Embed Size (px)
Citation preview
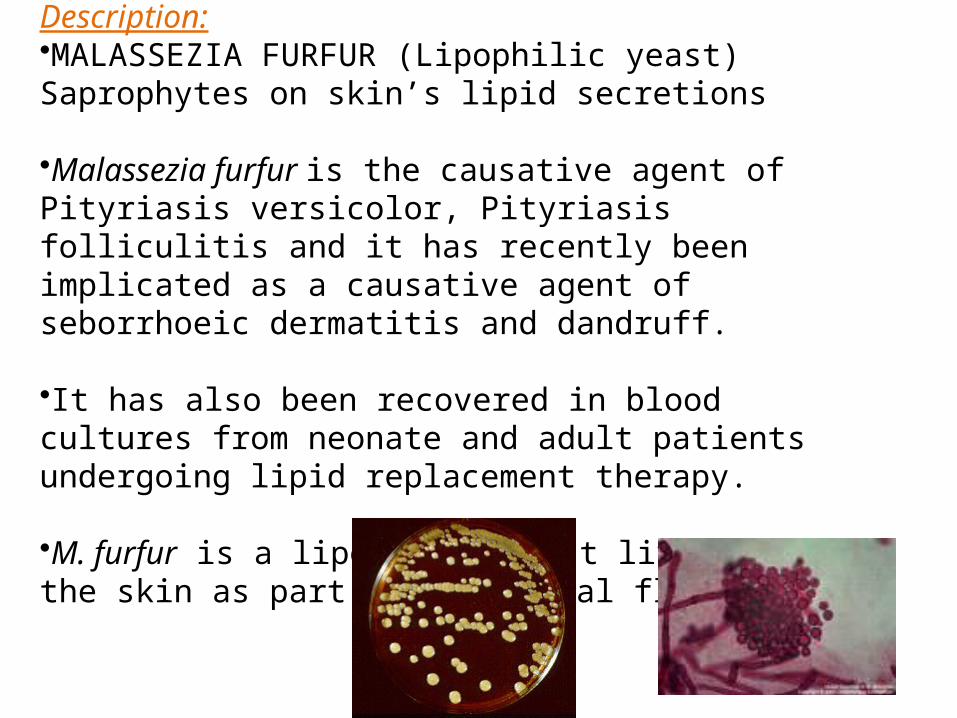
Malassezia infectionsDescription:•MALASSEZIA FURFUR (Lipophilic yeast) Saprophytes on skin’s lipid secretions
•Malassezia furfur is the causative agent of Pityriasis versicolor, Pityriasis folliculitis and it has recently been implicated as a causative agent of seborrhoeic dermatitis and dandruff.
•It has also been recovered in blood cultures from neonate and adult patients undergoing lipid replacement therapy. •M. furfur is a lipophilic yeast living on the skin as part of the normal flora.

Clinical manifestations1. Pityriasis versicolor:• showing hyperpigmented lesions in a Caucasian and in an Australian Aborigine(Tinea versicolor), which is a chronic and not serious disease infection of skin.
•Pityriasis versicolor: This is a chronic, superficial fungal disease of the skin characterised by well-demarcated white, pink, beige, or brownish lesions, often combining, and covered with thin furfuraceous scales. •The colour varies according to the normal pigmentation of the patient, exposure of the area to sunlight, and the severity of the disease. •Lesions occur on the trunk, shoulders and arms, rarely on the neck and face, and fluoresce a pale greenish colour under Wood's ultra-violet light.
•Young adults are affected most often, but the disease may occur in childhood and old age.
•Pityriasis versicolor showing hyperpigmented lesions in aCaucasian and hyphopigmented lesions in an Australian Aborigine

