2019 Mass Event Zone Planning
2/9
We open at a college championship football game in a
medium-sizedAppalachiancity. The scene is one ofbarely controlled
chaos, i fchaos is the correct word to describethe euphoria
expressed by thirty-fIVe thousandfootballfans at their star player
scoringthe tie breaking touchdown ofa hardfought game. The frenzy
builds to a crescendo ofjoyful screams and applause. The media pans
the crowdfrom their sideline positions,capturing this story as it
happens, hoping for that certain shot to make their day aproductive
one. Police and security officers strain to hear their radios while
they watchthe crowdfor trouble, or for that little lost child that
was reported twenty minutes ago.Event officials are simultaneously
overjoyed at the turnout and worried at the potentialfor problems
with this many people presentfor their game. And in the middle ofit
all--inthe midst of this mania--a sixty-two year old woman suddenly
realizes she's in seriollstrouble.
She's felt this way before, seven years ago when she had her
first heart attack.She spent two weeks in Intensive Care and months
in rehabilitation. Her doctor told hershe wouldn't survive another
one i fshe didn 'tfollow his instructions and get herselffitagain.
She had another, much milder problem two years ago after deciding
she wasbetter and could live "f ree." She was home injust afew
days, but swore she'd not let ithappen again. This is different,
however. She's dizzy and tired, having trouble breathingand her
chest feels as though there's a car parked on it. She leans on her
husband ofthirty-six years and looks up at him, watches his face
turn from greatjoy to intense fear,and sinks into
unconsciousness.
What do we, as Emergency Medical Technicians, do about this? How
do we bestprovide for the medical coverage necessary in such
situations? Why must our response inthis case be different from our
normal operating mode? The simplest answer that can begiven is
simply time. The best medicine we can ever give to any patient we
encounter istime; more precisely, the less time, the better. I f we
can keep the elapsed time for theresponse to a minimum, we go a
long way toward minimizing the patient's suffering andhopefully can
prevent an untimely death. Few can argue with this statement.
To understand the importance of preplanning a response path
during an eventsimilar to the one above, we must begin to
understand the true uniquenessof this class ofresponse areas. These
situations are known by several names: concerts, rallies, ball
gamesand so on. In EMS circles, they are not often thought of as a
definable situation, merely agathering of many potential patients.
Many municipalities seem to regard these situationsmerely as a
relocation of their patients to a more centralized area and may
move anotherambulance or two to the vicinity. little thought seems
to have been given to the idea thatthe event itself is an important
situation that must be looked at from a slightly
differentviewpoint. We have looked at it in depth and have even
given it a name: the Mass Event.
A mass event is defined within this framework as any event that
places a strain onpublic safety resources because of: a) the number
of people in attendance, b) the high ratioof attendees in a given
area to public safety p e r s o n n e ~ and c) the size of the
facility or areain which they are gathered produces a high density
population. They may range in sizefrom a few hundred people
participating in a Walk-a-Thon to the 1vfillion Man March
inWashington, DC a few years ago to Woodstock n. These events
present unique problems
-
8/14/2019 Mass Event Zone Planning
3/9
for the Emergency Medical Services provider not encountered
during a "normal" call. Amajor problem is that the potential for
injury and illness during the event increases simplydue to
overcrowding, the emotional state of the attendees, the propensity
for drink andrevelry, and the like. During a mass event, the EMS
providers are likely to have to plytheir craft with an audience
ofgawkers, of f duty medical professionals andparaprofessionals,
and the media. All the while, the clock is ticking minutes of f
the"golden sixty" and the ''platinum ten."
Every response plan to date seems to be very concerned with
time. We see it onour run sheets, in the Emergency Department, the
dispatch log sheets, and we have arunning cadence in our heads as
we package and treat each patient. When we try toperform our duties
in an extremely crowded, noisy and dangerous atmosphere, we
simplycannot treat the patient as we normally would in their home.
