Embed Size (px)
Citation preview

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 1/9
1
0886-9634/2404-000$05.00/0, THEJOURNAL OFCRANIOMANDIBULARPRACTICE,Copyright © 2006by CHROMA, Inc.
ABSTRACT: The purpose of this study was to investigate the outcome of a series of consecutive
patients with temporomandibular disorder (TMD) who were treated with manual physical therapy inter-
ventions and exercise. Consecutive patients with the clinical presentation of TMD completed several
self-report measures and underwent a standardized historical and physical examination. Following the
examination, patients received a multimodal treatment approach incorporating manual physical therapy
and exercise. All self-report questionnaires were completed at a 2-week follow-up. Paired t-tests were
performed between the baseline and 2-week follow-up scores. The mean TMD Disability Index scoreswere 32.1% (15.4%) at baseline and 18.3% (12.5%) at the 2-week follow-up, representing an improve-
ment of 13.9% (CI: 8.2%, 19.5%) (p<0.05). Patient Specific Functional Scale (PSFS) scores improved
3.1 points (CI: 2.3, 3.9) (p<0.05). These results suggest that patients with TMD who are treated with a
rehabilitation program including manual physical therapy interventions plus exercise, with or without
iontophoresis with dexamethasone, can demonstrate clinically meaningful improvements in disability
and overall perceived change in a relatively short period of time.
Eric Furto is a physical therapist in the Newsome Physical Therapy Center in
Plainfield, Illinois and is on faculty at theUniversity of St. Augustine for HealthSciences in St. Augustine, Florida. He
obtained his bachelor of physical therapydegree in 2000 from Northern Illinois
University. Additionally, Mr. Furto servesas a continuing education instructor onspinal manipulation for the University of
St. Augustine.
Over ten million people in the United States sufferfrom temporomandibular disorders (TMD).1
Temporomandibular disorders are classified as a
musculoskeletal condition resulting in craniofacial pain,
functional limitations and disability.2 Symptoms associ-
ated with TMD can include temporomandibular joint
(TMJ) pain, decreased jaw mobility, joint clicking,
headaches, neck pain, tinnitus, and pain of the intraoral
structures.3 Temporomandibular disorders may be the
result of osteoarthritic degeneration, disk dislocation, or
involuntary guarding of the muscles of mastication.3
The debate surrounding the effectiveness of surgical
intervention for TMD has led many patients to seek con-servative care for the management of their pain and asso-
ciated loss of function.4,5 A retrospective cohort study by
Godden, et al.5 revealed that only 50% of patients who
underwent a TMJ arthroplasty viewed their outcomes as
favorable. These outcomes were obtained through a six
year follow-up survey and demonstrated that patients
experienced a reduction in pain, as measured with the
visual analog scale, to within 75% of normal; however,
the majority of patients still reported their jaw opening
was restricted (66%).5 These outcomes were determined
Manual Physical Therapy Interventions and Exercise
for Patients with Temporomandibular Disorders
Eric S. Furto, P.T.; Joshua A. Cleland, D.P.T., Ph.D.; Julie M. Whitman, P.T., D.Sc.;
Kenneth A. Olson, P.T., D.H.Sc.
PHYSICAL THERAPY
Manuscript receivedMarch 16, 2006; revisedmanuscript receivedJuly 10, 2006; acceptedAugust 1, 2006
Address for reprint requests:Eric S. Furto, P.T.Newsome Rehabilitation, Inc.920 Essington Rd.Joliet, IL 60544E-mail: [email protected]

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 2/9
based on subjective interpretations when they were asked
if they were prepared to undergo a further arthroscopy.
