-
Management of Complex Open FractureIn WE
Pr ttaM ing
Te o theex wouex hadtar id; 6fra jointan derw1 r r usCli for
asta angeme od, fpla ht bco reewh he mfor iogrthe nkylTh
esultcomprehensive management with external fixation. (The Journal
of Foot & Ankle Surgery 45(5):308315,2006)
Ke
Cinjco
mu
ingdeofan
staso
CreUn
We
gar
Ch
30y words: midfoot, open fractures, external fixator, crush
rush injuries to the foot are categorized as seriousuries and
potentially can lead to amputation. A complexmbination of soft
tissue and bony injury may occur withltiple fractures of the tarsal
and metatarsal bones, result-in an unstable foot. Initial
management includes wound
bridement, anatomic realignment of the foot, stabilizationthe
fractures, and soft tissue coverage (1, 2). Early
atomic reduction of all fractures and dislocations withble
fixation can minimize long-term morbidity and hastenft tissue
healing (35).Traditionally, fractures and dislocations have been
re-
duced by open or closed methods and maintained by mul-tiple
smooth Kirschner wires or screws augmented by plas-ter
immobilization (611). However, these methods areassociated with
certain limitations such as inadequate fixa-tion, loss of
reduction, pin migration, and pin tract infec-tions. Adequate
anatomic restoration and maintenance ofstability in the severely
injured foot are often difficult withwires and screws alone. In
addition, open reduction andfixation can further devitalize the
soft tissues. Moreover,such injuries often require multiple
procedures to achievesoft tissue healing.
Despite a comprehensive treatment protocol for patientswith
crush injuries to the foot, functional results are notuniformly
good (5, 12). Unfortunately, injury classificationschemes do not
appear to be helpful in prognosticatingclinical outcomes.
Stabilization procedures intended to sal-vage the foot and improve
function carry a high rate ofinfection and soft tissue
complications, resulting in highamputation rates and persistent
pain. Therefore, it has beenrecommended that a decision for
amputation be consideredearly during treatment (13).
The management of severe injuries to the foot with ex-ternal
fixation is minimally invasive, thereby reducing fur-
Address correspondence to: Prakash Chandran, Specialist
Registrar, 15,sswell Close, Callands, Warrington, North Cheshire,
WA5 9UA,ited Kingdom. E-mail: [email protected]
Registrar, Scarborough General Hospital, Scarborough,st Yorkshire,
United Kingdom.2Orthopaedic Surgeon, Bradford, West Yorkshire,
United Kingdom.3Associate Professor, Department of Orthopaedics,
PGIMER, Chandi-h, India.4Professor in Orthopaedics, Department of
Orthopaedics, PGIMER,andigarh, India.Copyright 2006 by the American
College of Foot and Ankle
Surgeons1067-2516/06/4505-0001$32.00/0doi:10.1053/j.jfas.2006.06.002
8 THE JOURNAL OF FOOT & ANKLE SURGERYjuries of the
Midfootxternal Fixation
akash Chandran, MS, AFRCS,1 Ravindra Puandeep Singh Dhillon,
MS,3 and Shivender S
n patients (11 feet) with severe, high-velocity, open injuries
tternal fixation. The mean patient age was 38 years. Fivetensive
degloving of the foot extending into the lower leg. Allsal and
metatarsal bones: 9 patients had a fractured cuboctured cuneiform;
and all had metatarsal fractures. Lisfrancd intertarsal
dislocations were seen in 3 cases. Six patients unequired a
myocutaneous flap. The average duration of fixatonically, patients
were evaluated 1 year after fixator removalnd on tiptoe, presence
of a limp, deformity of an arch, and rtatarsophalangeal joints.
