Embed Size (px)
Citation preview
ORAL SURGERYIPAIN CONTROL LEGEND
Major Topic Abbreviation
Adrenal cortex Adren CortAnatomy AnatAnesthesia AnesthBiopsy BiopsyDisorders/Conditions Disord/CondDrugs DrugsExodontia ExoFractures FracturesGeneral Information Gen InfoImplants/Grafts Impl/GrftsMiscellaneous Misc.TMJ TMJ
Copyright (!;)2001 - DENTAL DECKS
FracturesORAL SURGERY/PAIN CONTROL
The treatment of a mandibular fracture using only intermaxillary fixat ion (IMF) iscalled:
• Open reduction• Closed reduction
Copyright © 2001 - DENTAL DECKS
• Closed reduction
" ' It is called closed reduction because it does not Involve direct opening, exposure, and manipulation of the fractured area.
Forms of immobili zati on of a fracture :1. A barton bandage is the simplest form of immobilization. Primarily a f irst aid measure
until definitive therapy can be instituted.2. Intermaxi llary fixation (IMF) is establishing a proper occlusal relationship by wiring the
teeth together. This method will successfully treat most fractures of the mandible. Themain methods for such fixation are wiring, arch bars, and splints. This is the classical wayto Immobilize the fracture after closed reduction.
3. External skeletal fixation is used in most cases in which the management of a fracturedbone segment is not satisfactorily accomplished by intermaxillary fixation. It involves theplacement of screws or pins through the skin on each side of the fracture and a cold cureacrylic bar which holds the screws in proper relationship with the fracture in the reduced position. It is cumbersome and esthetically displeasing.
4. Direct intraosseous wiring combined with a period of IMF is the traditional method of bonestabilization after open reduction . This method of stabilization can be accomplished througha variety of different wiring techniques. The wire is placed through holes on either side of thefracture and immobilization is accomplished by tightening the wires.
FracturesORAL SURGERYIPAIN CONTROL
Zygomatic arch fractures can be nicely demonstrated by which radiographic view?
• Water 's view• Lateral skull view• Posteroanterior skull view• Submental vertex view
Copyright © 2001 - DENTAL DECKS
• Subment&yerfex view
This type of fracture may not cause any problem other than perhaps a slight sinking ofthe cheekbone area. There may be some encroachment and impairment in closure ofthe jaw if it comes down and entraps the coronoid process of the mandible.
Possible complications include:• Paresthesia (most common) - usually subsides• The antrum (sinus) may be filled with a hematoma, which usually evacuates itself• Ocular muscle balance may be impaired because of fracture of the orbital process
Important: Fractures of the facial bones, particularly the zygomatic complex mayon rare occasions be complicated by damage to the contents of the superior orbitalfissure.
Note: Fracture of the infraorbital rim presents with the following symptoms:• Numbness of the following areas on the affected side: upper lip, cheek, and nose.
Remember: The Water's view is best to evaluate orbital rim areas. ....
FracturesORAL SURGERYIPAIN CONTROL
Which of the following is the most common pathognomonic sign of a mandibularfracture?
• Nasal bleeding• Exophthalmos• Malocclusion• Numbness in the infraorbital nerve distribution
Copyright © 2001 - DENTAL DECKS
• Malocclusion
Other signs and symptons of a mandibular body or angle fracture include:• Lower lip numbness• Mobility, pain, or bleed ing at the fracture site
Anatomic distribution of mandibular fractures:• Angle (30%) most common site• Condylar neck (25%)• Symphys is area (22%)• Body (17%)• Ramus (2%)• Coronoid process (1%) least common site
Notes:1. Indications for open reduction include continued gross displacement of the bony segments
and an unfavorable fracture that is likely to result in further displacement of the fractured segments caused by muscle pull, This type of reduct ion is commonly performed for displacedangle or body fractures. Remember: Condylar neck fractures are usually treated by closedreduction .
2. In a fracture involving the angle of an edentulous mandible, the proximal segment is usually displaced anteriorly and super iorly.
FracturesORAL SURGERYIPAIN CONTROL
In patients who have a LeFort II fracture, a common finding is paresthesia over thedistribution of the:
• Infraorbital nerve• Inferior alveolar nerve• Mylohyoid nerve• Hypoglossal nerve
Copyright © 2001 - DENTAL DECKS
• Infraorbital nerve
Midfacial fractures include fractures affecting the maxilla, the zygoma, and the nasoorbital ethmoid complex. Midfacial fractures can be classified as:• LeFort I (also called a horizontal fracture) is a horizontal segmented fracture of the alveolar
process of the maxilla, in which the teeth are usually contained in the detached portion of thebone. Result is an open bite.
• LeFort II (also called a pyramidal fracture) is a unilateral or bilateral fracture of the maxilla, inwhich the body of the maxilla is separated from the facial skeleton and the separated portionis pyramidal in shape. Signs include periorbital edema, ecchymosis, subconjunctivalhemorrhage, and nose bleeding.
• LeFort III (also called a transverse fracture or craniofacial dysfunction) is a fracture in whichthe entire maxilla and one or more facial bones are completely separated from the craniofacial skeleton. These patients will have restriction of mandibular movement.
• Also zygomaticomaxillary complex fractures, zygomatic arch fractures, or nasoorbital eth-moid fractures.
Important: The first step in the treatment of these fractures which affect the occlusal relationshipis similar to the treatment of mandibular fractures - to reestablish a proper occlusal relationshipby placing the maxilla into proper occlusion with the mandible.
Note: Due to the slope of the sphenoid bone comprising the floor of the cranial vault, blows tothe maxilla will cause the maxilla to be driven backwards and downwards. This may result inan open bite or Impingement of the airway.
FracturesORAL SURGERY/PAIN CONTROL
All of the following are weak points in the mandible where fractures are most common except
• The angle• The coronoid process• The condylar neck• The symphysis area
Copyright © 2001 - DENTAL DECKS
• The coronoid process
The location and extent of mandibular fractures are determined largely by the direction and intensity of the blow and the specific points of weakness in the mandible.
The angle is the most common anatomic site of fracture of the mandible (30% of fractures). Frequently third molars which are impacted are located in this region and furtheradd to the weakness of the mandible in this area.
The condylar neck (25% of fractures) is a safety feature which allows a blow to thejaw to be dispersed at this point rather than driving the condyle into the middle cranialfossa. Bilateral dislocated fractures of the condylar necks will cause an anterior openbite and the inability to protrude the mandible. A unilateral fracture through the neckmay cause forward displacement of the head of the condyle due to pull of the lateralpterygoid muscle.
The symphysis area or chin (22% of fractures) is usually where blows are sustained.These blows often result in fractures of the subcondylar region. Remember: Thepatient's mandible will deviate to side of injury upon opening.
FracturesORAL SURGERYIPAIN CONTROL
Which form of reduction listed below is best used to reduce a fracture when teeth aremissing in one or more of the fractured segments?
• Open reduction• Closed reduction
Copyright © 2001 - DENTAL DECKS
• Open reduction
Open reduction is the reduction of a fractured bone by manipulation after incisioninto skin and muscle over the site of the fracture. The most common site for openreduction is at the angle of the mandible. Once the incision is made, an intraosseouswire is placed through holes made on either side of the fracture. Reduction is accomplished under direct vision, and immobilization is obtained by tightening the wires. Thisprocedure is usually reserved for fractures that cannot be reduced and immobilizedadequately by closed methods.
