Embed Size (px)
Citation preview

Mark C. Bieniarz, MD
Andrew Harrell, MD
Peter Berger, MD

� Should PCI center activate the cath lab off EMS field interpretation of ECG? Is this happening consistently in New Mexico?
� What is acceptable rate of activation without intervention?
� How far is too far? Lytic vs. PCI and distance/time
� Fly or drive- distance, base locations and weather.
� Monitoring inappropriate activations and data feedback loops between EMS and hospital
� HIPPA rules around data sharing

� In rural state, transfer for STEMI care is necessary


ST-segment–elevation myocardial infarction reperfus ion pathways for non–percutaneous coronary intervention (PCI) centers.
Daniel Muñoz, and Christopher B. Granger Circulation . 2011;124:2477-2479
Copyright © American Heart Association, Inc. All rights reserved.

� The Way We’ve Always Done It…� Previous STEMI transfer mish mosh
� Prehospital ECG not available and chest pain patient taken to local hospital
� ECG there documented STEMI and transfer arranged calling the cardiologist or ER at PCI center
� Prior to acceptance, the ER doc assessed the patient for appropriateness of PCI, checked for CCU bed availability, then requested helicopter transfer
� On arrival, patient taken to ER where assessed by ER doc, general cardiologist on call and then interventional cardiologist consulted
� If appropriate, interventional card called in cath lab who were to arrive in 30 minutes to begin case
� Standard care at beginning of the STEMI network protocol 2004

� STEMI receives same priority as bleeding trauma� Transfer plans in place with backup� Patient stays on EMS stretcher for eval� Transport directly to cath lab� When possible exclude IV infusions of Heparin and
nitroglycerin� Transfer protocol goal should be speed NOT pain
relief. Don’t get distracted from goal.� Hospital records faxed to receiving facility. Should not
delay transfer. � No facility bias. Transfer should ALWAYS be to
closest PCI facility. Advanced life support units serving a specific hospital should always be willing to transfer to closest PCI facility

� STEMI receives same priority as trauma and 911 call
� 10 minute pickup time. Hot load. Standard across systems (Duke, Mayo)
� Helicopter capable of transferring with 10 minutes notice
� Avoid IV nitro, heparin when possible
� Transfer directly to cath lab

� Guidelines state aim for 90 minutes and transfer if possible for primary PCI in 120 minutes
Pinto, DS, et al. Circulation. 2011; 124: 2512-2521

� Multiple agencies involved
� Lack of cooperation between hospitals for the benefit of the community
� Failure to rapidly diagnose STEMI at referring hospital
� EMS not regarding STEMI with same priority as trauma

� Early identifcation of STEMI based on symptoms and prompt ECG
� Eyeballs to beltbuckles campaign
� Door to ECG standard of 5 minutes
� Early initiation of transfer
� Prehospital notification or rerouting of EMS to PCI center

High-risk ST elevation MI patients (>4 mm elevation), Sx < 12 hrs5 PCI centers (n=443) and 22 referring hospitals (n=1,129), transfer in < 3 hrs
High-risk ST elevation MI patients (>4 mm elevation), Sx < 12 hrs5 PCI centers (n=443) and 22 referring hospitals (n=1,129), transfer in < 3 hrs
Lytic therapyFront-loaded tPA 100
mg
(n=782)
Lytic therapyFront-loaded tPA 100
mg
(n=782)
Death / MI / Stroke at 30 DaysDeath / MI / Stroke at 30 Days
Primary PCIwith transfer
(n=567)
Primary PCIwith transfer
(n=567)
Primary PCIwithout transfer
(n=223)
Primary PCIwithout transfer
(n=223)
Stopped early by safety and efficacy committeeStopped early by safety and efficacy committee
N Engl J Med 2003; 349: 733-42N Engl J Med 2003; 349: 733-42

