Embed Size (px)
Citation preview

Republic of the Philippines
Dr Paulino J. Garcia Memorial Research and Medical Center
Cabanatuan City
Department of Surgery
CASE REPORT
OBJECTIVES of this case report is to: 1. To present a rare case of malignant phylloides
cystosarcoma, review of current literatures, management, update,. 2. To discuss the correlation
between phylloides tumor and pregnancy 2. Discuss disease progression, prognosis, and prevent
fatal outcome, 3.Promote patients education
A case of P.H. 41 y/o female, single, roman catholic, presently residing in Lambakan,
Jaen, Nueva Ecija, born on August 28, 1971 who came in with a chief complaint of right breast
mass.
The present condition started at about 8 years PTA, when the patient was diagnosed as
Low Grade Phylloides Tumor and underwent Total Mastectomy right.
Since then no follow-up was done and went unremarkable. Until 1 year PTA, when the
patient became pregnant, G1P0, she noticed a mass on the previous incision site of her right
chest areat no consult was done. Until 10 months PTA, patient had a spontaneous abortion at 16
weeks AOG, the mass progressively enlarged into 5x7 cm with ulceration and draining
abscesses. She sought consult with an OB Gyne, completion curettage was done and was then
referred at this institution for further management of tumor recurrence. But due to financial
constraint, patient failed consult.

3 months PTA, patient breast mass size progressively enlarged to 12x15cm with
ulcerations and draining sinuses. Still no consult was done.
1 month PTA, the size of the breast mass increased to 25x40cm with associated weight
loss and body weakness. Patient sought consult at our institution. Incision biopsy of the mass
was done revealing ____________________. Patient was advised for consult to oncologist for
neoadjuvant therapy. But patient cannot afford for the therapy and patient was given an option of
tumor rebulking. Patient was then cp cleared and was admitted for operation.
Past Medical History
8 years PTA, patient underwent total mastectomy right secondary to low grade phylloides, right.
Patient was a diagnosed case of Diabetes mellitus 1 year prior to admission with maintenance
medication of metformin 500mg TID
8 months prior to admission, patient admitted due to incomplete abortion PU+- 14 wks AOG and
underwent completion curettage.
Obstetrics and Gynecologic History: revealed the following Data: LMP: April 14 2012,
Menstruation: at 10 years of age, with irregular interval, for 3to5 days, amount varies from
moderate-markedly soaked pad per period, no apparent symptoms of dysmenorrheal seen.
Patient is a G1P0 (0-0-1-0) Incomplete abortion PU+ 14 weeks AOG underwent completion
curettage (Npvember 2011). No history of oral contraceptive pill therapy. Family History: A
known family of Diabetics: the patient is the eldest of four siblings. No history of breast cancer.

No other heredofamilial disease extracted. Social Environmental History: Subject is a non
smoker and a non alcoholic beverage drinker graduate as an average student of high school at
16years old.
Review of Systems revealed: GENERAL: (-) wt. loss, (-) anorexia ; HEENT: (-) icteric
sclera (-) seizure, (-)changes in sensorium, (-) epistaxis, (-)ear discharge, deafness,
CARDIOVASCULAR: (-) chest pain, (-)chest heavines, (-) palpitation, CHEST AND LUNGS:
(-) orthopnea, (-)Dyspnea, (-)shortness of breath, GASTROINTESTINAL: (-) occasionally
skip meals, (-)constipation (-) loose stool, (-)black tarry stool, GENITOURINARY: (-)
frequency,urgency, (-) hypogastric, (-)dysuria, (-) Discharges, MUSCULOSKELETAL: (-) joint
and muscle pain, SKIN: (-) jaundice, HEMATOLOGIC:(-) bruise
Physical Examination: At the ER: patient was conscious, coherent, awake, oriented,
ambulatory not in cardio pulmonary distress, afebrile. Vital Signs: BP: 120/80 CR:84 RR: 18
T: 36.7’C; Spo2: 98% at 2lpm, Wt= 59.2kg.
SKIN : no pallor, no cyanosis, no jaundice, no active dermatoses,
HEENT: pinkish-white eyebrow, pale palpebral conjunctiva, anicteric sclerae, no nasoaural
discharges, moist buccal mucosa, no gingival hemorrhages, no tonsilopharyngeal wall
congestion, no cervical lymphadenopathy, no neck vein engorgement.
BREAST: Right: 30x40cm movable, non tender, ulcerating with yellowish discharge breast mass
with palpable axillary lymph nodes