Closed reduction is the reduction of a fractured bone by manipulation without incision into the skin. It is the simplest method of reduction and is used most frequentlywhen both fractured segments contain teeth. After manipulation of the bone, it is usually maintained in place by intermaxillary fixation (lMF).
Remember: IMF is fixation obtained by applying wires or elastic bands between theupper and lower jaws in which suitable anchoring devices have been attached. Themost common technique for IMF is the use of prefabricated arch bars.
FracturesORAL SURGERY/PAIN CONTROL
Which of the following are likely signs and symptoms of a zygomatic fracture?
• Nasal bleeding• Pain over zygomatic region• Numbness in the infratemporal nerve distribution• Exophtalmos• Diplopia• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
Midfacial fractures include fractures affecting the maxilla, the zygoma, and thenasoorbital ethmoid complex. They may be classified as:• LeFort I, II, or III fractures• Zygomatic complex fractures (most common type of midfacial fracture)• Zygomatic arch fractures• Nasoorbital ethmoid fractures---The following radiographic views are often helpful to evaluate midfacial fractures:Water's view PAskull view, and submental vertex view.-Important: A zygomatic arch fracture can impinge on the coronoid process or temporalls muscle, causing various degrees of trismus.
Notes:1. The maxilla and mandible are in a critical relationship to the upper airway; therefore
displacement of fractures can cause obstruction of the airway resulting in respiratoryarrest. Control of airway is vital to any treatment of a patient with facial fractures.
2. Maxillary fractures have a greater tendency towards the production of facial deformity than do mandibular fractures.
ORAL SURGERY/PAIN CONTROLFractures
Which muscle below is responsible for the forward displacement of the condylarhead when the neck of the condyle is fractured?
• Masseter muscle• Mylohyoid muscle• Lateral pterygoid muscle• Medial pterygoid muscle
Copyright © 2001 - DENTAL DECKS
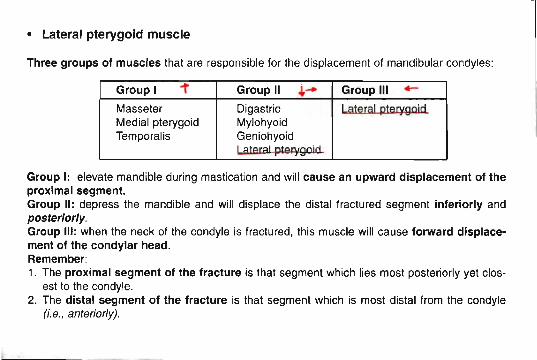
• Lateral pterygoid muscle
Three groups of muscles that are responsible for the displacement of mandibular condyles:
Group I -r Group II +- Group III 4-
Masseter Digastric Lateral pterygoidMedial pterygoid MylohyoidTemporalis Geniohyoid
I alem! pterygoid
Group I: elevate mandible during mastication and will cause an upward displacement of theproximal segment.Group II: depress the mandible and will displace the distal fractured segment inferiorly andposteriorly.Group III: when the neck of the condyle is fractured, this muscle will cause forward displacement of the condylar head.Remember:1. The proximal segment of the fracture is that segment which lies most posteriorly yet clos
est to the condyle.2. The distal segment of the fracture is that segment which is most distal from the condyle
(i.e.• anteriorly).
ExoORAL SURGERY/PAIN CONTROL
The most severe tissue reaction is seen with which type of suture material?
• Plain catgut• Chromic catgut• Polyglycolic acid• Polyglactin 910
Copyrig ht © 2001 - DENTAL DECKS
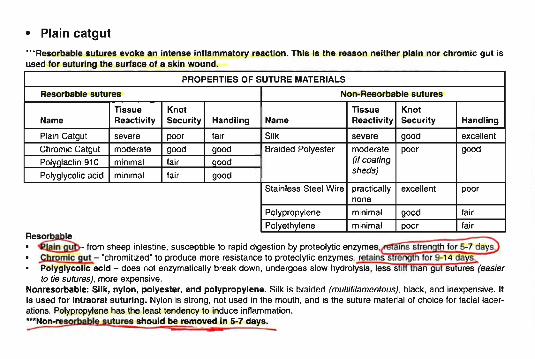
• Plain catgut
"""Resorbabl e sutures evoke an intense inf lammatory reacti on. Th is Is the reason neither plain nor chromic gut isused for suturing the surface of a skin wound.
PROPERTIES OF SUTURE MATERIALS
Resorbable sutu res Non -Resorbable sutures
TIssue Knot Tissue KnotName React iv ity secu rity Handling Name Reactiv ity Security Hand ling
Plain Catgut severe poor fair Silk severe good excellent
Chromic Catgut moderate good good Braided Polyester moderate poor good
Polvolactin 910 minimal fair oood (if coating
Polyglycol ic acid minimal fair goodsheds)
Stain less Steel Wire pract ically excellent poornone
Polypropylene minimal good fair
Polyethylene minimal poor fairRes~
•~ from sheep intestine. susceptible to rapid digestion by proteolytic enzymes,~ns strength for 5-7 dayi>• Chromic gut - "chromitized" to produce more resistance to proteolytic enzyme s. retains s rength for 9-14 daY§.,.• Polyglycolic ac id - does not enzymatically break down , undergoes slow hydrolysis, less sbfl than gut sutures (easier
to tie sutures), more expensive.Nonresorbable: Silk, nylon, polyester, and polypropylene. Silk is bra ided (multifitamentous) , black , and inexpensive . Itis used for Int raoral suturing. Nylon is strong, not used In the mouth , and is the suture material of choice for facial lacerations. Polypropylene has the least tendency to induce inflammation.~able sutures should be removed In 5-7 days..:-,
ORAL SURGERYIPAIN CONTROL
The most frequent location for a maxillary torus is:
• The right side of the hard palate• The left side of the hard palate• The midline of the hard palate• On the soft palate
Copyright © 2001 - DENTAL DECKS
Exo
• The midline of the hard palate
Here it is called the torus palatinus. They usually appear before the age of 30 andaffect females more frequently than males.
Maxillary tori present few problems when the maxillary dentition is present and onlyoccasionally interfere with speech or become ulcerated from frequent trauma to thepalate.
Indications for removal include a large, lobulated torus with a thin, mucoperiostealcover extending posteriorly to the vibrating line of the palate that prevents seating ofa denture and also prevents a posterior seal at the fovea palatini.
Technique for removal:• The maxillary torus should not be excised en masse to prevent entry into the
nose (the palatine bone will come out with torus).• It should be subdivided into segments by a bur.• The segments are then removed with an osteotome.• Any protuberances are smoothed out with a bone file .• The flap is loosely sutured.• A palatal splint is placed to prevent hematoma formation and to support the flap.
ExoORAL SURGERY/PAIN CONTROL
When removing maxillary teeth, the upper jaw of the patient should be where in relation to the dentist's shoulder?
• Below• Above• At the same height• It makes no difference where the patient's upper jaw is in relation to the dentist's
shoulder
Copyright © 2001 - DENTAL DECKS
• At the same height
For mandibular extractions, the patient should be positioned so that the occlusalplane of the mandibular arch is parallel to the floor when the mouth is opened. Thechair should be as low as possible.
Positioning of the surgeon: When extracting maxillary teeth, it is usually best tostand in front of and to the side of the patient for maximum visibility and leverage.When extracting mandibular teeth, it is often better to stand directly to the side orbehind the patient.
