Embed Size (px)
Citation preview

SOGC CLINICAL PRACTICE GUIDELINE
No. 336, September 2016
Management of Spontaneous Labour atTerm in Healthy Women
Kl
h
J
CoCaPu
TcTp
This Clinical Practice Guideline has been prepared by theClinical Practice Obstetrics Committee, reviewed by theFamily Physician Advisory, Maternal Fetal Medicine, Medico-Legal and Obstetrical Content Review Committees, andapproved by the Board of the Society of Obstetricians andGynaecologists of Canada.
PRINCIPAL AUTHORS
Lily Lee, RN, Vancouver BC
Jessica Dy, MD, Ottawa ON
Hussam Azzam, MD, Thompson MB
CLINICAL PRACTICE OBSTETRICS COMMITTEE MEMBERS
Hussam Azzam (Chair), MD, Thompson MB
Jon Barrett, MD, Toronto ON
Anne Biringer, MD, Toronto ON
Kim Campbell, RM, Vancouver BC
Louise Duperron, MD, Kirkland QC
Jessica Dy, MD, Ottawa ON
Ellen Giesbrecht, MD, Vancouver BC
Lisa Graves, MD, Toronto ON
Michael Helewa, MD, Winnipeg MB
Ian Lange, MD, Calgary AB
Lily Lee, RN, Vancouver BC
Suzanne Muise, MD, Bedford NS
ey Words: management of labour, labour dystocia, first stageabour, second stage labour, third stage labour
ttp://dx.doi.org/10.1016/j.jogc.2016.04.093
Obstet Gynaecol Can 2016;38(9):843e865
pyright ª 2016 The Society of Obstetricians and Gynaecologists ofnada/La Société des obstétriciens et gynécologues du Canada.blished by Elsevier Inc. All rights reserved.
his document reflects emerging clinical and scientific advances on the daonstrued as dictating an exclusive course of treatment or procedure to be folhey should be well documented if modified at the local level. None of theermission of the publisher.
Barbara Parish, MD, Halifax NS
SPECIAL CONTRIBUTOR
Roanne Preston, MD, Vancouver BC
Jennifer Hutcheon, PhD, Vancouver BC
Corinne Riddell, PhD, Montreal QC
Disclosure statements have been received from all members ofthe committee.
The authors wish to acknowledge the expertise and support of theSOGC Obstetrical Content Review committee in completing thisguideline.
Abstract
Objective: The purpose of this guideline is to provide guidancefor the intrapartum management of spontaneous labour, whethernormal or abnormal, in term, healthy women, and to provideguidance in the management of first and second stage dystociato increase the likelihood of a vaginal birth and optimize birthoutcomes.
Evidence: Published literature was retrieved through searches ofPubMed and the Cochrane Library in October 2011 usingappropriate, controlled vocabulary (e.g., labour pain; labour,obstetric; dystocia) and key words (e.g., obstetric labor, perinealcare, dysfunctional labor). When appropriate, results were restrictedto systematic reviews, randomized control trials/controlled clinicaltrials, and observational studies. Results were limited to the last 10years. Searches were updated on a regular basis and incorporatedin the guideline up to June 15, 2015.
Values: The quality of evidence in this document was rated using thecriteria described in the Report of the Canadian Task Force onPreventive Health Care (Table 1).
Summary Statements
1. The duration of the first stage of labour increases with maternal ageand body mass index. (II-2)
2. In low-risk nulliparous women in the active phase of labour (i.e.,equal to or greater than 4 cm dilatation), progress of cervicaldilatation greater than or equal to 0.5 cm/hour is considerednormal. (II-2)
te issued and is subject to change. The information should not belowed. Local institutions can dictate amendments to these opinions.se contents may be reproduced in any form without prior written
SEPTEMBER JOGC SEPTEMBRE 2016 l 843

Table 1. Key to evidence statements and grading of recommendations, using the ranking of the Canadian Task Force onPreventive Health Care
Quality of evidence assessment* Classification of recommendations†
I: Evidence obtained from at least one properly randomizedcontrolled trial
II-1: Evidence from well-designed controlled trials withoutrandomization
II-2: Evidence from well-designed cohort (prospective or retro-spective) or caseecontrol studies, preferably from more thanone centre or research group
II-3: Evidence obtained from comparisons between times or placeswith or without the intervention. Dramatic results in uncontrolledexperiments (such as the results of treatment with penicillin inthe 1940s) could also be included in the category
III: Opinions of respected authorities, based on clinical experi-ence, descriptive studies, or reports of expert committees
A. There is good evidence to recommend the clinical preventive actionB. There is fair evidence to recommend the clinical preventive actionC. The existing evidence is conflicting and does not allow to make a
recommendation for or against use of the clinical preventive action;however, other factors may influence decision-making
D. There is fair evidence to recommend against the clinical preventiveaction
E. There is good evidence to recommend against the clinical preven-tive action
L. There is insufficient evidence (in quantity or quality) to make arecommendation; however, other factors may influence decision-making
*The quality of evidence reported in these guidelines has been adapted from The Evaluation of Evidence criteria described in the Canadian Task Force on PreventiveHealth Care.
†Recommendations included in these guidelines have been adapted from the Classification of Recommendations criteria described in the Canadian Task Force onPreventive Health Care.
SOGC CLINICAL PRACTICE GUIDELINE
3. Each labour unit should have a guideline for opioid use during labourthat includes the method of action, average and maximum doses,route of administration, possible maternal and fetal side effects,precautions, and opioid antagonists and resuscitative measures foreach drug. (III)
4. Epidural analgesia provides the most effective pain relief for womenin labour. The timing of initiation of labour epidural is dependent onthe woman’s choice once the diagnosis of labour has been estab-lished. (I)
Recommendations
1. Health care providers should delay term labour admission to thebirthing unit until active labour (i.e., equal to or greater than 4 cmdilatation) is established. (II-2A)
2. Documentation and communication of labour progress are impor-tant aspects of labour management. Labour and delivery unitsshould establish local policy regarding labour documentation,including partogram use and its application in labour management.(III-A)
ABBREVIATIONSAMTSL active management of the third stage of labour
BMI body mass index
CCT controlled cord traction
CLS continuous labour support
CS Caesarean section
IUPC intrauterine pressure catheter
IV intravenous
OASIS obstetrical anal sphincter injuries
PCEA patient-controlled epidural analgesia
PPH postpartum hemorrhage
RCT randomized controlled trial
SOGC Society of Obstetricians and Gynaecologists of Canada
TENS transcutaneous electrical nerve stimulation
844 l SEPTEMBER JOGC SEPTEMBRE 2016
3. Women should be informed of the benefits of upright positioning inlabour and encouraged and assisted to assume whatever positionsthey find most comfortable. (I-B)
4. Women who are at low risk of requiring general anesthesia shouldhave the choice to eat or drink as desired or tolerated in labour. (I-A)
5. Continuous labour support is recommended for all women in activelabour. Each labour unit should aim to provide the opportunity foreach woman to receive continuous 1-to-1 labour support. (I-A)
6. Amniotomy and oxytocin, in addition to other measures, should beconsidered once a diagnosis of dystocia has been made in eitherthe first or second stage of labour. (I-B)
7. Women and health care providers should have information aboutcoping strategies for early labour and mechanisms for accessingsupport from caregivers. (III-A)
8. When appropriate, health care providers should support women intheir choice of analgesic options in labour. These may includepharmacological and non-pharmacological measures. (III-A)
9. Each woman should be provided with evidence-based informationabout labour analgesia options prior to the onset of labour andoffered ample opportunity to discuss the risks and benefits of eachoption available at her planned site of delivery. (III-A)
10. The use of meperidine as labour analgesia should be avoided dueto its long-acting active metabolites and negative effects onneonatal behaviours. (II-2B)
11. Low-dose epidural, when available, is preferred over high-doseepidural for labour analgesia and in promoting mobility in labour. (I-A)
12. Women who receive an epidural should be encouraged to maintainmobility and flexibility in positions of comfort throughout labour. (I-B)
13. Once an epidural has been established, the infusion should becontinued until completion of the third stage of labour. (I-A)
14. Pushing, as a component of secondstageprogress,maycommencewhen the cervix is fully dilated, the presenting part is confirmed to beengaged, and the woman feels an urge to push. (III-A)
15. Delayed pushing is preferred when the woman has no urge topush, particularly if the presenting part is above station þ2 and/orin a non-occiput anterior position, assuming the fetus does notdisplay abnormal monitoring and the pregnant woman’s status issatisfactory. (I-A)

Management of Spontaneous Labour at Term in Healthy Women
16. Delay of pushing according to parity and the presence or absenceof an epidural should follow the time limits described in the textunless there are extenuating circumstances. (II-2B)
17. The method of pushing, spontaneous or directed with Valsalvamanoeuvre, should be chosen using the woman’s own preference.Directed pushingmay assist with the final expulsion of the head. (II-2B)
18. Avoid theuseof routineepisiotomy inspontaneousvaginal births. (I-A)
19. Prophylactic oxytocics should be given after the delivery of thebaby. (I-A)
20. In term and preterm infants who do not require neonatal resusci-tation, delayed umbilical cord clamping for 60 seconds is recom-mended irrespective of the mode of delivery. (I-B)
21. Dystocia should not be diagnosed prior to the onset of the activephase of the first stage of labour or before the cervix is at least 4 cmdilated. (II-2D)
22. Oxytocin augmentation should be titrated to avoid tachysystoleor excessive uterine activity and to produce a uterine contractionpattern of 4 to 5 contractions in 10 minutes (200 Montevideounits). A minimum of 4 to 6 hours of adequate uterine activitymay be required to achieve the desired response. (I-A) It is
recommended that every obstetrical unit have an identified andaccessible protocol that includes a starting dose, increment in-terval, and maximum dose. Consistent use of 1 standardapproach to oxytocin administration in any 1 obstetrical unitshould be considered. (III-A)
23. Operative delivery less than 2 hours after commencing pushing isnot recommended, provided maternal status and fetal surveillanceare normal. (III-D)
24. When the second stage exceeds the recommended time limits (seetext), consideration should be given to expediting delivery.Extending these time limits may be appropriate in the presence ofcontinued descent of the head, satisfactory maternal and fetalstatus, and imminent vaginal birth. (II-2B)
25. High-dose oxytocin regimens have been shown to decreaselabour duration compared with low-dose regimens. The lowestdose needed to produce normal progress is recommended toreduce the risk of tachysystole or excessive uterine activityand to create a uterine contraction pattern of 3 to 5 con-tractions or 200 or more Montevideo units every 10 minutes.(I-A)
SEPTEMBER JOGC SEPTEMBRE 2016 l 845

SOGC CLINICAL PRACTICE GUIDELINE
INTRODUCTION
abour management supports the natural physiological
Lprocess of birth while identifying potential concerns.The purpose of this guideline is to provide guidance for theintrapartum management of normal and abnormal labour,to increase the likelihood of a vaginal birth, and to optimizematernal and fetal outcomes. Promotion of normal birthinvolves a balance between non-intervention and thejudicious use of technologies that support safe outcomesfor both the mother and baby.This guideline focuses on the management of spontaneouslabour in healthy women at term, with a singleton vertexfetus with no maternal or fetal risk factors. In addition, theguideline discusses the management of dystocia in the firstand second stages of labour in the same population.
Definitions of Labour
Labour: first stage Regular uterine contractions accompanied by cervical dilatation and/or effacement. The first stage of labourincludes the latent and active phases.
Latent phase Presence of uterine activity resulting in progressive effacement and dilatation of the cervix proceeding toactive phase. It is complete when a nulliparous woman reaches 4 cm dilatation and a parous woman reaches4 to 5 cm. Cervical length is generally less than 1 cm.
Active phase Presence of a pattern of contractions leading to cervical effacement and dilatation at 4 cm or greater in anulliparous woman or 4 to 5 cm dilatation in a parous woman.
Labour: second stage Full dilatation to delivery of the baby.
Passive second stage Full dilatation but without active pushing.
Active second stage Full dilatation with active pushing.
Labour: third stage Immediately after delivery of the baby to delivery of the placenta.
Labour: fourth stage Immediately after delivery of the placenta to 1 hour postpartum.
Dystocia Delayed or arrested progress in labour, irrespective of cause.
In active first stage Greater than 4 hours of < 0.5 cm/hour dilatation or no dilatation over 2 hours.1
In active second stage Greater than 1 hour of active pushing without descent of the presenting part.2
Obstructed labour No cervical dilatation or descent over 2 hours despite evidence of strong contractions (caput, molding, ormeasured using an IUPC).
PART I: NORMAL LABOUR
Diagnosis of LabourThe diagnosis of the active phase of labour is the singlemost important factor in labour management.3 The onsetof labour is defined as regular, painful uterine contractionsresulting in progressive cervical effacement and dilatation.
The onset of the latent phase is often difficult to define.Women frequently present to the hospital in the latentphase of labour. Health education for women and familiesabout when to come to the hospital, what symptoms areimportant, and what symptoms require urgent action is animportant component of care during pregnancy.
846 l SEPTEMBER JOGC SEPTEMBRE 2016
The diagnosis of the active phase of labour requires anassessment of both uterine activity and cervical status.Description of cervical status should include dilatation,effacement, station, consistency, and position.4
Labour Time FramesThe mean duration and longest acceptable duration oflabour and the “normal” rates of cervical dilatation werehistorically established by Friedman in the early 1950s.5
These were based on a mixed population of women whowere in either spontaneous or induced labour and withfetuses in the vertex and breech presentations and wereestablished before the introduction of epidural analgesia.6
More recently, Zhang et al.7 studied 1162 nulliparouswomen with a single term fetus in the vertex presentationin spontaneous labour who delivered vaginally anddemonstrated a markedly different curve than that of
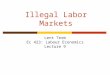
Friedman’s. Almost half of the women included in Zhang’sstudy received regional anesthesia and oxytocin augmen-tation. Although both labour curves depict a relatively slowrate of cervical dilatation during the latent phase, thetransition from the latent to active phase is less obvious inZhang’s labour curve (Figure 1). Cervical dilatation from 4to 10 cm took 5.5 hours in Zhang’s curve instead of 2.5hours in Friedman’s curve, and the rate of cervical changewas noted to be more gradual. In Zhang’s curve, women inthe lowest fifth percentile for rate of cervical dilatationexperienced dilatation less than 1 cm/hour. Several studies,including data from a large retrospective cohort from theConsortium of Safe Labor, further confirmed the findings