Left: no palpable mass, no axillary lymph node
CHEST: Symmetrical wall expansion, infection, no intercostals retraction, clear breath sounds,
no crackles and wheezes noted
HEART: Adynamic precordium, Normal rate regular rhythm, no murmur, PMI 5th ICS (L) MCL
ABDOMEN: flabby, no previous surgical scar, normoactive bowel sounds NABS, soft, no
tenderness elicited, no hepatosplenomegaly noted,
DRE: good sphincter tone, no pararectal tenderness, no palpable mass, full rectal vault, no blood,
no black tarry stool, positive stool on examining finger
EXTREMITIES: full and equal pulses, No bipedal edema, all are gross normal
Neurologic Examination revealed the following
Cerebral: conscious, awake, coherent, in an appropriate mood, oriented to 3spheres
cerebellar: no dysmetria, no dysdiadochokinesia, no intentional tremors, negative Romberg’s
sign
Cranial Nerve test: CRANIAL NERVE I can smell; CRANIAL NERVE II: photophobia,
3to4mm OU, ERTLA; CRANIAL NERVE Ill. IV. Vl: intact EOM’s; CRANIAL NERVE V : (+)
corneal reflex; CRANIAL NERVE VII: no facial asymmetry; CRANIAL NERVE VIII: can
hear; VESTIBULAR DIVISION; CRANIAL NERVE IX ,X good swallow reflex; CRANIAL
NERVE XI: shrugs shoulder full range; CRANIAL NERVE XII: no tongue deviation; no
weakness noted;

Motor: 5/5, full ROM, against gravity and resistance in all extrimities ; Sensory: 100% sensation;
Reflexes: ++/normoreflex; (-)babinski, (-)kernigs, (-)clonus.
Given the case presented: Salient points include:
Our initial impression: Malignant Phylloides Right s/p total mastectomy, right (2004;
PJGMRMC) secondary to low grade Phylloides tumor right
Differential Diagnosis:
Conditions to consider in the differential diagnosis of phyllodes tumors include the following:
Angiosarcoma Breast cancer Juvenile fibroadenoma Giant fibroadenoma Inflammatory carcinoma Sclerosing adenosis Radial scar Fat necrosis Fibrocystic change Breast abscess Adenocarcinoma Mastitis
Figure 1. Diagnostic Algorithm
Course in the ward:
Initial plan: For correction of anemia
For nutritional work up
For possible Subtotal gastrectomy with billroth II reconstruction after Cardiopulmonary
clearance
Patient was admitted and managed as table below:

Diagnostics Therapeutics
Cbc, blood typing, APC
Ctbt
PT, PTT
CXR-pa
12lead ECG
LIPID Profile
FBS, BUN, CREA
Serum Na/K
Pnss at KVO
Celecoxib 200mg BID
Coamoxiclav 625 mg BID
Aminoblend OD
Humulin R
Glimeperide 20mg OD PO
Diltiazem 30mg OD PO
Phytomenadione 10mg q 6 hrs
Ranitidine 50mg q 8 hrs
RESULTS:
1. Complete Blood Count Result: revealed anemia with,
5-09-12 5-12-12
Hgb 97 102
Hct 0.30 0.31
RBC ct
WBC ct 7.27 10
Neutro .68 0.74
Lympho .32 0.26