The fingers of the left hand (for a right-handed dentist) serve to:• Retract the soft tissue.• Provide the operator with sensory stimuli for the detection of expansion of the alve-
olar plate and root movement under the plate.• Help guide the forceps into place on the tooth.• Protect teeth in the opposite jaw from accidental contact with the back of the forceps.• Support the mandible while performing mandibular extractions.
ExoORAL SURGERY/PAIN CONTROL
Which type of maxillary third molar impaction is most likely to be displaced into theantrum (maxillary sinus) and infratemporal space if correct extraction techniques arenot employed?
• Vertical impaction• Distoangular impaction• Mesioangular impaction• Horizontal impaction
Copyright e 2001 - DENTAL DECKS
• Distoangular impaction
Impacted maxillary third molars are occasionally displaced into two areas:• Maxillary sinus (antrum) - from which they are removed via a Caldwell-Luc
approach• Infratemporal space - during elevation of the tooth the elevator may force the tooth
posteriorly through the periosteum into the infratemporal fossa. If access and lightare good, the tooth may be retrieved with a hemostat. If the tooth is not retrievedafter a short amount of time, the area should be closed. The patient should beinformed that the tooth has been displaced and will be removed by an oral surgeonwho will use a special technique to remove it.
ExoORAL SURGERY/PAIN CONTROL
Which of the following is the main reason to use water irrigat ion when cutting bone?
• It helps to wash away debris• Because heat generated by the drill affects bone vitality• To decrease the smell of freshly cut bone• It helps to flush out the highspeed suct ion hose
Copyright © 2001 - DENTAL DECKS
• Because heat generated by the drill affects bone vitality
Irrigation of the surgical wound during and after the procedure cannot be emphasized enough. Copious amounts of coolant spray are crucial in minimizing osseousnecrosis caused by heat generated from the bur. Irrigation serves also to cleanse thecrypt and areas beneath the flap of bony debris, tooth fragments, and blood.
ExoORAL SURGERY/PAIN CONTROL
Which sca lpe l below is universally used for oral surgical procedures?
• No.2 blade• No.6 blade• No. 10 blade• No. 15 blade
Copyright @ 2001 - DENTAL DECKS
• No. 15 blade
Three types of incisions used in oral surgery :1. Linear - straight line incision used for apicoectomies2. Releasing - used when adding a vertical leg to a horizontal incision. For extrac
tions, augmentations, etc.3. Semi-lunar - curved incision mostly used for apicoectomies
The basic principles of oral surgical flap design:• Flap design should ensure adequate blood supply ; the base of the flap should be
larger than the apex.• Reflection of the flap should adequately expose the operative field.• Flap design should permit atraumatic closure of the wounds.
Important: The correct position for ending a vertical releasing incision is at a tooth lineangle not over the buccal surface of a tooth. If it ends over the buccal surface, theedges are difficult to approximate and this may lead to periodontal problems.
ORAL SURGERY/PAIN CONTROLExo
Which of the following are local contraindications for tooth extractions?
• ANUG• Irradiated jaws• Malignant disease• All of the above
Copyright © 2001 - DENTAL DECKS
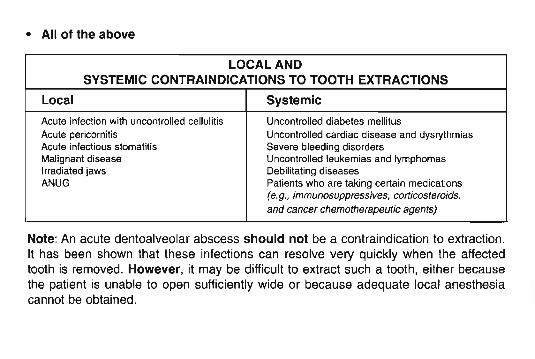
• All of the above
LOCAL ANDSYSTEMIC CONTRAINDICATIONS TO TOOTH EXTRACTIONS
Local Systemic
Acute infection with uncontrolled cellulitis Uncontrolled diabetes mellitusAcute pericornitis Uncontrolled cardiac disease and dysrythmiasAcute infectious stomat itis Severe bleeding disordersMalignant disease Uncontrolled leukemias and lymphomasIrradiated jaws Debilitating diseasesANUG Patients who are taking certa in medications
(e.g., immunosuppress ives, corticostero ids,
and cancer chemotherapeutic agents)
Note: An acute dentoalveolar abscess should not be a contraindication to extraction.It has been shown that these infections can resolve very quickly when the affectedtooth is removed. However, it may be difficult to extract such a tooth, either becausethe patient is unable to open sufficiently wide or because adequate local anesthesiacannot be obtained.
ORAL SURGERYIPAIN CONTROLExo
Which suture pattern (or method) listed below is most commonly used in oral surgery?
• Continuous pattern• Interrupted pattern
Copyright © 2001 - DENTAL DECKS
• Interrupted pattern
This suture pattern or method offers strength and flexibility due to each suture beingindependent to one another. If one suture is lost or becomes loose, the integrity of theremaining sutures is not compromised. The major disadvantage is the time requiredfor placement.
Advantages of a continuous pattern or method:• Ease and speed of placement• Distribution of tension over the whole suture line• A more watertight closure than the interrupted pattern or method
Note:1. Sutures should not be overtightened or closed under tension.2. Sutures should be 2-3 mm apart, placed from mobile tissue to fixed fiSSile and from
thin tissue to thick tissue. -
ORAL SURGERY/PAIN CONTROLExo
Which of the following is the primary direction of luxation for extracting maxillarydeciduous molars?
• Buccal• Palatal• Mesial• Distal
Copyright © 2001 - DENTAL DECKS
• Palatal*** As opposed to the buccal direction in adults. This is because the deciduousmolars are more palatally positioned and the palatal root is strong and less prone tofracture.
In general, the removal of deciduous teeth is not difficult. It is facilitated by the elasticity of young bone and the resorption of the root structure. Do not use the "cowhorn"forceps for extraction of lower primary molars because the sharp beaks of these forceps could cause damage to the unerupted permanent premolar teeth.
Notes:1. If the preoperative radiograph shows that the permanent premolar is wedged
tightly between the bell-shaped roots of the primary tooth, the best treatment is tosection the crown of the primary molar and remove the two portions separately. Thiswill help in not disturbing the permanent tooth.
2. After extraction of mandibular teeth on a child in which a mandibular block wasgiven, always advise child not to bite on lip while he or she is numb. Inform parentsas well to watch child so this does not occur.
ORAL SURGERY/PAIN CONTROL
Dead space in a wound usually fills with:
• Pus• Water• Blood• Tissue
Copyright © 2001 - DENTAL DECKS
Exo
• Blood
Dead space in a wound is any area that remains devoid of tissue after closure of thewound. It is created by either removing tissues in the depths of a wound or by not reapproximating tissue planes during closu re. Dead space in a wound usually fills withblood which creates a hematoma with a high potent ial for infection.
Ways in which you can eliminate dead space :• Close the wound in layers to minimize the postoperative void.• Apply pressure dressings• Use drains to remove any bleeding that accumulates.• Place packing into the void until bleeding has stopped.
ORAL SURGERY/PAIN CONTROL
When would you place a suture over a single extraction socket?
Exo
• Routinely• Never• If the patient requests it• When there is severe bleeding from the gingiva or if the gingival cuff is torn or loose.
Copyright © 2001 - DENTAL DECKS
• When there is severe bleeding from the gingiva or if the gingival cuff is torn orloose
Normal post-extraction procedure:• All loose bone spicules and portions of the tooth, restoration, or calculus are removed from
the socket as well as from the buccal and lingual gutters and the tongue.• The socket must be compressed by the fin gers to reestablish the normal width present
before the buccal plate was surgically expanded. Note : The natural recontouring of the residual ridge occurs primarily by resorption of the labial-buccal cortical bone.
