Embed Size (px)
Citation preview

Urologie
Management of mCRPC:
Hormonal therapy and treatment sequence for
CRPC
Professor Bertrand Tombal, MD, PhD
Cliniques universitaires Saint-Luc
Université catholique de Louvain
Brussels, Belgium

Urologie
Credentials and conflict of interests
Professor and Chairman, Division of Urology, Cliniques
universitaires Saint Luc, Brussels, BE
President of European Organization Of Research and
Treatment of Cancer (EORTC)
PI of Prevail, 9785-CL-0321, and EORTC GUCG 1333
Investigator and paid advisor for Amgen, Astellas, Bayer
Pfizer, Ferring, Janssen, Sanofi Aventis
This meeting is organized and funded by Astellas Pharma
SRL
SmPC is available at the promotional booth or Astellas
employees.
This presentation has been prepared by and reflects the
personal view of Bertrand TOMBAL
XTA/17/0096/SEEd; for healthcare professionals only; date of preparation: 10/2017.

Urologie
The advanced PCa landscape in 2016
± 2-4 years
M1 HNPC
RX
progr.SRE
PAIN
PSA
progr.
± 7-15 years
High-risk
localized PCaSRE
PAIN
Local T/
RX
progr.
PSA
progr.
ADT
T/ treatment; ADT: androgen deprivation therapy; HNPC: hormone-naïve prostate cancer; PCa: prostate cancer;
PSA: prostate-specific antigen; RX progr.: radiological progression; SRE: skeletal-related events
Mottet N et al. EAU guidelines on prostate cancer, update 2015; http://uroweb.org/guideline/prostate-cancer/
(accessed March 2016); Vale CL et al. Lancet Oncol 2016;17:243-46
± ADT ± MTT
Salvage
Local T/
mCRPC
± ADT
PSA
progr.PSA
progr.
M0 CRPC
ADT

Urologie
CRPC portfolio in 2017
1. Fizazi K et al. Lancet Oncol 2012;13:983-92; 2. Ryan C et al. Lancet Oncol 2015;16:152-60; 3. Scher HI et al. N Engl J Med
2012;367:1187-97; 4. Beer C et al. N Engl J Med 2014;371:424-33; 5. Tannock IF et al. N Eng J Med 2004;2351:1502-12; 6. de
Bono JS et al. Lancet 2010;76: 1147-54; 7. Kantoff PW et al. N Engl J Med 2010;363:411-22; 8. Parker et al. N Engl J Med
2013;369:213-23
Relative reduction
in
risk of death, %
HR
(95% CI; P value)
Abiraterone/P vs. placebo/P (post-DOC)1 260.74
(0.64–0.86; P<0.001)
Abiraterone/P vs. placebo/P (pre-DOC)2 190.81
(0.70–0.93; P=0.003)
Enzalutamide vs. placebo (post-DOC)3 370.63
(0.53–0.75; P<0.001)
Enzalutamide vs. placebo (pre-DOC)4 230.71
(0.60–0.84; P=0.001)
DOC (q3w)/P vs. mitoxantrone/P5 240.76
(0.62–0.94; P=0.009)
Cabazitaxel/P vs. mitoxantrone/P (post-DOC)6 300.70
(0.59–0.83; P<0.0001)
Sipuleucel-T vs. placebo (pre-DOC)7 220.78
(0.62–0.98; P=0.03)
Radium-223 vs. placebo (post-DOC or DOC
unfit)8 300.70
(0.58–0.83; P<0.0001)
CRPC: castration-resistant prostate cancer; DOC: docetaxel; P: prednisone; q3w: every 3 weeks

Urologie
32,5
0
20
40
60
80
100
120
10 12 14 16 18 20 22 24 26 28
PS
A (
ng/m
l)
Months post RT
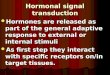
EBRT: external beam radiation therapy; ADT: androgen deprivation therapy, Images provided by B.Tombal &
F.Lecouvet , Clinique Universitaires Saint-Luc, Belgium
Case 1: 71 y.o. EBRT + 2 years ADT for locally-advanced PCa (T3b,
Gleason 8 (5+3), PSA 47 ng/ml, NO, MO), testosterone 43 ng/dl, PSA
doubling time 7 months
Months post initiation of ADT
following RP
Hot spot,
negative X-Rays

Urologie
When do you recommend initiating additional treatment for M0
CRPC patients (negative imaging, rising PSA, outside of clinical
trials) apart from maintaining ADT?
Gillessen S et al. Annals of Oncology 2015; 26: 1589–1604