Plt ct 260 447
BT ‘O+’
2. A. Protime : 15.3 secs (10-15 secs)
%activity: 50% ( 70-130%)
B. APTT : 28.3 secs ( 27-38secs)
3. Clotting time: 6 mins ( 3-5minutes)
Bleeding time: 4mins, 45 secs ( 2-6 minutes)
4. Lipid Profile
cholesterol : 166.4 mg/dl (<200mg/dl)
triglycerides: 120.3 mg/dl (60-150mg/dl)
HDL cholesterol:29 mg/dl (40-70mg/dl)
LDL cholesterol: 113.34 mg/dl (<150mg/dl)
5. Blood Chemistry:
Fasting blood sugar: 107.9 mg/dl ( 70-105mg/dl)
Creatinine: 1 mg/dl ( 0.5-1.7 mg/dl)
6. Serum electrolytes
Sodium: 150.3 mmol/L (135-155mmol/L)
Potassium: 3.14 mmol/L ( 3.4-5.3mmol/L)--------corrected to 3. 59mmol/L
Chloride: 114. 9 mmo/L ( 96-106mmol/L)
Calcium: 1.06mmol/L (1 -1.3 mmol/L)
7. Urinalysis:

Glucose: negative Protein: positive 1 Pus cells : 10-15/hpf Red blood cells : 2-4/hpf
8. Chest Xray:
Dome shaped soft tissue density noted at the lower 2/3 of right chest area obliterating the
right cardiac border, right hemidiaphragm and costophrenic sinus.
9. 12Lead ECG
normal sinus rhythm
10. Mammography of left breast: small breast nodule left lateral aspect; axillary
lymphadenopathies
Intraoperative

FINAL DIAGNOSIS
______________________________________________________________________________
Case Discussion:
Introduction:
The cysto-sarcoma phylloides (CP) tumors of the breast are fibroepithelial tumors which are
rarely seen and have potential recurrence [1-4]. Its name is derived from the Greek words
sarcoma, meaning fleshy tumor, and phyllo, meaning leaf. CP tumors about which a great deal
of studies have been done, was clinically identified first by Muller in 1838. Less than 1 % of all
the breast tumors consist of CP tumors [4]. Phyllodes tumors can appear in any age group of
women, although it is seldom seen in girls [5,6,]. CP tumors are the ones which are not considered
initially in clinical diagnosis, show slow or rapid growth pattern, and are diagnosed after biopsy.
These rarely encountered tumors are typically seen as mobile masses in the diameter of 5
centimeters and more. Nevertheless, CP’s with diameter of 40centimeters are reported in the

literature [7]. CP tumors which are clinically similar to fibroadenomas are distinguished
histopathologically by their cellular pattern, having increased cellular atypical changes and
excessive stromal growth. CP tumors typically have more frequent local recurrence and higher
malignancy compared with fibroadenomas. Grossly, the tumor displays characteristics of a
large, malignant sarcoma, takes on a leaflike appearance when sectioned, and displays epithelial,
cystlike spaces when viewed histologically. The malignant variety of the phylloides tumor is rare
with <1% occurrence. Metastasis is usually hematogenous, and axillary lymph node dissection is
not routinely performed. [8]
Phyllodes tumor during pregnancy grows fast and its size is relatively big. Malignant phylloides
tumors are exceedingly rare with few cases being reported in pregnancy. Blaker et al describe the
first case ever reported of a malignant phylloides tumor presenting in the first trimester of
pregnancy and provide insight into the complexities of management as well as a review of the
known literature. Six other cases of phylloides tumor presenting in pregnancy have been reported
in the literature, one of which had bilateral disease. Of these, the average patient age was 32
years (range, 28 to 35 years). The majority of these patients presented in their third trimester
(mean, 29 weeks; range, 20 to 36 weeks) and often had large tumors (mean, 15 cm; range, 5 to
21 cm). Four of the seven tumors (57%) required a mastectomy. Previous cases have shown
phylloides tumors to present in the third trimester as large masses that require mastectomy. With
early detection, malignant phylloides tumors can present in the first trimester of pregnancy at
smaller sizes; in these patients, breast-conserving surgery is possible. [9]