• Sutures are usually not placed unless the papillae have been excised.• The socket is covered with a gauze sponge that has been folded and moistened slightly at its
center with cold water.• The patient is instructed to bite down for 5-10 minutes• Remove this sponge and place another one. This should stay in place until the patient arrives
home.• A printed instruction sheet is given to the patient.• A prescription for pain is given if the need is anticipated.
If bleeding persists for some time following an extraction, it may be helpful to instruct thepatient to bite on a tea bag. The tannic acid in the tea bag will help promote hemostasis.
Remember :The most common cause of post-extraction bleeding is the failure of the patientto follow post-extraction instructions.
ORAL SURGERY/PAIN CONTROL
A patient with dry socket develops a severe dull throbbing pain:
• Two to three hours following a tooth extraction• One day following a tooth extraction• Two to four days following a tooth extraction• Immediately following a tooth extraction
Copyright © 2001 - DENTAL DECKS
Exo
• Two to four days following a tooth extraction
Th'e pain is often excruciating. may radiate to the ear, and is not relieved by oral analgesics.There may be an associated foul odor and taste. T!Jg.extraction site is filled with necrotic tissue.which is delaying wound healing.
Dry socket results from a pathologic process combining the loss of the healing blood clot with alocalized inflammation. It is most common following extraction of the mandibular molars.Smoking, spitting or drinking through a straw, which creates negative pressure in the oral cavity,may encourage this condition. Note: Careful technique and minimal trauma reduce the frequency of patients developing dry socket.
Treatment:• Flush out debris with saline solution (gent/y).• Carefully dry socket.• Place strip of iodoform gauze soaked in oil of cloves (eugenol). Note: The gauze provides
and attachment for the obtundent paste so it stays in the socket.• Prescribe analgesic drugs if necessary.
Note: Dry socket is the most common complication seen after the surgical removal of amandibular molar. Tetracycline is sometimes given prophylactically following the removal ofimpacted mandibular third molars to prevent dry socket. Dry socket is also referred to as postextraction alveolitis or localized alveolar osteitis.
ORAL SURGERYIPAIN CONTROL
The ideal time to remove impacted third molars is:
• When the root is fully formed• When the root is approximately two-thirds formed• Makes no difference how much of the root is formed• When the root is approximately one-third formed
Copyright © 2001 - DENTAL DECKS
Exo
• When the root is approximately two-thirds formed
- Patient would be around the age of 17-21.- At this time, the bone is more flexible and the roots are not formed well enough
to have developed curves and rarely fracture during extraction.
When the root is fully formed, the possibility increases for abnormal root morphology and for fracture of the root tips during extraction .
If the root development is insufficient (one-third or less), the tooth is more difficult toremove because it tends to roll in its crypt like a ball in a socket , which prevents easyelevation.
Notes:1. Patients who are young tolerate surgery very well. Postoperative complicat ions
are usually minimal.2. Older individuals have the most postoperative difficulties. The bone is more
dense and usually the patient responds more slowly to the entire process (anesthesia and surgery).
ORAL SURGERY/PAIN CONTROL
The mesioangular impaction is generally acknowledged as:
• The most difficult impaction to remove• The least difficult impaction to remove• Neither of the above
Copyright © 2001 - DENTAL DECKS
Exo
• The least difficult impaction to remove
···The mesioangular impaction is also the most common and comprises about 43% of allimpacted teeth.
For impacted mand ibu lar third molars the mesioangular is the least difficult to remove followed by the horizontal, vertical, and the most difficult to remove is the distoangularimpaction. Important: This is the exact opposite of impacted maxillary third molars, where themesioangular impactions are the most difficult and the vertical and distoangular impactions arethe easiest to remove.
Once sufficient amounts of bone have been removed from around the impacted tooth, thetooth is usually sectioned. Sectioning allows portions of the tooth to be removed separately withelevators through the opening provided by bone removal. Note: Bone is rarely, if ever, removedon the lingual aspect of the mandible because of the likelihood of damaging the lingualnerve.
Section ing of the tooth is done for the following reasons:• Allows for minimal bone removal• Allows for minimal force needed to remove tooth• Shortens the entire surgical procedure
Tooth sectioning can be performed with either a bur or chisel; however, the bur is used bymost surgeons.
Misc.ORAL SURGERY/PAIN CONTROL
Squamous cell carcinoma is most easily managed when found where?
• Floor of the mouth• Palate• Lower lip• Side of the tongue
Copyright © 2001 - DENTAL DECKS
• Lower lip
Squamous cell carcinoma (SCC) is the most common malignant oral tumor, representing a little over 90% of all oral malignancies. It is 9 to 10 times more frequent inmales than in females and, although seen in all ages, its highest incidence is after thefourth decade. It is more common on the lips than intraorally.
95% of lip carcinomas occur on the lower lip. They are usually discovered early andonly a small percentage show lymph node metastasis. Prognosis is very good.
SCC of the tongue is the most common intraoral malignancy. The most common location is the posterior lateral border, followed by the posterior one-third or base of thetongue. It is uncommon on the dorsum or tip of the tongue. These lesions usuallymetastasize early and the prognosis is not as good as lip lesions.
The floor of the mouth is the second most common intraoral location of sec. It isseen predominantly in older men, especially those who are chronic alcoholics andsmokers. These lesions metastasize early and the prognosis is very poor.
Remember: The treatment of choice for oral cancer is surgery.
ORAL SURGERY/PAIN CONTROLMisc.
All of the following are systemic contraind ications to elective surgery except
• Blood dyscras ias (i.e., hemophilia, leukemia)• Controlled diabetes mellitus• Addison's disease or any steroid deficiency• Fever of unexpla ined origin• Nephritis• Any debil itating disease• Cardiac disease
Copyright ~ 2001 - DENTAL DECKS
• Controlled diabetes mellitus
"'Uncontrolled diabetes mellitus is a systemic contraindication to elective surgery
Important: Patients with these systemic conditions can be treated, but you need toconsult with the patient's physician before treatment. In most cases, these patients arebest treated in the hospital by an oral surgeon.
Note: Cardiac disease such as coronary artery disease, uncontrolled hypertension,and cardiac decompensat ion can complicate exodontia. Usually a postinfarctionpatient is not subjected to oral surgery within six months of his infarction.However, emergency procedures can be performed provided the patient's physicianhas been consulted.
ORAL SURGERYIPAIN CONTROL
The most common site of a pericoronal infection (pericoronitis) is:
• Around the site of a recent extraction• Around a newly erupted primary tooth• Around periodontally involved mandibular incisors• Around mandibular third molars
Copyright © 2001 - DENTAL DECKS
Misc.
• Around mandibular third molars
The most typical symptoms of a pericoronal infection about the third molar are:• Submandibular lymphadenopathy• Trismus• Pain in the region of a mandibular third molar• Swollen, red tissue in the region of a mandibular third molar• General condition of malaise
Treatment includes:• Irrigate area• If possible, establ ish drainage• Place patient on antibiotics• Instruct patient to rinse with warm saline mouthwashes• As soon as the acute symptoms are relieved , a definitive treatment may be institut
ed
Important: The maxillary third molar is the most frequent contributing factor to pericoronal infections found around mandibular third molars. Always examine the maxillarythird molar, it may be supererupted or malaligned .
