Embed Size (px)
Citation preview

British Journal of Plastic Surgery (x973), ~6, x86-I87
MARSUPIALISATION OF PRE-AURICULAR SINUSES
By D. S. Mtrva~v, F.R.C.S.Ed., F.R.C.S.Eng. Birmingham Regional Plastic Surgery Centre, Wordsley Hospital, hr. Stourbridge
I~RE-AURICULAR sinuses are notoriously difficult to manage successfully and permanently. Their clinical features and the problem of recurrence after treatment has been reviewed by Sykes (197-2). Although they may be asymptomatic throughout life, many are the site of repeated inflammatory episodes and, for such a trivial lesion, cause much inconvenience and pain.
The most usuai treatment of this sinus is a careful dissection and removal of the epithelialised track, followed by obliteration of the dead space by suture (Minhowity and Hinkowitz, I964). If the sinus extends deeply, this method may result in facial nerve damage. Also, recurrent inflammatory episodes after incomplete removal of this sinus are not uncommon.
The only reason for operating on these sinuses is to permanently prevent infection in the sinus. Infection in pre-auricular sinuses is due to stenosis of the sinus at, or just below, skin level. Havens (I939) laid open pre-auricular sinuses and then destroyed the sinus epithe!ftma with diathermy. However, if normal epithelium is left, and this is almost inevitable in a deeply penetrating pre-auricular sinus, then the scarring produced by the coagulation will produce stenosis and inevitable recurrent infection. For the last 2o years in this Unit pre-auricular sinuses have been treated by simple marsupialisation; consequent free drainage of the sinus preventing any infection occm'ing in its remnants.
METHOD
Any acute inflammatory episode in the sinus is controlled by antibiotics and/or incision and drainage. When the inflammation is completely settled the operation is performed under local or general anaesthesia. It can easily be done on an out-patient basis.
A probe is gently inserted into the sinus and a narrow ellipse is drawn on the skin over the probe. A small amount of local anaesthetic with adrenalin is infiltrated around the ellipse which is incised to the sinus epithelium. Then at the stoma of the sinus, the incision is deepened on to the probe, cutting through the superficial epithelial lining of the sinus. As the ellipse of skin, subcutaneous tissue and hernicircumference of sinus epithelium is removed, the edges of the remaining sinus epithelium are sutured to the surrounding skin. The pre-auricular sinus is thus marsupia!qsed. The resultant pouch in the skin is inconspicuous (Figs. I, 2, 3).
Complicated sinuses with many stomata are treated in the same manner, each stoma being probed and laid open. All superficial ramifications of the sinus are explored. Pre- auricular sinuses which extend deeply are marsupialised only in their easily accessible portion. With the relief of the stenosis, free drainage is ensured and no inflammatory episodes occur in the deep portion of the sinus.
This method has been used for the past 2o years and no recurrence in over 20 cases has been noted. It is quick to perform, does not involve any risk to the facial nerve or parotid gland and prevents any inflammatory episode in the sinus remnant.
I86

MARSUPIALISATION GF PRE-AURICULAR SINUSES I8 7
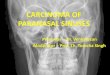
FIG. I. Pre-auricular sinus with two stomata. The seat of many inflammatory episodes. (The two dark spots anterior to the sinus in this figure and in Figures 2 and 3 are ink marks I5 ram. apart to
indicate the size of the sinus).
FI~. 2. Eight days after mar- supialisation showing skin sutured
~o the epithelial lining.
FIG. 3. One and a half years at'ter marsupialisation. The patient has had no further inflammatory
attacks.
SUMMARY
The simple technique of treating pre-auricular sinuses by marsupialisation is described and its use is recommended.
I wouM like to thank Mr O. T. MamfieMfor his guidance and advice in the preparation of this paper. My thanks are also due to Miss M. Robertson and Mr T. Coote for the photographs and Mrs Meredith for secretarial help.
R E F E R E N C E S
HAVENS, F. Z. (1939). Congenital branchiogenic preauricular sinus: a note regarding its treatment. Archives Otolaryngology, 29, 985-986.
MINHOWITY, S. arid MINKOWITZ~ F. (1964). Congenital aura/sinuses. Surgery Gynaecology and Obstetrics, Ix8, 8Ol-8O6.
SYKES, P. J. (1972). Pre-auxicular sinus: clinical features and the problems of recurrence. British Journal of Plastic Surgery, 25, I75-I79.













![fibrilacion auricular[1]](https://img.pdfslide.us/doc/110x75/577d2baa1a28ab4e1eab09b6/fibrilacion-auricular1.jpg)














