Embed Size (px)
Citation preview
Maryland’s New All-Payer Model—A Journey Together
3
Approved New All-Payer Model Maryland is implementing a new All-Payer
Model for hospital payment New Model approved by CMS/CMMI effective
January 1, 2014 Health Services Cost Review Commission
leading the implementation
The All-Payer Model shifts focus From per inpatient admission To all payer, per capita, total hospital
payment
4
Long Standing Medicare Waiver
Medicare waiver granted July 1, 1977 It’s what makes the system “all-payer” Old waiver test was based on rate of increase in
Medicare payment per admission New waiver based on total hospital revenue per
capita
Considerable value to State and hospitals All payers pay share of uncompensated care and
medical education costs Limits cost shifting
5
Shifts Focus to Patients Unprecedented effort to improve health and
outcomes, and control costs for patients Gain control of the revenue budget and focus on
providing the right services and reducing utilization that can be avoided with better care
Change delivery system together with all providers
Maryland’s All Payer Model
•Improve Patient Care
•Improve Population Health
•Lower Total Cost of Care
6
Approved Model Timeline Phase 1 - 5 Year Hospital Model
Maryland all-payer hospital model Developing in alignment with the broader health care
system
Phase 2 – Total Cost of Care Model Phase 1 efforts will come together in a Phase 2 proposal To be submitted in Phase 1, End of Year 3 Implementation beyond Year 5 will further advance the
three-part aim
7
Approved Model at a Glance
