Embed Size (px)
Citation preview

46 Nursing made Incredibly Easy! May/June 2008
Assessing
suicide risksuicide risk

JOESEPH GAINES, a single, 36-year-oldteacher, came to the emergency department(ED) by ambulance after his neighbor called911. He suffered a near-fatal overdose—afailed suicide attempt. He was transferredto your medical-surgical unit after being inthe intensive care unit (ICU) for 2 days. Ac-cording to the ICU nurse, when Mr. Gainesregained consciousness, he was angry aboutbeing rescued.
Nearly 500,000 ED admissions for suicide-related injuries are reported annually, sosooner or later you’re likely to care for apatient like Mr. Gaines (see Suicide in theUnited States: By the numbers). After a patientattempts suicide, hospital policy defines thenursing interventions needed. More difficult,however, is identifying suicide risk in apatient who’s admitted for an illness orinjury unrelated to a suicide attempt.
In this article, I’ll provide an overview ofsuicide and suicide prevention in a medical-surgical setting and discuss risk factors, ele-ments of an effective suicide assessment, andnursing interventions you can apply to youreveryday practice.
OvercomingbarriersPatients rarely attemptsuicide when admittedfor a specific physicalproblem, probably be-cause these patients aregenerally treated anddischarged as quicklyas possible. If a hospi-talized patient attemptssuicide, with or with-
out a permanent loss of function such asbrain damage, or commits suicide, it’s a sentinel event according to The Joint Commission.
Admission patient-assessment forms sel-dom include questions about suicide, andmost nurses don’t routinely screen patientsfor suicide risk, even though patients aren’tlikely to volunteer information about suici-dal thoughts. One study indicated that twoof every three people who commit suicidemay have seen a primary care provider inthe month before their death, suggesting thathealth care professionals are missing oppor-tunities to intervene. In hospitals, shorterstays hinder the development of nurse/patient relationships, so patients may notfeel comfortable enough to disclose suicidalthoughts to caregivers.
Like many nurses, you may feel uncom-fortable with the topic too. For instance, youmay be afraid that asking a patient aboutsuicidal intentions may trigger suicidalthinking or behavior. Or you may not knowwhat to say or do if he admits to having sui-cidal thoughts. To save lives, we need to
May/June 2008 Nursing made Incredibly Easy! 47
riskriskWould you recognize suicidal behavior in oneof your patients and know how to intervene?We’ll give you practical, potentially lifesavingguidelines you can follow.CONSTANCE CAPTAIN, RN, PHDClinical Nurse Specialist • Behavioral HealthNorth Broward Hospital District Service • Fort Lauderdale, Fla.
The author has disclosed that she has no significant relationships with or financial interest in anycommercial companies that pertain to this educational activity.
2.0ANCC/AACN
CONTACT HOURS