Conservative treatment options for TMD include
occlusion correction with the use of intraoral appliances,
orthodontics, cortisone injections, and joint manipula-
tion.3,5,6 Theoretically, intraoral appliances are used tocreate a natural resting position of the mandible, which in
turn should inhibit excessive tension in the muscles of
mastication and relieve pain and improve function.6
However, a decrease in pain does not necessarily corre-
late with an increase in range of motion (ROM) or
improvements in jaw function.5
Manual therapy directed at the TMJ combined with
exercise has been shown to be superior to treatment with
soft repositioning splint therapy in the management of
patients with radiographically confirmed anterior dis-
placed temporomandibular disk syndrome (ADTMD).7
In this study, the manual therapy combined with activeexercise group demonstrated significant reductions in
pain and increases in ROM, while the soft repositioning
splint group failed to show significant changes in either
dependent measure.7
Physical therapy management of TMD often consists
of manual therapy including TMJ and cervical/thoracic
spine mobilization/manipulation, soft tissue mobiliza-
tion, postural education/ergonomics, therapeutic exer-
cises for neuromuscular stabilization of the TMJ, and
physical modalities, such as iontophoresis, electrical
stimulation, or ultrasound.6 Rocabado6 has described
techniques to facilitate neuromuscular stabilizationthrough the use of repetitive lateral deviation motions
purportedly used to assist with mobility. Theoretically,
the muscles of mastication are then recruited to apply a
compressive force to the disk, thereby improving the
condylar-disk-eminence congruency and ultimately
improving function.6 These techniques can also be used
as a proprioceptive exercise to increase functional mobil-
ity with lowered pain response.6 However, limited evi-
dence exists to support such a treatment approach.
Only preliminary evidence exists to support the use of
manual physical therapy in the treatment of TMD.8-10 In a
single case design, Cleland, et al.9
described the outcomeof a patient with anterior bilateral disk displacement who
was treated with a combination of manual physical ther-
apy, exercise, and patient education.9 Over eight visits,
the patient achieved a reduction in pain of 48.8 mm on the
visual analog scale, an increase in mandibular depression
of 17.5 mm, and marked improvements in all three scales
of the Steigerwald/Maher TMD disability question-
naire.9,11 In a case series of 20 patients with TMD who
received TMJ exercises, postural education, and relax-
ation techniques, 16 participants experienced a complete
resolution of pain, 13 a full return to function, and only
three patients had continued ROM limitations at a six
month follow-up.8,10 Furthermore, data collected on these
patients at a 12-month follow-up visit continued to sug-
gest favorable results for the use of exercise and manual
therapy in the management of TMD.The evidence available regarding noninvasive care for
patients with TMD is sparse, and the literature is limited
by methodological shortcomings. Future studies should
ultimately examine clinical outcomes for patients prospec-
tively, including detailed descriptions of interventions
provided, use of well-defined self-report instruments to
capture levels of disability, and including a comparison
group. The current study is the first step in this process.
The purpose of this pilot study is to report clinical out-
comes (pain, disability, and function) for a series of
patients with TMD treated with manual physical therapy,
therapeutic exercise, and iontophoresis. The results of this pilot work will facilitate the design of future random-
ized controlled trials, as well as develop further hypothe-
sis formation.
Materials and Methods
During a six month period, fifteen participants were
recruited for participation in this case series (14 females).
Consecutive subjects referred to Northern Rehabilitation
and Sports Medicine Associates in DeKalb, IL with non-
specific orofacial pain were examined for eligibility crite-
ria over a 6-month period. All patients were referred fromlocal dentists, ear-eye-nose-throat physicians, and/or
general practitioners with a diagnosis of TMD or orofa-
cial pain. Eligible patients had to present with a primary
report of pain in the temporomandibular region. Eligible
patients could also exhibit cervical or thoracic spine pain,
headaches, radicular pain, and/or shoulder pain; however,
their most bothersome area had to be the TMJ. Exclusion
criteria included post surgical conditions involving the
neck or temporomandibular region. All examination and
treatment procedures in this case series were performed
by two physical therapists. Both therapists were trained in
the examination and treatment of TMD as a requirementof an American Physical Therapy Association creden-
tialed and American Acad-emy of Orthopaedic Manual
Physical Therapists recognized Manual Therapy
Fellowship Program. All participants signed an informed
consent approved by the Institutional Review Board at
Franklin Pierce College, Concord, NH prior to the initial
evaluation.
Data Collection
Prior to the initial examination, all participants com-
pleted a number of self-report questionnaires including:
PT INTERVENTIONS FOR TMD PATIENTS FURTO ET AL.