Figure 1. Comparison of Friedman’s curve and Zhang’scontemporary labour curve.7
Management of Spontaneous Labour at Term in Healthy Women
of these more contemporaneous labour patterns.8,9 Theupper limit of normal active phase dilatation appears to belonger and the rate of cervical dilatation slower that thoseinitially set by Friedman, ranging from 0.5 to 0.7 cm/hourfor nulliparous women and from 0.5 to 1.3 cm/hour forparous women. Only half of nulliparous women in theactive phase dilated at a rate greater than 1.2 cm/hour.Although authors from the Consortium of Safe Labor didnot identify labour duration for the diagnosis of dystocia inthe active phase, they suggested that the diagnosis shouldnot be made before 6 cm of cervical dilatation. This,however, has yet to be evaluated.9
Multiple factors can affect the length of labour for anygiven woman. Peisner and Rosen10 found that dilatation in90% of women who experienced a successful vaginal birthprogressed at greater than or equal to 1 cm/hour after 5cm. They concluded that when a woman’s cervix is notrapidly dilating after reaching 5 cm, her labour is probablyabnormal and should be closely evaluated.
From all of the aforementioned labour studies, it is evidentthat the duration of labour varies from woman to womanand the rate of cervical change is faster in the active phaseof the first stage of labour and in parous women.
Physiological Factors Influencing LabourSuccessful labour and vaginal delivery depend on thedynamic relationship between the fetus, the maternalpelvis, and uterine and maternal power. Dystocia can berelated to the difficulty with any of the 4 Ps: power,passenger, passage, and psyche, which can influence theprogress of labour and delivery.
Maternal factorsPower contractions
maternal expulsive efforts
During labour, palpation of uterine contractions is recom-mended to assess the uterine activity. Assessment of thestrength of contractions by palpation and/or external tocody-namometry does have limitations. Manual palpation provides asubjective estimate of intensity and can be more difficult toassess when obesity is a factor. External tocodynamometrycannot accurately detect contraction strength.Using an IUPC isthe only accurate method to assess the intensity of uterinecontractions. An IUPC may be considered in situations inwhich accurate assessment of uterine contractions cannot beassessed with external tocodynamometry.11 When using anIUPC, contraction strength is considered to be adequate at 50to 60 mmHg above baseline or> 200 Montevideo units (sumof uterine contraction pressure above baselinemultiplied by thenumber of contractions in 10 minutes).
Passage pelvic bony structure
soft tissue factors (pelvic tumours, full bladder/rectum, vaginal septum, obesity)
Clinical examination of the passage may reveal prominentspines or sacrum, a narrow pubic arch, or a space-occupying mass in the pelvis (e.g., fibroids). Neither ante-natal radiological nor clinical pelvimetry has been shown topredict the outcome of labour.12
Psyche pain
anxiety
“Hormones released in response to stresscan . bring about dystocia. Sources of stress varyfor each woman, but pain and the absence of asupport person are the two accepted factors.Confinement to bed and the restriction of maternalmovement can also be a source of psychologicalstress. Maternal anxiety may inhibit normal cervicaldilatation resulting in prolonged labour and increasedpain perception. Maternal anxiety also causes anincrease in the levels of stress-related hormones(b-endorphin, adrenocorticotropic hormone,cortisol, and epinephrine). These hormones, whichact on the smooth muscle of the uterus, can lead todystocia by reducing uterine contractions.”13
Fetal factorsPassenger position
attitude
SEPTEMBER JOGC SEPTEMBRE 2016 l 847

SOGC CLINICAL PRACTICE GUIDELINE
size
abnormalities (e.g., hydrocephalus)
The fetus should be assessed for size and position. Adequateuterine power in labour will often correct malposition,whereas inadequate power may result in persistent malpo-sition. A normal-sized infant may present an increaseddiameter to the pelvis because the head is not flexed or isasynclitic. Adequate maternal/uterine power may overcomethis problem. Use of the hands and knees position for 10minutes twice daily was not found to correct an occiputposterior fetal position in late pregnancy.14
The diagnosis of true or absolute cephalopelvic dispro-portion should be limited to the uncommon instance ofreal disproportion (i.e., the inability of the well-flexedhead [suboccipito bregmatic presentation] to passthrough the bony pelvis despite clinical evidence ofadequate uterine power [caput and molding or IUPC]).Malposition, on the other hand, may lead to relativedisproportion. Accurate assessment and descriptionguide management, and if a CS is performed for truecephalopelvic disproportion, it will help determine suit-ability for a future trial of labour after CS.
Other factors influencing labour
Prenatal education. Women and their partners seek prenataleducation to help them understand the process of birthand the potential options related to labour, pain relief, andinfant care. The effects of various forms of prenatal edu-cation on labour outcomes are largely non-conclusive andhave not been fully evaluated to date.15
Maternal age. The average maternal age is rising. The pro-portion of women who are 35 years or over giving birthhas increased steadily in the past decades.16 Older maternalage is associated with increased obstetrical and perinatalcomplications and increased obstetrical intervention,including labour induction, oxytocin augmentation, pro-longed labour, instrumental delivery, and intrapartumCaesarean birth.16,17 The effect of delayed child-bearing
Table 2. Adjusted duration of labour (hours) by BMI (kg/m2) c
Cervical dilatation 4 to 10 cm
BMI categories at admissio
< 25 25 to 29.9
Nulliparous 5.4 (18.2) 5.7 (18.8) 6
Parous 4.6 (17.5) 4.5 (17.4) 4
Adapted from Kominiarek MA, Zhang J, Vanveldhuisen P, Troendle J, Beaver J, HibbarObstet Gynecol 2011;205:244.e1e8.26
848 l SEPTEMBER JOGC SEPTEMBRE 2016
among 583 843 nulliparous women in Scotland between1980 and 2005 on primary Caesarean delivery rates wasstudied by Smith et al.18 For every 5-year increase in age,they noted an increase of 0.49 hours in duration of labour(95% CI 0.46 to 0.51). The authors also demonstrated areduction in spontaneous myometrial contractile activitywith increasing maternal age.
Obesity. A number of observational cohort studies haveexamined the relationship between maternal pre-pregnancyBMI and the duration of labour.19e25 Overall, the studieshave found that the duration of the first stage of labourincreases with a rising BMI. In a high-quality study of 5200deliveries in which the second stage of labour was reached,Norman et al.24 found that obese (BMI � 30) nulliparousand parous women took approximately 1 hour longer todilate from 4 to 10 cm compared with women with anormal pre-pregnancy BMI (� 25). In a smaller, secondstudy of 612 term deliveries to nulliparous women, Vahra-tian et al.19 found that dilatation from 4 to 10 cm was 105minutes longer in obese (BMI > 29) women, adjusted forlabour induction and augmentation. It is likely that the truedifference in first stage labour duration between obese andnon-obese women is larger than what was observed in thesestudies. Because obese women are more likely to undergo afirst stage Caesarean delivery due to dystocia, women withthe longest labour durations may have been excluded fromthe cohort.19e21,25
The median and 95th percentile values for the duration ofthe first stage of labour according to maternal BMI at thetime of delivery admission from a large cohort of 119 000deliveries may be useful in establishing normal and abnormalprogress.26 Table 2 shows that labour proceeds more slowlyas BMI increases, suggesting that labor management shouldbe tailored to allow for these differences.
Overall, there is good evidence that the duration of thefirst stage of labour increases with a rise in maternal BMI.Biological/physiological studies27 that have examinedhypothesized relationships in vitro between secretionsfrom adipose tissue and characteristics of uterinecontractility complement the epidemiological literature
ategories
n with median (and 95th percentile) traverse times in hours
30 to 34.9 35 to 39.9 � 40 P value for trend
.0 (19.9) 6.7 (22.2) 7.7 (25.6) < 0.0001
.7 (17.9) 5.0 (19.0) 5.4 (20.6) < 0.0001
d JU. Contemporary labor patterns: the impact of maternal body mass index. Am J

Management of Spontaneous Labour at Term in Healthy Women
and further elucidate the causal mechanism underlyingthis relationship.20
Summary Statement
1. The duration of the first stage of labour increases withmaternal age and body mass index. (II-2)
MANAGEMENT OF THE FIRST STAGE OF LABOUR
Labour is a normal physiological process. Most womenwho enter labour spontaneously would be expected toexperience their labour and birth with minimal in-terventions.28 Any interventions to this process should bebased on an identified real or potential problem. Use ofunnecessary interventions (e.g., routine amniotomy) maylead to further interventions, including Caesarean birth.
Over the past few decades there has been a dramaticincrease in the number of CS being performed.29 CS isassociated with increased maternal morbidity and mor-tality, increased neonatal morbidity, and increased healthcare costs. Labour dystocia and elective repeat CS ac-count for the majority of CS being performed. Optimalmanagement with support of the normal labour pro-cesses and the appropriate management of labourdystocia, if it occurs, could potentially lead to a significantreduction in the primary CS rate and the number ofwomen labouring in a subsequent pregnancy after a priorCS.
Latent Phase of the First Stage of LabourManagement during the latent phase of the first stage oflabour is controversial due to the limited number of pub-lished studies. Cohort studies have consistently shown thatwomen presenting to the hospital in the latent phase oflabour experience increased obstetrical interventions (e.g.,epidural analgesia, oxytocin use, Caesarean delivery)compared with women presenting in active labour.30e32
However, because of the observational nature of thesestudies, it is unclear whether the increased level of inter-vention is due to prolonged exposure to the hospitalenvironment or to underlying labour abnormalities amongwomen who present earlier. One small randomized trial byMcNiven et al.33 found that women who received an earlylabour assessment in a triage area required less oxytocinand epidural analgesia and reported a more positive labourand birth experience compared with women directlyadmitted to the labour and delivery unit. The small samplesize precluded the assessment of effects on Caesareandelivery and other important measures of maternal-newborn outcomes.
Early labour assessment and support at home from anobstetric nurse reduce the number of women presenting tothe hospital in the latent phase and the number of womennot coping with their contractions on admission comparedwith telephone support, but these measures did not reducethe use of obstetrical interventions such as oxytocin,epidural analgesia, or Caesarean delivery.34
Recommendation
1. Health care providers should delay term labouradmission to the birthing unit until active labour (i.e.,equal to or greater than 4 cm dilation) is established.(II-2A)
Active Phase of the First Stage of LabourPartogramPartograms are graphical records used during active labourto help visually assess labour progress by recording cervicaldilatation and the descent of the presenting part, facilitatingearly detection of dystocia and timely intervention ofamniotomy and oxytocin augmentation. For this purpose,some partograms include action lines to trigger the treat-ment of dystocia.
A 2013 Cochrane review that included 7706 women in 6randomized trials35 found no difference between the use ornon-use of a partogram related to outcomes of CS inwomen presenting in spontaneous labour at term, instru-mental vaginal delivery, or an Apgar score less than 7 at 5minutes. In the single high-quality trial performed in ahigher-resourced setting, there were no significant differ-ences between groups in these outcomes. When comparedwith a 4-hour action line, women in the 2-hour action linegroup were more likely to require oxytocin augmentationbut showed no difference in Caesarean delivery or othermaternal or neonatal outcomes. When the 3- and 4-houraction lines were compared, the CS rate was 70% lowerin the 4-hour action-line group. Despite the routine use ofa partogram in both low- and high-resourced settings, thereis insufficient evidence that its use results in measurableclinical outcomes. However, given its widespread use as adocumentation tool in monitoring maternal/fetal statusand labour progress, the use of a partogram maycontribute to overall team functioning and communication.
Recommendation
2. Documentation and communication of labourprogress are important aspects of labourmanagement. Labour and delivery units shouldestablish local policy regarding labour documentation,
SEPTEMBER JOGC SEPTEMBRE 2016 l 849

