Embed Size (px)
Citation preview

Sandra Simmons, RN Barbara Given, RN
Nissen fundoplication for hiatus hernia repair
Esophageal hiatus hernia is among the most common anatomic abnormalities of the upper gastrointestinal tract. Usually, it is not associated with dis- ease.’ A hiatus hernia is three times more common than a gastric ulcer. Al- though the hernia may have been pres- ent since birth, symptoms are not usu- ally noted until age 50 and may follow periods of increased abdominal pres- sure, which may be caused by obesity, pregnancy, physical exertion, or lifting; trauma to the chest or abdomen; or as- cites. Hiatus hernias are found more often in women than men. A brief re- view of normal anatomy and physiology aids in better understanding the pa- thology associated with hiatus hernia and the corrective surgery.
Anatomy and physiology. The esophagus connects the hypopharynx with the cardiac end of the stomach. It lies posterior to the trachea and larynx and passes through the diaphragm at the level of the eleventh thoracic ver- tebra. The esophagus is approximately 23 to 25 cm long and 1 t o 2 cm wide. The distal 3 to 5 cm constitute the lower esophageal sphincter (LES), which is composed of an ampulla and vestibule. Although the LES is called a sphincter, it is more accurately a zone of increased pressure rather than an anatomic struc- ture.
The pressure in the LES is approxi- mately 15 to 30 mm Hg or more above fundal pressure and appears to be the
prime factor preventing the reflux of gastric contents onto the sensitive esophageal mucosa. The LES functions independently of the stomach and the esophagus. The LES pressure and com- petence are increased by gastrin and some parasympathetic drugs and de- creased by secretin, cholecystokinin, anticholinergics, smoking, fatty foods, and alcohol.
The wall of the esophagus has four layers: the external or fibrous layer, muscular layer, areolar layer, and the inner mucous layer. The muscle in the upper portion of the esophagus is striated; in the lower portion, i t is smooth muscle. The blood and lymph vessels lie in the areolar layer, the sec- retory glands lie in the mucous layer, and the nerve fibers lie between the muscular and submucous layers.
The esophagus is innervated by both sympathetic and parasympathetic fib- ers. The parasympathetic innervation is derived from the vagus nerve. The sympathetic fibers come from the cervi- cal and thoracic ganglia and from pre- ganglionic fibers of the greater and les- ser splanchnic nerves. The LES receives both sympathetic and parasympathetic fibers, whereas the lower esophagus re- ceives vagal fibers. Visceral sensory in- nervation is via the autonomic nervous system, which may explain why some esophageal diseases have symptoms similar to other areas of the body with the same innervation.
AORN Journal, July 1981, Vol34 , No 1 35

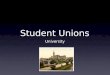
Fig 1. Hiatus hernia. A normal stomach is shown at left. At right, the cardia of the stomach is displaced through the diaphragm into the thoracic cavity. Reprinted with permission from B Given, S Simmons, Gastroenterology in Clinical Nursing, 3rd ed (St Louis: C V Mosby, 7979).
Arterial blood supply to the esoph- agus comes from the esophageal ar- teries of the aorta, inferior thyroid ar- tery, and the left gastric artery. Venous drainage is via the azygos, left gastric, and thyroid veins. Lymphatic drainage of the esophagus is to the internal jugu- lar vein from the cervical esophagus; to the intercostal nodes from the thoracic esophagus; and to the diaphragmatic, infracardiac, and left gastric nodes from the lower esophagus.
Pathophysiology. The terms hiatus her- nia, esophageal hernia, or diaphrag- matic hernia are used interchangeably and refer to herniation of a part of the stomach through an opening or hiatus in the diaphragm (Fig 1). Over 90% of esophageal hernias in adults are of the
“sliding” type, where the esophago- gastric junction “slides” into the thorac- ic cavity when intraabdominal pressure increases or when the patient assumes a supine position. Normally, the opening in the diaphragm tightly encircles the esophagus, preventing ascension of the stomach into the thoracic cavity.