Urologie
If you recommend treatment for M0 CRPC, what is your preferred
treatment option for M0 CRPC patients (negative imaging, rising PSA,
outside of clinical trials) apart from maintaining ADT?
Gillessen S et al. Annals of Oncology 2015; 26: 1589–1604

Urologie
Trial Drug N InclusionExpected
completion
Prosper(1) Enzalutamide 1560PSA DT
< 10 months08/2015
Spartan(2) ARN-509 1200PSA DT
< 10 months2016
Aramis(3) ODM-201 1500
PSA DT
< 10 months 2018
(1) NCT02003924; (2) NCT01946204; (3) NCT02200614
Randomized placebo- controlled trials in M0 CRPC
Primary endpoint: metastases free
survival (MFS).

Urologie• https://www.jnj.com/media-center/press-releases/janssen-submits-new-drug-application-to-us-fda-for-apalutamide-arn-
509-to-treat-men-with-non-metastatic-castration-resistant-prostate-cancer
• https://www.pfizer.com/news/press-release/press-release-
detail/pfizer_and_astellas_announce_positive_top_line_results_from_phase_3_prosper_trial_of_xtandi_enzalutamide_in
_patients_with_non_metastatic_castration_resistant_prostate_cancer

Urologie
32,5
49
64
0
20
40
60
80
100
120
10 12 14 16 18 20 22 24 26 28 32 34
PS
A (
ng/m
l)
Months post RT
EBRT: external beam radiation therapy; ADT: androgen deprivation therapy, Images provided by B.Tombal &
F.Lecouvet , Clinique Universitaires Saint-Luc, Belgium
Case 1. y.o. EBRT + 2 years ADT for locally-advanced PCa (T3b,
Gleason 8 (5+3), PSA 47 ng/ml, NO, MO), testosterone 43 ng/dl, PSA
doubling time 7 months
Months post initiation of ADT
following RP

Urologie
Mottet N et al. European Association of Urology Prostate Cancer Guidelines. https://uroweb.org/guideline/prostate-cancer.
Docetaxel is not registered for that indication in Romania
EAU Prostate Cancer Guidelines
Summary of Evidence LE
No definitive strategy regarding first treatment choice (which
drug/drug family first) can be devised.4
No clear-cut recommendation can be made for the most effective
drug for secondary treatment (i.e. hormone therapy, chemotherapy
or radium-223) as no clear predictive factors exist.
3
Recommendations LE GR
Ensure that testosterone levels are confirmed to be < 50
ng/mL4 A
Counsel, manage and treat patients with metastatic (m)CRPC
in a multidisciplinary team.3 A
Treat patients with mCRPC with life prolonging agents.
Base the choice of first line treatment on the performance
status, symptoms, comorbidities, location and extent of
disease (alphabetical order: abiraterone, docetaxel,
enzalutamide, radium-223, sipuleucel-T).
1b A

Urologie
Case 2: 71; 10/2009: acromio-clavicular pain; PSA >2500 ng/ml, ALP 450
UI/L, Gleason 7
Images copyrighted to CUSL, Brussels (BE0416.885.016) ALP: alkaline phosphatase; PSA: prostate-specific antigen
The historical standard of care is
androgen deprivation therapy
Additional treatment to be
discussed:
Docetaxel
Other to come ?

Urologie
Images copyrighted to CUSL, Brussels (BE0416.885.016)
10/2009 07/2010
Case 2: 71; 10/2009: acromio-clavicular pain; PSA >2500 ng/ml, ALP 450
UI/L, Gleason 7
Androgen deprivation therapy (ADT) started, pain disappears after 7 days.

Urologie
0
100
200
300
400
500
600
700
800
O-0
9
J-1
0
A-1
0
J-1
0
O-1
0
J-1
1
A-1
1
J-1
1
O-1
1
J-1
2
A-1
2
J-1
2
O-1
2
J-1
3
A-1
3
J-1
3
O-1
3
J-1
4
PSA (ngL/ml)
Al.P (UI/L)
Case 2: 71; 10/2009: acromio-clavicular pain; PSA >2500 ng/ml, ALP 450
UI/L, Gleason 7
ADT stopped after 2 years and then restarted

Urologie
Tombal B et al. Eur J Cancer 2011;47:S179-88
The androgen receptor (AR)
is the main driver of
the adaptation mechanisms

