Embed Size (px)
Citation preview

Stage 3: Improving Aboriginal Patient Journeys—
Study Report
Managing Two Worlds
Together
Janet Kelly Judith Dwyer
Brita Pekarsky Tamara Mackean
Eileen Willis Charlotte de Crespigny
Sharon Perkins Kim O’Donnell
Rosie King Laney Mackean
Alex Brown Monica Lawrence
Karen Dixon

Cover Artwork:Kuntjanu – Mingkiri Tjuta Tjukurpa (Marsupial Mouse Dreaming)
by Rama Sampson painting (no.74), courtesy Better World Arts

Stage 3: Improving Aboriginal Patient Journeys—
Study Report
Managing Two Worlds
Together
Janet Kelly Judith Dwyer
Brita Pekarsky Tamara Mackean
Eileen Willis Charlotte de Crespigny
Sharon Perkins Kim O’Donnell
Rosie King Laney Mackean
Alex Brown Monica Lawrence
Karen Dixon

© Flinders University, 2015
ISBN 978-1-921889-28-8
First published in April 2015
This work has been produced by Flinders University and is published as part of the activities of The Lowitja Institute, Australia’s national institute for Aboriginal and Torres Strait Islander health research, incorporating the Lowitja Institute Aboriginal and Torres Strait Islander Health CRC (Lowitja Institute CRC), a collaborative partnership funded by the Cooperative Research Centre Program of the Australian Government Department of Industry.
This work is the copyright of Flinders University. It may be reproduced in whole or in part for study or training purposes, or by Aboriginal and Torres Strait Islander community organisations subject to an acknowledgment of the source and no commercial use or sale. Reproduction for other purposes or by other organisations requires the written permission of the copyright holder(s).
Printed copies and a pdf of the Managing Two Worlds Together. Stage 3: Improving Aboriginal Patient Journeys—Study Report, along with a writeable pdf of the Workbook and pdfs of all five Case Studies, can be obtained from:
Authors: Janet Kelly, Judith Dwyer, Brita Pekarsky, Tamara Mackean, Eileen Willis, Charlotte de Crespigny, Sharon Perkins, Kim O’Donnell, Rosie King, Laney Mackean, Alex Brown, Monica Lawrence and Karen Dixon
Managing Editor: Jane Yule @ Brevity Comms
Cover Artwork: Kuntjanu – Mingkiri Tjuta Tjukurpa (Marsupial Mouse Dreaming) by Rama Sampson painting (no.74), courtesy Better World Arts
Design and Print: Inprint Design
For citation: Kelly, J., Dwyer, J., Pekarsky, B., Mackean, T., Willis, E., de Crespigny, C., Perkins, S, O’Donnell, K., King, R., Mackean, L., Brown, A., Lawrence, M. & Dixon, K. 2015, Managing Two Worlds Together. Stage 3: Improving Aboriginal Patient Journeys—Study Report, The Lowitja Institute, Melbourne.
The Lowitja InstitutePO Box 650, Carlton SouthVic. 3053 AUSTRALIA
T: +61 3 8341 5555 F: +61 3 8341 5599 E: [email protected]: www.lowitja.org.au
Department of Health Care ManagementFlinders UniversityBedford Park, SA 5042 AUSTRALIA
T: +61 8 8201 7755 F: +61 8 8201 7766 E: [email protected]: www.flinders.edu.au

iii
Table of Contents
The Managing Two Worlds Together Project v
Acknowledgments vi
Abbreviations and Terms vi
About this Report 1
Why the Need for Specific Patient Journey Mapping for Aboriginal People? 2
Study Design and Methods 4
Research Aims, Questions and Principles 7
The Patient Journey Mapping Process 8
Reflection and Evaluation of How the Tools Were Used in this Study 23
Conclusion 25
References 27
Diagrams, Figures and Tables
Diagram 1: The three stages, focus and outcomes of the Managing Two Worlds Together project vDiagram 2: Involvement of staff participants, patients and communities in Stage 3 5Diagram 3: The process of using the Aboriginal PJM tools – an overview 8
Example Figure 1: Visual mapping 11Example Figure 2: Comparison of patient journey to standards of care 18Example Table 1: Dimensions of health 12Example Table 2: Underlying factors 13Example Table 3: Multiple perspectives 14Example Table 4: Additional considerations 15Example Table 5: Action plan 22

iv

v
The Managing Two Worlds Together Project
The Improving Aboriginal Patient Journeys (IAPJ) study is the third stage of the Managing Two Worlds Together (MTWT) project. The MTWT project investigated what works well and what needs improvement in the health system for Aboriginal people who travel for hospital and specialist care from rural and remote areas of South Australia and the Northern Territory to city hospitals.
Stage 1 (2008–11) focused on understanding the problems that occur within and across patient journeys, and the barriers and enablers to access, quality and continuity of care. Challenges and strategies from the perspectives of individual Aboriginal patients, their families, and health and support staff and managers were examined using interviews, focus groups and patient journey mapping. Complex patient journeys were analysed and a patient journey analysis tool was developed collaboratively with staff, patients and carers.
Stage 2 (2012) focused on possible solutions and strategies. As the research team shared findings with health care providers, case managers and educators in a range of different health and education settings, the potential and scope of the Aboriginal patient journey mapping (PJM) tools for quality improvement, training and education
emerged. The resulting tools consist of a set of tables that enable an entire patient journey to be mapped across multiple health and geographic sites, from the perspective of the patient, their family and health staff in each location.
Stage 3 (2013–15) involved an expanded research team and staff participants working together in a range of health care and education settings in South Australia and the Northern Territory. The aim was to modify, adapt and test the Aboriginal PJM tools developed in Stages 1 and 2. As the project progressed the basic set of tools was further developed with flexible adaptations for each site. This involved three steps – Preparing to map the patient journey, Using the tools and Taking action on the findings – organised into 13 tasks with prompt questions. Careful consideration was given as to how the information that emerged from the use of the tools could best highlight communication, coordination and collaboration gaps within and between different health care providers (staff, services and organisations) so as to inform the design of effective strategies for improvement. These were compared and combined with existing policies, practice and protocols.
Diagram 1 (below) sets out these three stages, along with the focus and outcomes of each stage.
Focus: Understanding the problems
Identifying the barriers, enablers, gaps and strategies to care
MTWT reports
City Hospital Care for Country Aboriginal People—Project Report
City Hospital Care for Country Aboriginal People—Community Summary
Study 1—Report on Admissions and Costs
Study 2—Staff Perspectives on Care For Country Aboriginal
Patients
Study 3—The Experiences of Patients and their Carers
Study 4—Complex Country Aboriginal Patient Journeys
Focus: Exploring solutions and strategies
Considering application of findings and mapping tools
MTWT reports
Stage 2: Patient Journey Mapping Tools
Focus: Improving Aboriginal patient journeys
Modifying, adapting and testing mapping tools for quality improvement and education
Knowledge exchange and translation
MTWT reports
Stage 3: Improving Aboriginal Patient Journeys—Study Report
Stage 3: Improving Aboriginal Patient Journeys—Workbook
(Version 1)
Stage 3: Improving Aboriginal Patient Journeys—Case Studies
• Renal
• Cardiac
• Maternity
• Rural and Remote Sites
• City Sites
Stage 1: 2008–11 Stage 2: 2012 Stage 3: 2013–15
Diagram 1: The three stages, focus and outcomes of the Managing Two Worlds Together project

vi
Russell, Bronwyn Ryan, Amy Sawford, Rosalie Schultz, Tim Schultz, Kerry Taylor, Kym Thomas, Jeff Tinsley, Rachel Tipoti, Cheryl Wilden, Jacene Wiseman, Sarah Wyatt and Chris Zeitz.
Particular thanks to Jo Newham, Jacene Wiseman and Yvonne Inguz for their feedback on draft versions of this Study Report.
We would also like to acknowledge the editorial assistance of Jane Yule and Cathy Edmonds, the design work of Rachel Tortorella at Inprint Design, and the Lowitja Institute CRC for providing ongoing support for this study and publishing its outcomes.
We acknowledge the following people who were involved directly as participants, or indirectly as advisors or key stakeholders of this study and report:
Hugh Auckram, Jenny Brands, Sarah Brown, Lisa Catt, Christine Connors, Carol Cooper, Wendy Corkhill, Claire Davies, Kain Donily, Toni East, Joanne Else, Amy Graham, Kylie Herman, Liz Izquierdo, Denise Karpany, Wendy Keech, Michael Kirkbride, Natalie McCabe, Wendy McInnes, Jillian Marsh, Gay Martin, Lee Martinez, Sonia Mazzone, Paula Medway, Debra Miller, Jo Newham, Annapurna Nori, Daphne Perry, Pam Pratt, Holly Prest, Mark Ramage, Damian Rigney, Christine
Acknowledgments
Abbreviations and Terms
AHW Aboriginal Health Worker
ALO Aboriginal Liaison Officer
ECG Electrocardiogram (recording of heart’s electrical activity)
Echo Echocardiogram (a sonogram that creates images of the heart)
GP General Practitioner
IAPJ Improving Aboriginal Patient Journeys
Terminology
The use of the terms ‘Aboriginal’, ‘Aboriginal and Torres Strait Islander’, ‘Indigenous’ and ‘Elder’ reflect the preference of the people with whom we worked.
Case study – The use of the term ‘case study’ refers to specific problem-solving activities undertaken by participating health staff to better understand and improve care for their patients. We also recognise individual patients as ‘people’ rather than ‘cases’.
Patient – We have used the word ‘patient’ to identify the person undergoing a health care journey. In some services other terms may be used such as
MTWT Managing Two Worlds Together
PAR Participatory Action Research
PATS Patient Assistance Transport/Travel Scheme – South Australia/Northern Territory
PJM Patient Journey Mapping
RAN Remote Area Nurse
RFDS Royal Flying Doctor Service
‘client’ or ‘consumer’. At all times we recognise that ‘patients’ are individual people with unique personal, family and/or cultural needs and priorities.
Participants –This term has been used to describe those staff in city and rural and remote hospitals, health services and support services who participated with us in this study. The staff involved included Aboriginal Health Workers, nurses (clinical, managers and educators), public health physicians, coordinators and managers of Aboriginal and mainstream health and support services (at multiple levels).