SOGC CLINICAL PRACTICE GUIDELINE
including partogram use and its application in labourmanagement. (III-A)
Ambulation and upright positioningFor women who do not receive epidural analgesia,ambulation, position change, and upright positions mayreduce the length of the first stage of labour and opera-tive delivery. A 2013 Cochrane review found that womenrandomly assigned to upright positions (walking or up-right non-walking [e.g., sitting, standing, kneeling, squat-ting, and all fours]) compared with recumbent positions(supine, semi-recumbent, and lateral) experienced firststages that were 82 minutes shorter and lower rates of CS,were less likely to receive epidural analgesia, and deliveredbabies that were less likely to be admitted to neonatalintensive care. However, there was no difference in lengthof the second stage of labour or other outcomes relatedto the well-being of mothers and babies. Interestingly, forwomen who received epidural analgesia, there were nodifferences between those randomly assigned to uprightpositions versus recumbent positions for any of theoutcomes examined in the review.36
Recommendation
3. Women should be informed of the benefits of uprightpositioning in labour and encouraged and assisted toassume whatever positions they find mostcomfortable. (I-B)
Eating and drinking during labourA 2013 Cochrane review on restricting oral fluid andfood intake during labour examined women in active la-bour and at low risk of potentially requiring generalanesthesia. The investigators compared restrictingwomen to nothing except ice chips or sips of water orwater alone with providing women with fluid and foodsor the freedom to eat and drink at will and found nosignificant differences in CS, assisted vaginal births orApgar scores. The pooled data were insufficient to assessfor the incidence of the rare outcome of Mendelson’ssyndrome (aspiration associated with general anesthesia).The authors concluded that there is no evidence ofbenefits or harms associated with restricting women’saccess to fluids and foods during labour for women atlow risk of potentially requiring a general anaesthetic.37
No studies have assessed the restriction of oral fluid inwomen with risk factors for induction of general anes-thesia; the conclusion should not be extrapolated to non-low-risk populations.
850 l SEPTEMBER JOGC SEPTEMBRE 2016
It is recognized that a healthy woman entering labour maydevelop complications resulting in a change of her riskstatus and labour management; clear communication andcommon understanding among care providers about herrevised risk status are critical. Policies regarding oral intakein labouring women should be determined at each site bythe health care team.
Recommendation
4. Women who are at low risk of requiring generalanesthesia should have the choice to eat or drink asdesired or tolerated in labour. (I-A)
Birthing companion/continuous emotional supportCLS is defined as non-medical care provided during labourthat includes continuous presence, emotional support,comfort measures, advocacy, information, and advice.38
CLS may be provided by a trained person such as adoula, nurse, or midwife or from a friend or familymember of the woman’s choice.39
A 2013 Cochrane review of over 15 000 women in low-and middle-resource settings showed that CLS increasedthe likelihood of vaginal delivery, lowered the risk ofCaesarean delivery, reduced the use of epidural analgesia,and improved Apgar scores and maternal satisfaction.39
Subgroup analyses showed that CLS was most effectivewhen the provider was not part of the hospital staff orfrom the women’s social network.40
Recommendation
5. Continuous labour support is recommended for allwomen in active labour. Each labour unit should aimto provide the opportunity for each woman to receivecontinuous 1-to-1 labour support. (I-A)
Amniotomy/artificial rupture of membranesAn RCT (n ¼ 752) comparing early amniotomy alone withexpectant care found no difference in the overall Caesareanrate or neonatal outcome. Even though there was a modestreduction in labour duration, investigators found morefrequent abnormal fetal decelerations and CS performed incases in which abnormal fetal surveillance was either theonly or contributing indication in the amniotomy group.41
These findings suggest that in settings in which diagnosisof abnormal fetal surveillance is based primarily on elec-tronic fetal monitoring, routine early amniotomy may in-crease CS for abnormal fetal monitoring. An updated 2013Cochrane review examined routine first stage amniotomy

Management of Spontaneous Labour at Term in Healthy Women
compared with no amniotomy in 5583 women whose la-bour started spontaneously and when labour becameprolonged.42 The findings showed no difference in thelength of the first stage labour, CS, maternal satisfaction, orApgar score less than 7 at 5 minutes, concluding thatroutine amniotomy should not be standard practice.
Early routine amniotomy and oxytocin augmentation werecompared for the prevention or treatment of dystocia in a2013 Cochrane review. The primary analysis that includedall trials showed no difference in the risk of CS. However,subgroup analyses found that the use of amniotomy andoxytocin for slow labour progress in unselected womenundergoing normal spontaneous labour were associatedwith a modest reduction in the CS rate and labourduration.43
In normally progressing labour, routine amniotomy is ofquestionable benefit and may result in more frequentvariable decelerations in fetal heart rate. If amniotomy isperformed, it is necessary to ensure that the fetal head iswell applied to the cervix (not ballottable) to minimize therisk of cord prolapse. If these conditions have been met,the woman is free to ambulate after amniotomy.
Recommendation
6. Amniotomy and oxytocin, in addition to othermeasures, should be considered once a diagnosis ofdystocia has been made in either the first or secondstage of labour. (I-B)
Active Management of LabourThe active management of labour was originally defined asincluding clear criteria for the diagnosis of labour (regularcontractions with spontaneous rupture of membranes orcomplete cervical effacement), routine amniotomy in la-bour, close attention to progress in labour, and liberal useof high-dose oxytocin if cervical dilatation was less than 1cm/hour. Observational studies by the initial advocates ofactive management demonstrated lower CS rates, a lowerincidence of prolonged labour, better neonatal outcomes,and improved maternal satisfaction.44 Subsequent follow-up observational studies also supported these results.45,46
Active management requires more interventions and cre-ates a more medicalized birth process. A 2013 Cochranereview stated “Active management is associated with smallreductions in the CS rate, but is highly prescriptive andinterventional. It is possible that some components of theactive management package are more effective than others.We therefore suggest that the term ‘active management of
labour’ should not be used unless all components of thepackage of care were applied as originally described.Further work is required to determine the acceptability ofactive management to women in labour.”47
Summary Statement
2. In low-risk nulliparous women in the active phase oflabour (i.e., equal to or greater than 4 cm dilatation),progress of cervical dilation greater than or equal to0.5 cm/hour is considered normal. (II-2)
Comfort Measures and Pain ReliefLabour hurts. Using the McGill pain scale, the average painin labour equals that of amputation of a digit. Womenexperience a wide range of pain during labour. The severityand tolerance of pain are unique to each labouring womanand cannot be predicted reliably prior to the occurrence ofpain. Because pain and a woman’s response to it are in-dividual, women need to be aware of a variety of strategiesto assist with their management of pain. Using a pain scaleto assess pain during labour helps to determine the needfor offering interventions and the effectiveness of thoseinterventions. It has been suggested that in addition to apain scale, a coping scale be used. This differentiates thosewomen able to cope with significant pain from thoserequiring intervention.48
Some women in labour reach the limit of their paintolerance. Women experiencing excessive pain or anxietyhave high endogenous catecholamines.49,50 This producesa direct inhibitory effect on uterine contractility and es-tablishes a vicious circle of poor uterine progress, leadingto increased anxiety, leading to increased catecholamines,and leading to further impairment of progress. The reliefof pain by effective support and analgesia may allow forrelease of the uterus from the constraints of the endoge-nous catecholamines and allow for progress in labour.High endogenous catecholamine levels may adverselyaffect uterine blood flow and therefore fetal oxygenation.
The management of pain during labour involves more thanthe simple and timely administration of the best anestheticagent available. Successful control of pain during labourrequires active management of the entire process. This painmanagement should begin with prenatal education andcounselling. Measures to enhance comfort and reduceapprehension are required for the care of all women inlabour. If appropriate measures are used early in the pro-cess of labour, analgesic needs decrease. Health care pro-viders who care for women in labour need to be awareof all the available options for the prevention and
SEPTEMBER JOGC SEPTEMBRE 2016 l 851

SOGC CLINICAL PRACTICE GUIDELINE
management of pain. When the health care team un-derstands the indications, possible variations, and potentialside effects, the woman and her family are able to makechoices in a less stressful environment.
Non-pharmacologic pain reliefA 2006 Cochrane review on complementary and alterna-tive therapies for labour pain management showed benefitsin pain reduction from self-hypnosis and acupuncture.However, the study results were limited by small samplesize. The efficacy of acupressure, aromatherapy, audioanalgesia, and massage has not been established. Therequirement for more 1-to-1 care in these situations mayhave influenced outcomes.51
A 2009 Cochrane review on TENS reported that womenreceiving TENS were less likely to report severe pain andmost would use it again; however, there was no differencein pain scores, mode of delivery, duration of labour, use ofother analgesia, or augmentation of labour.52 The analgesiceffect of TENS was found to be weak.53
A 2009 Cochrane review of 12 RCTs evaluated immersionin water during labour. Water immersion was found tosignificantly reduce the use of epidural/spinal/paracervicalanalgesia and result in shorter duration of first stage labouramong women compared with control patients. There wasa reduction in the duration of the first stage of labour withno difference in assisted vaginal deliveries, CS, oxytocinuse, perineal trauma, or maternal infection. Similarly, nodifference was found in Apgar score less than 7 at 5 mi-nutes, neonatal unit admissions, or neonatal infection rates.There was insufficient evidence about water immersion inthe second stage of labour. Further research wasrecommended.54
A 2009 systematic review of 828 women found that thoserandomized to intracutaneous sterile water injectionsexperienced significantly reduced visual analogue scale painscores for up to 2 hours and a reduced CS rate (4.6%)compared with a saline comparison group (9.9%). How-ever, the heterogeneity and quality of trials were weak, andthe authors recommended a large RCT to validate theirfindings.55 Additional Cochrane review of intracutaneousinjection of sterile water was found not to be effective forlow back or any other labour pain.56
Recommendations
7. Women and health care providers should haveinformation about coping strategies for early labourand mechanisms for accessing support fromcaregivers. (III-A)
852 l SEPTEMBER JOGC SEPTEMBRE 2016
8. When appropriate, health care providers shouldsupport women in their choice of analgesic options inlabour. These may include pharmacological and non-pharmacological measures. (III-A)
9. Each woman should be provided with evidence-basedinformation about labour analgesia options prior tothe onset of labour and offered ample opportunity todiscuss the risks and benefits of each option availableat her planned site of delivery. (III-A)
Pharmacological methodsdsystemicProviding satisfactory and effective pain relief in labour is aprimary responsibility of the health care team. Havingthorough knowledge of the pharmacology of the drugsused during labour is necessary to promote appropriateand satisfactory care and to limit side effects. It is impor-tant to understand the following:
� Sedative and hypnotic drugs do not provide pain reliefand may increase respiratory depression when given inconjunction with opioids. However, in women with highlevels of anxiety not alleviated by support and reassurance,sedative drugs can reduce episodes of nausea/vomitingand enhance the analgesia obtained with opioids.
� Anticholinergic side effects are common with anti-emetics and sedatives, and care should be directed atrecognizing and addressing discomforts.
� No drug is devoid of maternal or fetal side effects. Withalmost all pharmaceutical therapies, some amount of thedrug reaches the fetus. This may interfere with thesuccess of breastfeeding.
� Although all opioids provide analgesic effects, someopioids have active metabolites that may have a veryprolonged half-life in the newborn (e.g., meperidine).
� Women can be medicated with opioids or an inhalationalagent just before birth without causing significant res-piratory depression in the newborn.
When the health care team understands the indications,limitations, and side effects of these drugs, adversematernal and fetal outcomes can be minimized. Ideally, thecare provider should discuss options and provide writteninformation and links to other sources of information, inappropriate languages, regarding medications, possiblevariations, and potential side effects during the antenatalperiod. This allows the woman and her family the oppor-tunity to make decisions in a less stressful environment.When labour occurs, appropriate and individually desirednon-pharmacological or pharmacological agents may beused.

