Embed Size (px)
Citation preview
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific
conditions. Clinical data in a particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are
institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
Optima Health
Management of Bipolar Disorder
Guideline History
Date
Approved 5/02
Date
Revised 1/06, 1/09, 1/11
Date
Reviewed 5/06, 1/08, 1/13, 1/15
Next
Review
Date 1/17
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical
data in a particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed
recommendations and are not intended as a substitute for clinical judgment.
Key Points
NOTE: Upon the recommendation of our Medical Care Review Committee (MCRC),
Optima Health does not support the following components contained in this
guideline:
1. Use of lamotrigine as monotherapy for bipolar depression (p. 19)
2. Maximum dose of 60 mg citalopram (due to FDA warning regarding
QT interval prolongation) (Appendix D, p. 61)
The lifetime prevalence of bipolar I disorder is estimated at 0.8% of the adult population,
with a range between 0.4% and 1.6%. Bipolar II disorder affects approximately 0.5% or
more of the population. Bipolar II disorder is more common in women; bipolar I disorder
appears to be evenly distributed between men and women.
Bipolar disorder is often comorbid with a range of other mental disorders such as substance
misuse and anxiety disorders.
Patients with Bipolar disorder can present with: a major depressive episode, manic episode,
hypomanic episode or a combination of manic and depressive symptoms (mixed episode).
This guideline contains separate algorithms based on presentation.
A complete clinical assessment should include: medical comorbidities, psychiatric
comorbidities, psychosocial status, current medications, response to past medications,
medication compliance and substance use.
Medications for mania and mixed episodes may take 5-10 days to begin showing a
significant positive effect. After any change in medication or dose, monitor the patient for
both positive and adverse effects. Reassess every 1-2 weeks for at least 6 weeks.
DSM-IV-TR defines Full Remission as “a period of at least 2 months in which there are no
significant symptoms” of mania or depression.
Patients with bipolar disorder who achieve a satisfactory clinical response (symptom
remission) should continue maintenence treatment.
Patients being prescribed an atypical antipsychotic should be monitored for possible
metabolic effects. (Our guideline “Monitoring Clients on Atypical Antipsychotics and
Management of Metabolic Effects” is available on the Optima website.) Communicate
and coordinate care with patient’s primary care physician (PCP) as needed.
Recent studies indicate positive benefit of psychoeducation and psychotherapy to address
stressors and comorbidities, symptom management, coping strategies and medication
adherence.
VA/DaD Clinical Practice GuidelineforManagement of Bipolar Disorder in Adults
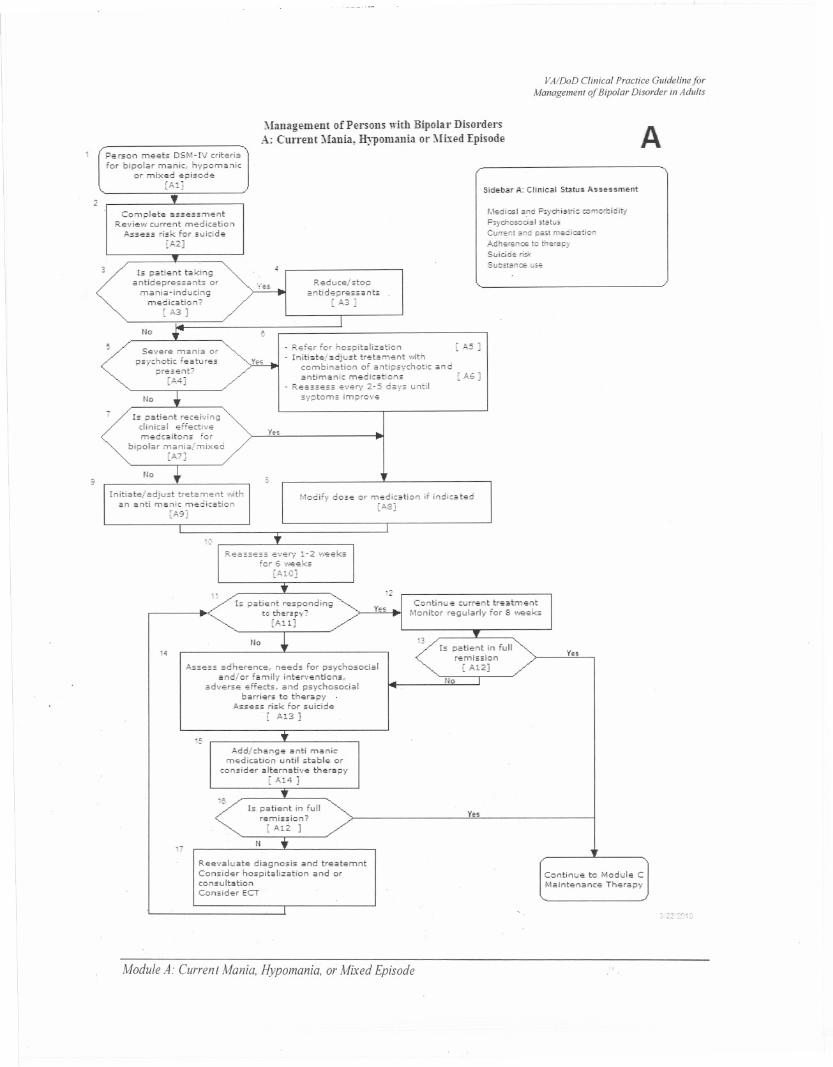
Management of Persons with Bipolar DisordersA: Current Mania, HypomanIa or Mixed Episode A
Person me.ets DSM-l\! criteri"for bipolar manic, hypomanic
or mixed episode[AIJ Sidebar A: Clinical Status Assessment
2
No
Medicsl smj P5yd1iatric romerbidit1
Psyd10seda I .tstu.Current sndpsstmee! ication
Adhersnce te therspySuidde ris,SubstanO? use
Complete assessm..ntRe...i~w current medication
Assess risk fo.r suicide
[A2]
Is patient takingantidepressants or
mania-inducingmedication?
[ ,0.3 ]
Reduce/stopantidepres5<",ts
["'3 J
Se'.'ere mani" orpsychotic Features
present?[M]
- Ref..r for hospitalization- Initiate/adjust tr.;tament with
combination of antipsychotic andantimanic medications
- Reassess every 2-5 days untilsyptoms improve
[,0.5 J
[A6 ]
Is patient recei'.'ingdin lea I e ffeetivemedcaitons For
bipolar mani,,/mixed[Al]
y.,
No3
Initiate/adjust tretarnent ",ithan anti manic medication
[A9]
Modif',' dose or medication if indicated[A8J
"0
Is patient respondingto ther"p~'?
[Ail]
Ccntinu e current tr"atment
f'.lonitor regularly for 8 "",eks
NoIs patient in full
remission[ A12]
Ye..14
Ass"ss adh"rence, n"eds For psychosocialand/or family interventions.,
adverse "FFeets; and p.sI'chasodalbarri"rs to th"rapy .
Assess risk for suicide
[ ,0.13]
No
f~,
Add/change anti manicmedication until stable or
consider alternative therap',[ ,0..14 J
'eIs. patient in Full
remission?[Ali ]
Ye"
17N
R"evaluat" diagnosis and treatemntConsider hospitalizahon and orconsultationConsider ECT
C,mtinue to Module CMaintenance ThErapy
22:YYC,
Module A: Current Mania, Hypomania,or Mixed Episode
VAlDoD Clinical Practice Guideline forManagement of Bipolar Disorder in Adults
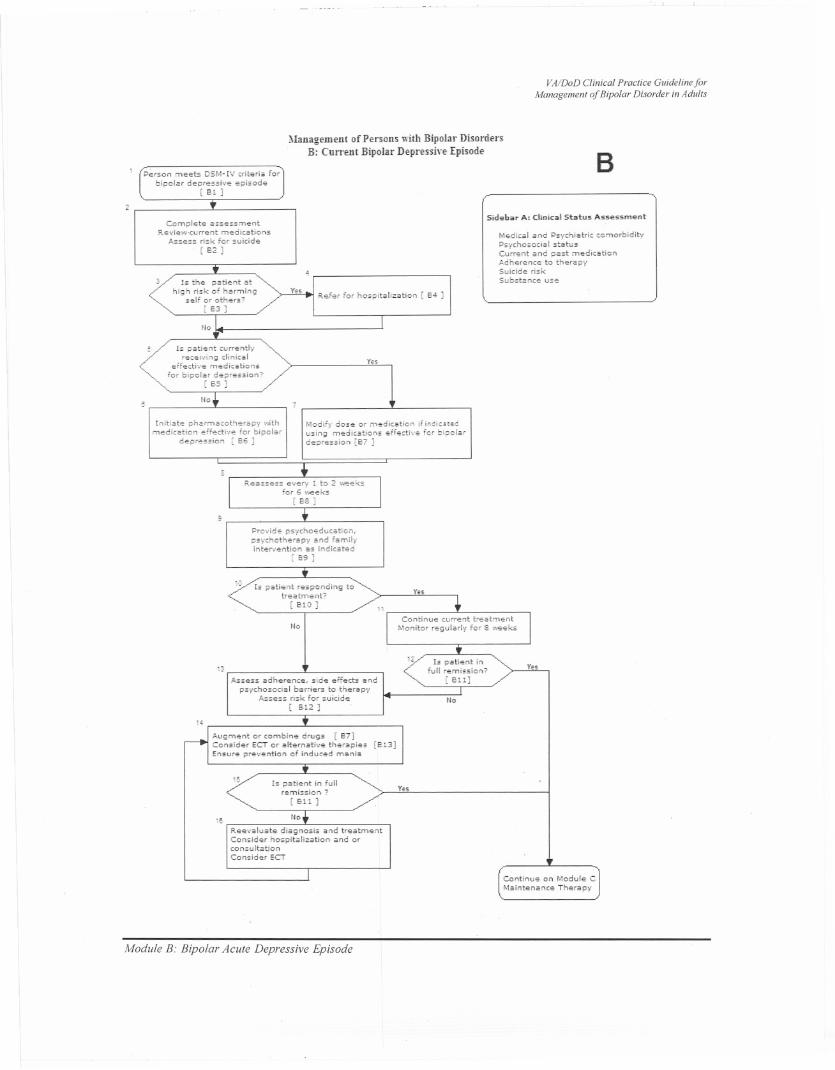
Management of Pel'sons with Bipolar DisordersB: Current Bipolar Depressive Episode
Person meets D5M-IV <rite ria fo,bipolar depre.,.;,e episode
[ 101 )
2
Complete asse.smentRe,iew.wrrent medications
A,sess risk for sukide[62 ]
Is the patient athigh ri.k of harm;ne
-self or others? -[63 ]
Refer for hospitalization [ 64 ]
No
Is pati..nt currentlyrH..iving dinical
e,f..di"... m..dieation.for bipolar depre.sion?
