Embed Size (px)
Citation preview

Malnutrition
Malnutrition is the condition that occurs when your body does not get enough nutrients.
Causes
There are a number of causes of malnutrition. It may result from:
Inadequate or unbalanced diet
Problems with digestion or absorption
Certain medical conditions
Malnutrition can occur if you do not eat enough food. Starvation is a form of malnutrition. You may
develop malnutrition if you lack of a single vitamin in the diet. In some cases, malnutrition is very mild and causes
no symptoms. However, sometimes it can be so severe that the damage done to the body is permanent, even
though you survive. Malnutrition continues to be a significant problem all over the world, especially among
children. Poverty, natural disasters, political problems, and war all contribute to conditions -- even epidemics -- of
malnutrition and starvation, and not just in developing countries.
Symptoms
Symptoms vary and depend on what is causing the malnutrition. However, some general symptoms
include fatigue, dizziness, and weight loss.
Treatment
Treatment usually consists of replacing missing nutrients, treating symptoms as needed, and treating
any underlying medical condition.
Outlook (Prognosis)
The outlook depends on the cause of the malnutrition. Most nutritional deficiencies can be corrected.
However, if malnutrition is caused by a medical condition, that illness has to be treated in order to reverse the
nutritional deficiency.
Possible Complications
If untreated, malnutrition can lead to mental or physical disability, illness, and possibly death. Treatment
is necessary if you or your child have any changes in the body's ability to function. Contact your health care
provider if the following symptoms develop:
Fainting
Lack of menstruation
Lack of growth in children
Rapid hair loss
Kwashiorkor

Kwashiorkor is a form of severe protein-energy malnutrition characterized by edema,
irritability, anorexia, ulcerating dermatoses, and an enlarged liver with fatty infiltrates. Sufficient calorie intake, but
with insufficient protein consumption, distinguishes it from marasmus. Kwashiorkor cases occur in areas of
famine or poor food supply. Cases in the developed world are rare.
Jamaican pediatrician Cicely Williams introduced the name into the medical community in her
1935 Lancet article. The name is derived from the Ga language of coastal Ghana, translated as "the sickness the
baby gets when the new baby comes", and reflecting the development of the condition in an older child who has
been weaned from the breast when a younger sibling comes. Breast milk contains proteins and amino acidsvital
to a child's growth. In at-risk populations, kwashiorkor may develop after a mother weans her child from breast
milk, replacing it with a diet high incarbohydrates, especially starches, but deficient in protein.
Signs and symptoms
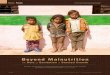
Child in the with symptoms of Kwashiorkor Typical ulcerating dermatosis seen on a Malawian child with kwashiorkor
One of many kwashiorkor cases in relief camps during the Nigerian–Biafran War
Kwashiorkor is preventable, categorized by ICD-9 as disease category 260, other severe protein-calorie
malnutrition. The defining sign of kwashiorkor in a malnourished child is pedal edema (swelling of the ankles and
feet). Other signs include a distended abdomen, an enlarged liver with fatty infiltrates, thinning hair, loss of teeth,

skin depigmentation and dermatitis. Children with kwashiorkor often develop irritability and anorexia. Victims of
kwashiorkor fail to produce antibodies following vaccination against diseases,
including diphtheria and typhoid. Generally, the disease can be treated by adding protein to the diet; however, it
can have a long-term impact on a child's physical and mental development, and in severe cases may lead to
death.
In dry climates, marasmus is the more frequent disease associated with malnutrition. Another
malnutrition syndrome includes cachexia, although it is often caused by underlying illnesses. These are important
considerations in the treatment of the patients.
Causes
Kwashiorkor is a severe form of malnutrition, caused by a deficiency in dietary protein. The extreme lack
of protein causes an osmotic imbalance in the gastro-intestinal system causing swelling of the gut diagnosed as
an edema or retention of water. Extreme fluid retention observed in individuals suffering from kwashiorkor is a
direct result of irregularities of the lymphatic system and capillary exchange. The lymphatic system serves three
major purposes: fluid recovery, immunity, and lipid absorption. Victims of kwashiorkor commonly exhibit a
reduced ability to recover fluids, immune system failure, and low lipid absorption, all of which result from severe
undernourishment. Fluid recovery in the lymphatic system is accomplished by re-absorption of water and proteins
which are returned to the blood. Compromised fluid recovery results in the characteristic belly distension
observed in highly malnourished children.
Capillary exchange between the lymphatic system and the bloodstream is stunted due to the inability of
the body to effectively overcome the hydrostatic pressure gradient. Proteins, mainly albumin, are responsible for
creating the colloid osmotic pressure (COP) observed in the blood and tissue fluids. The difference in the COP of
the blood and tissue is called the oncotic pressure. The oncotic pressure is in direct opposition with the
hydrostatic pressure and tends to draw water back into the capillary by osmosis. However, due to the lack of
proteins, no substantial pressure gradient can be established to draw fluids from the tissue back into the blood
stream. This results in the pooling of fluids, causing the swelling and distention of the abdomen.
The low protein intake leads to some specific signs: edema of the hands and feet, irritability, anorexia, a
desquamative rash, hair discolouration, and a large fatty liver. The typical swollen abdomen is due to two causes:
ascites because of hypoalbuminemia (low oncotic pressure), and enlarged fatty liver.
Ignorance of nutrition can be a cause. Latham, director of the Program in International Nutrition at Cornell
University, along with Keith Rosenberg cited a case where parents who fed their child cassava failed to recognize
malnutrition because of the edema caused by the syndrome and insisted the child was well-nourished despite the
lack of dietary protein.
Protein should be supplied only for anabolic purposes. The catabolic needs should be satisfied
with carbohydrateand fat. Protein catabolism involves the urea cycle, which is located in the liver and can easily
overwhelm the capacity of an already damaged organ. The resulting liver failure can be fatal. This means in
patients suffering from kwashiorkor, protein must be introduced back into the diet gradually. Clinical solutions
include weaning the affected with milk products and increasing the intake of proteinaceous material to daily
recommended amounts.
Marasmus

