Embed Size (px)
Citation preview

Making Education Effective and Fun:
Stations-Based Approach to Teaching Radiology
and Anatomy to Third-Year Medical Students
Rahul Arya, MD, Trevor Morrison, MD, Ann Zumwalt, PhD, Kitt Shaffer, MD, PhD
Ac
FrHaK.of24
ªht
Rationale and Objectives: A hands-on stations-based approach to teaching anatomy to third-year medical students is used at BostonUniversity. The goal of our study was to demonstrate that such an interactive, team-based approach to teaching anatomy would be well
received and be helpful in recall, comprehension, and reinforcement of anatomy learned in the first year of medical school.
Materials andMethods: Each radiology-anatomy correlation lab was focused on one particular anatomic part, such as skull base, pelvis,coronary anatomy, etc. Four stations, including a three-dimensional model, computer, ultrasound, and posters, were created for each lab.
Informed consent was obtained before online survey dissemination to assess the effectiveness and quality of radiology-anatomy correla-
tion lab. This study was approved by our institutional institutional review board, and data were analyzed using a c2 test.
Results: Survey data were collected from February 2010 throughMarch 2012. The response rate was 33.5%.Overall, the highest percent-
age of students (46%) found the three-dimensional model station to be the most valuable. The computer station was most helpful in recall
of the anatomic principles from the first year of medical school. Regarding the quality of the anatomy lab, less than 2% of the students
thought that the images were of poor quality or the material presented was not clinically relevant.
Discussion: Our results indicate that an interactive, team-based approach to teaching anatomy was well received by the medical stu-
dents. It was engaging and students were able to benefit from it in multiple ways.
Key Words: Medical education; radiology anatomy lab; resident teaching; radiology clerkship; radiology rotation.
ªAUR, 2013
Astrong working knowledge of anatomy is essential to
learn radiology, for radiologists as well as clinicians
reviewing cases with their patients or interpreting
imaging reports. In a traditional medical school curriculum,
human anatomy is taught in the first year, whereas radiology
clerkships, if offered, are generally in the clinical third or
fourth years (1). Studies have shown that retention of ana-
tomic knowledge from the first year to clinical third or fourth
years is poor (2,3). In studies examining retention of anatomic
knowledge in Dutch medical students, it was shown that
learning anatomy in a clinically oriented manner and
revisiting topics later in the clinical curriculum led to
improved test performance (4). From these studies, it can be
inferred that medical students would benefit from revisiting
key anatomic concepts during the radiology clerkship to
enhance their level of understanding and retention. Based
on this belief, radiology-anatomy correlation labs (RACL)
were developed in collaboration between the Anatomy
Department and the Radiology Department, to allow third-
ad Radiol 2013; 20:1311–1318
om the Department of Radiology, Boston University Medical Center, 820rrison Avenue, FGH Building, 3rd Floor, Boston, MA 02118 (R.A., T.M.,S.); Department of Anatomy and Neurobiology, Boston University SchoolMedicine, Boston, MA 02118 (A.Z.). Received May 8, 2013; accepted July, 2013. Address Correspondence to: R.A. e-mail: [email protected]
AUR, 2013tp://dx.doi.org/10.1016/j.acra.2013.07.012
year medical students to revisit key concepts learned in first-
year anatomy course and place them in the context of a clinical
setting. Our group has previously published the description of
these active learning exercises, which are integrated into
RACL stations (5).
At our institution, radiology is a required month-long clin-
ical clerkship for third-year medical students. RACL takes
place once during the radiology clerkship, giving students a
chance to rotate through the lab once during their rotation.