[ 65 ]
No
Initiat.. p"armacob..rapy ,',it;,medication ..ffecti',e fo, biod.r
d..pre.sion [66 ] .
B
Sidebar A; Clinical Status Asse..ment
Medical and ".vchiatrio comorbidit--",.,cho.ocial .t~tu. .Current and paot medic.tionA.dherence to therapySuidde ri.kSubstanc.. us..
Yu
Modify dose or medication if inoiotedusing medications effedive for bipola,d..pression [67 ]
~
Pro,'ide p.ycho"ducation,a"rchab"rapy and familyinte""ntion as indioated
[ 69 ]
,'JIs pati"nt r"".pending to
treatment?[ 610 ]
No
'J;"sess adher..nce, side eff..ds and
pS',ohesocial barri..rs to therapyAss..ss risk for suioid..
[ Bl2 ]
Augment or combin.. drugs [E!t]Consider 6CT or altemativ.. therapies [Bl3]Ensur.. p, ntion of induced m.nia
15Is patient in full
remission?[ 611]
:e No
Reevaluate diagnosis and treatmentConsid..r hospitalization and orconsultationCOMid"r ECT
Yu
Yu
No
Yu
Continue on Module CMaintenanc<: Th",apy
Module B: Bipolar Acute Depressive Episode
VAlDoD Clinical Practice Guideline forManagement of Bipolar Disorder in Adults
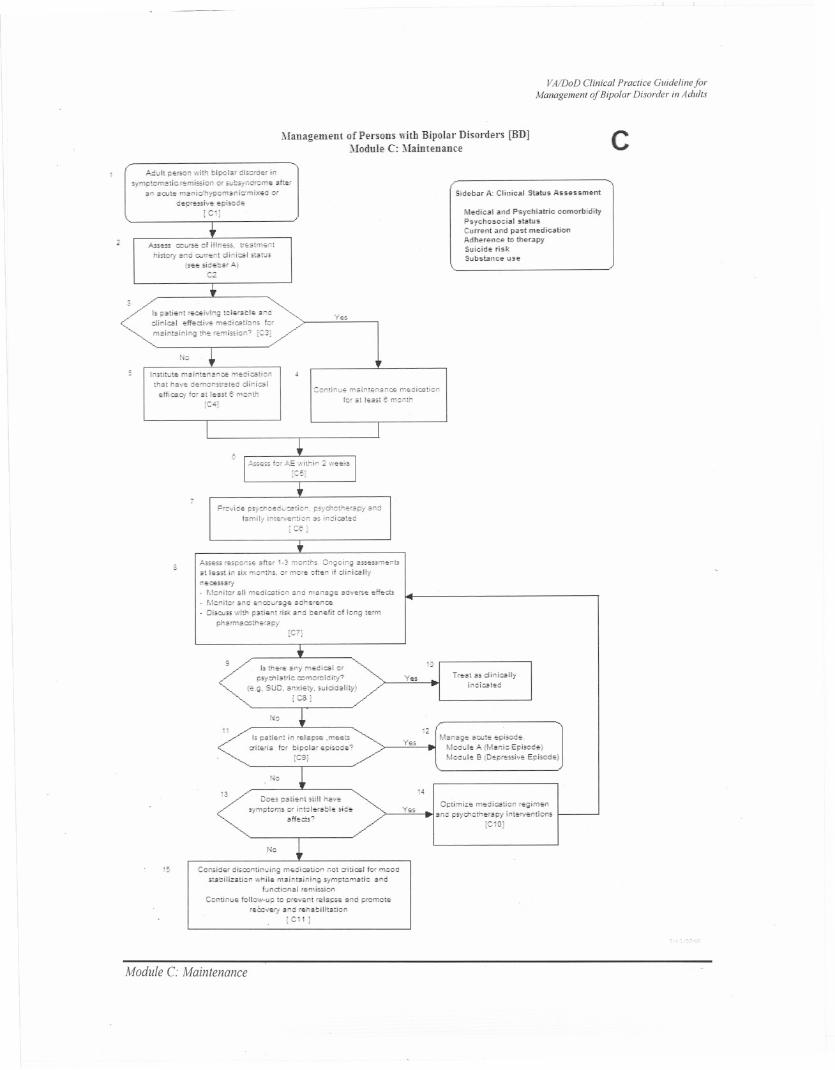
1Ilanagement of Pel'sons with Bipolar'Disorders [BDJModule C: Maintenance c
I'"""tt PE""" with hipolEr dIS"'<:H insimptcm"ticrEmission '" se!o3).oc{cm", aftE'
an acctE manldhypcms.oidmixec "'fcEp'"",iv" "'plsooe
iC1!
Sid..b2r A: CHnica.1 Status Aasessm..nt
AssESS rocrse d IIIness, ""atment
hist",", s"ccw,ent dioiesl st.w.(.e", sld~baf ,A,j
D.2
M..dical and Ps.ychiatric comorbldftyPsychosocial status,C"rrent and past medicationAdh..r..n<:e to tn..rapySuicide riskSubslanc," us,"
3
Is pstlent "'eEI>;hg tclHSbl.. aoddlnl"".1 ~ffEdivE meeiD!!ti,,", kr
maintaining th"r~mlssi"n? IC3!,/'"
YES
Nc
losmut", mE"t"nEOeE m;;diesti':nthat ha'f" d..m"nsirat"d dlnl"",1
"mcaey f", at 1"5;; e mcnth[C4I
Gontine" rr,alntenance mEdicationfo, ,at I"as' " m':oth
~
"ro'ii"" !,->yd1""ceostice, psy&':thS'ap"i Endlamlli 1","NEnti"n as indiest,,"
I Ct)
;'.$,:".>5'''.p"ns. aftS' ,-3 m"eths, On,g"icg a""..m.nt>at 1.5st In six -nt"" (X mcrE clt.n if dioies.llyn.cessa,,!- Mcnitcr Ell m.dication ano n,.ea.g" adv.,," Eff.ct>- Mcnitcand .nrours-g..adh",.no;,- Dis,",ss with pati..nt ,is. and O;""..frt ot 10"9 tS'm
ph~"m~ ""th.,apy[CT)
, IsthS'.. any meeical '"~fxiatic =mo,bidi!y?
(e,.g, SUD, ."xl"t';', suiddEJiiy)fC<8!
10
y", TI.st as di,icarlyIndicat,,"
N:
!1 13M.nag. acct plsod.,
Mooel. A (Manic Eplsod.)MOdel. 5 (D"",""lv", Epiooo,,)
I. pali",,,!in '.Iapo.. ,m..",,,o-it6io kf blpolar"piS:'<i",
ICe]
YES
r-lc
Do", p~ti"nt ,till h"v.sympt:ms", IntdeJabi.. ,id",
.ff.::;is?
,4
y.s Optimiz" ""'dlesti:, '''9i"",nane 1"')'''''''10,''''10/IntiON..nti"ns
iC10]
rb
1:, Censid"" disrontinuing m..dicatic" net critical for meedstabilizati"" "hi!.. msln'"ieing oymptomatic and
functional ,,,mlssi,,n
Continue tonC"""p to pt,="..nt ,..I~1OSE'and p'""",te'''C:>;''-':; am! ,,,habilitEtion
IC,1 j
Module C: Maintenance
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a
particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
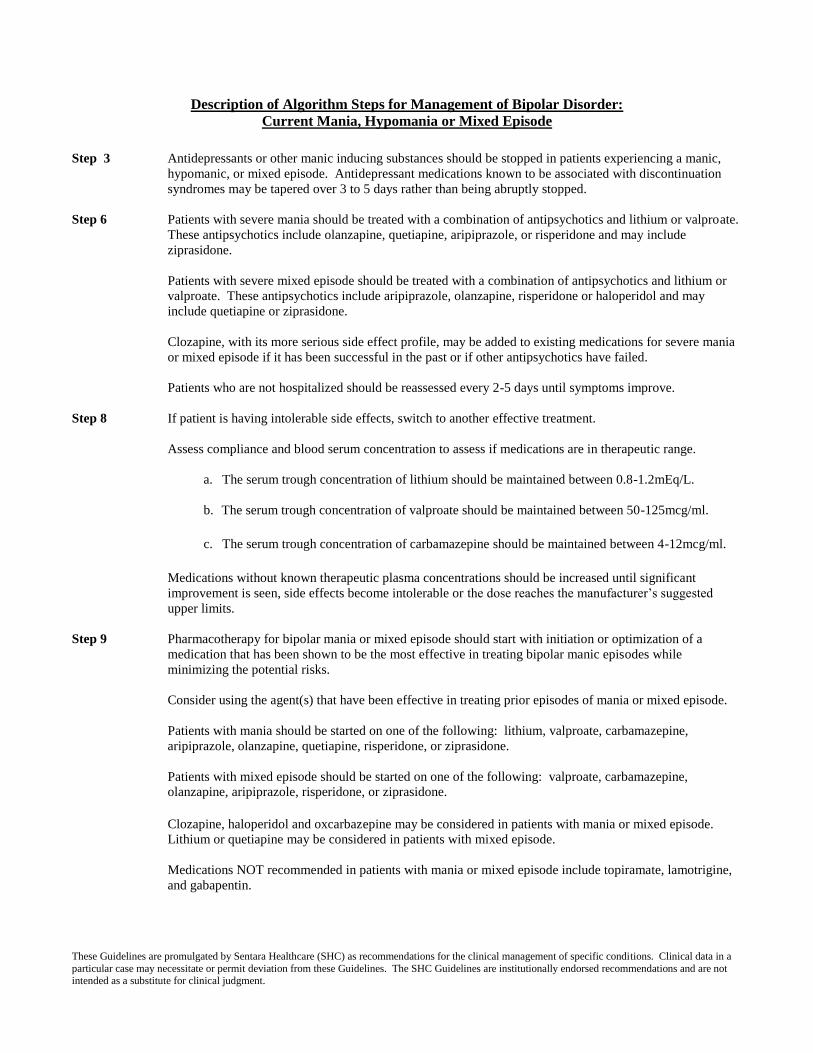
Description of Algorithm Steps for Management of Bipolar Disorder:
Current Mania, Hypomania or Mixed Episode
Step 3 Antidepressants or other manic inducing substances should be stopped in patients experiencing a manic,
hypomanic, or mixed episode. Antidepressant medications known to be associated with discontinuation
syndromes may be tapered over 3 to 5 days rather than being abruptly stopped.
