Embed Size (px)
Citation preview
30 Am J Geriatr Psychiatry 12:1, January-February 2004
Managing Suicide Risk in Late Life
Access to Firearms as a Public Health Risk
David W. Oslin, M.D., Cynthia Zubritsky, Ph.D.Greg Brown, Ph.D., Marian Mullahy, M.S.S.Anthony Puliafico, Thomas Ten Have, Ph.D.
Objective: The authors assessed the prevalence of gun availability for elderly patientsto determine whether gun availability is related to the presence of suicidal or depres-sive symptoms. Methods: This is a cross-sectional epidemiologic survey of firearmavailability and safety practices. A random sample of older adults with a scheduledprimary-care clinic appointment was selected and screened with the General HealthQuestionnaire and questions about suicidality and alcohol use. Participants were alsoasked about the availability of firearms in their home and about safe gun practices.Results: Of 1,023 patients screened, 285 (27.9%) reported having some type of firearmin the home, and 202 (19.7%) reported having a handgun in the home. Patients withsuicidal ideation or high levels of depression or psychological distress were not sig-nificantly more or less likely to have a gun in the home than those without theseemotional stressors. The strongest predictors of firearm availability were being maleand being married. Conclusions: These preliminary data suggest that a significantproportion of elderly people have firearms available to them in their homes. Thosepatients with emotional distress did not differ from those without distress with respectto having firearms available to them. These data strongly suggest the need for screen-ing for firearm availability and education about the safe storage of firearms as apotential means of prevention of suicide among elderly patients suffering from emo-tional distress or suicidal ideation. (Am J Geriatr Psychiatry 2004; 12:30–36)
Received September 15, 2002; revised November 15, 2002, February 5, 2003; accepted February 11, 2003. From the Section on GeriatricPsychiatry,Department of Psychiatry, University of Pennsylvania, Philadelphia, PA (DWO,GB,AP), the Center for the Study of Addictions, Department ofPsychiatry, University of Pennsylvania, Philadelphia, PA (DWO), the Philadelphia VA Medical Center, VISN 4 MIREECC (DWO), the Center forMental Health Care Policy and Services Research, Department of Psychiatry, University of Pennsylvania, Philadelphia, PA (CZ,MM), and theDepartment of Epidemiology and Biostatistics, University of Pennsylvania, Philadelphia, PA (TTH). Send correspondence to David Oslin, M.D.,University of Pennsylvania, 3600 Chestnut Street, Room 790, Philadelphia, PA 19104. e-mail: [email protected]
Copyright � 2004 American Association for Geriatric Psychiatry
According to suicide data from the Center for Dis-ease Control and Prevention’s National Center
for Health Statistics, white men over the age of 65 aremore likely to commit suicide than those in other age-groups.1 Approximately 20% of all suicides in theUnited States occur in elderly persons, although these
people constitute only 10% of the general population.Among elderly persons, the most significant risk fac-tor associated with suicide is the presence of a mentalhealth problem, especially a depressive disorder.2,3
The proportion of elderly patients committing suicidewho have a mental illness is over 90%.4 Limited social

Oslin et al.
Am J Geriatr Psychiatry 12:1, January-February 2004 31
support and depressive symptoms, especially moresevere symptoms or depression comorbid with anxi-ety, and have also been demonstrated to be associatedwith both death ideation or passive suicidal ideationin elderly persons.5 Thus, depression, in particular, isa salient risk factor for suicide as well as a potentialtarget of intervention for preventing suicide.