Management of Spontaneous Labour at Term in Healthy Women
Nitrous oxide. Entonox is a mixture of 50% nitrous oxideand 50% oxygen that provides mild to moderate analgesia.It must be self-administered for safety reasons via ademand-valve and used with scavenging in a well-ventilatedroom for workplace safety.57 Deep inhalation should beginas soon as the woman is aware of the onset of acontraction for maximal benefit. It is often useful for thewoman who has coped well until transition and then re-quires some form of analgesia for a short time. It may alsobe used as an adjunct during other procedures, such asplacement of a pudendal block or perineal repair.
Opioids. Opioids are widely used in many centres. A varietyof options are available, and opioids may be given intra-muscularly, subcutaneously, or by repeated IV boluses,including patient-controlled administration. The IV routehas the advantage of a rapid effect when needed. Opioidsmay be usefully combined with an antiemetic. A 2010Cochrane review found that parenteral opioids provide somepain relief in labour and were associated with maternal sideeffects of nausea, vomiting, and drowsiness. Overall, thetrials were of low quality evidence. There was insufficientevidence to recommend which opioid drug provides the bestpain relief with the least adverse outcomes.58
A number of studies have reported on the negativeneonatal effects of opioids with a longer half-life (e.g.,meperidine).59e61 The negative effects are based on the activemetabolite half-life in the newborn that may last 2 to 3 daysandmay include respiratory depression and neurobehaviouraloutcomes affecting regulation of states of consciousness andreflexes.59,60 The use of meperidine is discouraged, whereasother opioids with a shorter half-life, such as morphine orfentanyl, are preferred. It is important to note that eventhough fentanyl is a short-acting opioid, it has a long half-lifeonce maximum doses have been used.
When pharmacological agents are used for pain controlduring labour, guidelines regarding their safe and effectiveuse should be available for all staff. These guidelinesshould include the method of action, average andmaximum doses, possible maternal and fetal side effects,precautions for use, and resuscitative measures for eachdrug. When any opioid is used, an opioid antagonist (e.g.,naloxone) and resuscitation capabilities should be available,with a clear protocol on how to administer the naloxone,including appropriate dosing (because complete reversal ofanalgesia is not a desired outcome).
Summary Statement
3. Each labour unit should have a guideline for opioiduse during labour that includes the method of action,
average and maximum doses, route of administration,possible maternal and fetal side effects, precautions,and opioid antagonists and resuscitative measures foreach drug. (III)
Peripheral nerve blocks. The local anesthetic agents typicallyused for labour analgesia are lidocaine and bupivacaine.Providers using these agents need to be knowledgeableabout the maximum safe doses, how to calculate the dose,and the signs/symptoms of early local anesthetic toxicity.Action should be taken to prevent toxicity with all localanesthetics. Protocols for managing local anesthetic toxicityshould be in place.62
Pudendal nerve blocks. Pudendal nerve blocks are used foranalgesia of the perineum in the second stage of labour.This form of analgesia can be very useful and should beconsidered when other regional analgesia is not available.Local anesthesia with epinephrine allows for the safeadministration of larger volumes of anesthetic, leading togreater effectiveness as the epinephrine limits the peaksystemic levels in the mother and therefore the amounttransferred to the fetus. An injection of 10 mL of 1%lidocaine or equivalent is made in 2 locations through orjust inferior to the sacrospinal ligament, just medial to theischial spine on each side. The effect is usually felt within 3to 4 minutes.63
Perineal infiltration. Perineal infiltration is used for repairof lacerations and episiotomy. Generous and widespreadinfiltration should be used. Use of an agent withepinephrine is helpful. Care should be taken to not injectintravascularly or exceed the maximum dose. Themaximum dose of plain lidocaine is 4 to 5 mg/kg or asingle dose of 300 mg of a 1% solution. The maximumdose of lidocaine with epinephrine is 7 mg/kg or a 500 mgsingle dose (Table 3).62
Regional analgesia/anesthesia
Epidural block. Epidural block can provide effective painrelief throughout all stages of labour and delivery. Thehormonal response to pain includes a rise in endogenouscatecholamines. The effective relief of pain lowersepinephrine concentrations and may result in improveduterine contractions and possibly improved placentalperfusion. A particular benefit of epidural analgesiaexists for women with labour dystocia and who requireaugmentation. Effective pain relief may increase theacceptance of augmentation and the likelihood of subse-quent vaginal delivery.
SEPTEMBER JOGC SEPTEMBRE 2016 l 853

SOGC CLINICAL PRACTICE GUIDELINE
A2011Cochrane review involving 9658women showed thatcompared with an opiate or no analgesia, epidural analgesiaprovided superior pain relief in labour, a small decrease inneonatal acidosis, and less need for naloxone. However,epidural analgesia was associated with increased risk ofassisted vaginal birth, maternal hypotension, motorblockade, maternal fever, urinary retention, longer secondstage of labour, oxytocin administration, and increased riskof CS for fetal distress.64 There was no significant differencein overall risk of CS, long-term backache, Apgar score lessthan 7 at 5 minutes, and maternal satisfaction with pain re-lief.64 A separate 2012meta-analysis of RCTs involving 4667women showed increased neonatal septic workup and anti-biotic treatment in women receiving epidural analgesia.65,66
Even though it provides excellent pain relief, epiduralanalgesia often slows second stage labour and results inmotor blockade, which interfere with mobility andmaternal pushing efforts.
Modern epidural techniques use lower concentration of localanesthetics (0.1% or less) than those used previously (up to0.25%). In a meta-analysis of 2000 women, low-dose epi-durals were as effective as high-dose epidurals at relievingpain but were less likely to cause motor blockade and urinaryretention or to interfere with ambulation.67 Compared withlow-dose epidurals, high-dose epidurals are more likely tocause prolongation of the second stage of labour. This maybe due to blockage of the natural increase in endogenousoxytocin that occurs in the second stage. Oxytocinaugmentation may be necessary if contractions are infre-quent or ineffective. Relaxation of the pelvic floor muscu-lature may result in persistent fetal head malposition. Low-dose epidurals are preferred because they lead to less mo-tor blockade and therefore lessmalposition, a shorter secondstage of labour, and less hypotension. Women who receivedlow-dose epidurals were less likely to require assisted vaginalbirth, although there was no difference in the CS rate.67
Maintaining an upright position and mobility during labourhas been shown to be beneficial in promoting vaginal birth.Mobility is associated with greater maternal satisfactionwhen a labour epidural is providing analgesia, although thatmay be due to the typical manner of managing a mobilelabour epiduraldwith PCEA. Mobility does not neces-sarily mean freely ambulating; it means labouring in a non-recumbent position, attempting to void spontaneously, andusing a non-lithotomy delivery position. Ambulation, perse, with a labour epidural has not been shown to alter birthoutcome; however, all of the studies were flawed by thefact that few women actually ambulated for a significantperiod following epidural insertion.68 Weiniger et al.69
noted that women who received a low-dose epidural and
854 l SEPTEMBER JOGC SEPTEMBRE 2016
who were encouraged and able to ambulate to the toiletduring labour had a significantly improved ability to emptythe bladder, avoiding urinary catheterization.
Promoting mobility may be more beneficial than focusingon actual walking after receiving an epidural. Allowing formobility means tailoring the labour epidural to minimizemotor blockade. Even though no “ideal” epidural solutionmixture or PCEA program has been found, the basicprinciples include the following: low-dose local anesthetic/opioid mixture with a low background infusion andgenerous patient-controlled bolus function to maintainanalgesia without causing cumulative motor blockade.70
PCEA has been shown to produce greater maternalsatisfaction and excellent analgesia despite the use of low-dose/very low-dose epidural solutions compared withtraditional continuous epidural infusion. A 2002 meta-analysis of 9 studies (n ¼ 640) demonstrated a loweranesthetic dose and less motor blockade with PCEAcompared with continuous epidural infusion.71
A 2011 RCT demonstrated lower overall local anestheticdose, less motor blockade, and fewer operative vaginal de-liveries with programmed intermittent bolus administrationversus continuous epidural infusion of a local anesthetic.72
A 2009 randomized trial of 12 793 nulliparous womenreported that epidural initiation early in the first stage ofspontaneous labour (cervical dilatation of at least 1.0 cm)does not seem to prolong labour or increase the CS ratecompared with later initiation at a cervical dilatation of 4.0cm or greater).73 A systematic review of over 15 000nulliparas compared early versus late initiation of labourepidural; early epidural was administered prior to 4 to 5cm, whereas late epidural was administered after 4 to 5 cmcervical dilatation. The investigators found no difference inall measured outcomes, including CS, instrumental births,duration of second stage of labour, Apgar scores, andumbilical arterial or umbilical venous pH.74
Summary Statement
4. Epidural analgesia provides the most effective painrelief for women in labour. The timing of initiation oflabour epidural is dependent on the woman’s choiceonce the diagnosis of labour has been established. (I)
Recommendations
10. The use of meperidine as labour analgesia should beavoided due to its long-acting active metabolites andnegative effects on neonatal behaviours. (II-2B)

Management of Spontaneous Labour at Term in Healthy Women
11. Low dose epidural, when available, is preferred overhigh dose epidural for labour analgesia and inpromoting mobility in labour. (I-A)
12. Women who receive an epidural should beencouraged to maintain mobility and flexibility inpositions of comfort throughout labour. (I-B)
SECOND STAGE LABOUR MANAGEMENT
Position in Second Stage of LabourA 2005 meta-analysis reported limited studies (n ¼ 281)comparing the upright versus recumbent position in the sec-ond stage of labour.With anupright position, therewas a non-significant reduction in instrumental andCaesarean births anda statistically significant reduction in labour duration.75 TwoCochrane reviews compared upright versus the recumbentposition in the second stage of labour in women who did ordid not receive epidural analgesia. No difference in outcomeswas found for women who received epidural analgesia,although the sample size was small. For women without anepidural, upright posture reduced the risk of operative vaginaldeliveries, episiotomy, and abnormal fetal heart rate patternbut increased the likelihood of second-degree perineal lacer-ation and blood loss over 500 mL.76,77
Epidural AnalgesiaContinue the epidural. Discontinuing an epidural in thesecond stage of labour to allow “effective” pushing oftenresults in the sudden return of pain. This practice may beworse than if no relief had been provided at all. The womanmay become so distressed by the pain that she cannot pusheffectively. Maintaining the epidural does not significantlyincrease the incidence of assisted vaginal birth.78,79 A sec-ondary analysis of early versus late pushing in an RCTrevealed an increased incidence of Caesarean birth, mid-pelvic procedures, and third- and fourth-degree tears forwomen who reported suboptimal pain control during thesecond stage of labour in the early pushing group.80
Recommendation
13. Once an epidural has been established, the infusionshould be continued until completion of the thirdstage of labour. (I-A)
Table 3. Maximum dose of local anesthetic peripheral nerve b
Agent Lidocaine Lidocaine with epin
Dose 4 to 5 mg/kg 7 mg/kg
Maximum single dose 300 mg 500 mg
NOTE: Conversion formula % to mg/mL: multiply the % concentration by 10 (i.e., 1%
Delayed Pushing
The 2000 PEOPLE trial randomized 1862 nulliparouswomen who received an epidural at full dilatation to im-mediate pushing or delayed pushing for a maximum of 2hours. Women in the delayed pushing group experiencedmore spontaneous and fewer difficult births. This wasmost marked in women whose babies were abovestation þ2 (zero station at the level of the ischial spines) orin a non-occiput anterior position during the early secondstage.81,82 In women who do or do not receive epiduralanesthesia, waiting up to 2 hours prior to the onset ofpushing is appropriate in the presence of continueddescent of the head and fetal and maternal status aresatisfactory.82,83Duration of PushingThere is a lack of quality evidence on defined time limitsfor the active second stage once it has commenced. Severalcohort studies examining the duration of the second stageof labour found no evidence of adverse neonatal outcomesor increased maternal morbidity and operative deliverieswith longer second stages.84e86 However, most studies didnot distinguish between the passive and active phases ofthe second stage of labour. It appeared that the duration ofactive pushing has more direct impact on maternal andneonatal outcomes than does the total duration of thesecond stage of labour.87,88 In light of these findings,documentation of the time of the onset of active pushing isimportant; it is reasonable that hourly reassessment ofprogress in fetal descent and rotation should be made todetermine whether intervention or assisted birth isrequired. Table 483,89 describes the recommended practicesfor pushing by parity and use of epidural anesthesia.Oxytocin administration may be indicated if there is evi-dence of slow or lack of progress or when contractions areassessed as being inadequate (e.g., < 200 Montevideounits).
Total Duration of the Second Stage of LabourMenticoglou et al.90 studied the duration of the secondstage of labour and perinatal outcomes. They found noassociation between the duration of the second stage oflabour and low Apgar scores at 5 minutes, neonatal sei-zures, or admission to neonatal intensive care units.Limited evidence makes it difficult to a set time limit for
locks and infiltration
ephrine Bupivacaine Bupivacaine with epinephrine
2.5 mg/kg 3 mg/kg
175 mg 225 mg
¼ 10 mg/mL).
SEPTEMBER JOGC SEPTEMBRE 2016 l 855