Each parameter was graded as gontigrade feet, with 2 patients who
experienced pain on weigmfortably on tiptoe, and 2 who limped
because of pain. Thereas 4 had cavus deformity. All demonstrated
stiffness at tefoot motion, with 5 also having restricted ankle
motion. Radtime of follow-up; 4 were malunited, with 1
demonstrating a
ese results suggest that crush injuries to the midfoot often
rith
swamaiah, MS,2
h Gill, MS4
midfoot were treated with uniplanarnds measured 10 cm, and 3
hadgrossly comminuted fractures of thehad a fractured navicular; 7
had adislocations were present in 7 feet,ent split-thickness skin
grafting, ande was 9 weeks (range, 615 weeks).ny residual pain in
the foot, ability toof motion at the ankle, subtalar, andair, or
poor. All patients had sensateearing, 5 who had difficulty
standingpatients exhibited flatfoot deformity,idfoot and
restriction of subtalar andaphically, all fractures were healed
atosis across the tarsometatarsal joint.in persistent morbidity
despite early
-
the(14tisdisintwialsclia u
Pa
dethepreideopfralevex
ca
tarthi
taiinjpaAsthene
ou
stephpowe
ex
an
idelat
an
ideredtiopowithefix
an
haderotwa
ofplathrve
aspsec
fou
TABLE 1 Clinical parameters and observations
Parameters Good Fair Poor
NoStaNoGaNoDeNoRaNo
ASTr devascularization (5), and helps maintain alignment) and
stability (1517). Unobstructed access for soft
sue management and early joint motion (1, 17) are alsotinct
advantages. External fixation can be combined withernal fixation to
obtain additional stability. When usedth a dynamic device, minor
postoperative corrections cano be achieved. The purpose of this
study is to present thenical and functional outcomes of 10 patients
treated withniplanar external fixator for midfoot crush
injuries.
tients and Methods
Ten patients (11 feet) who presented to the emergencypartment
with severe midfoot injuries were included in
study. All patients were seen by one of the authors atsentation;
patients with complex midfoot injuries werentified and recruited. A
complex injury was defined as anen, high-velocity injury to the
midfoot, with unstablectures or fracture dislocations that involved
more than 1el, were severely comminuted, and were associated
with
tensive soft tissue damage. Isolated fractures of the cal-neus,
talus, and simple closed fractures of the remainingsal, metatarsal,
or phalangeal bones were excluded froms study.After an initial
general assessment and resuscitation, de-ls were collected
regarding the type and mechanism ofury to the foot. A complete
clinical evaluation of thetient was performed with special
attention to the foot.sessment included the condition of the skin,
the extent of
soft tissue injury, contamination, bony injury, and aurovascular
evaluation of the foot. The wound was copi-sly irrigated with
saline solution and covered with arile dressing. All patients were
checked for tetanus pro-ylaxis history and received antibiotic
coverage. Antero-sterior (AP), lateral, and oblique radiographs of
the footre obtained to identify the bony injury, type of
fracture,tent of comminution, and displacement and evidence of
Residual Pain None or Trivial
of feet (11) 9nding tiptoe (stability) Ableof feet (11) 6
it (limp) Normalof patients (9) 7
formity (Cavus/Flat feet) Noneof feet (11) 4
nge of movement Full rangeof feet (11)nkle 6ubtalar joint and
midfoot 5oes 0
VOLUMEy subluxation or dislocation. The pattern of injury
wasntified depending on involvement of the medial and/oreral
columns.At the time of surgery, the wound was adequately debridedd
irrigated. Fractures, dislocations, and subluxations werentified
and reduced. All fractures and dislocations wereuced by either
direct or indirect manipulation. Open reduc-n of intraarticular
fractures was performed wheneverssible to achieve anatomic
reduction. Initially, Kirschnerres were used to stabilize the
fractures/dislocations, andfoot was held to length by an assistant