Each RACL session, which lasts 1.5–2 hours, focuses on one
specific anatomic region. Labs designed to date include bra-
chial plexus, pelvic anatomy, coronary circulation, skull base
anatomy, liver/portal system, and upper/lower extremity vas-
cular access sites. One month, the group rotating through
the radiology clerkship may participate in the pelvic anatomy
RACL, while during another month, another group may par-
ticipate in a skull base anatomy RACL, and so on. For the
RACL, students are divided into four groups that rotate among
four task-oriented stations, which are focused on a single ana-
tomic part: (a) a station of 3D (three-dimensional) model con-
struction, where students assemble a complex part of the body
from component parts; (b) a poster stationwith typical imaging
of the body area being studied for identification; (c) a computer
station with video clips that allow scrolling through cross-
sectional exams or angiography/fluoroscopy in real-time; and
(d) a hands-on ultrasound (US) station for students to practice
scanning techniques pertinent to the specific anatomic part.
1311

ARYA ET AL Academic Radiology, Vol 20, No 10, October 2013
Each RACL is lead by three or four instructors, which may
include radiology residents, radiology attendings, and anatomy
department faculty (The instructors were recruited on a volun-
tary basis via an e-mail, which included information on the
anatomy module being covered.) The goal of our study was
to demonstrate that such an interactive, team-based approach
to teaching anatomy would be well received and would be
helpful in recall, comprehension, and reinforcement of anat-
omy learned in the first year of medical school.
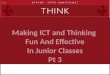
Figure 1. Assembled heart model showing anomalous origin of theleft anterior descending coronary artery (LAD) from the right coronary
artery (RCA) with a nonmalignant course anterior to the pulmonary
outflow tract.
METHODS
Initially, when the RACLs were devised, cadaver prosections
were planned for one of the stations. However, there are
inherent difficulties in the use of cadavers in this setting.
They are costly to store and maintain, degrade in quality
over time, and are not equally available throughout the aca-
demic year. Additionally, since cadaveric dissection is a
destructive process, in the process of dissecting students are
often forced to destroy some structures to subsequently access
deeper structures. Our solution was to build inexpensive 3D
models using computed tomography (CT) or magnetic reso-
nance (MR) data, which are suitable for a medical student lab
exercise in terms of durability. To produce models, we
enlarged the CT images to desired proportions, printed as
two-dimensional images, and subsequently applied to a
foam board of appropriate thickness, thus generating a ‘‘to-
scale’’ 3D model. The areas of interest were then assembled
to form the rigid model, with additional removable compo-
nents as needed. These 3D models were created using inex-
pensive materials that can be found at a craft store or
ordered online, such as foam rubber, duct tape, plastic tubing,
and wire. The final models are sturdy and can be constructed
for less than $100. Students during the RACL work as a team
to assemble the model from its component parts (Fig 1).
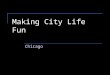
For the poster station, a large-format image pertaining to
the specific anatomic region was created using radiographic
and cross-sectional CT and MR images (Fig 2). The images
on the poster indicate structures for identification with arrows
or outlines. Worksheets are provided to the students to fill in
the answers. Instructors lead the students through the poster
and encourage discussion of the covered information through
additional questions. Answer sheets are provided to the
instructors for review before the lab.
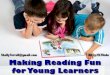
For the web-based station, separate modules for each ana-
tomic part were created on the web. Printed instructions are
provided to the students for recording answers during the
RACL. These interactive web-based modules allow the stu-
dents to scroll through labeled and nonlabeled anatomic struc-
tures (Fig 3). Specific questions about both anatomy and
imaging techniques are asked, and open discussion is encour-
aged by the instructors.
For the US station, a region is chosen for examination that
is relevant to the particular region of focus for the RACL.
This particular station was not included in every RACL due
to limited availability of the US machine. Survey results
1312
from only the labs that included a US station are included in
this study. Initially, we used a portable US machine loaned
to us by the manufacturer (GE Healthcare, Waukesha, WI).
For later labs, we used the US machine from the interven-
tional radiology suite when it was not being used for
procedures.
The study was approved by the institutional review board of
the Boston University Medical Center. Medical students were
notified verbally at the end of each RACL session about an
optional survey. This verbal notification was followed by an
e-mail soliciting their participation with a hyperlink to the
online survey. The students were notified as part of the con-
sent, which was displayed as a pop-up message immediately
before beginning of the online survey, that their participation
was completely optional and anonymous and would not have
an effect on their grades. The survey, which was itself pass-
word protected for access, was created using the Survey
Monkey website (https://www.surveymonkey.com). The
information collected was password protected, completely
anonymous, and untraceable to the respondents.