Marasmus is a form of severe malnutrition characterized by energy deficiency. A child with
marasmus looks emaciated. Body weight is reduced to less than 60% of the normal (expected) body weight
for the age.[1] Marasmus occurrence increases prior to age 1, whereas kwashiorkor occurrence increases
after 18 months. It can be distinguished from kwashiorkor in that kwashiorkor is protein deficiency with
adequate energy intake whereas marasmus is inadequate energy intake in all forms, including protein.
Protein wasting in kwashiorkor may lead to edema.
The prognosis is better than it is for kwashiorkor but half of severely malnourished children die due
to unavailability of adequate treatment. The word “marasmus” comes from the Greek
μαρασμός marasmos ("decay").
Signs and symptoms
The malnutrition associated with marasmus leads to extensive tissue and muscle wasting, as well
as variable edema. Other common characteristics include dry skin, loose skin folds hanging over the
buttocks (glutei) and armpit (axillae), etc. There is also drastic loss of adipose tissue (body fat) from normal
areas of fat deposits like buttocks and thighs. The afflicted are often fretful, irritable, and voraciously
hungry.
Causes
Marasmus is caused by a severe deficiency of nearly all nutrients, especially protein and carbohydrates.
Treatment

It is necessary to treat not only the causes but also the complications of the disorder,
including infections, dehydration, and circulation disorders, which are frequently lethal and lead to high
mortality if ignored. Ultimately, marasmus can progress to the point of no return when the body's ability
for protein synthesis is lost. At this point, attempts to correct the disorder by giving food or protein are futile.
Cachexia
Cachexia (/ k ə ̍ k ɛ k s i ə / ; from Greek κακός kakos "bad" and ἕξις hexis "condition")[1] or wasting
syndrome is loss of weight, muscle atrophy, fatigue, weakness, and significant loss of appetite in someone
who is not actively trying to lose weight. The formal definition of cachexia is the loss of body mass that
cannot be reversed nutritionally: Even if the affected patient eats more calories, lean body mass will be lost,
indicating a primary pathology is in place.
Cachexia is seen in patients with cancer, AIDS,[2] chronic obstructive lung disease, multiple
sclerosis, congestive heart failure, tuberculosis, familial amyloid polyneuropathy, mercury
poisoning (acrodynia) and hormonal deficiency. It is a positive risk factor for death, meaning if the patient
has cachexia, the chance of death from the underlying condition is increased dramatically. It can be
a sign of various underlying disorders; when a patient presents with cachexia, a doctor will generally
consider the possibility of cancer, metabolic acidosis (from decreased protein synthesis and increased
protein catabolism), certaininfectious diseases (e.g., tuberculosis, AIDS), chronic pancreatitis, and
some autoimmune disorders, or addiction to amphetamine. Cachexia physically weakens patients to a
state of immobility stemming from loss of appetite, asthenia, and anemia, and response to standard
treatment is usually poor. Cachexia includes sarcopenia as a part of its pathology.
Disease settings
Cachexia is often seen in end-stage cancer, and in that context is called cancer cachexia. Patients
with congestive heart failure can have a cachectic syndrome. Also, a cachexia comorbidity is seen in
patients who have any of the range of illnesses classified as chronic obstructive pulmonary disease.[5] Cachexia is also associated with advanced stages of chronic kidney disease, cystic fibrosis, multiple
sclerosis, motor neuron disease, Parkinson's disease, dementia, HIV/AIDS and other progressive illnesses.
Mechanism
The exact mechanism in which these diseases cause cachexia is poorly understood, but there is
probably a role for inflammatory cytokines, such as tumor necrosis factor-alpha (which is also nicknamed
'cachexin' or 'cachectin'), interferon gamma and interleukin 6, as well as the tumor-secreted proteolysis-
inducing factor.
Related malnutrition syndromes are kwashiorkor and marasmus, although these do not always have an
underlying causative illness; they are most often symptomatic of severe malnutrition. Those suffering from
the eating disorder anorexia nervosa appear to have high plasma levels of ghrelin. Ghrelin levels are also
high in patients who have cancer-induced cachexia.