ORAL SURGERY/PAIN CONTROL
Which of the following can result in masticator space infections?
Misc.
• Infections of the mandibular molars, especially the third molar• Nonaseptic technique in local anesthesia of the inferior alveolar nerve• Trauma to the mandible (either external or fracture into the socket of a diseased
third molar)• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
The masseteric, pterygomandibular, and temporal spaces as a group are known asthe masticator space because they are bounded by the muscles and fascia of mastication. Infections of the masticator space are practically always of dental origin, particularly the lower molar region. Note: Needle tract infections following an inferior alveolar block injection would initially involve the pterygomandibular space.
Clinically, the picture of masticator space infection is dominated by trismus, pain, andswelling occurring within a few hours following a molar extraction or trauma to themandible. These signs increase rapidly to reach a peak in 3 to 7 days. Spontaneousintraoral drainage usually takes place between the 4th and 8th day. If this does notoccur, surgical drainage is indicated.
Notes :1. The most definite clinical sign indicating extension of an odontogenic infection into
the masticator space is trismus. Trismus is difficulty in opening the mouth due to atonic spasm of the muscles of mastication.
2. Trismus may also result from passing the needle through the medial pterygoid muscle during an inferior alveolar nerve block.
Misc.ORAL SURGERY/PAIN CONTROL
The mandibu lar left second molar of a 14 year-old boy is unerupted. Radiographs showa small dentigerous cyst surrounding the crown. What is the treatment of choice?
• Surgically extract the unerupted second molar• Uncover the crown and keep it exposed• Prescribe an anti-inflammatory medication and schedule a follow-up appointment in
six months• No treatment is necessary at this time
Copyright © 2001 - DENTAL DECKS
• Uncover the crown and keep it exposed
Dentigerous cysts are those associated with the crowns of unerupted teeth. Some literature refers to these cysts as "follicular" or "primordial" cysts. Note: They areprobably the result of degenerat ive changes in the reduced enamel epithelium.
Remember: If cysts form when a tooth is erupting, they are called eruption cysts.These cysts interfere with normal eruption of the teeth. Eruption cysts are more commonly found in the child and young adult and may be associated with any tooth. If treatment is indicated, simple incision or "deroofing" is all that is needed.
Misc.ORAL SURGERY/PAIN CONTROL
Which of the following statements are true concerning ecchymosis?
• Ecchymosis is an area of hemorrhage into the skin and subcutaneous tissue>1 cmin diameter
• An ecchymosis is often the result of injury; however, clott ing and bleeding disorderscan predispose to the formation of an ecchymosis
• Grossly, an ecchymosis presents as a bluish lesion at the earliest stages of onset• As the red blood cells in the lesion undergo progressive degeneration and the hemo
globin becomes converted through bilirubin into hemosiderin , the lesion progressively changes color from blue through green through purple to finally a brownish discolorat ion
• All of the above statements concerning ecchymosis are true
Copyright © 2001 - DENTAL DECKS
• All of the above statements concerning ecchymosis are true
Postoperative ecchymosis is a result of trauma to the underlying blood vessels.Blood escapes from the vascular tree and accumulates in the tissues. It is commonafter extractions in elderly patients due to the fragility of the vessel walls. All patientsshould be warned that it may occur following extractions. Note: Sometimes the patientwill complain of a diffuse, non-painful, yellowish discoloration of the skin. Moist heatoften speeds the resolution of postoperative ecchymosis.
Remember : Osteoradionecrosis is the most serious potential complication afterextractions from areas previously irradiated. It is the necrosis of bone caused by exposure to ionizing radiation.
ORAL SURGERY/PAIN CONTROLMisc.
Incision for drainage (I & 0) in an area of acute infection should only be performedafter which of the following has occurred?
• A culture for antibiotic sensitivity has been performed• Localization of the infection• A sinus tract is formed• All of the above
Copyright © 2001 - DENTAL DECKS
• Localization of the infection
Physiologically, it is at this time that nature has constructed a barrier around theabscess, walling it off from the circulation and making it possible to palpate the presence of purulent material within the abscess cavity (known as fluctuance) .
Note: After you incise and drain the fluctuant mass, it may be prudent to do a culturefor antibiotic sensitivity. This should always be done if after incision and drainage theswelling does not subside despite large doses of antibiotics.
Prior to actual abscess formation, however, the infection is capable of producing acellulitis in the soft tissues of the region involved. The palpable tissues take on a condition known as induration (they appear hard, dense, and brawny) . Treatment duringthis period should be directed towards localizing the infection. Early employment ofantibiotics may be extremely important in a severe and life-threatening infection.Localization of the infection may be aided by using warm compresses and warm mouthrinses at frequent intervals.
ORAL SURGERYIPAIN CONTROL
Cavernous sinus thrombosis can be caused by:
• An infection of the central face or paranasal sinuses• Bacteremia• Trauma• Infections of the ear or maxillary teeth• All of the above
Copyright © 2001 - DENTAL DECKS
Misc.
• All of the above
Cavernous sinus thrombosis (CST) is an unusual occurrence that is rarely the resultof an infected tooth. CST is generally a fulminant process with high rates of morbidityand mortality. Fortunately, the incidence of CST has been decreased greatly with theadvent of effective antibiotics. Most cases are due to an acute infection in an otherwisehealthy individual. However, patients with chronic sinusitis or diabetes mellitus may beat a slightly higher risk. Note: The causative agent is generally Staphylococcusaureus.
Infections of the face can cause a septic thrombosis of the cavernous sinus.Furunculosis and infected hair follicles in the nose are frequent causes. Extractions ofmaxillary anterior teeth in the presence of acute infection and especially curettage ofthe socket under such circumstances can cause this condition. The infected thrombusascends in the veins against the usual venous flow. It usually occurs in the ophthalmic vein. This is possible because of the absence of valves in the angular, facial,and ophthalmic veins.
L
Misc.ORAL SURGERY/PAIN CONTROL
Which of the following tests should be routinely performed in the preoperativeworkup for a patient that is being admitted to a hospital for surgery?
• A complete blood count (CSC)• A total white blood cell count• An assessment of the circulating platelets• A urinalysis• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
Routine admission tests include:
• A complete blood count that includes an evaluat ion of the hemoglobin and hema-tocrit indices
• A total white blood cell count with a differential count• An assessment of the circulating platelets• A gross and microscopic urinalysis
Anyone scheduled for general anesthesia should have a chest x-ray and patientsover 40 years old should also have an E.K.G.
Factors to be considered in the decision to hospitalize a patient for an elective procedure:• Medical problems compromising treatment (diabetes, hemophilia. etc.)• Difficulty and extent of surgery .• Considerat ion of the individual patient (emotionally disturbed, handicapped, etc.)• Cost of hospital ization (time and money)
Misc.ORAL SURGERY/PAIN CONTROL
By far and away the most commonly performed mandibular procedure for the correction of mandibular retrognathia is the:
• Segmental osteotomy• Sagitta l split osteotomy• Vertical ramus osteotomy• Body osteotomy
Copyright © 2001 - DENTAL DECKS
• Sagittal split osteotomy
***This is due primarily to its simplicity and versatility.
The mandible is split sagittally and can either be used to advance the mandible (in thecase ofretrognathia) or set back the mandible (in treating prognathia). It is the standard procedure used today. Note: The position of the condyle is unchanged duringcorrection of mandibular prognathism or retrognathism.