Methods for committing suicide vary among dif-ferent age-groups and cultures. Among elderly pop-ulations, there are consistent data suggesting that theuse of a firearm is a common method of completingsuicide. The Center for Disease Control has reportedthat the rate of firearm suicides among older men was27.7 per 100,000 during a 5-year period.6 The rate was1.8 per 100,000 for women over 65. Among elderlymen, firearms account for 80% of the suicides, withrates of firearm use increasing during the years 1979to 1991.7 This was also seen among elderly personsage 75 and greater in data spanning the years 1962 to1993.8 Although elderly women commit suicide atsignificantly lower rates than elderly men, by 1992,firearms replaced poisoning as the most commonmethod of suicide for elderly women.9
Research has also shown that the presence of a fire-arm in the home is associated with an increased riskof suicide for all ages. A case-control study found thata handgun in the home is a risk factor for suicide inmid- and late life.10 The same study found that anunlocked household gun and a loaded householdgun were associated an increase in the risk of suicide.Similarly, a study by Wintemute and colleagues11
found that in the first year after the purchase of ahandgun, suicide was the leading cause of deathamong handgun buyers. The overall rate of suicideafter a handgun purchase was highest for women andpersons 75 years of age and older. This high rate ofsuicide persisted for up to 6 years after the gun pur-chase. Other epidemiological data also suggest geo-graphical relationships between gun availability andsuicide rates.12,13 Despite these findings, most physi-cians do not discuss gun ownership and storage prac-tices with patients and their families.14,15
Given that older adults are at the highest risk ofsuicide and the use of a firearm is the most commonmethod for completed suicide, the purpose of thisstudy was to explore the prevalence of gun availabil-ity among older primary-care patients. Moreover,since depression is a significant risk factor for late-lifesuicide, a second purpose of the study was to exam-
ine the prevalence of gun ownership among thosewith and without significant depressive symptomsand among those with suicidal thoughts. We soughtto test the hypothesis that firearm availability waslowest among those with depression or suicidal ide-ation. We reasoned that if we were unable to dem-onstrate lower rates of availability in this high-riskgroup, greater efforts to identify older adults withpsychiatric distress and available firearms would bejustified. Thus, the overall goal was to estimate theextent to which psychiatric and gun-related risk fac-tors for suicide coexisted so as to inform the designof prevention programs.
METHODS
This study was conducted as a site-specific compo-nent of a larger multisite study comparing the effec-tiveness of various models of care for older adultssuffering from depression, anxiety, or at-risk drinking(PRISM-E study). The PRISM-E study is an 11-site ef-fectiveness trial comparing traditional referral care tospecialty mental health and substance abuse provid-ers versus integrated-care models delivering spe-cialty care in collaboration with primary-care physi-cians. PRISM-E is sponsored jointly by the SubstanceAbuse and Mental Health Services Administration,the Department of Veterans Affairs, the Health Re-sources and Services Administration, and the Centersfor Medicare and Medicaid Services. Because thescreening data collected for this current study wereonly obtained for a limited time and at only two ofthe sites (the Philadelphia VAMC and the Universityof Pennsylvania), the data should not be consideredrepresentative of the entire multisite study. These twosites were the only sites in the PRISM-E to collect dataon firearms availability and safety.
During the time between March 2000 and Septem-ber 2000, all patients age 65 and over who had anappointment with one of 34 primary-care clinicians(23 in the VA and 11 in non-VA community practices)were eligible for participation. The data presentedhere represent the first 10 months of screening datacollected in the PRISM-E multisite study; the entirescreening and enrollment period continued for an ad-ditional 8 months. Each week during the study, a ran-dom subset of patients was selected from each prac-

Suicide Risk and Access to Firearms
32 Am J Geriatr Psychiatry 12:1, January-February 2004
tice’s appointment list. Primary-care clinicians couldrequest that screening not be conducted on patientsknown to be terminally ill, severely cognitively im-paired, or who they felt could not participate in thescreening. The remaining patients were sent a letterfrom their physician describing the screening proce-dures to be used to identify those with mental healthdisorders. They were invited to return a form if theydid not wish to be contacted for telephone screening.Approximately 1 week before the scheduled medicalappointment, those who had not declined participa-tion were contacted by the research staff by tele-phone, to screen for depression, anxiety, and at-riskalcohol use.
