Management of CBD injury - · PDF fileManagement of biliary injury after laparoscopic...
35
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 downstatesurgery.org
Management of CBD injury - · PDF fileManagement of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital . 8/19/2010
– Chemistry, amylase , and lipase are within normal limits
downstatesurgery.org
Case Presentation
• RUQ ultrasound – cholelithiasis with gallstone in gallbladder neck, no pericholecytic fluid, distended gallbladder, normal gallbladder wall
downstatesurgery.org
Case Presentation
• HOD#2 – Pt. taken to OR for laparoscopic cholecystectomy– Operative Detail
• The gallbladder fundus was retracted superiorly and the infundibulum retracted laterally
– Reduced mobility of gallbladder secondary to its “socked-in” nature
• The peritoneum was released along the medial and lateral portions of the infundibulum.
– Difficult dissection
downstatesurgery.org
Presenter
Presentation Notes
Operating surgoens said that the mobility of the gallbladder was reduced secondary to its socked in nature. Dissection was challenging because as a result of extensive fibrosis and fusion of tissue planes. The peritoneum at the ICD junction should be released to allow for greater mobility of the gallbladder and meticulous dissection of the duct and artery. Retraction of the gallbladder fundus should be performed superiorly and the infundibulum retracted laterally to avoid tenting of the CBD
Case Presentation
– Operative Detail (cont’d)
• Cystic duct and artery were identified and ligated
• Gallbladder was released from hepatic bed with electrocautery
• 10mm flat Jackson Pratt drain
downstatesurgery.org
Presenter
Presentation Notes
JP drain was left as a percautionary measure because bile staining was noted in hepatic bed . Operating surgeons thought this to be from gallbladder. Some advocate closed suction drains in Morrison's pouch for intrahepatic gallbladders, possibly leading to extensive exposed liver parenchyma following dissection from the gallbladder fossa. No data support this practice. Routine use of intraoperative cholangiogram (IOC) is controversial. Most surgeons advocate for selective approach to IOC when CBD stones are clinically suspected preoperatively or when the anatomy appears unclear intraoperatively. Proponents of the selective approach argue that routine IOC unnecessarily adds time and expense to the operation because the vast majority of CBD stones are detected and treated preoperatively with endoscopic retrograde cholangiopancreatography (ERCP). They also contend that normal preoperative bilirubin translates to clinically insignificant stones that will pass spontaneously with no sequelae. Selective proponents also argue that the clinical impact and significance of occult retained stones are overstated. A review of the literature by Metcalfe and colleagues that included 5179 laparoscopic cholecystectomies performed without IOC and without preoperative indication of common bile duct stones demonstrated that only 0.6% developed symptoms from residual stones postoperatively. This study also showed no statistically significant difference in the rate of CBD transection during laparoscopic cholecystectomy with (0.02%) and without (0.09%) IOC.
Case Presentation
• POD #1– Afebrile & vitals signs are within normal limits
There was rapid clearance of the radiopharmaceutical from the blood pool. A �linear area of collection is seen felt to represent dilated extra-hepatic �biliary duct with spillage of bile inferiorly and superiorly. Bile is seen �along the inferior left subdiaphragmatic surface. The common bile duct and �duodenum are not visualized. Gallbladder is not visualized consistent with �provided history of cholecystectomy.�On delayed imaging, again seen is a dilated tubular structure with persistent �visualization of the liver suggestive of delayed clearance and possibly biliary �obstruction. There is apparent extraluminal extravasation into the free �peritoneum.�IMPRESSION: �Gallbladder is not visualized consistent with provided history of �cholecystectomy. There appears to be a linear collection of bile, which may �represent a dilated common hepatic duct with extensive peritoneal spillage that �does not conform to normal intraluminal anatomic structure. This is suggestive �of leakage likely eminating from the region of the common hepatic duct. ��
Case Presentation
• POD #3– 400 - 500 ml of bilious fluid from JP drain
– Endoscopic retrograde cholangiopanctreography performed
downstatesurgery.org
Case Presentation – ERCPdownstatesurgery.org
Presenter
Presentation Notes
Jackson-Pratt drains and surgical clips are identified in the right upper �quadrant. �CBD is cannulated and is of normal diameter. No filling defects identified. �Ill defined contrast collection overlying the common hepatic duct. Small �amount of contrast noted in nondilated intrahepatic biliary tree. Common �hepatic duct is not clearly demonstrated due to underfilling as well as �overlying extraluminal contrast collection.�A plastic stent was placed at the CBD at the conclusion of the examination.�Impression: Findings consistent with leak at the level of the common hepatic �duct. The exact site of the leak and the anatomy of the common hepatic duct �not demonstrated on this examination. �
Case Presentation
• POD #5– 400 - 500 ml of bilious fluid from JP drain
– Interventional Radiology service consulted for percutaneous transhepatic cholangiogram
downstatesurgery.org
Case Presentation – PTCdownstatesurgery.org
Presenter
Presentation Notes
MEDICATIONS: Lidocaine 1%, 300 mics Fentanyl, 30 mg Toradol�Procedure: 1. Fluoroscopic guided biliary access via accustick. 2. �Placement of 10 French APD drain in the gallbladder bed. 3. attempts to �traverse from the peripheral common bile duct into the central part of the CBD �were unsuccessful..�PROCEDURE: �The patient was placed in the supine position. The biliary tree was opacified �by injecting contrast media through the Jackson Pratt drain. The right �subcostal and flank areas were prepped and draped in standard fashion. A 21 �gauge needle was placed my multiple attempts percutaneously from the anterior �axillary line subcostally into the lateral to midportion of the right lobe of �the liver. When bile was aspirated, contrast medium was injected to outline the �biliary tree. An 0.018 inch guidewire was advanced through the 21 gauge needle �into the biliary system. The 21 gauge needle was then exchanged for an �Accustick set over the wire. Multiple attempts were made to find the distal �end of the common bile duct with a 5 Fr Bernstein cather and glidewire. The �system was removed and an 0.035 in guidewire was coiled within the collection. �Sequential dilatation using 8 and 10 dilators were used. A 10 Fr APD drainage �catheter pigtail drain was left in the biliary tree for external drainage. The �catheter tip was positioned within the collection and the pigtail was �successfully formed under fluoroscopic visualization. The catheter was sutured �to the skin and a sterile dressing was applied. The catheter was connected to �a drainage bag.�CHOLANGIOGRAPHY was performed. The examination revealed a walled off cavity �that communicated well with the JP drain. The Peripheral portion of the common �hepatic duct communicated with the cavity. �The patient tolerated the procedure without problems and returned to the �recovery room in satisfactory condition, similar to that at arrival in the �department. �RECOMMENDATIONS: It is possible that we can stent across the dehiscence by a �"Rendevous" procedure whereby i can snare a wire placed via endoscopy into the �gallbladder bed biloma. and then place a stent across the dehiscence.��
Case Presentation
• POD # 9– Hepatobiliary surgeon was consulted for Roux-
en-Y hepaticojejunostomy
– Pt. was discharged home with external biliary drain and JP drain.
downstatesurgery.org
Case Presentation
• HOD #1/POD # 42– Admitted for exploratory laparotomy and Roux-
en-Y hepaticojejunostomy and intraoperative cholangiogram
downstatesurgery.org
Case Presentation
• HOD #1/POD # 42– Operative Detail
• Right subcostal incision
• Strasberg type E2/ Bismuth type 2 injury
• Several clips around the common hepatic duct
• Single layer common hepatic duct to antecolic Roux limb anastomosis over an 8Fr feeding tube using interrupted 4-0 PDS sutures
• Intraoperative cholaingogram performed
downstatesurgery.org
Presenter
Presentation Notes
Right subcostal incision was made with a small extension onto the left side in a chevron fashion
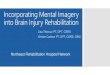
Case Presentation – Intraoperative cholangiogram
downstatesurgery.org
Presenter
Presentation Notes
FINDINGS: �The tip of endotracheal tube is demonstrated 3.5 cm from the carina. �2 nasogastric tubes are demonstrated with the tip located below the �hemidiaphragm. A right-sided catheter demonstrated in the RIGHT upper �quadrant with tip located within the biliary tree and with contrast �opacifying the biliary system. Another right-sided catheter with �smaller lumen in the RIGHT abdomen with tip located within the small �bowel. A biliary stent is in demonstrated in the RIGHT paraspinal �region at levels T11-L1. � �The biliary system is opacified with contrast and appears �unremarkable. There is communication of the common bile duct with �adjacent loop of small bowel. No evidence of contrast extravasation. � �IMPRESSION: �No evidence of contrast extravasation from biliary enteric �anastomosis.�
Case Presentation
• POD # 2– Passing flatus and started on clear liquid diet
• POD# 3– Tolerating regular diet
• POD#4– Post-op cholangiogram performed
downstatesurgery.org
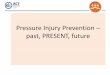
Case Presentation – Post-op cholangiogram
downstatesurgery.org
Presenter
Presentation Notes
Findings: �20 cc of Cysto-Conray was injected into the biliary tree via the �T-tube catheter. � �Intrahepatic biliary tree is visualized without evidence of obvious �filling defects. Delayed images demonstrate passage of contrast into �the small bowel without evidence of extravasation into the �surrounding peritoneal cavity. � �Impression: �Patent biliary-enteric anastomosis without evidence of extravasation �or obstruction/stricture. �
Case Presentation
• POD #8
– Discharged home with clamped external biliary drain.