The major clinical problems associ- ated with a sliding hiatus hernia are usually not due to the herniation itself but t o symptoms associated with changes in pressure and reflux. Pyrosis (heartburn), the major symptom, occurs in 90% of patients. This is due to the reflux of gastric contents into the esophagus. Heartburn usually is not de- scribed as pain but rather as an uncom- fortable burning sensation below the
36 AORN Journal, July 1981, Vol34 , No 1

sternum tending to move up into the neck. It is often associated with a dull, full, heavy, bloating feeling. This dis- comfort most frequently occurs one-half hour to one hour after meals and at bed- time. Any increase in the intraabdomi- nal pressure, such as may be caused by bending over, vigorous exercise, or as- suming a recumbent position, pre- cipitate discomfort. Heartburn can also be induced by drinking citrus juice.
Regurgitation of a sour and bitter tasting hot fluid into the throat and mouth is another symptom of reflux. This usually occurs at night or when the patient is bending over. The regurgita- tion is not accompanied by nausea. Painful swallowing, or odynophagia, may occur when swallowing or when taking liquids or fluids. Odynophagia varies in intensity from mild discomfort to severe substernal pain and is usually described as sharp, sticking, and stab- bing.
Other symptoms of hiatus hernia in- clude nausea and vomiting, esophageal obstruction, acute hemorrhage, chronic anemia, or dysphagia. Since it is dif- ficult to differentiate the symptoms of angina from those of hiatus hernia, it is important to determine the etiology of the pain carefully when obtaining a pa- tient history (Table l). Pain caused by the hernia may travel via the vagus nerve and reduce the flow of coronary blood, causing an angina attack.
Differentiation between gastric or duodenal ulcer and hiatus hernia is also
Table 1
Factors to assess in haitus hernia patients
Discomfort related to activity Dysphagia Eructation Odynophagia (painful swallowing) Pyrosis (heartburn) Regurgitation Taste in mouth
important. In both conditions, pain oc- curring a t night is accompanied by burning sensations that are relieved by milk and antacid therapy. Pain that oc- curs in the daytime persists longer after eating if it is caused by an ulcer than if the cause is a hiatus hernia. Diagnosis of hiatus hernia will include barium swallow, esophagoscopy, and motility and pressure studies.
If the esophageal hernia causes no symptoms, treatment is usually not necessary. For treatment, medical management is preferred and consists of alterations in activity, regularly scheduled meals, and antacid therapy. Highly seasoned foods, coffee, and fruit juices should be avoided. Patients should not assume a recumbent position for up to two hours after meals. Tight clothing should be avoided, smoking stopped, weight reduced, and emotional stress decreased. If medical treatment is unsuccessful and reflux with symptoms
Sandra Simmons, RN, MS, is assistant pro- fessor and director of life-long education at the Michigan State University College of Nursing, East Lansing. A graduate of Miami Valley Hospital School of Nursing, Dayton, Ohio, she received a baccalaureate in nursing and a master's degree from Ohio State University, Columbus.
Barbara Given, RN, PhD, FAAN, is professor and assistant dean in the Michigan State Uni- versity College of Nursing. She received a dip- loma from Miami Valley Hospital School of Nursing, a baccalaureate in nursing and mas- ter's degree from Ohio State University, and a doctorate from Michigan State University.
Simmons and Given are authors of Gas- troenterology in Clinical Nursing, 3rd ed, pub- lished by C V Mosby in 1979.
AORN Journal, July 1981, Vol34, NO 1 37

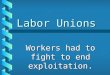
Fig 2. Steps in Nissen fundoplication (left to right). First, the fold of fundus is placed
posterior to the esophagus, which is being held with a Penrose drain. Next, seromuscular
sutures are used to form the plication. The esophageal wallis not included in the sutures.
On the right is the completed plication.
persists, surgery may be indicated. Preoperative care. In addition to gen-
eral preoperative care, the patient with a hiatus hernia will need special atten- tion in several areas. Although the pa- tient may have all of the usual fears about surgery, these may be over- shadowed by the wish for relief of the uncomfortable, long-standing symp- toms.
During preoperative contacts, the nurse should ensure that the patient understands the nature of the surgery by asking him or her to describe the surgery. Any significant errors in un- derstanding should be reported to the physician and documented. The patient should also be given the opportunity to express how he or she feels about having surgery, as well as the results expected.