Upon reaching the patient by telephone, we ob-tained oral consent in accordance with both the Phila-delphia VAMC and University of Pennsylvania IRBregulations. Screening was conducted using the fol-lowing instruments: the General Health Question-naire (GHQ),16 the Brief Orientation-Memory-Con-centration (BOMC) test,17 two screening questions forsuicidal ideation modified from the PRIME-MD thatidentified passive suicidal ideation or death ideationand suicidal ideation,18 quantity and frequency of al-cohol use, demographic data, a rating of global healthabstracted from the Medical Outcome Study (MOSSF-36),19 and questions related to firearm availabilityand firearm safety. The screening questions used fordeath ideation and suicidal ideation were “In the last2 weeks, have you had thoughts that you would bebetter off dead?” and “Have you had thoughts ofhurting yourself in some way?” Those with a BOMCscore of 16 or greater were excluded from furtherscreening. Those who screened positive on the GHQ,or who reported consumption of seven or moredrinks in the previous week, were invited to receivefurther evaluation of their psychiatric symptoms anddiagnoses, in accordance with the PRISM-E multisiteprotocol.
Statistical Analysis
Statistical analyses used SPSS Version 10.0.5 forWindows. Descriptive analyses included means andstandard deviations (SD) for continuous variablesand frequencies for categorical variables. Logistic-regression analyses were applied to assess the rela-tionship between firearm availability and safety prac-tices as binary outcomes and multiple baseline char-
acteristics, including depression severity, race, maritalstatus, cognition, age, and gender as covariates. A lo-gistic-regression analysis was also used to assess therelationship between significant distress, suicidal ide-ation, or significant cognitive impairment and firearmavailability and safety practices. In these analyses, dis-tress, suicide, and cognition were used as the depen-dent variable. Significant distress or depression wasexamined categorically in accordance with the use ofthe GHQ as a screening tool and was given the non-normal distribution of GHQ scores. Similarly, cogni-tion was also dichotomized. To compare the multiplereasons for owning handguns with those for owninga rifle, we used generalized estimating equations, inmultiple logistic regressions, to account for the corre-lated observations due to subjects’ providing morethan one reason for both types of guns.
RESULTS
During the study period, 1,869 patients were ran-domly selected for screening. Of those selected, 1,039(55.6%) consented and were able to complete thescreening process. The remaining patients refusedparticipation (N�458; 24.5%), were unable to be con-tacted during the screening period (N�195; 10.4%),were severely cognitively impaired (N�54; 2.9%),were hearing-impaired (N�21; 1.1%), were removedfrom the screening sample by their primary-care cli-nician (N�37; 2.0%), were too medically ill to answerquestions (N�17; 0.9%), had recently died (N�9;0.5%), or were in a nursing home (N�6; 0.3%). Thesample of screened patients is predominately white(73.0%), male (66.6%), currently married/partnered(58.8%), and living with someone else (72.7%). Themean age of participants was 74.7 years (SD 5.8), re-flecting the inclusion of only those 65 years of ageand older; 466 of the screened patients (44.9%) werefrom VA clinics, and 573 (55.1%) were from othercommunity primary-care practices. Of those patientswho were screened, 16 (1.5%) refused to answer thequestions regarding firearms.
Screening results identified 20.4% (N�212) of thesample as having significant depressive symptoms(GHQ �2) and 8.5% (N�88) as having death or sui-cidal ideation. Half of the sample (55.3%) reported nodrinking in the last year; 3.3% (N�34) reported more

Oslin et al.
Am J Geriatr Psychiatry 12:1, January-February 2004 33
than three binge drinking episodes in the last 3months, and 7.5% (N�78) reported drinking morethan seven standard drinks in the previous week. Al-though individuals with severe cognitive impairmentwere specifically excluded, a portion of the sampleexhibited mild-to-moderate cognitive impairment,with 6.9% of the patients scoring more than 10 errorson the BOMC.
