Embed Size (px)
Citation preview

Correspondence
doi:10.1016/S0964-3397(02)00047-2
Management of severe tonguetrauma with custom made oralapplianceFollowing several recent requests made to theregional maxillofacial service by ITU nurses Iwish to bring the following appliance to yourattention. As a result of prolonged oro-trachealintubation, traumatic intubation orneurological conditions leading to repeatedtongue biting, massive tongue swelling andinfection can occur. The patient then enters acycle of increasing swelling and consequenttrauma which frustrates the efforts of ITU staffto replace the whole tongue intra-orally.Tracheostomy and intensive oral nursing caremay be ineffective and autoamputation of theanterior tongue or severe cellulitis may result.Following four recent referrals to ourspeciality (from general and neuro ITU), andsuccessful management with this appliance, I
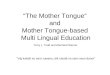
Fig. 1 Oral appliance in situ showing 30mm anterior gap.
am convinced the trouble and expense may bejustified.
Under increased sedation, analgesia andpossibly muscle relaxation, a dentally qualifiedclinician takes upper and lower standardalginate impressions and a jaw registration. Adental or maxillofacial technician constructsworking models and subsequently polytheneocclusal covers (3–5 mm thickness) in the sameway as a sports gumshield. These are fixed inthe correct registration on an articulator withan anterior opening of 10–30 mm dependingon the degree of tongue swelling, and a gapanteriorly to facilitate oral hygiene, NG tube orET tube (Fig. 1). This appliance is simply fittedin the ITU, antibiotics with broad spectrumand anaerobic cover may be indicated andregular use of chlorohexidine 0.2% on spongesis recommended. Rapid reduction in tonguesize and infection is to be expected (Fig. 2).These appliances inhibit oral hygiene measuresand are not durable, consequently I wouldexercise caution in use beyond two weeks.
302 Intensive and Critical Care Nursing (2002) 18, 302–303 © 2002 E l sev i e r S c i ence L td . A l l r i gh t s re se r ved .

Correspondence
Fig. 2 Close up of custom made oral appliance.
Cases of intra-cranial haematoma, diffuseaxonal injury, viral encephalitis and delayedpost laparotomy recovery have recently beentreated with good effect. It was notable thatneither nursing staff or anaesthetists hadpreviously encountered this device on anyoccasion.
Richard ShawFDS, FRCS
Specialist Registrar in Oral &Maxillofacial Surgery Maxillofacial Unit
University Hospital AintreeLiverpool L9 7AL, UK
E-mail: [email protected]
© 2002 E l sev i e r S c i ence L td . A l l r i gh t s re se r ved . Intensive and Critical Care Nursing (2002) 18, 302–303 303