1
This Study Report summarises the activities, findings and challenges of the Improving Aboriginal Patient Journeys study, which is Stage 3 of the Managing Two Worlds Together project. The aim of the IAPJ study was to develop, refine and evaluate a set of Aboriginal patient journey mapping tools for use in quality improvement and education. A collaborative approach to knowledge exchange was used, with the research team working with staff and managers from a range of health settings in South Australia and the Northern Territory. Together we explored how the tools could be adapted and used to make real improvements in communication, coordination and collaboration within and across a diverse range of patient journeys.
The study focuses on improving the health care journey for Aboriginal people as they travel from home to hospital to home across numerous geographical and health care sites. The tools are designed to assist patients, families, health staff, managers, educators, students and other key stakeholders to better understand the complexities of each journey in order to make positive changes.
The main advancement in the format of the tools from Stage 2 to Stage 3 is that they have been developed from an original set of three tables into this comprehensive report and accompanying Workbook and Case Studies, all of which have a greater emphasis on planning, comparing each patient journey to standards and quality of care, and working with the findings.
In this study we again identify that many care journeys are complex, challenging and overwhelming not only for the person experiencing them, but also for their families and the staff members supporting them within and across various health and support services.
The Aboriginal PJM tools described in this report were used:
1. to understand and identify the complexity of the patient journey
2. to make the complex patient journeys visible
3. to organise the journey for analysis and response
4. to highlight the critical steps, gaps and responses, thus providing a focus for targeted action by health care providers.
They can also be used to assist staff in identifying local solutions for wider systemic problems, as well as emphasising particular patient risks that require immediate organisational, policy and procedural changes.
Six other documents accompany this Study Report. The first is a practical Workbook, which explains how to adapt and use the Aboriginal PJM tools in a new setting, with tools provided in a writeable PDF format. The other five are Case Studies – focusing on Renal, Cardiac, Maternity, Rural and Remote Sites, and City Sites – that provide examples of how health professionals and support staff have adapted and used the tools for a diverse range of settings and patient journey types. Copies of these and of this Study Report are available at: www.lowitja.org.au/lowitja-publishing.
The value of the Case Studies is that they show practical application of the tools. It is important to note, however, that these Case Studies were an integral part of the development of the Aboriginal PJM tools and were undertaken at different times during the year. Therefore, they do not all reflect this final format of the tools as not all tasks within each step were developed at that time.
About this Report

2
Aboriginal people from rural and remote areas of South Australia and the Northern Territory often need to travel to city hospitals for inpatient and outpatient services, and to receive specialist care, tests and investigations that are unavailable in their own geographic locations. Their journeys may be planned for existing health problems or unplanned as a result of urgent or emergency situations arising from a new illness or injury. They may travel alone or with family, and have greater or lesser practical and financial support. English might be their first, second or third language and they may or may not be provided with an interpreter or clear explanations about the journey or their illness.
At times they could be required to make difficult or life-changing decisions, while also feeling isolated and a long way from home. Their own priorities and commitments may or may not be recognised and respected in a mainstream city setting, and only some of them might receive access to and support from Aboriginal Liaison Officers (ALOs), social workers or rural coordinators. Findings from Stage 1 of the M2WT project indicate that Aboriginal patients and their families cannot reliably anticipate that they will receive culturally safe and supportive care in all health care sites, from all staff members.
Usually there is no one person or service supporting their entire patient journey from home to hospital to home. Communication and support gaps are often encountered, particularly when travelling between rural and remote and city services, primary health and hospital care, and between Aboriginal-specific and mainstream services. Sometimes patient journeys are smooth, uncomplicated and well supported; at other times such journeys are stressful or confusing and, as a result, some people opt out.
This study seeks to enable a better understanding of actual Aboriginal patient journeys in order to improve the coordination, communication, collaboration, cultural safety and support provided.
The current situation
Staff in rural and remote health settings prepare patients and carers as best they can for their journey to a city hospital. However, time, resources, funding and different levels of understanding about city services may compromise the level of support, coordination and information exchange established before the patient journey begins, particularly when a person’s health concern requires testing or investigation while in the city.
Specialist visits to rural and remote areas may significantly reduce the number of long distance journeys that patients (and their families) need to travel. These visits also enable relationships to develop between the patient, the specialist and support staff prior to, and throughout, the journey, leading to improved communication.
Once the patient has been admitted to the city hospital, the health staff back in their community may or may not be informed of the patient’s progress, or be involved in plans for their return. On discharge from the hospital, staff may receive adequate transfer of care information for ongoing treatment and follow-up, or spend hours chasing discharge letters and new medication regimes. Depending on their location, it may take up to a week to order and receive new medications from a regional centre, and when patients are discharged with only one week’s supply of medications and have a long journey home, staff may struggle to ensure essential medication is available.
Staff in city hospitals bring a diverse range of experiences and skills, and work with the challenges of providing care within a busy city hospital. Most have not lived or worked in rural or remote or Aboriginal communities, and many have little understanding of the vast distances, the limited range of local health services, the unique challenges of rural and remote living, or the preferences of individual people and communities.
Why the Need for Specific Patient Journey Mapping for Aboriginal People?

3
Both staff new to Australia and those who have grown up here may hold a wide range of personal views – many of which may be unhelpful – regarding Aboriginal people and the care they require for equitable outcomes. These views often remain unchallenged, particularly when positive cultural safety training has not been provided and there is little discussion about social determinants of health and geographic distances, and how these impact on patients and community groups.
Despite these difficulties, many health staff strive to ensure positive care experiences and coordinated journeys, and to enhance their knowledge and expertise so they can enact specific strategies to ensure good care. Wards and units with high numbers of Aboriginal rural and remote patients may have an increased focus on working well with Aboriginal people and their families, and thus could be more likely to ensure required services and supports are in place to meet complex needs.
Opportunities for change
There is great potential value in working with staff and leaders of health services, wards and units to review patient journeys, policies and practices and to work toward strategies for improving the quality and coordination of care for rural and remote Aboriginal people. Key staff members often understand the health system, and have identified the gaps within it and worked out the most effective strategies to fill them.
Coordinators and Aboriginal staff hold unique knowledge, understanding and experience of the current health systems and, as a result, have often developed strong problem-solving skills. But they face difficulties in effecting change due to short-term funding, poor recognition of their role by other staff, or a lack of authority and opportunity to effect health service and systems change. However, more senior staff may be in the position to make policy and practice changes within their unit, and advocate for wider service and systems change.
Bringing together staff with different knowledge, skills and positions in a structured but participative way can enable real quality improvement in care. Discussing the findings and their implications for system-level changes with higher level managers and policy makers, as well as with educators to update professional education, are key strategies for effective change.

4
The research team consisted of the following Aboriginal and non-Aboriginal researchers, clinicians, managers and coordinators: Janet Kelly, Judith Dwyer, Sharon Perkins, Kim O’Donnell, Laney Mackean, Monica Lawrence, Karen Dixon, Brita Pekarsky, Tamara Mackean, Rosie King, Alex Brown, Eileen Willis and Charlotte de Crespigny. A collaborative approach between Aboriginal and non-Aboriginal research team members and health service partners enabled patient journeys to be considered from both Indigenous and Western world views, and from clinical, support and community perspectives.
This study focused on working with a number of staff participants, some of whom began working with the research team in earlier stages of the Managing Two Worlds Together project; several became involved in Stage 3 at the invitation of the research team or people already involved in the project; and others heard about the research and asked to be included. All involvement was voluntary.
Those staff participating in the study worked with the research team to modify and adapt the Aboriginal patient journey mapping tools to reflect the particular challenges faced by patients in their local settings, with some focusing on specific conditions and others on specific locations.
The specific conditions and settings were:
• Renal – Royal Adelaide Hospital, Port Augusta Hospital and Health Services, Country Health SA, Western Desert/Purple House Alice Springs (n = 6)
• Cardiac – Royal Adelaide Hospital, Flinders Medical Centre, The Queen Elizabeth Hospital, Alice Springs Hospital, Royal Darwin Hospital, NT Health (n = 10)
• Maternity – Flinders Medical Centre, Country Health SA, Aboriginal Family Birthing Project and Flinders University School of Nursing and Midwifery (n = 7).
Study Design and Methods
And the specific locations were:
• Rural and remote location-specific for all illnesses and conditions – Oak Valley, Tennant Creek, Port Augusta, Umoona Aged Care Coober Pedy (n = 8)
• City-based issues for specific Aboriginal client groups – The Queen Elizabeth Hospital, Lyell McEwin Hospital Emergency Department, Northern Adelaide Medicare Local – Close the Gap Team, Watto Purrunna Aboriginal Primary Health Care (n = 8).
Patient and community involvement
In Stage 1 of the MTWT project, the research team worked closely with patients, their families and community Elders to better understand individual and community experiences, which provided an important basis for the mapping tools. In this third stage the research team focused on how health and support staff and educators could adapt and use the tools and findings from Stage 1 to identify and address the journey gaps of the patients for whom they care.
As a result, in Stage 3 the research team did not work directly with patients and communities themselves; rather, they supported staff in each site to work closely with local patients and families as they modified and adapted the tools in their particular settings, using existing worksite confidentiality arrangements. The completed mapping tools and case study examples were then de-identified by staff before they were shared with the research team and included as part of the research project data. Diagram 2 shows the involvement of staff participants, patients and communities in Stage 3.

