Embed Size (px)
Citation preview

DR BIVIN WILSON DNB REGISTRAR CARDIOLOGY

Cyanosis -- Greek word meaning "dark blue")
Cyanosis is dependent upon the absolute concentration of the reduced hemoglobin and not on the ratio of reduced hemoglobin to oxyhemoglobin.
Central cyanosis is one, which is present throughout the body, including the mucous membranes and tongue. If cyanosis is limited to the extremities, it is called peripheral cyanosis

Differential cyanosis - PDA with reversal of shunt or severe left sided obstructive lesions
In Reverse differential cyanosis -TGA with PHT&PDA and TAPVC above the diaphragm with PDA.

General causes of Cyanosis
PulmonaryPulmonary CardiacCardiac OthersOthers
Airway diseaseAirway disease Intrapulmonary shunting
Intrapulmonary shunting
Intracardiac shunting
Intracardiac shunting
CyanosisCyanosis

CAUSES OF CENTRAL CYANOSIS
A. Congenital Heart Disease
1) Cyanosis with PBF 2) Cyanosis with PBF
a) TOF a) D-TGA b) Pulm. Atresia b) DORV c) Tricuspid Atresia c) TAPVC d) Critical PS d) Truncus
arteriosus

CAUSES OF CENTRAL CYANOSIS B) LUNG DISEASE D) CNS DEPRESSION a) RDS a) IVH b) Pneumonia b) Perinatal asphyxia c) Pneumothorax c) Heavy maternal sedation d) Pleural effusion e) Diaphragmatic hernia f) T.E.Fistula
C) PERSISTENT PULMONARY E) MISCELLANOUS HYPERTENSION a) shock & sepsis b) Hypoglycemia c) Methemoglobinemia d) Neuromuscular
conditions ( Werdnig – Hoffman)

STEPS IN THE MANAGEMENT OF CYANOTIC NEWBORNS ABG in room air: confirm or reject
central cyanosis. An elevated PCO 2 suggests
pulmonary or central nervous system problems.
A low pH may be seen in sepsis, circulatory shock, or severe hypoxemia

Hyperoxia test: To differentiate between Cardiac from Pulmonary cause. Oxygen should be administered through a plastic hood
for at least 10 minutes to replace the alveolar air completely with oxygen.
With pulmonary disease, arterial PO 2 usually rises to> 150 mm Hg.
When there is a significant intracardiac right-to-left shunt, the arterial PO 2 does not exceed 100 mm Hg, and the rise is not more than 10 to 30 mm Hg.
However in Persistent Pulmonary Hypertension of newborn with a normal heart) PaO 2 may not have a rise in arterial PO 2 to 100 mm Hg.
The purpose of positive hyperoxia test helps in ruling out significant cyanotic congenital heart defect but when negative does not differentiate between cyanotic heart and PPHN.

ECG may be helpful in cardiac origin of cyanosis
Chest x-ray films: may reveal pulmonary causes of cyanosis. They can also hint at the presence or absence of cardiac defects and the type of defect
2-D Echocardiography and a Doppler examination

RADIOLOGICAL FEATURES CXR may exclude non cardiac causes of cyanosis e.g. RDS. .
Meconium aspiration, Diaphgramatic hernia, PneumothoraxPulmonary Vascular Markings
Decreased Increased
Heart Size Heart Size
Normal Increased Increased( “Boot shaped”) (“ Wall-to-Wall”) TOF Ebstein (“ egg-on-end”) D-TGA Aortic Arch \ Mediastinum
Abdominal Situs

CLUES TO DIAGNOSIS


TRANSIENT CYANOSIS – ASD,Ebsteins anomaly, DORV with subaortic VSD without PS & Truncus arteriosus
INTERMITTENT CYANOSIS --Ebsteins anomaly, TAPVC unobstructed,Complete A-V canal defect & Eisenmengers with bidirectional shunt

PERSISTENT AND PROGRESSIVE CYANOSIS –TGA, Single ventricle,Hypoplastic left heart Syndrome ,Tricuspid atresia ,Pulmonary atresia &Ebsteins anomaly
DEFERRED CYANOSIS –TOF,TGA with VSD with PS, Corrected TGA with VSD with PS, DORV with VSD with PS & Single ventricle with VSD with PS

