Embed Size (px)
Citation preview

Management of bleeding
Andrew McDonaldAlberts Cellular Therapy
“All bleeding eventually stops”

n Modified Virchow’s triad
BLEEDING
Blood flowSizeBP
Vessel wallEndothelial activation
Collagen disordersAge
Corticosteroids
CoagulationPlatelets
Clotting factorsFibrinolytic system

n
• n

n

n Thrombin generation
LOW [Thrombin]
• VIII activation and release from vWF
• V activation and release from platelets
• Platelet activation
• XI activation
HIGH [Thrombin]
• Fibrin formation
• TAFI activation
• XIII activation
• Protein C activation (with thrombomodulin)

n
• n
Categories of patients
• Known “bleeders”– Anticoagulants or anti-
platelet agents– Other drugs
• Starch vol expanders, cephalosporins
– Inherited– Acquired
• ITP• Inhibitors• Cirrhosis• Uraemia
• Unknown– With bleeding history– Unexpected bleed
• Type of bleed:– ACUTE vs CHRONIC
– Minor– Major
• Admission required• 2 units RBC• Critical organ
– Life threatening• ICH• Massive GIT• Airway

n
• n
Nutrition and bleeding risk

n
Make a better clot
Drug• DDAVP• Oestrogen• Factor 8 concentrate• Activated rVIIa (Novoseven)• PCC (plasma derived –
Haemosolvex)• Fibrin glue
Transfusion• FFP• Platelets• Cryoprecipitate• [RBC]
Hold on to clot
• Make a better clot in the first place
• Tranexamic acid
Strategies for stopping bleeding

Clotting factors
Fibrinogen (I) Liver Cryoppt
Prothrombin (II)
Liver PCC
Factor V Liver (Cryoppt)
Factor VII Liver PCC
Factor VIII Liver Cryoppt Factor 8
Factor IX Liver PCC
Factor X Liver PCC
Factor XI Liver
(Factor XII) Liver
Factor XIII Liver + Megakaryocytes
Cryoppt
vWF Endothelium + Megakaryocytes
Cryoppt Factor 8

n
• n

n• Tranexamic acid –synthetic lysine analogue
– Blocks lysine binding site on plasminogen, preventing activation to plasmin
• Oral / mouthwash / IV• Typical dose 1-1.5G 6-8 hourly (range dose 2.5-100mg/kg)
• Useful in:– Menorrhagia– Dental extractions– Major surgery – orthopaedic, cardiac, urologic– Bleeding associated with
• Mild Haemophilia A and VWD• Platelet disorders
• Risk of thrombosis low
Anti-fibrinolytic agents

n• Modified analogue of ADH (AVP) • IV formulation (dose 0.3ug/kg/day)
– NB tachyphylaxis (25% less effective on day 2)
• Oral tabs and low dose nasal spray not effective for haemorrhage
• Increases endogenous factor 8 and VWF levels (via V2 receptor)
• Useful in mild Haemophilia A and Type 1 VWD• Also useful in platelet derived bleeding
– Mild inherited cytopathies– Antiplatelet agents– Mild/mod thrombocytopenia
• Contraindicated in known coronary artery disease• Side effect – headache, flushing, hyponatraemia
DDAVP

rhVIIa (Novoseven)
• Registered for bleeding in haemophilia with inhibitors• Used as a general haemostatic in severe life threatening
bleeding– Massive trauma– Massive APH / PPH– Cardiac surgery– ICH
• Expensive – reimbursement issues• Increased thrombotic events (OR 1.6)• Dose 90ug/kg; not effective in severe acidosis,
hypothermia, and low platelets
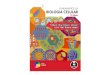
Perc
ent
of
pati
ents
(%
)
0102030405060708090
100
RBC units within 48 hours 0 5 10 15 20 25 30 35 40 45 50
NovoSeven® (N=52)
Placebo
(N=59)
P= 0.019
≥ 8
Boffard KD et al. J Trauma 2005;59(1):8-18

