Embed Size (px)
Citation preview

Management of Breastfeeding
Associated Pain
Holly Montgomery, PGY2
03/22/17
Disclosures
No financial disclosures
Currently breastfeeding

Outline
Why is breastfeeding important?
Why do women quit?
Focused H&P
Breastfeeding-associated pain differential
Treatment options
Infant Benefits
↓ Otitis media
↓ Asthma
↓ Atopic dermatitis
↓ Gastrointestinal tract infections
↓ Obesity
↓ Diabetes
↓ High blood pressure
↓ SIDS
Maternal Benefits
↓ Breast cancer
↓ Ovarian cancer
↓ Type II diabetes
↓ Hypertension
↓ Heart Disease
Recommendations
Exclusive breastfeeding for up to around 6 months, followed by continued breastfeeding
for at least 1 year
American Academy of Pediatrics, American College of Obstetricians and Gynecologists,
WHO/UNICEF
Healthy People 2020
Increasing worksite lactation programs
Reducing formula supplementation of BF infants in the first 2 days of life
Increasing the proportion of births that occur in facilities that provide recommended care for
lactating women and their infants
Contraindications – galactosemia, HIV, HTLV, active TB or varicella, active HSV on nipple
The Ten Steps to Successful Breastfeeding
1. Have a written breastfeeding policy that is routinely communicated to all health care
staff
2. Train all health care staff in the skills necessary to implement this policy
3. Inform all pregnant women about the benefits and management of breastfeeding
4. Help mothers initiate breastfeeding within one hour of birth
5. Show mothers how to breastfeed and how to maintain lactation, even if they are
separated from their infants

The Ten Steps to Successful Breastfeeding
6. Give infants no food or drink other than breast-milk, unless medically indicated
7. Practice rooming in – allow mothers and infants to remain together 24 hours a day
8. Encourage breastfeeding on demand
9. Give no pacifiers or artificial nipples to breastfeeding infants
10.Foster the establishment of breastfeeding support groups and refer mothers to them on
discharge from the hospital or birth center
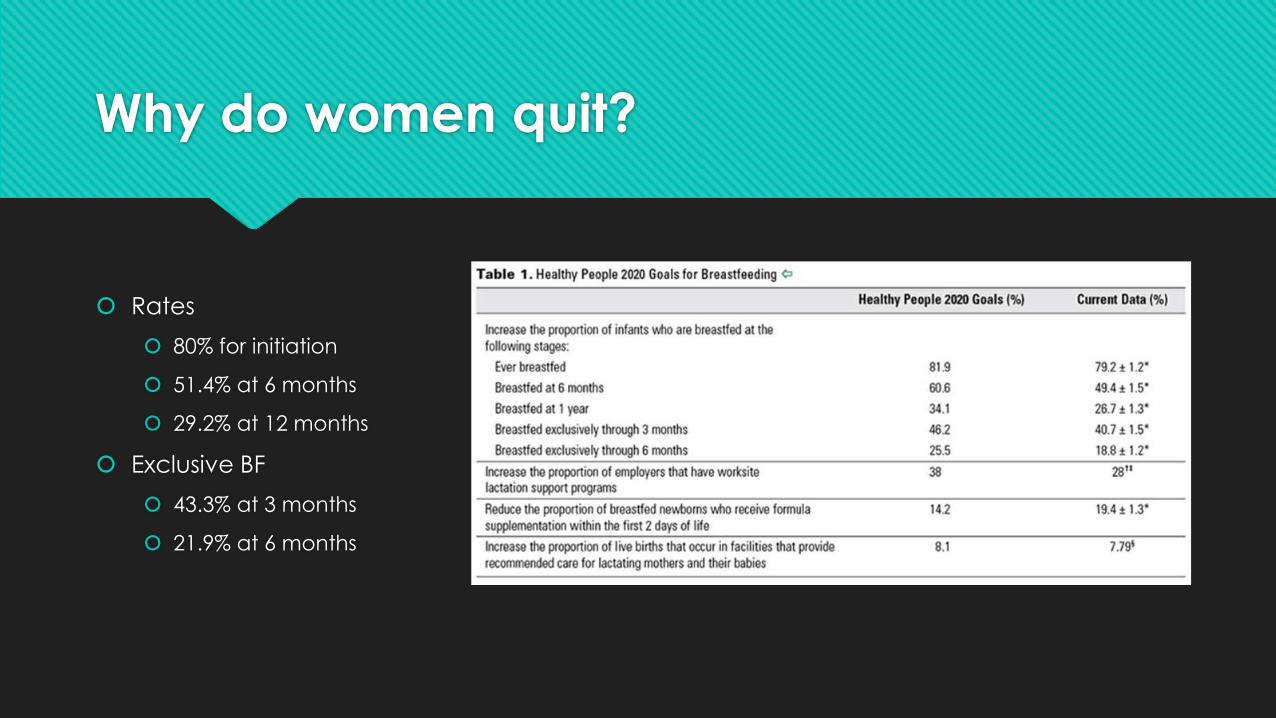
Why do women quit?