The survey was similar for each RACL with a few minor
modifications to the stem of the question, depending on the
topic area (Fig 4). Two major categories of questions were
asked: (1) those pertaining to the perceived benefits of
RACL and (2) those pertaining to the quality of the RACL.

Figure 2. Coronary anatomy poster.
Academic Radiology, Vol 20, No 10, October 2013 STATIONS-BASED APPROACH TO RADIOLOGY AND ANATOMY
Regarding the benefits of RACL, students were asked whether
the stations helped them recall anatomic principles from first
year of medical school, improved their understanding of 3D
anatomic and physiologic relationships, and helped them to
correlate 3D structures and two-dimensional images. Regard-
ing the quality of the RACL, students were asked whether
clinically relevant material was presented, whether the instruc-
tions were clear, whether the instructors were helpful, and
whether the time allotted was appropriate. Multiple answers
were permissible for many of the questions. The students
were also asked whether they had a positive experience at
the stations and to rank stations based on their overall educa-
tional value. Data was analyzed using c2 test with P value
<.05 considered statistically significant. There were also fields
for comments for feedback for every station and instructor.
RESULTS
TheRACL has been conducted monthly for the past 3 years as
part of the radiology clerkship, with RACL lab sessions held
during each clerkship block. Survey data were collected
from February 2010 through March 2012. Attendance is
strongly encouraged but not required for the RACL. By our
observation estimates, approximately 80% of the students
attend the RACL. Taking this into account, the response
rate for the survey was 33.5%. Figure 5 shows the breakdown
of the RACL by each anatomic part. The differences in pref-
erences of the overall educational value of the various stations
chosen by the students were statistically significant, yielding a
P value of .0005, calculated using c2 test. Forty-six percent
found the 3D model to be most valuable, 25% found the
US to be most valuable, 20% found the computer station to
be most valuable, and 15% found the poster to be most valua-
ble (Fig 6).
A comparison of the specific survey questions for the dif-
ferent stations of the RACL is shown in Figure 7. The dif-
ferences in results in all the categories were statistically
significant with P values <.05, which were calculated using
c2 test. The computer workstation was most helpful in recall
of anatomic principles from the first year of medical school.
1313

Figure 3. Sample images from web-based computer station for
cardiac radiology-anatomy correlation lab, with cine angiogram
showing stenosis of a coronary artery.
ARYA ET AL Academic Radiology, Vol 20, No 10, October 2013
With regard to improving understanding of 3D physical rela-
tionships, the 3D model and computer station were equally
more helpful than other stations. Greater numbers of stu-
dents believed that the computer station and US stations
presented clinically relevant material compared to other sta-
tions. In addition, 32% of the students expressed that the US
station did not help their understanding of 3D physical rela-
tionships, which was significantly different than other sta-
tions, for which the percentage ranged from 0% to 3% (P
< .05). Regarding the quality of the lab, for each station,
greater than 80% of the students responded that the instruc-
tors were helpful and that the instructions were clear. Less
than 2% of the students thought that the images were of
poor quality or the material presented was not clinically
relevant.
There were a total of 47 subjective responses. Since
some of these responses had multiple parts, these were bro-
ken down into 82 individual comments. Of these 44 com-
ments were positive, 9 comments were negative, and 28
comments were neutral suggestions (Fig 8). The difference
in the comments was statistically significant with a P value
of .000013, calculated using c2 test. One of the positive
comments was, ‘‘There was also a very manageable amount
of information for the length of the session.’’ Another one
of positive comments was, ‘‘Nice supplement to the cour-
sework, made us remember anatomy.’’ Another positive
comment was, ‘‘Fun, a blast from the past in terms of anat-
omy.’’ A negative comment mentioned, ‘‘Often times
when there is too much going on in a short period of
time, students don’t remember anything.’’ Another nega-
tive comment was, ‘‘The computer station was too
detailed. It took a long time and some of the material
we could have gone over on our own.’’