overcome these barriers by making suicideassessment part of routine nursing assess-ment.
Let’s consider some basic information youneed to know before you can assess a pa-tient’s risk and intervene effectively.
Along the continuumMost suicide attempts are expressions of ex-treme distress, not bids for attention. Suici-dal behavior develops along this contin-uum:n ideation. This is the process of contem-plating suicide or the methods used withouttaking action. At this point, the person mightnot talk about these thoughts unless he’spressed.n suicidal gestures. These are actions thataren’t likely to be lethal, such as taking a few
pills or making superficial cuts on the wrist.They suggest that the person is ambivalentabout dying or hasn’t planned to die. He hasthe will to survive, wants to be rescued, andis experiencing a mental conflict. A suicidalgesture is often called a cry for help becausethe person is struggling with unmanageablestress.n suicide attempts. An attempt, such as tak-ing a potentially lethal dose of medication,indicates that the person wants to die andhas no wish to be rescued.n suicide. The act of intentionally killingoneself may follow previous attempts, butabout 30% of those who commit suicide arebelieved to have done so on their first at-tempt. Suicide results when the person cansee no other option for relief from unbear-able emotional or physical pain.
Physiologically speakingResearch is beginning to unravel some ofthe physiologic reasons for suicidal behav-ior. For example, psychological autopsystudies suggest that in 90% of completedsuicides, the person had one or more men-tal disorders, usually major depression andsubstance abuse, particularly alcoholism. Apsychological autopsy, which is a techniqueused to discover a suicide victim’s state ofmind before his death, is often used for le-gal purposes.
Researchers are also investigating howalterations in neurotransmitters such as sero-tonin negatively affect mood and judgment.Diminished levels of this brain chemicalhave been found in people with depression,impulsive disorders, or a history of suicideattempts and also in suicide victims (see Therole of neurotransmitters).
Understanding the motivation behindsuicidal behavior is difficult not only fornurses, who are dedicated to saving lives,but also for suicidal patients themselves.Those who’ve attempted suicide most com-monly express their need to escape from anunbearable situation, usually one involvingdespair and mental or physical pain. Many
48 Nursing made Incredibly Easy! May/June 2008
Don’t be afraidto ask your
patient aboutsuicidal
thoughts.
Suicide in the United States: By the numbers• Over 30,000 suicides occur each year. • Suicide is the 11th leading cause of death overall. • Over 60% of all people who die by suicide suffer from major depression;
alcoholism is a factor in about 30% of all completed suicides.
By age• Suicide is the third leading cause of death for young adults between the
ages of 15 and 24. • It’s the fourth leading cause of death in adults between the ages of 18
and 65.• It’s the fifth leading cause of death in children and adolescents between
the ages of 5 and 14.
By gender• Four men commit suicide for every one woman, but twice as many
women attempt suicide than men.• Seven times the number of men than women over age 65 commit sui-
cide.• The suicide rate for men increases after age 65; the rate for women
peaks between the ages of 45 and 54 and again after age 75.
By method• Firearms account for 52% of all suicides.
Adapted from American Foundation for Suicide Prevention, Facts and figures:National statistics. http://www.afsp.org/index.cfm?fuseaction=home.viewPage&page_id=050FEA9F-B064-4092-B1135C3A70DE1FDA. Accessed January 15, 2008.

patients describe their emotional pain as aconstant, intolerable, inescapable heaviness.Depression and despair often accompanymedical conditions that are characterized byphysical pain, disfigurement, limited func-tion, and loss of independence.
But how do you know if your patient is atrisk for suicide? Let’s take a closer look.
Recognizing risksTo prevent suicide, the first steps are identi-fying and understanding risk factors. A riskfactor is anything that increases the likeli-hood that a person will harm himself, and itshould alert you to the need to assess himfurther for suicidal ideation.
Consider why your patient is currently inthe hospital; this may be the first indicationof increased risk. For many patients, hospi-talization is likely to mean bad news: a con-firmed diagnosis, troubling test results, adecline in health, or difficult medical deci-sions. You’ll need to evaluate your patient’semotional response to his medical condition,not just his physical status.
Don’t be afraid to ask about suicidalthoughts (see Interview do’s and don’ts). Mostpatients who are suicidal are relieved totalk about their feelings and to be assuredthat they aren’t crazy for thinking this way.First, assess your patient for depression byasking a question like this: Are you feelingdepressed (or sad or discouraged)? If theanswer is yes, then ask these standard sui-cide assessment questions:n How long have you felt like this?n Do you feel that your life is no longerworth living?n Are you thinking of acting on that feelingby hurting yourself or taking your own life?n Do you have a suicide plan?n Can you tell me about your plan?
You should ask for detailed informationif your patient has a suicide plan. A plan ismore likely to be lethal if he can articulatespecifics, such as method and place;believes the plan can succeed; and hasdevised precautions to avoid interruption
or discovery. Ask whether he has madefinal arrangements, such as a will or otherinstructions, or has given away treasureditems. His responses will provide you witha sense of the seriousness of his suicidalintentions. If you determine that he’s at riskfor suicide, never leave him alone even ifhe can’t carry out his plan in the hospital.You’ll also need to implement suicide pre-cautions.
Now let’s take a look at what you need todo if your patient is suicidal.
One on oneBecause a nonpsychiatric hospital environ-ment is loaded with potentially dangerousitems, you can’t make it completely safe fora patient at risk for suicide. Initiate one-to-one observation status according to your
May/June 2008 Nursing made Incredibly Easy! 49
Interview do’s and don’tsWhen interviewing a patient at risk for suicide, follow these guidelines.
Do set clear goalsThe assessment interview isn’t meant to be a random discussion. Makesure you have clearly set goals, such as investigating for depression orsuicidal thoughts.
Do heed unspoken signalsListen carefully for indications of anxiety or distress. What topics does thepatient ignore or pass over vaguely? You may find important clues in hismethod of self-expression and in the subjects he avoids.
Do check yourselfMonitor your own reactions. The patient may provoke an emotionalresponse strong enough to interfere with your professional judgment.
Don’t rushDon’t rush through the interview. Remember, building a trusting therapeu-tic relationship takes time.
Don’t make assumptionsDon’t make assumptions about how past events affected the patient emo-tionally. Try to discover what each event meant to him. For example, if hesays one of his parents died, don’t assume that the death provoked sad-ness. A death by itself doesn’t cause sadness, guilt, or anger. What mat-ters is how the patient perceives the loss.
Don’t judgeDon’t let personal values cloud your professional judgment.