Urologie
“Historical” second line hormonal agents
Drug RefPatients
(n)
N°
Trials
% PSA
Response
(range)
Duration
(months)
Bicalutamide (150 mg qd ) 1-4 31-52 4 14 - 45 4
Flutamide (250 mg tid) 5 101 1 23 4,2
Nilutamide (200 or 300 mg
qd)6-7 14-28 2 29-50 7-11
Ketoconazole (200- 400 mg
tid) + cortisone ± AAW8-13 28-128 6 27-63 3.5 -20
DES (1-3 mg) 14-15 21-42 2 24-43 NA-2.8
% PSA response: % of patients achieving 50% decrease in PSA; AAW = anti-
androgen withdrawal
1) JCO 1997 15(8):2928-38; 2) J Urol. 1998 159(1):149-53; 3) Urology 2001 58(1):53-8; 4) Urology. 2010
76(5):1189-93; 5) JCO 2001 19(1):62-71; 6) J Urol. 2003 169(5):1742-4; 7) Urology 2001 58(6):1016-20; 8) J Urol.
1997 157(4):1204-7; 9) Cancer 1997 80(9):1755-9; 10) JCO 2004 22(6):1025-33; 11) J Urol. 2002 168(2):542-5;
12) Urol Oncol. 2001 6(3):111-115; 13) Clin Cancer Res. 2009 15(22):7099-105; 14) JCO 2004 22(18):3705-12; 15)
Urology. 1998 52(2):257-60

Urologie
Molecular biology of CRPC
Imamura et al. International Journal of Urology (2016) 23, 654--665
Enzalutamide(Apalutamide)
(Darolutamide)Enzalutamide(Apalutamide)
(Darolutamide)
Abiraterone

Urologie
De Bono et al. N Engl J Med 2011;364:1995-2005.
HR 0.646 0.54 – 0.77
P < 0.0001
Mode of action of new AR pathways inhitor lead to increase in overall
survival in post-docetaxel setting, thus demonstrating the depency of
mCRPC on the AR
Overall Survival abiraterone + prednisone vs. prednisone (COU-AA_301)
OS 95%CI
Abiraterone
/P14.8 14.1-15.5
Placebo/P 10.9 10.2-12

Urologie
19H.I. Scher, NEJM 2012 Sep 27;367(13):1187-97.
OS 95%CI
Enzalutamid
e18.4 17.3-NYR
Placebo 13.6 11.3-15-6
Mode of action of new AR pathways inhitor lead to increase in overall
survival in post-docetaxel setting, thus demonstrating the depency of
mCRPC on the AR
Overall Survival enzalutamide vs. placebo post-docetaxel (AFFIRM)

Urologie
0
100
200
300
400
500
600
700
800
O-0
9
J-1
0
A-1
0
J-1
0
O-1
0
J-1
1
A-1
1
J-1
1
O-1
1
J-1
2
A-1
2
J-1
2
O-1
2
J-1
3
A-1
3
J-1
3
O-1
3
J-1
4
PSA (ngL/ml)
Al.P (UI/L)
Case 2: 71; 10/2009: acromio-clavicular pain; PSA >2500 ng/ml, ALP 450
UI/L, Gleason 7
Degarelix stopped after 2 years and then restarted

Urologie
The management of mCRPC before abiraterone and
enzalutamide
CRPC survival
M0
Radiographic
progression
Chemo-based
treatment3
Symptoms

Urologie
22Graph and table are updated results from J Clin Oncol 26:242-245. 2008
Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for
Advanced Prostate Cancer.
Tannock IF et al. N Engl J Med 2004;351:1502-12

Urologie
Disease Burden Median SurvivalChemotherapy
Indicated
Rising PSA only ~4 years ? No
Asymptomatic
metastases
(limited)
~18 to 24 months Individualize
Asymptomatic
metastases
(extensive)
~18 months Yes
Symptomatic
metastases
~9 to 16 monthsYes
Calabrò F, Sternberg CN., Eur Urol. 2007 Jan;51(1):17-26 ,
modified
When Should Chemotherapy be Started?