5
Diagram 2: Involvement of staff participants, patients and communities in Stage 3
Legend
Discussion between staff participants and patients and families
De-identified case studies
Existing worksite confidentiality arrangements
Central research
team
Renal nurses
Rural and remote
staff
City-based staff
Maternity staff
Cardiac staff
Cardiac patients and families
Renal patients and families
Local patients and community
Patients and families
Mothers, babies and
families

6
Some participants involved patients directly in the mapping process in significant ways. For example, Umoona Aged Care involved Elder women residents and board members in the process and approval of the final version of the tools, while the Queen Elizabeth Hospital Aboriginal Patient Pathway Officer worked closely with patients to map their extended journeys across multiple sites. In both of these situations, the patient undergoing the journey had significant control over what was included in the mapping and how it was presented. In addition, one Northern Territory Aboriginal health professional used the tools to map her own family member’s journey, and reported that it helped her to identify clearly the gaps in the system and led to discussions with staff as to how best to address these gaps.
Ethical considerations
Ethics approvals
Ethics approval was provided by the Aboriginal Health Research Ethics Committee (SA), Flinders University Social and Behavioural Research Ethics Committee, Human Research Ethics Committee (The Queen Elizabeth Hospital), Central Australian Human Research Ethics Committee, and Human Research Ethics Committee of Northern Territory Department of Health and Menzies School of Health Research. Site Specific Assessments were sought from The Queen Elizabeth Hospital, Royal Adelaide Hospital, Lyell McEwin Hospital, Flinders Medical Centre, Watto Purrunna Aboriginal Primary Health Care and Country Health SA. Support letters were received from managers of each health, support or education setting involved in the project.
Intellectual property
This research project was designed so that each staff participant and site involved in the research could develop and retain their own intellectual property. All were provided with the basic
Aboriginal patient journey mapping tool format, which they then adapted to suit their setting and needs. The resulting new localised version was held by staff and services for their continued use and recognised as their intellectual property. The research team recorded the process and result of each modification to build a picture of how the tools could be adapted to different health care and education sites. De-identified case studies were provided to the project for broader knowledge sharing, and these have been included as case study examples. Staff participants’ contact details are provided where possible, so that those wanting more information about the case studies can contact them directly. In some cases, staff are no longer in their positions due to completion of contracts or other role changes.
Confidentiality
Care was taken to ensure that the research team was given no patient identifying information, thereby maintaining confidentiality. Similarly, being staff, participants were guided by their existing workplace confidentiality and patient information sharing agreements. Patient details in case study examples were de-identified, unless it was the express wish of the person to tell their story openly and in its entirety. The Elder women in Umoona Aged Care, for example, have asked to be acknowledged in this way.
Consent
Each participant staff member was provided with written information about the project and their potential involvement prior to signing a consent form, and advised they could leave the project at any time: three left the study following changes in their work role or employment status.

7
The aim of the study is to develop, refine and evaluate the Aboriginal patient journey mapping tools for use in education and health care practice. The research questions that need to be answered are:
1. Can the Aboriginal patient journey mapping tools developed in the MTWT project be transformed for a range of settings for the following applications:
o quality improvement in patient journeys across health care settings and systems
o education and training?
2. What are the technical and practical requirements for these tools to be effective in various settings?
Planned outputs
1. A set of tools for reviewing actual patient journeys that will enable health care staff to assess the need for, and nature of, the required changes in the referral, transfer, coordination, liaison and support services for patients in their settings and clinical areas of care.
2. Education packages that consist of de-identified case study examples and explanations of how to use the Aboriginal PJM tools to map individual journeys and highlight the implications for care systems as a learning activity.
Developing the tools for Aboriginal patient journey mapping
During this study, the format of the tools was tested and adapted to suit a range of different priorities, patient journeys and locations. The ‘three table’ tool format of MTWT Stage 2 was expanded to include a three-stage process involving preparation, more comprehensive mapping and comparison to standards of care, and action on findings. It became
obvious during the study that one of the tools’ main strengths was that they could be adapted to suit local need. Although the underlying principles and prompt questions guided the use of the tools, the exact format and headings of the tables used for personalised journey mapping could be adjusted to more accurately reflect each journey and the focus each participant wished to emphasise.
An important phase in the development of the tools was to work closely with staff participants in each setting and then compare the effectiveness, and their experiences, of using the tools and the resulting (de-identified) case studies across the entire study. This enabled a collaborative identification of the changes needed to improve the ‘generic’ set of tools, and created an effective mechanism for sharing knowledge with all those involved in the study. For example, some of the details that Umoona Aged Care added to its tools were helpful for the renal nurses who were supporting clients with end-of-life journeys.
Participatory action research process
The research team used Participatory Action Research (PAR) to work with staff and adapt and trial the Aboriginal PJM tools. Repeated cycles of ‘Look and Listen’, ‘Think and Discuss’, and ‘Take Action’ (Kelly 2008) were enacted both at individual sites and across the project as a whole. This multi-layered, multi-site, knowledge exchange approach enabled both individualised development of the tools for each site as well as collaborative learning about their overall development across the entire project.
Working with other key stakeholders, programs and projects facilitated the further combination of evidence-based practice and practice-based evidence. As the project progressed, people not immediately involved in this study, but interested in mapping patient journeys, began using the tools and providing feedback. Their insights and experiences were also considered when developing the tools.
Research Aims, Questions and Principles

8
By the end of the study the process of mapping Aboriginal patient journeys consists of three main steps:
• Step 1: Preparing to map the patient journey
• Step 2: Using the tools
• Step 3: Taking action on the findings
The Patient Journey Mapping Process
Each step involves a number of tasks that were developed throughout the project by pulling together the experiences of staff participants involved in testing and using the Aboriginal PJM tools. Diagram 3 (below) provides an overview of these tasks.
It is important to note that in the Case Studies not all of the tasks described here are carried out fully in every case study. This is because the case study activities occurred before the final version of the tools and tasks were developed.
Diagram 3: The process of using the Aboriginal PJM tools – an overview
Step 1: Preparing to map the patient journey
Focus: How to prepare adequately prior to mapping patient journeys
Considerations
Task 1.1: Planning for mapping – who, what, when, where, why and how
Task 1.2: Guiding principles for respectful engagement and knowledge sharing
Step 2: Using the tools
Focus: How to map and analyse a patient journey
Data gathering
Task 2.1: Providing a narrative account of the journey (telling the story)
Task 2.2: Providing a visual map of the actual journey across locations
Task 2.3: Recognising the whole person experiencing the patient journey
Task 2.4: Considering the underlying factors that affect access and quality of care
Task 2.5: Bringing together multiple perspectives in chronological mapping
Task 2.6: Additional considerations for this patient journey mapping
Analysis
Task 2.7: Comparing this journey to particular standards of care and procedures
Task 2.8: Identifying key findings
Task 2.9: Reflecting on what was learned about patient journeys
and the mapping process
Focus: How to share findings and take action towards improving practices and policies
Knowledge translation
Task 3.1: Deciding how best to share the findings, with whom, and in what format
Planning and taking action
Task 3.2: Identifying actions at the personal and professional service and systems levels to improve patient care and the coordination of journeys
Step 1 Step 2
Step 3
Step 3: Taking action on the findings

9
Each of these three steps will now be explained in more detail.
Step 1: Preparing to map the patient journey
This step involves identifying the reasons for mapping patient journeys – the issue, problem or need, and which journeys to map and how. An important aspect of this step is the respectful engagement with both community members (people, patients, clients, family members, carers) and health service staff. The other is to become familiar with the tools and the underlying principles that guide their use.
Task 1.1: Planning for mapping – who, what, when, where, why and how
Ideally the person – patient, client, community member – or a family member would be involved in the mapping. If this is not possible, then involving staff or other people who worked closely with the person ensures the mapping can be more realistic and complete. It is important to avoid making assumptions about what happened for the person, how they felt, and what their priorities and concerns were.
There are a range of aspects to consider, including:
• Whose journey do you wish to map – which patients, locations, with what illness or injury?
• What is the issue, problem, need, trigger – what is the main/primary reason for mapping patient journeys?
• What aspects do you wish to highlight – e.g. discharge planning, cultural safety, follow-up, rehabilitation, transport costs?
• When will you be mapping the journeys, before or while they are happening (planning, referral) or after they have occurred (retrospective) – why and how will you do this?
• How will you conduct the mapping – face-to-face, interviews, with a range of people, or alone as a reflective practice exercise?
• Who will be involved in the mapping – patients/clients/community members, carers/family
members, staff, researchers, students, other key stakeholders?
• What do you envision doing with the results and who will you share them with – managers, peers, students, key stakeholders, community members, educators – and in what formats – reports, discussions, presentations?
• Which standards of care, policies, standards or key performance indicators could you compare the journey to and why – e.g. cardiac standards, cultural safety, clinical handover, timely follow-up, patient satisfaction, re-admission rates?
The answers to these questions help to work out what permissions will be required.
Task 1.2: Guiding principles for respectful engagement and knowledge sharing
We developed a set of underlying principles to guide the use of the tools. These are important because the way we use the tools and the way we interact with each other impacts on how people – patients, carers, staff, students, educators – experience the mapping process, and what our findings will be.
All collaborative activities in this project were guided by the following set of principles agreed upon by project participants, key stakeholders and the research team.
• Respectful engagement and knowledge sharing. Recognising the need for joint planning and decision making and supporting Indigenous and Western knowledges to come together to generate innovations and new ways of thinking and working together (Durie 2005; Echo-Hawke 2011; The Lowitja Institute 2014).
• A wider view of health. A comprehensive understanding of Aboriginal health as involving psychological, social, spiritual, cultural and physical aspects for a person and community (AIDA & CHETRE 2010).
• High standard of clinical care. Aboriginal people should have access to a high standard of clinical, specialist and biomedical care when required.
• Strengths based rather than deficit based. The strengths and abilities of the person undergoing the journey, and of the staff supporting them, are acknowledged (AHRC 2010).