Preoperative teaching of turning, coughing, and deep breathing is espe- cially important for this patient because the incision is near the diaphragm, and a high number of patients also have chronic obstructive pulmonary disease. The proximity of the incision to the diaphragm will make coughing and deep breathing very painful. The pa- tient should know this preoperatively as well as the need for coughing and deep breathing. Appropriate ways to support the incision when coughing should also be reviewed.
Obese patients should be encouraged to lose weight before surgery, and pa- tients who smoke should be encouraged to stop five days before the operation to provide time for the lungs to clear somewhat. The patient should also know that just before surgery and for several days following surgery, a
nasogastric tube will be in place, intr; venous fluids will be given, and oral in- take will be limited.
The patient needs to know that the drainage through the tube may be dark brown for eight hours after surgery. This may decrease apprehension when bloody drainage is seen. Following surgery, the patient will be assisted in learning how to decrease aerophagia and possibly alter some eating habits. The success of postoperative recovery rests in good preoperative teaching and support.
Surgical indications. The major rea- son for surgery for hiatus hernia is to correct the reflux, thus relieving the symptoms. A secondary reason is to re- place and anchor the displaced viscus and to prevent recurrence.2 Other indi- cations for surgery are obstruction, usually due to stricture, and hemor- rhage. Associated conditions treated during hiatus hernia surgery include cholelithiasis and gastric andlor duodenal ulcer. Ulcers occur in approx- imately 16% of hiatus hernia cases and require entry into the abdominal cav- it^.^
The first surgery for hiatus hernia,
38 AORN Journal, July 1981, Vol34, No 1

done by William Mayo in 1911, was aimed at correcting the anatomic defect. In 1951, Allison expanded the knowl- edge and repair by developing a mecha- nism to prevent reflux. In 1955, Nissen in Switzerland and Belsey in England independently developed similar surgi- cal techniques, and in 1967, Hill added his operative a p p r ~ a c h . ~ The latter three continue to be the most common approaches, along with the newer Collis gastropexy combined with the Belsey Mark IV. A description of the Nissen fundoplication will provide an under- standing of the other approaches.
The intent of the Nissen fundoplica- tion is to prevent the fundus of the stomach from sliding through the dia- phragm and prevent reflux of gastric con- tents into the e~ophagus.~ Fundoplica- tion is based on the valve principle-an increase in pressure or volume within the stomach will close the cardia and block reflux into the esophagus. Fun- doplication creates not only a valve-like unidirectional flow in the esophagus but also an active substitute sphincter with inherent contractability.6
Procedure. Access is gained to the surgical site through an abdominal in-
I I cision, usually an upper median lap- arotomy. The esophagus is identified by prior placement of a large-lumen gastric tube. This tube helps to ensure that the plication is not made too tight. The left hepatic lobe is displaced to allow full vision and movement of the lower esophagus and fundus. By placing light traction on the stomach, the her- nia can be reduced and the cardia vis- ualized.
The distal esophagus is freed and ele- vated with a Penrose drain. A fold of the fundal wall is brought completely around the esophagus from back to front and sutured or stapled to itself, not in- corporating the esophagus' (Fig 2). Manometric studies are conducted be- fore, during, and after the plication to determine the pressure in the sphincter area of the esophagus and prevent the plication from being too tight. The sur- geon should be able to slip a finger be- tween the esophageal wall and fundus after the suturing is completed.
The large-lumen gastric tube is re- moved following surgery and a smaller sized one inserted if needed. Before re- moval, 250 ml of saline may be inserted into the stomach to test the adequacy of
AORN Journal, July 1981, Vol34, No 1 39

he “gas-bloat” syndrome T is the most significant postoperative problem.