while the external
ator was applied.The external fixator was constructed with
Kirschner wiresd connecting rods. The connecting rod was threaded
andd clamps for attachment to the Kirschner wires. Using thisvice,
compression or distraction could be achieved byating the threaded
rod. The frame of the external fixators built by first passing 2
Kirschner wires in the safe zonethe calcaneus (18) from medial to
lateral in the transversene. Two pairs of Kirschner wires were then
passedough the metatarsals distal to the fracture in the trans-rse
plane; 1 pair of wires was introduced from the medialect through
the first and second metatarsals, while theond pair was passed from
the lateral aspect through therth and fifth metatarsals. The
proximal and distal sets of
rschner wires (calcaneus and medial metatarsals, calca-us and
lateral metatarsals, respectively) were intercon-cted with
connecting rods on both sides of the foot. Whenly 1 column was
injured, unilateral Kirschner wires withingle connecting rod were
used. In patients with gross
mminution, in whom open manipulation and fixationre not
possible, the reduction was achieved along thenciples of
ligamentotaxis. In such cases, the external fix-r frame was
initially applied, reduction was subsequentlyieved by distraction
applied to the fracture site, and directssure was also applied, if
necessary, to achieve satisfactoryuction. During surgery, attempts
were made to reduce all
Mild to Moderate Pain Severe Pain
2 0Difficult Unable
5 0Limp Unable to weight bear
2 0Mild Severe
7 0Some restriction No movements
3 22 47 4
NUMBER 5, SEPTEMBER/OCTOBER 2006 309Kine
ne
on
a s
co
we
priatoachprered
45,
-
intalo
ac
gratarbeme
3)tarDi
briwe
izewiac
ex
TABLE 2 Patient Summary with Outcome
CaseNu
Age Side Wound Contamination Fractures Dislocations Duration
of
rate
re
re
rate
rate
rate
al
Ablate
31raarticular fractures to less than 2-mm displacementng the
joint surface.Radiographs were taken intraoperatively to check
forcuracy of reduction according to the following radio-phic
criteria: 1) congruity of the midtarsal and tarsometa-sal joints on
AP, lateral, and oblique views; 2) continuitytween the medial
aspect of second metatarsal with thedial aspect of the second
cuneiform (Lisfranc joint); andcontinuity between the medial aspect
of the fourth meta-sal with the medial aspect of the cuboid
(Lisfranc joint).splacement of less than 2 mm was considered
acceptable.All wounds were reevaluated after 48 hours and rede-ded
if necessary. Patients with skin and soft tissue lossre treated
with split-thickness skin grafting or vascular-d free-tissue
transfer. Plaster splints were used in patientsth additional ankle
or leg injuries. Patients were allowedtive ankle and
metatarsophalangeal joint range-of-motionercises immediately after
surgery.Postoperatively, AP, lateral, and oblique radiographs
of
mber andSex
Size (cm)
1 26/M R 10 Mode
2 40/M L Degloving Seve
3 55/M R Degloving Seve
4 36/M R 10 Mode
5 35/F L 10 Mode
6 25/M R 10 Mode
7 35/M R 10 Minim
8 30/M L 10 Mode
9 50/M L 10 Seve
10 35/M R Degloving Seve
11 L 10 Seve
breviations: M, male; F, female; R, right; L, left; Cub, cuboid;
Navral; PWB, pain on weight bearing; MTP, metatarsophalangeal;
Min
0 THE JOURNAL OF FOOT & ANKLE SURGERYfoot were obtained and
reassessed with the same criteria.y loss of reduction or
incongruence of the joint surfaces noted, and an attempt was made
to re-reduce thecture or subluxation during subsequent wound
debride-nt.The fixator was kept in place for a minimum of 6
weeksuntil adequate soft tissue healing was achieved. Theme was
removed 2 weeks after satisfactory soft tissuealing was obtained.
After fixator removal, all patientsre kept nonweight bearing for 3
weeks and then allowedrtial weight bearing with a protective boot
and arch sup-rt for an additional 6 weeks. All patients received
com-hensive physiotherapy and gait training.