We must take into accountthe dangers associated with working in the
masses. We must be vigilant for our own safetyand the patient's. We
must be cautious when using advanced life support procedures
(I'vepersonally witnessed on two occasions the defibrillation of an
entire row of spectators onmetal bleachers!). We must also keep our
eyes on the clock. It simply takes more time tomove a patient in a
crowd. The more we dawdle, the faster they die!Several major
problems must be addressed and overcome for a mass eventresponse
plan to be effective. First and foremost is the lengthy response
times common tothese situations. A method must be found by which
providers can get to the patients morequickly and safely. Provider
fatigue is a factor, especially in the large sports stadiumscornmon
to universities and large cities. I f the EMTs must make their way
up flight afterflight of steep stairs carrying all their equipment
while fighting the crowd, package thepatient and extricate them
back down those stairs to the ambulance, the likelihood
ofbeinginjured or making mistakes on the call increases
dramatically. Access to EMS is, ironically,more difficult in a sea
of people due to the low relative visibility of public safety
personneland lack of easily accessed telephones (excluding cell
phones, of course). Command andcontrol of the response teams can
provide either a solid foundation for the response or theweak link
in the chain of events leading to the patient's death.
Frantically, her husband tries to awaken her with the ful l
knowledge that ifhecan't get her to open her eyes, she'/I die.
Panic-stricken, he gains the attention of theperson standing beside
him (who didn' t notice the emergency because ofthe standingovation
and the noise) and sends him for help. This messenger tries to move
down thepacked row ofspectators to the aisle, where he hopes he'l
lfind a security guard. Hebreaks into the open and looks toward the
tunnel entrance to his section for the guards hesaw earlier that
day. He sees one cheering with the crowdand runs up severalflights
ofstairs to him. The woman's husband is oblivious to everyone
around him as he begins toweep.
The example above is typical of the first stages of an emergency
in any mass eventscenario. Bystanders recognize the situation
exists and try to take action. The mostimportant step, however, has
taken place long before the victim succumbs to her illness:the
pre-planning of the event's medical coverage. The pre-plan covers
all aspects of thechain of events from initial recognition to
delivery of the patient to the EmergencyDepartment, as well as team
recovery back to the event site. Recognizing the importance
-
8/14/2019 Mass Event Zone Planning
4/9
of each step in the call cycle is paramount to the effectiveness
of the pre-plan and of theactual response.
The pre-plan starts where the call starts...initial
recognitionof the emergency andrapid access to the medical teams
there to provide coverage. We, as providers, cannotcontrol the
occurrences, but we can assist the victims by making access to EM S
as simpleand visible as possible. Every event official, from the
ushers to the director,must be madeaware of the importance of rapid
action in dispatching medical teams to the scene. Theyshould be
made aware that official visibility will greatly decrease the time
from onset of theillness or injury to the arrival of the medical
team. A rapid response will assist in "'decreasing the
morbidity/mortalityof patients, and this in tum will keep liability
(andmaybe even insurance costs) to a minimum. This isone of the
most important concepts ofmass event medicalcoverage and should not
be taken lightly.
As an aside, the proliferation of cellular phones today poses a
unique problemforthis situation. Calling 911 may actually increase
the response time due to the addition ofseveral more steps in the
response chain. I f the 911 dispatch center is not made aware ofthe
method by which the event is covered and who is responsible, an
ambulance fromoutside the mass event plan may be directed to the
scene. In the time that it would take foran ambulance to respond,
the patient may have been on his or her way to the hospital i f
thecaller had simply spoken to security. Emergency dispatch
centersneed to be made awareof the ev ent's intrinsic medical
coverage so that they may refer the call to the event'scommand
center for a more efficient response.
Once access to EM S has been gained, the focus of the response
is on speed andefficiency. Prior to the event, EM S officials and
rescue personnel need to go to the siteand develop their specific
response plan. Each plan is unjque to the event and mustbedeveloped
in the light of the unique variables associated with the event.
These variablesinclude, but are not limited to, the physical size
and layout of the site, the number ofparticipants expected, the
number of providers available, the EM S resources that can
beutilized, availability of mutual aid from outside EM S sources,
etc. Pathways of movementfor th e initial response teams, ambulance
supportand supporting agencies must berecognized and defined. An
efficient method of intrinsic mutual aid must be developedshould
the need arise. And lastly, an event protocol should be developed
that takes intoaccount the unique structure of the response plan.
Mapping the event site and providing awritten directive for the
medical teams is also most helpful.
These authors will not attempt to provide a "unified theory of
event coverage" thatis a catch-all for every situation. We will
merely discuss the methods by which we covermass events at Marshall
University and the surrounding area. From this discussion, wehope
to stress the importance of pre-planning the coverage and
demonstrate the method bywhich we've arrived at our current
plan.
There seem to be two primary methods by which mass event
coverage responsesare done. These are defined by these authors as
the Unit Team method and the ZoneTeam method. Unit Team responses
are those in which the responding medical team hascontrol of the
patient from initial dispatch to the ambulance's arrival at the ED.