the plication. After saline is inserted, the tube is raised above the plication, the pylorus is pinched shut, and the stomach is squeezed in an attempt to cause reflux. If the plication is ade- quate, no reflux will occur. The tube may then be lowered and the saline as- pirated. If reflux occurs, revision of the plication may be done immediately to ensure competence, eliminating the need for reoperation.8
A Penrose drain may be inserted into the wound or a stab wound following the procedure. In the Nissen procedure, more than other plication procedures, excess resection around the head of the spleen may necessitate its concurrent removal due to excessive t r a ~ m a . ~
The major difference between the Nissen repair and other hiatus hernia repairs is the amount of fundal wrap around the esophagus. The Belsey re- pair does a 270-degree wrap; Hill uses 180 degrees. The Belsey repair places sutures in the esophagus with the wrap; some variations of the Nissen procedure also do. The Hill approach does not su- ture the plication directly t o the esophagus but sutures around the gas- troesophageal junction to the posterior abdominal wall.lo
The Belsey repair is always done through a thoracotomy. The Nissen re- pair may be carried out through a thoracic approach but usually is done abdominally, as is the Hill repair. The Belsey procedure also restructures the
angle of entry of the esophagus into the stomach. Other variations in these pro- cedures include wrapping the fundus around the esophagus in an anterior to posterior manner, rather than the pos- terior to anterior wrap used in the Nis- sen procedure.
Surgical complications following the fundoplication are uncommon but need to be discussed. With any fundoplica- tion, especially the complete wrap- around Nissen, care must be taken that the wrap is not too tight, obstructing the esophagus. On the other hand, if the plication is patulous, reflux will still oc- cur, and reoperation will be necessary (Fig 3). The wraparound might also slip down and encircle the body of the stom- ach, causing a partial obstruction. If the wraparound is sutured to the esoph- ageal wall, this complication is pre- vented unless the sutures pull out of the esophageal wall.
If sutures are taken in the esophageal wall and then pull out, either blcdding or fistulas may result, and reoperation may be needed. It is also possible for the sutures to pull out of the stomach and for a partial or complete disruption of the plication to occur (Fig 4). If a disrup- tion occurs, reflux may reoccur or the wrap may slip down, causing an ob- struction.
A less frequent but possible complica- tion of the surgical repair is intussus- ception of the gastric mucosa into the esophagus.” Other postoperative com-
40 AORN Journal, July 1981, Val 34, No 1

plications include wound infection, phlebitis, pulmonary embolis, pancrea- titis, atelectasis, dysphagia, esophageal perforation, gastric dilation, and fistula formation.12
Postoperatiue nursing care. General aspects of care need to be addressed for any postoperative patient following gastrointestinal surgery. These are identified in the postoperative stan- dards in Table 2. The patient with a Nissen fundoplication will have added needs and require extra attention to certain of these general areas.
Although ventilation is extremely important to any postoperative patient, this patient will need closer adherence to the ventilatory regimen. Good sup- port for the incision during coughing minimizes stress on the incision. Medi- cation should be given in sufficient amounts to relieve the pain associated with coughing but not in sufficient
amounts to depress coughing or deep breathing.
Smoking should not be allowed for at least a week following surgery to provide maximum pulmonary function- ing. Hydration must also be maintained so the secretions will remain as liquid as possible. If positive pressure treatments are used, they must be followed by supervised coughing; otherwise the ef- fects are minimized.
The patient with a Nissen procedure will probably have a nasogastric tube in place for two or three days following surgery. During this time, special mouth hygiene must be maintained. Patency of the tube must also be en- sured to prevent pressure on the suture line. The tube must be properly an- chored to prevent it from becoming dis- lodged. If it is dislodged, the physician should replace it to avoid esophageal perforation at the site of the plication.
Fig 3 (left). A patulous complication of Nissen fundoplication. There is an inadequate barrier to reflux, indicated by the arrow.
Fig 4 (right). fn this surgical complication, there has been total disruption of the plication suture line.
Reprinted with permission from Louis D Hill et al, “Reoperation for disruption and recurrence after Nissen fundoplication,” Archives of Surgery 114 (April 1979) 543. Copyright with American Medical Association.
