Embed Size (px)
Citation preview

Managing Hypotension and Bleeding
(and Decreased LOC) Dr Ann Marie McCallum
Anaesthetist, Westmead Hospital Slide contents with thanks to Dr Gerri Khong

Objectives Assess & manage patients with: Hypotension Bleeding Decreased conscious level
Recognise early/ late signs/symptoms of deterioration
Blood Transfusions – what, when, how fast
Seizure Management

You are paged again…..

Case 1: Mr RS 69 year old male
RTW at 1830 after angio / attempted stent of left
lower limb “screaming in pain”

Initial Management: What do you do?

Initial Management: Initial Ax / Mx concurrent
A-G Assessment +/- Call for help
Ix

Hx – minimal from patient, from notes: COPD, IHD with AMI 10 years ago, PVD, T2DM on OHG Ex – disoriented and agitated HR 120 – 130 BP 155/90 SaO2 92-94% RA Heart sounds dual, chest clear
Ix


You reassess the patient Still agitated
HR 125 bpm BP 75/40
SaO2 94% 4L/min via HM

What will you do next?

Could this be blood loss? Visible/external Upper GI – haematemesis, maelena Lower GI PV (Obstetric or otherwise!) Epistaxis Occult: intra-thoracic, intra-abdominal, intra-pelvic,
retroperitoneal

ABG results pH 7.18 pCO2 33 pO2 75 K 3.5 Na 134 Hb 76 Glu 8.2 HCO3 21 Lactate 4.2
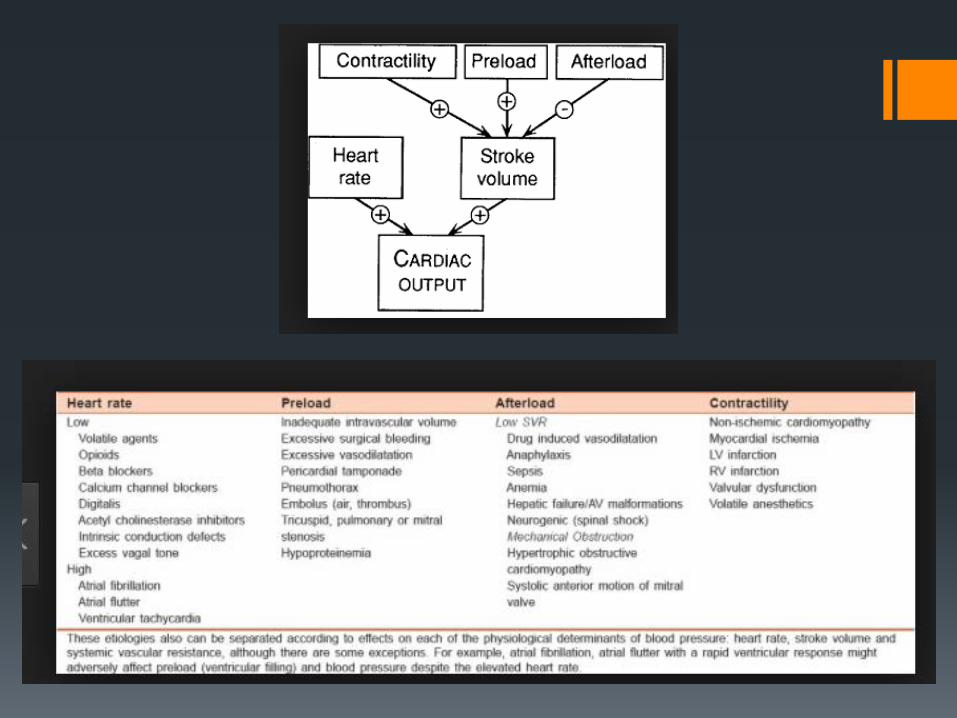
HYPOTENSION – Causes?? Sepsis Cardiogenic Cardiac tamponade PE Occult blood loss (or overt blood loss! Eg melaena) Anaphylaxis Addisonian crisis Autonomic dysfunction Poisoning/drug induced

HYPOTENSION – Causes?? Sepsis Cardiogenic (Post myocardial
infarct) Cardiac tamponade PE Occult blood loss (or overt
blood loss! Eg melena) Anaphylaxis Addisonian crisis Autonomic dysfunction
Poisoning/drug induced

HYPOTENSION – Causes?? Sepsis Cardiogenic (Post myocardial
infarct) Cardiac tamponade PE Occult blood loss (or overt
blood loss! Eg melena) Anaphylaxis Addisonian crisis Autonomic dysfunction
Poisoning/drug induced

HYPOTENSION – Causes?? Sepsis Cardiogenic (Post myocardial
infarct) Cardiac tamponade PE Occult blood loss (or overt
blood loss! Eg melena) Anaphylaxis Addisonian crisis Autonomic dysfunction
Poisoning/drug induced

HYPOTENSION – Causes?? Sepsis Cardiogenic (Post myocardial
infarct) Cardiac tamponade PE Occult blood loss (or overt
blood loss! Eg melena) Anaphylaxis Addisonian crisis Autonomic dysfunction
Poisoning/drug induced


BLOOD – How fast to give it? 1) Stable patient - 2 – 4 hours - Consider cardiac function - Review after each unit 2) Bleeding/unstable patient - Stat! - Appropriate IV access - ALS!