Urologie
Efficacy vs. sequencing
N Engl J Med. 2012 Sep 27;367(13):1187-97
• Efficacy trial: evaluating the benefit of Enzalutamide when the rest has failed

Urologie
• Efficacy trial: evaluating the benefit of Enzalutamide when the rest has failed
Efficacy vs. sequencing
N Engl J Med. 2012 Sep 27;367(13):1187-97
• Sequencing trial: opposing a new approach, immediate enzalutamide, to the older one, wait and give chemotherapy

Urologie
COU-AA-302 and PREVAIL are sequencing Trial
Advanced
PCa
Random
isation
SOCmCRPC
SOC: standard of care (ADT ± local T)
ARpI: AR pathways inhibitors abiraterone or enzalutamide
Docetaxel
AAO: all available options
ARpI AAO
Docetaxel
Tumour load
Pain, QoL deterioration, SRE,
fatigue….
Historical reference
arm
Investigational arm
SOCmCRPC
ARpI
Docetaxel
AAO

Urologie
Impact of PREVAIL and COU-AA-302 on the modern CRPC
landscape
CRPC survival
M0
Radiographic
progression
Enzalutamide2
Abiraterone1
CRPC: castration-resistant prostate cancer
Ryan CJ, et al. N Engl J Med 2013;368:138–48.
Basch E, et al. Lancet Oncol. 2013 Nov;14(12):1193-9..
Chemo-based
treatment
Symptoms

Urologie
Abiraterone (COU-AA-302)
Important secondary endpoints
Abi/Pred Pred. Δ p
Time to chemotherapy 25.2 16.8 17.2 < 0.001
Time to PSA progression (months) 11.1 5.6 8.4 < 0.001
Time to SRE < 0.001
Time to time to opiate use NR 23.3
Median time to progression of mean pain
intensity(1) 26.7 18.4 0.049
Time to HRQoL degradation (months)(2) 12.7 8.3 0.03
PSA response > 50% (%) 62 24
Objective response (% 36 16 < 0.001
1. Median time to progression of pain interference
2. Median time to functional status deterioration (FACT-P total score)
Ryan CJ, et al. N Engl J Med 2013;368:138–48.
Basch E, et al. Lancet Oncol. 2013 Nov;14(12):1193-9..

Urologie
Enzalutamide (PREVAIL):
Important secondary endpoints
Enzalutamide Placebo ∆ P
Time to chemotherapy (mo) 28.0 10.8 17.2 <0.001
Time to PSA progression (mo) 11.2 2.8 8.4 <0.001
Median time to 1st SRE (mo) 31.1 31.3 <0.001
SRE at first analysis (%) 32% 37% 0.74 <0.001
Time to pain (mo)1 NR yet
Time to HRQoL degradation
(FACT-P) (mo)² 11.3 5.6 5.7 <0.0001
PSA response >50% (%) 78 3.5 <0.001
Objective response (%) 58.8 5 <0.001
Beer TM et al. N Engl J Med 2014;371:424-33; Loriot Y et al. Lancet Oncol 2015;16:509-21
1Median time to progression of pain interference; ²Time to deterioration in HRQoL based on FACT-P total score. FACT-
P: Functional Assessment of Cancer Therapy – Prostate; HRQoL: health-related quality of life; SRE: skeletal-related
event

Urologie
40
18
4548
38
55
23
13
27
33
22
34
0
10
20
30
40
50
60
Total Physical WBSocial/family WBEmotional WB Functional WB PCa subscale
Pa
tie
nts
sh
ow
ing
im
pro
ve
me
nt
in F
AC
T-P
(%
)Enzalutamide efficacy: QoL (PREVAIL)
Loriot Y et al. Lancet Oncol 2015;16:509-21
P<0.0001
EnzalutamidePlacebo
P=0.001
8
P<0.0001P<0.0001
P<0.000
1
P<0.00
01
Improvement is defined by a score increase of:
10 (Total score); 4 (Social/family WB); 3 (Physical, emotional and functional WB and PCa
subscale)
WB: wellbeing

Urologie
Adjusted mean (95% CI) change in FACT-P PCa subscale
Loriot Y et al. Lancet Oncol 2015;16:509-21

Urologie
COU-AA-302 and PREVAIL are sequencing Trial
Advanced
PCa
Random
isation
SOCmCRPC
SOC: standard of care (ADT ± local T)
ARpI: AR pathways inhibitors abiraterone or enzalutamide
Docetaxel
AAO: all available options
ARpI AAO
Docetaxel
Tumour load
Pain, QoL deterioration, SRE,
fatigue….
Historical reference
arm
Investigational arm
SOCmCRPC
ARpI
Docetaxel
AAO