10
• Person-/patient-centred care. Health care that is respectful of, and responsive to, the preferences, needs and values of the person and their experiences as they journey through multiple health system sites (ACSQHC 2014; AIHW 2014; Nguyen 2008; Picker Institute Europe 2013).
• Equity. Not everyone begins at the same starting point with the same resources available to them. Consideration of equity assists in understanding why some patients may require additional assistance to ensure the same health outcomes. The starting point and level of complexity for an Aboriginal person living in a remote community may be vastly different to that of a city-based patient (AHRC 2014).
• Cultural safety/competency. Health care is culturally safe if it is considered so by the recipients of care. Staff can begin enacting cultural safety by being aware of their own personal and professional cultures and that of the hospital and/or health system they work within, and how this impacts and/or meets the needs of individual patients (Browne & Varcoe 2006; Taylor & Guerin 2010).
• No blame, no shame. The focus needs to be on continuous quality improvement and problem solving rather than blame. The aim is to better understand the complexities of current situations and challenges in order to identify issues and gaps early and enact effective strategies, thereby preventing negative outcomes (Bailie et al. 2007). The tools were described by one remote area doctor as ‘like a root cause analysis but proactive’.
• Verify and avoid making assumptions. Obtain correct information about both patient/client priorities and needs, and other health staff and services, by talking with people directly to build and maintain relationships and a ‘no blame, no shame’ approach.
• Collaboration rather than competition. The project team and staff participants actively sought to work with existing programs and emerging projects (Nirrpurranydji, Fraser & Dhunupa 2012).
• Complexity principle. There are often multiple complexities occurring within and along the entire patient journey for patients, their families and health care professionals. This complexity is often predictable and, once identified, appropriate strategies and supports may be established (Dwyer et al. 2011).
• Systems-level approach. Often individual staff and services provide good care, but this is not always supported or coordinated across the entire health system. A focus on improving communication across, as well as within, health services is needed (Lawrence et al. 2009).
• Risk assessment and management. Once gap points and breaks in the patient journey and care pathway are identified, they need to be addressed to reduce the risk for subsequent journeys (Standards Australia 2009).
Co-researchers determined that is important to be respectful of different people’s perceptions and not to make assumptions or judgments. The tool is designed to assist people to work together to identify and solve problems, not to cast blame or cause hurt intentionally or unintentionally.
Step 2: Using the tools
The tools consist of nine tasks, which are detailed in Diagram 3 (p. 8). These tasks, the first six of which focus on data gathering and the last three on analysing the results, enable a person’s entire health journey to be mapped – from home to hospital to home. They centre on the person/patient experience and include family and staff support at each location. The tools, which map the involvement of Aboriginal-specific and mainstream health and support services, can be used and adapted for:
• any person in any location
• a planned, urgent or emergency event involving primary and hospital care
• rural/remote and urban settings.
It is important to note that some of the case study examples accompanying this report do not show all of the tasks, as the work occurred while the final tool format was still being developed. However, each case study was vital to the development of the mapping tools and process.
Task 2.1: Providing a narrative account of the journey (telling the story)
Following an individual’s story about their journey enables the uniqueness and complexity of each person’s experiences to be understood in the context in which it happened. Ideally, staff would work closely with the person involved to ensure their perspective is embedded within the narrative,

11
and to determine what aspects of their story can be told, and in what contexts. If a resulting case study is to be used outside the immediate health service, it is important to de-identify the story. A shortened example of a cardiac journey is provided below.
An Aboriginal person living in a remote community experienced increasing shortness of breath and a heavy chest on a Friday afternoon. Their family encouraged them to attend the local clinic and they were found to be having a myocardial infarction (heart attack) and were rapidly retrieved to Alice Springs and then Adelaide. Initial urgent treatment occurred at both hospitals, and then they had surgery.
There was no room for this person’s partner on the retrieval plane (RFDS/doctor plane) and so they followed by car to the nearest bus stop and then by bus to Alice Springs and Adelaide and then stayed in the hostel, visiting the hospital every day. There was no interpreter service for their first language available in Adelaide, and English was their third language. A telephone interpreter who spoke their second language was located for informed consent. Ongoing discussion and explanations were given in English, but some staff were too busy and spoke quickly, and the person and their partner also had difficulty understanding the doctor’s accent.
There was no Aboriginal hospital liaison or social work support available until the Monday. The hospital social worker assisted in arranging financial assistance so that the partner could afford to stay in Adelaide. The person had a relatively uncomplicated recovery and was flown back to Alice Springs, and then returned to their own community on the community bus. The Aboriginal Liaison Officer worked with the Rural Liaison Nurse to ensure that the partner could also travel home by plane. Their local health service provided follow-up care.
Task 2.2: Providing a visual map of the actual journey across locations
A visual map may be hand drawn or constructed using Microsoft Word ‘shapes’ or C Maps, of which there are a range of versions available. It tracks an individual’s journey across multiple geographic and health sites and can include distances travelled, where family and supports are located, and the staff and services involved. It may also be useful to map the season and time taken to complete the journey, as these can have significant implications both for the person/patient and the journey. There are various styles that can be used; one example is shown below.
Example Figure 1: Visual mapping
City hospitalPatient flown to city hospital
(2.5 hours)Patient flown to regional hospital
(30–60 minutes)
Both patient and partner return home by community bus
Both patient and partner flown back to Alice Springs
Home in remote
community
Hostel
Alice Springs Hospital
Local clinic
21 hours travel by bus6 hours travel by community bus
Car journey
Patient journey
Partner journey
Travelling together
Legend

12
Task 2.3: Recognising the whole person experiencing the patient journey
The first set of prompt questions (below), and the dimensions of health set out in Table 1, encourage staff to recognise the ‘whole person’ entering the journey. We found that these dimensions of health can only be identified in conversation with the person themselves, or the person’s family and carers. It is also crucial that staff do not make assumptions about what is important for the person/patient. Respectful consideration of these aspects can assist with improved patient-centred and culturally safe care. The physical/biological questions are purposely positioned last so that the whole person is considered, not just their health condition or injury. Repeatedly we found that
clinicians tended to focus on physical dimensions, and these are most often recorded in case notes.
Example answers to the prompt questions have been entered into Example Table 1.
Prompt questions include:
• Who is the person entering the journey?
• What is important for this person?
• What are this person’s family and community commitments?
• What changes for the person and the family when the person is transferred as a ‘patient’ to the city for health care?
• How is the person’s physical health?
Example Table 1: Dimensions of health
Dimension of health Situation
Local community City/regional hospital
Social and emotional wellbeing
Family and community commitments
Personal, spiritual and cultural considerations
Is a well-recognised and respected Elder in their community with a close extended family network
Has had a recent loss of a family member, and is caring for grandchildren
Is a member of the local council currently advocating with government for community improvements
Brother died of cardiac complications a year ago
Patient is worried about diagnosis and feels disconnected, lonely and undervalued in city setting, although this has been alleviated by the support of some staff and the arrival of their partner
Partner arrives after travelling by bus for two days
Patient has had both positive and uncomfortable interactions with staff, other patients and members of the public
Extended family are helping to care for the patient’s grandchildren
Patient is missing major decision-making meetings
Both patient and partner feel isolated and a long way from home and family
Physical and biological Diabetes for five years
New cardiac condition
Investigations have been carried out and new medications administered for patient’s acute cardiac condition
Task 2.4: Considering the underlying factors that affect access and quality of care
The second set of prompt questions (p. 13), and the underlying factors affecting a person’s health set out in Example Table 2, enable staff to take into account factors that may impact on access and quality of care for the person as a patient, as well
as factors that affect the family/community and the health services. Often it is useful to consider factors both in the home community and in the city hospital as well. If relevant, another column can be added to include regional hospital settings. In some settings, it may be more useful to identify factors for the individual patient, the family member and health services separately by using different colour text.