BLOOD – What if the patient needs A LOT?
MASSIVE TRANSFUSION PROTOCOL
Blood bank: ext 57700 for Emergencies
Australian Red Cross Blood Service, www.transfusion.com.au


MTP
(Plus Platelets)

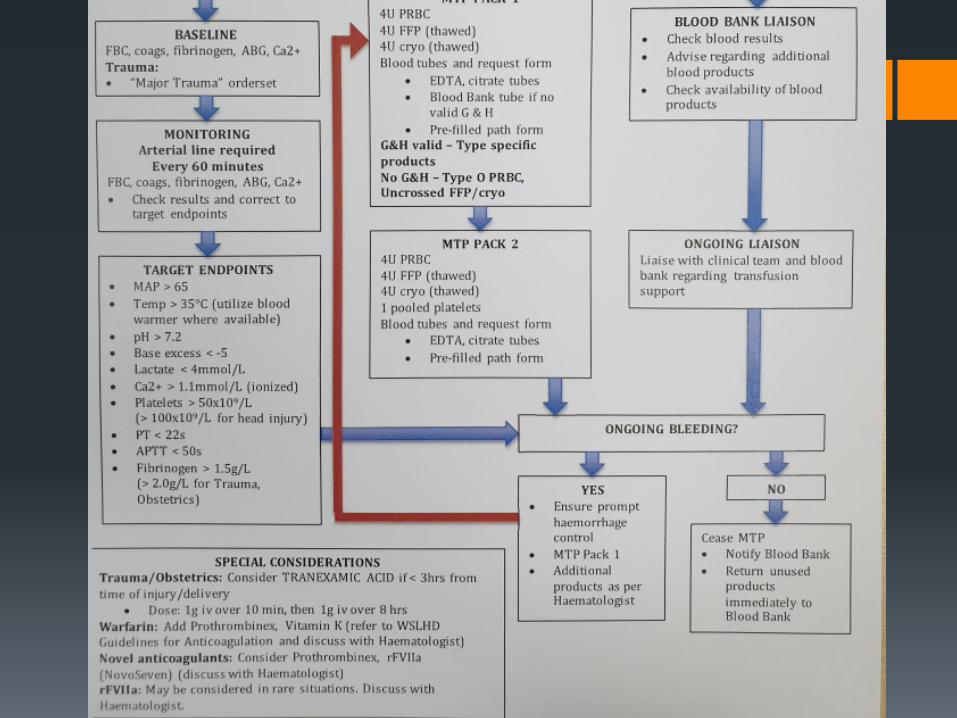

One MTP Pack contains: 4 units PRBC 4 units FFP 4 units Cryoprecipitate

What happened… 1830 RTW “screaming in pain”, HR 110, BP
155/90, SaO2 94% RA, disoriented No further obs are done-’difficult patient’ 2100 HR 115, BP 64/34, RR 22, 89%RA
PACE(??) 2103 ALS called A5a (wrong ward) 2105 ALS called A5c

2156 Hb 79 DDx: Retroperitoneal bleed 2230 8/24 IVF
2330 CT: “Large left retroperitoneal bleed”
0040 OT – pale, sweaty. Induction HR 160 VT PEA 0120 Resuscitation ceased

You are paged again….

Mr KJ 81yo male admitted with community acquired pneumonia
PMH: COPD, T2DM on s/c insulin, PVD
Noted to be “drowsy”

What do you do?

What do you do? Focused Hx/Ex GCS / AVPU Prodromal events
Focal signs
Ix Bloods – ABG, EUC, FBC, LFT +/- TFT, osmolality Septic screen ECG Imaging




Whilst you are assessing him….

Management of an acute episode: A,B,C
Stop the seizure
Identify any causes
Prevent complications

Medication: 1st line benzodiazepines
IV Midazolam – 0.02 – 0.1 mg/kg Usually 1-2 mg
PR diazepam 10 mg

Medication: 2nd line phenytoin
Phenytoin 15 mg/kg in normal saline slower than 50mg/min eg 1g in 100mls N/saline over 30 mins for 50kg

ABG pH 7.25 pCO2 46 PO2 79 K 3.9 Na 135 Hb 105 Glu 2.1 HCO3 22 Lactate 1.9

Objectives Assess & manage patients with: Hypotension Bleeding Decreased conscious level
Recognise early/ late signs/symptoms of deterioration
Blood Transfusions – what, when, how fast
Seizure Management