DIAGNOSTIC CRITERIA Usually large and grossly circumscribed
Fibroepithelial proliferation with broad "leaf-like" papillae inserting into slit-lilke or cleft-like spaces
- Exaggerated intracanalicular pattern
Cellular stroma- Periductal stromal condensation may seen
Frankly sarcomatous stroma may be seen in malignant phyllodes tumor- Heterologous differentiation may occur in malignant phyllodes tumor
A. Liposarcoma B. Osteosarcoma
C. Chondrosarcoma D. Rhabdomyosarcoma
Grading determined by presence or absence of atypical stromal features
Benign Versus Malignant Phyllodes Tumors
Because of limited data, the percentage of benign versus malignant phyllodes tumors is not well
defined. Reports suggest, however, that about 85-90% of phyllodes tumors are benign and that
approximately 10-15% are malignant.[4-10]
Although the benign tumors do not metastasize, they have a tendency to grow aggressively and
can recur locally.[2-11] Similar to other sarcomas, the malignant tumors metastasize
hematogenously. Unfortunately, the pathologic appearance of a phyllodes tumor does not always
predict the neoplasm's clinical behavior; in some cases, therefore, there is a degree of uncertainty
about the lesion's classification.

The characteristics of a malignant phyllodes tumor include the following[5-12] :
Recurrent malignant tumors seem to be more aggressive than the original tumor
The lungs are the most common metastatic site, followed by the skeleton, heart, and liver
Symptoms of metastatic involvement can arise from as early as a few months to as late as
12 years after the initial therapy
Most patients with metastases die within 3 years of the initial treatment[6-13]
No cures for systemic metastases exist
Roughly 30% of patients with malignant phyllodes tumors die from the disease
Frequency

Phyllodes tumors account for less than 1 percent of all breast tumors. The malignant variety of
the phylloides tumor is rare with <1% occurrence.
Race
As far as is known, phyllodes tumors occur with the same frequency in women of all races and in
all parts of the world.
Sex- and age-related demographics
Phyllodes tumors occur almost exclusively in females, although rare case reports have been
described in males. The tumors can develop in people of any age; however, the median age is the
fifth decade of life.
History
Phyllodes tumors generally manifest as larger masses and display rapid growth. A small mass
may rapidly increase in size in the few weeks before the patient seeks medical
attention.Phyllodes tumor include the rapid but painless growth of a smooth, bulky mass within
the affected breast. The patient may notice that her entire breast is enlarged and its shape
distorted. The skin over-lying the tumor may feel warm to the touch and develop a shiny
appearance; it may also become translucent. Tumors rarely involve the nipple-areola complex or
ulcerate to the skin. Patients with metastases may present with such symptoms as dyspnea,
fatigue, and bone pain.
Physical examination
A firm, mobile, well-circumscribed, nontender breast mass is appreciated. Curiously,
cystosarcoma phyllodes tends to involve the left breast more commonly than the right one.

Overlying skin may display a shiny appearance and be translucent enough to reveal underlying
breast veins. Physical findings (ie, the occurrence of mobile masses with distinct borders) are
similar to those of fibroadenoma.[3-14]
The median size of phyllodes tumors is around 4 cm [1]. Twenty percent of tumors grow larger
than 10 cm, the arbitrary cut off point for the designation as a giant tumor. These tumors can
reach sizes up to 40 cm in diameter [2].
Journal of Surgical Oncology 2008, 6:117 doi:10.1186/1477-7819-6-117 Giant breast tumors: Surgical management of phyllodes tumors,potential for reconstructive surgery and a review of literatureMargaret I Liang1, Bhuvaneswari Ramaswamy2, Cynthia C Patterson1,Michael T McKelvey3, Gayle Gordillo4, Gerard J Nuovo5 andWilliam E Carson III*6Address: 1The Ohio State College of Medicine, Columbus, Ohio, USA, 2The Ohio State University Department of Haematology-Oncology, ArthurG. James Cancer Hospital and Richard J. Solove Research Institute, Division of Internal Medicine, Columbus, Ohio, USA, 3The Ohio StateUniversity Division of Dermatology, Columbus, Ohio, USA, 4The Ohio State University Division of Plastic Surgery, Columbus, Ohio, USA, 5TheOhio State University Department of Pathology, Columbus, Ohio, USA and 6The Ohio State University Department of Surgery, Arthur G. JamesCancer Hospital and Richard J. Solove Research Institute, Division of Surgical Oncology, Columbus, Ohio, USA
Differential Diagnosis
Conditions to consider in the differential diagnosis of phyllodes tumors include the following:
Angiosarcoma Breast cancer Juvenile fibroadenoma Giant fibroadenoma Inflammatory carcinoma Sclerosing adenosis Radial scar Fat necrosis Fibrocystic change Breast abscess Adenocarcinoma Mastitis
Juvenile Fibroadenoma Low Grade Phyllodes Tumor