Urologie
The impact of PREVAIL and COU-AA-302 in the modern
mCRPC landscape
1. Ryan et al. Lancet Oncol 2015;16:152-60; 2. Beer TM et al. N Engl J Med 2014;371:424-
33
Abiraterone
N (%)
Prednisone
N (%)
Subsequent
therapy for
mCRPC
365 (67) 435 (80)
Abiraterone 69 (13) 238 (44)
Cabazitaxel 100 (18) 105 (19)
Docetaxel 311 (57) 331 (61)
Enzalutamide 87 (16) 54 (10)
Ketoconazole 42 (8) 68 (13)
Radium-223 20 (4) 7 (1)
Sipuleucel-T 45 (8) 32 (6)
Enzalutamide
N (%)
Placebo
N (%)
Subsequent
therapy for
mCRPC
457 (52.4)685
(81.1)
Docetaxel 358 (41.1)504
(59.6)
Abiraterone 256 (29.4)417
(49.3)
Cabazitaxel 79 (9.1)149
(17.6)
Enzalutamide 21 (2.4)249
(29.5)
Sipuleucel-T 17 (1.9) 11 (1.3)
Radium-223 16 (1.8) 22 (2.6)

Urologie
COU-AA-302 and PREVAIL are sequencing Trial
Advanced
PCa
Random
isation
SOCmCRPC
SOC: standard of care (ADT ± local T)
ARpI: AR pathways inhibitors abiraterone or enzalutamide
Docetaxel
AAO: all available options
ARpI AAO
Docetaxel
Tumour load
Pain, QoL deterioration, SRE,
fatigue….
Historical reference
arm
Investigational arm
SOCmCRPC
ARpI
Docetaxel
AAO

Urologie
The impact of PREVAIL and COU-AA-302 in the modern
mCRPC landscape
1. Ryan et al. Lancet Oncol 2015;16:152-60; 2. Beer TM et al. N Engl J Med 2014;371:424-33
Improvement in
OS (median)
HR
(95% CI; P-value)
Abiraterone/P vs.
placebo/P (COU-AA-302)1
4.4 mo0.81
(0.70-0.93; P <0.001)
Enzalutamide vs. placebo
(PREVAIL) 2 4 mo0.77
(0.67-0.8; P =0.0002)
The benefit is for the sequence not for
simply the drug.

Urologie
The Standard treatments sequence in 2017
CRPC survival
M0
Radiographic
progression
Enzalutamide2
Abiraterone1
CRPC: castration-resistant prostate cancer
Ryan CJ, et al. N Engl J Med 2013;368:138–48.
Basch E, et al. Lancet Oncol. 2013 Nov;14(12):1193-9..
docetaxel
Symptoms
Enzalutamide
Abiraterone
Cabazitaxel
Bone targeted therapies, including RA223

Urologie
First line treatment of early mCRPC: The
view from the experts of APCC
86
6
08
Abiraterone orenzalutamideCabazitaxel
Docetaxel
Radium 223
Sipuleucel-T90
22
6
What is your preferred
first-line mCRPC
treatment option:
Asymptomatic men who did
not receive docetaxel in the
HNPC setting
Gillessen S, Eur Urol. 2017 Jun 24. pii: S0302-2838(17)30497-9.
Asymptomatic men who did
receive docetaxel in the
HNPC setting

Urologie
ADT + docetaxel has supplanted ADT as upfront
systemic treatment.
Enzalutamide or Abiraterone are the reference
treatments of early mCRPC.
How early is early?
The Standard treatments sequence in 2017
Docetaxel is not registered for that indication in Romania

Urologie
The PREVAIL Study: Primary Outcomes by Site and Extent of Baseline
Disease for Enzalutamide-treated Men with Chemotherapy-naïve
Metastatic Castration-resistant Prostate Cancer.
CI = confidence interval; HR = hazard ratio; mets = metastases; NYR = not yet reached.
Evans CP et al. Eur Urol. 2016 Mar 19. pii: S0302-2838(16)00274-8.
Kaplan–Meier estimates of OS by number of bone metastases at
screening (<4 vs I4).

Urologie
The PREVAIL Study: Primary Outcomes by Site and Extent of Baseline
Disease for Enzalutamide-treated Men with Chemotherapy-naïve
Metastatic Castration-resistant Prostate Cancer.
Kaplan–Meier estimates of OS in the non-visceral and visceral
subgroups.
CI = confidence interval; HR = hazard ratio; mets = metastases; NYR = not yet reached.
Evans CP et al. Eur Urol. 2016 Mar 19. pii: S0302-2838(16)00274-8.