Overall, 287 (28.1%) respondents reported theavailability of a gun in the home. Of all respondents,204 (20.2%) respondents had handguns available; 157(15.6%) had a rifle, shotgun, or other gun available,and 79 (7.6%) had both available in the home. Amongthose homes in which a firearm was available, themajority were stored unloaded (74.9%) and locked(55.4%), but ammunition was available for most ofthese firearms (79.0%). There were significant differ-ences in the reasons for having a handgun versus arifle, shotgun, or other gun. Handguns were more of-ten kept for protection (49.5% versus 14.2% in thosewith a rifle, shotgun, or other gun; Wald statistic [1df]: 55.21; odds ratio [OR]: 6.16; 95% confidence in-terval [CI]: 3.81–9.94; p �0.001) or for job-related ac-tivities (7.4% versus 0.6%; Wald statistic [1 df]: 5.91;OR: 12.51; 95% CI: 1.63–95.69; p�0.015), whereas ri-fles were more often kept for hunting (44.3% versus9.4%; Wald statistic [1 df]: 67.08; OR: 7.95; 95% CI:4.84–13.06; p �0.001). Firearms kept for protectionwere also much less likely to be kept unloaded, com-pared with those not kept for protection. Amongthose with handguns kept for protection, 58.6% werekept unloaded (versus 87.0% kept unloaded amongthose not keeping the gun for protection; Wald statis-tic [1 df]: 19.1; p �0.001). Among those with rifleskept for protection, 78.3% were kept unloaded (ver-sus 99.2% kept unloaded among those not keepingthe gun for protection; Wald statistic [1 df]: 21.9; p�0.001). Most participants said that having a firearmdid not make them feel any more or less safe in theirhome (N�180; 62.7%), although some did report feel-ing safer (N�78; 27.2%). Feeling safer because therewas a firearm available was significantly related tohaving a handgun (Wald statistic [1 df]: 8.54; OR: 3.09;95% CI: 1.45–6.60; p�0.003), having a handgun forprotection (Wald statistic [1 df]: 30.80; OR: 10.34; 95%CI: 4.53–23.60; p �0.001), having a rifle for protection(Wald statistic [1 df]: 11.38; OR: 6.70; 95% CI: 2.22–20.23; p�0.001), having a loaded weapon available(Wald statistic [1 df]: 20.72; OR: 4.73; 95% CI: 2.42–
9.23; p �0.001), and having ammunition available(Wald statistic [1 df]: 10.48; OR: 6.14; 95% CI: 2.05–18.44; p�0.001).
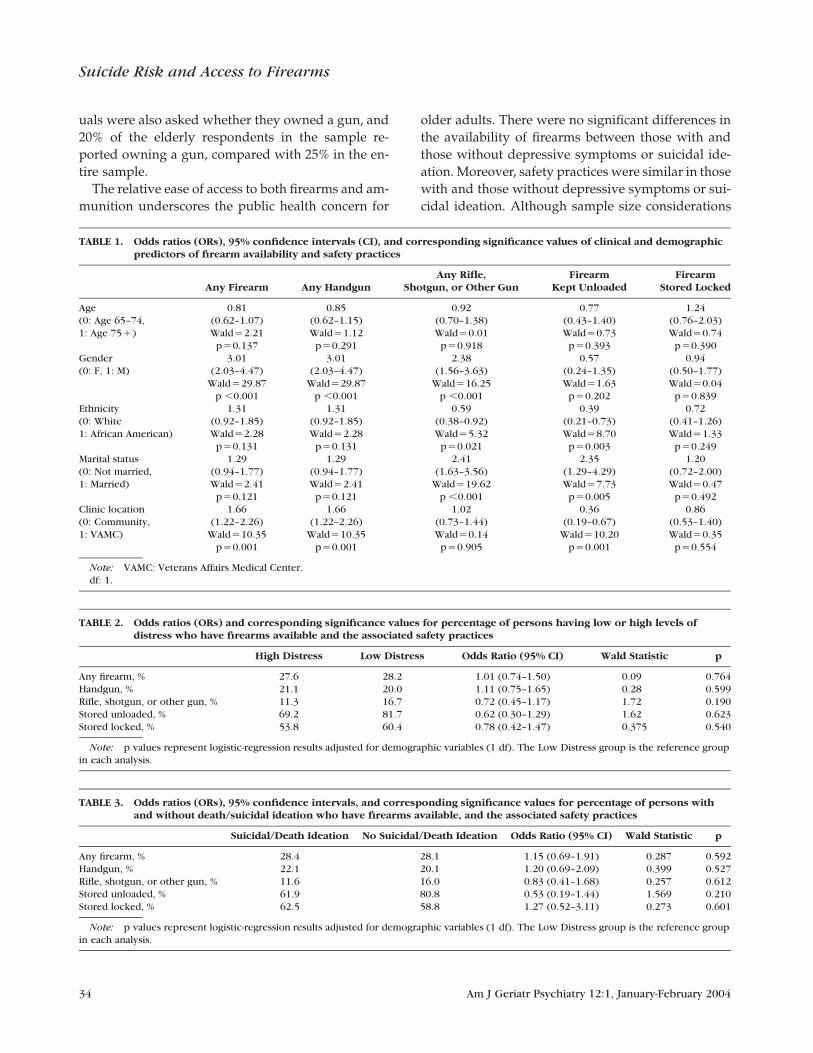
