Embed Size (px)
Citation preview

Managing Sudden CardiaC death riSk in new OnSet COngeStive heart Failure PatientS—CaSe Study Prakash Desai, MDAmarillo Heart Group Hospital
History of Present illness (HPi) A 73-year-old male presented to his primary care physician with complaints of shortness of breath and signs of peripheral edema that had progressively worsened over the previous 2–3 weeks. The patient was convinced the symptoms were a result of bulging disks in his back. He was referred to the emergency room and was ultimately hospitalized due to atrial fibrillation with rapid ventricular response and elevated cardiac enzymes. He had a history of hypertension, cirrhosis, and colon cancer, which was treated with a partial colectomy in 2005. The patient was not established with a cardiologist and was not taking any medications at home.
social History The patient is married with four children and five grandchildren. He reported a history of heavy alcohol consumption with a recent reduction in use. Additionally, he reported smoking two packs of cigarettes per day.
PHysical examination/labs The physical examination revealed bilateral lower extremity 2+ pitting edema with reports of occasional dizziness, palpitations, shortness of breath, and coughing. The patient had a distended soft abdomen and a mild jugular venous distention. Low-pitched wheezing sounds were noted in the base of his lungs. The patient was awake, alert, and had no appearance of acute distress.
Relevant labs: sodium 125, potassium 4.6, chloride 92, CO2 21, glucose 120, BUN 39, creatinine 1.7, BNP 1461, CPK 528, CK-MB 35.6, troponin 0.06, AST 78, ALT 95
Hematology: white blood count 9.6, hemoglobin 15.5, hematocrit 48.1, platelets 210,000
studies/results The patient’s electrocardiogram (EKG) revealed atrial fibrillation with a ventricular rate of 103 beats per minute and a right bundle branch block. The chest x-ray revealed a small right effusion and biventricular enlargement. An echocardiogram revealed moderate enlargement of all four chambers of the heart with a left ventricular ejection fraction (EF) of 10–15% and mild mitral and tricuspid valve regurgitation.

Managing Sudden CardiaC death riSk in new OnSet COngeStive heart Failure PatientS—CaSe Study By Prakash Desai, MD, Amarillo Heart Group Hospital
imPressions/Plan The patient was diagnosed with new onset congestive heart failure. The patient assessment also included probable chronic obstructive pulmonary disease secondary to long-term tobacco abuse, hyponatremia secondary to congestive heart failure, and renal dysfunction secondary to cirrhosis.
The patient was started on heparin, amiodarone, diltiazem, digoxin, and metoprolol. He was monitored for the next six days.
Cardiac catheterization confirmed severely dilated cardiomyopathy and significant left ventricular dysfunction with an EF of 15%. Left main, left anterior descending, left circumflex, and right coronary arteries were all noted as normal and revealed no significant occlusions.
It was determined that the patient’s severely low EF in combination with renal dysfunction put him at an elevated risk for sudden cardiac death (SCD). The patient was prescribed a wearable cardioverter defibrillator (WCD) (manufactured by ZOLL, Pittsburgh, PA, marketed under the brand name LifeVest®) for three months and discharged on day ten.
The patient was discharged on the following medications:
• spironolactone 12.5 mg q am• carvedilol 9.375 mg bid (with instructions to titrate up to 12.5 mg bid)• furosemide 20 mg qd• hydralazine 12.5 mg bid• digoxin 0.125 qd• nicotine patch• aspirin 81 mg qd• warfarin 5 mg qd• fluticasone/salmeterol bid• levofloxacin 750 mg q48h
The patient was scheduled for a follow-up visit to reevaluate his ejection fraction. If at that time his EF remained ≤35%, an implantable cardioverter defibrillator (ICD) would be considered for long-term protection from SCD.
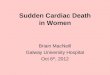
clinical uPdate Just over nine weeks later, the patient was working alone twenty miles from home when he started to feel uneasy. He sat down in his vehicle and suddenly lost consciousness. The WCD detected ventricular tachycardia at a rate of 208 BPM (see Figure 1) and delivered a 150J biphasic treatment shock 32 seconds after detection. The treatment successfully converted his arrhythmia and he awoke moments later. He drove himself home and his wife immediately brought him to the hospital.
The patient went on to receive a biventricular cardiac resynchronization therapy defibrillator (CRT-D) implant. He returned home and is back to work as a contractor in the oil industry. His EF and heart failure symptoms are improving.
PAGE 2

Managing Sudden CardiaC death riSk in new OnSet COngeStive heart Failure PatientS—CaSe Study By Prakash Desai, MD, Amarillo Heart Group Hospital
PAGE 3
Figure 1: EKG downloaded from WCD. The WCD continuously monitors the patient’s EKG using a 4 electrode, 2 lead system—side-to-side (SS, top) and front-to-back (FB, bottom).
discussion In this case study, a patient with no history of heart failure, presented to his primary care physician with progressively worsening shortness of breath and peripheral edema. A physical examination along with routine diagnostic tests ruled out coronary artery disease and revealed the diagnosis of nonischemic dilated cardiomyopathy with an EF of 10–15%.
New onset congestive heart failure with low EF can quickly deteriorate and lead to potentially lethal ventricular arrhythmias. Optimized doses of beta blockers have been shown to reduce total mortality including SCD, but often require three or more months of titration to achieve mortality benefits.1 The patient’s discharge plan included instructions for titration of the beta-blocker dose with the addition of a WCD to provide protection from SCD until optimal doses were achieved. In this case, the patient experienced a dangerous episode of sustained ventricular tachycardia only eleven weeks from the original presentation of congestive heart failure symptoms. The WCD can be a useful tool to manage risk of SCD during medical therapy optimization while the need for ICD implantation is being evaluated.
REFERENCES 1. MERIT-HF Study Group, Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353: 2001–07.
208 BPM

20C0296 Rev FI
ZOLL • Pittsburgh© 2014 ZOLL Medical Corporation. All rights reserved. ZOLL and LifeVest are registered trademarks of ZOLLMedical Corporation in the United States and/or other countries.