One year after fixator removal, all patients were assessedthe
follow-up clinic by one of the authors. Clinical andiographic
evaluation was performed using the following
rameters. Residual pain, ability to stand on tiptoe (stabil-),
limp, deformity of the arch (assessed with footprintsd
differentiated into cavus or flat feet), stiffness (assessed
Fixator(wk)
Cub, Nav,Mt 1, 2, 3
9
Nav, Mt 1, 2,3, 4, 5
Phal 2, 3, 4, 5
Lisfrancdislocation
6
Cub, Nav,Cunie 1,2, 3
Mt 2, 3, 4
Lisfrancdislocation
15
Cub 2, Mt 3,4, 5
PP 1
7
Nav, Cub,Cunie 1,2, 3
Mt 3
MTPdislocation2, 3, 4
7
Nav, Cub,Cunie 1,2, 3
Mt 1, 2, 3, 4,5
Lisfrancdislocation
13
Cub, Cunie 1,2, 3
Mt 5
Lisfrancdislocation
4
Cunie 1, 2Mt 2, 3, 4, 5
9
Cub, Cunie 2,3
Mt 4, 5
Lisfranc andmidtarsaldislocation
13
Cub, Latcunie
Mt 1, 2, 3,4, 5
Lisfranc andmidtarsaldislocation
15
Cub, Nav,Mt 2, 3, 4
PP 1
Lisfrancdislocation
6
icular; Mt, metatarsals; Phal, phalangeal; Cunie, cunieform;
Lat,imal; PP, proximal phalanx.theAnwa
frame
or
frahewe
papopre
inradpaityan
rate
re
re
re
, nav, min
-
byof-so
res
Tafrajoi
Re
mi(rahiginjTa5 hex
TABLE 2 Patient Summary with Outcome
ResidualP
Arch Suppleness Movements Fracture Joint Congruity
N
Pion
Nion
N
N
Nion
N
P
N
P
Nthe ability to pronate and supinate the foot), and range-motion
measurements of the ankle subtalar and metatar-
phalngeal joints were recorded. For each parameter, theults were
graded as good, fair, or poor as described inble 1.
Radiographically, the foot was also assessed forcture healing,
nonunion, malunion, congruity of thents, and any persisting
subluxation or dislocation.
sults
Ten patients (11 feet) who sustained an injury to thedfoot were
studied. The mean patient age was 38 yearsnge, 2555 years), and 90%
were men. All patients hadh-velocity injuries due to road traffic
accidents. Theury and treatment profiles for all patients can be
found inble 2. Three feet had wounds that measured 2 to 10 cm,ad
wounds that measured greater than 10 cm, and 3 had
tensive degloving of the foot extending to the lower leg.
ain DeformityAnkle
il Nil Minimumstiffness
Full
WB Flatfoot Grossly stiff Grossrestrict
il Flatfoot Grossly stiff Minrestrict
il Cavusdeformity
Minimumstiffness
Full
il Cavusdeformity
Minimumstiffness
Full
il Cavusdeformity
Grossly stiff Minrestrict
il Nil Minimumstiffness
Full
WB Nil Minimumstiffness
Full
il Cavusdeformity
Minimumstiffness
Minrestrict
WB Flatfoot Grossly stiff Grossrestrict
il Nil Minimumstiffness
Full
VOLUMEe wounds were severely contaminated, 5 were moder-ly
contaminated, and 1 had minimal contamination. Se-re contamination
was seen in either degloved wounds orger wounds.One foot had an
isolated lateral column injury, and the
aining had involvement of both the medial and laterallumns. All
cases had fractures involving 1 or more tarsalnes. Nine patients
had fractured the cuboid, 6 had frac-ed the navicular, and 7 had
fractured cuneiforms. Alltients had at least 1 or more metatarsals
fractured, with 3ving fractured all the metatarsal bones and 3
havingncomitant phalangeal fractures. Seven patients had Lis-nc
joint dislocations, and 2 patients had midtarsal dislo-tions with
disruption of intercuneiform and naviculocu-iform joints. One
patient had a dislocation of the second,rd, and fourth
metatarsophalangeal joints.Ten feet required biplanar fixators (on
either side of thet) to support both columns, and 1 patient
required stabi-
UnionToe
Minrestriction
Reduced,united
Congruent
Grossrestriction
Malunion Congruent
Grossrestriction
Reduced,united
Union acrossLisfranc joint
Minrestriction
Malunion Congruent
Minrestriction
Reduced,united
MildincongruenceLisfranc
Grossrestriction
Malunion Congruent
Minrestriction
Reduced,united
Congruent
Minrestriction
Reduced,united
Congruent
Minrestriction
Reduced,united
Congruent
Grossrestriction
Malunion MildincongruenceLisfranc
Minrestriction
Reduced,united
Congruent
NUMBER 5, SEPTEMBER/OCTOBER 2006 311Fivateve
lar
rem
co
boturpahaco
fraca
ne
thi
foo
ion
ion
45,
-
lizadfeerec
cu
typ
31ation of only the lateral column. Eight feet requiredditional
Kirschner wires to stabilize the fractures. Eightt required more
than 1 wound debridement. Six patientseived split-thickness skin
grafting, and 1 required a myo-
taneous graft to obtain coverage. Figure 1 demonstrates aical
patient enrolled in this case series.