Gun availability was significantly related to certaindemographic factors. Table 1 presents results of anal-yses predicting gun availability and safety practicesrelative to these demographic factors. In general, fire-arms (both handguns and rifles or other guns) wereavailable more often among men and to persons whowere married. Handguns were also more likely to bepossessed by persons enrolled in health care at theVA medical center, and rifles were less likely to bepresent in African American homes. As for safetypractices, married subjects were more likely to havetheir firearms unloaded, whereas African Americansand veterans were much less likely to have their fire-arms unloaded. No demographic factors predictedwhich patients kept their firearms locked. As shownin Table 2 and Table 3, there were no significant as-sociations found between distress or suicidal ideationand availability of firearms or safety practices. Alco-hol use at consumption levels greater than one stan-dard drink per day was associated with having a rifleavailable (Wald statistic [1 df]: 4.00; OR: 1.77; 95% CI:1.01–3.11; p�0.045). We also examined differences inthose with and without significant cognitive impair-ment. There were no differences in gun availabilityfor those with or without cognitive impairment (Waldstatistic [1 df]: 1.67; OR: 0.20; 95% CI: 0.30–1.28;p�0.196), having a handgun (Wald statistic [1 df]:2.42; OR: 0.53; 95% CI: 0.24–1.18; p�0.120) or rifle(Wald statistic [1 df]: 0.86; OR: 0.64; 95% CI: 0.25–1.64;p�0.354), or whether the gun was stored locked(Wald statistic [1 df]: 1.45; OR .47; 95% CI: 0.13–1.62;p�0.229) or loaded (Wald statistic [1 df]: 1.67; OR:2.55; 95% CI: 0.62–10.52; p�0.196).
DISCUSSION
Results from this study demonstrate that a significantproportion of older adults have ready access to a fire-arm, particularly, a handgun, and that most house-holds have ammunition for these firearms. This isconsistent with a survey conducted by the NationalInstitute of Justice.20 The survey, conducted in 1994,was a random sampling of 2,568 households. Fire-arms were available in 35% of households. Individ-
Suicide Risk and Access to Firearms
34 Am J Geriatr Psychiatry 12:1, January-February 2004
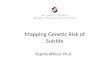
TABLE 3. Odds ratios (ORs), 95% confidence intervals, and corresponding significance values for percentage of persons withand without death/suicidal ideation who have firearms available, and the associated safety practices
Suicidal/Death Ideation No Suicidal/Death Ideation Odds Ratio (95% CI) Wald Statistic p
Any firearm, % 28.4 28.1 1.15 (0.69–1.91) 0.287 0.592Handgun, % 22.1 20.1 1.20 (0.69–2.09) 0.399 0.527Rifle, shotgun, or other gun, % 11.6 16.0 0.83 (0.41–1.68) 0.257 0.612Stored unloaded, % 61.9 80.8 0.53 (0.19–1.44) 1.569 0.210Stored locked, % 62.5 58.8 1.27 (0.52–3.11) 0.273 0.601
Note: p values represent logistic-regression results adjusted for demographic variables (1 df). The Low Distress group is the reference groupin each analysis.