1314
DISCUSSION
Our results indicate that an interactive, team-based
approach to teaching anatomy was well received by the
medical students. It was engaging and students were able
to benefit from it in multiple ways. The 3D models were
an important aspect of RACL with highest percentage of
students (46%) finding this station to be of the highest edu-
cational value compared to the other stations. We believe
that the 3D models have many benefits with regard to com-
prehension and knowledge retention. Since the learner is
given a disassembled set of components and asked to build
the region of interest from scratch, a high understanding
of anatomic relationships is required. Construction forces
the learner to grapple with how complex areas are intercon-
nected and to reach an appreciation of 3D relationships that
is difficult to obtain from simply observing dissection or
online models. Compared to learning from an anatomy
atlas, when students construct they are required to synthe-
size relationships from scratch, and thus develop their ana-
tomic knowledge at a deeper level than learned by
identification alone.
Almost half of students found the 3D model building sta-
tion to be the most helpful, but the distribution of students
selecting other stations as ‘‘most helpful’’ was relatively even,
suggesting that different learning styles were being reached
by each type of approach. Such ‘‘blended learning’’ (described
as ‘‘the thoughtful integration of classroom face-to-face learn-
ing experiences with online learning experiences’’) has been
used successfully in similar settings to teach anatomy (6–9).
Traditionally, the term is applied to classroom and Internet-
based learning modules (7). In our RACLs, we extended
the blended learning approach to additional components,
including 3D models and posters as visual tools, to reinforce
the concepts being taught. A blended curriculum encourages
the students to learn both individually and together, allowing
for a personalized reflective element of review (7). During the
RACL, the student–instructor relationship was student cen-
tered rather than instructor centered. The instructors were
able to act more as a guide and less as a disseminator of knowl-
edge since the students worked in teams to solve problems
raised by the different stations. The instructors provided
guidelines and created environments where students were
encouraged to arrive at their own conclusions (10). Addition-
ally, working as a team promoted interaction, which is
thought to enhance learning and retention of anatomic
knowledge (11).
Strong visuospatial ability has been linked to improved
retention of anatomy. A study by Lufler et al. demonstrated
that participation in medical gross anatomy increases students’
visuospatial ability, and students’ preexisting visuospatial abil-
ity is predictive of performance in medical gross anatomy (12).
Assembling 3D models requires students to interact with
actual physical objects, introducing additional sensory modal-
ities (touch, proprioception), in addition to just visual input.
Research suggests that teaching using more than one input

Figure 4. Sample survey. Questions 2, 3, and 4 were the same format and pertained to the three-dimensional model, ultrasound, and com-
puter workstations.
Academic Radiology, Vol 20, No 10, October 2013 STATIONS-BASED APPROACH TO RADIOLOGY AND ANATOMY
system and more than one method is helpful in enhancing
learning and retention (13). Most available online 3D pro-
grams only function at the level of recognition, with rotatable
models that students must manipulate or ‘‘fly’’ through (using
virtual endoscopic reconstructions) to identify structures of
interest (14). These may be inferior to actual physical 3D
1315

Figure 5. Number of labs for each anatomic part.
Figure 6. Students’ rating of ‘‘most valuable station.’’ US,
ultrasound.
ARYA ET AL Academic Radiology, Vol 20, No 10, October 2013
models due to lack of tactile input; however, more research is
required.
Gross anatomy is usually taught to medical students during
first year of medical school via classroom didactics and in
cadaveric anatomy laboratory. Although cadaveric anatomy
laboratory forms the foundation of anatomy learning and is
considered a rite of passage for physicians-to-be, it may
decline in the future due to logistical and financial constraints
(15). The 3D models are relatively inexpensive and require no
specialized preparation and room to store. Additionally, they
can be used repeatedly, whereas cadavers can only be used
once. Our 3D models were inexpensive, with materials cost-
ing less than $100 for each model. The 3D models may serve
as an adjunct in teaching anatomy when cadaveric models are
unavailable due to expense. More research is required com-
paring learning outcomes using 3D models versus cadaveric
anatomy.