Management
The treatment or management of cachexia depends on the underlying causes, the general
prognosis and other person related factors. Reversible causes, underlying diseases and contributing
factors are treated if possible and acceptable. Non-drug therapies which have been shown to be effective
in cancer induced cachexia include nutritional counselling, psychotherapeutic interventions, and physical
training.
Currently, no widely accepted drugs to treat cachexia and no FDA-approved drugs to treat cancer
cachexia are available. Treatment involving different combinations for cancer cachexia is recommended in
Europe, as a combination of nutrition, medication and non-drug-treatment may be more effective than
monotherapy. Steroids may be beneficial in cancer cachexia but their use is recommended for maximal 2
weeks since a longer duration of treatment increases the burden from side effects. Progestins such
as megestrol are an option in refractory cachexia withanorexia as a major symptom. Other drugs that have
been used or are being investigated in cachexia therapy, but which lack conclusive evidence of efficacy or
safety, and are not generally recommended include:
Thalidomide and cytokine antagonists
Cannabinoids
Omega-3 fatty acids, including eicosapentaenoic acid (EPA)
Non-steroidal anti-inflammatory drugs
Prokinetics
Ghrelin and ghrelin receptor agonist
Anabolic catabolic transforming agents such as MT-102
Selective androgen receptor modulators
Cyproheptadine
Hydrazine
Medical marijuana has been allowed for the treatment of cachexia in some US states, such as
Delaware, Nevada, Michigan, Washington, Oregon, California, Colorado, New Mexico, Arizona, Vermont,
New Jersey, Rhode Island and Connecticut. There is insufficient evidence to support the use of oral fish oil
for the management of cachexia associated with advanced cancer.
Prevalence
According to the 2007 AHRQ National Inpatient sample, in a projected 129,164 hospital
encounters in the United States, cachexia was listed as at least one of up to 14 listed diagnosis codes,
based on a sample of 26,325 unweighted encounters. The CDC National Ambulatory Medical Care Survey,
a sample of US outpatient visits listed no visits where cachexia was listed as one of up to three recorded
diagnoses treated during the visit, out of a sample of 32,778 unweighted visits.
Cancer cachexia

About 50% of all cancer patients suffer from cachexia. Those with upper gastrointestinal and
pancreatic cancers have the highest frequency of developing a cachexic symptom. This figure rises to 80%
in terminal cancer patients.[17] In addition to increasing morbidity and mortality, aggravating the side effects
of chemotherapy, and reducing quality of life, cachexia is considered the immediate cause of death of a
large proportion of cancer patients, ranging from 22% to 40% of the patients.
Symptoms of cancer cachexia include progressive weight loss and depletion of host reserves of
adipose tissue and skeletal muscle. Cachexia should be suspected if involuntary weight loss of greater
than 5% of premorbid weight occurs within a six-month period. Traditional treatment approaches, such as
appetite stimulants, 5-HT3 antagonists, nutrient supplementation, and COX-2 inhibitor, have failed to
demonstrate success in reversing the metabolic abnormalities seen in cancer cachexia.
Pathogenesis
Much research is currently focused on determining the mechanism of the development of
cachexia. The two main theories of the development of cancer cachexia are:
Alteration of control loop: High levels of leptin, a hormone secreted by adipocytes, block the release of
neuropeptide (NPY), which is the most potent feeding-stimulatory peptide in
thehypothalamic orexigenic network, leading to decreased energy intake, but high metabolic demand
for nutrients.
Cachectic syndrome maintained by tumor-derived factors: Factors, such as lipid mobilizing factor
extracted from the urine of cachectic patients, were suspected to induce protein degradation in skeletal
muscle by upregulation of the ubiquitin-proteasome pathway and lipolysis in adipocytes. However, how
they interact and whether they come into play at the beginning or at the end stage of the disease is
uncertain .
Although the pathogenesis of cancer cachexia is poorly understood, multiple biologic pathways are
known to be involved, including proinflammatory cytokines such as TNF-alpha, neuroendocrine
hormones, IGF-1, and tumor-specific factors such as proteolysis-inducing factor.
The inflammatory cytokines involved in wasting diseases are interleukin 6, TNF-alpha, IL1B,
and interferon-gamma. Although many different tissues and cell types may be responsible for the increase
in circulating cytokines during some types of cancer, evidence indicates the tumors are an important
source. Cytokines by themselves are capable of inducing weight loss. TNF-alpha has been shown to have
direct catabolic effect on skeletal muscle and adipose tissue and produces muscle atrophy through the
ubiquitin–proteasome proteolytic pathway. The mechanism involves the formation of reactive oxygen
species leading to upregulation of the transcription factor NF-κB. NF-κB is a known regulator of the genes
that encode cytokines, and cytokine receptors. The increased production of cytokines induces proteolysis
and breakdown of myofibrillar proteins.
Treatments
Only limited treatment options exist for patients with clinical cancer cachexia. Current strategy is to
improve appetite by using appetite stimulants to ensure adequate intake of nutrients. Pharmacological
interventions with appetite stimulants, nutrient supplementation, 5-HT3 antagonists and Cox-2 inhibitor have
been used to treat cancer cachexia, but with limited effect.
Recent studies using a more calorie-dense (1.5 kcals/ml) and higher protein supplementation have
suggested at least weight stabilization can be achieved, although improvements in lean body mass have
not been observed in these studies.
Therapeutic strategies have been based on either blocking cytokines synthesis or their
action. Thalidomide has been demonstrated to suppress TNF-alpha production in monocytes in vitro and to
normalize elevated TNF-alpha levels in vivo. A recent randomized, placebo-controlled trial in patients with
cancer cachexia showed the drug was well tolerated and effective at attenuating loss of weight and lean
body mass (LBM) in patients with advanced pancreatic cancer. An improvement in the LBM and improved
quality of life were also observed in a randomized, double-blind trial using a protein and energy-
dense, omega-3 fatty acids-enriched oral supplement, provided its consumption was equal or superior to
2.2 g of eicosapentaenoic acid per day. It is also through decreasing TNF-alpha production. However,
recent data arising from a large, multicenter, double-blind, placebo-controlled trial indicate EPA
administration alone is not successful in the treatment of weight loss in patients with advanced
gastrointestinal or lung cancer.
Peripheral muscle proteolysis, as it occurs in cancer cachexia, serves to mobilize amino acids
required for the synthesis of liver and tumor protein. Therefore, the administration of exogenous amino
acids may theoretically serve as a protein-sparing metabolic fuel by providing substrates for both muscle
metabolism and gluconeogenesis. Recent studies have demonstrated dietary supplementation with a
specific combination of high protein, leucine and fish oil improves muscle function and daily activity and the
immune response in cachectic tumor-bearing mice. In addition, β-hydroxy-β-methyl butirate derived from
leucine catabolism used as a supplement in tumor-bearing rats prevents cachexia by modifying NF-κB
expression.
A recent phase-2 study involving the administration of antioxidants, pharmaconutritional
support, progestogen (megestrol acetate and medroxyprogesterone acetate), and anticyclooxygenase-
2drugs, showed efficacy and safety in the treatment of patients with advanced cancer of different sites
suffering cachexia. These data reinforce the use of the multitargeted therapies (nutritional supplementation,
appetite stimulants, and physical activity regimen) in the treatment of cancer cachexia.
EMACIATIONEmaciation is defined as extreme weight loss and thinness due to a loss of subcutaneous fat (the fatty,
or adipose tissue beneath the skin) and muscle throughout the body. It affects human beings and animals, is
often described as "wasting", and is caused by severe malnourishment and starvation. Emaciation is a
predominant symptom of malnourishment, a basic component of poverty and famine that also occurs with
diseases that interfere with the digestive system and appetite, other systems, and eating disorders. These
include nutrient deficiency disorders, diseases with prolonged fever and
infection, malignant diseases, parasitic infections that can result from contamination, anorexia nervosa and other
conditions. The malnourishment associated with emaciation has been referred to as " inanition", while infection by
parasites has been described as "adulteration". Treatment of emaciation includes gradual renourishment with a
slow increase of daily caloric intake to help rebuild tissues and regain weight. Rest, and emotional and
psychological therapy and support may be included.
Characteristics