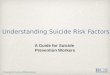
TABLE 2. Odds ratios (ORs) and corresponding significance values for percentage of persons having low or high levels ofdistress who have firearms available and the associated safety practices
High Distress Low Distress Odds Ratio (95% CI) Wald Statistic p
Any firearm, % 27.6 28.2 1.01 (0.74–1.50) 0.09 0.764Handgun, % 21.1 20.0 1.11 (0.75–1.65) 0.28 0.599Rifle, shotgun, or other gun, % 11.3 16.7 0.72 (0.45–1.17) 1.72 0.190Stored unloaded, % 69.2 81.7 0.62 (0.30–1.29) 1.62 0.623Stored locked, % 53.8 60.4 0.78 (0.42–1.47) 0.375 0.540
Note: p values represent logistic-regression results adjusted for demographic variables (1 df). The Low Distress group is the reference groupin each analysis.
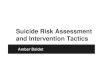
TABLE 1. Odds ratios (ORs), 95% confidence intervals (CI), and corresponding significance values of clinical and demographicpredictors of firearm availability and safety practices
Any Firearm Any HandgunAny Rifle,
Shotgun, or Other GunFirearm
Kept UnloadedFirearm
Stored Locked
Age(0: Age 65–74,1: Age 75�)
0.81(0.62–1.07)Wald�2.21
p�0.137
0.85(0.62–1.15)Wald�1.12
p�0.291
0.92(0.70–1.38)Wald�0.01
p�0.918
0.77(0.43–1.40)Wald�0.73
p�0.393
1.24(0.76–2.03)Wald�0.74
p�0.390Gender(0: F, 1: M)
3.01(2.03–4.47)
Wald�29.87p �0.001
3.01(2.03–4.47)
Wald�29.87p �0.001
2.38(1.56–3.63)
Wald�16.25p �0.001
0.57(0.24–1.35)Wald�1.63
p�0.202
0.94(0.50–1.77)Wald�0.04
p�0.839Ethnicity(0: White1: African American)
1.31(0.92–1.85)Wald�2.28
p�0.131
1.31(0.92–1.85)Wald�2.28
p�0.131
0.59(0.38–0.92)Wald�5.32
p�0.021
0.39(0.21–0.73)Wald�8.70
p�0.003
0.72(0.41–1.26)Wald�1.33
p�0.249Marital status(0: Not married,1: Married)
1.29(0.94–1.77)Wald�2.41
p�0.121
1.29(0.94–1.77)Wald�2.41
p�0.121
2.41(1.63–3.56)
Wald�19.62p �0.001
2.35(1.29–4.29)Wald�7.73
p�0.005
1.20(0.72–2.00)Wald�0.47
p�0.492Clinic location(0: Community,1: VAMC)
1.66(1.22–2.26)
Wald�10.35p�0.001
1.66(1.22–2.26)
Wald�10.35p�0.001
1.02(0.73–1.44)Wald�0.14
p�0.905
0.36(0.19–0.67)
Wald�10.20p�0.001
0.86(0.53–1.40)Wald�0.35
p�0.554
Note: VAMC: Veterans Affairs Medical Center.df: 1.
uals were also asked whether they owned a gun, and20% of the elderly respondents in the sample re-ported owning a gun, compared with 25% in the en-tire sample.