The Internet station was made part of the RACL with the
thought that such electronic media can allow the user to inter-
act with the material to be learned in a virtual environment,
thereby enhancing learning (16). Additionally, the electronic
media, which can be custom built for the user, targets the
needs of that particular user. In our case, the website was
developed by one of the instructors. Each online anatomic
module was developed from scratch and customized to corre-
spond to the material presented by the poster and the 3D
model. Cases for different anatomic modules were created
from real patient anonymized dataset obtained from our
department picture archiving and communication system.
1316
QuickTime videos and static images without labels (for dis-
cussion purposes) and with labels (for review purposes)
were used. The students interacted with themedia by scrolling
through the QuickTime videos to identify the anatomic
structures. But even with its possible benefits, electronic
media remain underused in the field of medical education
(17). Specifically, Durfee et al (18) reported that despite the
use widespread use of digital technology and picture archiving
and communication system in the field of radiology, digital
technology was underused in radiology courses. Various bar-
riers toward incorporating digital technology may include
cost of the equipment, the personnel time required to develop
the educational programs, and the difficulty of integrating
new technology into medical curriculum (18).
Approximately, 20% of the students found the computer
station to be the most valuable, which was less than for the
3D model station and the US station. This may be due to
the fact that the computer station was not as unique as the
3D model station and US station, since there are many web-
sites already available for review of anatomy. But a large pro-
portion of the students (>80%) did report that the computer
station helped them recall important principles from the first
year of medical school and that it improved their understand-
ing of important physical relationships. These results demon-
strate the complementary role of the computer station in the
RACL. Based on student comments, we plan to provide stu-
dents the link to the website in advance, so that they have a
chance to review the material beforehand, which would serve
to familiarize students with the material and likely save time
during the RACL. The computer station was also most valua-
ble in presenting clinically relevant material (along with US
station). This may be because the computer station included
real life abnormal cases demonstrating different pathologies,
so students were able to translate that knowledge gained
more readily to their clinical rotations.
Compared to the stations, the US station was least helpful in
helping recall anatomic principles from the first year of med-
ical schools and improving understanding of important 3D
relationships. However, the US station was most helpful in
presenting clinically relevant material (along with the com-
puter station). These results were initially perplexing to us
but easily explainable. Medical students are not directly
exposed to this important diagnostic hands-on modality dur-
ing any stage of their training in the first 2 years of medical
school. While they are tested on cross-sectional images as
part of their first year anatomy course, they do not have a
lot, if any, exposure to US. Therefore, correlating the anatomy
seen onUS to the anatomy learned during first year of medical
school would be difficult, given the small amount of hands-on
time with the probe. US studies are frequently performed as
part of diagnostic workup. Presumably, students perceived
that the basic knowledge of US that they obtained during
the RACL would be clinically relevant while they rotate
through their other clinical rotations.
Each month during the radiology rotation, we currently
conduct a single RACL, so students are given a detailed

Figure 7. Perceived benefits and drawbacks of different stations. 3D, three dimensional; US, ultrasound.
Academic Radiology, Vol 20, No 10, October 2013 STATIONS-BASED APPROACH TO RADIOLOGY AND ANATOMY
review of only one anatomic region. Although there were a
couple of negative subjective comments with regards to the
different workstations getting repetitive, there were many
benefits of learning via repetition and reinforcement as dem-
onstrated by our results. Also, we hope that anatomic teaching
in even a single area will stimulate student interest and make
them more likely to strive to recall their anatomic knowledge
from first year and apply it in all of their clinical rotations.
In conclusion, we believe that our interactive multista-
tion, team-based approach to teaching anatomy was well
received and was helpful in recall, comprehension, and
reinforcement of anatomy learned in the first year of
1317

Figure 8. Subjective comments from students.