Rates
80% for initiation
51.4% at 6 months
29.2% at 12 months
Exclusive BF
43.3% at 3 months
21.9% at 6 months
Why do women quit?
Low milk volume
Work
Lack of support
PAIN
Differential
Nipple trauma
Mastitis
Areolar Dermatitis
Vasospasm
Oversupply
Engorgement
Blocked Duct
Candida
History
Onset – early (latch) vs. late (infectious)
Clinical setting (fullness vs. during pumping)
Feeding history (when milk came in, latch)
Previous breastfeeding experience
History of yeast infections
Maternal breast surgeries, implants, inverted nipples
Nipple pain during pregnancy
Hx of Raynaud’s or autoimmune disease
Physical Exam
Infant – focus on head and neck
Torticollis > unilateral sore nipple
Tight lingual frenulum > sore, traumatized nipples
Cleft lip/palate, retrognathia, large adenoids, oral defensiveness
Mucocutaneous candidiasis
Breast exam
Swelling, rash, vasospasm, impetiginized nipples pores, blocked pores, abrasions, ulcers, open cracks
Overfullness, masses, abscesses, tenderness, erythema
Feeding
Assessment of the latch and feeding technique
Nipple Soreness - timeline
Normal – subsides approx. 30 s to 1 m
after suckling begins; improves aver
PPD#4 and resolves after PPD#7
Not normal – persists at the same or at an
increasing level throughout nursing
episode; extends beyond the first
postpartum week

Nipple injury
Poor latch
Biting
Prevention
Proper positioning and latch
Avoidance of excessive moisture of the nipples and irritating cleansers
Lactation consultant
Evaluation of infant oral cavity
Anticipatory guidance regarding engorgement prior to hospital discharge
Care
Moist wound-healing principles
If cracked or abraded – antibiotic ointment (bacitracin or mupirocin)
If infected – culture
If thrush is suspected – KOH prep
Cool or warm compresses
Mild analgesics
APNO – mupirocin, miconazole, hydrocortisone
If persistent – consider exclusive pumping
Frenotomy with ankyloglossia
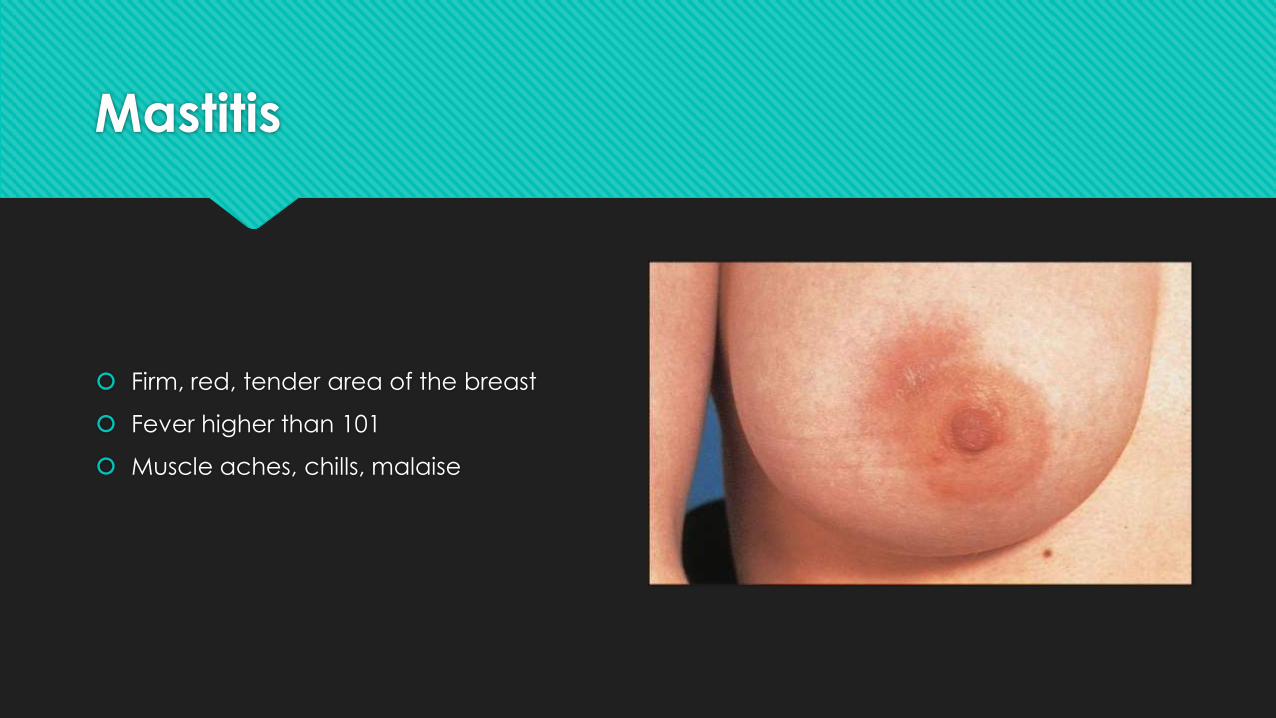