n
• All anticoagulants increase bleeding risk• Scoring systems to predict, but bleeding often
unpredictable• HAS-BLED score
– Hypertension,abnormal kidney/liver, Stroke, Bleeding history, labile INR, Elderly (>65), Drugs/alcohol
Reversal of anticoagulation
Risk of bleed
Difficulty in reversal
OLD NEW

n
Warfarin:Withhold warfarin only:• 2 older case series total 299 pts, with 352 INR values >6• 2 pts (0.6%) suffered haemorrhage
Glover et al 1995
Lousberg et al 1998
• 1104 pts with INR >5• 30 day incidence of major bleeds low at 1.3%• Subanalysis of 42 pts (4.3%) with INR >9
- incidence major bleeds 9.6% (4pts)
- more likely to receive Vitamin K (62% vs 7%)
Garcia et al 2006
Reversal of anticoagulation

n
Warfarin:Withhold wafarin and give Vit K:• IV Vit K - 2 small studies
– 31 pts (10 received 1mg, 21 received 0.5mg IV)– 50% pts with 1mg INR @24h <2, – all pts with 0.5mg between INR 2 - 5.5 @24h Shetty et al 1992
– Anaphylaxis est. 3 / 10 000 administrations
• Oral Vit K 1 – 2.5 mg safe and no risk of warfarin resistance– 7 small studies: less bleeding with Vit K use and more rapid control– 59 pts with mechanical heart valve with INR 6 - 12– 13/29 vs 4/30 with INR in range @24h with Vit K 1mg vs placebo– 3/29 (10%) with INR <1.8 @24h with Vit K Ageno et al 2005
ORAL > IV > Subcut
Reversal of anticoagulation

n
Warfarin:Urgent reversal• CNS or vital organ haemorrhage• Major bleed (requiring admission, transfusion
RBC)
• Uncertainty of variable vs fixed dose PCC - Haemosolvex
Reversal of anticoagulation

n• UFH
– Short T1/2 – expectant management possible
– Reversal with protamine sulphate 1mg/100IU IV• Max 50mg in 10 min
• LMWH– Longer T1/2, but more predictable, less bleeding
– Prolonged effect in renal dysfunction– Protamine sulphate 50-70% effective– Dose as above or 0.5-1mg/mg enoxaparin
• Fondaparinux– Long T1/2 of 20 hours, longer in renal failure
– Protamine not effective– Novoseven ???
Reversal of anticoagulation

n Reversal of anticoagulation
Rivaroxaban Dabigetran
• Anti –Xa• Dose 10mg daily• Tmax 2.5-4h
• T1/2 5-9h, 9-13h (elderly)
• Daily dose• 66% faecal, 33% renal• PCC / VIIA / FEIBA for
bleeding• Assay: anti-Xa• Drug interaction CYP3A4
• Anti-thrombin• Dose 150-200mg• Tmax 2h
• T1/2 14-17 h
• Daily or BD dose• 80% renal, 20% fecal• No current antidote
• Possible dialysis
• Assay: Ecarin clotting time• PPI decrease absorption

nDRUG ACTUAL T1/2
EFFECTIVE THERAPY for
BLEED
Aspirin 15-30min 4-5 days DDAVPPlatelet
transfusion
P2Y12 receptor inhibitors: clopidogrel
8h 5-7 days ? DDAVPPlatelet
transfusion
P2Y12 receptor inhibitors: prasugrel
7 hours 5-7 days Platelet transfusion
P2Y12 receptor inhibitors: ticagrelor
7 hours < 30% effect after 2 days
Wait
Reversal of anti-platelet agents

n
• Chronic bleeding– Lab tests – make a diagnosis
• Acute bleed with anticoagulants– Reverse as per guidelines
• Acute bleed – unexpected– TEG and lab– Tranexamic acid/DDAVP/FFP
SUMMARY