2 .Pityriasis folliculitis:
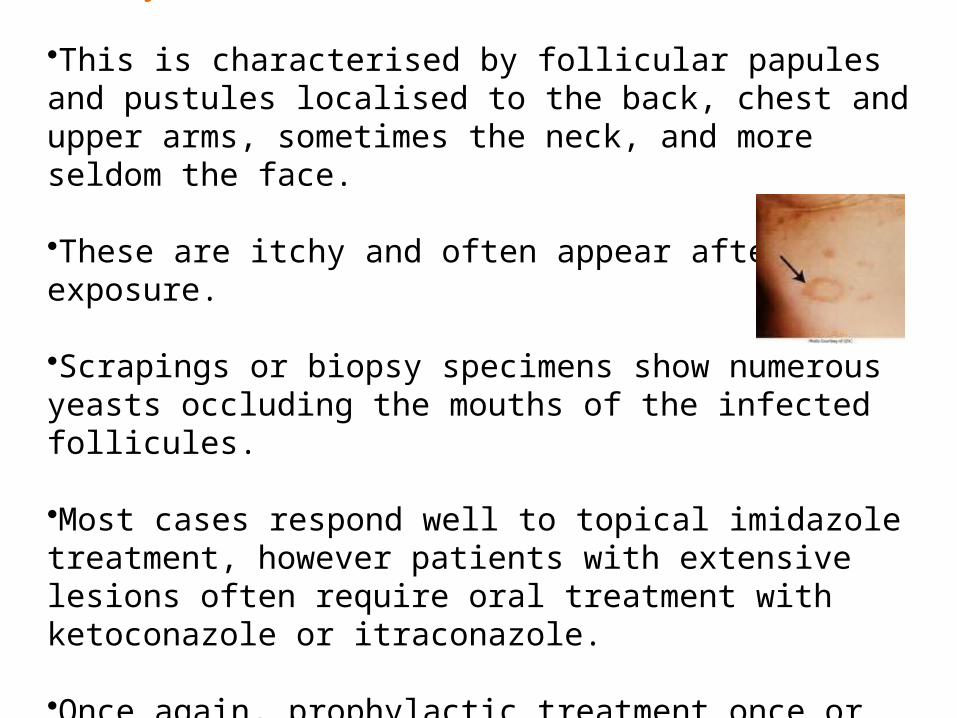
•This is characterised by follicular papules and pustules localised to the back, chest and upper arms, sometimes the neck, and more seldom the face. •These are itchy and often appear after sun exposure. •Scrapings or biopsy specimens show numerous yeasts occluding the mouths of the infected follicules. •Most cases respond well to topical imidazole treatment, however patients with extensive lesions often require oral treatment with ketoconazole or itraconazole. •Once again, prophylactic treatment once or twice a week is mandatory to prevent relapse

3 .Seborrhoeic dermatitis and dandruff:
•Current evidence suggests M. furfur, combined with multifactorial host factors is also the direct cause of seborrhoeic dermatitis, with dandruff being the mildest manifestation.
•Host factors include genetic predisposition, an emotional component (possible endocrine or neurologically mediated factors), changes in quantity and composition of sebum (increase in wax esters and a shift from triglycerides to shorter fatty acid chains), increase in alkalinity of skin (due to excessive sweating) and external local factors such as occlusion.
•Patients with neurological diseases such as Parkinson's disease and those with AIDS are commonly affected.
•Clinical manifestations are characterised by scaling in areas with a rich supply of sebaceous glands ie the scalp, face, eyebrows, ears and upper trunk.
•Lesions are red and covered with greasy scales and itching is common in the scalp.
•The clinical features are typical and skin scrapings for a laboratory diagnosis are unnecessary.
•Once again, the use of a topical imidazole is recommended, especially ketoconazole which has proved to be the most effective agent.
•Relapse is common and retreatment when necessary is the simplest approach for long term management.

4 .Fungaemia: •M. furfur has also been reported as causing catheter acquired fungaemia in neonate and adult patients undergoing lipid replacement therapy.
•Such patients may also develop small embolic lesions in the lungs or other organs. •Diagnosis requires special culture media and blood drawn back through the catheter is the preferred specimen. Culture of the catheter tip is also recommended.
Transmission:The fungus exists as a free living saprophyte and probably spread from one to another by exposure to desquamated scales. Lack of personal hygiene facilitates development of skin lesions.
Laboratory diagnosis:1. Clinical material: Skin scrapings from patients with superficial lesions,
blood and indwelling catheter tips from patients with suspected fungaemia.
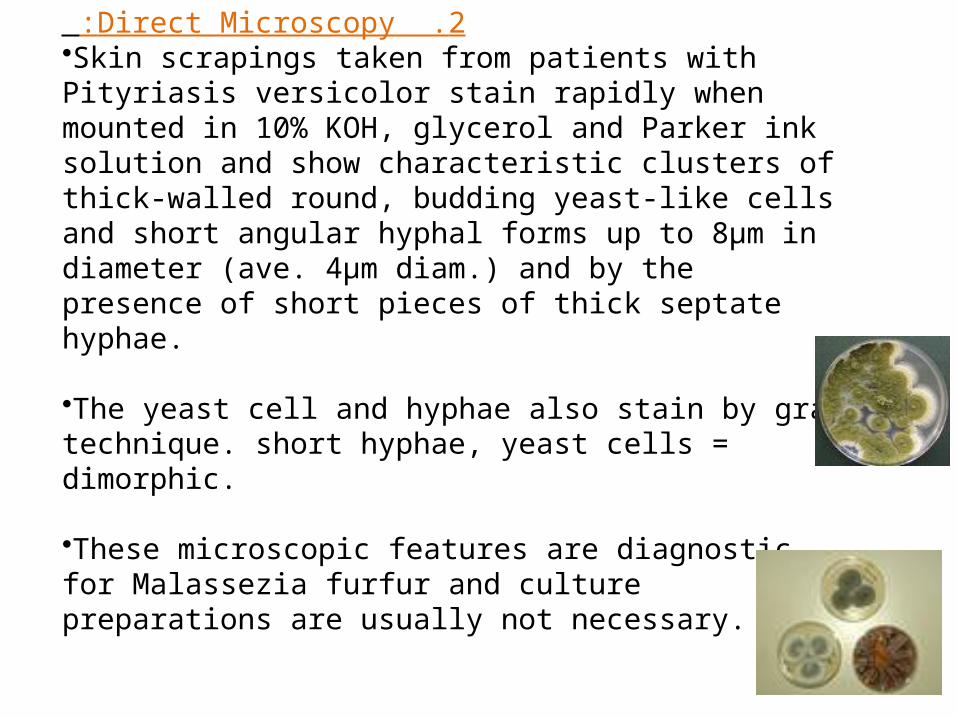
2 .Direct Microscopy: •Skin scrapings taken from patients with Pityriasis versicolor stain rapidly when mounted in 10% KOH, glycerol and Parker ink solution and show characteristic clusters of thick-walled round, budding yeast-like cells and short angular hyphal forms up to 8μm in diameter (ave. 4μm diam.) and by the presence of short pieces of thick septate hyphae.
•The yeast cell and hyphae also stain by gram technique. short hyphae, yeast cells = dimorphic.
•These microscopic features are diagnostic for Malassezia furfur and culture preparations are usually not necessary.