2 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE OCTOBER 2006, VOL. 24, NO. 4

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 3/9
the TMD Disability Index, two pain diagrams and the
Numeric Pain Rating Scale (NPRS). The TMD Disability
Index consists of ten questions regarding disability asso-
ciated with TMD, and each question is scored from 0-4.
Higher scores represent greater levels of disability. The
psychometric properties of this questionnaire have notbeen reported. The NPRS was used to capture the patient’s
level of pain. Patients were asked to indicate the intensity
of current, best, and worst levels of pain over the past 24
hours using an 11-point scale ranging from 0 (no pain) to
10 (worst pain imaginable).12-14 The average of the three
ratings was used to represent the patient’s level of pain
over the previous 24 hours. In addition, all patients com-
pleted the Patient Specific Functional Scale (PSFS).15
The PSFS is a patient-specific outcome measure, which
investigates functional status by asking the patient to
nominate activities that are difficult to perform based on
their condition, and rate the level of limitation with eachactivity. The patient rates each activity on a 0-10 scale,
with 0 representing the inability to perform the activity,
and 10 representing the ability to perform the activity
as well as they could prior to the onset of symptoms.16
The PSFS has been shown to identify changes in status
and to be valid and responsive to change for patients with
various clinical conditions, including neck pain,16 cervi-
cal radiculopathy,17 knee pain,18 and low back pain,15
however, the PSFS has not been used to study patients
with TMD.
Following the completion of the self-report measures,
the patient’s therapist performed a standardized historicaland physical examination. The historical examination
consisted of recording the patient’s age, gender, past
medical history, symptom location (with the use of
a body diagram), duration and nature of symptoms,
relieving/aggravating activities, and prior episodes of
TMJ pain.
The physical examination consisted of a comprehen-
sive evaluation of the TMJ and the upper quarter. Quantity
and quality of the bilateral active and passive TMJ, cervi-
cal, and thoracic mobility were assessed as described by
Paris.19,20 Active range of motion was assessed visually
by asking the patient to initially maneuver his/her cervi-cal spine throughout the cardinal planes, followed by an
assessment of the thoracic spine.19,20 Passive mobility of
the cervical spine was assessed by applying overpressure
in the direction of the ROM being tested actively.19,20
Temporomandibular joint active range of motion was
assessed by asking the patient to actively depress the
mandible, laterally deviate the mandible bilaterally, and
protrude the mandible.6,22 The motion was quantified in
millimeters utilizing a millimeter ruler between the cen-
tral incisors of the mandibular and maxillary row.6,22
Passive overpressure was not applied for the TMJ. The
quality of the motion was also assessed for compensatory
motions, visible through lateral condylar motion, through-
out the range. Accessory motion and joint play of the
TMJ, cervical spine and thoracic spine were also assessed
in combination with the patient’s pain response (eitherincreased symptoms, no change, or decreased symp-
toms).19,20 Each cervical and thoracic vertebral segment
was assessed for passive intervertebral mobility. 19,20
Capsular mobility of the temporomandibular joint was
assessed by applying a long axis distraction through the
mandible for six repetitions.6,22
Other assessments applied included an anterior
mandibular glide, a medial mandibular glide, and a lateral
mandibular glide.6,22 Mobility was graded on a 0 to 6
scale with three indicating normal capsular mobility, six
being unstable, and zero being ankylosed.19,20 Tissue
tension and flexibility were assessed for the cervicalmusculature, posterior subcranial musculature, and the
lateral pterygoid muscles.21,22 Occlusion was also assessed
by the evaluating physical therapist using maximal inter-
cuspation (MIC). MIC assesses the closed pack position
of the TMJ after swallowing. The patient is asked to bring
his/her teeth together with maximal force through biting.