Vertical ramus osteotomy: Is used for the correction of prognathism. The objectiveis vertical sectioning of the ramus in a line from the lower aspect of the mandibularnotch vertically downward over the mandibular foramen or just posterior to the lowerborder of the mandible at the angle.
Body osteotomy: Is a procedure that involves extracting mandibular teeth bilaterally(usually bicuspids) . A piece of bone is also removed from the mandible and you slideeverything back. Used for prognathism.
Segmental osteotomy: Maxillary procedure where more than one segment of bone isremoved.
Note: A LeFort I osteotomy is most commonly used to correct maxillary retrognathia.
Misc.ORAL SURGERY/PAIN CONTROL
On physical examination, painless induration of soft tissue is suggestive of:
• Normal tissue• Infection• Invasive malignant lesions• Benign lesions
Copyright © 2001 - DENTAL DECKS
• Invasive malignant lesions
Characteristics of lesions that raise the suspicion of malignancy :
• Erythroplasia - lesion is totally red or speckled red and white• Ulceration - lesion is ulcerated or is an ulcer• Duration - more than two weeks• Rapid growth• Bleeding - bleeds on gentle manipulation• Induration - lesion and surrounding tissue is firm to the touch• Fixation - feels attached to adjacent structures
Misc.ORAL SURGERY/PAIN CONTROL
Muscle fibers covered by a mucous membrane that attaches the cheek, lips, and/ortongue to associated dental mucosa is called:
• Gingiva• Frenum• Operculum• Abutment
Copyright @ 2001 - DENTAL DECKS
• Frenum
When a frenum is positioned in such a way as to interfere with the normal alignmentof teeth or results in pulling away of the gingiva from the tooth surface causing recession it is often removed using a surgical process known as a frenectomy.
There are three surgical techniques that are used for a frenectomy:• Simple excision and Z-plasty are effective when the mucosal and fibrous tissue
band is relatively narrow. These techniques relax the pull of the frenum.• v-v plasty (sometimes called a localized vestibuloplasty) is often preferred when the
frenal attachment has a wide base. This technique is good for lengthening tissue andusually results in less scarring.
Note: Local anesthetic infiltration is usually sufficient for surgical treatment of frenalattachments. Care must be taken to avoid excessive infiltration directly in the frenumarea since it may obscure the anatomy that must be visualized at the time of excision.
ORAL SURGERY/PAIN CONTROL
Which of the following can be used for removing bo ne?
• Rongeur forceps• Chisel and mallet• Bone file• Bur and handpiece• All of the above
Copyright © 2001 - DENTAL DECKS
Misc.
• All of the above
Rongeur forceps are the most commonly used instruments for removing bone.However, the technique that most oral surgeons use when removing bone is the burand handpiece.
Very Important: Most high-speed turbine drills used for routine restorative dentistry aretotally unacceptable for removing one. The air exhausted from these drills goes into thewound and may be forced deeper into tissue planes and produce tissue emphysema,a potentially dangerous situation.
Note: Acute infected tissue emphysema is usually caused by the indiscreet use of:1. Air-pressure syringes: In drying out a root canal with a compressed air syringe,
septic material may be forced through the apical foramen into the cancellous portionof the alveolar process and ultimately out through the nutrient foramina into adjacentsoft tissues, resulting in formation of a septic cellulitis and tissue emphysema .
2. Atomizing spray bottles activated by compressed air: A similar condition can beinduced by the use of a compressed -air spray bottle for irrigation of wounds , particularly in the retromolar region. It is safer to use a hand-activated syringe when irrigating wounds or drying root canals since it is unlikely that a tissue emphysemawould be produced under these circumstances.
Misc.ORAL SURGERY/PAIN CONTROL
Before dental treatment , prophylactic antibiotic coverage is indicated for patients witheach of the following conditions except.
• Previous coronary artery bypass graft surgery• Rheumatic heart disease• Prosthetic aortic valve• Kidney damage needing hemodialysis• Total joint prosthesis• Mitral valve prolapse with valvular regurgitat ion
Copyright @ 2001 - DENTAL DECKS
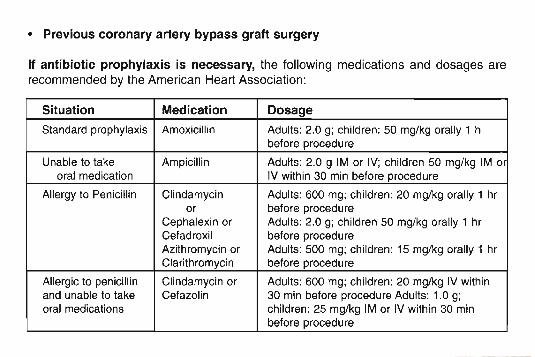
• Previous coronary artery bypass graft surgery
If antibiotic prophylaxis is necessary, the following medications and dosages arerecommended by the American Heart Association :
Situation Medication Dosage
Standard prophylaxis Amoxicill in Adults: 2.0 g; children : 50 mg/kg orally 1 hbefore procedure
Unable to take Ampicill in Adults: 2.0 9 1M or IV; children 50 mg/kg 1M ororal medication IV within 30 min before procedure
Allergy to Penicillin Clindamycin Adults : 600 mg; children : 20 mg/kg orally 1 hror before procedure
Cephalex in or Adults : 2.0 g; children 50 mg/kg orally 1 hrCefadroxil before procedureAzithromycin or Adults : 500 mg; children: 15 mg/kg orally 1 hrClarithromycin before procedure
Allergic to penicill in Clindamycin or Adults: 600 mg; children: 20 mg/kg IV withinand unable to take Cefazolin 30 min before procedure Adults : 1.0 g;oral medications children: 25 mg/kg 1M or IV within 30 min
before procedure
ORAL SURGERY/PAIN CONTROL
The universal sign of laryngeal obstruction is:
• Mydriasis• Stridor (crowing sounds)• Sweating• Tachycardia
Copyright © 2001 - DENTAL DECKS
Misc.
• Stridor (crowing sounds)"'Stridor is a high-pitched, noisy respiration, like the blowing of the wind. It is a sign of respiratory obstruction, especially in the trachea or larynx.
Because total airway obstruction usually occurs during inspiration, there is usually adequate oxygen left in the cerebral blood to permit up to 2 minutes of consciousness. If the obstruction is notrecognized and managed and oxygen delivered to the victim's lungs, blood, and brain, permanent neurologic damage occurs within 3 to 5 minutes.
Noninasive procedures for obstructed airway:• Back blows, manual thrusts, Heimlich maneuver, chest thrust, and finger sweep
Invasive procedures for obstructed airways; '-' These procedures should only be performed bypersons trained in these techniques and if proper equipment is available• Tracheotomy: Is used more for long-term airway maintenance and not for emergency air
ways• Cricothyrotomy: Is a procedure for establishing an emergency airway where other methods
are unsuitable or impossible. The access site is the cricothyroid membrane of the trachea,located on the anterior neck, between the cricoid and thyroid cartilages.
Important: A cricothyrotomy may be lifesaving in an anaphylactic reaction in which a patientshows signs of laryngeal obstruction. If a patient shows signs of laryngeal obstruction, thatis, stridor (crowing sounds), epinephrine should be given and oxygen administered . If a patientloses consciousness and appears to be unable to breathe, an emergency cricothyrotomy maybe required to bypass the laryngeal obstruction.
ORAL SURGERY/PAIN CONTROLMisc .