Urologie
The PREVAIL Study: Primary Outcomes by Site and Extent of Baseline
Disease for Enzalutamide-treated Men with Chemotherapy-naïve
Metastatic Castration-resistant Prostate Cancer.
CI = confidence interval; HR = hazard ratio; mets = metastases; NYR = not yet reached.
Evans CP et al. Eur Urol. 2016 Mar 19. pii: S0302-2838(16)00274-8.

Urologie
ADT + docetaxel has supplanted ADT as upfront
systemic treatment.
Enzalutamide or Abiraterone are the reference
treatments of early mCRPC.
How early is early?
Is there still a role for hormonal
therapies without proven
benefit ?
The Standard treatments sequence in 2017
Docetaxel is not registered for that indication in Romania

Urologie
Use of first generation second line hormone
therapies in Prevail and COU-AA-302
CRPC survival
M0
Radiographic
progression
Enzalutamide1
Abiraterone2
Study % patient having received
antiandrogen prior to entering the
trial
COU-AA-
302(1)
100% (compulsory per protocol)
PREVAIL(2) 65%
(1) Ryan CJ, et al. N Engl J Med 2013;368:138–48 (appendix); (2) Beer TM, NEJM
2014;371:424-33 (appendix)
Second line
hormonal
manipulations?

Urologie

Urologie
ADT + docetaxel has supplanted ADT as upfront
systemic treatment.
Enzalutamide or Abiraterone are the reference
treatments of early mCRPC.
How early is early?
Is there still a role for hormonal
therapies without proven benefit ?
Is it abiraterone or enzalutamide, or
both one after the other ?
The Standard treatments sequence in 2017
Docetaxel is not registered for that indication in Romania

Urologie
Administration and Side Effect profile and relative
contra-indications of Zytiga®
Abiraterone:
4 250 mg tablets without food (No food should be eaten for at least 2
hours before and for 1 hour after). Swallow whole. With prednisone 5 mg
BID
Control hypertension and correct hypokalemia before and during
treatment. Monitor blood pressure, serum potassium, and symptoms of
fluid retention at least monthly. Measure ALT and AST) and bilirubin levels
prior to starting treatment with ZYTIGA®, every two weeks for the first
three months of treatment, and monthly thereafter.
Side-effect of interest: hypertension, hypokalemia, fluid retention, liver
enzyme
Relatives contra-indications: patients with a history of cardiovascular
disease or with medical conditions that might be compromised by
increases in blood pressure, hypokalemia, or fluid retention. YP2D6
substrates with a narrow therapeutic index.Zytiga ® Summary of Product Characteristics (SmP) accessed on Nov 1, 2017 http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002321/WC500112858.pdf

Urologie
Administration and Side Effect profile and relative
contra-indications of Xtandi ®
Enzalutamide
Four 40 mg capsules (160 mg) orally with or without food.
No additional tests, except if is co-administered with
warfarin (CYP2C9 substrate), conduct additional INR
monitoring.
Side-effect of interest: fatigue, HTA, arthralgia,
Relatives contra-indications: patients who had a seizure,
with predisposing factors for seizure, or using concomitant
medications that may lower the seizure threshold. Avoid
CYP3A4, CYP2C9 and CYP2C19 substrates with a
narrow therapeutic index. Xtandi® Summary of Product Characteristics (SmP) accessed on Nov 1, 2017 http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002639/WC500144996.pdf

Urologie
Gillessen S et al. Eur Urol. 2017 Jun 24. pii: S0302-2838(17)30497-9
What is your preferred choice between Abiraterone and Enzalutamide at any time
in the treatment sequence in men with mCRPC if all options are available in case
of the following medical situations?
Enzalutamide Abiraterone Either
Stable brain metastases 6% 73% 10%
History of falls 2% 94% 4%
Baseline significant fatigue 6% 88% 6%
Baseline significant
neurocognitive impairment4% 84% 10%
Long QTc-syndrome or men
on not replaceable drugs with
potential QT prolongation
27% 31% 24%
Diabetes mellitus requiring
prescription drug therapy84% 6% 10%
Cardiac ejection fraction
below 45-50%63% 6% 27%
Active liver dysfunction 68% 8% 14%

Urologie
CRPC prostate cancer is an
heterogonous disease
Early enzalutamide or abiraterone is
the new reference treatment of early
asymptomatic mCRPC
There is no valid reason to delay
treatment
Optimal sequencing is based on the
administration of a maximum of agents
taking in consideration the very high
rate of cross-resistance between
agents.
Conclusion