•GMS stained (Gomori- Grocott methenamine silver) skin biopsy showing characteristic spherical yeast cells and short pseudohyphal elements typical of M. furfur.
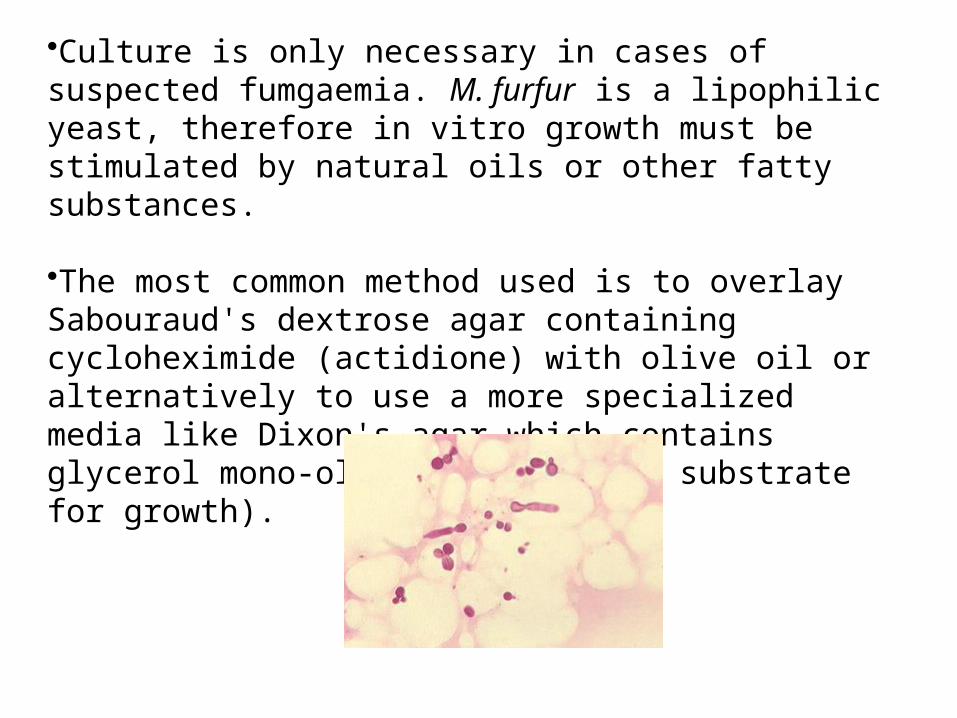
3 .Culture: •Culture is only necessary in cases of suspected fumgaemia. M. furfur is a lipophilic yeast, therefore in vitro growth must be stimulated by natural oils or other fatty substances. •The most common method used is to overlay Sabouraud's dextrose agar containing cycloheximide (actidione) with olive oil or alternatively to use a more specialized media like Dixon's agar which contains glycerol mono-oleate (a suitable substrate for growth).

4 .Serology :•There are currently no commercially available serological procedures for the diagnosis of Malassezia infections.
5. Identification: Microscopic evidence of inipolar, broad base budding yeast cells and special lipid requirements for growth in culture are usually diagnostic. Causative agents:Malassezia furfur










![Malassezia Folliculitis versus Truncal Acne Vulgaris ... · 278 Malassezia Folliculitis versus Truncal Acne Vulgaris (Clinical and Histopathological Study) support the diagnosis [5,6,10]](https://img.pdfslide.us/doc/110x75/5cdf712988c99399558c9005/malassezia-folliculitis-versus-truncal-acne-vulgaris-278-malassezia-folliculitis.jpg)