Step 6 Patients with severe mania should be treated with a combination of antipsychotics and lithium or valproate.
These antipsychotics include olanzapine, quetiapine, aripiprazole, or risperidone and may include
ziprasidone.
Patients with severe mixed episode should be treated with a combination of antipsychotics and lithium or
valproate. These antipsychotics include aripiprazole, olanzapine, risperidone or haloperidol and may
include quetiapine or ziprasidone.
Clozapine, with its more serious side effect profile, may be added to existing medications for severe mania
or mixed episode if it has been successful in the past or if other antipsychotics have failed.
Patients who are not hospitalized should be reassessed every 2-5 days until symptoms improve.
Step 8 If patient is having intolerable side effects, switch to another effective treatment.
Assess compliance and blood serum concentration to assess if medications are in therapeutic range.
a. The serum trough concentration of lithium should be maintained between 0.8-1.2mEq/L.
b. The serum trough concentration of valproate should be maintained between 50-125mcg/ml.
c. The serum trough concentration of carbamazepine should be maintained between 4-12mcg/ml.
Medications without known therapeutic plasma concentrations should be increased until significant
improvement is seen, side effects become intolerable or the dose reaches the manufacturer’s suggested
upper limits.
Step 9 Pharmacotherapy for bipolar mania or mixed episode should start with initiation or optimization of a
medication that has been shown to be the most effective in treating bipolar manic episodes while
minimizing the potential risks.
Consider using the agent(s) that have been effective in treating prior episodes of mania or mixed episode.
Patients with mania should be started on one of the following: lithium, valproate, carbamazepine,
aripiprazole, olanzapine, quetiapine, risperidone, or ziprasidone.
Patients with mixed episode should be started on one of the following: valproate, carbamazepine,
olanzapine, aripiprazole, risperidone, or ziprasidone.
Clozapine, haloperidol and oxcarbazepine may be considered in patients with mania or mixed episode.
Lithium or quetiapine may be considered in patients with mixed episode.
Medications NOT recommended in patients with mania or mixed episode include topiramate, lamotrigine,
and gabapentin.
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a
particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
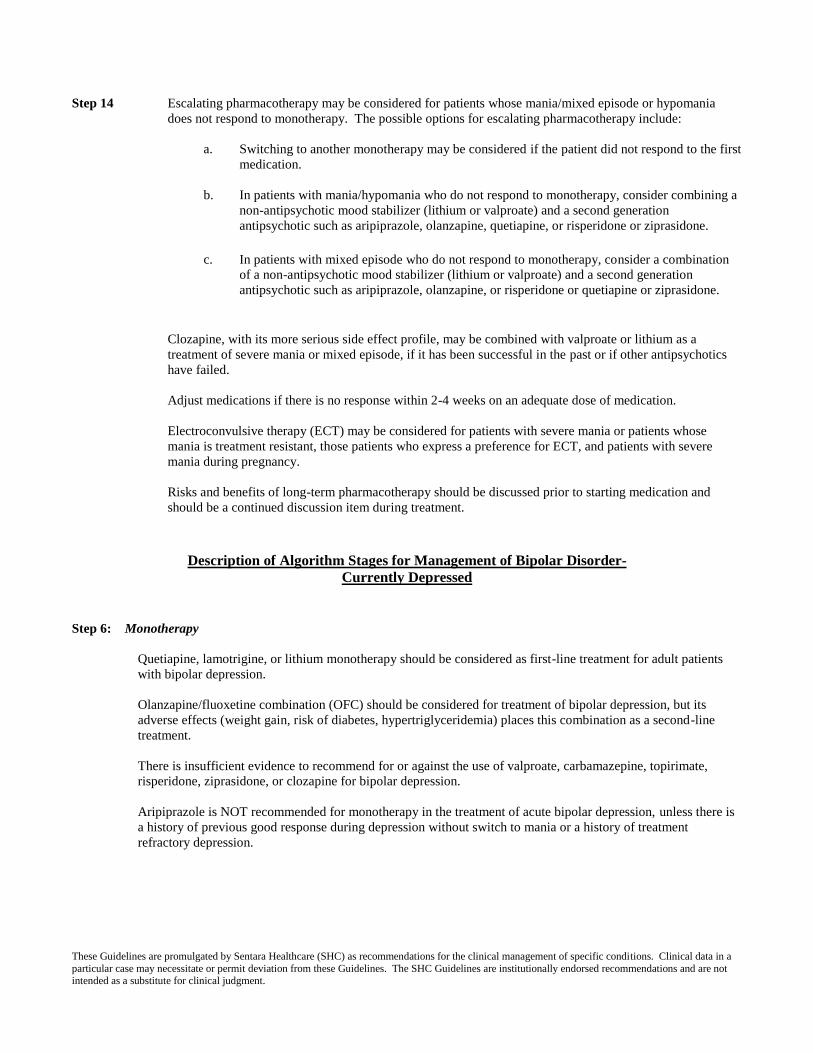
Step 14 Escalating pharmacotherapy may be considered for patients whose mania/mixed episode or hypomania
does not respond to monotherapy. The possible options for escalating pharmacotherapy include:
a. Switching to another monotherapy may be considered if the patient did not respond to the first
medication.
b. In patients with mania/hypomania who do not respond to monotherapy, consider combining a
non-antipsychotic mood stabilizer (lithium or valproate) and a second generation
antipsychotic such as aripiprazole, olanzapine, quetiapine, or risperidone or ziprasidone.
c. In patients with mixed episode who do not respond to monotherapy, consider a combination
of a non-antipsychotic mood stabilizer (lithium or valproate) and a second generation
antipsychotic such as aripiprazole, olanzapine, or risperidone or quetiapine or ziprasidone.
Clozapine, with its more serious side effect profile, may be combined with valproate or lithium as a
treatment of severe mania or mixed episode, if it has been successful in the past or if other antipsychotics
have failed.
Adjust medications if there is no response within 2-4 weeks on an adequate dose of medication.
Electroconvulsive therapy (ECT) may be considered for patients with severe mania or patients whose
mania is treatment resistant, those patients who express a preference for ECT, and patients with severe
mania during pregnancy.
Risks and benefits of long-term pharmacotherapy should be discussed prior to starting medication and
should be a continued discussion item during treatment.
Description of Algorithm Stages for Management of Bipolar Disorder-
Currently Depressed
Step 6: Monotherapy
Quetiapine, lamotrigine, or lithium monotherapy should be considered as first-line treatment for adult patients
with bipolar depression.
Olanzapine/fluoxetine combination (OFC) should be considered for treatment of bipolar depression, but its
adverse effects (weight gain, risk of diabetes, hypertriglyceridemia) places this combination as a second-line
treatment.
There is insufficient evidence to recommend for or against the use of valproate, carbamazepine, topirimate,
risperidone, ziprasidone, or clozapine for bipolar depression.
Aripiprazole is NOT recommended for monotherapy in the treatment of acute bipolar depression, unless there is
a history of previous good response during depression without switch to mania or a history of treatment
refractory depression.
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a
particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
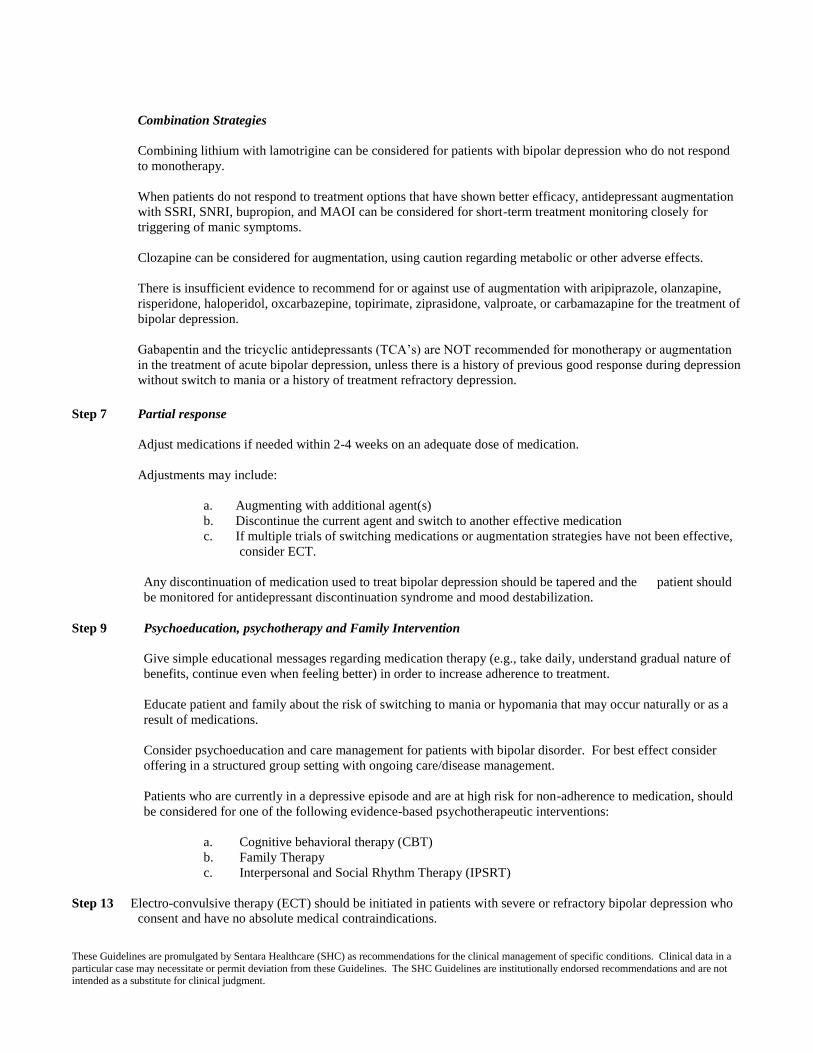
Combination Strategies
Combining lithium with lamotrigine can be considered for patients with bipolar depression who do not respond
to monotherapy.