They carryall necessary equipment to effect the response and
maintain patient contact throughout thecall cycle. This is how EMS
responses in the normal prehospital environment usuallywork. Tw o
significant types of Unit Team response strategies are the Central
Unit Teamand the Dispersed Unit Team strategies. The Central Unit
Team strategy is most like
-
8/14/2019 Mass Event Zone Planning
5/9
''nonnal'' EMS in that all EMS resources and personnel are
dispatched out of a singlestaging area. The Dispersed Unit Team
strategy is one in which the individual teams areplaced in
strategic locations and, with patient in tow, meet the ambulance at
a designatedtransport point. Usually, with this last strategy, a
"flying" equipment pool responds to thepatient location to provide
bulky items to the team, so as to avoid an extremely largeequipment
requirement (that way each team won't have to tote a cot around
with them).
The major advantages of the previous strategies are that the
information from thepatient/bystanders is less likely to be
confused during transfer than i f there were more thanone team
involved. The transporting crew goes to the scene itself and may be
able to gainmore information as to the nature of the call than
might be transmitted between two teams.Patient rapport is likely to
be more solid than i f several teams are involved. Several
majordisadvantages exist,' however, that in our opinion are less
desirable than the advantagesgained. First, and possibly most
important, is team fatigue. In many cases, the accessextrication
distance and situation are long and difficult. Fatigue leads to
judgment errorsand increases the likelihood of provider injury. Of
these plans, the Central Unit Team planhas the longest response
time and the highest probability of provider fatigue. In an
event(such as a small walk-a-thon) where these methods are
effective, it is most easily adapted toby providers and yields more
solid patient rapport. The Dispersed Unit Team plan hasmuch shorter
response times, but may yield high levels of provider fatigue as
the teamsextricate the patient all the way to the waiting
ambulance. Mutual aid during the call is asslow or slower and just
as tiring as the initial response.
We have tried variations of these methods and found them
inefficient for thereasons stated above (and others) and have
attempted to develop a more efficient plan forour needs. Marshall
University EMS provides coverage for several different mass
eventscenarios during the year and we needed to develop a flexible
plan that we could adapt toeach of these. Primarily, our concern
has focused on the NCAA sporting events held atany of our major
facilities during the school year. We have a medium sized
basketballarena and a 33,150 seat football stadium within our
response area on the MU campus.Several times each year, the campus
swells with spectators and participants, as well as ournonnal
campus population, and we must be able to quickly and efficiently
provide medicalresponse to everyone within our district.
MUEMS is a volunteer service, and as such, we may have more or
less thenumbers of personnel required to provide effective coverage
at an event using thepreviously-mentioned methods of coverage. We
also maintain only one ambulance oncampus and have needed to
develop a plan for mutual aid while that single vehicle isengaged
on a call. To efficiently utilize our limited personnel and
resources, we havedeveloped what we call the Zone Team method of
coverage.The Zone Team plan is a tiered response plan that was
developed by a fusion ofwartime military medical response methods,
civilian EMS methods, and mass casualtyincident response plans.
Simply put the response area is divided into Central CommandZones
of coverage and there are teams ~ i t h i n those zones
pre-positioned to affect animmediate response. A Central Command
Zone, or CCZ, is analogous to an EMS district.It has its own
command and control and its own director. It functions as a
separate entityand possesses its own resources. Each CCZ should
have its own command! dispatchcenter, but several may be able to
function under a single command/dispatch center i f it isorganized
well.
-
8/14/2019 Mass Event Zone Planning
6/9
Each CCZ is divided into major zones of response. Each zone has
a single rovingAdvanced Life Support (ALS) team with all necessary
equipment for the extrication of apatient from the scene (i.e. cot,
stair chair, spine board, etc.) as well as for ALS-Ieveltreatment.
These zones are further divided into primary response areas where
Basic LifeSupport (BLS) teams are stationed. In many cases, the BLS
teams are the initial point ofcontact for the access into the EMS
system as they have such a high visibility within theirareas,
yielding extremely short response times. The ALS teams are
responsible for the
'rBLS teams in their zone and provide a basic level of command
and control as well asmutual aid should the BLS team require it.
The director (or the designated assistant)provides command and
control for the ALS teams within their CCZ. Each call is
treatedlike a rescue in that it follows the LASET (Locate, Access,
Stabilize, Extricate, Treat!Transport) method.