The relative ease of access to both firearms and am-munition underscores the public health concern for
older adults. There were no significant differences inthe availability of firearms between those with andthose without depressive symptoms or suicidal ide-ation. Moreover, safety practices were similar in thosewith and those without depressive symptoms or sui-cidal ideation. Although sample size considerations

Oslin et al.
Am J Geriatr Psychiatry 12:1, January-February 2004 35
do not allow us to demonstrate unequivocally anequal distribution in gun availability or safety prac-tices, on the basis of the confidence intervals pre-sented in Table 2 and Table 3, it is highly unlikely thatthose with significant depression are any less likelyto have a gun available to them. This is an importantfinding when evaluated in the context of reports thatdemonstrate an association between suicide and theavailability of a firearm. The findings from this studywould suggest a hypothesis that the association be-tween firearm availability and suicide is mediated byalcohol use or depression. If true, this would havesignificant public health significance in terms of link-ing the identification and educational efforts for fire-arm safety with the identification and treatment ofdepression and at-risk drinking. This is especially im-portant given the demonstration that education andtraining on the safe use of firearms is effective in in-creasing the safe storage of firearms.21
Future research should further explore possible ad-ditional predictors of unsafe gun practices, such asunemployment or education level, as well as exploreinterventions that either increase the safe storage ofguns or reduce the availability of guns in those withsignificant emotional distress or alcohol use. Resultsfrom this survey do provide possible target behaviorsfor reducing the risk of suicide associated with fire-arm availability. In addition to reducing availabilityof firearms among those with depression or suicidal-ity, education and interventions could focus on re-ducing the availability of ammunition or increasingthe use of trigger locks or other safety measures. Theresults suggest that educational programs might befocused on those persons maintaining firearms forprotection, those at VAMC clinics, African Ameri-cans, and those who consume alcohol.
There are significant limitations in this study thatmay affect interpretation of the findings. Althoughthe sampling of patients was randomly conducted,only half of the sample was screened, and thus thereis a potential for significant selection bias that we can-not address. Despite this, there were only a few peo-ple who refused to answer the questions about fire-
arms when the screening was conducted. This studyis also unable to address differences in gun availabil-ity and safety practices in different geographic re-gions such as rural areas or the southern or westernUnited States. Despite this limitation, the prevalenceof gun availability is very consistent with that foundin the National Institute of Justice report and thusmay in fact be generalizable across the country. Fi-nally, with regard to the association with depressionand suicide, it is difficult to test for similarities ratherthan differences in gun availability or safety prac-tices.
Overall, the results of this study raise importantquestions regarding the relationship between depres-sion, alcohol use, suicidal ideation, and access to fire-arms. Given that the present study found that ap-proximately 20% of elderly patients in primary carereported having a handgun available to them andthat the availability of handguns has been linked tosuicide, it is important that clinicians assess firearmavailability and safety practices. The assessment offirearm availability is especially important when talk-ing with individuals who are in crisis or who havemental disorders, substance abuse problems, or sui-cidal thoughts.22,23 Efforts to educate patients andtheir caregivers about the potential dangers of gunsand appropriate strategies for improving safety whenusing and storing firearms may have a profound im-pact on the prevention of suicide in this population.Further research should also address questions aboutthe appropriateness of recommendations for remov-ing firearms from homes.
Results from this manuscript were presented at theAnnual Meeting of the American Psychiatric Associationin May 2001, Chicago, IL.
Funding was provided by the Department of VeteransAffairs, SAMHSA (#1UD1SM53033); the National In-stitute of Mental Health (#1K08MH 01599); the NationalInstitute of Mental Health (#5P30MH52129); and theMental Illness Research, Education, and Clinical Centerat the Philadelphia VAMC.