When patients do not respond to treatment options that have shown better efficacy, antidepressant augmentation
with SSRI, SNRI, bupropion, and MAOI can be considered for short-term treatment monitoring closely for
triggering of manic symptoms.
Clozapine can be considered for augmentation, using caution regarding metabolic or other adverse effects.
There is insufficient evidence to recommend for or against use of augmentation with aripiprazole, olanzapine,
risperidone, haloperidol, oxcarbazepine, topirimate, ziprasidone, valproate, or carbamazapine for the treatment of
bipolar depression.
Gabapentin and the tricyclic antidepressants (TCA’s) are NOT recommended for monotherapy or augmentation
in the treatment of acute bipolar depression, unless there is a history of previous good response during depression
without switch to mania or a history of treatment refractory depression.
Step 7 Partial response
Adjust medications if needed within 2-4 weeks on an adequate dose of medication.
Adjustments may include:
a. Augmenting with additional agent(s)
b. Discontinue the current agent and switch to another effective medication
c. If multiple trials of switching medications or augmentation strategies have not been effective,
consider ECT.
Any discontinuation of medication used to treat bipolar depression should be tapered and the patient should
be monitored for antidepressant discontinuation syndrome and mood destabilization.
Step 9 Psychoeducation, psychotherapy and Family Intervention
Give simple educational messages regarding medication therapy (e.g., take daily, understand gradual nature of
benefits, continue even when feeling better) in order to increase adherence to treatment.
Educate patient and family about the risk of switching to mania or hypomania that may occur naturally or as a
result of medications.
Consider psychoeducation and care management for patients with bipolar disorder. For best effect consider
offering in a structured group setting with ongoing care/disease management.
Patients who are currently in a depressive episode and are at high risk for non-adherence to medication, should
be considered for one of the following evidence-based psychotherapeutic interventions:
a. Cognitive behavioral therapy (CBT)
b. Family Therapy
c. Interpersonal and Social Rhythm Therapy (IPSRT)
Step 13 Electro-convulsive therapy (ECT) should be initiated in patients with severe or refractory bipolar depression who
consent and have no absolute medical contraindications.
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a
particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
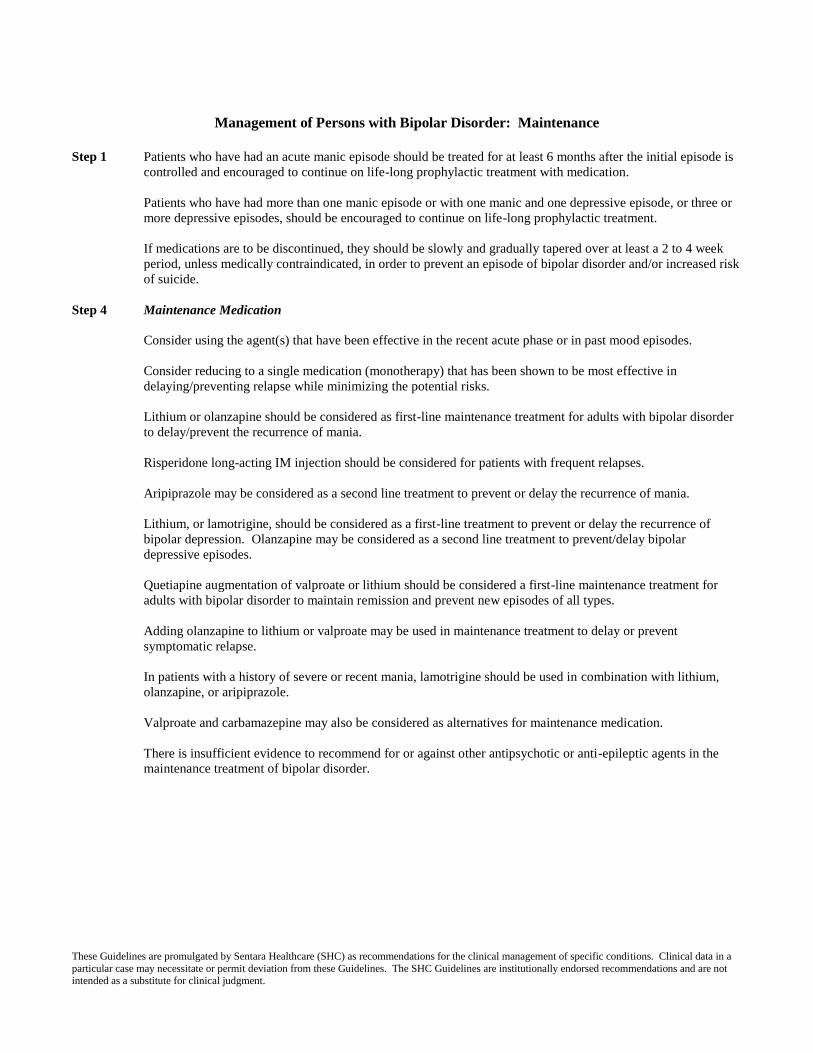
Management of Persons with Bipolar Disorder: Maintenance
Step 1 Patients who have had an acute manic episode should be treated for at least 6 months after the initial episode is
controlled and encouraged to continue on life-long prophylactic treatment with medication.
Patients who have had more than one manic episode or with one manic and one depressive episode, or three or
more depressive episodes, should be encouraged to continue on life-long prophylactic treatment.
If medications are to be discontinued, they should be slowly and gradually tapered over at least a 2 to 4 week
period, unless medically contraindicated, in order to prevent an episode of bipolar disorder and/or increased risk
of suicide.
Step 4 Maintenance Medication
Consider using the agent(s) that have been effective in the recent acute phase or in past mood episodes.
Consider reducing to a single medication (monotherapy) that has been shown to be most effective in
delaying/preventing relapse while minimizing the potential risks.
Lithium or olanzapine should be considered as first-line maintenance treatment for adults with bipolar disorder
to delay/prevent the recurrence of mania.
Risperidone long-acting IM injection should be considered for patients with frequent relapses.
Aripiprazole may be considered as a second line treatment to prevent or delay the recurrence of mania.
Lithium, or lamotrigine, should be considered as a first-line treatment to prevent or delay the recurrence of
bipolar depression. Olanzapine may be considered as a second line treatment to prevent/delay bipolar
depressive episodes.
Quetiapine augmentation of valproate or lithium should be considered a first-line maintenance treatment for
adults with bipolar disorder to maintain remission and prevent new episodes of all types.
Adding olanzapine to lithium or valproate may be used in maintenance treatment to delay or prevent
symptomatic relapse.
In patients with a history of severe or recent mania, lamotrigine should be used in combination with lithium,
olanzapine, or aripiprazole.
Valproate and carbamazepine may also be considered as alternatives for maintenance medication.
There is insufficient evidence to recommend for or against other antipsychotic or anti-epileptic agents in the
maintenance treatment of bipolar disorder.
These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a
particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
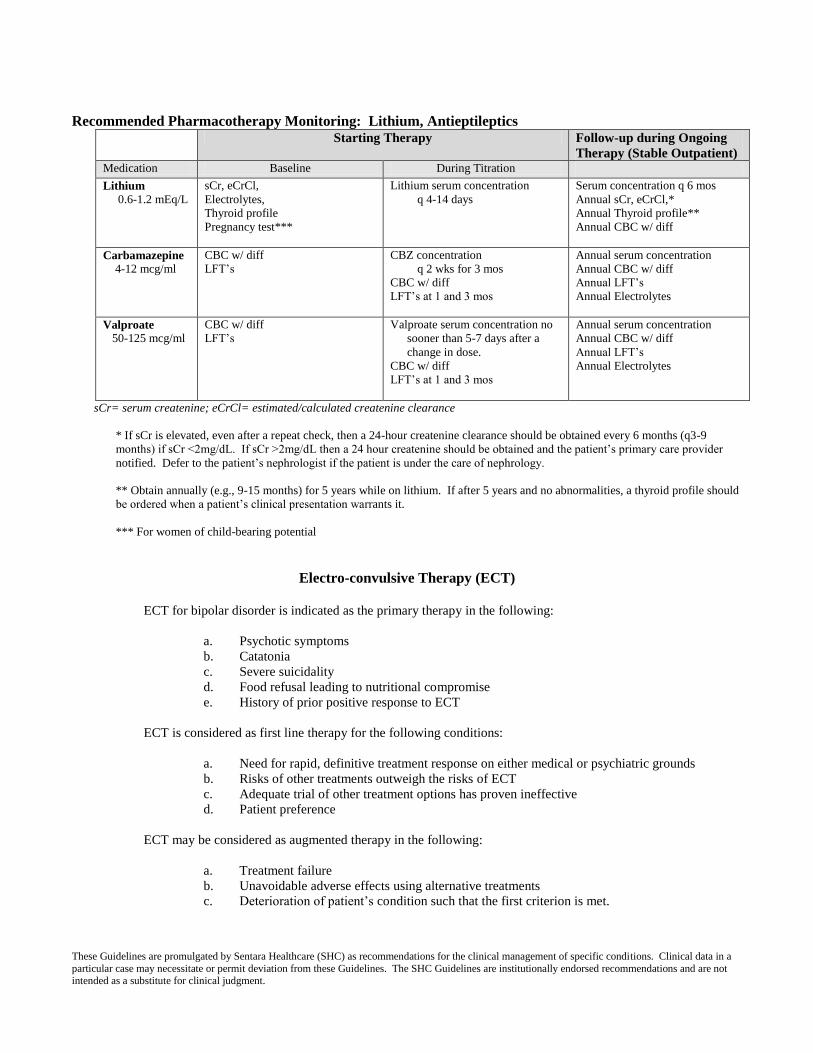
Recommended Pharmacotherapy Monitoring: Lithium, Antieptileptics
Starting Therapy Follow-up during Ongoing
Therapy (Stable Outpatient) Medication Baseline During Titration Lithium
0.6-1.2 mEq/L
sCr, eCrCl,
Electrolytes,
Thyroid profile
Pregnancy test***
Lithium serum concentration
q 4-14 days
Serum concentration q 6 mos
Annual sCr, eCrCl,*
Annual Thyroid profile**
Annual CBC w/ diff
Carbamazepine
4-12 mcg/ml
CBC w/ diff
LFT’s
CBZ concentration
q 2 wks for 3 mos
CBC w/ diff
LFT’s at 1 and 3 mos
Annual serum concentration
Annual CBC w/ diff
Annual LFT’s
Annual Electrolytes
Valproate
50-125 mcg/ml
CBC w/ diff
LFT’s
Valproate serum concentration no
sooner than 5-7 days after a
change in dose.