Each CCZ is also divided into major transport zones and defined
transport pointsare established where the ambulance meets the
patient. Each transport team is staffed andequipped the same as the
ALS rove teams because they provide mutual aid to the roveteams
while they are engaged with a call (in other words, dispatch will
designate a transportteam to act as an ALS rove team until the
original team clears from the call). Eachtransport zone has its own
assigned ambulance that responds to transport patients to
thehospital.
The command and control element consists of the director, a
designated assistantand the command center. The director is
responsible for all areas and actions within theCCZ. He usually
refrains from direct patient contact, as his primary role is
direction of theresponse (a traffic cop, i f you will). The
designated assistant provides on scene commandsupport, direction
and medical assistance i f necessary. He is the on scene eyes and
ears forthe director and ensures the response chain moves as
planned. He also may provide therapport link for the patient as he
or she is transferred from one team to another. Thecommand/
dispatch center is the primary command and control device used for
theresponse. It receives calls and dispatches teams to the scene,
provides a communicationslink between supporting agencies and the
director, keeps pertinent call data (times,mileages, etc.) and
receives communications from and directs communications to
theindividual teams and personnel involved with the response. The
command/dispatch centeralso ensures mutual aid is available when
and where it is needed.
It is probably easier to understand the method by which the Zone
Team plan worksi f we follow the call in progress within this
discussion. It seems complicated at frrst, butwhen one realizes
that it is merely a series of coordinated steps already outlined in
the preplan, it really is simple. Let 's follow the response path
as it happens.
The radio in the command center crackles and the dispatchers
glance toward it."We need a medical team to section 124, row six.!
" the guard yells into his mike, trying toovercome the intense
noise around him. The security/police dispatcher tries to elicit
anyfurther information, but there is none. He gives this to the
medical dispatcher who, inturn, decides which primary team is
responsible/or this area. He keys his mike and says,"Team 3
respond. section 124, row six. unknown medical problem." Team
3acknowledges and makes their way toward the scene. The dispatcher
again keys his mikeand sends Rove 2 to the nearest stagmg area to
await the primary team's report.
-
8/14/2019 Mass Event Zone Planning
7/9
Hearing these transmissions, the designated assistant begins
moving in the direction ofthe call (elapsed time: 45 seconds).
The passage above represents the access and dispatch stages of
the response chain.The primary (BLS) team moves to the scene itself
while the Rove (ALS) team moves tothe nearest designated staging
area to await the transport decision. There is no need for therove
team to go to the scene itself until their services are deemed
necessary...why haul twohundred pounds of equipment up twenty
flights of stairs for a hangnail? This is one of theways in which
this plan maximizes ALS resources.
Team 3 arrives at the patient's location, guided by the security
guard stationed atthe tunnel entrance (elapsed time: 1 minute, 50
seconds). They see that CPR is beingperformed by two men, one
ofwhom informs them that he is a registered nurse and thiswoman is
pulseless and had been downjust afew seconds before they
intervened. Rove 2arrives at the staging area and waits. The team
leader directs his assistants to take overCPR, advises dispatch
that this is a working code and requests the rove team move upwith
the backboardfor rapid extrication. Two rove team members take the
board andmove rapidly to the scene while the third member prepares
the ALS equipment to receivethe patient. Dispatch determines which
transport team is responsible for that zone andsends them to the
nearest gate. The security/police dispatcher sends four security
guardsto the staging area to provide safe transit for the patient.
The patient is placed on thebackboard and the medical teams begin
their ascent to the tunnel entrance (elapsed time:3 minutes, 15
seconds).
At this point, the call has entered the extrication phase. The
patient is moved onthe backboard (with CPR in progress) to the
staging area. There, advanced life supportprocedures will be done
in a safe and organized atmosphere. The flow of this call will
beoverseen by the designated assistant to ensure the response path
is uninterrupted and thatevery chance for success is given.
The adjacent primary teams (Teams 2 and 4) move a little bit
tOl-l'ards each otherto ease access to what has become their
expanded areas ~ responsibility, according tothe briefing they all
had that morning. The command center alerts Transport Team 1
toassume responsibility for Rove 's zone until they clear from the
call (elapsed time: 3minutes, 20 seconds).
We see here the intrinsic back up provided by the Zone Team
plan. There isalways some way to fill the gaps in coverage caused
by a team or teams engaged with acall. The adjacent primary teams
split the responding team's area and cover it while theyare busy.