In humans, the overall physical appearance of emaciation includes a thinning of the limbs, upper body
and buttocks to an almost skeletal-looking state with an apparent absence of fat and muscle tone. The skin is
thin, dry and translucent in some areas of the body, to the point that veins beneath the skin are somewhat visible.
The face is thin and drawn with a hopeless, vacant and distressed demeanor; the eye sockets are sunken, giving
the eyes a bulging appearance. The scalp is bony with dry, withering hair that is lacking. On the torso, the collar
bone, chest bone and ribs are quite pronounced; the stomach is bloated, which indicates gastrointestinal distress
associated with nutritional depletion. The mouth and tongue may be excessively dry, or moist with the tongue
thickly coated; there is usually strong halitosis, or foul breath.
There is great fatigue, inability and lack of physical effort in the emaciated. Mental efficiency, problem
solving and reasoning are somewhat impaired. The emotional state of an emaciated individual is often poor;
feelings of depression, hopelessness, fear, anxiety and worthlessness may prevail. A person who is emaciated is
usually submissive, both mentally and physically, to the will of others. Behavior is generally passive.
The underlying starvation, malnourishment, and usually dehydration, associated with emaciation, affect
and are harmful to organ systems throughout the body. The emaciated individual experiences disturbances of the
blood, circulatory, and urinary systems;
theseinclude hyponatremia and/or hypokalemia (low sodium and/or potassium in the blood,
respectively), anemia (lowhemoglobin), improper function of lymph (immune system-related white blood matter)
and the lymphatic system, and pleurisy (fluid in the pleural cavity surrounding the lungs) and edema (swelling in
general) caused by poor or improper function of the kidneys to eliminate wastes from the blood.
Cause
In most of Africa, poverty, malnutrition and disease are common. Among third world countries, India is
one of the leading countries plagued by malnutrition, with more than 200 million people affected. Emaciation in
India is referred to as "shosha roga", which means "exploitative disease". Diseases such as these are nutrient
deficiency disorders that can cause varying degrees of emaciation based on the type of nutrient(s) chronically
and persistently lacking or absent from the diet of an individual. Famine and third world conditions are usually
involved. Severe emaciation can be caused by marasmus, a disorder that is seen in children that are deprived of
proteins, fats and carbohydrates. Both weight and growth are affected. A similar disorder, seen in very young
malnourished children, is kwashiorkor. With emaciation mostly confined to the upper body, kwashiorkor
oftentimes occurs after a child has been weaned and thus deprived of protein it was getting from its mother's
milk. Slight emaciation is seen with nutrition disorders such as beriberi, caused by a lack of thiamine (vitamin B1),
and pellagra, caused by insufficient intake of niacin (vitamin B3). The former is mainly characterized by mental
impairment, and the latter is more serious, often leading to death.
Other diseases and disorders associated with emaciation include malaria and cholera, tuberculosis and
other infectious diseases with prolonged fever, parasitic infections, many forms of cancerand
their treatments, lead poisoning, and eating disorders like anorexia nervosa.
Treatment
Other than treating, curing or remedying the underlying cause of emaciation, it as a symptom is treated
by regaining the weight and restoring the tissues. This is done through renourishment, or reintroducing
nourishing liquids and foods to the body while increasing the intake of food energy. The process, usually begun
in an individual deprived of food for a period of time, must be done slowly to avoid complications such
as regurgitation and vomiting. It begins with spoonsful of water and salted broth, advancing to increased amounts