ARYA ET AL Academic Radiology, Vol 20, No 10, October 2013
medical school. Future directions for the RACL include
creating 3D models of other regions from CT data, such
as the temporal bone and skull base, which are both small
anatomic regions with many complex structures of clinical
importance. A model of the brachial plexus region (using
coronal MR data to construct a framework of bony and
deep muscular structures, with removable superficial
muscles, vessels and nerves) is currently being used and
evaluated. Models of the knee (using sagittal MR data)
and the brain stem (using axial CT data) are also planned.
Residents and medical students are included in the planning
team for each new lab and the initial model construction
also includes faculty from the anatomy department. An
elective rotation for fourth-year students is also planned
where each student could develop a new model and review
all existing labs.
REFERENCES
1. Ganske I, Su T, Loukas M, et al. Teaching methods in anatomy courses in
North American medical schools the role of radiology. Acad Radiol 2006;
13:1038.
1318
2. Feigin DS, Magid D, Smirniotopoulos JG, et al. Learning and retaining nor-
mal radiographic chest anatomy: does preclinical exposure improve stu-
dent performance? Acad Radiol 2007; 14:1137.
3. Prince KJ, Scherpbier AJ, Van Mameren H, et al. Do students have suffi-
cient knowledge of clinical anatomy? Med Educ 2005; 39:326–332.
4. Bergman EM, Prince KJ, Drukker J, et al. How much anatomy is enough?
Anat Sci Educ 2008; 1:184–188.
5. Zumwalt AC, Lufler RS, Monteiro J, et al. Building the body: active learning
laboratories that emphasize practical aspects of anatomy and integration
with radiology. Anat Sci Educ 2010; 3:134–140.
6. Faraone KL, Garrett PH, Romberg E. A blended learning approach to
teaching pre-clinical complete denture prosthodontics. Eur J Dent Educ
2013; 17:e22–e27.
7. Garrison DR, Kanuka H. Blended learning: uncovering its transformative
potential in higher education. Internet Higher Educ 2004; 7:95–105.
8. Lujan HL, DiCarlo SE. First-year medical students prefer multiple learning
styles. Adv Physiol Educ 2006; 30:13–16.
9. Shaffer K, Small JE. Blended learning in medical education: use of an
integrated approach with web-based small group modules and didac-
tic instruction for teaching radiologic anatomy. Acad Radiol 2004; 11:
1059.
10. Rosenbaum PE, Mikalsen Ø, Lygre H. A blended learning course design in
clinical pharmacology for post-graduate dental students. Open Dent J
2012.
11. Terrell M. Anatomy of learning: instructional design principles for the ana-
tomical sciences. Anat Rec Part B New Anatomist 2006; 289:252–260.
12. Lufler RS, Zumwalt AC, Romney CA, et al. Effect of visual-spatial ability on
medical students’ performance in a gross anatomy course. Anat Sci Educ
2012; 5:3–9.
13. Sugand K, Abrahams P, Khurana A. The anatomy of anatomy: a review for
its modernization. Anat Sci Educ 2010; 3:83–93.
14. Rodt T, Ratiu P, Becker H, et al. 3D visualisation of the middle ear and ad-
jacent structures using reconstructed multi-slice CT datasets, correlating
3D images and virtual endoscopy to the 2D cross-sectional images. Neu-
roradiology 2002; 44:783–790.
15. Gabard DL, Lowe DL, Chang JW. Current and future instructional methods
and influencing factors in anatomy instruction in physical therapy and
medical schools in the US. J Allied Health 2012; 41:53–62.
16. Azer SA. Cost consciousness and medical education. N Engl J Med 2010;
363:890. author reply 890-891.
17. Vozenilek J, Huff JS, Reznek M, et al. See one, do one, teach one: ad-
vanced technology in medical education. Acad Emerg Med 2004; 11:
1149–1154.
18. Durfee SM, Jain S, Shaffer K. Incorporating electronic media into medical
student education: a survey of AMSER members on computer and web
use in radiology courses. Acad Radiol 2003; 10:205–210.