downstatesurgery.org
Case Discussion
• Mechanisms of bile duct injury
• Critical View of Safety
• Classification of biliary injuries
• Long –term results of surgical reconstruction
downstatesurgery.org
Introduction
• Incidence of bile duct injury has risen from 0.2% to 0.6%
• Substantial effect on the quality of life of patients suffering biliary injury
– Excess of $50,000 per event
downstatesurgery.org
Presenter
Presentation Notes
By the early 1990s, laparoscopic cholecystectomy (LC) had supplanted open cholecystectomy in the operative management of gallbladder stone disease. Unfortunately, the widespread application of LC has led to a concurrent rise in the incidence of major bile duct injuries (BDI). Reports have estimated the incidence of BDI has risen from 0.1 - 0.2% to 0.4 - 0.6% between the era of open cholecystectomy and the age of LC. Several prospective single-institution studies have demonstrated a substantial effect on the quality of life of patients suffering biliary injury and estimated the financial cost for the management of patients with biliary injury to be in excess of $50,000 per event
“Classic” mechanism of injury
• Misidentification of the biliary anatomy
downstatesurgery.org
Presenter
Presentation Notes
Iatrogenic injury during laparoscopic cholecystectomy is usually the result of a misidentification of the biliary anatomy by the operating surgeon. In the classic laparoscopic injury, excessive cephalad retraction of the gallbladder fundus or insufficient lateral retraction on the infundibulum aligns the cystic duct and the common bile duct. The common bile duct is then mistakenly perceived to be the cystic duct and is clipped and divided .
“Critical View of Safety”
• In 1995, Soper and Strasberg introduced the concept of the “critical view of safety”
• Essential to clear the triangle of Calot
• Must separate the lowest part of gallbladder from the cystic plate
• Finally, only 2 structures should be seen entering gallbladder – cystic duct and artery
downstatesurgery.org
Presenter
Presentation Notes
In attempt to prevent iatrogenic injury, In the mid-1990s, Soper and Strasberg introduced the concept of the “critical view of safety” whereby the infundibulum is retracted laterally and careful effort is made to essentially to clear the triangle of Calot of all fat and fibrous tissue. The second requirement is that the lowest part of the gallbladder be separated from the cystic plate, the flat fibrous surface to which the nonperitonealized side of the gallbladder is attached. The cystic plate is sometimes referred to as the liver bed of the Gallbladder And Finally, only 2 structures should be seen entering gallbladder – cystic duct and artery Propents of this method recommned limited thermal energy use and to not divide the cystic duct or artery until this view is achieved.
Critical View of Safetydownstatesurgery.org
Presenter
Presentation Notes
Also note that the common bile duct does not have to be seen
Critical View of Safetydownstatesurgery.org
• Retrospective review of all laparoscopic cholecystectomies done over a 5 year period in a single institution
• “Critical View” technique was used in all procedures
• Out of 3,042 cases analyzed, only 1 bile duct injury occurred– Less than the expected 2 to 4 injuries per 1000 patients
Am Surg 2008;74:985-957
downstatesurgery.org
Presenter
Presentation Notes
So does this concept or method prevent biliary injury… Laparoscopic cholecystectomies were performed mainly by surgical residents (postgraduate year [PGY] 2 to 5) under supervision of experienced attending surgeons.