of clear liquids including broth, tea and fruit juices. This soon is advanced to full liquids such as milk (if no lactose
intolerance is present) and cream-based soups. Once solid food is introduced, an emaciated individual is usually
given up to eight small meals per day, at two-hour intervals. Meals may consist of a small milkshake to minor
portions of meat with a starchy side item. For the purposes of weight gain and tissue rebuilding, the diet will be
focused on proteins, fats and carbohydrates that are rich in vitamins and minerals, and relatively high in energy.
Oily foods and high-fiber foods like grains and certain vegetables are discouraged because they are difficult to
digest, and filling while lower in energy. Treatment of emaciation also includes much sleep, rest and relaxation,
and counseling
Childhood obesity
Children with varying degrees of body fat
Childhood obesity is a condition where excess body fat negatively affects a child's health or
wellbeing. As methods to determine body fat directly are difficult, the diagnosis of obesity is often based
on BMI. Due to the rising prevalence of obesity in children and its many adverse health effects it is being
recognized as a serious public health concern. The term overweight rather than obese is often used in
children as it is less stigmatizing.
Classification of Childhood Obesity

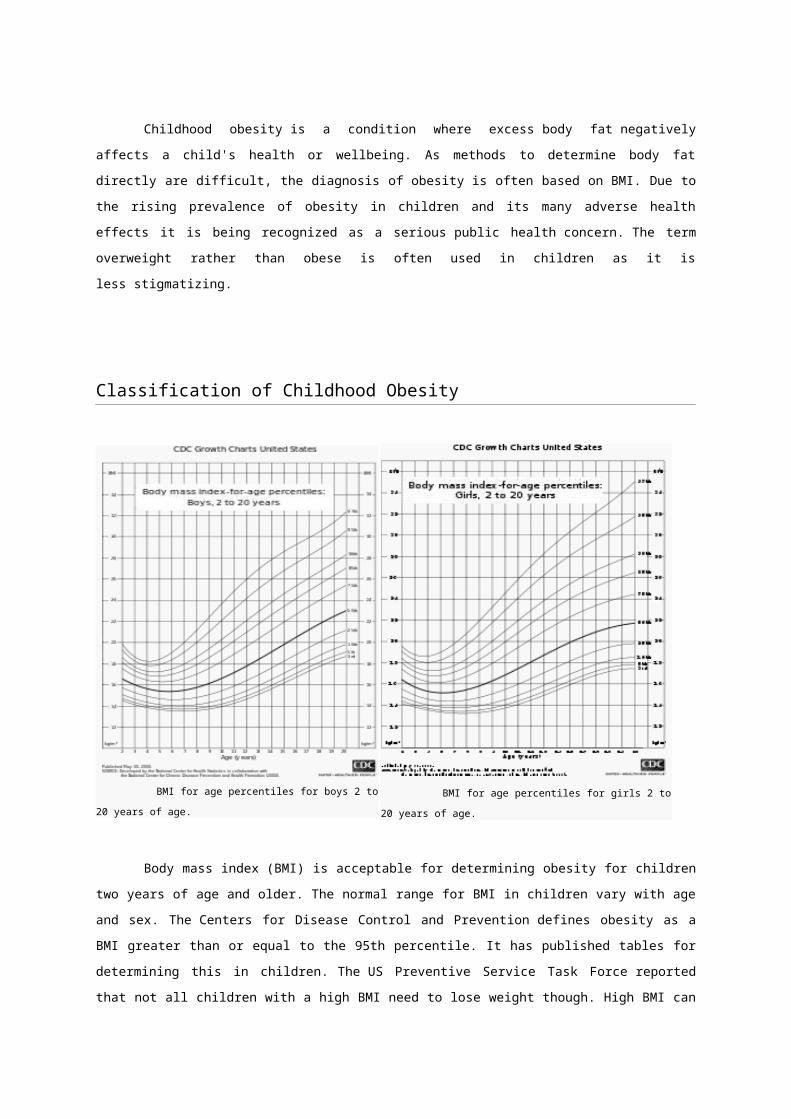
BMI for age percentiles for boys 2 to 20 years of age. BMI for age percentiles for girls 2 to 20 years of age.
Body mass index (BMI) is acceptable for determining obesity for children two years of age and
older. The normal range for BMI in children vary with age and sex. The Centers for Disease Control and
Prevention defines obesity as a BMI greater than or equal to the 95th percentile. It has published tables for
determining this in children. The US Preventive Service Task Force reported that not all children with a high
BMI need to lose weight though. High BMI can identify a possible weight problem, but doesn’t differentiate
between fat or lean tissue.
Effects on health
The first problems to occur in obese children are usuallyemotional or psychological.[6] Childhood obesity
however can also lead to life-threatening conditions including diabetes, high blood pressure, heart
disease, sleep problems, cancer, and other disorders. Some of the other disorders would includeliver
disease, early puberty or menarche, eating disorders such as anorexia and bulimia, skin infections, and
asthma and other respiratory problems. Asthma severity is not affected by obesity however. Overweight
children are more likely to grow up to be overweight adults. Obesity during adolescence has been found to
increase mortality rates during adulthood.
Obese children often suffer from teasing by their peers. Some are harassed
or discriminated against by their own family. Stereotypes abound and may lead to low self-esteem and
depression. A 2008 study has found that children who are obese have carotid arteries which have
prematurely aged by as much as thirty years as well as abnormal levels of cholesterol.
System Condition System Condition
Endocrine Impaired glucose tolerance Cardiovascula Hypertension
Diabetes mellitus
Metabolic syndrome
Hyperandrogenism
Effects on growth and puberty
Nulliparity and nulligravidity[16]
r
Hyperlipidemia
Increased risk of coronary heart
disease as an adult
Gastroentestinal Nonalcoholic fatty liver disease
CholelithiasisRespiratory
Obstructive sleep apnea
Obesity hypoventilation syndrome
Musculoskeletal
Slipped capital femoral
epiphysis (SCFE)
Tibia vara (Blount disease)
Neurological Idiopathic intracranial hypertension
Psychosocial
Distorted peer relationships
Poor self-esteem
Anxiety
Depression
Skin Furunculosis
Intertrigo
Long term health effects
Children who are obese are likely to be obese as adults. Thus, they are more at risk for adult
health problems such as heart disease, type 2 diabetes, stroke, several types of cancer, and osteoarthritis.