The physical therapist can then assess the role the
neuromusculoskeletal system will have with maximal
muscle contraction (i.e., biting into food).6 Similar to that
of a patient with rotator cuff pathology, the neuromuscu-
lar control of the musculature surrounding the TMJ can
have an effect on the biomechanics of the mandible anddirectly affect MIC. The MIC can be compared to the
loose pack position of the mandible, or freeway space,
where the teeth rest together without biting.6,22 If there
is a shift with biting during MIC, the neuromuscular con-
trol of the muscles of the TMJ are likely participating in
the pathology.6,22
Interventions
The patient’s therapist used an impairment-based
manual physical therapy approach for the treatment of the
TMJ, cervical spine, thoracic spine, posture, and the use
of iontophoresis as indicated. In an impairment-basedmodel of care, the therapist prioritizes identified physical
impairments in the order of hypothesized importance or
contribution to the patient’s disorder. The therapist then
provides treatment, or interventions, targeting these iden-
tified physical impairments, such as joint mobility restric-
tions, muscle length limitations, postural limitations and
neuromuscular deficits.
Manual physical therapy directed at identified impair-
ments of the cervical spine consisted of nonthrust manip-
ulations for facet upglides and downglides to facilitate
FURTO ET AL. PT INTERVENTIONS FOR TMD PATIENTS
OCTOBER 2006, VOL. 24, NO. 4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 3

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 4/9
normal facet joint motion, subcranial forward bending
and sidebending non-thrust manipulations, and subcra-
nial myofascial distraction.19,20 Stretches to the surround-
ing cervical musculature were also applied as described
by Kendal.21 Non-thrust temporomandibular joint manip-
ulations consisted of long axis distraction, medial glide,and lateral glide as described by Rocabado.22 Acupressure
techniques were also applied to the lateral pterygoid mus-
culature.22 All treatment applications are described in
Table 1.
Each patient was instructed in a condylar remodeling
exercise program as described by Rocabado.22 Phase one
of this program consists of painfree lateral deviation
away from the side of pain or hypermobility as deter-
mined with accessory motion testing with a 0.5 inch piece
of surgical tubing resting between the mandibular and
maxillary row of teeth. If pain is bilateral, the device is
maneuvered away from the side of greatest hypermobil-ity. If painfree, a bite is incorporated.6 The patient was
instructed to release the contraction before returning to
midline. The third phase consists of the same submaximal
contraction as phase two, but the contraction is main-
tained until the tubing returns to midline. The fourth
through sixth phases are similar to phases one through
three, but are performed for protrusion rather than lateraldeviation. Patients were instructed to perform six repeti-
tions every two hours3 (see Appendix). The exercise
program was reviewed at each treatment session. The
exercise program focused on ROM and stability exercises
for all patients suspected to exhibit anterolateral disk
translation during the clinical examination (n=8). The lat-
eral deviation motion that accompanies the condylar
reeducation exercise program has been purported to
enhance mobility throughout the range of motion. This
program can be converted to a controlled neuromuscular
stabilization exercise program by incorporating and
maintaining a bite throughout the ROM.22
In addition to the aforementioned interventions, ion-
tophoresis with dexamathasone was incorporated with
patients where ROM was restricted primarily due to pain
(less than 20 mm of mandibular opening). An aqueous
solution of 2.5 cc dexamethasone was applied superfi-
cially at 40 milliamps minutes to the affected TMJ. The
treatment was applied for fifteen minutes and then
removed.
Follow-Up
At the two-week follow-up visits, all patients again
completed the TMD Disability Index, PSFS, body dia-grams, and NPRS. In addition, all patients completed the
Global Rating of Change scale.23 Patients were asked to
rate their overall perception of improvement since begin-
ning physical therapy on a scale ranging from –7 (a very
great deal worse) to zero (about the same) to +7 (a very
great deal better). It is recommended that scores on the
GROC between ±1 and ±3 represent small changes,
scores between ±4 and ±5 represent moderate changes,
and scores of ±6 or ±7 convey large changes in patient
status.23
Statistical Analysis
Descriptive information including patient gender, age,
duration of symptoms, number of physical therapy visits,
and interventions provided was recorded for all patients.
The mean change score and associated 95% confidence
intervals were calculated for all outcome measures
assessed at baseline and at the 2-week follow-up. Paired
t-tests were performed between the baseline and 2-week
follow-up scores (α=0.05) to evaluate if the change expe-
rienced was significant over time.
PT INTERVENTIONS FOR TMD PATIENTS FURTO ET AL.