13
Example answers to the prompt questions have been entered into Example Table 2.
Prompt questions include:
• How long, and using what means, does the patient and family travel to access health care? Are there specific geographical, seasonal or road condition factors to consider?
• What is the impact of existing and new health concerns when the patient is at home, and also when the patient is in the city?
• What is the preferred language/s? Are interpreters required for informed consent? What languages do the health staff speak in each location? How clear is communication between the patient, family and staff in, and across, each location?
• What are the costs of accessing health care? Does the patient have the ability to pay or difficulty in paying? Are there additional supports available? Has the patient’s ability to work, access his/her bank, pay bills/rent/mortgage or make arrangements for family been affected? Have there been increased costs or decreased supports for accessing services?
• How does the patient feel about accessing health services? Does the patient or family/community have specific cultural or personal concerns or past experiences (e.g. have there been repeated one-way trips to the city for other community members)?
• Does the patient have specific preferences for how his/her health care is delivered and how major decisions are made (e.g. same gender provider for intimate care, discussing major surgery with their family etc.)?
Example Table 2: Underlying factors
Underlying factor Impact of location and access
Local health services City/regional hospital
Rural and remote/city
Travel to health care, environmental, proximity of family and support networks
Local health clinic and community centre within walking distance
Long distance to city – flight or extended bus trip
Impact of illness or injury
Chronic or complex conditions, being acutely ill or injured
Manages diabetes medications and diet
New medications and heart conditions require adjustments
Language and communication
Ease or difficulty of communication between patients and staff, access to interpreters, dentures, hearing devices
English is the patient’s third language
Staff in local clinic speak both the patient’s first language and English
No staff speak the patient’s first language
Particular difficulty understanding staff who also speak English as a second language
Interpreter needed for informed consent
Financial resources
Ability to meet costs of transport, treatment, health care, medications, inability to work, caring duties
Some costs covered by community arrangements
Financial stress of being in city, unable to access bank accounts easily
Need to purchase warm clothes
Additional accommodation costs for partner
There may be changes to financial assistance due to change in government policies
Cultural safety
Experiences of an Aboriginal person within a health system
Combines traditional and Western understanding of health and diabetes
New cardiac condition and Western interventions

14
Task 2.5: Bringing together multiple perspectives in chronological mapping
The third set of prompt questions, and the Multiple perspectives matrix set out in Example Table 3, enables the user to track the patient journey chronologically from the perspective of the person/patient, the family/carers, and health and support staff. Additional rows and columns can be added as required to focus on specific aspects such as timelines, discharge planning, best practice and clinical guidelines. When this table became more complex than the simplified example below – in the cardiac patient journeys, for example – staff used Excel spreadsheets to enable tracking across multiple columns.
Example answers to the prompt questions have been entered into Example Table 3.
Prompt questions include:
• What happened for the person, especially as he/she became a patient, across the entire journey? What happened for the family? What were the person’s priorities, commitments and concerns at each stage?
• What were the health care/health services priorities?
• Where are there service gaps?
• What responses to these gaps were available or added?
Example Table 3: Multiple perspectives
Perspective Patient history
Diagnosis/referral
Trip to city In hospital Discharge/transfer
Follow-up
Patient’s journey
Shortness of breath and heavy chest
ECG
Rapid referral to regional centre
Via RFDS to regional city for stabilisation then flight to Adelaide
Cardiac investigations and treatment
Fly back to regional city and then bus to remote community
Local clinic
No local cardiac rehab
Family/carer journey
Whole family worried about the patient’s health and wellbeing
No room on RFDS plane for partner
Partner followed by bus
Partner in hospital accommodation
Remaining family in contact via clinic phone
Wondering whether the partner can fly back as well – who will cover costs?
Support in community
Patient priorities, concerns and commitments
Being with family and community
To maintain wellness
Needing to arrange care of grandchildren at home
Understanding what is going on and what their choices are
Loneliness
Discharge information sent back to regional hospital and local clinic
Keep well
Health care/services priorities
Management of chronic condition – diabetes
Assess new health condition
Need tertiary hospital investigations
Investigate and treat condition
Need to get informed consent
Get patient and partner back home
Uncomplicated recovery
Service gaps No GP at local clinic
No room on plane for partner so had to follow by bus
Support for partner
No ALOs on weekends
Little support for partner to get home
No cardiac rehab locally
Responses to gaps
Ongoing chronic conditions support in local clinic
Good use of AHW and RAN skills and protocols
PATS assistance
Aboriginal Liaison Unit
Social work assistance
Aboriginal Land Council assisted with flight costs
Outreach service
Local clinic staff update skills

15
Once the table is complete, the overall patient journey, gaps and strategies become more obvious.
Prompt questions include:
• What was most significant for the person (what was the best and the worst thing/experience in the journey)?
• What strategies are in place and working well?
• What gaps were identified and how could these be addressed?
Task 2.6: Additional considerations for this patient journey mapping
The mapping process highlighted how, and which aspects of, care journeys and patient experiences were recorded and which were not. For example, case notes, particularly those from the hospital, focused on recording single episodes of care and were not useful for tracking the entire patient journey. This led to dangerous breakpoints in care between primary and hospital settings.
In addition, the underlying factors impacting on patients and their families and how they felt about their care are rarely mentioned in hospital case notes because these are not prioritised in clinical records.
In the case studies this meant that if the patient was not directly involved in the mapping process, and the staff members doing the mapping did not know the patient well, it was difficult to answer the prompt questions and fill out the first two tables about the whole person and the underlying factors impacting on their journey and care.
This discovery led to further discussions about what is and what is not recorded in case notes and shared during patient hand over or between health services. The challenge of providing care to meet individual and cultural needs (i.e. equity and cultural safety) when the focus is to ‘treat all people the same’ (i.e. equality) was often discussed as a result of mapping journeys. Staff who worked in coordination or support roles often provided insights of which other clinical staff were unaware.
Where required a table, or a model, can be added to document additional considerations that meet specific needs. For example, a renal nurse wished to map the discharge planning sequence that led to an early discharge and potentially dangerous gap in care (see Case Study B of the Renal Case Studies at: www.lowitja.org.au/lowitja-publishing). This is illustrated in Example Table 4: Additional considerations, which focuses on ‘Discharge planning and processes, the problems with late Friday discharges’.
Example Table 4: Additional considerations
Ward/unit/staff involvement
Date/day Time Reality/complexities Results/consequences
Renal ward
Clinical Services Coordinator
Friday Discharge plan is that this patient will go to Kanggawodli Aboriginal Hostel on Saturday and transfer home the following week
Coordinated transfer of care, with transport arrangements at Port Augusta available
Renal doctors Friday Need review by infectious diseases and cardio units prior to discharge
Probably unable to predict exact time of review and discharge
Pharmacy Friday Script filled, pharmacist telephoned and faxed Port Augusta late Friday re medication changes
Port Augusta Hospital was able to ensure new medications were available

16
Ward/unit/staff involvement
Date/day Time Reality/complexities Results/consequences
Infectious diseases
Echocardiogram (Echo)
Friday Echo takes a while – uncertain when this was booked
Review late Friday or Saturday – included the need for new antibiotics [unsure how was this communicated to Port Augusta – no documentation]
Delay in decision making and review
Cardio Saturday Review Echo Delay in decision making and review
Uncertain exactly who made this decision – possibly medical
Friday/Saturday
Arrangements made for discharge late Friday night, with return to Port Augusta on Saturday following dialysis (medical officer failed to notify all parties concerned)
Poor discharge planning, and poorly connected and supported journey home
Nurses on renal ward
Friday evening
Coordinate and manage complex discharge
After-hours minimal staff and resources
Multiple pressures, e.g., bed state on skeleton staff
Links in communication broken (staff unaware patient was for discharge home)
Aboriginal Liaison Officer
Friday night Not available after hours or weekends
Support unavailable
Rural Liaison Nurse
– Not available after hours or weekends
Support and coordination unavailable
Kanggawodli Aboriginal Hostel
– Very brief stay – late night to early morning
Minimal opportunity for hostel to be involved in coordination and preparing for transfer
City-based dialysis unit: Nurse and Registrar
Friday night Provide dialysis and transfer to bus station
Telephone Port Augusta Hospital and say she is on the 4.00pm bus
Miscommunication of travel time and assumptions made on how the woman could get from the bus to home
Port Augusta dialysis staff
Saturday morning
Dialysis staff working morning clinic received the call from city based dialysis unit that the woman was on her way to Port Augusta and could they arrange a taxi for her to get home
Dialysis chair arranged for Tuesday
No Aboriginal Health Service support staff available after Saturday morning
Port Augusta staff unable to contact the woman or her family, and so could not arrange to leave a taxi voucher for her
Example Table 4 cont...

17
Example Table 4 cont...
Ward/unit/staff involvement
Date/day Time Reality/complexities Results/consequences
Kanggawodli Aboriginal Hostel
Saturday morning
Hostel staff phone Port Augusta dialysis expressing concern as the woman did not seem lucid when she left them early in the morning
Port Augusta staff alerted of potential for disconnected journey and the woman being unwell
Port Augusta dialysis staff
Saturday morning
Port Augusta dialysis nurses telephone city dialysis unit to enquire if the woman’s blood sugar levels were stable, if she had eaten pre- and post-dialysis, and if she had money with her
Unable to elicit this information and the woman had already been taken to the bus depot
Port Augusta nurses decide they would meet the bus themselves in their own car to ensure the woman got home safely
They were unable to contact the woman or her family as they have no telephone number
Nurses met the 4.00pm and 9.00pm bus
Staff have no option but to meet each bus in their own car on Saturday afternoon and evening
Poor communication between sites
Underestimation of impact of the journey home for the woman, who possibly had no food, drink, money or escort for 9.5 hours while travelling
Having diabetes, being post-dialysis and post-infection, and on new medications – significant risk of hypoglycaemia or other complications
Renal CSC Plans for review regarding discharge of rural and remote patients
Changes in policy and practice to be strongly advised
Task 2.7: Comparing this journey to particular standards of care and procedures
The next task is to compare the case study to the relevant standards (policies, procedures, practices) of care, and then identify positive personal, professional, service and systems level actions that could improve patient journeys. Staff are encouraged to identify which standards are most relevant, such as:
• clinical handover
• culturally safe care
• cardiac clinical standards of care
• early discharge planning
• informed consent
• safe transition between services and geographical locations
• the provision of effective and timely follow-up care.
This enables the patient journey mapping to be considered within a quality improvement framework. Subsequent patient journeys can be compared to the same standards over time, which can lead to the identification of key gaps and the development, implementation and measurement of policy and practice responses.
One way of communicating the results of all this is to display the trajectory of patient journeys, the opportunities for positive health and support service intervention, and the patient care outcomes that result. Adding the actual patient journey narratives makes this a strong method of knowledge