Table 4. Recommended practices in second stage of labour by parity and use of epidural analgesia (after full cervicaldilatation and when power is adequate)
Nulliparous Parous
No epidural Epidural No epidural Epidural
Total duration* 3 hours 4 hours 2 hours 3 hours
Passive second stage† May wait up to 2 hours beforepushing, particularly when thepresenting part is above þ2station or in an non-OAposition and the urge to push isabsent. Encourage waiting toallow passive descent.
May wait up to 1hour
May wait up to 2 hours before pushing,provided continued passive descent
Commence pushing When urge to push presentand not able to allow passivedescent orAfter 2 completed hours ofpassive second stage
When urge to push present orAfter 2 completed hours of passive second stage
Assessment Hourly for descent and position. Reassess the need for assisted birth after 2 hours of active pushing.
OA: Occiput anterior.
*Continuing beyond the following time limits should be carefully evaluated, and consideration should be given to expedite delivery. Extending these time limits may beappropriate in the presence of continued descent of the head, when maternal status and fetal surveillance are normal, and when spontaneous vaginal birth is imminent.
†Waiting for up to the period indicated prior to the onset of pushing is appropriate in the presence of continued descent of the head and if fetal and maternal conditionsare satisfactory.
Sources: SpragueA,Oppenheimer L,McCabeL,Brownlee J,Graham I, DaviesB. TheOttawaHospital’s clinical practice guideline for the second stage of labour. JObstetGynaecol Can 2006;28:769e79.83 Perinatal Services BC. Core competencies for management of labour: evaulation of progress of labor/dystocia. Perinatal Services BC;2011. Available at: http://www.perinatalservicesbc.ca/Documents/Guidelines-Standards/Standards/Competencies/4CoreCompDSTEvalofLabourDystocia.pdf.Accessed January 23, 2013.89
SOGC CLINICAL PRACTICE GUIDELINE
the duration of the second stage of labour. It is suggestedthat assessment of maternal status, fetal status, and rate ofdescent should be the basis of individualizing appropriatemanagement. It is reasonable to consider interventionwhen there is no further descent of the fetus despite op-timum uterine contractions and maternal expulsive efforts.
The effect of pre-pregnancy BMI on the duration of thesecond stage of labour is unclear. Some authors reportedno significant difference in duration of the second stage oflabour by BMI,25,91e94 whereas other studies have re-ported a reduced length of the second stage in obesewomen.19,95 The interpretation of any estimates based onsecond stage characteristics is challenging. This is becausethe group of women that progresses to the second stage oflabour excludes women who had a Caesarean deliveryduring the first stage. Thus, any observed differences incharacteristics between obese and non-obese women in thesecond stage may be due to selection factors, limiting thegeneralizability of findings.
Recommendations
14. Pushing, as a component of second stage progress,may commence when the cervix is fully dilated, thepresenting part is confirmed to be engaged, and thewoman feels an urge to push. (III-A)
856 l SEPTEMBER JOGC SEPTEMBRE 2016
15. Delayed pushing is preferred when the woman hasno urge to push, particularly if the presenting part isabove station þ2 and/or in a non-occiput anteriorposition, assuming the fetus does not displayabnormal monitoring and the pregnant woman’sstatus is satisfactory. (I-A)
16. Delay of pushing according to parity and thepresence or absence of an epidural should follow thetime limits described in the text unless there areextenuating circumstances. (II-2B)
17. The method of pushing, spontaneous or directedwith Valsalva manoeuvre, should be chosen by thewoman’s own preference. Directed pushing mayassist with the final expulsion of the head. (II-2B)
METHOD OF PUSHING
A meta-analysis of 3 trials comparing Valsalva and spon-taneous pushing in 425 nulliparous women who did notreceive labour epidural found no difference in rates ofoperative deliveries, perineal repair, and PPH. For theValsalva technique, a woman is instructed to take a deepbreath at the start of the contraction and hold her breathand push hard for the duration of the contraction. In thespontaneous pushing method, the woman is self-directed

Management of Spontaneous Labour at Term in Healthy Women
and may push with an open glottis, using an intermittentexhalation or vocalization technique. Although a significantreduction in duration of second stage labour by 18.59minutes was found in the Valsalva group, the mean dif-ference diminished to 9.75 minutes after sensitivity ana-lyses. Women who used Valsalva pushing showed asignificant decrease in urodynamic factors in first urge tovoid and bladder capacity measured at 3 months post-partum. There were no differences in other importantmaternal and newborn outcomes. The authors concludedthat the Valsalva pushing technique should not be routinelyused until more evidence is available.96
EPISIOTOMY AND PERINEAL MANAGEMENT
A 2009 Cochrane review of 8 studies related to episiotomyfor vaginal birth concluded that restrictive episiotomypolicies appear to have a number of benefits comparedwith routine episiotomy policies. There was less posteriorperineal trauma, less suturing, and fewer complications,with no difference for most pain measures or severevaginal and/or perineal trauma. However, there was anincreased risk of anterior perineal trauma with a restrictiveepisiotomy policy.97 When the perineum is preventing de-livery, particularly if the fetal heart rate is abnormal, anepisiotomy may expedite a vaginal birth, although this hasnot been examined prospectively.
Although routine episiotomy has been shown to causemore harm than good, selective mediolateral episiotomyshould be considered in women who are considered at anincreased risk of OASIS, such as nulliparous womenrequiring assisted vaginal birth or those with a history ofprior OASIS. Randomized evidence is limited98 but cor-roborates observational evidence that more liberal (but notroutine) use of mediolateral episiotomy prevents OASIS atassisted vaginal births, particularly with forceps.99e101
The angle at which a mediolateral episiotomy is cut isimportant. An observational study showed that the angleof an episiotomy from midline when performed atcrowning decreased by 20 degrees on average after de-livery.102 An episiotomy performed at 45 degrees leaves anincision after delivery at 25 degrees from midlinedveryclose to the anal sphincter. To avoid causing OASIS, anepisiotomy should be performed more than 60 degreesfrom midline when the head is crowning (i.e., less than 30degrees from horizontal). Midline episiotomy increases therisk of anal sphincter injury.
Quality improvement efforts in large regions of Norwayover the past decade have succeeded in reducing theincidence of OASIS from 4% to less than 2%.103 The key
components have been controlled, slow delivery of thecrowning fetal head and selective use of mediolateralepisiotomy.
A 2011 Cochrane review (n ¼ 1525) of warm perinealcompresses in labour versus no intervention showed areduction in third- and fourth-degree perineal tears from5% to 2.5%.104 Investigators also found no difference inthe reduction of perineal trauma between a hands-on andhands-off technique on the perineum. Due to the highclinical heterogeneity and poorly described perineal tech-niques in the studies, it was not possible to conductplanned analyses on outcomes. The only common themewas that a slow, controlled delivery of the fetal head wasused to facilitate delivery.
Recommendation
18. Avoid the use of routine episiotomy in spontaneousvaginal births. (I-A)
Perineal RepairA 2010 Cochrane review involving 10 171 womendemonstrated decreased pain and need for re-suturing withsynthetic versus catgut suture material for episiotomy andperineal tear repairs. Rapidly absorbable synthetic sutureneeded to be removed less often than did regular syntheticsuture. There were no differences in long-term pain ordyspareunia.105
A 2012 Cochrane review involving 8184 women demon-strated decreased analgesia use, less pain for up to 10 days,and reduced need for suture removal with continuousversus interrupted perineal repair technique. There was nodifference in long-term pain or need for re-suturing.106
A randomized trial of 147 women with OASIS found thata single 1 g IV dose of cefotetan or cefoxitin given duringrepair reduced the incidence of perineal complicationsfrom 24% to 8% (P ¼ 0.037).107 The evidence in this 1study may not be sufficient to recommend routine antibi-otic prophylaxis for third- and fourth-degree lacerationsafter delivery.
THIRD STAGE LABOUR MANAGEMENT
AMTSL involves a package of interventions that includesadministering prophylactic uterotonics, early cord clamp-ing, and CCT to assist in placental expulsion and to preventor reduce blood loss. Personnel with the training and skillsto actively manage the third stage of labour should be inattendance. Even though an SOGC guideline recom-mended AMTSL as a package of care in 2009, the package
SEPTEMBER JOGC SEPTEMBRE 2016 l 857

SOGC CLINICAL PRACTICE GUIDELINE
of 3 interventions is no longer recommended for allwomen.108 A 2015 Cochrane review of AMTSL involving8247 women, in all but 1 high-income countries, found thatcompared with expectant management, active managementdemonstrated a reduction in PPH of more than 1000 mLand in the maternal hemoglobin level of less than 9 g/dL at24 to 72 hours after delivery, regardless of the woman’sbleeding risk profile. Although AMTSL reduced the risk ofbleeding greater than 1000 mL and blood transfusions in amixed risk population, it also demonstrated a statisticallysignificant increase in postpartum hypertension, pain, andreturn to the hospital due to bleeding. In addition, AMTSLis associated with a lower average birth weight, likely as aresult of reduction in the neonate’s blood volume fromearly cord clamping.109 No statistical difference was iden-tified between the groups in the mean length of the thirdstage of labour, manual or surgical removal of retainedproducts, or maternal blood transfusion. Overall, high-quality evidence was lacking and more studies areneeded. The authors concluded that AMTSL carried bothbenefits and harms and that the individual components ofAMTSL should be evaluated separately to determinewhether all components are required to reduce PPH orwhich component confers the most benefit.109
Routine Use of Prophylactic UterotonicsRecent evidence in a 2013 Cochrane review of 20 trialsinvolving 10 806 women showed that prophylacticoxytocin at any dose decreases both PPH greater than 500mL and the need for therapeutic uterotonics comparedwith placebo and ergot alkaloids.110 Prophylactic oxytocinis preferred over ergot alkaloids for prevention of PPHbecause it has minimal side effects. The benefit of pro-phylactic oxytocin in reducing PPH greater than 500 mLwas found regardless of the route of delivery, the man-agement of the third stage labour, or the dose of oxytocingiven. The benefits of prophylactic oxytocin associatedwith decreased use of therapeutic uterotonics was seenonly in trials in which oxytocin was given in the context ofAMTSL, delivered intravenously, and administered as a 10IU dose slow IV bolus. If an IV is not available, anintramuscular dose of 10 IU offers similar clinical benefitin reducing blood loss greater than 500 mL and a non-significant trend in reduced use of therapeutic utero-tonics.110 Prophylactic oxytocin administered as an IVinfusion is preferred over a rapid bolus IV due to potentialadverse maternal cardiovascular effects and potentialplacental separation but retention due to entrapment. Theeffect of the timing of oxytocin administration as a pro-phylactic to prevent PPH was studied in a 2010 Cochranereview of 3 trials involving 1671 women. Investigatorsfound that administration of oxytocin before and after the
858 l SEPTEMBER JOGC SEPTEMBRE 2016
delivery of the placenta does not affect the risk of PPHgreater than 500 mL, rate of retained placenta, third stagelabour duration, and use of additional uterotonics.111
Controlled Cord TractionAfter delivery of the baby, the uterus continues to contract.Once there is evidence of placental separation, traction isapplied to the umbilical cord with counter pressure to thesuprapubic area on the uterus until the placenta delivers.Until recently, CCT was not studied independently inrelation to the prevention of PPH. A 2015 Cochrane re-view involving 27 665 women showed that CCT is asso-ciated with reduced blood loss of 500 mL or more and lessmanual removal of the placenta; the latter occurred mainlyin settings in which ergometrine was used routinely in thethird stage of labour. Although CCT can be routinelyoffered during the third stage of labour, the authorscautioned that it should only be applied in settings in whichthe birth attendant has the necessary skills.112
Timing of Cord ClampingIt appears that the adverse effects of reduced placentaltransfusion can be decreased if late cord clamping ispractised and is equally beneficial in both term and pretermbirths. Delaying cord clamping by at least 60 to 180 sec-onds is associated with less need for transfusion for ane-mia, less intraventricular hemorrhage, and less risk ofnecrotizing enterocolitis in non-resuscitated premature in-fants under 37 weeks’ gestation compared with immediateclamping.113
In a 2013 Cochrane review that included a total of 3911women and neonates at term, late cord clamping (> 60seconds) was associated with enhanced hemoglobin levelsand iron stores in infants for up to 6 months comparedwith the early cord clamping (< 60 seconds) group. Therewere no significant differences in maternal outcomes interms of severe PPH or blood loss greater than 500 mL.Although fewer neonates in the early cord clamping grouprequired phototherapy for jaundice, in settings where thereis ready access of phototherapy for treatment of jaundice,the authors concluded that late cord clamping is warrantedfor healthy term infants.114
Recommendations
19. Prophylactic oxytocics should be given after thedelivery of the baby. (I-A)
20. In term and preterm infants who do not requireneonatal resuscitation, delayed umbilical cordclamping for 60 seconds is recommendedirrespective of the mode of delivery. (I-B)