No leaf-like architecture Prominent leaf-like architectureNo condensation around ducts Stromal condensation around ductsDoes not infiltrate May infiltrate surrounding breast***The histologic border between these two is not always sharp
Juvenile Fibroadenoma High Grade Phyllodes TumorNo stromal atypia Atypical stromaStromal mitotic rate < 3/hpf Elevated stroma mitotic rateNo stromal overgrowth Stromal overgrowthDoes not infiltrate May infiltrate surrounding breast ***Stromal overgrowth defined as at least one low power field (40x total magnification) composed entirely of stroma
Fibroadenoma Low Grade Phyllodes TumorLacks significant stromal hypercellularity Hypercellular stroma is prominentNo stromal overgrowth May have stromal overgrowthNo leaf-like architecture Prominent leaf-like architectureNo condensation around ducts Stromal condensation around ductsDoes not infiltrate May infiltrate surrounding breast***The histologic border between these two is not always sharp
Metaplastic Carcinoma Phyllodes TumorSpindled component may be positive for high molecular weight keratin or p63
Stromal component negative for high molecular weight keratin and p63
Epithelial component is malignant Epithelial component is benignSquamous differentiation may be present No squamous differentiation
Pure Sarcoma of the Breast Very rare The presence of an epithelial component defines phyllodes tumor
Fibromatosis
Bland spindle cells Stellate configuration Absence of intrinsic epithelial component
May entrap normal breast lobules Myofibroblastoma
Resembles solitary fibrous tumor

Lacks intrinsic epithelial component
Biopsy and Histology
Open excisional breast biopsy for smaller lesions and incisional biopsy for large lesions are the
definitive methods for diagnosing phyllodes tumors.
Fine-needle aspiration for cytologic examination usually is inadequate for the diagnosis of
phyllodes tumors. Core biopsy is more reliable, but there still can be sampling errors and
difficulty in distinguishing the lesion from a fibroadenoma.
All phyllodes tumors contain a stromal component that can vary significantly in histologic
appearance from one lesion to another.[7] In general, benign phyllodes tumors demonstrate a
markedly increased number of regular fusiform fibroblasts in the stroma. Occasionally, highly
anaplastic cells with myxoid changes are observed. A high degree of cellular atypia, with
increased stromal cellularity and an increased mitotic count, is almost always observed in the
malignant form of cystosarcoma phyllodes.
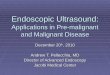
Micrograph of a phyllodes tumor (right of image) with the characteristic long clefts and myxoid cellular stroma. Normal breast andfibrocystic change are also seen (left of image). H&E stain

Fig.1. Panoramic view of the tumor showing tubular and malignant adipose components (H&E, x 40)Fig.2.
Fig.2. Stromal component with liposarcomatous differentiation (H&E, x 100)
Fig.3. Leaf-like projections characteristic of phyllodes tumor (H&E, x 40)
Fig.4. Tubular component with juxtaposed regular mammary lobules (H&E, x 40)
Ultrastructurally, in the benign and malignant forms of phyllodes tumors, nucleoli may reveal a coarsely meshed nucleolonema and abundant cisternae in the endoplasmic reticulum.
Laboratory and Imaging Studies

Laboratory studies
No specific hematologic tumor markers or other blood tests can be used to diagnose
cystosarcoma phyllodes.[7]
Imaging studies
Although mammography and ultrasonography generally are important in the diagnosis of breast
lesions, they are notoriously unreliable in differentiating benign cystosarcoma phyllodes from the
malignant form of the condition or from fibroadenomas. (The phyllodes tumor’s mammographic
appearance, as a round density with smooth borders, is similar to that of fibroadenoma.) Thus,
findings on imaging studies are not definitively diagnostic of phyllodes tumors.[8]
Clinical Staging, Treatments, and Prognosis
Staging
Phyllodes tumors are not staged in the usual sense; they are classified on the basis of their
appearance under the microscope as benign, borderline (or indeterminate), or malignant. The
pathologist makes the decision on the basis of the cells' rate of division (mitosis) and the number
of irregularly shaped cells in the biopsy sample. In one series of 101 patients with phyllodes
tumors, 58 percent were identified as benign, 12 percent as borderline, and 30 percent as
malignant.
GradingAdverse features
Stromal overgrowth (> one 40x field without epithelium) High mitotic index (>10 /10 hpf) Sarcomatous stroma (stromal nuclear pleomorphism and atypia) Infiltrative margin
Benign