One study showed that children who became obese as early as age 2 were more likely to be obese as
adults. According to an article in the New York Times all of these health effects are contributing to a shorter
lifespan of five years for these obese children. It is the first time in two centuries that the current generation
of children in America may have a shorter life span than their parents.
Causes
Childhood obesity can be brought on by a range of factors which often act in
combination. “Obesogenic environment” is the medical term set aside for this mixture of elements. The
greatest risk factor for child obesity is the obesity of both parents. This may be reflected by the family's
environment and genetics. Other reasons may also be due to psychological factors and the child's body
type. A 2010 review stated that childhood obesity likely is the result of the interaction of natural selection
favouring those with more parsimonious energy metabolism and today's consumerist society with easy
access to energy dense cheap foods and less energy requirements in daily life.
Genetics
Childhood obesity is often the result of an interplay between many genetic and environmental
factors. Polymorphisms in various genes controlling appetite and metabolism predispose individuals to
obesity when sufficient calories are present. As such obesity is a major feature of a number of rare genetic
conditions that often present in childhood.

Prader-Willi syndrome with an incidence between 1 in 12,000 and 1 in 15,000 live births is
characterized by hyperphagia and food preoccupations which leads to rapid weight gain in those
affected.
Bardet-Biedl syndrome
MOMO syndrome
Leptin receptor mutations
Congenital leptin deficiency
Melanocortin receptor mutations
In children with early-onset severe obesity (defined by an onset before ten years of age and body
mass index over three standard deviations above normal), 7% harbor a single locus mutation. One study
found that 80% of the offspring of two obese parents were obese in contrast to less than 10% of the
offspring of two parents who were of normal weight. The percentage of obesity that can be attributed to
genetics varies from 6% to 85% depending on the population examined.
Socioeconomic status
It is much more common for young people who come from a racial or ethnic minority, or for those
who have a lower socioeconomic status, to be overweight and to engage in less healthy behaviors and
sedentary activities, like playing video games and computer games.
Prevention
Schools play a large role in preventing childhood obesity by providing a safe and supporting
enviornment with policies and practices that support healthy behaviors. At home, parents can help prevent
their children from becoming overweight by changing the way the family eats and exercises together. The
best way children learn is by example, so parents need to lead by example by living a healthy lifestyle.
Dietary
The effects of eating habits on childhood obesity are difficult to determine. A three-year
randomized controlled study of 1,704 3rd grade children which provided two healthy meals a day in
combination with an exercise program and dietary counsellings failed to show a significant reduction in
percentage body fat when compared to a control group. This was partly due to the fact that even though
the children believed they were eating less their actual calorie consumption did not decrease with the
intervention. At the same time observed energy expenditure remained similar between the groups. This
occurred even though dietary fat intake decreased from 34% to 27%. A second study of 5,106 children
showed similar results. Even though the children ate an improved diet there was no effect found on
BMI. Why these studies did not bring about the desired effect of curbing childhood obesity has been
attributed to the interventions not being sufficient enough. Changes were made primarily in the school
environment while it is felt that they must occur in the home, the community, and the school simultaneously
to have a significant effect.