4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE OCTOBER 2006, VOL. 24, NO. 4
Table 1
Descriptive Characteristics of ParticipatingPatients at Baseline (N=15)
Number (%)Variable of Patients*
Age (years), mean (SD) 50.5 (15.5)
Sex - female 14 (93%)- male 1 (7%)Race - Caucasian 15 (100%)Median duration of
TMD symptoms (range) 6 mos. (0.07-120)Depression (self-report) 6 (40%)Symptom descriptions
TMJ region symptoms 15 (100%)- bilateral 3 (20%)- painful 13 (87%)- sharp 3 (20%)- dull 2 (13%)- aching 13 (87%)
Headache symptoms 13 (87%)- median duration
symptoms (range) 6 mos. (0.07-60)- dizziness associated
with headache 2 (13%)Cervical spine symptoms 9 (60%)
- median durationsymptoms (range) 30 mos. (2-252)
- bilateral symptoms 6 (40%)Thoracic spine symptoms 7 (47%)Upper extremity symptoms 5 (33%)
- bilateral symptoms 2 (13%)*n (%) provided unless otherwise noted

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 5/9
Results
All participants were asked to complete the TMD
Disability Index, with three (20%) participants electing to
bypass the question regarding the level of sexual function
limitation. Demographics for all patients can be found inTable 1. The median length of symptoms in the region of
the TMJ was six months (range 0.07-120 months).
Thirteen (87%) of the patients also experienced headache
symptoms with the median duration also being six months
(range 0.07 to 60 months). As recorded by the PSFS, the
following percentage of patients noted difficulty chew-
ing, yawning, talking, and opening the jaw, respectively:
15 (100%), seven (47%), four (27%), and one (7%). At
the two-week follow-up session, the group had received a
mean of 4.3 physical therapy intervention sessions.
Specific interventions received can be found in Table 2.
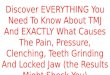
The mean TMD Disability Index scores were 32.1% atbaseline and 18.3% at the 2-week follow up, representing
an improvement of 13.9% (CI: 8.2%, 19.5%) (p<0.05)
(Figure 1). Eleven patients (73%) reported they were
somewhat better to a very great deal better on the GROC
(Table 3), and Patient Specific Functional Scale (PSFS)
scores improved 3.1 points (CI: 2.3, 3.9) (p<0.05) (Figure
2).
Discussion
There currently is a lack of conclusive evidence to sup-
port the use of conservative management strategies in themanagement of TMD. The purpose of this study was to
describe the outcomes of a cohort of patients undergoing
physical therapy management of their TMD. Outcomes
were favorable for all patients in this study and are simi-
lar to findings of Nicolakis, et al.8 who provided a six and
twelve month follow-up supporting the use of manual
therapy and exercise with a case series of twenty patients
with TMD.10 Interventions used in the Nicolakis, et al.8
study were similar this study and included nonthrust
manipulative therapy directed at the TMJ and an isomet-
ric exercise program aimed at maximizing stability of the
TMJ.We have provided a detailed description of the inter-
ventions used to treat TMD in this pilot study and used
physical impairment as well as self-report outcomes to
capture the patient’s levels of pain and disability. Our
patients, similar to those in the Nicolakis, et al.8 case
series, demonstrated an overall reduction in pain and
improvement in function following two weeks of physi-
cal therapy management. During a six-month period, fif-
teen participants received intervention for their TMD
complaints.10 Of the 15 patients treated in this pilot study,
13 also experienced headache symptoms at the time of the initial examination. It is hypothesized that poor pos-
ture with increased posterior rotation of the cranium on
the atlas will place undue strain on the posterior occipital
musculature.6,22 This strain may impinge upon the greater
occipital nerve and may result in referred pain into the
craniofacial region, most typically into the distribution of
the trigeminal nerve.24 In a study by Aprill, et al.25 it was
discovered that 21 of 34 participants who underwent a
nerve block to C1/C2 experienced complete resolution of
their headache symptoms. These findings are indicative
of the comorbidity between TMJ pain and headache and
may also support the possibility of referred pain to theTMJ from the subcranial spine. Therefore, it is possible
that participants in the study may have not experienced
symptoms related to the TMJ, but they could also have
been experiencing symptoms referred from the cervical
spine.