References
1. Hoyert DL, Kochanek KD, Murphy SL: Deaths: Final Data for1997. National Vital Statistics Reports, 1999, 47:1–104
2. Conwell Y, Duberstein PR, Cox C, et al: Relationships of age andAxis I diagnoses in victims of completed suicide: a psychologicalautopsy study. Am J Psychiatry 1996; 153:1001–1008
3. Beautrais AL: A case-control study of suicide and attempted sui-cide in older adults. Suicide Life Threat Behav 2002; 32:1–9
4. Conwell Y: Depression as a “cause” of late-life suicide. Crisis1992; 13:55–56
5. Bartels SJ, Coakley E, Oxman TE, et al: Suicidal and death ideation

Suicide Risk and Access to Firearms
36 Am J Geriatr Psychiatry 12:1, January-February 2004
in older primary care patients with depression, anxiety, and at-risk alcohol use. Am J Geriatr Psychiatry 2002; 10:417–427
6. Centers for Disease Control and Prevention: National Summaryof Injury Mortality Data, 1989–1995. Centers for Disease Controland Prevention, National Center for Injury Prevention and Con-trol, Atlanta, GA, 1997
7. Adamek ME, Kaplan MS: Firearm suicide among older men. Psy-chiatr Serv 1996; 47:304–306
8. Ikeda RM, Gorwitz R, James SP, et al: Trends in fatal firearm-related injuries, United States, 1962–1993. Am J Prev Med 1997;13:396–400
9. Kaplan MS, Adamek ME, Geling O, et al: Firearm suicide amongolder women in the U.S. Soc Sci Med 1997; 44:1427–1430
10. Conwell Y, Duberstein PR, Connor K, et al: Access to firearmsand risk for suicide in middle-aged and older adults. Am J GeriatrPsychiatry 2002; 10:407–416
11. Wintemute GJ, Parham CA, Beaumont JJ, et al: Mortality amongrecent purchasers of handguns. New Engl J Med 1999; 341:1583–1589
12. Miller M, Azrael D, Hemenway D: Firearm availability and unin-tentional firearm deaths. Accid Anal Prev 2001; 33:477–484
13. Miller M, Azrael D, Hemenway D: Household firearm ownershipand suicide rates in the United States. Epidemiology 2002;13:517–524
14. Grossman D, Mang K, Rivara F: Firearm injury prevention coun-seling by pediatricians and family physicians: practices and be-liefs. Arch Pediatr Adolesc Med 1995; 149:973–977
15. Kaplan MS, Adamek ME, Rhoades JA: Prevention of elderly sui-cide: physicians’ assessment of firearm availability. Am J Prev Med1998; 15:60–64
16. Goldberg D: Manual of the General Health Questionnaire. Wind-sor, England, National Foundation for Educational Research,1978
17. Blessed G, Tominson BE, Roth M: The association between quan-titative measures of dementia and of senile change in the cerebralgray matter. Br J Psychiatry 1968; 114:797–811
18. Spitzer RL, Williams JBW, Kroenke K: Utility of a new procedurefor diagnosing mental disorders in primary care: the PRIME-MD1000 Study. JAMA 1994; 272:1749–1756
19. McHorney CA, Ware JE, Lu JFR, et al: The MOS 36-Item Short-Form Health Survey (SF-36), III: tests of data quality, scaling as-sumptions, and reliability across diverse patient groups. MedCare 1994; 32:40–66
20. Cook PJ, Ludwig J: Guns in America: National Survey on PrivateOwnership and Use of Firearms. National Institute of Justice,Washington, DC, 1997, pp 1–12
21. Hemenway D, Solnick S, Azrael D: Firearm and training and stor-age. JAMA 1995; 273:46–50
22. Goldman L, Silverman M, Alpert E: Violence and aggression, inPsychiatry for Primary Care Physicians. Edited by Goldman L,Wise T, and Brody D. Chicago, IL, American Medical Association,1998, pp 155–180
23. World Health Organization: Preventing Suicide: A Resource forPrimary Health Care Workers. Geneva, Switzerland, World HealthOrganization Dept. of Mental Health, 2000, Report #WHO/MNH/MBD/00.4