Management of Spontaneous Labour at Term in Healthy Women
DYSTOCIA
Dystocia is the most common problem associated withlabour and primarily affects nulliparous women. Eventhough the diagnosis of active labour requires assessmentof uterine activity and cervical status, the diagnosis ofdystocia first requires the confirmation of active labour. ADublin study demonstrated a decrease in dystocia whenactive management of labour principles were followed,including the use of specific criteria to diagnose labour toavoid inappropriate intervention in the pre-active labourphase.44 Dystocia cannot be diagnosed prior to the onsetof labour or during the latent phase of labour (before 4cm); CS carried out at this time for an indication ofdystocia is inappropriate.
Definition and Diagnosis of DystociaDystocia is defined as delayed or arrested progress in la-bour, irrespective of causes. Dilatation of less than 0.5 cm/hour over 4 hours or no cervical change over 2 hours inthe active first stage or greater than 1 hour of activepushing and no descent of the presenting part in the sec-ond stage is well below the 5th percentile for a popula-tion.2,115 It is associated with increased CS, maternal stressand anxiety, maternal infection, and PPH.
Recommendation
21. Dystocia should not be diagnosed prior to the onsetof the active phase of the first stage of labour orbefore the cervix is at least 4 cm dilated. (II-2D)
Table 5. Complications of Oxytocin
Adverseeffects Mechanism Prevention
Fetalcompromise
Tachysystole Correct dose
Uterinerupture
Tachysystole Correct dose
Waterintoxication
ADH effect Use crystalloid IV solution withconcentrated oxytocin to limit thevolume of water infused
Hypotension Vasodilatation Avoid IV bolus injection, including forAMTSL
ADH: Antidiuretic hormone.
Management of Dystocia in the First Stage ofLabourOxytocinIn the event of dystocia due to inadequate power despiteappropriate analgesia, hydration, and rest with or withoutamniotomy, oxytocin is indicated to achieve adequate con-tractions before operative delivery is considered.116,117 Prin-cipal concerns about the use of oxytocin are fetalcompromise and uterine rupture. It must be rememberedthat it is not oxytocin that causes the problem but ratherexcessive contractions. The correct use of oxytocin achievesadequate contractions while avoiding excessive uterine ac-tivity that could compromise the fetus or cause uterinerupture.
Even with close titration of oxytocin, excess uterine activitycan occur. All labour and delivery units must be preparedto manage uterine tachysystole whether or not it is asso-ciated with oxytocin use. This is outlined in the ClinicalPractice Guideline on the induction of labour.4
Complications of oxytocin. Table 5 describes possible com-plications of oxytocin administration, their mechanism ofoccurrence, and the preventive management associatedwith the use of oxytocin.
Sensitivity to oxytocin. Each woman’s uterus varies in itssensitivity to oxytocin. Even in the same uterus, thesensitivity may change during the course of labour. Thedose used must be sufficient to achieve adequatecontractions. Protocols or guidelines for the adminis-tration of oxytocin vary, but many suggest starting witha low dose followed by small increments at intervals of30 minutes.118,119 The starting incremental dosages foraugmentation may be less than those used for induc-tion. Every obstetrical unit must have an identified andaccessible protocol that includes a starting dose,increment interval, and maximum dose. Consistent useof one standard method to infuse oxytocin in any oneobstetrical unit is recommended.120,121 The doseshould be ordered and recorded as milliunits/minute,not as volume of infusion. For example, an obstetricalunit may administer an infusion solution of 30 U ofoxytocin in 500 mL saline; thus the dose of oxytocin inmilliunits/minute equals the volume of infusion inmL/hour. Therefore, conversion calculations of dose tovolume of the infusion pump need not be performed.Electronic fetal monitoring should be initiated orcontinued when oxytocin is started.
IV oxytocin can be administered using a low- or high-doseprotocol. The choice of protocol should be based on therelative risks of uterine rupture, sensitivity to oxytocin, andthe likelihood of placental compromise. Any oxytocinprotocol used should be assessed against uterine responseand the fetus’s tolerance of associated contractions. If anearly adverse uterine response (tachysystole) is noted with ahigh-dose protocol, then a low-dose protocol should beused.
SEPTEMBER JOGC SEPTEMBRE 2016 l 859

Table 6. Clinical considerations for oxytocinaugmentation protocol
Clinical considerations Suggested oxytocin protocol
Prior CS Low dose
Fetal growth restriction Low dose
Parity > 4 Low dose
Parous augmentation, no epidural Low dose
Parous induction Low or high dose
Parous augmentation with epidural Low or high dose
Nullipara augmentation, no epidural Low dose
Nullipara induction Low or high dose
Nullipara with epidural Consider high dose
SOGC CLINICAL PRACTICE GUIDELINE
A 2010 meta-analysis of RCTs including 5400 womenconcluded that high-dose oxytocin protocols were associ-ated with a lower CS rate than were low-dose protocols.Tachysystole was more common with high-dose protocols,but there was no difference in maternal or neonatalmorbidity. Low dose was defined as 1 to 2 mU/min in-crements, and high-dose was defined as � 4 mU/minincrements.119 This meta-analysis was dominated bystudies that included only nulliparous women. Evidencespecific to parous women or women with a prior CS scar islacking. Therefore it may be prudent to use a low-doseprotocol in women labouring with a prior CS or otheruterine surgery because of a potential increase in the risk ofuterine rupture. It is also prudent to use a low-dose pro-tocol in grand multiparous women because of theirincreased sensitivity to oxytocin and women with suspectedfetal growth restriction due to risks of placental insuffi-ciency (Table 6).
Oxytocin and EpiduralThere is limited evidence to determine whether high-doseoxytocin regimens should be used for labour augmentationamong women who have received an epidural. One large,high-quality, contemporary observational study from theUnited States and several smaller RCTs compared high-and low-dose oxytocin augmentation protocols in womenwith high (67% to 94% and higher) epidural use.122e126
One of these trials evaluated high-dose oxytocin as partof an active management of labour intervention, decreasingthe applicability of the results.124
Based on available evidence, high-dose oxytocin for labouraugmentation has consistently been shown to shorten labourduration compared with low-dose oxytocin. In the largeobservational study, the first stage of labour in women whoreceived high-dose oxytocin (� 4 mU/min starting dose)
860 l SEPTEMBER JOGC SEPTEMBRE 2016
was shortened by 1.3 hours (95% confidence interval 1.0 to1.7 hours) compared with low-dose oxytocin (1 mU/minstarting dose) after adjusting for potential confounders.122
However, evidence on the relationship between high-doseoxytocin for labour augmentation and Caesarean deliveryis inconsistent. Although most studies reported a trendtowards lower Caesarean delivery rates in women whoreceived high-dose regimens,122e124,126 only 1 reached sta-tistical significance.126
Nulliparous women and women who receive an epiduralanalgesia during labour are particularly likely to benefitfrom high- versus low-dose oxytocin augmentation.127 Theclinical goal of oxytocin augmentation is to achieve aneffective uterine contraction mechanism of 4 to 5 con-tractions in 10 minutes. If an IUPC is used, the goal is 200or greater Montevideo units (e.g., 4 contractions of 50 to60 mmHg in 10 minutes).Several studies have examinedthe optimal duration of oxytocin augmentation when la-bour dystocia or arrest occurrs.128e130 A prospectivecohort study evaluated labour progress in 220 nulliparouswomen and 99 parous women who entered labour spon-taneously and subsequently were assessed as having un-satisfactory progress. Investigators found that in womenwho received oxytocin for a total of 8 hours, 38% deliveredvaginally. In nulliparous women, the CS rate was 18% after8 hours of oxytocin augmentation with no resultingadverse neonatal outcomes. Another study of over 500women evaluated a mandated protocol of 4 hours or moreof oxytocin augmentation before CS for active phase la-bour arrest. Investigators found that extending the mini-mum period of oxytocin augmentation from 2 to 4 to 6hours increased the vaginal delivery rate without severeadverse maternal or neonatal outcomes.129 This wasfurther corroborated in a similar study by the sameresearchers.130
Recommendation
22. Oxytocin augmentation should be titrated to avoidtachysystole or excessive uterine activity and toproduce a uterine contraction pattern of 4 to 5contractions in 10 minutes (200 Montevideo units).A minimum of 4 to 6 hours of adequate uterineactivity may be required to have the desired response.(I-A) It is recommended that every obstetrical unithave an identified and accessible protocol thatincludea a starting dose, increment interval, andmaximum dose. Consistent use of 1 standardapproach to oxytocin administration in any 1obstetrical unit should be considered. (III-A)

Management of Spontaneous Labour at Term in Healthy Women
Management of Dystocia in the Second Stage ofLabourProlonged second stageIn the presence of strong contractions, prolonged secondstage of labour may be defined by the following:
� Nulliparous women: 3 hours with regional anesthesia or2 hours without regional anesthesia
� Parous women: 2 hours with regional anesthesia or 1hour without regional anesthesia
If no urge to push occurs after 1 hour of the second stageof labour, reassess the contractions and fetal presentingposition and descent and consider the use of oxytocin ifcontractions are inadequate.
A population-based cohort analysis of 120 000 womenidentified an increase in the risk of maternal obstetricaltrauma, postpartum hemorrhage, puerperal febrilemorbidity, composite maternal morbidity, low 5-minuteApgar score, birth depression, admission to the neonatalintensive care unit, and composite perinatal morbidity asthe duration of the second stage surpassed 3 hours innulliparous women and 2 hours in parous women.131
Recommendations
23. Operative delivery less than 2 hours aftercommencing pushing is not recommendedprovided, maternal status and fetal surveillanceare normal. (III-D)
24. When the second stage exceeds the recommendedtime limits (see text), consideration should be givento expediting delivery. Extending these time limitsmay be appropriate in the presence of continueddescent the head, satisfactory maternal and fetalstatus, and imminent vaginal birth. (II-2B)
25. High dose regimens have been shown to decreaselabour duration compared with low dose regimens.(I-A) The lowest dose needed to produce normalprogress is recommended to reduce the riskof tachysystole or excessive uterine activity andcreate a uterine contraction pattern of 3 to 5contractions or 200 or more Montevideo unitsevery 10 minutes. (IA)
MANAGEMENT SUMMARY
Prevention of Dystocia
� Encourage the use of prenatal education.
� Avoid unnecessary/non-indicated induction of labour.
� Admit only women in the active phase of labour (seedefinition in the previous text) to the hospital.
� Provide continuous support with non-hospital associatedpersons to labouring women.
� Use appropriate analgesia.
Management of Dystocia
� Assess the adequacy of labour progress.
� Intervene when necessary.
B AnalgesiaB Rest
B Amniotomy
B Augmentation
� For women who received an epidural analgesia, if inad-equate labour progress is suspected, augment with earlyartificial rupture of membranes and IV oxytocin. A high-dose IV oxytocin protocol may be particularly beneficial.
� Intervene operatively when necessary.
SUMMARY
� Labour is a normal physiological process.
� Normal labour is enhanced with supportive care, delayedadmission until active labour, comfort measures,appropriate pain management, and interventions onlywhen necessary.
� There is an increasing trend towards induction of labourand an increase in CS primarily due to dystocia andrepeat CS.
� Dystocia can only be diagnosed once active labour isestablished.
Interventions for dystocia may include analgesia, rest,amniotomy, augmentation, and assisted vaginal birth.
REFERENCES
1. Induction and augmentation of labor. ACOG Technical Bulletin Number157dJuly 1991. Int J Gynaecol Obstet 1992;39:139e42.
2. Fraser WB, Krauss I, Boulvain M, Oppenheimer L, Milne KJ, Liston RM,Dystocia. SOGC Clinical Practice Guidelines, No. 40, October 1995.Available at: http://sogc.org/wp-content/uploads/2013/11/gui40EPS9510.pdf. Accessed May 5, 2016.
3. O’Driscoll K, Meagher D, Robson M. Active management of labour: theDublin experience. ed 4. London: Mosby; 2003.
4. Leduc D, Biringer A, Lee L, Dy J. Induction of labour. SOGC ClinicalPractice Guidelines, No. 296, September 2013. J Obstet Gynaecol Can2013;35:840e60.
SEPTEMBER JOGC SEPTEMBRE 2016 l 861