2 THE JOURNAL OF FOOT & ANKLE SURGERYThe average duration of
time the fixator was maintaineds 9 weeks (range, 615 weeks). A
longer duration of fixatorplication was required in patients with
large and severelyntaminated wounds. Two patients required
additional plasterinting for associated injuries to the ankle and
leg.Two patients developed pin tract infections, which were
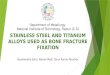
FIGURE 1 (A) AP radiograph of severedual-column crush injury.
(B) Obliqueview. (C) Oblique view showinguniplanar bilateral
fixator applicationand reduction of all dislocations.Kirschner
wires were sued to stabilizethe first and second metatarsal
frac-tures. (D) Lateral view with fixator inplace. (E) One-year
postoperative APradiograph showing alignment of thefoot. (F)
Lateral view showing the de-velopment of a cavus deformity.wa
apco
spl
-
ma
theOntha
wo
we
paco
mu
pa
(a(a2ma
ca
(a(a(a(abe
micav
Alass
tarsus
1 h
wa
strstrpatiefooan
thedeofco
pa
Alran
(poma
shstrdedeThmitoOnbores
rem
posu
far
Di
injApso
mo
pafra
ca
ofshtioco
ac
TABLE 3 Summary of wound size with outcome
Wound Number of Average Pain Deformity Stiffness
tg
11Denaged by local wound care topical antibiotics. None
ofinfections were severe enough to require pin relocation.
e patient developed compartment syndrome of the foott required
fasciotomy and skin grafting.At 1-year follow-up, all patients had
functional feet, allunds had healed, and all fractures had united.
All patientsre able to ambulate with full weight bearing, except
1tient, who was kept partial weight bearing because of ancomitant
ipsilateral femur and tibia fracture that requiredltiple surgeries.
No patient developed complex regional
in syndrome.Eight patients (9 feet) reported no complaints of
paingood outcome), 2 had moderate pain on weight bearingfair
outcome), and no patient experienced rest pain. Thepatients who had
pain with weight bearing exhibited alunion of midtarsal and
metatarsal fractures. A modifi-
tion in their shoe gear helped to reduce their symptoms.Six
patients were able to stand on tiptoe comfortablygood outcome), and
5 could stand on tiptoe with difficultyfair outcome). Seven were
able to walk comfortablygood outcome), 2 were able to mobilize with
some painfair outcome), and 1 patient was still nonweight
bearingcause of associated injuries.Seven patients (64%) exhibited
some degree of arch defor-ty. Three of these exhibited a flatfoot
deformity, 4 had aus deformity, and all were rated as having a fair
outcome.
l patients with flatfoot deformity had double-column
injuriesociated with Lisfranc joint dislocations and at least 3
meta-sal fractures. In those patients with cavus deformity, 3
hadtained an injury to both the medial and lateral columns andad an
isolated lateral-column injury.