No adverse features 20% recurrence rate after local excision 10% recurrence rate after wide excision (at least 1 cm margin) No reported metastases
Borderline One or more adverse features but short of definition for malignant (see below) 45% recurrence rate after local excision 30% recurrence rate after wide excision (at least 1 cm margin) No reported metastases
Malignant High mitotic index and sarcomatous stroma OR Stroma overgrowth and either high mitotic index or sarcomatous stroma 65% recurrence rate after local excision 35% recurrence rate after wide excision (at least 1 cm margin) 30% metastatic rate
Staging Not applicable
Report Grade Size Margin status Presence and type of heterologous differentiation
Treatments
Multidisciplinary approach
The treatment team for a patient with a phyllodes tumor will usually include a diagnostic
radiologist, a gynecologist, a general surgeon, oncologist and a pathologist

Surgical excision is the usual treatment for phyllodes tumors, whether benign or malignant. In
the case of benign tumors, the surgeon will usually try to spare as much breast tissue as possible,
generally removing about 1 in (2 cm) of normal breast tissue from the area around the tumor as
well as the tumor itself. If the tumor is very large, however, the doctor may remove the entire
breast.
Tumor Excision and Mastectomy
Complete excision, with accurate histologic examination and continued follow-up care, is the
best way to treat phyllodes tumors. In most cases of cystosarcoma phyllodes, perform wide local
excision, with a rim of normal tissue included.[9, 10, 11] No absolute rules on margin size exist.
However, a 2cm margin for small (< 5cm) tumors and a 5cm margin for large (>5cm) tumors
have been advocated.
The lesion should not be "shelled out," as might be done with a fibroadenoma, or the recurrence
rate will be unacceptably high.[6]
If the tumor-to-breast ratio is sufficiently high to preclude a satisfactory cosmetic result by
segmental excision, total mastectomy, with or without reconstruction, is an alternative. More
radical procedures are generally not warranted.[10]
Perform axillary lymph node dissection only for clinically suspicious nodes. However, virtually
all of these nodes are reactive and do not contain malignant cells.[12]
Postoperative complications

As with most breast surgery, postoperative complications from the surgical treatment of
phyllodes tumors include the following:
Infection
Seroma formation
Local and/or distant recurrence
Adjuvant therapy
There is no proven role for adjuvant chemotherapy or radiation therapy in the treatment of
phyllodes tumors. Response to chemotherapy and radiotherapy for recurrences and metastases
has been poor, and no success with hormonal manipulation has been documented.
Alternative and Complementary Therapies
Women who have had surgery for removal of a phyllodes tumor appear to use CAM therapies as
often and for the same reasons as women treated for breast cancer. According to the Behavioral
Research Center of the American Cancer Society, breast cancer survivors are highly likely to use
some form of alternative or complementary therapy during cancer treatment or within a year or
two of completing conventional treatment. A survey of 608 longer-term (8 years or longer)
breast cancer survivors reported in early 2005 that the majority were still using CAM therapies.
The survey respondents gave four reasons for using alternative treatments:
To maintain an active role in recovery from cancer.
To reduce their stress level.
To reduce the risk of recurrence.