50 Nursing made Incredibly Easy! May/June 2008
Dendrites
AxonCell body
Myelin sheath
Node of Ranvier
Nucleus
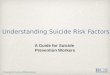
The role of neurotransmittersAffecting behavior, mood, and thought, neurotransmitters are chemical messengers released into the synapses (gaps) between neu-rons (nerve cells) that carry messages from one neuron to another. If a person has low levels of the neurotransmitters norepinephrineand serotonin in areas of the brain that control mood and emotion, depression may result.
facility’s policy, notify his primary careprovider, and explain to him why you’retaking precautions. Assure him that youwant to keep him safe until he’s feeling lessdespondent and more in control. Most hos-pitals have a written policy on caring for asuicidal patient who has already attemptedsuicide like Mr. Gaines. Follow your facil-ity’s policy; obtain a copy and use it as aguide.
If you initiate one-to-one observation,instruct the observer to stay at least an arm’slength away from the patient at all times. Anappropriate observer is a staff nurse who’sbeen trained on how to observe and how torespond. Although family members may askto fill this role, it isn’t appropriate for them todo so because they may not know how torespond. Using them could also present lia-bility issues.
Other common safety measures include:n removing all sharp or hazardous objects(including plastic bags and metal coat hang-ers) from the patient’s roomn requesting that food be served with paperplates and cups and plastic eating utensilsn taking away potentially hazardous per-sonal items, such as shoelaces, belts, glassobjects, and lightersn performing a contraband check of all per-sonal belongingsn telling visitors not to leave anything withthe patient unless the nurse approvesn observing the patient to make sure heswallows medicationsn restricting him to the unitn locating him near the nurses’ station
Risk factors for suicideConsider your patient at risk if he:• verbalizes suicidal thoughts, wishes, or a plan• has a history of one or more suicide attempts• has a family history of suicide• feels depressed or anxious or expresses feelings of hopelessness• has a chronic mental illness or history of mental illness• abuses alcohol or another substance• has a physical illness with a poor prognosis• has impulsive or aggressive tendencies• has suffered a significant loss or multiple losses (such as the death of aspouse, job loss, or financial setback)• has access to lethal methods, such as firearms or medications• feels ambivalent about treatment or doesn’t cooperate with treatment• suffers from loneliness and lacks a social network.
sheet
cheat