CBC w/ diff
LFT’s at 1 and 3 mos
Annual serum concentration
Annual CBC w/ diff
Annual LFT’s
Annual Electrolytes
sCr= serum createnine; eCrCl= estimated/calculated createnine clearance
* If sCr is elevated, even after a repeat check, then a 24-hour createnine clearance should be obtained every 6 months (q3-9
months) if sCr <2mg/dL. If sCr >2mg/dL then a 24 hour createnine should be obtained and the patient’s primary care provider
notified. Defer to the patient’s nephrologist if the patient is under the care of nephrology.
** Obtain annually (e.g., 9-15 months) for 5 years while on lithium. If after 5 years and no abnormalities, a thyroid profile should
be ordered when a patient’s clinical presentation warrants it.
*** For women of child-bearing potential
Electro-convulsive Therapy (ECT)
ECT for bipolar disorder is indicated as the primary therapy in the following:
a. Psychotic symptoms
b. Catatonia
c. Severe suicidality
d. Food refusal leading to nutritional compromise
e. History of prior positive response to ECT
ECT is considered as first line therapy for the following conditions:
a. Need for rapid, definitive treatment response on either medical or psychiatric grounds
b. Risks of other treatments outweigh the risks of ECT
c. Adequate trial of other treatment options has proven ineffective
d. Patient preference
ECT may be considered as augmented therapy in the following:
a. Treatment failure
b. Unavoidable adverse effects using alternative treatments
c. Deterioration of patient’s condition such that the first criterion is met.
VA/DoD Clinical PracTice Guideline forManagement of Persons with Bipolar Disorder
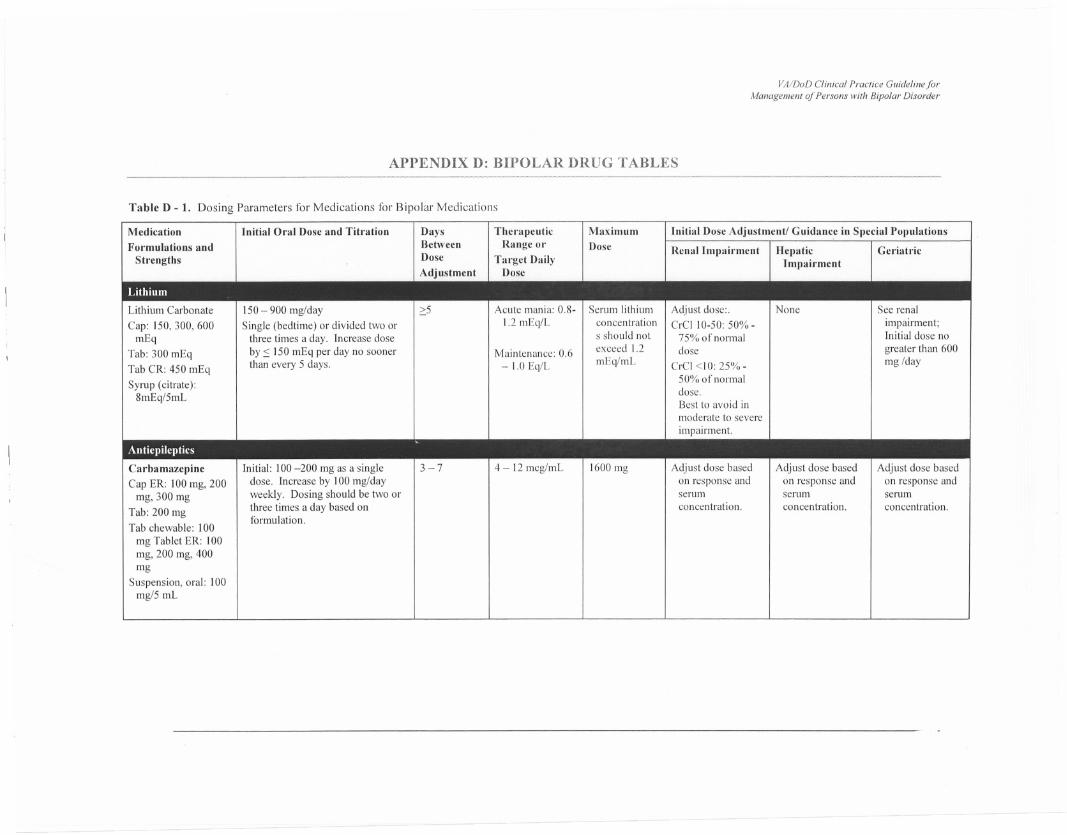
APPENDIX D: BIPOLAR DRUG TABLES-~~-"-~--""--""-"""'-"'---"-'~' _m",_,_,
Table D - 1. Dosing Parameters for Medications for Bipolar Medications
Lithium Carbonate
Cap: 150, 300, 600mEq
Tab: 300 mEq
Tab CR: 450 mEq
Syrup (citrate):8mEq/5mL
150 - 900 mg/day
Single (bedtime) or divided two orthree times a day. Increase doseby:so 150 mEq per day no soonerthan every 5 days.
;::5 Acute mania: 0.8-
1.2 mEq/L
Maintenance: 0.6
- 1.0Eq/L
Serum lithiumconcentrations should notexceed 1.2mEq/mL
Adjust dose:.CrClI0-50: 50%-
75% of normaldose
CrCI <10: 25%-50% of normaldose.Best to avoid inmoderate to severe
impairment.
None See renal
impairment;Initial dose no
greater than 600mg /day
-'---- - - - - - --
Medication Initial Oral Dose and Titration Days The,"apeutic Maximum Initial Dose Adjustment/ Guidanc,e in Special PopulationsFormulations and Between Range or Dose Renal Impairment Hepatic Geriatric
Strengths Dose Tm"get Daily ImpairmentAdjustment Dose
Lithium
.Anticpilcptics
Carbamazepine Initial: 100 -200 mg as a single 3-7 4 - 12 mcg/mL 1600 mg Adjust dose based Adjust dose based Adjust dose based
Cap ER: 100 mg, 200 dose. Increase by 100 mg/day on response and on response and on response and
mg, 300 mg weekly. Dosing should be two or serum serum serum
Tab: 200 mg three times a day based on concentration. concentration. concentration.
Tab chewable: 100formulation.