CYANOSIS WITH FAILURE
Congestive cardiac failure in a patient with cyanosis denotes cyanotic heart disease with increased pulmonary blood flow physiology.
1) Transposition of great vessels 2) Taussing Bing anomaly 3) Truncus arteriosus 4) Total anomalous Pulmonary venous
connection 5) Single ventricle with low PVR and no
pulmonary stenosis 6) Common atrium

CYANOSIS WITH SQUATTING
1) Tetralogy of Fallot 2) Tricuspid atresia 3) Pulmonary atresia 4) Double outlet right ventricle 5) Single ventricle 7) Eissenmengers syndrome

CYANOSIS WITH COLLAPSING PULSE --TOF with AR ,Truncus arteriosus TOF/PA with increased aorto-pulmonary collaterals , Following shunt surgeries & Cyanotic CHD with PDA
CYANOSIS WITH a WAVE IN JVP -Tricuspid atresia, Pulmonary atresia with intact IVS,TGA with intact IVS, Eissenmengers ASD &TOF

CYANOSIS WITH CONTINUOUS MURMUR - Pulmonary atresia with VSD ,Truncus arteriosus ,TOF with peripheral artery stenosis ,Post shunt surgery,& Hypoplastic left heart
CYANOSIS WITHOUT MURMUR--PAH / Eisenmenger,

CYANOSIS WITH LEFT AXIS DEVIATION IN ECG
Cyanotic heart disease with LAD in ECG are
1) Tricuspid atresia 2) Complete AV canal defect 3) Single ventricle –LV type 4) Large Pulmonary AV fistula

INTERVENTIONS

Ductus dependent lesions
Those with severe RVOT obstruction: Pulmonary atresia, TOF, Severe pulmonary stenosis.
Transposition of great arteries with intact ventricular septum.
Tricuspid atresia with pulmonary stenosis.
Hypoplastic left heart syndrome.

Interventions to maintain ductal patency
Prostaglandin infusion to maintain ductal patency.
Transcatheter intervention
Endo vascular stents

PROSTAGLANDINS :
PG E1 : 0.01 – 0.1 mcg / kg / min
PG E2 : 0.003 – 0.01 mcg / kg / min
Start low dose and increase at 15 – 30 mins. interval, if no response.
> 3 fold increase in dose – rarely needed.
Oral PG E 2 – 25 – 40 mcg / kg / h . go stepwise to 4 – 6 hourly for c/h use.

Balloon atrial septostomy
Introduced by Rashkind
Improves mixing of oxygenated and deoxygenated blood in pts with transposition physiology or in those requiring venting of an atrium with restricted outflow


Better inter - atrial mixing. Transposition of great arteries
Augmentation of L-R shunt Mitral atresia DORV with restrictive left A-V valve, Univentricular heart with restrictive left A-
V valve,
Augmentation of R-L shunt TAPVC Pulmonary atresia, tricuspid atresia Ebstein's anomaly

Blalock – Taussig shunt Allows partially desaturated systemic blood to
enter the pulmonary artery, thus increasing pulmonary blood flow, and hence, oxygenation.
To avoid the problems of growth retardation of the limb associated with the ligation of the subclavian artery, modification was introduced
Modification of the Blalock - Taussig shunt in which a Teflon prosthetic tube is anastomosed end to side to the undivided subclavian artery and end to side to the pulmonary artery was first described by Klinner and colleagues.