Calorie-rich drinks and foods are readily available to children. Consumption of sugar-laden soft
drinks may contribute to childhood obesity. In a study of 548 children over a 19 month period the likelihood
of obesity increased 1.6 times for every additional soft drink consumed per day. Calorie-dense, prepared
snacks are available in many locations frequented by children. As childhood obesity has become more
prevalent, snack vending machines in school settings have been reduced by law in a small number of
localities. Some research suggests that the increase in availability of junk foods in schools can account for
about one-fifth of the increase in average BMI among adolescents over the last decade. Eating at fast
food restaurants is very common among young people with 75% of 7th to 12th grade students consuming
fast food in a given week.[39]The fast food industry is also at fault for the rise in childhood obesity. This
industry spends about $4.2 billion on advertisements aimed at young children. McDonald's alone has
thirteen websites that are viewed by 365,000 children and 294,000 teenagers each month. In addition, fast
food restaurants give out toys in children's meals, which helps to entice children to buy the fast food. Forty
percent of children ask their parents to take them to fast food restaurants on a daily basis. To make matters
worse, out of 3000 combinations created from popular items on children's menus at fast food restaurants,
only 13 meet the recommended nutritional guidelines for young children. Some literature has found a
relationship between fast food consumption and obesity. [41] Including a study which found that fast food
restaurants near schools increases the risk of obesity among the student population.
Whole milk consumption verses 2% milk consumption in children of one to two years of age had
no effect on weight, height, or body fat percentage. Therefore, whole milk continues to be recommended
for this age group. However the trend of substituting sweetened drink for milk has been found to lead to
excess weight gain.
Legal
Some jurisdictions attempt to use laws and regulations to steer kids and parents towards making
healthier food choices. Two examples are calorie count laws and banning soft drinks from sale at vending
machines in schools.
Physical activity
Physical inactivity of children has also shown to be a serious cause, and children who fail to
engage in regular physical activity are at greater risk of obesity. Researchers studied the physical activity of
133 children over a three-week period using an accelerometer to measure each child's level of physical
activity. They discovered the obese children were 35% less active on school days and 65% less active on
weekends compared to non-obese children.
Physical inactivity as a child could result in physical inactivity as an adult. In a fitness survey of
6,000 adults, researchers discovered that 25% of those who were considered active at ages 14 to 19 were
also active adults, compared to 2% of those who were inactive at ages 14 to 19, who were now said to be
active adults.[45] Staying physically inactive leaves unused energy in the body, most of which is stored
as fat. Researchers studied 16 men over a 14 day period and fed them 50% more of their energy required
every day through fats and carbohydrates. They discovered that carbohydrate overfeeding produced 75–
85% excess energy being stored as body fat and fat overfeeding produced 90–95% storage of excess
energy as body fat.
Many children fail to exercise because they are spending time doing immobile activities such as
computer usage, playing video games or watching television. Technology has a large factor on the
children's activeness. Researchers provided a technology questionnaire to 4,561 children, ages 14, 16, and
18. They discovered children were 21.5% more likely to be overweight when watching 4+ hours of TV per
day, 4.5% more likely to be overweight when using a computer one or more hours per day, and unaffected
by potential weight gain from playing video games. A randomized trial showed that reducing TV viewing
and computer use can decrease age-adjusted BMI; reduced calorie intake was thought to be the greatest
contributor to the BMI decrease.
Technological activities are not the only household influences of childhood obesity. Low-
income households can affect a child's tendency to gain weight. Over a three-week period researchers
studied the relationship of socioeconomic status (SES) to body composition in 194 children, ages 11–12.
They measured weight, waist girth, stretch stature, skinfolds, physical activity, TV viewing, and SES;
researchers discovered clear SES inclines to upper class children compared to the lower class children.
Childhood inactivity is linked to obesity in the United States with more children being overweight at younger
ages. In a 2009 preschool study 89% of a preschoolers' day was found to be sedentary while the same
study also found that even when outside, 56 percent of activities were still sedentary. One factor believed
to contribute to the lack of activity found was little teacher motivation, but when toys, such as balls were
made available, the children were more likely to play.
Home environment
Children's food choices are also influenced by family meals. Researchers provided
a household eating questionnaire to 18,177 children, ranging in ages 11–21, and discovered that four out of
five parents let their children make their own food decisions. They also discovered that compared to
adolescents who ate three or fewer meals per week, those who ate four to five family meals per week were
19% less likely to report poor consumption of vegetables, 22% less likely to report poor consumption of
fruits, and 19% less likely to report poor consumption of dairy foods. Adolescents who ate six to seven
family meals per week, compared to those who ate three or fewer family meals per week, were 38% less
likely to report poor consumption of vegetables, 31% less likely to report poor consumption of fruits, and
27% less likely to report poor consumption of dairy foods. The results of a survey in the UK published in
2010 imply that children raised by their grandparents are more likely to be obese as adults than those
raised by their parents. An American study released in 2011 found the more mothers work the more
children are more likely to be overweight or obese.
Developmental factors
Various developmental factors may affect rates of obesity. Breast-feeding for example may protect
against obesity in later life with the duration of breast-feeding inversely associated with the risk of being
overweight later on. A child's body growth pattern may influence the tendency to gain weight. Researchers
measured the standard deviation (SD [weight and length]) scores in a cohort study of 848 babies. They
found that infants who had an SD score above 0.67 had catch up growth (they were less likely to be
overweight) compared to infants who had less than a 0.67 SD score (they were more likely to gain weight).
A child's weight may be influenced when he/she is only an infant. Researchers also did a cohort
study on 19,397 babies, from their birth until age seven and discovered that fat babies at four months were