AORN Journal, July 1981. Vol34. No 1 41

~~
Table 2
Nursing care standards for postoperative patients
Problems Expected outcomes Deadline Nursing orders
Potential shock (anesthesia or hemorrhage)
Potential ventilatory complications (hypostatic pneumonia or pulmonary emboli)
Pain in incision site
Potential nausea and vomiting
a. Blood pressure stable
b. Pulse between 60 and 100
c. No blood-saturated dressing or linen
d. No bright red bleeding in gastrointestinal tube
a. No obvious respiratory congestion
b. Normal respiratory pattern
c. Normal temperature (under 100 F)
d. Normal pCOn and PO2
a. Free of incisional pain most of the time
a. Take and tolerate 500 to 600 cc oral fluids without nausea, vomiting, or discomfort per 8 hrs (unless contraindicated)
12 hrs postoperatively
Seventh postoperative day
Sixth postoperative day
Third to fourth postoperative day
a. Take temperature, pulse, respiration, and blood pressure every 2 hours for 12 hours; then every4 hours for 36 hours.
b. Check dressings and tubes with vital signs. Note color and amount of drainage.
c. If shock occurs: 1. call physician 2. start oxygen if air hunger
apparent 3. get intravenous (IV)
setup ready (1,000 cc lactated Ringer’s).
a. Cough and deep breathe x 10 every hour for 72 hours.
b. Ambulate at least tid, beginning second postoperative day unless contraindicated.
c. Check pCOn and pOe level on laboratory test.
d. Note quantity and characteristics of sputum.
a. Assess and give pain medication every 3 to 4 hrs for first 72 hrs unless contraindicated.
a. Start with sips of fluid. Gradually increase amounts.
b. Give antiemetic medication as prescribed. If nausea persists through second postoperative day, notify physician.
c. Obtain order for IVs if not tolerating oral fluids.
d. Record toleration of 500 to 600 cc oral fluids per 8 hrs when oral fluids permitted.
e. Check for nausea, vomiting, distention, or discomfort and record for 72 hrs.
42 AORN Journal, July 1981, Vol34, No 1

5.
6.
7.
8.
9.
Potential oliguria or bladder distention
Potential fainting due to postural hypotension
Potential infection of a. incision and
drains b. bladder
Potential paralytic ileus, distention, and gas pains
Potential throat irritation due to intubation during surgery
a. Decreased urinary output
b. Normal urine output (1,20Occ/24 hrs) and no distention
a. No falls when ambulatory No dizziness when UP
a. Clean wound No separation No purulent drainage Temperature below 99.6 F
b. No dysuria No frequency
a. Abdomen soft to palpation Passing gas Evacuating bowels per regular routine
a. Swallowing without difficulty No complaints of sore throat
Second to third postoperative day By sixth postoperative day
12 to 24 hrs postoperatively
Third to seventh postoperative days
Fourth to fifth postoperative day
First to second postoperative day
a. Record input and output every 8 hrs x 48 hrs.
b. Try alternative means to void before catheterizing.
c. Catheterize if ordered as needed. 1. Clamp catheter to allow
distention before removing.
a. Change from flat to vertical
b. Have patient deep breathe
c. Assist when up as long as
position slowly.
prior to getting up.
faintness persists.
a. Use aseptic techniques when changing dressing. Inspect operative area at time of each dressing change for signs of wound separation and drainage. Adequate nutrition Take temperature every 8 hrs.
b. Hydration at least 500 to 600 cc every 8 hrs Teach hygiene of urinary tract. Check color of urine.
a. Keep active in bed or ambulating.
b. Check for passing flatus every 8 hrs x 72 hrs.
c. Checkdaily and record each bowel movement (expect to start fourth postoperative day).
distention every 8 hrs for 72 hrs. Position patient to facilitate expulsion of gas.
e. Get order for enema or laxative if no bowel movement after 4 days.
f. Record abdominal fullness, distress, or nausea.
d. Check abdomen for
a. Explain reason for sore throat.
b. Offer fluids unless contraindicated.
c. Gargle with mouthwash or salt water as needed.