n placing him in a room with anotherpatient.
I find that having the patient write andsign a no-harm contract is a good way toencourage him to start taking charge of hisown behavior and become an active partnerin his treatment. It might include state-ments such as “I won’t harm myself whileI’m in the hospital. I’ll tell the nurse if I havethoughts of harming myself.” Another earlyintervention is to involve the family, if yourpatient consents. Ask him if he has a familymember or friend whom he wants to involvein his care.
Comprehensive documentation for yourpatient should include risk factor data, directquotes that capture his suicidal thoughts orplans, actions you took to keep him safe,who you notified about his suicidal behav-ior, and precautions taken.
Working through itReassess your patient at least once per shiftto determine his current level of suicidal in-tent and whether one-to-one observationshould continue. Ask him to rate his levelof suicidal intent on a 0-to-10 scale, with 0meaning no thoughts of suicide and 10
May/June 2008 Nursing made Incredibly Easy! 51
Synapticcleft
Nerve message
Neurotransmittersbind to receptor site
Release ofneurotransmittermolecules(norepinephrineand serotonin)
Membranechannel opensas a result ofbindingneurotransmitter
Nerve messageis transmitted toadjoining neuron
Dendritesreceiving neuron
Closedmembranechannels
Brainchemistry canplay a role indepression.Here’s how.

meaning constant thoughts of suicide. Doc-ument the score during each shift so staffmembers can track trends.
You can also use the comparisons to helpyour patient understand what factors may ormay not be decreasing his suicidal thoughtsor underlying depression. For instance, didhe have visitors, receive cards or flowers,sleep well, or participate in self-care? Thiswill give him some insight into factors con-tributing to his improved mood or sense ofhope.
You can help your patient by talkingabout his experience in a sincere and sup-
portive way. You’ll want to spend uninter-rupted, but not necessarily long, periodswith him. One approach is to relieve theobserver for breaks and meals. Focus yourinteractions on your patient’s present crisis.For example, you might say, “Help meunderstand. Can you tell me what’s goingon in your life that’s unbearable?” Thisapproach encourages him to talk about hiscircumstances and perceptions. To assess hisemotional status, focus on how he feels.After a suicide attempt, some patients areembarrassed and some are relieved thatthey were rescued. Others, like Mr. Gaines,are disappointed and angry.
As his nurse, show empathy by listeningas your patient expresses his frustration. Ifhe says he’s feeling discouraged or de-pressed, explain that, until it lifts, depressionlimits a person’s ability to see other options.Suicidal behaviors are often transient andtime limited and can be precipitated by apersonal crisis. Focus on the precipitatingfactors and events leading up to the attemptand look for an opportunity to talk aboutalternative problem-solving approaches hecould have used. For example, you mightask, “Have you ever been in a similar situa-tion? How did you handle that?” Ask open-ended questions, listen, and reinforce hisefforts to work through his feelings and con-cerns. Don’t try to resolve his problems, giveadvice, or point out how much better off heis than someone who’s less fortunate.
Ultimately, you want your patient toregain a sense of hope. This process beginswith helping him identify personal strengthsand setting small achievable goals. Listen forand pick up on any reference to the future,which is a positive sign suggesting improve-ment.
What are the treatments available for apatient who’s suicidal as a result of depres-sion? That’s up next.
Looking to the futureStandard treatment for a patient with ma-jor depression is antidepressant medication
52 Nursing made Incredibly Easy! May/June 2008
Mental health assessmentreviewObtaining a mental health history• Establish a trusting, therapeutic relationship.• Choose a quiet, private setting.• Maintain a calm, nonthreatening tone of voice to encourage opencommunication.• Determine your patient’s chief complaint, using his own words to docu-ment it.• Discuss past psychiatric disturbances and previous psychiatric treat-ment, if any.• Obtain his demographic and socioeconomic data.• Discuss his cultural and religious beliefs.• Obtain a medication history.• Ask about a history of medical disorders; some conditions may adverse-ly affect his mental health.
Mental status checklist• Appearance• Demeanor and overall attitude• Extraordinary behavior• Inconsistencies between body language and mood• Orientation to time, place, and person• Confusion or disorientation• Attention span• Ability to recall events• Intellectual function• Speech characteristics that indicate altered thought processes• Insight• Coping or defense mechanisms• Self-destructive behavior• Psychological and mental status test results
sheet
cheat