In terms of ankle joint range of motion, a poor outcomes
observed in 2 patients who demonstrated gross re-iction of ankle
motion, and 3 patients had some re-iction in motion (fair outcome),
with the remainingtients demonstrating good ankle joint motion. All
pa-nts exhibited some stiffness of the subtalar and mid-t joints: 4
patients had gross stiffness (poor outcome)
d 2 patients were considered to have a fair result,
withremaining rating a good outcome. Of the patients who
monstrated significant stiffness, 3 exhibited a malunionthe
tarsals and metatarsals, with residual abnormal
nfiguration of cuneiforms, cuboid and navicular, and 1tient had
spontaneous fusion across the Lisfranc joint.
Size Patients DurationFixator Nil Weigh
Bearin
0 cm 3 8 3 00 cm 5 9 4 0gloving 3 12 1 2
VOLUMEl patients had restricted metatarsophalangeal jointge of
motion, with gross restriction seen in 4 patientsor outcome) and
moderate restriction seen in the re-ining 7 (fair outcome).
Radiographic assessment at 1 year after fixator removalowed that
all fractures had united; 4 patients demon-ated a malunion of
metatarsal and tarsal bones. Eight feetmonstrated congruence of all
joints, whereas 2 patientsmonstrated minimal incongruence at the
Lisfranc joint.ese 2 patients had initially demonstrated severely
com-nuted cuneiform and cuboid fractures, and it was
difficultclearly assess the joint line in the postoperative
images.e developed a malunion across the Lisfranc joint, withny
ankylosis between the base of the metatarsals and thepective
cuneiforms.It was noted that larger wounds required the fixator
to
ain in place for a longer duration and had a greatertential for
residual pain with weight bearing (Table 3). Inmmary, 49%
demonstrated a good outcome and 14%ed poorly.
scussion
In severe injuries to the foot, the severity and pattern ofury
play an important role in determining the outcome.propriate wound
management, stabilization, and early
ft tissue coverage all contribute to decreasing the
potentialrbidity (6, 7, 10, 19). However, the highly variable
injury
tterns make comparative evaluation of a series of thesectures
difficult.Incomplete or loss of reduction of the fracture and
dislo-tion frequently results in permanent disability in the
formchronic pain, persisting deformity, and difficulty with
oe gear (20). Although anatomic reduction and stabiliza-n can
improve the outcome (2, 2123) in patients withmplex comminuted
fractures, it is often difficult tohieve satisfactory results. The
results of the current studypport the premise that achieving
satisfactory reductiond maintenance of alignment with early soft
tissue cover-e allows early bone healing. However, the incidence
ofrmanent morbidity due to stiffness and restricted motionn seldom
be controlled. Even with seemingly anatomictoration of normal
alignment, many patients fare poorly
Nil Cavus FlatFoot
Minimum Gross
1 2 0 2 13 2 0 5 00 0 3 0 3
NUMBER 5, SEPTEMBER/OCTOBER 2006 313su
an
agpeca
res
45,
-
(20). Extensive soft tissue crushing with resultant scarringadds
to the stiffness and restricted joint motion (15).
Although ring fixators play an increasing role in treatingsu
toex
pleforstainprepreredlatif
tiobiltiehape
tatsivser
reqticex
foo
ex
pares
ofthrthepin
froan
ne
syditofbildrode
thesev
ser
ca
mi
position of the fracture and the shape of the foot, scarringand
subsequent contracture can seldom be prevented.
In our series, 49% of cases demonstrated good results
and14son
cru
co
co
relcar
pacu
tisco
me
no
inj
ityplirieabyie
Su
fooma
an
isgostaofap
Re
1.
2.
3.
4.
5.
6.
7.
31ch complex injuries, we observed that adequate stabilitythe
foot could be provided with a uniplanar bilateral
ternal fixator (16, 23). These devices are technically sim-r,
provide adequate stability, and also allow good accesssoft tissue
management (15, 17). External fixators can
bilize major open fracture dislocations, maintain lengththe
presence of bone loss or extensive comminution,vent soft tissue
contractures, control joint position, andvent further
devascularization that may occur with openuction (17). The fixator
also allows for further manipu-
ion of the fracture postoperatively to improve the
positionrequired.The use of an external fixator eliminates the need
for addi-nal plaster immobilization (1, 17) and allows for early
mo-ization of surrounding joints. In the current series, all pa-nts
demonstrated some restriction in toe motion, and 48%d restriction
of ankle motion. The severity of the injury wasrhaps a major factor
in determining the final outcome.Up to 21% of crush injuries to the
foot result in ampu-ion because of either uncontrollable deep
sepsis or mas-e injury (15). Even though most of the injuries in
ouries were severe, no patient developed deep sepsis oruired an
amputation. Adequate initial management, me-
ulous wound care, and the minimally invasive nature ofternal
fixation contributed to our ability to salvage thet.