AORN Journal, July 1981, Vol34, No 1 43

10. Thrombophlebitis
11. Potential concerns regarding going home, changes in self, job, family, and work due to surgery
12. Potential complications due to lack of information
a. No calf tenderness or pain No leg edema Pulses equal quality No temperature elevation
a. Can verbalize instructions and concerns regarding - activity - incision care - elimination - medications - restrictions on
travel - stairs - lifting - returning to work,
school, and driving
- nutrition - signs and
symptoms indicating need for medical follow-up
a. Verbalizes correct information
Fifth to seventh postoperative day
Fifth to seventh postoperative day (at least two days before discharge)
One to two days before discharge
d. Obtain order for medication if sore throat persists.
e . Routine mouth care every 8 hrs until hydration is adequate.
a. Leg exercise in bed 10 x every 2 hrs.
b. Ambulate 9id c. Antiemboli stockings d. Do not gatch knee of bed. e. Do not let patient sit with
legs dependent or crossed for any period of time.
a. Review patient's normal
b. Refer to community
c. Follow educational
d. Determine patient's
lifestyle.
resources.
programs (eg, ostomy).
understanding of prescribed regimen.
perception of barriers and benefits of instructions.
e. Determine patient's
a. Explore with patient understanding of discharge plan, including: -supplies - changes in lifestyle - any assistance needed -what signs and
symptoms of complications to report
-when to return to physician.
44 AORN Journal, July 1981, Vol34 , No 1

Oral intake will be limited to fluids until the tube is removed. Prior to re- moval of the tube, the patient’s toler- ance of fluids should be tested by clamp- ing the tube for intervals following in- gestion.
After removal of the tube, oral intake will gradually increase to a regular diet except for carbonated beverages and foods that are gas producing for that individual. Meals will have to be smal- ler and possibly more frequent than be- fore surgery, because the stomach‘s food storage area, the fundus, is no longer available. The patient should be in- structed to eat slowly, decreasing aero- phagia. Use of straws should be avoided because they increase the amount of air swallowed. It is advisable that the pa- tient not assume a recumbent position for several hours after eating and avoid physical activity that increases in- traabdominal pressure.
Nausea and vomiting occur in 30% to 4W of all postoperative patients. These will not be problems as long as the nasogastric tube is in place and func- tioning. A major nursing responsibility is to ensure the patency of the tube. After the nasogastric tube is removed, increased tension on the stomach walls and distention of the lower esophagus associated with retching will strain the suture line, which could lead to its dis- ruption.
The “gas-bloat” syndrome is the most significant problem of the postoperative patient who has had a Nissen proce- dure.13 Since the procedure is a total wraparound, and the wrap serves as a valve that permits only one-way flow of contents, eructating and vomiting, which require a reverse flow, may be difficult. In some patients, the inability t o eructate causes problems. With proper instruction, most patients learn to decrease their aerophagia to the point where this is only a minor nuisance.14
Dysphagia is usual and generally
transitory postoperatively. If it persists, the plication may be stretched slightly by dilation with a bougie. In severe cases where no other relief can be found, reoperation may be necessary. This complication does not happen in the pli- cations tha t use the partial wrap- around, because reverse flow of contents can still take place.
Gas pains are a normal and expected, although unpleasant, problem for pa- tients who have undergone gastrointes- tinal surgery. Postoperatively, there is not only a decrease in general activity but an increase in aerophagia due to pain and apprehension. This is in addi- tion to already excessive aerophagia that a patient used to clear the esophagus preoperatively. Postopera- tively, there is difficulty removing the swallowed air as general peristalsis is now also decreased.
Motility returns first in the small in- testine within 24 hours. Motility next returns to the stomach in 24 to 48 hours, and then to the colon in three to five days.15 Nursing actions are important in minimizing this problem for the pa- tient. A supine position promotes small intestine contents to remain in the pyloric area and regurgitate into the stomach. The semi-Fowler’s or low- Fowler’s position promotes the passage of contents through the colon. The right lateral position also prompts the move- ment of contents through the stomach. Lying on the stomach or a side knee- chest position also promotes the passage of gas as flatus, because gas rises. Therefore, if the rectal area is elevated, expulsion of flatus may be easier. Am- bulating the patient early helps relieve gas as well as improves ventilation.
Special attention must be given to the wound and drain, if one is in place. The nurse should know about the wound- healing process and remember that the danger period for the suture line is the fourth to twelfth postoperative day. If
AORN Journal, July 1981, Vol34, No 1 45

retaining sutures will not remain after the regular sutures are removed, then every other suture or every third suture will be left when the others are removed at the end of the first postoperative week. Vertical incisions must be ob- served closely for dehiscence.