Mastitis
Firm, red, tender area of the breast
Fever higher than 101
Muscle aches, chills, malaise
Mastitis
2-10% of breastfeeding women
Week 1-6 – most common
Staph aureus – most common but don’t forget about MRSA
Damaged nipples or engorgement
Etiology
Partial blockage of milk duct
Pressure on the breast
Oversupply
Infrequent feedings
Nipple excoriation or craking
Rapid weaning
Illness in the mother or baby
Maternal stress or excesive fatigue
Maternal malnutrition
Mastitis
Symptomatic treatment
NSAIDs
Cold compresses
Complete emptying of the breast
Antibiotics (10-14 day course)
Dicloxacillin 500 mg PO QID or cephalexin 500 mg PO QID or clindamycin 300 mg PO TID
Clindamycin 300 mg PO TID or TMP-SMX 1 tab PO BID (not in newborns or compromised infants)
Vancomycin 15-20 mg/kg/dose Q8-12 hrs (do not exceed 2 g per dose)
No improvement within 24 hours > US imaging to look for abscess

Areolar Dermatitis
Tender, burning, red, fissures without
exudate
Itching, oozing with well-defined plaques
Areolar Dermatitis
Hx of eczema or psoriasis
Soaps, fragrances
Topical agents: lanolin, antifungals,
antibiotics
Management
Avoidance
Medium potency topical steroids (apply
after feeding and remove prior to next
feeding)
Vasospasm
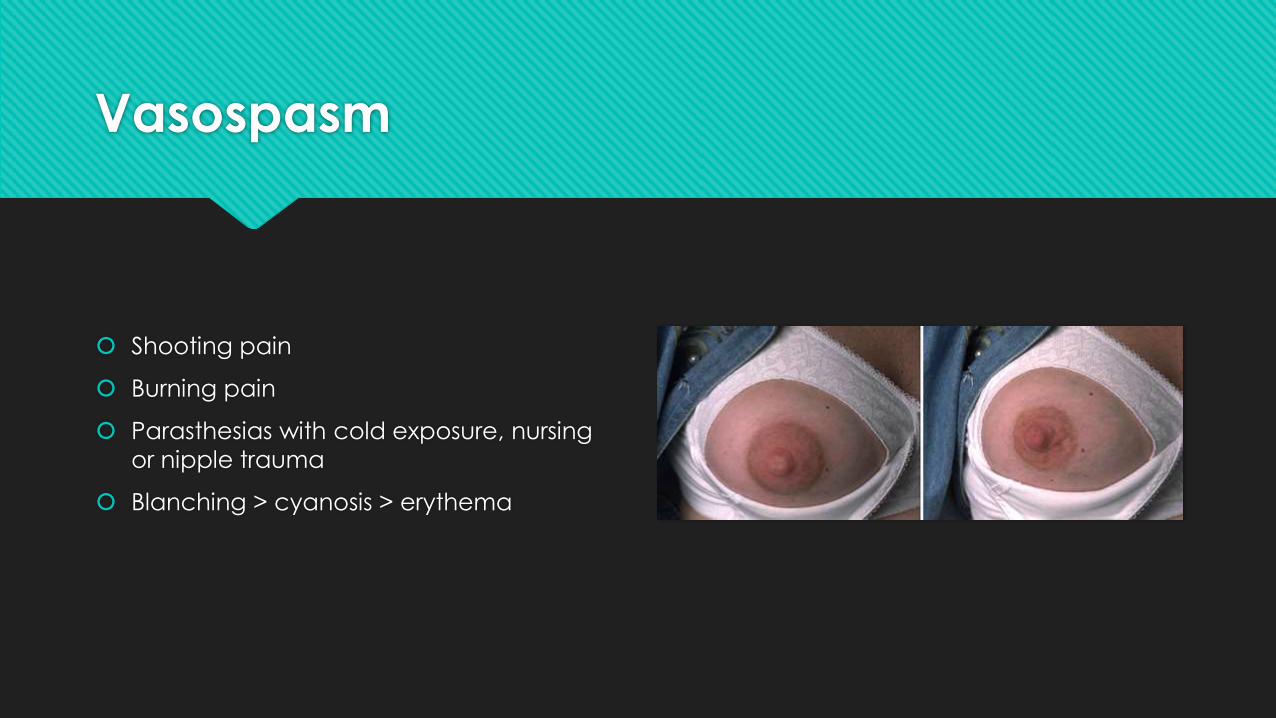
Shooting pain
Burning pain
Parasthesias with cold exposure, nursing
or nipple trauma
Blanching > cyanosis > erythema
Vasospasm
Prior nipple trauma with persistent pain
despite intact skin
Past hx of Raynauds, migraines or cold
sensitivity
Management
Warmth
Avoidance of vasoconstricting meds
(nicotine and caffeine)
Nifedipine
Oversupply
Infant pulls off breast in distress
Pain with latch
Infant coughs with let down
Explosive stools
Excellent weight gain or poor weight gain
Oversupply
Typically resolves over the first few weeks
Evaluate for drugs that increase milk
production
Thyroid disorder
Management
Nurse with infant in more upright position