mg Tablet ER: 100mg, 200 mg, 400mg
Suspension, oral: 100mg/5 mL
VA/DaD Clinical Practice GuidelineforManagement of Persons with Bipolar Disorder
Medication Initial Oml Dose and Titration Days Therapeutic Maximum Initial Dose Adjustmentl Guidance in Special PopulationsFormulations and Between Range or Dose
Renal Impairment Hepatic GeriatricStrengths Dose Target Daily Impairment
Adjustment Dose
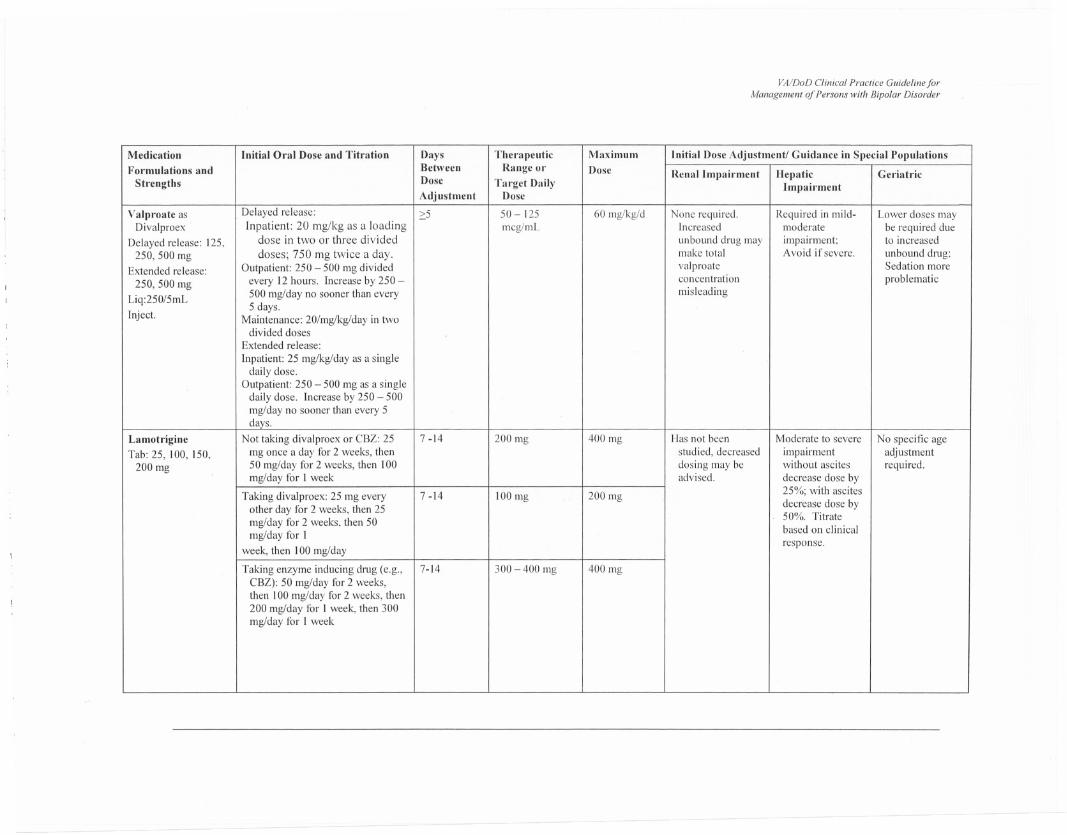
Valproate as Delayed release: 5 50 - 125 60 mg/kg/d None required. Required in mild- Lower doses mayDivalproex Inpatient: 20 mg/kg as a loading mcg/mL Increased moderate be required due
Delayed release: 125. dose in two or three divided unbound drug may impairment; to increased
250, 500 mg doses; 750 mg twice a day. make total Avoid if severe. unbound drug;
Extended release: Outpatient: 250 - 500 mg divided valproate Sedation more
250, 500 mg every 12 hours. Increase by 250 - concentration problematic
Liq:250/5mL 500 mg/day no sooner than every misleading
5 days.Inject. Maintenance: 20/mg/kg/day in two
divided dosesExtended release:
Inpatient: 25 mg/kg/day as a singledaily dose.
Outpatient: 250 - 500 mg as a singledaily dose. Increase by 250 - 500mg/day no sooner than every 5days.
Lamotrigine Not taking divalproex or CBZ: 25 7 -14 200 mg 400 mg Has not been Moderate to severe No specific ageTab: 25, 100, 150, mg once a day for 2 weeks, then studied, decreased impairment adjustment
200 mg 50 mg/day for 2 weeks, then 100 dosing may be without ascites required.mg/day for I week advised. decrease dose by
Taking divalproex: 25 mg every 7 -14 100 mg 200 mg 25%; with ascites
other day tor 2 weeks, then 25 decrease dose by
mg/day tor 2 weeks, then 5050%. Titrate
mg/day tor Ibased on clinical
week, then 100 mg/dayresponse.
Taking enzyme inducing drug (e.g., 7-14 300 - 400 mg 400 mgCBZ): 50 mg/day tor 2 weeks,then 100 mg/day for 2 weeks, then200 mg/day tor I week, then 300mg/day tor I week
VA/DaD Clinical Practice GliidelinejorManagement of Persons with Bipolar Disorder
Medication Initial Oml Dose and Titration Days
I Therapeutic I Maximum
Initial Dose Adjustment/ Guidance in Special PopulationsFormulations and Between Range or Dose Renal Impairment
Strengths Do'" .- ..
A(
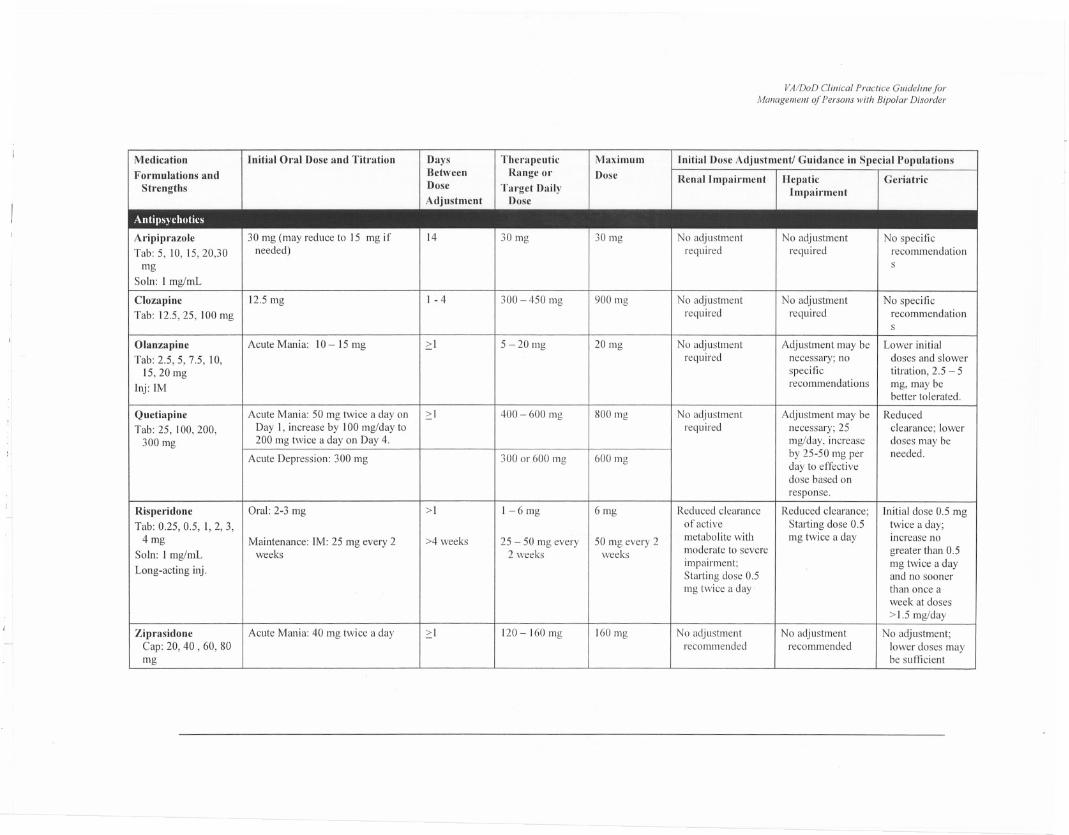
Aripiprazole
130 mg 130mg I No adjustment 1 No adjustment I No specificTab: 5, 10, 15,20,30 required required
:ecommendationmg
Soln: I mg/mL
Clozapine 112.5 mg
1- 4 300 - 450 mg 900 mg No adjustment No adjustment No specificTab: 12.5,25, 100 mg required required recommendation
s
Olanzapine Acute Mania: 10 - 15 mg 2:1 5 - 20 mg 20 mg No adjustment Adjustment may be Lower initial
Tab: 2.5,5,7.5,10, required necessary; no doses and slower
15,20 mg specific titration, 2.5 - 5
Inj: 1Mrecommendations mg, may be
better tolerated.
Quetiapine
I Acute Mania: 50 mg twice a day on
2:1 400 - 600 mg 800 mg No adjustment Adjustment may be Reduced
Tab: 25, 100, 200, Day I, increase by 100 mg/day to required necessary; 25 clearance; lower
300 mg 200 mg twice a day on Day 4. mg/day. increase doses may be
Acute Depression: 300 mg 300 or 600 mg 600 mg by 25-50 mg per needed.
day to effectivedose based on
response.