All-Payer total hospital per capita revenue growth ceiling of 3.58% annual growth
Medicare payment savings of $330 million over 5 years.
Patient and population centered-measures and targets to promote care improvement Medicare readmission reductions to national average 30% reduction in preventable conditions under
Maryland’s Hospital Acquired Condition program (MHAC) over a 5 year period
Other quality improvement targets

9
HSCRC Model Implementation Timeline
Phase 1(to
6/30/14)
Phase 2 (7/1/14 – 3/30/15)
Phase 3 (4/1/15 – 3/30/16)
Phase 4
(2016-Beyond
)Bring hospitals onto global revenue budgets
Identify, monitor, and address clinical and cost improvement opportunities
Implement additional population-based and patient centered approaches
Develop proposal to focus on the broader health system beyond 2018
Begin public input process: advisory council and work groups
•Enhance models, monitoring and infrastructure•Formalize partnerships for engagement and improvement
•Evolve alignment models and payment approaches•Increase focus on total cost of care
Secure resources, and bring together all stakeholders to develop approach
Com
plet
e
10
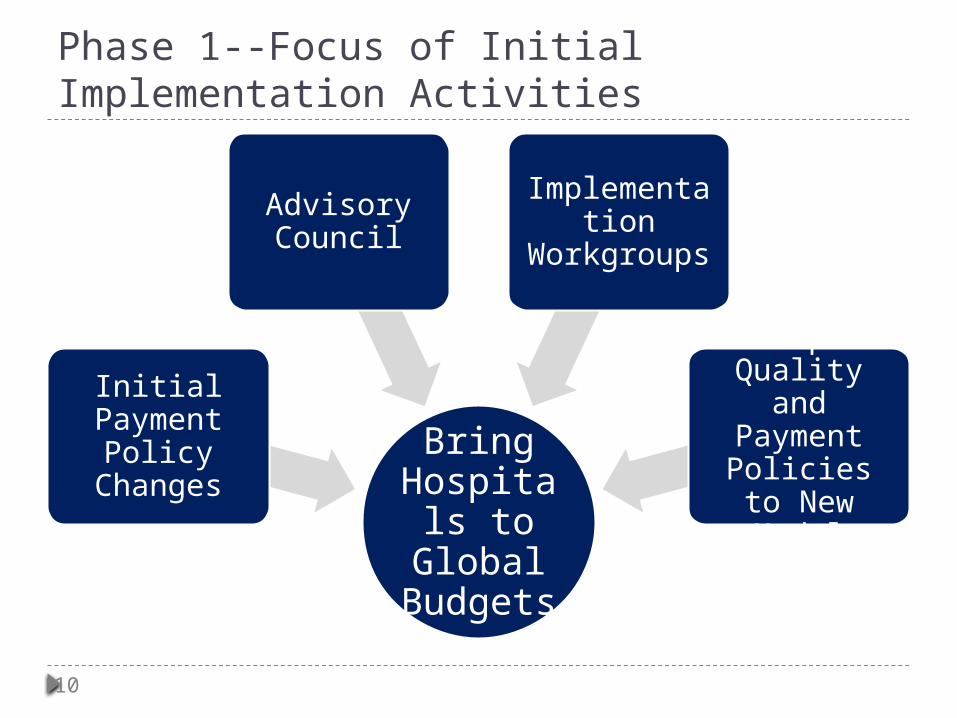
Phase 1--Focus of Initial Implementation Activities
Bring Hospitals to
Global Budgets
Initial Payment
Policy Changes
Advisory Council
Implementation
Workgroups
Adapt Quality and Payment
Policies to New Model
11
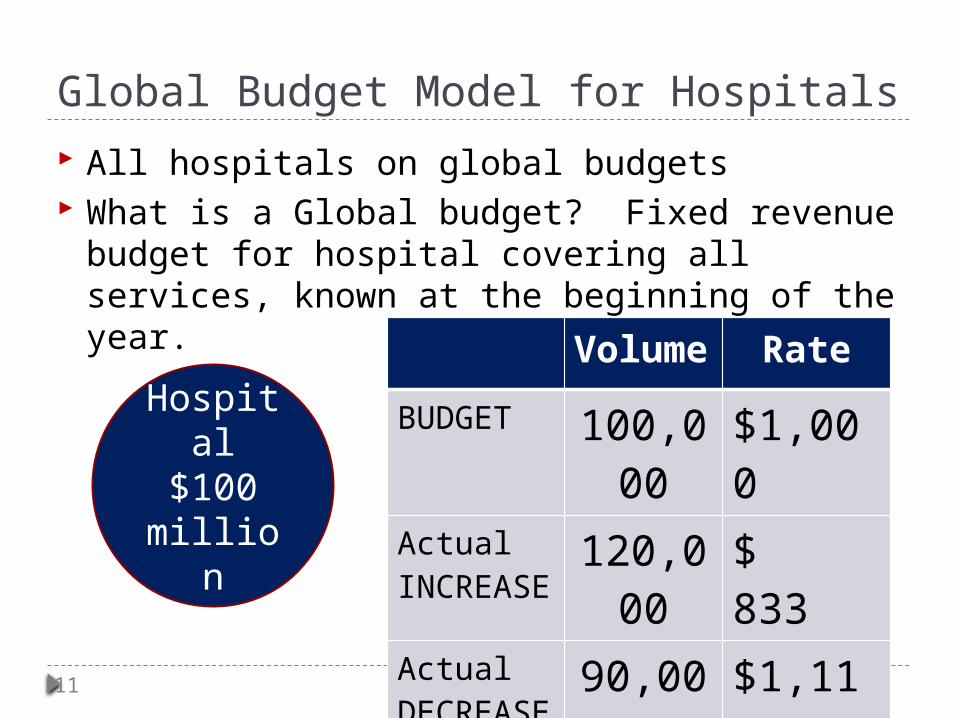
Global Budget Model for Hospitals All hospitals on global budgets What is a Global budget? Fixed revenue
budget for hospital covering all services, known at the beginning of the year.