Manual reduction of flow
Frequent burping
Block feedings
Avoid pumping
Cold compresses!
Low dose OCPs or pseudoephedrine
Engorgement
Breast fullness and firmness
Pain and tenderness

Engorgement
Primary
Onset of copious milk production
Day 3-5
Interstitial edema due to decreased
progesterone levels after placenta delivers
Secondary
Mismatch between production and
extraction
Management
Proper latch
Optimal positioning
Manual expression prior to nursing if areola
is involved
Pumping if needed
Warm compress/warm shower
Cold compresses between feedings
Analgesics
Cold green cabbage leaves
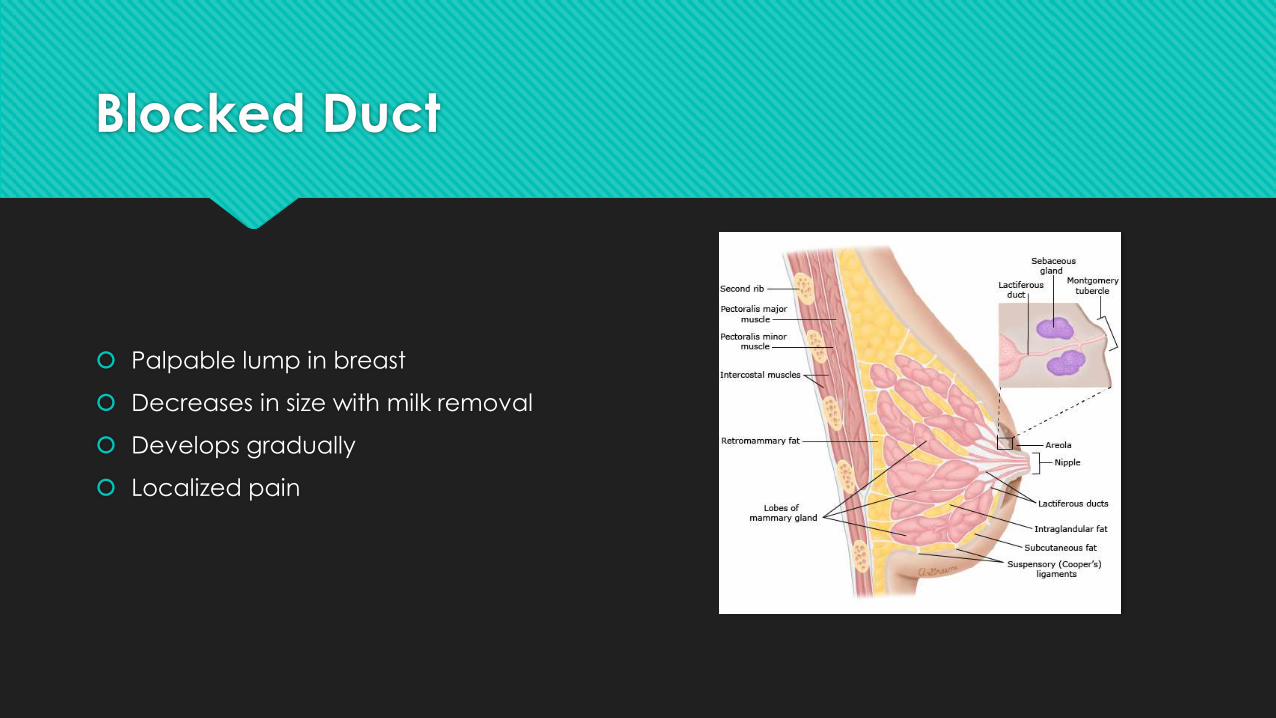
Blocked Duct
Palpable lump in breast
Decreases in size with milk removal
Develops gradually
Localized pain
Blocked Duct
Poor feeding technique
Tight clothing or ill-fitting brassiere
Abrupt decrease in feeding
Engorgement
Bacterial intraductal infections
Management
Optimize feeding (chin near area of
concern)