Classification of biliary injury
• Strasberg type A
– Leak from cystic duct stump or minor liver bed ducts
– Tx : ERCP with stenting and percutaneous drainage of localized bile collections
downstatesurgery.org
Presenter
Presentation Notes
Once you have Biliary injuries, it can be classified as described by Strasberg Strasberg type A injuries include leaks from the cystic duct stump or minor ducts on the liver bed with intact intrahepatic and extrahepatic ducts. Leakage from the cystic duct occurs secondary to clip failure (improperly applied or crossed clips or inadequate occlusion of the entire width of the cystic duct) or a burst phenomenon in the presence of retained common duct stones; it may also be seen when the clips are applied too tightly and local ischemia leads to necrosis of the cystic duct stump. Patients with this type of injury present with symptoms related to the presence of intraperitoneal bile—namely, abdominal pain, anorexia, ileus, nausea, or bile peritonitis with sepsis. Cystic duct leaks are usually treated with endoscopic transampullary stenting to decrease endobiliary pressure in addition to percutaneous drainage of localized bile collections. Endoscopic sphincterotomy may be necessary in some cases to facilitate stent placement but may fail when used alone (without stenting). Success with nonoperative management of an isolated cystic duct stump leak approaches 90%.
Classification of biliary injury
• Strasberg type B
– An aberrant right hepatic duct is mistaken for the cystic duct and ligated
– Tx : non-operative management versus Roux-en-Y hepaticojejunostomy
downstatesurgery.org
Presenter
Presentation Notes
Type B injuries occlude a portion of the biliary tree and may occur when the cystic duct drains into the right hepatic duct rather than the common duct. The right hepatic duct, or an aberrant right hepatic duct, is then mistaken for the cystic duct and is ligated or divided. Patients with type B injuries may remain asymptomatic as the obstructed lobe or segment atrophies and the remaining liver hypertrophies. Type B biliary injuries may or may not require operative repair. If the injury involves a minor branch of the right hepatic duct, the patient may show elevated liver tests as the involved segment atrophies, but little long-term consequence will be noted unless infection occurs. If the injury obstructs the main right hepatic duct or two or more subsegmental branches, then operative drainage with a Roux-en-Y hepaticojejunostomy will likely be necessary.
Classification of biliary injury
• Strasberg type C
– Sectoral duct injury without occlusion
– Tx : Percutaneous drainage vs. Roux-en-Y hepaticojejunostomy
downstatesurgery.org
Presenter
Presentation Notes
A type C injury is a leak from a duct not in continuity with the common duct and is also known as a sectoral duct injury without occlusion of the injured duct, so that bile leakage into the peritoneal cavity occurs. Patients become symptomatic secondary to the presence of a peritoneal bile collection, presenting with pain, nausea, peritoneal irritation, and signs of sepsis. Radiographically, these injuries are usually defined only after percutaneous drainage of a bile collection, followed by establishment of a biliary fistula and subsequent contrast injection of the fistula. Type C injuries present earlier and with more sepsis and inflammatory changes than type B injuries because there is ongoing leakage of bile from the injured duct(s). However, if the injury is to a small sectoral right branch, simple percutaneous drainage will likely suffice with subsequent delineation of the exact duct injury pattern. However a persistent of biliary fistula will require a Roux-en-Y hepaticojejunostomy
Classification of biliary injury
• Strasberg type D
– Partial injury to any extrahepatic duct
– Tx : Primary repair vs. Roux-en-Y hepaticojejunostomy
downstatesurgery.org
Presenter
Presentation Notes
The type D injury is a lateral injury to any extrahepatic duct, and, like many injuries, may be caused by cautery, scissors, or improper placement of clips. This injury may have several manifestations depending on whether the injury is a laceration, cautery burn, or partial clip obstruction. Partial lacerations from scissors or cautery injury present early with bile peritonitis. However, a cautery burn may present later as a stricture if there is not full thickness injury to the duct. Partial clip applications across the common hepatic or bile duct may present early with peritonitis if there is necrosis of the duct in that area, but more commonly they present later with a bilary stricture. When D injuries involve less than 25% of the circumference of the bile duct, they may be repaired primarily with fine absorbable sutures over a T-tube. It is preferable to bring the T-tube out of the bile duct through a separate opening in the duct so that one of the arms or the tube crosses the repair. When D injuries involve a larger circumference reconstruction by hepaticojejunostomy is the preferred solution
Classification of biliary injury
• Strasberg type E1-5/ Bismuth 1 - 5
– Excision or complete occlusion of the common hepatic or bile duct
– Tx : Roux-en-Y hepaticojejunostomy
downstatesurgery.org
Presenter
Presentation Notes
A type E injury is an excision or complete occlusion of the common hepatic or common bile duct that totally disrupts biliary-enteric communication. Type E injuries most commonly present with early sepsis and peritonitis if there is bile leaking from the duct injury or can present later with jaundice or cholangitis if the duct is totally occluded by clips or ligatures. Virtually all will require a Roux-en-Y hepaticojejunostomy. If the injury involves the bifurcation of the hepatic duct, repair will be difficult and may require two or more hepatic duct anastomoses.