18
exchange as it combines visual representation, storytelling, logic and quality standards.
In Example Figure 2, the results of three actual (de-identified) journeys were presented to managers and services to highlight the importance of
timely and coordinated staff, service and system response. The vertical arrows indicate opportunities both for positive interactions and responses. Each arrow can be numbered and a detailed description of the opportunity and intervention given.
Example Figure 2: Comparison of three different patient journeys to standards of care
Patient journeys and outcomes depending on journey risk and system response
Systems response, risk and standards of care
-
Low
risk
, with
in
stan
dard
M
ediu
m ri
sk,
outs
ide
of s
tand
ard
Ris
k/S
tand
ard
Hig
h ris
k,
unac
cept
able
dis
tanc
e fro
m s
tand
ard
Poor
Good
Legend
Patient 1 journey
Patient 2 journey, with good outcomes
Patient 2 journey, with poor outcomes
Patient 3 journey with severe outcomes
Positive interaction and system response changes trajectory, improves outcome
System response
Little or no progress, patient feels like they are going around in circles
Outcomes
Primary health care Primary health careHospital
+
Severe or death

19
Patient 1 journey in Example Figure 2 is near to ideal with few complexities. This may represent the journey of a person who lives near the city hospital, and has both personal and health care resources nearby. As a result, the journey is reasonably uneventful and variations in care are not far from the standard so only have a minor impact on health outcomes and experiences.
Patient 2 journey reflects an experience with some unaddressed complexities. However, if specific measures are put in place, this care journey can move from being moderately far from acceptable to a standard of care that only moderately impacts on a patient’s outcomes. If services and supports are provided at key moments, this person can experience positive health outcomes, but if there is no response, or not timely response, their experiences and outcomes will be much poorer.
Patient 3 journey has many unaddressed complexities and at times seems to be going in circles or backwards. It veers dangerously far from the standard, and the patient’s experiences and outcomes are significantly compromised by a lack of resources or gaps in care.
To illustrate this comparison more clearly, three representative cardiac patient journeys – de-identified actual patient experiences – are presented below. In cardiac care, there exist clear standards relating to the timing of assessment, electrocardiogram (ECG) and medication so as to prevent a worsening of a patient’s condition. Distance and remoteness add to complexity, but if appropriate protocols and procedures are in place, the impact of remoteness on care outcomes can be reduced. In the following examples, we consider variations that may occur for patients, family and staff in a cardiac patient journey – from uncomplicated to very complicated.
Patient 1 journey – relatively uncomplicated, near ideal
An Aboriginal person living in the suburbs and working in a city office in Adelaide experiences chest pains and shortness of breath, indicating a possible heart attack. Their colleague calls 000 and within minutes an ambulance arrives and they are taken to a city hospital for assessment, investigation and treatment. They also have a split lip and staff assume (correctly) that it was through sport or a similar activity. The person can clearly understand what the doctor, nurses and investigation staff are saying, and informed consent is uncomplicated. Family are close by and are at the hospital within the hour, and work colleagues also visit during the
hospital stay, providing emotional and social support. This person’s care and recovery are personally distressing, but relatively uneventful. They return for follow-up visits and cardiac rehabilitation, and negotiate a return-to-work plan. They have the blue line patient journey.
Patient 2 journey – moderately complex journey, good systems response
An Aboriginal person living in a remote community experiences chest pains and shortness of breath, indicating a possible heart attack on a Friday afternoon. They walk the short distance across to the remote clinic to see the health worker and nurse. They also have a split lip from a vigorous game of sport the day before. The health worker greets them, asks what is wrong and quickly gets the nurse. An assessment and ECG is done and a cardiac cause is identified. The nurse rings the designated doctor, begins appropriate medical treatment, including anti-clotting medication (thrombolysis), and the RFDS plane is diverted from another case and sent to this community immediately. The nurse notes the split lip and its cause on the transfer letter, knowing that wrong assumptions could be made further along the care journey, and applies some healing cream.
The person is flown to the nearest regional hospital, stabilised and transferred by air to an Adelaide city hospital. Family members are unable to accompany them as there is no room on the RFDS plane. A bilingual worker in the regional hospital and an interpreter in the city hospital explain what is happening and the person is able to give informed consent for investigations and treatment. In the city hospital an Aboriginal Liaison Officer visits and a phone is made available so they can talk to family.
Their return journey to the regional hospital and remote community is well coordinated. Staff in the city and in the regional hospital ensure that the person has enough medications and that the discharge letter is accessible to each health carer they see on their journey home. On their return home, the local clinic provides ongoing care and modified cardiac rehabilitation. Early administration of appropriate medication and treatment mean that although they began their journey in a remote location, their outcome is within ideal standards of cardiac care. Good communication, coordination and collaboration of care throughout the journey lessened the impact of distance, language and cultural differences.

20
Patient 3 journey – very complex journey with limited systems response
An Aboriginal person living in a regional town experiences chest pains and shortness of breath, indicating a possible heart attack on a Friday afternoon. They are at home alone without a car, don’t have ambulance cover, and can’t afford a taxi. As a result, they ring around to find a family member with a car to come and pick them up and take them to the hospital across town. By the time they get to hospital they are feeling most unwell and agitated, and the staff member on duty seems slow to respond to their concerns. The person also has a split lip, from a recent vigorous game of sport, and the staff member assumes they have been fighting and fears for their own safety.
The person begins to feel nauseous and dizzy, and the staff member wonders if they have been drinking. The family member is getting increasingly concerned and loudly demands that the staff member do something. The staff member interprets this as a threat of violence and calls security. An Aboriginal worker alerted by the coded message also attends, and together with the security officer assess the situation. They ask the person and their family member what is happening and quickly determine the seriousness of the symptoms, and relay this to the clinical staff. They reassure the patient and family member that something will be done. With additional staff on site, the person is assessed, an ECG is done, a doctor is called and they are given appropriate medications, although not within the ideal timeframe. They are stabilised and then transferred to a city hospital via ambulance. Their transfer notes contain the original assessment that they had been fighting, drinking and were violent. In the ambulance they become agitated and claustrophobic and take off the oxygen mask. The ambulance officer notes in the transfer document that they are also non-compliant.
The patient arrives in the city hospital on a Friday evening for further investigations and treatment. A family member catches the next available bus and arrives early the next morning. There is no support or Aboriginal staff available on the weekend for either the person or their family member. As English is their second language, they don’t understand the detailed clinical information being given. They can understand some aspects when staff take time to explain things clearly, although some staff seem reluctant to do so. No interpreter is offered and they do not see an Aboriginal
Liaison Officer until the last day of their stay. Due to the delay in their initial access, assessment and treatment, their cardiac care is more complicated and they have to stay longer.
At discharge they are given a week’s supply of medication, the discharge letter is sent to the hospital which referred them, and they are advised to stay in the city a few days before travelling home. They make arrangements to stay with family, as the Aboriginal hostels are all full. They then return to their regional town on the bus, which gets in late Friday night, and a family member picks them up. The next day their discharge medications run out, but they don’t want to go back to the local hospital, so they wait until Monday to go to the Aboriginal health clinic. By this time, they are feeling unwell again. The clinic staff quickly re-assess them and assist with medication after tracking down their discharge letter from the city hospital. They encourage regular visits and provide cardiac rehabilitation including a follow-up appointment with the visiting cardiologist. A worker accompanies them for support and to interpret any information.
This person’s journey has large fluctuating variations, many of which are attributable to access barriers, negative assumptions and stereotypes, and significant gaps in care. Although key opportunities for communication, coordination and collaboration were missed, instances of good care and support were still able to improve both the patient experiences and their health care outcomes.
These three journeys are representative of the many stories we have heard and assessed. It is important to note that:
• remoteness does not automatically lead to a highly complex journey if good systems and supports are in place
• many Aboriginal people receive very good care in regional centres
• all three people in these cardiac journeys, and their families, would have experienced high levels of anxiety and worry that come with any cardiac or other life-threatening event
• in some instances, based on past experience, staff members may have also felt unsupported and concerned.
These examples also convey the importance of ensuring cultural safety and highlight the unintended impact of racism and assumptions on care experiences and outcomes. They emphasise,

21
too, the need for transfer of care rather than discharge, and the way that small actions in a city hospital can have significant implications on the entire patient journey and follow-up (such as the limited supply of discharge drugs and no discharge letter). There is also another kind of journey that occurs too often, in which the person dies as a result of illness or injury, and/or because of miscommunication, lack of access to medical care and inadequate resources.
Task 2.8: Identifying the key findings
In this task, staff participants are encouraged to identify the key findings most relevant to their purpose for taking part in the mapping exercise; these may include the main gaps and strategies. For example, in the scenarios above a key finding is that no matter where in Australia a cardiac event occurs, there is now immediate thrombolysis available, which is leading to improved health outcomes for all Australians regardless of geographic location. Another finding may be that although there is improved clinical responsiveness with protocols and medication availability, a lack of access due to financial and transport difficulties and/or a communication breakdown may result in delayed care and treatment.
Task 2.9: Reflecting on what was learned about patient journeys and the mapping process
The experiences of the Renal Focus Group and the Cardiac Focus Groups are useful examples of this task in action.
The challenge of incorporating research into clinical practice – or finding the timeThe Renal Focus Group consisted of senior nurse clinicians, educators and coordinators from South Australia and parts of the Northern Territory who worked collaboratively via teleconferences. They also focused individually on a specific aspect of the patient journey mapping that was occurring in their clinical practice. Together the group shared challenges and devised strategies and ensured that new knowledge was embedded in ongoing staff and student education. In the final evaluation discussion they reported that, although they struggled to find time to do this work within their busy clinical roles, they highly valued the teleconferences and collaboratively mapping journeys and problem solving. All are committed to continuing the work into 2014 and beyond.
The two Cardiac Focus Groups were formed in Darwin and Alice Springs, with ongoing work
continuing with cardiac coordinators in Adelaide. Those involved in half-day workshops/focus groups reported that the tools were useful in identifying specific gaps in care, and tracking patient journeys across a myriad of health services. They also saw value in comparing results with cardiac standards. One remote area physician described the tools and mapping process as a proactive means of establishing a root cause analysis with the potential to identify issues and gaps before an adverse incident occurred. A Northern Territory health manager supported the ongoing use of the tools for quality improvement and service planning.
In both Darwin and Alice Springs focus group participants found it difficult to provide information for the first two tables (Dimensions of health and Underlying factors) when no one had worked directly with the patient, because this information is not routinely recorded in case notes. The inclusion of primary care and support staff from across the entire patient journey assisted in discussions as to the wider complexities of cardiac patient journeys. The work with cardiac coordinators is continuing into 2014/15 with a Heart Foundation Focus Grant.
Step 3: Taking action on the findings
Once the mapping is complete, the next step is to decide how best to share the findings and what action needs to be taken, by whom and when.
Task 3.1: Deciding how best to share the findings, with whom, and in what format
Findings may be shared with colleagues, integrated into training, taken to a service, unit or specific meeting, or used for reflective practice. Both strengths and gaps in care can be communicated, ensuring that good practice is recognised and that gaps are addressed.
Prompt questions include:
• Who do you wish to convey the results to?
• What actions or changes do you think may need to occur?
• What has become obvious to you now that wasn’t obvious before, or what was confirmed for you?
Some examples from the case studies include the renal nurses who incorporated their findings into the revised renal education package, and also shared