Osteomyelit is is an infection of the bone and bone marrow. It is most often causedby:
• Streptococcus pyogenes• Staphylococcus aureus• Mycobacterium tuberculosis• Neisseria meningitidis
Copyright © 2001 - DENTAL DECKS
• Staphylococcus aureus
Osteomyelitis is an infection in the bones. Often, the original site of infection is elsewhere in the body, and spreads to the bone by the blood. This may be predisposed toinfection due to a recent minor trauma that results in a blood clot. In children, the longbones are usually affected. In adults. the vertebrae and pelvis are most commonlyaffected. Pus is produced within the bone, which may result in a bone abscess. Theabscess then deprives the bone of its blood supply. Note: Chronic osteomyelitisresults when bone tissue dies as a result of the lost blood supply.
Important: Acute osteomyelitis occurs more frequently in the mandible as opposedto the maxilla. The primary reason for this is that the blood supply to the maxilla ismuch richer and is derived from a number of different arteries, while the mandibletends to draw its primary blood supply from the inferior alveolar artery. The dense overlying cortical bone of the mandible prevents penetration of periosteal blood vessels,thus the mandibular cancellous bone is more likely to become ischemic and thereforeinfected. Important point: Reduced blood supply will predispose bone toosteomyelitis.
Misc.ORAL SURGERY/PAIN CONTROL
Body temperature can be measured in several different ways, wh ich one is the leastaccurate?
• Orally• Axillary• Rectally• Aurally
Copyright @ 2001 - DENTAL DECKS
• Axillary"'Rectally Is the most accu rate
General considerations when checking vital signs:The patient should not have had alcohol, tobacco, caffeine, or performed vigorous exercise within 30 minutes of theexam.Ideally the patient should be silting with feet on the floor and their back supported. The examination room should be quietand the patent comfortable.History of hypertension. slow or rapid pulse. and current medications should always be obtained.
Rout ine vital signs Include:Blood pressure (normal 120/80)Pulse rate (normal 72)Respiration rate (normal 15)Temperature can be measured in several different ways:
Oral with a glass, paper, or electronic thermometer (normal 98.6 'F/37"C)AXillary with a glass or electronic thermometer (normal 97.6'FI36.3 ' C)Rectal or 'core' with a glass or electronic thermometer (99.6°FI37.7°C)Aural (the ear) with an electronic thermometer (normal 99.6°F/37.7'C)
Note: Abnormalities of vital signs are often clues to diseases, the aneranons in vital signs are used to evaluate a panenrsprogress.
Five major areas to be discussed when taking a patient history:1. Chief complaint2. History of present Illness3. Spec ific drug allegeries4. Review of systems (heart, liver, kidney, brain, etc.)5. Nature of symptoms
In complicated cases, don't be hesitant to call patient's physician, previous dentists, or other health professionals.
Misc.ORAL SURGERY/PAIN CONTROL
A surgical procedure for recontouring alveolar structures, usually in preparation fora prosthesis is called a (an):
• Closed reduction• Operculectomy• Alveoloplasty• Gingivoplasty
Copyright © 2001 - DENTAL DECKS
• Alveoloplasty
An alveoloplasty is the surgical preparation of the alveolar ridges (i.e., removing undercuts) for the reception of dentures or shaping and smoothing the socket margins afterextractions of teeth with subsequent suturing to insure optimal healing.
The objectives of this recontouring should be to provide the best possible tissuecontour for prosthesis support , while maintaining as much bone and soft tissue as possible.
Remember:1. A closed reduction is the closing of the space between fractured bone without cut
ting through the soft tissue or surrounding bond.2. A gingivoplasty is a surgical procedure to reshape the gingivae to create a nor
mal, functional form.3. An operculectomy is the removal of the operculum. which is the flap of tissue over
an unerupted or partially erupted tooth.
Gen InfoORAL SURGERYIPAIN CONTROL
Which of the following is the most common error in recording blood pressure?
• Applying the blood pressure cuff too tightly• Applying the blood pressure cuff too loosely• Overinflating the blood pressure cuff• Underinflating the blood pressure cuff• Use of the wrong size cuff
Copyright © 2001 - DENTAL DECKS
• Applying the blood pressure cuff too loosely"'This will give falsely elevated readings
Use of the wrong cuff size can result in erroneous readings. A normal adult bloodpressure cuff placed on an obese patient's arm will produce falsely elevated readings.This same cuff applied to the very thin arm of a child will produce falsely low readings.The width of the compression cuff should be approximately 20% greater than the diameter of the extremity on which the blood pressure is being recorded.
If you need to take additional readings, a wait of at least 15 seconds is requiredbefore reinflating the blood pressure cuff.
Notes:1. Elective dental care should be postponed if the systolic blood pressure is greater
than 160 mm Hg or the diastolic pressure is greater than 100 mm Hg.2. Emergency dental care should be postponed if the systolic pressure is greater
than 180 mm Hg or the diastolic pressure is greater than 110 mm Hg.Po~'"1 .00 €"\({:l\~ DQ ' " 0 0 t'~-E~EM'-'( :
\lo0 hoo \"b0ll\o
ORAL SURGERYIPAIN CONTROL
A prothrombin time (PT) of:
• 5-7 seconds is considered normal• 6-9 seconds is considered normal• 12-14 seconds is considered normal• 20-25 seconds is considered normal
Copyright © 2001 - DENTAL DECKS
Gen Info
• 12-14 seconds is considered normal
"··The PT (prothrombin time) results should be within 5-7 seconds of the control sample
Other tests used to measure a patient's clotting mechanisms:
• PTT (partial thromboplastin time): detects coagulation defects of the intrinsic system.Basic test for hemophilia. Normal value =25-36 seconds.
• Bleeding time: (Ivy method), normal value = less than 9 minutes.• Platelet counts: normal value =150,000-450,000 per 1 cu mm of blood. The mini
mal platelet count for oral surgery is 50,000.
Important: Perhaps the single most important consideration in ruling out hemorrhagic disorder is history.
Note: The PT test is the bes st to erform in order to determine whether oral surgery can be safely performed on a patient taking coumadin (or any oral an icoequant.To be a good candidate for surgery, the PT time should be within 5-7 seconds of thecontrol sample.
ORAL SURGERY/PAIN CONTROL
Major oral surgery includes all of the following procedures except
• The treatment of maxillary and mandibular fractures• Exodontia• Pre-prosthetic surgery• Reconstructive surgery• Traumatology
Copyright @ 2001 - DENTAL DECKS
Gen Info
• Exodontia"·Including routine, multiple, and surgical extractions
Major oral surgery Includes:• The treatment of fractures• Pre-prosthetic surgery:
- Tuberosity reductions- Vestibuloplasty
• Reconstructive surgery:- Orthognathic surgery- Facial deformities
• Traumatology:- Treatment of wounds, injuries, and resulting disabilities
General concerns of surgery: Nutritional status of patient, body fluids & electrolytes, pre-op &post-op information, wound healing (i.e., primary, secondary) and most importantly infection.
Note: The discipline of oral surgery is defined as "The diagnosis and surgical treatment ofinjuries, diseases, and malformation of the mouth and jaws."
Remember : The difference between acceptable and an excellent surgical outcome rests on howthe surgeon handles the tissue.
Gen InfoORAL SURGERY/PAIN CONTROL
All of the following drugs can potentiate a patient's bleeding following an extractionexcept
• Aspirin• Anticoagulants• Broad-spectrum antibiotics• Antianxiety drugs• Alcohol• Anticancer drugs
Copyright © 2001 - DENTAL DECKS
• Antianxiety drugs
If a patient is taking any one of these 5 drugs (aspirin, anticoagulants, broad-spectrumantibiotics, alcohol or anticancer) , you should be prepared to take special measuresin order to control the bleeding. Note: Patients with specific systemic diseases willalso have a prolonged bleeding time. These include nonalcoholic liver disease, hepatitis, cirrhosis, and hypertension.