The exercise program used in this pilot study was
aimed at neuromuscular reeducation of the musculature
surrounding the temporomandibular joint (Appendix).
The exercises prescribed to each patient used a piece of
tubing in a similar fashion to that of an anterior loading
splint.6 The piece of tubing was placed between the
incisors and a series of motions were performed and com-bined with biting. Once the patient was able to perform
painfree lateral deviation with the exercise program, they
were instructed to perform protrusion. Lateral deviation
is typically performed initially to ensure appropriate
ROM of the affected TMJ before recruiting the opposite
joint during protrusion. The patients were instructed to
perform the exercises in a pain free fashion, every two
hours to enhance functional joint stability.6
Exercise has been shown to be effective in the man-
agement of TMD. In a randomized clinical trial, Yoda, et
FURTO ET AL. PT INTERVENTIONS FOR TMD PATIENTS
OCTOBER 2006, VOL. 24, NO. 4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 5
Table 2
Number (Percentage) of Patients (n=15) TreatedWith Various Physical Therapy Interventions
Number (%)Manual technique of Patients
Cervical spine manipulation- subcranial (occiput-C2) 11 (73%)- cervical spine (C2-C7) 6 (40%)
TMJ manipulation 15 (100%)Thoracic spine manipulation 4 (27%)Postural education 12 (80%)Iontophoresis to the TMJ 5 (33%)

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 6/9
al.26 compared an exercise program to education on the
condition for patients with anterior disk displacement
with reduction (ADDWR). The results demonstrated that
the exercise group had statistically significant better out-
comes for decreased pain and increased ROM (p=0.0001).
Forty-two patients participated in the study, of which
61.9% of the exercise group had favorable outcomes
(13/21 patients), while 0% of the control group had favor-able results.26 Success was measured on the severity of
joint sounds and/or pain with maximal mouth opening.
Of the 13 patients that experienced a successful outcome,
only 23.1% (three) of the patient’s TMJ disks were actu-
ally recaptured when reexamined on MRI. The authors
reported that the 61.9% success rate experienced by the
exercise group is similar to that of splint therapy but is a
more cost effective option.26
The exercises proposed by Yoda, et al.26 differ fromthose proposed by Rocabado22 in that maximal ROM is
PT INTERVENTIONS FOR TMD PATIENTS FURTO ET AL.
6 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE OCTOBER 2006, VOL. 24, NO. 4
Figure 1TMD Disability Index scores at baseline
and at 2-week follow-up.
Figure 2Patient Specific Functional Scale scores atbaseline and at 2-week follow-up.

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 7/9
required in the Yoda approach from the initiation of the
exercise program. In many cases, painful ROM is the
reason for consultation by a physical therapist, thus
making maximal ROM to the point of reduction a diffi-
cult starting point for the initiation of exercises. The pro-
gram described by Rocabado22 and used in the currentstudy encourages small ranges of motion into lateral
deviation, which may accomplish the same objective:
reduced pain and improved function. While research
exists to support the use of exercise in the management of
TMD, limited evidence exists to support the specific
exercise regimen used in this study.6,26,27
Additionally, we included the use of iontophoresis
with dexamethasone in the treatment of patients within
this pilot study. While dexemethasone has been demon-
strated to be effective in reducing pain and inflammation,
the delivery method of iontophoresis has been ques-
tioned. In a study by Majwer, et al.,28 27 of 32 cases of post-traumatic TMD benefited with decreased pain from
the application of dexamethasone (n=8) or xylocane
(n=24) through iontophoresis. Since different medica-
tions were used, it is possible that the patients benefited
most from the electrical stimulation of the iontophoresis
rather than the medication itself.
The present study allows for hypothesis formulation
and the development of a future randomized clinical trial.
Follow-up studies should include examining the effec-
tiveness of exercise and manual physical therapy when
compared to other conservative treatment approaches.
The patients in this study exhibited positive outcomesafter receiving only two weeks of the above described
multimodal physical therapy treatment regimen.