Risperidone Oral: 2-3 mg >1 1-6mg 6mg Reduced clearance Reduced clearance; Initial dose 0.5 mgTab: 0.25, 0.5, 1, 2, 3, of active Starting dose 0.5 twice a day;
4mg Maintenance: 1M: 25 mg every 2 >4 weeks 25 - 50 mg every 50 mg every 2metabolite with mg twice a day increase no
SoIn: 1mg/mL weeks 2 weeks weeks moderate to severe greater than 0.5
Long-acting inj.impairment; mg twice a dayStarting dose 0.5 and no soonermg twice a day than once a
week at doses
> 1.5 mg/day
Ziprasidone
1 Acute Mania: 40 mg twice a day
2:1 120- 160mg 160 mg No adjustment No adjustment No adjustment;Cap: 20, 40 , 60, 80 recommended recommended lower doses maymg be sunicient
VA/DoD Clinical Practice GuidelineforManagement of Persons with Bipolar Disorder
Medication Initial Oral Dose and Tih"ation Days Therapeutic Maximum Initial Dose Adjustment/ Guidance in Special PopulationsFormulations and Between Range or Dose
Renal Impairment Heplltic GeriatricStrengths Dose Tm"get Daily Impairment
Adjustment Dose
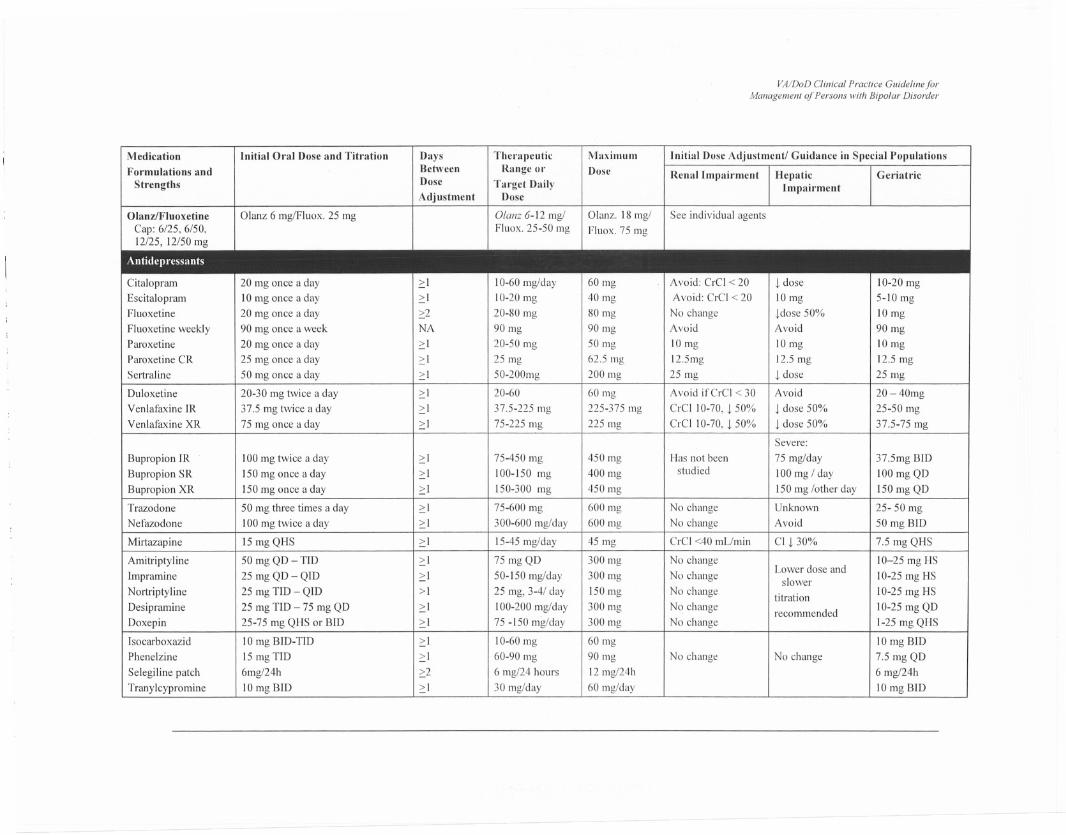
OlanziFluoxetine Glanz6 mg/Fluox.25 mg Glanz 6-12 mg/ Glanz. 18 mg/ See individual agentsCap: 6/25,6/50, Fluox. 25-50 mg Fluox. 75 mg12/25, 12/50 mg
Antidepressants
Citalopram 20 mg once a day ;::1 10-60 mg/day 60 mg Avoid: CrCI < 20 t dose 10-20 mg
Escitalopram 10 mg once a day ;::1 10-20 mg 40 mg Avoid: CrCI < 20 10mg 5-10 mgFluoxetine 20 mg once a day ;::2 20-80 mg 80 mg No change tdose 50% 10mg
Fluoxetine weekly 90 mg once a week NA 90 mg 90 mg Avoid Avoid 90 mgParoxetine 20 mg once a day ;::1 20-50 mg 50 mg 10mg IOmg 10mgParoxetine CR 25 mg once a day ;::1 25 mg 62.5 mg l2.5mg 12.5 mg 12.5 mgSertraline 50 mg once a day 2:1 50-200mg 200 mg 25 mg t dose 25 mg
Duloxetine 20-30 mg twice a day ;::1 20-60 60 mg Avoid ifCrCl < 30 Avoid 20 - 40mgVenlafaxine IR 37.5 mg twice a day ;::1 37.5-225 mg 225-375 mg CrCIIO-70, t 50% t dose 50% 25-50 mgVenlafaxine XR 75 mg once a day ;::1 75-225 mg 225 mg CrCI 10-70, t 50% t dose 50% 37.5-75 mg
Severe:
Bupropion IR 100 mg twice a day ;::1 75-450 mg 450 mg Has not been 75 mg/day 37.5mg BID
Bupropion SR 150 mg once a day 2:1 100-150 mg 400 mg studied 100 mg / day 100 mg QD
Bupropion XR ISO mg once a day ;::1 150-300 mg 450 mg 150 mg /other day 150 mg QD
Trazodone 50 mg three times a day 2:1 75-600 mg 600 mg No change Unknown 25- 50 mgNefazodone 100 mg twice a day ;::1 300-600 mg/day 600 mg No change Avoid 50 mg BID
Mirtazapine 15 mg QHS 2:1 15-45 mg/day 45 mg CrCI <40 mL/min CI t 30% 7.5 mg QHS
Amitriptyline 50 mg QD- TID ;::1 75 mg QD 300 mg No changeLower dose and
10-25 mg HS
Impramine 25 mg QD - QID 2:1 50-150 mg/day 300 mg No change slower 10-25 mg HS
Nortriptyline 25 mg TID - QID >1 25 mg, 3-4/ day ISO mg No change titration 10-25 mg HS
Desipramine 25 mgTID-75 mgQD ;::1 100-200 mg/day 300 mg No change recommended 10-25 mg QD
Doxepin 25-75 mg QHS or BID ;::1 75 -ISO mg/day 300 mg No change 1-25 mg QHS
Isocarboxazid 10 mg BID-TID ;::1 10-60 mg 60 mg 10 mg BIDPhenelzine ]5 mg TID 2:1 60-90 mg 90 mg No change No change 7.5 mg QD
Selegiline patch 6mg/24h ;::2 6 mg/24 hours 12 mg/24h 6 mg/24h
Tranylcypromine 10 mg BID ;::] 30 mg/day 60 mg/day 10 mg BID
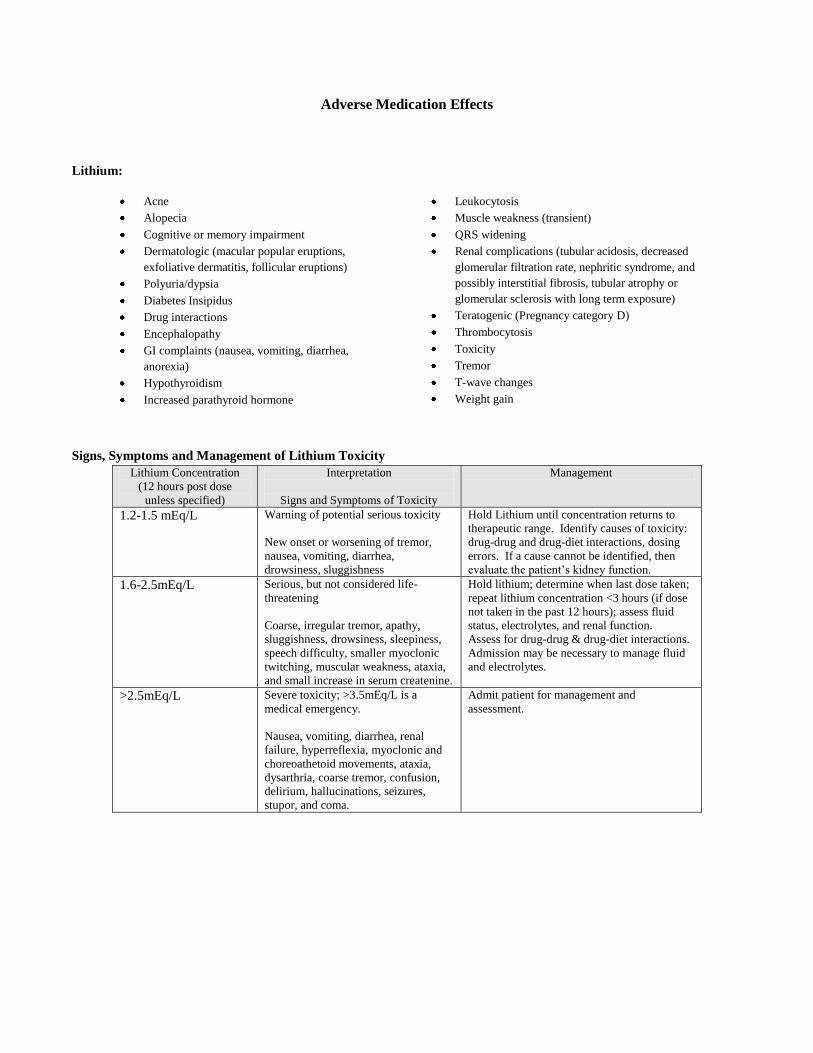
Adverse Medication Effects
Lithium:
Acne
Alopecia
Cognitive or memory impairment
Dermatologic (macular popular eruptions,
exfoliative dermatitis, follicular eruptions)
Polyuria/dypsia
Diabetes Insipidus
Drug interactions
Encephalopathy
GI complaints (nausea, vomiting, diarrhea,
anorexia)
Hypothyroidism
Increased parathyroid hormone
Leukocytosis
Muscle weakness (transient)
QRS widening
Renal complications (tubular acidosis, decreased
glomerular filtration rate, nephritic syndrome, and
possibly interstitial fibrosis, tubular atrophy or
glomerular sclerosis with long term exposure)
Teratogenic (Pregnancy category D)
Thrombocytosis
Toxicity
Tremor
T-wave changes
Weight gain
Signs, Symptoms and Management of Lithium Toxicity
Lithium Concentration
(12 hours post dose
unless specified)
Interpretation
Signs and Symptoms of Toxicity
Management
1.2-1.5 mEq/L Warning of potential serious toxicity
New onset or worsening of tremor,
nausea, vomiting, diarrhea,
drowsiness, sluggishness
Hold Lithium until concentration returns to
therapeutic range. Identify causes of toxicity:
drug-drug and drug-diet interactions, dosing
errors. If a cause cannot be identified, then
evaluate the patient’s kidney function.
1.6-2.5mEq/L Serious, but not considered life-
threatening
Coarse, irregular tremor, apathy,
sluggishness, drowsiness, sleepiness,
speech difficulty, smaller myoclonic
twitching, muscular weakness, ataxia,
and small increase in serum createnine.
Hold lithium; determine when last dose taken;
repeat lithium concentration <3 hours (if dose
not taken in the past 12 hours); assess fluid
status, electrolytes, and renal function.
Assess for drug-drug & drug-diet interactions.
Admission may be necessary to manage fluid
and electrolytes.
>2.5mEq/L Severe toxicity; >3.5mEq/L is a
medical emergency.
Nausea, vomiting, diarrhea, renal
failure, hyperreflexia, myoclonic and
choreoathetoid movements, ataxia,
dysarthria, coarse tremor, confusion,
delirium, hallucinations, seizures,
stupor, and coma.
Admit patient for management and
assessment.