combined with counseling or other talktherapy. Teach your patient about his med-ications and explain that these drugs maynot be fully effective for weeks. In addi-tion, prepare him for follow-up psychiatriccare. He may have a psychiatric consultwhile he’s in your unit or he may be trans-ferred to a psychiatric facility or the psy-chiatric unit within your facility. Informinghim of this in advance will help him ac-cept and cooperate with this routinepractice.
If your patient is discharged home, askhis permission to have a family memberensure that the home environment is safeand free from weapons, potentially danger-ous medications, and other hazards.
Assess and actBy knowing how to assess a patient’s riskof suicide and taking appropriate nursingactions, you may prevent a suicide attempt.You don’t need to be a psychiatric nurse to
recognize a vulnerable patient and initiateinterventions that may save his life. n
Learn more about itAssessment Made Incredibly Easy!, 3rd edition. Philadel-phia, Pa., Lippincott Williams & Wilkins, 2005:67.
Captain C. Is your patient a suicide risk? Nursing2006.36(8):43-47, August 2006.
Pathophysiology Made Incredibly Visual! Philadelphia, Pa.,Lippincott Williams & Wilkins, 2008:80-81.
Psychiatric Nursing Made Incredibly Easy!Philadelphia, Pa., Lippincott Williams &Wilkins, 2004:20.
May/June 2008 Nursing made Incredibly Easy! 53
On the WebThese online resources may be helpful to your patients and their families:American Foundation for Suicide Prevention: http://www.afsp.org Centers for Disease Control and Prevention:http://www.cdc.gov/ncipc/factsheets/suifacts.htmNational Institute of Mental Health: http://www.nimh.nih.gov/health/topics/suicide-prevention/index.shtmlSuicide Prevention Resource Center: http://www.sprc.orgWorld Health Organization: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en.
INSTRUCTIONS
Assessing suicide riskDISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published by Lippincott Williams& Wilkins together and deduct $0.95 from the price of each test.• We also offer CE accounts for hospitals and other health care facilities onnursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATIONLippincott Williams & Wilkins, publisher of Nursing made Incredibly Easy!, willaward 2.0 contact hours for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing education by theAmerican Nurses Credentialing Center’s Commission on Accreditation.
LWW is also an approved provider of continuing nursing education by theAmerican Association of Critical-Care Nurses #00012278 (CERP Category A),District of Columbia, Florida #FBN2454, and Iowa #75. LWW home study activi-ties are classified for Texas nursing continuing education requirements as Type1. This activity is also provider approved by the California Board of RegisteredNursing, Provider Number CEP 11749, for 2.0 contact hours. Your certificate isvalid in all states.
Earn CE credit online: Go to http://www.nursingcenter.com/CE/nmie and receive a certificate within minutes.
TEST INSTRUCTIONS• To take the test online, go to our secure Web site atwww.nursingcenter.com/ce/nmie.• On the print form, record your answers in the test answersection of the CE enrollment form on page 55. Each ques-tion has only one correct answer. You may make copies ofthese forms.• Complete the registration information and course evalu-ation. Mail the completed form and registration fee of$21.95 to: Lippincott Williams & Wilkins, CE Group,2710 Yorktowne Blvd., Brick, NJ 08723. We will mail yourcertificate in 4 to 6 weeks. For faster service, include a faxnumber and we will fax your certificate within 2 businessdays of receiving your enrollment form. Deadline is June 30, 2010.• You will receive your CE certificate of earned contacthours and an answer key to review your results. There is nominimum passing grade.




![Suicide prevention and depression apps’ suicide risk ......ness of online interventions and mobile apps [31, 32], app store descriptions of apps [33], or assessing suicide pre-vention](https://img.pdfslide.us/doc/110x75/60a0387215361146994a9b3b/suicide-prevention-and-depression-appsa-suicide-risk-ness-of-online-interventions.jpg)