Limitations of the current study include the lack of a
control or comparison group which precludes the abil-
ity to infer a cause and effect relationship between the
treatment and outcomes, as well as, only short-term out-
comes are provided in this report. It is the aim of the
authors to identify the long-term effects of the treatment
interventions used in this pilot study and determine if a
specific subgroup of patients with TMD exists that would
be most likely to benefit from exercise and manual phys-
ical therapy.
Conclusion
The results of this study demonstrate that physical
therapy intervention consisting of manual therapy, a
specific exercise program, and iontophoresis with
dexamethasone can be beneficial to patients presenting
with symptoms similar to that of TMD. Future research
should focus on the specific interventions as described
above to determine the most beneficial form of treatment.
Clinical decision making rules may also be established to
enhance the identification of particular patients that are
likely to respond rapidly and dramatically to specific
interventions.
References
1. TMJ Diseases & Disorders - Basics - Overview. www.tmj.org/basics.asp.
2. Merskey H, Bogduk N: Classification of chronic pain. Seattle, WA: IASP
Press, 1994.3. Kraus S: Clinics in Physical Therapy: temporomandibular joint disorders.
New York: Churchill Livingstone, 1994.
4. Dolwick MF, Dimitroulis G: Is there a role for temporomandibular jointsurgery? Br J Oral 1994; 32:307-313.
5. Godden DRP, Robertson JM: The value of patient feedback in the audit of
TMJ arthroscopy. Br Dent J 2000; 188:125.6. Rocabado M: Intermediate craniofacial. Chicago; 2003.
7. Carmeli E, Sheklow S, Bloomenfeld I: Comparative study of repositioning
splint therapy and passive manual range of motion techniques for anteriordisplaced temporomandibular disks with unstable excursive reduction.
Physiother 2001; 87:26-36.
8. Nicolakis P, Burak EC, Kollmitzer J, Kopf A, Piehslinger E, Wiesinger GF,
Fialka-Moser V: An investigation of the effectiveness of exercise andmanual therapy in treating symptoms of TMJ osteoarthritis. J Craniomandib
Pract 2001; 19:26-32.
9. Cleland J ,Palmer J: Effectiveness of manual physical therapy, therapeuticexercise, and patient education on bilateral disk displacement without
reduction of the temporomandibular joint: a single-case design. J Orthop
Sports Phys Ther 2004; 34:535-548.10. Nicolakis P, Erdogmus B, Kopf A, Ebenbichler G, Kollmitzer J, Piehslinger
E, Fialka-Moser V: Effectiveness of exercise therapy in patients with inter-
nal derangement of the temporomandibular joint. J Oral Rehabi l 2002;29:362-368.
11. Steigerwald DP, Maher JH: The Steigerwald/Maher TMD disability ques-
tionnaire. Today’s Chiropractic 1997; July-August:86-91.12. Jensen MP, Karoly P, Braver S: The measurement of clinical pain intensity: a
comparison of six methods. Pain 1986; 27:117-126.
13. Childs JD, Piva S, Fritz JM: Responsiveness of the numeric pain rating scalein patients with low back pain. Spine 2004:
14. Pengel HM, Refshauge K, Maher C: Responsiveness of pain, disability, and
physical impairment outcomes in patients with low back pain.Spine 2004;
29:879-883.15. Stratford P, Gill C, Westaway M, Binkley J: Assessing disability and change
of individual patients: a report of a patient-specific measure. Physiother
Can 1995; 47:258-263.
16. Westaway M, Stratford P, Binkley J: The Patient Specific Functional Scale:
validation of its use in persons with neck dysfunction. J Orthop Sports Phys
Ther 1998; 27:331-338.
17. Cleland JA, Fritz JM, Whitman JM, Palmer J: Construct validity of the Neck
Disability Index and Patient Specific Functional Scale in a patient popula-tion with cervical radiculopathy. Spine In Press
18. Chatman A, Neel J, Hyams S: The Patient Specific Functional Scale: mea-
surement properties in patients with knee dysfunction. Phys Ther 1997;77:820-829.
19. Paris SV: Intro to spinal manipulation. 2000; S1.
20. Paris SV: Advanced manipulation of the cervical spine. 2000; S3.21. Peterson-Kendall F, Kendall-McCreary E, Provance PG: Muscle testing and
function. Baltimore: Williams and Wilkins, 1993.