22
findings at a Renal Society of Australasia seminar. A cardiac coordinator developed a staff education package to share the findings with colleagues. An Aboriginal Patient Pathway Officer shared a case study and findings at a health care forum. Umoona Aged Care used its patient journey mapping to discuss budget implications at a board meeting.
Task 3.2: Identifying actions at personal, professional, local service and systems levels to improve patient care and coordination of journeys
The next task involves making an action plan, which is set out in Example Table 5, with dates for reviewing progress. Action planning may occur at multiple levels for increased impact.
• Personal – are there immediate actions for the patient, the family, community or health staff members involved?
• Professional – are there changes, education, training required for any specific professional group? For example, renal nurses in a dialysis service, registrars discharging patients to remote areas, new Aboriginal coordinator positions?
• Service/agency/unit – are there policy, procedural or other changes needed? For example, earlier and more comprehensive discharge planning or an increased use of interpreters?
• System – what needs to change or be strengthened across the health system and between agencies? For example, clinical handover between primary and tertiary care, transfer of care arrangements that provide improved continuity of care, interstate sharing of health care resources in remote areas?
It is worth considering who has the interest, influence and ability to implement change. A concise way to record planning and actions is to use an action plan table. This is particularly useful for work-based and quality improvement processes, and can be continually revised and updated, with different versions and dates recorded.
In the case studies, actions included sharing results with community members or colleagues, discussing results at meetings, advocating for policy or practice changes, and making recommendations. In some cases a simple action plan, as shown in Example Table 5, was developed.
Example Table 5: Action plan
Issue Level Action required
By whom When How Review date
Action taken
Improved communication and cultural safety
Personal Personal commitment
All staff This year
Reflect on interactions
Nov. 2014 Individual reflection
Professional Reflective practice
Nurses, doctors, allied health professionals
This year
Professional development
Nov. 2014 Included in annual review process
Local service
Cultural safety and communication training
Unit manager to arrange
Within 6 months
External facilitator
July 2014 Workshop held June 2014
System Evaluate effectiveness and implementation of policies
Executive representative
Within 12 months
Review complaints, patient outcomes, policy implementation
Dec. 2014 Sub committee formed
Action plan prepared by ______________________________________ On / /

23
Staff participants used the tools in diverse ways for a range of purposes including:
• the mapping of recent actual patient journeys (case studies) for quality improvement, team debriefing, reflective practice, information sharing, education and training
• to highlight a specific issue and provide practice-based evidence
• to test whether new policies or practices were effective, or to review existing policies and practices
• for service planning – to predict potential problems and support action to avoid building them in
• as a proactive root cause analysis – identifying and investigating problems before they result in adverse patient events.
Case Studies are available as part of the study outcomes at: www.lowitja.org.au/lowitja-publishing. These provide detailed information about the location, intention, adaptation of the tools, resulting tools format and experiences of the participants.
Best use of the tools
Originally the research team anticipated that the tools could be engineered into a specific electronic version that would be used to plan patient journeys. However, participants were concerned that many staff were already struggling with the introduction of a new electronic system in some hospitals and could be loath to learn to use a new piece of software. The feedback was that they would prefer a Microsoft Word or Excel version that could be easily adapted and shared with colleagues via email. However, when considering the workbook format, we decided upon a writable PDF as the most appropriate option as the majority of Word users are
also familiar with using PDFs. In addition, the format of a writable PDF should assist busy practitioners to produce a well-presented report relatively easily.
Other feedback found that the tools were too complex to use in day-to-day practice. Instead their value lay in reflective practice, risk mitigation, quality improvement, education and planning – particularly for complex patient journeys.
These insights led the research team to consider the relationship between these tools and the many electronic and manual systems already in use to record and track aspects of care (such as laboratory results and discharge planning) in health care agencies. We decided that the tools would be best used for learning and improvement purposes, rather than as part of routine care delivery. It also became clear that one likely result of using them would be an indication of the need for change in those systems that are used routinely.
What makes these tools unique?
We are not aware of any equivalent tools that enable the mapping of the entire patient journey across multiple settings, modes, times and places for a diverse range of admissions and health interactions. The tools can be adapted for use with any client group with only slight amendments to Table 1: Dimensions of health.
These tools are inherently adaptable and flexible; they have a global format with local adaptations. The unchanged elements are the core principles underlying the use of the tools. There is no additional cost or training required to use them, as most staff are already familiar with Word and/or Excel.
Reflection and Evaluation of How the Tools Were Used in this Study

24
Evaluation, knowledge exchange and dissemination of findings
Evaluation of this study was conducted through:
• recording PAR processes at each site – describing how each person and group adapted and used the tools, and shared the knowledge within their site and with the study
• examining the evaluation forms provided to participants to complete anonymously
• conducting a roundtable workshop and discussions involving all participants, research team members, key stakeholders and funders.
Across the entire study participants favoured a flexible and easily applied Word or Excel version of the tools. This was in preference to a centrally structured electronic version that might not have been compatible with all computer systems, and would have required them to receive specific training. There was also agreement that the most useful outcomes would be the production of a mapping tools workbook/user guide with prompt questions, and a set of case study examples of how the tools could be adapted and used in practice. These evaluations guided the end products of the study.
This study involved significant collaborations across a number of health and education sites and professions. Participants agreed that the collaboration and the sharing of knowledge, draft tools and strategies across the entire study enabled a more relevant set of tools to be developed.
Facilitating knowledge exchange and disseminating findings was a priority of this study and occurred at multiple levels and in many forms. Staff participants shared the tools, experiences and their findings with colleagues and peers – with some presenting at forums, meetings and special interest groups. Dr Janet Kelly became the conduit between each participant, and between participants and the research team, sharing emerging ideas and adapting the tools and processes to meet individual and general needs. She also discussed the tools and the patient journey mapping concepts with a range of key stakeholders, service providers, researchers and project workers, thereby enabling
new insights to be incorporated. Staff from other States and services became interested in the tools and mapping processes, with some adapting and trialling the tools at their own sites.
The research team used a range of dissemination strategies to share the finding of the study. They were involved in planning and co-facilitating sessions within a forum run by the South Australian Aboriginal Health Partnership entitled ‘Working Better Together to Improve the Patient Journey’. This forum brought together managers from key areas of the health sector, including the Australian Government Department of Health and Ageing (now the Department of Health), the SA Department for Health and Ageing, Local Health Networks, Medicare Locals and Aboriginal Community Controlled Health Services. The research team also presented at national continuous quality improvement, public health and research conferences, State research network meetings, an international health services research conference and public forums, and to nursing, medical, midwifery and health care management students.
Study challenges
A range of challenges occurred during the study; some prevented the research progressing as it was originally intended, while others led to new opportunities.
Most participants were extremely busy health professionals, managers and coordinators for whom prioritising research was difficult. We worked flexibly with each participant, at a time and location most convenient for them, using face-to-face, telephone and email contact as preferred.
Some of the participants who began working on the tools had short-term funding or position changes that meant they were unable to continue on the study. This was particularly evident with Aboriginal Patient Pathway Officers, Aboriginal Maternal Infant Care Workers and Midwives, Aboriginal Health Workers, Aboriginal Hospital Liaison staff and remote area workers. Two remote area sites discontinued involvement in the study when key staff contracts ended.