To maintain hope.
Specific CAM therapies mentioned by the women in the ACS survey included exercise, humor,
self-help books (bibliotherapy), prayer or spiritual practice, vitamin treatments, relaxation
exercises, and support groups. Dr. Kenneth Pelletier, the former director of the program
in complementary and alternative medicine at Stanford University School of Medicine,
lists hypnosis, visualization, naturopathy, and journaling as other alternative approaches that
breast cancer patients find helpful. Acupuncture is frequently mentioned as a useful method of
pain control.
Coping With Treatment
Coping with the aftereffects of surgery for a phyllodes tumor is similar to coping with the effects
of surgery for breast cancer. Patients who have had a complete mastectomy may experience pain,
limited range of motion or weakness in the affected arm, scarring, or swelling.
Exercises, outpatient physical therapy, and massage help to relieve these side effects of breast
surgery. In terms of follow-up, most patients treated for phyllodes tumors are scheduled for
a postoperative visit with the surgeon 1–2 weeks after surgery, with periodic checkups thereafter.
Clinical Trials
The National Cancer Institute (NCI) is not conducting any clinical trials involving phyllodes
tumors as of 2005. There is, however, an ongoing study at the Dartmouth-Hitchcock Medical
Center in New Hampshire of the effectiveness of radiation therapy in preventing recurrences of
borderline or malignant phyllodes tumors in patients who have been treated with local excision
of the tumor. Women who have had a borderline or malignant phyllodes tumor removed within
the past three months may wish to consider participating in this study.

Prognosis
The prognosis for benign phyllodes tumors is good following surgical removal, although there is
a 20–35 percent chance of recurrence, particularly in patients over the age of 45. Recurrence is
usually treated with further surgery, either another local excision or a complete mastectomy.
The prognosis for patients diagnosed with borderline or malignant phyllodes tumors is more
guarded. About 4 percent of borderline tumors will eventually metastasize. A Mayo Clinic study
of 50 patients with malignant tumors found that 32 percent had a recurrence within two years
after surgery; 26 percent developed metastases, and 32 percent of the group died from
their malignancy. The most common sites for metastases from malignant phyllodes tumors are
the lungs, bones, liver, and chest wall, although metastases to the lymph nodes have also been
reported. Most patients with metastases from a malignant phyllodes tumor die within three years
of their first treatment.
Prevention
There is no way to prevent phyllodes tumors as of the early 2000s because their cause is not yet
known.
Outpatient Care

Although specific guidelines regarding follow-up care for phyllodes tumors are limited because
of the rarity of these lesions, regular, long-term follow-up care should be performed to detect
possible local recurrences.
An initial visit 1-2 weeks after surgery to detect any initial complications should be followed by
periodic visits as determined by the patient's surgeon. A reasonable schedule might be physical
examinations every 6 months and mammograms yearly for at least 5 years. Carefully observe
patients for any possible recurrence.
References
1. Carter BA, Page DL. Phylloides tumor of the breast: Local recurrence versus metastatic capacity. Hum Pathol. 2004; 35: 1051-1052
2. Korula A, Varghese J, Thomas M, Vyas F, Korula A. Malignant phyllodes tumour with intraductal and invasive carcinoma and lymph node metastasis. Singapore Med Journal 2008; 49(11); e318
3. Moffat CJC, Pinder SE, Dixon AR, Elaston CW, Blarney RW, Elis IO. Phyllodes tumors of the breast: a clinicopathological review of thirty-two cases. Histopathology. 1995;27:205-218.