Ann Surg 2005; 241:786.
• Single tertiary care institution’s retrospective analysis of 200 patients with major duct injuries– Largest experience reported by a single institution
• Rate of perioperative complications was 43%
• The timing of operation (defined as early, intermediate and delayed) did not change the incidence of the most common perioperative complications
downstatesurgery.org
Presenter
Presentation Notes
The timing of operation, defined as early (less than 1 month after referral), intermediate (1–12 months after referral), and delayed (more than 12 months after referral), presenting symptoms (jaundice, bile leak/biloma, cholangitis, and pain), and history of prior repair did not affect the incidence of the most common perioperative complications noted above or the length of stay in any of the groups
downstatesurgery.org
Presenter
Presentation Notes
High rate of complications however, the most common complications were wound infections (8%), cholangitis (5.7%), and intra-abdominal abscess (2.9%). The postoperative mortality rate was 1.7%. Early postoperative cholangiography revealed an anastomotic leak in 4.6%. None of the patients required reexploration postoperatively
Conclusion
• Timing of operation had no influence on perioperative complications.– Median of 5.4 weeks after initial injury
• Most of these complications, although troublesome, can be managed conservatively
• Early referral to a tertiary care center to assure optimal short-term and long-term outcomes.
downstatesurgery.org
Presenter
Presentation Notes
Authors concluded that Timing of operation (early, intermediate, and delayed, as indicated by clinical presentation), presenting symptoms, and prior attempt at repair had no influence on perioperative complications and length of stay There fore these authors recommended definite repair at a median of 5.4 weeks after initial injury so that associated inflammation has subsided making the operation technically easier. Most of these complications, although troublesome, can be managed conservatively, and therefore, no patient required reoperation in the perioperative period And finally the authors advocate early referral to a tertiary care center with experienced hepatobiliary surgeons and skilled interventional radiologists to assure optimal short-term and long-term outcomes.
References• Cohen J, Sharp K: Complications of laparoscopic cholecystectomy. Laparoscopic surgery of
the abdomen, New York: Springer-Verlag; 2004.• Deziel DJ: Complication of cholecystectomy: incidence, clinical manifestations, and
diagnosis. Surg Clin North Am 1994; 74:809.• Kaffes AJ, Hourigan L, De Luca N: Impact of endoscopic intervention in 100 patients with
suspected postcholecystectomy leak. Gastrointest Endosc 2005; 61:269.and others• Lee CM, Stewart L, Way LW: Postcholecystectomy abdominal bile collections. Arch
Surg 2000; 135:538.• Lee VS, Chari RS, Cucchiaro G: Complications of laparoscopic cholecystectomy. Am J
Surg 1993; 165:527.and others• Murr M, Gigot JF, Nagorney DM: Long-term results of biliary reconstruction after
laparoscopic bile duct injuries. Arch Surg 1999; 134:604.and others• Sicklick J, Camp M, Lillemoe K: Surgical management of bile duct injuries sustained during
laparoscopic cholecystectomy: perioperative results in 200 patients. Ann Surg 2005; 241:786.and others
• Tumer AR, Yuksek YN, Yasti AC: Dropped gallstones during laparoscopic cholecystectomy: the consequences. World J Surg 2005; 29:437.and others
• Varshney S, Buttirini G, Gupta R: Incidental carcinoma of the gallbladder. Eur J Surg Oncol 2002; 28:4.