If a drain is in place, it will probably be in a stab wound separate from the incision. Drains should be advanced a few centimeters daily, allowing time for the tract to fill in without an open sinus forming behind it. The drain should be kept free from organisms and secured so it does not slip into the abdomen. The dressing around the drain should be kept dry.
The educational aspects of care for this, or any, patient undergoing surgery are of the utmost importance. Not only is there new information to be given but misinformation to be corrected. While the major aspects of care for the patient with a Nissen fundoplication have been covered, the general preoperative and postoperative aspects of care have only been briefly discussed.
In view of the high incidence of hiatus hernia and the number of surgical pro- cedures being done, the OR nurse needs to be familiar with the forms of treatment tried before surgery as well as preoperative and postoperative care. Advantages of the plication procedure are that there are no anatomic excisions or insertions of foreign substances. Per- sonal dietary modifications are mini- mal compared with preoperative dis- comfort. With understanding and com- ments such as these, the OR nurse rein- forces continuity of care and helps in- form the rest of the staff. These factors can increase patient confidence and satisfaction. 0 Notes
1. J Vansant, “Surgical management of hiatal hernia with esophageal reflux,” American Surgeon 44 (April 1978) 179-1 93.
2. L Hill, “Surgical management of hiatal her-
nia,” in Hernia, 2nd ed, L Nyhus, R Condon, eds. (Philadelphia: J B Lippincott, 1978) 693-721.
3. Vansant, “Surgical management,” 179-1 93; R E M Mokka et al, “Surgical treatment of axial hiatal hernia-reflux complex by Nissen fundoplication,” Acta Chirurgica Scandinavica 143 (1 977) 265-269.
4. Vansant, “Surgical management,” 179-1 93. 5. Hill, “Surgical management of hiatal hernia,”
6. M Rossetti, K Hell, “Sliding hiatus hernia: Fundoplication or Nissen repair,” in Hernia, 2nd ed, L Nyhus, R Condon, eds. (Philadelphia: J B Lippin-
693-721.
cott, 1978) 668-674. 7. Ibid, 668-674. 8. S Shirazi, ”Experiences with Nissen fundopli-
cation,” in Hernia, 2nd ed, L Nyhus, R Condon, eds. (Philadelphia: J B Lippincott, 1978) 678-681.
9. D M Rogers, J L Herrington, C Morton, “lnci- dental splenectomy associated with Nissen fundo- plication,” Annals of Surgery 191 (February 1980)
10. R Belsey, ”The Mark IV repair,” in Hernia, 2nd ed, L Nyhus, R Condon, eds. (Philadelphia: J B Lippincott, 1978) 682-689.
11. L Hill et al, ”Reoperation for disruption and recurrence after Nissen fundoplication,” Archives of Surgery 114 (April 1979) 542-547.
12. Vansant, “Surgical management,” 179-1 93; Belsey, ”The Mark IV repair,” 682-689.
13. Hill, “Reoperation for disruption and recur- rence,” 542-547; Woodward, “Sliding hiatus her- nia,” 675-677.
14. E Dilling et al, “Comparison of Nissen fundo- plication and Belsey Mark IV in the management of gastroesophageal reflux,” American Journal of Surgery 134 (December 1977) 730-733.
15. M M Nachlas et al, “Gastrointestinal motility studies as a guide to postoperative management,” Annals of Surgery 175 (April 1972) 510-522).
Suggested reading Cooper, J D, et al. “lntraoperative and postoperative
esophageal manometric findings with Collis gas- troplasty and Belsey hiatal hernia repair for gas- troesophageal reflux.” The Journal of Thoracic and Cardiovascular Surgery 74 (November 1977)
Given, B; Simmons, S. Gastroenterology in Clinicai Nursing, 3rd ed. St Louis: C V Mosby, 1979.
Singh, S V. “Present concept of the Belsey Mark IV procedure in gastro-oesophageal reflux and hiatus hernia.” British Journal of Surgery 67
Urschel, H; Razzuk, M. “‘Collis-Belsey’ fundoplica- tion for uncomplicated hiatal hernia and gas- troesophageal reflux.” Annals of Thoracic Surgery 27 (June 1979) 564-566.
153-1 56.
744-751.
(1980) 26-28.
46 AORN Journal, July 1981, Vol34, No 1