13.7%
8.0%
0%
4%
8%
12%
16%13.7%
8.0%
0%
4%
8%
12%
16%
30
Da
y D
ea
th /
MI
/ S
tro
ke
(%
)3
0 D
ay
De
ath
/ M
I /
Str
ok
e (
%)
LyticLytic Primary PCIPrimary PCI
P<0.001P<0.001 P=0.002P=0.002
CombinedCombined Transfer SitesTransfer SitesP=0.05P=0.05
Non-Transfer SitesNon-Transfer Sites
LyticLytic Primary PCIPrimary PCI LyticLytic Primary PCIPrimary PCI
14.2%
8.5%
0%
4%
8%
12%
16%14.2%
8.5%
0%
4%
8%
12%
16%
12.3%
6.7%
0%
4%
8%
12%
16%
12.3%
6.7%
0%
4%
8%
12%
16%
N=27N=27 N=15N=15N=80N=80 N=48N=48
N Engl J Med 2003; 349: 733-42N Engl J Med 2003; 349: 733-42
N=107N=107 N=63N=63
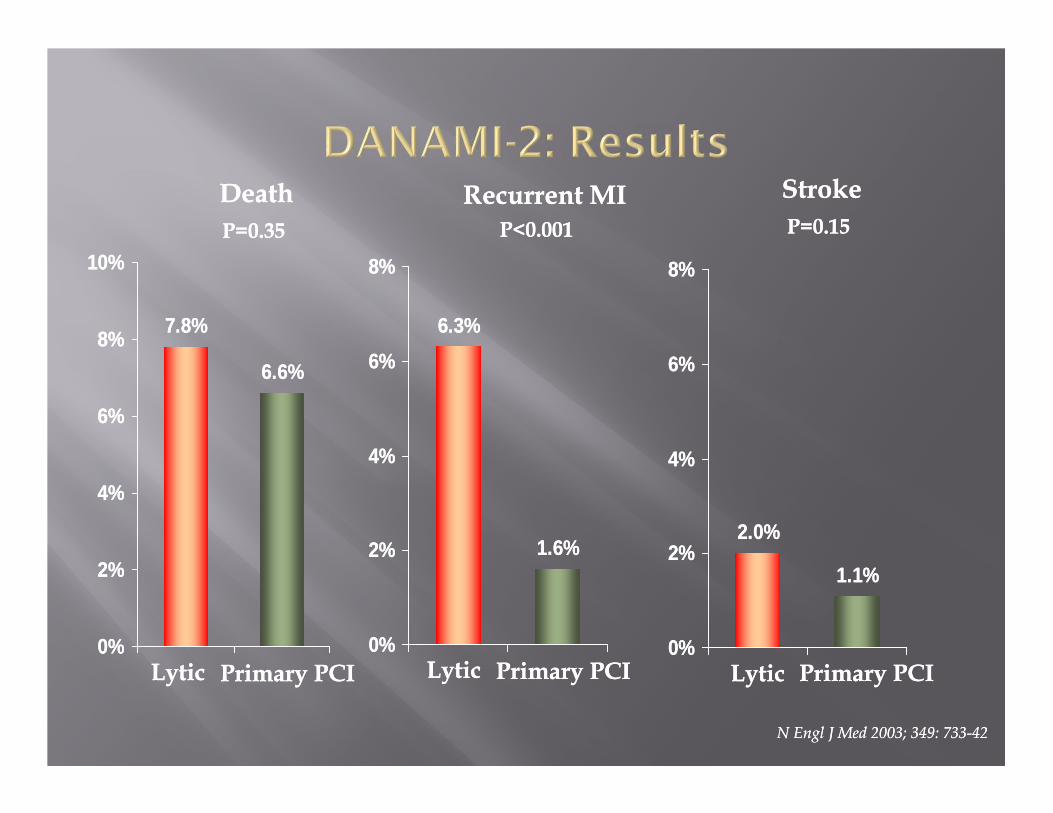
2.0%
1.1%
0%
2%
4%
6%
8%
2.0%
1.1%
0%
2%
4%
6%
8%
6.3%
1.6%
0%
2%
4%
6%
8%
6.3%
1.6%
0%
2%
4%
6%
8%
7.8%
6.6%
0%
2%
4%
6%
8%
10%
7.8%
6.6%
0%
2%
4%
6%
8%
10%
LyticLytic Primary PCIPrimary PCI
P=0.35P=0.35
DeathDeath
LyticLytic Primary PCIPrimary PCI
P=0.15P=0.15
StrokeStroke
LyticLytic Primary PCIPrimary PCI
P<0.001P<0.001
Recurrent MIRecurrent MI
N Engl J Med 2003; 349: 733-42N Engl J Med 2003; 349: 733-42

Pinto D, et al. Cardiovascular Reviews and Report. 2003;24:267-276.
0
Med
ian
Tim
e (
min
)M
ed
ian
Tim
e (
min
)
DANAMIOn-Site Primary PCI
DANAMIOn-Site Primary PCI
DANAMITransfer Primary PCI
DANAMITransfer Primary PCI
US AMITransfer Primary PCI
US AMITransfer Primary PCI
90
110
185
50
100
150
200
225
25
75
125
175


http://www.mmclc.org/
Coordination across care systems

STEMI Receiving HospitalSTEMI Referring Hospital



� Each hospital and EMS system should have contingency plan for STEMI care
� Transfer protocols
� STEMI medical protocols
� STEMI consortium development for shared protocols and data. Mission:lifeline facilitating this.