Hospital$100
million
Volume
Rate
BUDGET 100,000
$1,000
Actual INCREASE
120,000
$ 833
Actual DECREASE
90,000
$1,111

12
Initial Public Engagement Process Engaged broad set of stakeholders in HSCRC
policy making and implementation of new model Advisory Council, 4 workgroups and 6 subgroups 100+ appointees Consumers, Employers, Providers, Payers, Nurses Technical White Papers – 18 Shared Publically
Established processes for transparency and openness Public meetings Access to information Opportunity for comment
14
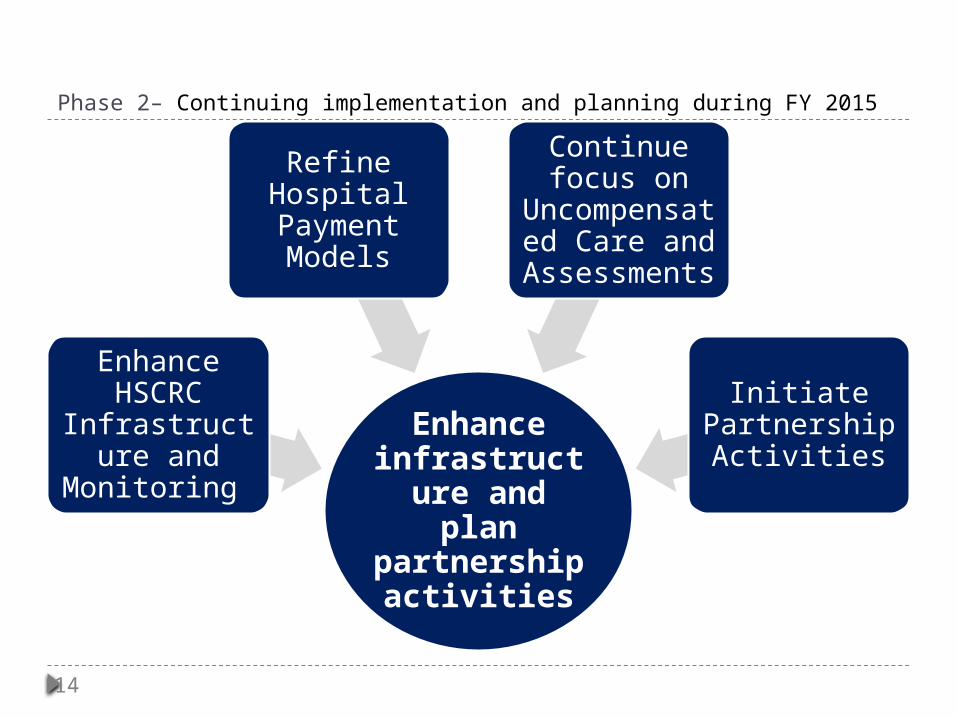
Phase 2– Continuing implementation and planning during FY 2015
Enhance infrastructure
and plan partnership
activities
Enhance HSCRC
Infrastructure and
Monitoring
Refine Hospital Payment Models
Continue focus on
Uncompensated Care and Assessments
Initiate Partnership Activities
15
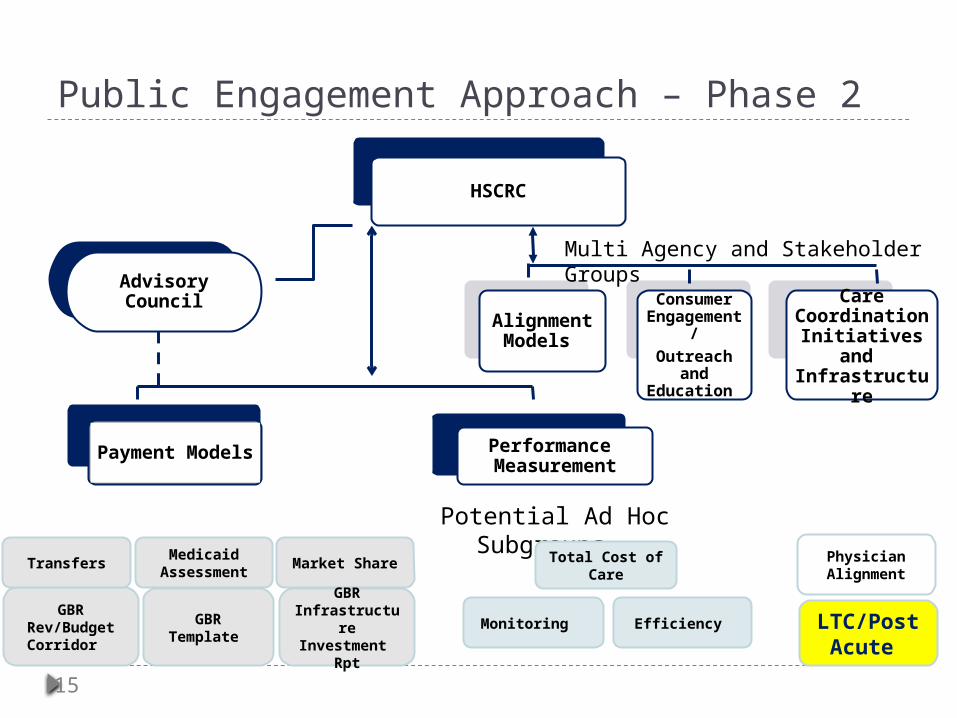
Public Engagement Approach – Phase 2
HSCRC
Advisory Council
Alignment Models
Consumer Engageme
nt/Outreach
and Education
Care Coordination
Initiatives and
Infrastructure
Payment Models
Performance Measurement
Potential Ad Hoc Subgroups
Medicaid Assessment
Market Share Total Cost of Care
Monitoring
GBR Infrastructur
e Investment
Rpt
GBR Rev/Budget Corridor
GBR Template
Multi Agency and Stakeholder Groups
Efficiency
Physician Alignment
LTC/Post Acute
Transfers
17
Population Health for Seniors Generations now alive are among the first
in history to be raised with the expectation of old age, forerunners of a longevity revolution that will be felt for centuries to come. Some twenty percentage of all humans who have ever lived past the age of 65 are now alive. So profound is this demographic revolution that every aspect of social life and society is affected.
18
Opportunities for Success M
od
el O
pp
ort
un
itie
s
• Transition to global models (COMPLETE)
• Reduce Medicare cost
• Lower use—reduce avoidable volumes with effective care management and quality improvement
• Integrate population health approaches
• Thoughtful controlled shifts to lower cost settings with net savings
• Rethink the business model/capacity and innovate
Deliv
ery
Syst
em
O
bje
ctiv
es • Improved
value
• Sustainable delivery system
• Support provider alignment & delivery reform
19
Potentially Avoidable Hospital Utilization (PAUs) In order balance the revenue model, PAUs must be
reduced PAUs are “Hospital care that is unplanned and can be
prevented through improved care, coordination, effective primary care and improved population health.”