Cyanotic Heart DiseaseCyanotic Heart Disease
Tetralogy ofFallot
Tetralogy ofFallot
Transposition Of Great Arteries
Transposition Of Great Arteries
TruncusArteriosusTruncus
Arteriosus
TricuspidAtresia
TricuspidAtresia
Total AnomalousPulmonary venous Return
Total AnomalousPulmonary venous Return

Tetralogy of Fallot (TOF)1. RVOT
obstruction2. VSD3. Overriding
aorta4. RV
hypertrophy

Tetralogy of Fallot (TOF)1. RVOT
obstruction2. VSD3. Overriding
aorta4. RV
hypertrophy

Hypercyanotic spell
Primary problem is decreased pulmonary blood flow with increased R->L shunting
Typically occurs in morning of after sleep (SVR is low, and blood volume is low)
May be precipitated by activity or fright, but may also be spontaneous

Hypercyanotic spell
Cyanosis will be accompanied by Hyperpnea
Increased rate and depth of respirations Increased fussiness progressing to
decreased level of consciousness Increasing acidosis, can be fatal

Hypercyanotic spell
Theories Primary infundibular spasm (unlikely) Hyperpnea as a primary cause Circulating catecholamines Reduced SVR
Spells are an indication for need of surgical intervention

Tachycardia
Impaired RV filling
RVOT obstruction
Rt Lt shunt
Agitation
Hypovolemia
Age PVR
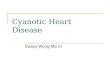
Hypercyanotic Spells ( TET spells)
Cyanosis
Syncope
FluidMorphine
Oxygen
Phenylepherine
Knee-chest

Cyanotic Spells Increase systemic vascular resistance Squat/Knee chest position Ketamine 1-2mg/kg IV Phenylephrine 0.02mg/kg IV Tachycardia Propranolol 0.1mg/ Kg IV Release of infundibular spasm Irritability Morphine 0.2mg/ Kg S.C or IM
Hypoxia Oxygen Dehydration Volume
Acidosis NaHco3 1mEq/ Kg IV

Surgical Palliation

Surgical Management
VSD closure transatrial access if possible Infundibular resection for visualization Patch closure
Relief of RVOT obstruction Infundibular resection vs. transannular
patch

Transposition of Great Areries (TGA)
Aorta originating from the right ventricle, and pulmonary artery originating from the left ventricle
Accounts for 5-7% of all congenital heart disease

TGA .. Acute Management
PGE-1 with no supplemental O2 Maintain ductus arteriosus patency, this
will increase the effective pulmonary blood flow, and thence increase the left atrial pressure, therefore inhance the left to right shunt at the atrial level
Balloon atrial septostomyLife saving procedure in the presence of
inadequate atrial septal defect

TGA .. Surgical Management
Arterial switch with re-implantation of the coronary artery
to the new aortic site.
Atrial switch : the old style surgery Redirecting the pulmonary and systemic
venous return to result in a physiologically normal state
The right ventricle remains the systemic ventricle
Rarely needed

Truncus Arteriosus
The presence of a common trunk that supply the systemic, pulmonary and coronary circulation
Almost always associated with VSD
1.2-2.5% of all congenital heart disease

Managment Acute management
Diuretics Afterload reduction to enhance systemic
blood flow
•Surgical management: complete repair with VSD closure and conduit placement between the right ventricle and pulmonary arteries•Long term problems :
–truncal valve dysfunction–RV conduit obstruction

Trcuspid Atresia
Complete absence of communication between the right atrium and right ventricle
About 3 % of congenital heart disease

Management
PBF
Decreased Increased
PGE-1, and minimal supplemental O2 to maintain ductal patency
Afterload reductionDiuretics

Surgical ManagementSingle ventricle paliation First stage : to establish a reliable source
of PBF Aorta to pulmonary artery shunt ( BT shunt) Pulmonary arterial banding in cases of
increased PBF
Second stage: Glenn Anastomosis ( superior vena cava to pulmonary artery
Third stage : Fontan anastomosis ( Inferior vena cava to pulmonary artery

TAPVC Treatment
Correct acidosis
Antifailure
Surgery: Anastomosis of Common Pulmonry Vein to the left
atrium

Cyanotic Heart DiseaseCyanotic Heart Disease
Tetralogy ofFallot
Tetralogy ofFallot
Transposition Of Great Arteries
Transposition Of Great Arteries
TruncusArteriosusTruncus
Arteriosus
TricuspidAtresia
TricuspidAtresia
Total AnomalousPulmonary venous Return
Total AnomalousPulmonary venous Return
THANK YOU