25
This study builds on earlier work (Dwyer et al. 2011) in which we found that the differing levels of communication, collaboration and coordination within and between various health care and support services greatly impacts on Aboriginal patient journeys, experiences and outcomes. If individual staff, wards, units and services, and electronic systems are not able to communicate effectively with each other, there is a risk of assumptions being made about what is available and occurring in other sites.
In this study we again found that many care journeys were particularly complex and challenging not only for the Aboriginal person experiencing them, but also for the family and the staff members assisting in various health and support services. There was a sense that both patients and staff were sometimes overwhelmed by the number of factors that might at any stage render care unworkable. Using the tools to map the entire patient journey in a structured and organised way enabled the apparent chaos to become manageable in three ways.
1. Makes the complex patient journey visible.
Following a patient’s journey through a series of health care silos dotted across the health care and geographic landscape, rather than viewing it only from the perspective of each health care professional or location, highlights the complexity of the entire journey. The multiple perspectives matrix enables staff to see where they sit within the person’s health care journey, and who they need to communicate and collaborate with before and after their own involvement in the patient’s journey, and what additional services or considerations may be required.
2. Organises the journey for analysis and response.
The mapping process highlights the many sectors and settings involved: primary/secondary/tertiary; city/rural/remote; public/private; Aboriginal-specific/mainstream; prevention/planned/emergency; acute/chronic; health care/support services. The tools enable health care providers to focus on the gaps and responses in a single journey, and
Conclusion
then apply the findings more broadly using quality improvement and staff education.
3. Enables the critical steps, gaps and responses to be highlighted, thus providing a focus for targeted action by health care providers.
The tools enable local solutions for wider systemic problems, as well as emphasising particular patient risks that require organisational, policy and procedural changes. The tools highlight critical aspects and break points that need to be addressed; for example:
• usually no single person or service is responsible for coordinating the entire patient journey
• because of this patients are left vulnerable during transfer or discharge from one service to another
• these transition points can be dangerous, particularly for patients with communication difficulties or high-care needs
• communication, coordination and collaboration are key aspects to successful journeys and a continuity of care.
The mapping process highlighted how and which aspects of care journeys and patient experiences were recorded, and which were not. For example, case notes, particularly hospital case notes, focused on recording single episodes of care and were not useful for tracking the entire patient journey. This led to dangerous breakpoints in care between primary and hospital care.
Furthermore, the underlying factors impacting on Aboriginal patients and their families, and how patients felt about their care, were rarely mentioned in hospital case notes because they are not a priority in clinical records. This meant that if the patient was not directly involved in the mapping process, and the staff doing the mapping did not know the patient well, it became difficult for them to answer the prompt questions and for staff to fill out the first two tables (Dimensions of health and Underlying factors). This discovery led to further discussions about what is and what is not recorded

26
in case notes, and what is shared during hand over or between health services.
The challenge of providing care to meet individual and cultural needs (equity and cultural safety) – when the focus is to ‘treat all people the same’ (equality) – was often discussed as a result of mapping Aboriginal patient journeys in this way. Interestingly, staff who worked in coordination or support roles often provided insights and implications of which other clinical staff were unaware.
Where to from here?
Work is continuing on improving Aboriginal and other patient journeys with participants and key stakeholders. A Heart Foundation Focus Grant is enabling continued and more detailed mapping of cardiac patient journeys across the Northern Territory that involve patients, families
and communities, cardiac coordinators, and primary and hospital staff. The Renal Focus Group is continuing its work in South Australia and the Northern Territory by focusing on how best to support end-of-life journeys, particularly for those wishing to return to remote communities. Midwives are using the tools to highlight specific issues for Aboriginal mothers and their families, with educators incorporating the tools into training courses. Patient journeys and the mapping tools are also increasingly being introduced into nursing, medical and health care management training in a range of health care sites and tertiary institutions. Researchers and students are also incorporating the Aboriginal PJM methodology into their projects.
We perceive that there is a growing interest in improving communication and continuity of care across health care systems within Australia and internationally. These tools provide a practical approach toward achieving this – both for Aboriginal patients and their families specifically and for all people accessing health care generally.

27
Australian Commission on Safety and Quality in Health Care (ACSQHC) 2014, Patient and Consumer Centred Care, ACSQHC, Canberra. Accessed 20 June 2014 at: www.safetyandquality.gov.au/our-work/patient-and-consumer-centred-care.
Australian Human Rights Commission (AHRC) 2010, Social Justice and Aboriginal and Torres Strait Islander Peoples Access to Services, AHRC, Canberra. Accessed 26 May 2014 at: www.humanrights.gov.au/news/speeches/social-justice-and-aboriginal-and-torres-strait-islander-peoples-access-services-2010.
Australian Human Rights Commission 2014, Close the Gap: Indigenous Health Campaign, AHRC, Canberra. Accessed 10 May 2014 at: www.humanrights.gov.au/close-gap-indigenous-health-campaign.
Australian Indigenous Doctors’ Association (AIDA) & Centre for Health Equity Training, Research and Evaluation (CHETRE) 2010, Health Impact Assessment of the Northern Territory Emergency Response, AIDA and CHETRE (UNSW), Canberra.
Australian Institute of Health and Welfare (AIHW) 2014, The Measurement of Patient Experience in non-GP Primary Health Care Settings, AIHW, Canberra.
Bailie, R., Si, D., O’Donoghue, L. & Dowden, M. 2007, ‘Indigenous Health: Effective and sustainable health services through continuous quality improvement’, Medical Journal of Australia, vol. 186, no. 10, pp. 525–7.
Browne, A. J. & Varcoe, C. 2006, ‘Critical Cultural Perspectives and Health Care Involving Aboriginal Peoples’, Contemporary Nurse, vol. 22, no. 2, pp. 155–67.
Cass, A., Lowell, A., Christie, M., Snelling, P., Flack, M., Marrngnanjin, B. & Brown, I. 2002, ‘Sharing the True Stories: Improving communication between Aboriginal patients and healthcare workers’, Medical Journal of Australia, vol. 176, May, pp. 446–70.
Durie, M. 2005, ‘Indigenous Knowledge within a Global Knowledge System’, Higher Education Policy, vol. 18, pp. 301–12.
References
Dwyer, J., Kelly, J., Willis, E., Glover, J., Mackean, T., Pekarsky, B. & Battersby, M. 2011, Managing Two Worlds Together: City Hospital Care for Country Aboriginal People—Project Report, The Lowitja Institute, Melbourne.
Echo-Hawke, H. 2011, ‘Indigenous Communities and Evidence Building’, Journal of Psychoactive Drugs, vol. 43, no. 4, pp. 269–75.
Kelly, J. 2009, Moving Forward Together in Aboriginal Women’s Health, unpub. PhD thesis, School of Nursing and Midwifery, Flinders University, Adelaide.
Kelly, J., Dwyer, J., Pekarsky, B., Mackean, T., Willis, E., Battersby, M. & Glover, J. 2012, Managing Two Worlds Together: Stage 2—Patient Journey Mapping Tools, The Lowitja Institute, Melbourne.
Lawrence, M., Dodd, Z., Mohor, S., Dunn, S., de Crespigny, C., Power, C. & Mackean, L. 2009, Improving the Patient Journey, Cooperative Research Centre for Aboriginal Health, Darwin.
Nirrpurranydji, S., Fraser, J. & Dhunupa, Dhwu 2012, Enhancing Strengths, Researching with the Community, The Lowitja Institute, Melbourne. Accessed 10 May 2014 at: www.lowitja.org.au/dhunupa-dhwu-enhancing-strengths-researching-community.
Nguyen, H. T. 2008, ‘Patient Centred Care: Cultural safety in Indigenous health’, Australian Family Physician, vol. 37, no. 12, pp. 990–4.
Picker Institute Europe 2013, Patient & Service User Experience Surveys, Oxford. Accessed 20 June 2014 at: www.pickereurope.org/adult-and-patient-service-user-surveys.
Standards Australia 2009, AS/NZS ISO 31000:2009 Risk Management— Principles and Guidelines, Council of Standards Australia. Accessed 31 May 2014 at: http://sherq.org/31000.pdf.
Taylor, K. & Guerin, P. 2010, Health Care and Indigenous Australians: Cultural Safety in Practice, Palgrave Macmillan, Melbourne.
The Lowitja Institute 2014, ‘Knowledge Exchange’. Accessed 6 August 2014 at: www.lowitja.org.au/knowledge-exchange.

28


30

31
About the Authors
Janet Kelly
Study Leader, Improving Aboriginal Patient Journeys Study and Research Fellow, Flinders University, and Research Fellow, School of Nursing, University of Adelaide and Heart Foundation
Judith Dwyer
Project Leader, Managing Two Worlds Together Project and Professor, Health Care Management, Flinders University
Brita Pekarsky
Health Economist, Flinders University and South Australian Health and Medical Research Institute
Tamara Mackean
Senior Research Fellow, Poche Centre for Indigenous Health and Wellbeing, Flinders University
Eileen Willis
Deputy Executive Dean, Faculty of Medicine, Nursing and Health Sciences, Flinders University
Charlotte de Crespigny
Professor of Drug and Alcohol Nursing, School of Nursing, University of Adelaide
Sharon Perkins
Aboriginal Services Manager, Country Health SA Local Health Network
Kim O’Donnell
Research Associate, Health Care Management, Flinders University, and Teacher, Aboriginal Health Council of South Australia
Rosie King
Senior Research and Ethics Officer, Aboriginal Health Council of South Australia
Laney Mackean
Manager, Karpa Ngarrattendi Aboriginal Health Unit, Flinders Medical Centre
Alex Brown
Aboriginal Research Program Leader, Deputy Director, South Australian Health and Medical Research Institute – SAHMRI, and Professor of Population Health and Research Chair Aboriginal Health, School of Population Health, University of South Australia
Monica Lawrence
Senior Lecturer Indigenous Health, Poche Centre, Flinders University, previously Acting Regional Manager, Aboriginal Family Clinic, Southern Adelaide Local Health Network
Karen Dixon
Clinical Lead Country, EPAS Program, SA Health

The Lowitja Institute PO Box 650, Carlton SouthVic. 3053 AUSTRALIAT: +61 3 8341 5555 F: +61 3 8341 5599 E: [email protected]: www.lowitja.org.au













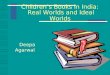

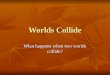





![Cambridge IGCSE Biology - Mackean, D. G [SRG].pdf](https://img.pdfslide.us/doc/110x75/563dbb6f550346aa9aad23a7/cambridge-igcse-biology-mackean-d-g-srgpdf.jpg)