22. Rocabado M, Iglarsh Z: Musculoskeletal approach to maxillofacial pain.
New York: JB Lippincott Co., 1991.23. Jaeschke R, Singer J, Guyatt G: Measurement of health status. Ascertaining
the minimal clinically important difference. Controlled Clinical Trials
1989; 10:407-415.24. Packard RC: The relationship of neck injury and post-traumatic headache.
Curr Pain Headache Rep 2002; 6:1-7.
25. Aprill C, Axinn M, Bogduk N: Occipital headaches stemming from the lateralatlanto-axial (C1-C2) joint. Cephal 2002; 22:15-22.
26. Yoda T, et al.: A randomized controlled trial of therapeutic exercise for click-
ing due to disk anterior displacement with reduction in the temporo-mandibular joint. J Craniomandib Pract 2003; 21:10-16.
27. Deodato F, Cristiano S, Trusendi R, Giorgetti R: A functional approach to the
TMJ disorders. Prog Orthod 2003; 4:20-37.28. Majwer K, Swider M: Results of treatment with iontophoresis of posttrau-
matic changes of temporomandibular joints with an apparatus of own
design. Prothet Stomatol 1989; 39:172-176.
FURTO ET AL. PT INTERVENTIONS FOR TMD PATIENTS
OCTOBER 2006, VOL. 24, NO. 4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 7

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 8/9
PT INTERVENTIONS FOR TMD PATIENTS FURTO ET AL.
8 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE OCTOBER 2006, VOL. 24, NO. 4
Appendix

7/26/2019 Manual Therapy for TMJ Dysfunction Furto Joshua Whitman
http://slidepdf.com/reader/full/manual-therapy-for-tmj-dysfunction-furto-joshua-whitman 9/9
Dr. Joshua A. Cleland is currently an assistant professor at FranklinePierce College and is the research coordinator at Rehabilitation Servicesof Concord Hospital. He recently completed a fellowship in the manual
therapy program through Regis University in Denver, Colorado. Dr.
Cleland’s research interest includes investigating the effectiveness of manual therapy and exercise in patients with extremity and spinal disor-ders. He recently authored a text on the orthopedic clinical examinationand has published numerous articles in peer reviewed journals.
Dr. Julie M. Whitman is an assistant professor in the Department of Physical Therapy at Regis University in Denver, Colorado. She received
an M.P.T. degree from the U.S. Army-Baylor University GraduateProgram in Physical Therapy from Baylor University in 2001. Shecompleted a manual physical therapy residency program in 2000 and has
over 12 years of primary care physical therapy experience in the civilianand military environments. Dr. Whitman is actively involved in clinicalresearch relating to orthopedic/manual physical therapies for muscu-
loskeletal disorders and has over 20 publications in these areas.
Dr. Kenneth A. Olson is president of the physical therapy private
practice, Northern Rehabilitation and Sports Medicine Associates in DeKalb, Illinois. Dr. Olson is also a guest lecturer at Marquette
University and serves as a mentor for the University of St. Augustine Manual Therapy Fellowship program. He graduated with a B.S.P.T. from Northern Illinois University, a Master of Science in orthopedic
physical therapy from the University of St. Augustine, and a Doctor of Health Science USA. He is also a graduate of the USA Manual Therapy
Fellowship Program.
FURTO ET AL. PT INTERVENTIONS FOR TMD PATIENTS
OCTOBER 2006, VOL. 24, NO. 4 THE JOURNAL OF CRANIOMANDIBULAR PRACTICE 9






![furto - A.S.L. Napoli 1 Centro · QUESTURA di MILANO COMMISSARIATO DI P.s. "PORT:] T]C7NËSE - CFFtClO DENC.NCE- OGGVITO: DENUNCIA DI FURTO. Resa da la sig.r;t DI Laura Consilia,](https://img.pdfslide.us/doc/110x75/5be7cd1a09d3f246788d124f/furto-asl-napoli-1-questura-di-milano-commissariato-di-ps-port-tc7nese.jpg)