30- Day Readmissions/Rehospitalizations (includes ER)
Preventable Admissions and ER Visits (based on AHRQ Prevention Quality Indicators and other)
Avoidable admissions for SNF and assisted living residents beyond PQIs)
Potentially preventable complicationsAdmissions and ER visits for high needs patients
can be moderated with better chronic care and care coordination
20
Partnerships to Improve Outcomes Prevent admissions—integrate care, avoid
and provide early treatment for conditionsNew conversation with hospitals on global budgets
Expedite discharges to post-acute care services;
Optimize post acute services; Avoid ER observation and selected
admissions with alternative SNF treatment; Better manage care transitions; and Establish protocols for referrals back to acute care
21
Partnerships to Improve Outcomes-INTERACTGOAL: Increase use of INTERACT approach INTERACT is a quality improvement program designed
to improve the early identification, assessment, documentation, and communication about changes in the status of residents in skilled nursing facilities and assisted living facilities. The goal of INTERACT is to improve care and reduce the frequency of potentially avoidable transfers to the acute hospital. Such transfers can result in numerous complications of hospitalization, and billions of dollars in unnecessary health care expenditures.
Recent survey conducted by Lifespan shows few providers using tools and forms

22
Partnerships to Improve Outcomes-GET CONNECTEDGOAL: Increase information exchange, especially
information about patterns of care between SNFs, assisted living, and hospitals
The Chesapeake Regional Information System for our Patients (CRISP) is a nonprofit corporation created to function as Maryland’s state-designated health information exchange CRISP has information on all hospital admissions and
discharges, lacks source of admissions through ERs State applied for grant to connect long term and post acute providers

23
Partnerships to Improve Outcomes--TRANSITIONGOAL: Improve care transitions between
hospitals and long-term/post-acute providers/back to home to reduce readmissions
Work with hospitals to improve transitions, including back to home transitions from post-acute settings
Participate: Transitions: Handle With Care The Maryland Hospital Association is working
with partner organizations to reduce avoidable readmissions within Maryland and improve care transitions for patients and families.
24
A Journey Together
Thank you for the opportunity to work together to improve care for Marylanders.