SOGC CLINICAL PRACTICE GUIDELINE
5. Friedman EA. Labor: clinical evaluation and management. ed 2. New York:Appleton Century Crofts; 1978.
6. Alexander JM, Sharma SK, McIntire DD, Leveno KJ. Epidural analgesialengthens the Friedman active phase of labor. Obstet Gynecol2002;100:46e50.
7. Zhang J, Troendle JF, Yancy MK. Reassessing the labor curve in nulliparouswomen. Am J Obstet Gyecol 2002;187:824e8.
8. Neal JL, Lowe NK, Ahijevych KL, Patrick TE, Cabbage LA, Corwin EJ.“Active labor” duration and dilation rates among low-risk, nulliparouswomen with spontaneous labor onset: a systematic review. J MidwiferyWomen’s Health 2010;55:208e318.
9. American College of Obstetricians and Gynecologists. Safe prevention ofthe primary Cesarean delivery. Obstet Gynecol 2014;123:603e711.
10. Peisner DB, Rosen MG. Transition from latent to active labor. ObstetGynecol 1986;68:448e51.
11. Bakker JJ, Verhoeven CJ, Janssen PF, van Lith JM, van Oudgaarden ED,Bloemenkamp KM. Outcomes after internal versus externaltocodynamometry for monitoring labor. N Engl J Med 2010;362:306e13.
12. Pattinson RC, Farrell EME. Pelvimetry for fetal cephalic presentations at ornear term. Cochrane Database Syst Rev 1997;(2):CD000161.
13. Taipale P, Hiilesmaa V. Predicting delivery date by ultrasound and lastmenstrual period in early gestation. Obstet Gynecol 2001;97:189e94.
14. Hunter S, Hofmeyr G, Kulier R. Hands and knees posture in late pregnancyor labour for fetal malposition (lateral or posterior). Cochrane Database SystRev 2007;(4):CD001063.
15. Gagnon AJ, Sandall J. Individual or group antenatal education for childbirthor parenthood, or both. Cochrane Database Syst Rev 2007;(3):CD002869.
16. Canadian Institute for Health Information. In due time: why maternal agematters. Canadian Institute for Health Information. 2011. Available at: https://secure.cihi.ca/free_products/AIB_InDueTime_WhyMaternalAgeMatters_E.pdf.Accessed on April 10, 2015.
17. Johnson JA, Tough S. Society of Obstetricians and Gynaecologists ofCanada. Delayed child-bearing. J Obstet Gynaecol Can 2012;34:80e93.
18. Smith GGS, Cordeaux Y, White IR, Pasupathy D, Missfelder-Lobos H,Pell JP, et al. The effect of delaying childbirth on primary cesarean rates.PLoS Med 2008;5:e144.
19. Vahratian A, Zhang J, Savitz DA, Siega-Riz AM. Maternal prepregnancyoverweight and obesity and the pattern of labor progression in termnulliparous women. Obstet Gynecol 2004;104(5 Pt 1):943e51.
20. Zhang J, Bricker L, Wray S, Quency S. Poor uterine contractility in obesewomen. BJOG 2007;114:343e8.
21. Pevzner L, Powers BL, Rayburn WF, Rumney P, Wing DA. Effects ofmaternal obesity on duration and outcomes of prostaglandin cervicalripening and labor induction. Obstet Gynecol 2009;114:1315e21.
22. Cedergren MI. Non-elective caesarean delivery due to ineffective uterinecontractility or due to obstructed labour in relation to maternal bodymass index. Eur J Obstet Gynecol Reprod Biol 2009;145:163e6.
23. Kjaergaard H, Dykes AK, Ottesen B, Olsen J. Risk indicators for dystocia inlow-risk nulliparous women: a study on lifestyle and anthropometricalfactors. J Obstet Gynaecol 2010;30:25e9.
24. Norman SM, Tuuli MG, Odibo AP, Caughey AB, Roehl KA, Cahill AG.The effects of obesity on the first stage of labor. Obstet Gynecol2012;120:130e5.
25. Hilliard AM, Chauhan SP, Zhao Y, Rankins NC. Effects of obesity onlength of labor in nulliparous women. Am J Perinatol 2012;29:127e32.
26. Kominiarek MA, Zhang J, Vanveldhuisen P, Troendle J, Beaver J,Hibbard JU. Contemporary labor patterns: the impact of maternal bodymass index. Am J Obstet Gynecol 2011;205:244.e1e8.
862 l SEPTEMBER JOGC SEPTEMBRE 2016
27. Lowe N, Corwin RJ. Proposed biological linkages between obesity, stress,and inefficient uterine contractiliy during labor in humans. MedHypotheses 2011;76:755e60.
28. BC Perinatal Health Program. Perinatal health report 2008. Vancouver: BCPerinatal Health Program; 2008.
29. Public Health Agency of Canada. Canadian perinatal health report. ed 2008.Ottawa: Public Health Agency of Canada; 2008.
30. Bailit J, Dierker L, Blanchard M, Mercer B. Outcomes of women presentingin active versus latent phase of spontaneous labor. Obstet Gynecol2005;105:77e9.
31. Holmes P, Oppenheimer L, Wen S. The relationship between cervicaldilatation at initial presentation in labour and subsequent intervention.BJOG 2001;108:1120e4.
32. Rahnama P, Ziaei S, Faghihzadeh S. Impact of early admission in labor onmethod of delivery. Int J Gynaecol Obstet 2006;92:217e20.
33. McNiven PS, Williams JI, Hodnett E, Kaufman K, Hannah ME. An earlylabor assessment program: a randomized, controlled trial. Birth1998;25:5e10.
34. Janssen PA, Still DK, Klein MK, Singer J, Carty EM, Liston RM, et al. Earlylabor assessment and support at home versus telephone triage: arandomized controlled trial. Obstet Gynecol 2006;108:1463e9.
35. Lavender T, Hart A, Smyth R. Effect of partogram use on outcomesfor women in spontaneous labour at term. Cochrane Database Syst Rev2013;(7):CD005461.
36. Lawrence A, Lewis L, Hofmeyr GJ, Styles C. Maternal positions and mobilityduring first stage labor. Cochrane Database Syst Rev 2013;(10):CD003934.
37. Singata M, Tranmer J, Gyte MG. Restricting oral fluid and food intakeduring labour. Cochrane Database Syst Rev 2013;(8):CD003930.
38. Bowers BB. Mothers’ experiences of labor support: exploration ofqualitative research. J Obstet Gynecol Neonatal Nurs 2002;31:742e52.
39. Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous support forwomen during childbirth. Cochrane Database Syst Rev 2013;(7):CD003766.
40. Sibley L, Ann ST. What can a meta-analysis tell us about traditional birthattendant training and pregnancy outcomes? Midwifery 2004;20:51e60.
41. Goffinet F, Fraser W, Marcoux S, Breart G, Moutquin JM, Daris M. Earlyamniotomy increases the frequency of fetal heart rate abnormalities.Amniotomy Study Group. Br J Obstet Gynaecol 1997;104:548e53.
42. Smyth R, Markham C, Dowswell T. Amniotomy for shorteningspontaneous labour. Cochrane Database Syst Rev 2013;(6):CD006167.
43. Wei S, Wo BL, Qi HP, Xu H, Luo ZC, Roy C, et al. Early amniotomy andearly oxytocin for prevention of, or therapy for, delay in first stagespontaneous labour compared with routine care. Cochrane Database SystRev 2013;(8):CD006794.
44. O’Driscoll K, Foley M, MacDonald D. Active management of labor as analternative to cesarean section for dystocia. Obstet Gyencol1984;63:485e90.
45. Peaceman AM, Lopez-Zeno JA, Minogue JP, Socol ML. Factors thatinfluence route of deliverydactive versus traditional labor management.Am J Obstet Gynecol 1993;169:940e4.
46. Thornton JG, Lilford RJ. Active management of labour: current knowledgeand research issues [published erratum appears in BMJ 1994;309(6956):704]BMJ 1994;309(6951):366e9.
47. Brown HC, Paranjothy S, Dowswell T, Thomas J. Package of care for activemanagement in labour for reducing caesarean section rates in low-riskwomen. Cochrane Database Syst Rev 2013;(9):CD004907.
48. Simkin P, Bolding A. Update on nonpharmacologic approaches to relievelabor pain and prevent suffering. J Midwifery Womens Health2004;49:489e504.

Management of Spontaneous Labour at Term in Healthy Women
49. Alehagen S, Wijma B, Lundberg U, Wijma K. Fear, pain and stresshormones during childbirth. J Psychosom Obstet Gynaecol2005;26:153e65.
50. Mahomed K, Gulmezoglu AM, Nikodem VC, Wolman WL, Chalmers BE,Hofmeyr GJ. Labor experience, maternal mood and cortisol andcatecholamine levels in low-risk primiparous women. J Psychosom ObstetGynaecol 1995;16:181e6.
51. Smith CA, Collins CT, Cyna AM, Crowther CA. Complementary andalternative therapies for pain management in labour. Cochrane DatabaseSyst Rev 2006;(4):CD003521.
52. Dowswell T, Bedwell C, Lavender T, Neilson JP. Transcutaneous electricalnerve stimulation (TENS) for pain management in labour. CochraneDatabase Syst Rev 2009;(2):CD007214.
53. Borup L, Wurlitzer W, Hedegaard M, Kesmodel US, Hvidman L.Acupuncture as pain relief during delivery: a randomized controlled trial.Birth 2009;36:5e12.
54. Cluett ER, Burns E. Immersion in water in labour and birth. CochraneDatabase Syst Rev 2009;(2):CD000111.
55. Hutton EK, Kasperink M, Rutten M, Reitsma A, Wainman B. Sterile waterinjection for labour pain: a systematic review and meta-analysis ofrandomised controlled trials. Br J Obstet Gynaecol 2009;116:1158e66.
56. Derry S, Straube S, Moore RA, Hancock H, Collins SL. Intracutaneous orsubcutaneous sterile water injection compared with blinded controls forpain management in labour. Cochrane Database Syst Rev2012;(1):CD009107.
57. Kronberg JE, Thompson DEA. Is nitrous oxide an effective analgesic forlabor? In: Halpern SH, Douglas MJ, editors. Evidence-based obstetricanesthesia. Malden, MA: Blackwell Publishing; 2005. p. 38e55.
58. Ullman R, Smith LA, Burns E, Mori R, Dowswell T. Parenteral opioids formaternal pain management in labour. Cochrane Database Syst Rev2010;(9):CD007396.
59. Kuhnert BR, Linn PL, Kennard MJ, Kuhnert PM. Effects of low doses ofmeperidine on neonatal behavior. Anesth Analg 1985;64:335e42.
60. Wittels B, Glosten B, Faure EA, Moawad AH, Ismail M, Hibbard J, et al.Postcesarean analgesia with both epidural morphine and intravenouspatient-controlled analgesia: neurobehavioral outcomes among nursingneonates. Anesth Analg 1997;85:600e6.
61. Nissen E, Widström AM, Lilja G, Matthiesen AS, Uvnäs-Moberg K,Jacobsson G, et al. Effects of routinely given pethidine during labour oninfants’ developing breastfeeding behaviour. Effects of dose-delivery timeinterval and various concentrations of pethidine/norpethidine in cordplasma. Acta Paediatr 1997;86:201e8.
62. Stoelting R, Hillier SC. Pharmacology and physiology in anesthetic practice.ed 4. Philadelphia, PA: Lippincott Williams and Wilkins; 2006.
63. Cunningham FG, Leveno KJ, Hauth JC, Bloom SL, Gilstrap III L,Wenstrom KD. Obstetrical anesthesia. In: Cunningham FG, Hauth JC,Leveno KJ, Gilstrap III L, Bloom SL, Wenstrom KD, editors. Williamsobstetrics. ed 22. New York: McGraw-Hill Medical Publishing Division;2005.
64. Anim-Somuah M, Smyth R, Jones L. Epidural versus non-epidural or noanalgesia in labour. Cochrane Database Syst Rev 2011;(12):CD000331.
65. Heeson M, Klohr S, Rossaint R, Straube S, Van de Velde M. Labourepidural analgesia and anti-infectious management of the neonate: ameta-analysis. J Perinat Med 2012;40:625e30.
66. Buxton EJ, Redman C, Obhrai M. Delayed pushing with lumbar epidural inlabour-does it increase the incidence of spontaneous delivery? J ObstetGynaecol 1988;8:258e61.
67. Sultan P, Murphy C, Halpern S, Carvalho B. The effect of lowconcentrations versus high concentrations of local anesthetics for labouranalgesia on obstetric and anesthetic outcomes: a meta-analysis. Can JAnaesth 2013;60:840e54.
68. Wilson MJ, MacArthur CC, Shennan A. Ambulation in labour and deliverymode: a randomised controlled trial of high-dose vs mobile epiduralanalgesia. Anaesthesia 2009;64:266e72.
69. Weiniger CF, Yaghmour H, Nadjari M, Einav S, Elchalal U, Ginosar Y, et al.Walking reduces the post-void residual volume in parturients with epiduralanalgesia for labor: a randomized-controlled study. Acta Anaesthesiol Scand2009;53:665e72.
70. Halpern SH, Carvalho B. Patient-controlled epidural analgesia for labour.Anesth Analg 2009;108:921e8.
71. van der Vyver M, Halpern S, Jospeh G. Patient-controlled epidural analgesiaversus continuous infusion for labour analgesia: a meta-analysis. Br JAnaesth 2002;89:459e65.
72. Capogna G, Camorcia M, Stirparo S, Farcomeni A. Programmedintermittent epidural bolus versus continuous epidural infusion for laboranalgesia: the effects on maternal motor function and labor outcome. Arandomized double-blind study in nulliparous women. Anesth Analg2011;113:826e31.
73. Wang F, Shen X, Guo X, Peng Y, Gu X. Epidural analgesia in the latentphase of labor and the risk of cesarean delivery: a five-year randomizedcontrolled trial. Anesthesiology 2009;111:871e80.
74. Sng B, Leong W, Zeng Y, Siddiqui F, Assam P, Lim Y, et al. Early versus lateinitiation of epidural analgesia. Cochrane Database Syst Rev2014;(10):CD007238.
75. Roberts C, Algert C, Cameron C, Torvaldsen S. A meta-analysis of uprightpositions in the second stage to reduce instrumental deliveries in womenwith epidural analgesia. Acta Obstet Gynecol Scand 2005;84:794e8.
76. Gupta JK, Hofmeyr G, Shehmar M. Position in the second stage of labourfor women without epidural anaesthesia. Cochrane Database Syst Rev2012;(5):CD002006.
77. Kemp E, Kingswood C, Kibuka M, Thornton J. Position in the secondstage of labour for women with epidural anaesthesia. Cochrane DatabaseSyst Rev 2013;(1):CD008070.
78. Torvaldsen S, Roberts CL, Bell JC, Raynes-Greenow CH. Discontinuationof epidural analgesia late in labour for reducing the adverse deliveryoutcomes associated with epidural analgesia. Cochrane Database Syst Rev2004;(4):CD004457.
79. Toledo P, McCarthy R, Ebarvia M, Wong C. A retrospective case-controlledstudy of the association between request to discontinue second stage laborepidural analgesia and risk of instrumental vaginal delivery. Int J ObstetAnesth 2008;17:304e8.
80. Abenhaim H, Fraser W. Impact of pain level on second-stage deliveryoutcomes among women with epidural analgesia: results from thePEOPLE study. Am J Obstet Gynecol 2008;199:500.e1e6.
81. Petrou S, Coyle D, Fraser W. Cost-effectiveness of a delayed pushing policyfor patients with epidural anesthesia. The PEOPLE (Pushing Early orPushing Late with Epidural) Study Group. Am J Obstet Gynecol2000;182:1158e64.
82. Fraser W, Marcoux S, Krauss I, Douglas J, Goulet C, Boulvain M.Multicenter, randomized, controlled trial of delayed pushing fornulliparous women in the second stage of labor with continuous epiduralanalgesia. Am J Obstet Gynecol 2000;182:1165e72.
83. Sprague A, Oppenheimer L, McCabe L, Brownlee J, Graham I, Davies B.The Ottawa Hospital’s clinical practice guideline for the second stage oflabour. J Obstet Gynaecol Can 2006;28:769e79.
84. Cheng YW, Hopkins LM, Caughey AB. How long is too long: does aprolonged second stage of labor in nulliparous women affect maternaland neonatal outcomes? Am J Obstet Gynecol 2004;191:933e8.
85. Paterson CM, Saunders NS, Wadsworth J. The characteristics of the secondstage of labour in 25 069 singleton deliveries in the North West ThamesHealth Region, 1988. Br J Obstet Gynaecol 1992;99:377e80.
SEPTEMBER JOGC SEPTEMBRE 2016 l 863