4. Reinfuss M, Mitus J, Duda K, Stelmach A, Rys J, Smolak K. The treatment and prognosis of patients with phyllodes tumor of the breast – analysis of 170 cases. Cancer 1996;77: 910-16.
5. Carter BA, Page DL. Phylloides tumor of the breast: Local recurrence versus metastatic capacity. Hum Pathol. 2004; 35: 1051-1052
6. Korula A, Varghese J, Thomas M, Vyas F, Korula A. Malignant phyllodes tumour with intraductal and invasive carcinoma and lymph node metastasis. Singapore Med Journal 2008; 49(11); e318
7. Moffat CJC, Pinder SE, Dixon AR, Elaston CW, Blarney RW, Elis IO. Phyllodes tumors of the breast: a clinicopathological review of thirty-two cases. Histopathology. 1995;27:205-218.
8. Reinfuss M, Mitus J, Duda K, Stelmach A, Rys J, Smolak K. The treatment and prognosis of patients with phyllodes tumor of the breast – analysis of 170 cases. Cancer 1996;77: 910-16.
9. Blaker KM, Sahoo S, Schweichler MR, Chagpar AB. Malignant phylloides tumor in pregnancy Department of Surgery, University of Louisville, Louisville, Kentucky, USA.
10. Jones AM, Mitter R, Poulsom R, et al. mRNA expression profiling of phyllodes tumours of the breast: identification of genes important in the development of borderline and malignant phyllodes tumours. J Pathol. Dec 2008;216(4):408-17. [Medline]
11. Parker SJ, Harries SA. Phyllodes tumours. Postgrad Med J. Jul 2001;77(909):428-35. [Medline]. [Full Text].
12. Abe M, Miyata S, Nishimura S, Iijima K, Makita M, Akiyama F, et al. Malignant transformation of breast fibroadenoma to malignant phyllodes tumor: long-term outcome of 36 malignant phyllodes tumors. Breast Cancer. Oct 2011;18(4):268-72. [Medline].
13. Brooks HL, Priolo S, Waxman. Cystosarcoma phylloides: a case report of an 11-year survival and review of surgical experience. Contemp Surg. 1998;53:169-72.
14. Yohe S, Yeh IT. "Missed" diagnoses of phyllodes tumor on breast biopsy: pathologic clues to its recognition. Int J Surg Pathol. Apr 2008;16(2):137-42. [Medline].
15.
1. Hoover HC. Cystosarcomas of the breast. In: Raaf JH, ed. Soft Tissue Sarcomas: Diagnosis and Treatment. St Louis, Mo: Mosby; 1993:113-21.
2. Parker SJ, Harries SA. Phyllodes tumours. Postgrad Med J. Jul 2001;77(909):428-35. [Medline]. [Full Text].

3. Yohe S, Yeh IT. "Missed" diagnoses of phyllodes tumor on breast biopsy: pathologic clues to its recognition. Int J Surg Pathol. Apr 2008;16(2):137-42. [Medline].
4. Jones AM, Mitter R, Poulsom R, et al. mRNA expression profiling of phyllodes tumours of the breast: identification of genes important in the development of borderline and malignant phyllodes tumours. J Pathol. Dec 2008;216(4):408-17. [Medline].
5. Abe M, Miyata S, Nishimura S, Iijima K, Makita M, Akiyama F, et al. Malignant transformation of breast fibroadenoma to malignant phyllodes tumor: long-term outcome of 36 malignant phyllodes tumors. Breast Cancer. Oct 2011;18(4):268-72. [Medline].
6. Brooks HL, Priolo S, Waxman. Cystosarcoma phylloides: a case report of an 11-year survival and review of surgical experience. Contemp Surg. 1998;53:169-72.
7. Al-Masri M, Darwazeh G, Sawalhi S, Mughrabi A, Sughayer M, Al-Shatti M. Phyllodes Tumor of the Breast: Role of CD10 in Predicting Metastasis. Ann Surg Oncol. Oct 18 2011;[Medline].
8. Cole-Beuglet C, Soriano R, Kurtz AB. Ultrasound, x-ray mammography, and histopathology of cystosarcoma phylloides. Radiology. Feb 1983;146(2):481-6. [Medline]. [Full Text].
9. Chen WH, Cheng SP, Tzen CY, et al. Surgical treatment of phyllodes tumors of the breast: retrospective review of 172 cases. J Surg Oncol. Sep 1 2005;91(3):185-94. [Medline].
10. Contarini O, Urdaneta LF, Hagan W. Cystosarcoma phylloides of the breast: a new therapeutic proposal.Am Surg. Apr 1982;48(4):157-66. [Medline].
11. Pezner RD, Schultheiss TE, Paz IB. Malignant phyllodes tumor of the breast: local control rates with surgery alone. Int J Radiat Oncol Biol Phys. Jul 1 2008;71(3):710-3. [Medline].
12. Gullett NP, Rizzo M, Johnstone PA. National surgical patterns of care for primary surgery and axillary staging of phyllodes tumors. Breast J. Jan-Feb 2009;15(1):41-4. [Medline].
13. Jones AM, Mitter R, Springall R, et al. A comprehensive genetic profile of phyllodes tumours of the breast detects important mutations, intra-tumoral genetic heterogeneity and new genetic changes on recurrence.J Pathol. Apr 2008;214(5):533-44. [Medline].