The transport team designated by dispatch covers the responding
rove team'szone until they clear from the call. and then will
assume responsibility for the busytransport team's transport zone
until they return from the hospital. Admittedly, it
soundscomplicated, but when one thinks about it as teams just
moving up a notch in the chain fora bit, it becomes less cloudy.
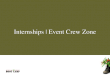
Schematically, it might be represented as follows (for a verysimple
CCZ):
-
8/14/2019 Mass Event Zone Planning
8/9
Director
DesignatedAssistant
Command/DispatchCenter
Primary Teams Primary Teams1,2 and 3 4, 5 and 6
By tracing the solid lines of the above chart, one can see the
hierarchy along whichthe chain of command flows. The dashed lines
represent mutual aid options (i.e. Transport1 can back up Transport
2 or either of the rove teams). It should be stressed, however,that
mutual aid can only flow "down" or "across." A BLS team cannot
provide mutual aidto an ALS team, but an ALS team can provide aid
to a BLS team. BLS teams mayprovide aid to other BLS teams (such as
covering their area until the busy team clears).
The designated assistant directs the security officers to clear
a path for the patientand the teams to the staging area. The
patient is placed on the cot and the first threeshocks are
delivered (elapsed time: 4 minutes, 55 seconds). As ALS
interventions arebegun. the rove team leader releases all but one
ofTeam 3 's members, and they return totheir zone, releasing teams
2 and 4. The high-pitched beep of the ambulance's back upalarm
signals the arrival of the transport team (elapsed time: 5 minutes
25 seconds) andstabilization measures are completed. The rove team
begins to move the patient to thetransport poin t and transfers
care to the ambulance's crew. The designated assistanttakes the
woman 's husband to the front seat and assures him that all that
can be done isbeing done. Final stabilization takes place in the
back of the truck and the doors close.The siren chirps to clear
gawkers from the sidewalk and the ambulance begins its waytowards
the hospital (elapsed time: 7 minutes, 50 seconds).
The elapsed time for this call from receipt of the call to
beginning transport was lessthan eight minutes--not at all
unrealistic for this situation. I f all the teams know their
jobs
-
8/14/2019 Mass Event Zone Planning
9/9
and responsibilities, the response path will not be like walking
down an unfamiliar trail, butlike following road signs to the
terminus of the call. Actual call data were analyzed formedical
responses both prior to and after inception of the Zone Team plan.
This data wasbroken down into response time, time on scene and
total time of call (dispatch to deliveryto the ambulance). The data
for mass event call times prior to the Zone Team plan are
asfollows:
Average Response Time 3.25 minutesAverage Time on Scene 11.08
minutesAverage Total Call Time 14.08 minutes.
After development of the Zone Team plan, mass event call times
were:Average Response Time 0.92 minutesAverage Time on Scene 6.85
minutesAverage Total Call Time 7.77 minutes.
To test the validity of the changes observed, a statistical
method called the MatchPaired T Test was calculated along with the
confidence factor (P). Our results were acalculated T of3.73,
p=0.07. These results show two important points: 1) the
changesobserved were large enough to mean something and, 2) that
there was a 93% chance thatthese changes were due to the Zone Team
plan, not jus t dumb luck.
How will this plan affect the mass event EMS coverage arena?
That has yet to beseen. The only data available for the Zone Team
plan is for Marshall University sportingevents and other mass
events for the years 1996 and 1997. It would be very interesting
tosee i f this plan causes significant changes in response times
for other organizations. It isoW' belief that this plan can be
adapted and used by other services for their mass eventresponses
with favorable results. We have had great success adapting this
plan to ourvaried mass event situations. We use it for the
football, basketball, and other large-drawsporting events, for the
annual West Virginia State Special Olympics Summer Games heldon our
campus, as well as a couple of large crowds drawn by notable
political figureswho've visited recently. The Zone Team plan hasn't
let us down yet.
With appropriate command and controL thorough briefings of
personnel and goodpre planning, this plan serves extremely well.
Undoubtedly, it can be adapted and used byother organizations with
equal success. Simply, it is a web of intrinsic mutual aid
planspaired with a hierarchy along which the call flows. The
presence of a defmable method toprovide coverage cuts down on
confusion among providers and increases confidence withevent
sponsors that their event will not be marred by tragedy. We have
seen in the pastthat medical teams get bogged down all too easily
when the situation involves highparticipant density and multitudes
of people. This plan is merely a single effort designed tominimize
this risk.