SOGC CLINICAL PRACTICE GUIDELINE
86. Rouse DJ, Weiner SJ, Bloom SL, et al. Second-stage labor duration innulliparous women: relationship to maternal and perinatal outcomes. AmJ Obstet Gynecol 2009;201:357.e1e7.
87. Le Ray C, Audibert F, Goffinet F, Fraser W. When to stop pushing: effectsof duration of second-stage expulsion efforts on maternal and neonataloutcomes in nulliparous women with epidural analgesia. Am J ObstetGynecol 2009;201:361e7.
88. Hansen SL, Clark SL, Foster JC. Active pushing versus passive fetal descentin the second stage of labor: a randomized controlled trial. Obstet Gynecol2002;99:29e34.
89. Perinatal Services BC. Core competencies for management of labour: evaulationof progress of labor/dystocia. Perinatal Services BC; 2011. Available at: http://www.perinatalservicesbc.ca/Documents/Guidelines-Standards/Standards/Competencies/4CoreCompDSTEvalofLabourDystocia.pdf. Accessed January23, 2013.
90. Menticoglou SM, Manning F, Harmon C, Morrison I. Perinatal outcome inrelation to second-stage duration. Am J Obstet Gynaecol 1995;173:906e12.
91. Robinson BK, Mapp D, Bloom S, Rouse D, Spong C, Varner M, et al.Increasing maternal body mass index and characteristics of the secondstage of labor. Obstet Gynecol 2001;118:1309e13.
92. Verdiales M, Pacheco C, Cohen W. The effect of maternal obesity on thecourse of labor. J Perinat Med 2009;37:651e5.
93. Buhimschi C, Buhimschi I, Malinow A, Weiner C. Intrauterine pressureduring the second stage of labor in obese women. Obstet Gynecol2004;103:225e30.
94. Ranta P, Jouppila P, Spalding M, Jouppila R. The effect of maternal obesityon labour and labour pain. Anaesthesia 1995;50:322e6.
95. Arrowsmith S, Wray S, Quenby S. Maternal obesity and labourcomplications following induction of labour in prolonged pregnancy.BJOG 2001;118:578e88.
96. Prins M, Boxem J, Lucas C, Hutton E. Effect of spontaneous pushingversus Valsalva pushing in the second stage of labour on mother andfetus: a systematic review of randomised trials. BJOG 2011;118:662e70.
97. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database SystRev 2009;(1):CD000081.
98. Murphy D, Macleod M, Bahl R, Goyder K, Howarth L, Strachan B.A randomised controlled trial of routine versus restrictive use ofepisiotomy at operative vaginal delivery: a multicentre pilot study. Br JObstet Gynaecol 2008;115:1695e702.
99. de Leeuw J, de Wit C, Kuijken J, Bruinse H. Mediolateral episiotomyreduces the risk for anal shphincter injury during operative vaginaldelivery: a multicentre pilot study. Br J Obstet Gynaecol 2008;115:104e8.
100. de vogel J, van der Leeuw-van Beek A, Gietelink D, Vujkovic M, de LeeuwJ, van Bavel J, et al. The effect of a mediolateral episiotomy during operativevaginal delivery on the risk of developing obstetrical anal sphincter injuries.Am J Obstet Gynecol 2012;206:404.e1e5.
101. Fretheim A, Odgaard-Jensen J, Rottingen J, Reinar L, Vangen S, Tanbo T.The impact of an intervention programme employing a hands-on techniqueto reduce the incidence of anal sphincter tears: interrupted time-seriesreanalysis. BMJ Open 2013;10:e003355.
102. Kalis V, Karanova J, Horak M, Lobovsky L, Kralickova M, Rokyta Z. Theincision angle of mediolaterial episiotomy before delivery and after repair.Int J Gynaecol Obstet 2008;103:5e8.
103. Laine K, Skjeldestad F, Sandvik L, Staff A. Incidence of obstetric analsphincter injuries after training to protect the perineum: cohort study.BMJ Open 2012;2:e001649.
104. Aasheim V, Nilsen A, Lukasse M, Reinar L. Perineal techniques during thesecond stage of labour for reducing perineal trauma. Cochrane DatabaseSyst Rev 2011;(12):CD006672.
864 l SEPTEMBER JOGC SEPTEMBRE 2016
105. Kettle C, Dowswell T, Ismail K. Continuous and interrupted suturingtechniques for repair of episiotomy or second-degree tears. CochraneDatabase Syst Rev 2012;(11):CD000947.
106. Kettle C, Dowswell T, Ismail K. Absorbable suture materials for primaryrepair of episiotomy and second degree tears. Cochrane Database SystRev 2010;(6):CD000006.
107. Duggal N, Mercado C, Daniels K, Bujor A, Caughey A, El-Sayed Y.Antibiotic prophylaxis for prevention of postpartum perineal woundcomplications: a randomized controlled trial. Obstet Gyncol2008;111:1268e73.
108. Leduc D, Senikas V, Lalonde AB. Active management of third stage oflabour: prevention and treatment of postpartum hemorrhage. Br J ObstetGynaecol 2009;31:980e93.
109. Begley CM, Gyte GML, Devane D, McGuire W, Weeks A. Active versusexpectant management for women in the third stage. Cochrane DatabaseSyst Rev 2015;(3):CD007412.
110. Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the thirdstage of labour to prevent postpartum hemorrhage. Cochrane DatabaseSyst Rev 2013;(10):CD001808.
111. Soltani H, Hutchon DR, Poulose TA. Timing of prophylactic uterotonicsfor the third stage of labour after vaginal birth. Cochrane Database SystRev 2010;(8):CD006173.
112. Hofmeyr G, Mshweshwe N, Gülmezoglu A. Controlled cord traction forthe third stage of labour. Cochrane Database Syst Rev 2015;(1):CD008020.
113. Rabe H, Diaz-Rossello J, Duley L, Dowswell T. Effect of timing ofumbilical cord clamping and other strategies to influence placentaltransfusion at preterm birth on maternal and infant outcomes. CochraneDatabase Syst Rev 2012;(8):CD003248.
114. McDonald S, Middleton P, Dowswell T, Morris P. Effect of timing ofumbilical cord clamping of term infants on maternal and neonataloutcomes. Cochrane Database Syst Rev 2013;(7):CD001808.
115. Zhang J, Landy H, Branch D, Burkman R, Haberman S, Gregory K, et al.Contemporary patterns of spontaneous labour with normal neonataloutcomes. Consortium on Safe Labour. Obstet Gynecol 2010;116:1281e7.
116. Wei S, Luo Z, Xu H, Fraser W. The effect of early oxytocin augmentation inlabor: a meta-analysis. Obstet Gynecol 2009;114:641e9.
117. Garite T, Weeks J, Peters-Phair K, Pattillo C, Brewster W. A randomizedcontrolled trial of the effect of increased intravenous hydration on thecourse of labor in nulliparous women. Am J Obstet Gynecol2000;183:1544e8.
118. Crane J, Young D. Metea-analysis of low-dose versus high-dose oxytocin forlabour induction. JOGC 1998;20:1215e23.
119. Wei S, Luo Z, Qi H, Xu H, Fraser W. High-dose vs low-dose oxytocin forlabor augmentation: a systematic review. Am J Obstet Gynecol2010;203:296e304.
120. Simpson KR, Knox GE. Oxytocin as a high-alert medication: implicationsfor perinatal patient safety. MCN Am J Matern Child Nurs 2009;34:8e15.
121. Clark SL, Simpson KR, Knox E, Garite TJ. Oxytocin: new perspectives onan old drug. Am J Obstet Gynecol 2009;200:35.e1e6.
122. Zhang J, Branch D, Ramirez M, Laughon S, Reddy U, Hoffman M, et al.Oxytocin regimen for labor augmentation, labor progression, andperinatal outcomes. Obstet Gynecol 2011;118(2 Pt1):249e56.
123. Bidgood K, Steer P. A randomized control study of oxytocin augmentationof labour. 1. Obstetric outcome. Br J Obstet Gynaecol 1987;94:512e7.
124. López-Zeno J, Peaceman A, Adashek J, Socol M. A controlled trial of aprogram for the active management of labor. N Engl J Med1992;326:450e4.
125. Merrill D, Zlatnik F. Randomized, double-masked comparison of oxytocindosage in induction and augmentation of labor. Obstet Gynecol1999;94:455e63.

Management of Spontaneous Labour at Term in Healthy Women
126. Xenakis E, Langer O, Piper J, Conway D, Berkus M. Low-dose versus high-dose oxytocin augmentation of laborda randomized trial. Am J ObstetGynecol 1995;173:1874e8.
127. Kotaska AJ, Klein MC, Liston RM. Epidural analgesia associated with low-dose oxytocin augmentation increases cesarean births: a critical look at theexternal validity of randomized trials. Am J Obstet Gynecol2006;194:809e14.
128. Arulkumaran K, Koh C, Ingemarsson I, Ratnam S. Augmentation oflabourdmode of delivery related to cervimetric progress. Aust NZ JObstet Gynaecol 1987;27:304e8.
129. Rouse D, Owen J, Hauth J. Active-phase labor arrest:oxytocin augmentation for at least 4 hours. Obstet Gynecol1999;93:323e8.
130. Rouse D, Owne J, Savage K, Hauth J. Active phase labor arrest: revisitingthe 2-hour minimum. Obstet Gynecol 2001;98:550e4.
131. Allen V, Baskett T, O’Connell C, McKeen D, Allen A. Maternal andperinatal outcomes with increasing duration of the second stage of labor.Obstet Gynecol 2009;113:1248e58.
SEPTEMBER JOGC SEPTEMBRE 2016 l 865