Pumping/hand expressing after feeding
DO NOT STOP BREASTFEEDING
Warm compresses or showers
Analgesics
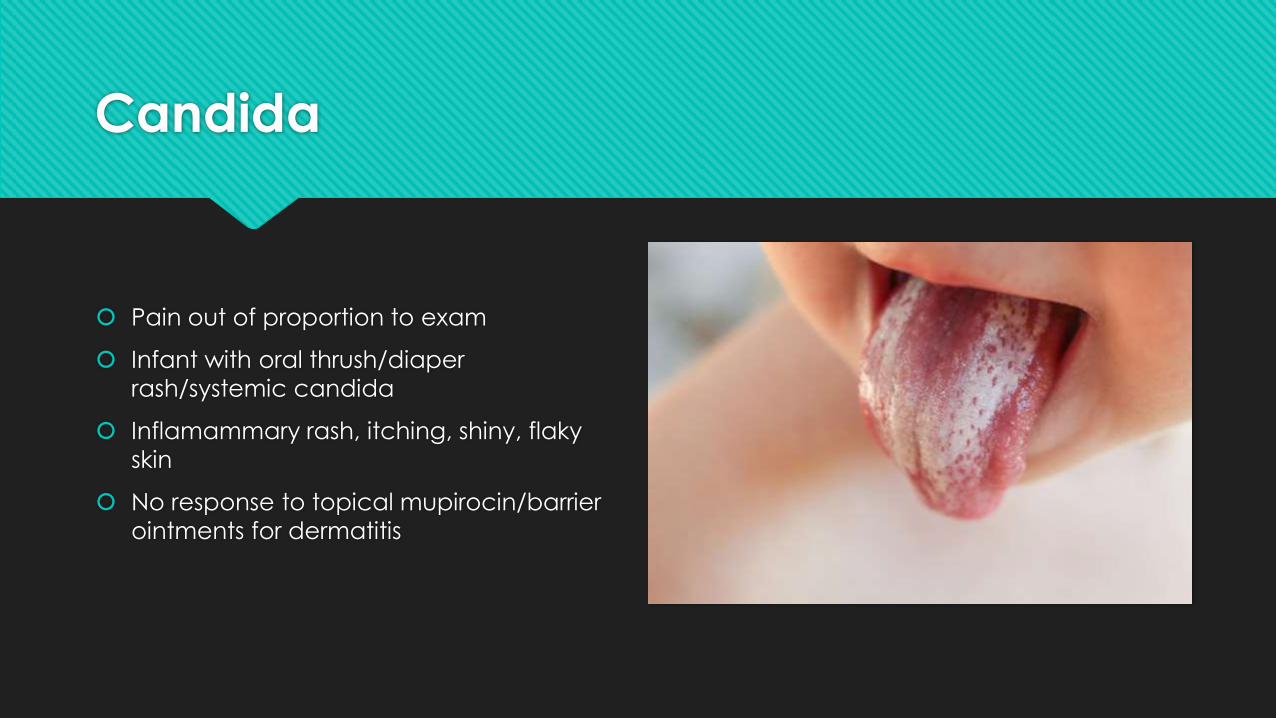
Candida
Pain out of proportion to exam
Infant with oral thrush/diaper
rash/systemic candida
Inflamammary rash, itching, shiny, flaky
skin
No response to topical mupirocin/barrier
ointments for dermatitis
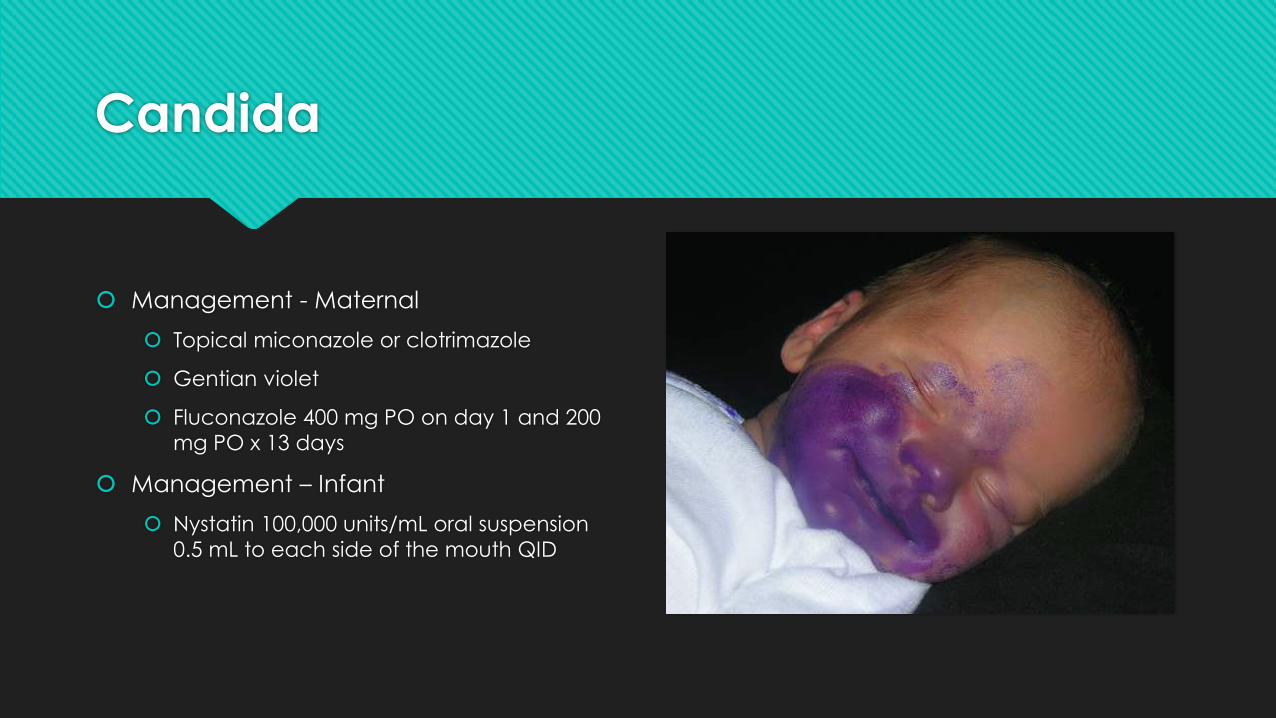
Candida
Management - Maternal
Topical miconazole or clotrimazole
Gentian violet
Fluconazole 400 mg PO on day 1 and 200
mg PO x 13 days
Management – Infant
Nystatin 100,000 units/mL oral suspension
0.5 mL to each side of the mouth QID
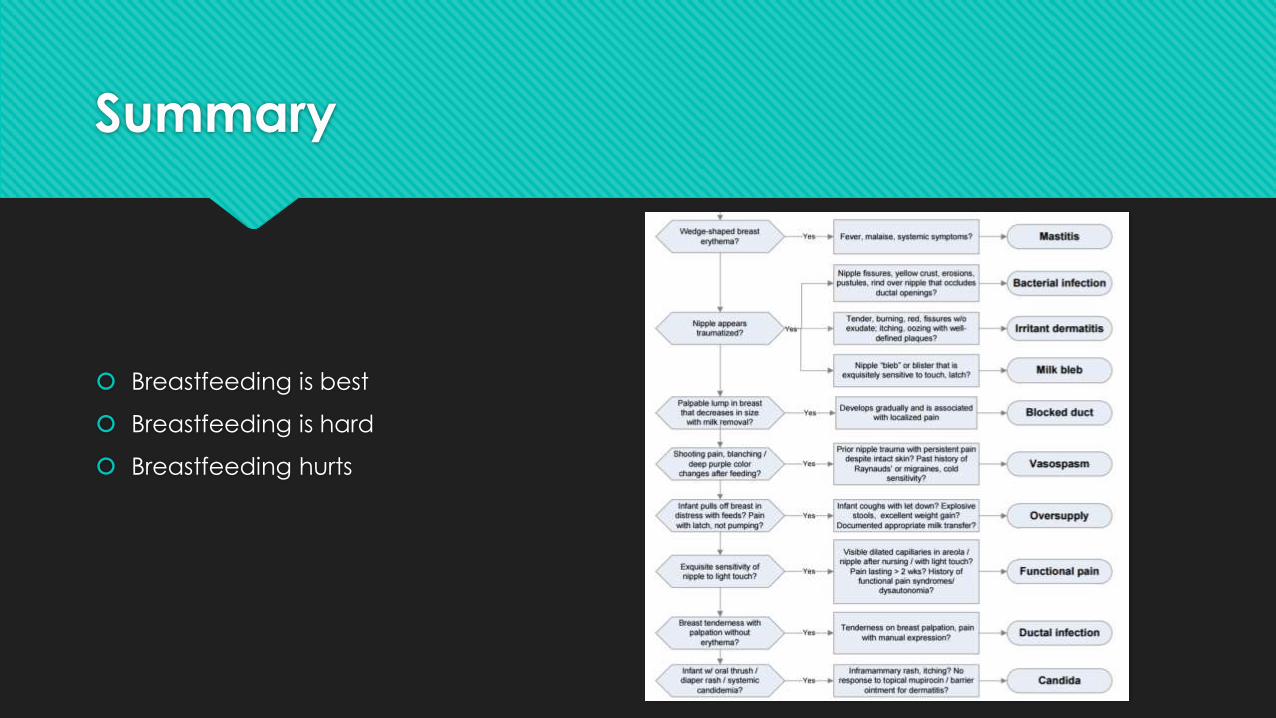
Summary
Breastfeeding is best
Breastfeeding is hard
Breastfeeding hurts
Thank you!
Resources
USPSTF Breastfeeding: Primary Care Interventions
WHO/UNICEF’s Ten Steps to Successful Breastfeeding
ACOG Committee Opinion #658, #570
UNC Center for Maternal and Infant Health OB Algorithms
Up to Date





