Pin site infection is known to occur with the use ofternal
fixation in up to 37% of cases (15, 24, 25). Twotients in this
study developed pin site infections thatolved with wound care and
local antibiotics. Higher ratespin tract infection are seen when
the pins are placedough large volumes of soft tissue (for example,
thigh);relatively limited soft tissue envelope of the foot
makestract infection less common.
Chronic pain after crush injuries to the foot can resultm
neuroischemia, direct trauma to the peripheral nerves,d intraneural
or extraneural fibrosis. Direct trauma to therve may also cause
chronic neuritis, which can trigger ampathetically mediated pain
syndrome (26). With expe-ious treatment, adequate wound coverage,
managementany compartment syndromes, and early aggressive
reha-itation, many complications, such as chronic pain syn-mes, can
be minimized. No patient in the current series
veloped chronic regional pain syndrome.Nemec et al (1) looked at
39 patients with war injuries of
foot and concluded that the external fixator preventedere
contractures and facilitated fracture healing. In ouries, 64%
developed an arch deformity of the foot: either
vus or flat feet due to scarring, contracture, and bonygration.
Although external fixation may help maintain the
4 THE JOURNAL OF FOOT & ANKLE SURGERY% fared poorly. These
results are similar to those of Myer-et al (5), who retrospectively
reviewed 58 patients with
sh injuries to the foot at a mean interval of 3.3 years.
Theyncluded that 46% of the patients had good functional out-mes,
and 25% demonstrated poor results. A significant cor-ation was
observed between a good functional outcome andeful adherence to the
treatment protocol. However, some
tients fared poorly regardless of treatment. Poor results
oc-rred if treatment was not initiated immediately and if softsue
coverage was delayed. Brunet et al (27) observed norrelation
between the initial fracture type and the treatmentthod used with
subsequent function of the foot. They foundcorrelation between the
radiographic appearance of the
ury and the patients symptoms.Consideration should be given to
the patients bone qual-, age, cognitive ability, psychological
tolerance, and com-ance level when deciding on management of these
inju-s. With these factors kept in mind, the surgeon should bele to
select the patient for whom external fixation willld a superior
result (28).
mmary
This case series demonstrates that crush injuries of thet are
associated with prolonged morbidity, and initialnagement should be
directed toward skeletal stabilization
d early soft tissue coverage. The use of external fixationless
invasive, can achieve adequate stability, and provideod access for
wound management without compromisingbility. However, arch
deformity, stiffness, and restrictionsubtalar, midfoot, and toe
joint motion occur despite
propriate early management.
ferences
Nemec B, Santic V, Matovinovic D, Gulan G. War wounds to the
foot.Mil Med 165:1820, 2000.Adelaar RS. Complications of forefoot
and midfoot fractures. ClinOrthop 391:2632, 2001.Brunet JA, Tubin
S. Traumatic dislocations of the lesser toes. FootAnkle Int
18:406411, 1997.Richter M, Wippermann B, Krettek C, Schratt HE,
Hufner T, ThermanH. Fractures and fracture dislocations of the
midfoot: occurrence,causes and long-term results. Foot Ankle Int
22:392398, 2001.Myerson MS, McGarvey WC, Henderson MR, Hakim J.
Morbidityafter crush injuries to the foot. J Orthop Trauma
8:343349, 1994.Main BJ, Jowett RL. Injuries of the midtarsal joint.