1.38 times more likely to be overweight at seven years old compared to normal weight babies. Fat babies
at the age of one were 1.17 times more likely to be overweight at age seven compared to normal weight
babies.
Medical illness
Cushing's syndrome (a condition in which the body contains excess amounts of cortisol) may also
influence childhood obesity. Researchers analyzed two isoforms (proteins that have the same purpose as
other proteins, but are programmed by different genes) in the cells of 16 adults undergoing abdominal
surgery. They discovered that one type of isoform created oxo-reductase activity (the alteration
of cortisone to cortisol) and this activity increased 127.5 pmol mg sup when the other type of isoform was
treated with cortisol and insulin. The activity of the cortisol and insulin can possibly activate Cushing's
syndrome.
Hypothyroidism is a hormonal cause of obesity, but it does not significantly affect obese people
who have it more than obese people who do not have it. In a comparison of 108 obese patients with
hypothyroidism to 131 obese patients without hypothyroidism, researchers discovered that those with
hypothyroidism had only 0.077 points more on the caloric intake scale than did those without
hypothyroidism.
Psychological factors
Researchers surveyed 1,520 children, ages 9–10, with a four-year follow up and discovered
a positive correlation between obesity and low self-esteem in the four-year follow up. They also discovered
that decreased self-esteem led to 19% of obese children feeling sad, 48% of them feeling bored, and 21%
of them feeling nervous. In comparison, 8% of normal weight children felt sad, 42% of them felt bored, and
12% of them felt nervous.[58] Stress can influence a child's eating habits. Researchers tested the stress
inventory of 28 college females and discovered that those who were binge eating had a mean of 29.65
points on the perceived stress scale, compared to the control group who had a mean of 15.19 points. This
evidence may demonstrate a link between eating and stress.
Feelings of depression can cause a child to overeat. Researchers provided an in-home interview
to 9,374 adolescents, in grades seven through 12 and discovered that there was not a direct correlation
with children eating in response to depression. Of all the obese adolescents, 8.2% had said to be
depressed, compared to 8.9% of the non-obese adolescents who said they were
depressed. Antidepressants, however, seem to have very little influence on childhood obesity. Researchers
provided a depression questionnaire to 487 overweight/obese subjects and found that 7% of those with low
depression symptoms were using antidepressants and had an average BMI score of 44.3, 27% of those
with moderate depression symptoms were using antidepressants and had an average BMI score of 44.7,
and 31% of those with major depression symptoms were using antidepressants and had an average BMI
score of 44.2.
Management
The escalation of obese children is due to the upsurge of technology, increase in snacks and
portion size of meals, and the decrease in the physical activity of children. If children were more mobile and

less sedentary, the rate of obesity would decrease. Children have to put down the electronic devices and
spend more time outside playing or exploring other options of physical acitvity. A study found kids that use
electronic devices 3 or more hours a day had between a 17- 44% increased risk of being overweight, or a
10- 61% increased risk of obese (Cespedes 2011). Parents have to recognize the signs and encourage
their children to be more physically active. There are many programs designed to encourage activities such
as Letsmove.gov, a program launched by the first lady, Michelle Obama to help combat problems with this
epidemic of obesity.
Lifestyle
Exclusive breast-feeding is recommended in all newborn infants for its nutritional and other
beneficial effects. Parents changing the diet and lifestyle of their offspring by offering appropriate food
portions, increasing physical activity, and keeping sedentary behaviors at a minimum may also decrease
the obesity levels in children.
Medications
There are no medications currently approved for the treatment of obesity in
children. Orlistat and sibutramine may however be helpful in managing moderate obesity in
adolescence. Sibutramine is approved for adolescents older than 16. It works by altering the brain's
chemistry and decreasing appetite. Orlistat is approved for adolescents older than 12. It works by
preventing the absorption of fat in the intestines.
Pictures of Malnutrition













![Malnutrition [Autosaved]](https://img.pdfslide.us/doc/110x75/577cd2051a28ab9e7895192c/malnutrition-autosaved.jpg)