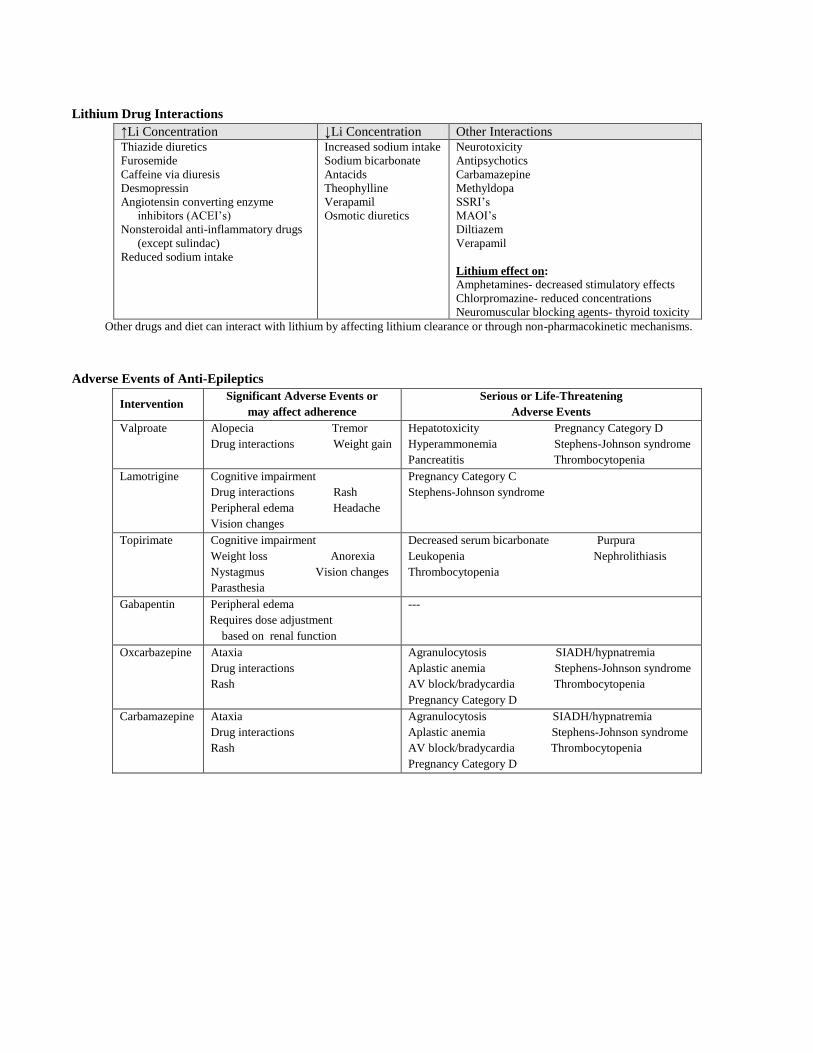
Lithium Drug Interactions
↑Li Concentration ↓Li Concentration Other Interactions Thiazide diuretics
Furosemide
Caffeine via diuresis
Desmopressin
Angiotensin converting enzyme
inhibitors (ACEI’s)
Nonsteroidal anti-inflammatory drugs
(except sulindac)
Reduced sodium intake
Increased sodium intake
Sodium bicarbonate
Antacids
Theophylline
Verapamil
Osmotic diuretics
Neurotoxicity
Antipsychotics
Carbamazepine
Methyldopa
SSRI’s
MAOI’s
Diltiazem
Verapamil
Lithium effect on:
Amphetamines- decreased stimulatory effects
Chlorpromazine- reduced concentrations
Neuromuscular blocking agents- thyroid toxicity
Other drugs and diet can interact with lithium by affecting lithium clearance or through non-pharmacokinetic mechanisms.
Adverse Events of Anti-Epileptics
Intervention Significant Adverse Events or
may affect adherence
Serious or Life-Threatening
Adverse Events
Valproate Alopecia Tremor
Drug interactions Weight gain
Hepatotoxicity Pregnancy Category D
Hyperammonemia Stephens-Johnson syndrome
Pancreatitis Thrombocytopenia
Lamotrigine Cognitive impairment
Drug interactions Rash
Peripheral edema Headache
Vision changes
Pregnancy Category C
Stephens-Johnson syndrome
Topirimate Cognitive impairment
Weight loss Anorexia
Nystagmus Vision changes
Parasthesia
Decreased serum bicarbonate Purpura
Leukopenia Nephrolithiasis
Thrombocytopenia
Gabapentin Peripheral edema
Requires dose adjustment
based on renal function
---
Oxcarbazepine Ataxia
Drug interactions
Rash
Agranulocytosis SIADH/hypnatremia
Aplastic anemia Stephens-Johnson syndrome
AV block/bradycardia Thrombocytopenia
Pregnancy Category D
Carbamazepine Ataxia
Drug interactions
Rash
Agranulocytosis SIADH/hypnatremia
Aplastic anemia Stephens-Johnson syndrome
AV block/bradycardia Thrombocytopenia
Pregnancy Category D
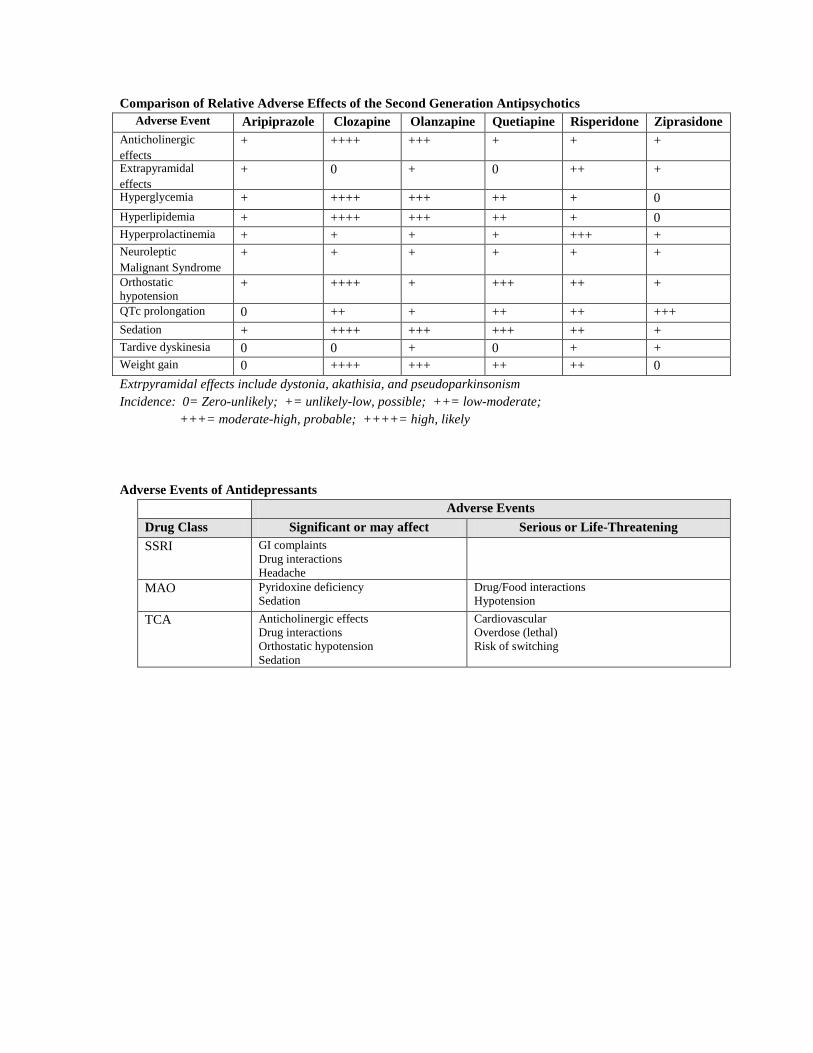
Comparison of Relative Adverse Effects of the Second Generation Antipsychotics
Adverse Event Aripiprazole Clozapine Olanzapine Quetiapine Risperidone Ziprasidone
Anticholinergic
effects
+ ++++ +++ + + +
Extrapyramidal
effects
+ 0 + 0 ++ +
Hyperglycemia + ++++ +++ ++ + 0
Hyperlipidemia + ++++ +++ ++ + 0
Hyperprolactinemia + + + + +++ +
Neuroleptic
Malignant Syndrome
+ + + + + +
Orthostatic
hypotension + ++++ + +++ ++ +
QTc prolongation 0 ++ + ++ ++ +++
Sedation + ++++ +++ +++ ++ +
Tardive dyskinesia 0 0 + 0 + +
Weight gain 0 ++++ +++ ++ ++ 0
Extrpyramidal effects include dystonia, akathisia, and pseudoparkinsonism
Incidence: 0= Zero-unlikely; += unlikely-low, possible; ++= low-moderate;
+++= moderate-high, probable; ++++= high, likely
Adverse Events of Antidepressants
Adverse Events
Drug Class Significant or may affect
adherence
Serious or Life-Threatening
SSRI GI complaints
Drug interactions
Headache
MAO Pyridoxine deficiency
Sedation
Drug/Food interactions
Hypotension
TCA Anticholinergic effects
Drug interactions
Orthostatic hypotension
Sedation
Cardiovascular
Overdose (lethal)
Risk of switching

These Guidelines are promulgated by Sentara Healthcare (SHC) as recommendations for the clinical management of specific conditions. Clinical data in a particular case may necessitate or permit deviation from these Guidelines. The SHC Guidelines are
institutionally endorsed recommendations and are not intended as a substitute for clinical judgment.
Reference
Adapted from VA/DoD Evidence Based Practice Clinical Practice Guideline on Management of
Bipolar Disorder in Adults, May 2010. http://www.healthquality.va.gov/bipolar/bd_306_sum.pdf
Accessed 1/2/13.
Resources for Patients/Families
Depression and Bipolar Support Alliance
http://www.dbsalliance.org
Mental Health America
http://www.mentalhealthamerica.net
National Institute of Mental Health
http://www.nimh.nih.gov
National Mental Health Information
Center http://mentalhealth.gov/