J Bone Joint SurgBr 57:8997, 1975.Tan YH, Chin TW, Mitra AK, Tan
SK. Tarsometatarsal (Lisfrancs)injuriesresults of open reduction
and internal fixation. Ann AcadMed Singapore 24:816819, 1995.
-
8. Sands AK, Grose A. Lisfranc injuries. Injury 35(suppl
2):SB7176,2004.
9. Thompson MC, Mormino MA. Injury to the tarsometatarsal
jointcomplex. J Am Acad Orthop Surg 11:260267, 2003.
10. Weber M, Locher S. Reconstruction of the cuboid in
compressionfractures: short to midterm results in 12 patients. Foot
Ankle Int23:10081013, 2002.
11. Wilson DW. Injuries of the tarso-metatarsal joints.
Etiology, classifi-cation and results of treatment. J Bone Joint
Surg 54B:677686, 1972.
12. Mawhinney IN, McCoy GF. The crushed foot. J R Coll Surg
Edinb40:138139, 1995.
13. Necmioglu S, Subasi M, Kayikci C, Young DB. Lower limb
landmineinjuries. Prosthet Orthot Int 28:3743, 2004.
14. Pinney SJ, Sangeorzan BJ. Fractures of the tarsal bones.
Orthop ClinNorth Am 32:2133, 2001.
15. Kenzora JE, Edwards CC, Browner BD, Gamble JG, DeSilva
JB.Acute management of major trauma involving the foot and ankle
withHoffmann external fixation. Foot Ankle 1:348361, 1981.
16. Beals TC. Applications of ring fixators in complex foot and
ankletrauma. Orthop Clin North Am 32:205214, 2001.
17. Seibert FJ, Fankhauser F, Elliott B, Stockenhuber N, Peicha
G. Ex-ternal fixation in trauma of the foot and ankle. Clin Podiatr
Med Surg20:159180, 2003.
18. Santi MD, Botte MJ. External fixation of the calcaneus and
talus: ananatomical study for safe pin insertion. J Orthop Trauma
10:487491,1996.
19. Hendrich V. Fractures and luxations of the mid- and
forefoot. Radio-loge 26:333336, 1986.
20. Teng AL, Pinzur MS, Lomasney L, Mahoney L, Havey R.
Functionaloutcome following anatomic restoration of
tarsal-metatarsal fracturedislocation. Foot Ankle Int 23:922926,
2002.
21. Kuo RS, Tejwani NC, Digiovanni CW, Holt SK, Benirschke
SK,Hansen ST Jr, Sangeorzan BJ. Outcome after open reduction
andinternal fixation of Lisfranc joint injuries. J Bone Joint Surg
82A:16091618, 2000.
22. Wiss DA, Kull DM, Perry J. Lisfranc fracture-dislocations of
the foot:a clinical-kinesiological study. J Orthop Trauma 1:267274,
1987.
23. Eastaugh-Waring SJ, Saleh M. The management of a complex
midfootfracture with circular external fixation. Injury 25:6163,
1994.
24. Hedin H, Hjorth K, Rehnberg L, Larsson S. External fixation
ofdisplaced femoral shaft fractures in children: a consecutive
study of 98fractures. J Orthop Trauma 17:250256, 2003.
25. Alonge TO, Ogunlade SO, Salawu SA, Adebisi AT. Management
ofopen tibia fractureAnderson and Hutchins technique re-visited.
AfrJ Med Med Sci 32:131134, 2003.
26. Vora A, Myerson MS. Crush injuries of the foot in the
industrialsetting. Foot Ankle Clin 7:367383, 2002.
27. Brunet JA, Wiley JJ. The late results of tarsometatarsal
joint injuries.J Bone Joint Surg 69B:437440, 1987.
28. Baker MJ, Offutt SM. External fixation indications and
patient selec-tion. Clin Podiatr Med Surg 20:926, 2003.
45,VOLUME NUMBER 5, SEPTEMBER/OCTOBER 2006 315
Management of Complex Open Fracture Injuries of the Midfoot With
External FixationPatients and
MethodsResultsDiscussionSummaryReferences