Five means of obtaining wound hemostasis:1. By assisting natural hemostatic mechanisms: usually accomplished by placing a
cotton sponge with pressure on bleeding vessels or the use of a hemostat directlyon the vessel
2. By the use of heat on the cut vessels (called thermal coagulation)3. By suture ligation of the vessel4. By the placement of a pressure dressing over the wound: most bleeding from
oral surgery can be controlled this way5. By placing vasoconstrictive substances (epinephrine) on the wound
Remember: Excessive bleeding causes the formation of hematomas which increasethe chance of infection.
ORAL SURGERY/PAIN CONTROLGen Info
Which of the following is the process by which the total removal of a cystic lesion isachieved?
• Marsupialization• Decompression• Enucleation• The Partsch operation
Copyright © 2001 - DENTAL DECKS
• Enucleation
"" Enucleat ion is the treatment of choice whenever possible
Marsupialization, decompression, and the Partsch operation all refer to creating asurgical window in the wall of the cyst. The cyst is uncovered or "deroofed" and the cystic lining made continuous with the oral cavity or surrounding structures. The cyst sacis opened and emptied.
Enucleation is the treatment of choice for:• Congenital cysts• Mucoceles• Most odontogenic cysts
Marsupialization is the treatment of choice for:• Ranula -(Note: For a recurrent ranula treatment would also include the excision of
the sublingual gland.)• When cyst is large and close to vital structures
Whether a bone cyst or other cysts are completely enucleated or treated by marsupialization depends on the size and location to vital structures.

ORAL SURGERY/PAIN CONTROLGen Info
When performing CPR, if there is a pulse but the victim is not breathing, you shouldgive rescue breathing at a rate of:
• 2 breaths every 20 seconds• 1 breath every 15 seconds• 1 breath every 5 seconds• 2 breaths every 30 seconds
Copyright © 2001 - DENTAL DECKS
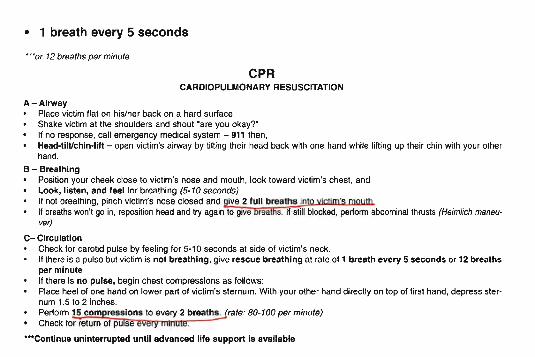
• 1 breath every 5 seconds
"r or 12 breaths per minute
CPRCARDIOPULMONARY RESUSCITATION
A - AirwayPlace victim flat on his/her back on a hard surface.Shake victim at the shoulders and shout ' are you okay? 'If no response, call emergency medical system - 911 then,Head-tll tlchin-Iift - open victim's airway by tilting their head back with one hand while lifting up their chin with your olherhand.
B - BreathingPosition your cheek close to victim's nose and mouth, look toward victim's chest, andLook, listen, and feel for breathing (5·10 seconds)If not breathing, pinch victim's nose closed and give 2 full breaths into victim's mouthIf breathswon't go in, repositionhead and try again to give breaths. If still blocked, perform abdominal thrusts (Heimlich maneuver)
C- CirculationCheck for carotid pulse by feeling for 5·10 seconds at side of victim's neck.If thera is a pulse but victim is not breathing, give rescue breathing at rate of 1 breath every 5 seconds or 12 breathsper minuteIf there Is no pu lse , begin chest compressi ons as follows:Place heel of one hand on lower part of victim's sternum. With your other hand direct ly on top of first hand, depress sternum 1.5 to 2 inches.Perform 15 com ressions to every 2 breaths. rate: 80-100 per minute)Check for return of pu se
"'Contl nue un interrupted until advanced life support Is available
ORAL SURGERY/PAIN CONTROL
What is the first step when init iati ng CPR?
• Administer oxygen• Establish unresponsiveness• Administer epinephrine• Place a cool towel on the person's forehead
Copyright @ 2001 - DENTAL DECKS
Gen Info
• Establish unresponsiveness (shake and shout, "are you OK?")
Followed by ABC's:• Airway (head tilt-chin lift): in most medical emergencies, this is the easiest tech
nique for opening a victim's airway• Breathing (look, listen, and feel)• Circulation (check carotid pulse)
Important points to remember in CPR:• If efforts are effective, the pupils will constrict• If too much pressure is incorrectly applied directly over the xyphoid process, the
liver may be injured• The result of interruptions in chest compressions while performing CPR is a reduc
tion of the blood flow and fall in the blood pressure to zero
Remember, you should stop CPR only under the following conditions:• If another trained person takes over CPR for you• If EMS personnel arrive and take over care of the victim• If you are exhausted and unable to continue• If the scene becomes unsafe
Gen InfoORAL SURGERY/PAIN CONTROL
Serum calcium will be increased in all of the following conditions except
• Hyperparathyroidism• Chronic glomeru lonephritis• Diabetes mellitus• Hypervitaminosis D• Malignant diseases of the skeleton (i.e., multiple myeloma)
Copyright © 2001 - DENTAL DECKS
• Diabetes mellitus
Calcium levels are regulated by parathyroid hormooe @creased hormone causes bone resorIGtion) which in turn increases calcium levels. Calcium is also regulated to some extent by the kidney tubules and GI mUcosa (iowenng pH will cause increased calcium absorption), Low serumcalcium levels will result in hyperirritabi lity of nerves and musc les,
Phosphorus concentration is also regulated by parathyroid hormone . Increased hormonecauses the kidneys to increase the rate of phosphate excretion which causes a decrease in plasma phosphate concentration.
Note ' ood health the ratio of calcium to phosphorus in the blood is 10: f there is a glandular imbalance, especia y In regard to the parat yroi g an s, en this ratio will be maintained ata different level, causing long-term health deterioration. In part icular, a high ratio of phosphorusto calcium sensitizes the body and increases inflammatory tendencies.
• BJnod glucose concentrat ion is regUlated by jnslJlin (Jowers glucose levels) !!Dd gil Ica§OO-...,(increases glucose levels) . Glucose normally does not appear in the urine although it is freely filtered because it is reabsorbed in the proximal convoluted tubule of the kidney. Serum glucosewill be increased In diabetes mellitus, adrenal tumors, Increased growth hormone, andliver dysfunction.
ORAL SURGERYIPAIN CONTROL
Minor oral surgery includes all of the following procedures except
• Exodontia• The treatment of maxillary and mandibular fractures• The treatment of dental infections• The treatment of hard tissue pathologies• The treatment of soft tissue pathologies
Copyright © 2001 - DENTAL DECKS
Gen Info
• The treatment of maxillary and mandibular fractures***This is considered to be major oral surgery
Minor oral surgery includes:• Exodontia:
- Routine extractions, multiple extractions, and surgical extractions• Treating dental infections:
- Periapical- Periodontal- Pericornitis- Facial infections (cellulitis)
• Soft tissue pathology:- Biopsy- Benign lesions
• Hard tissue pathology:- Alveoloplasty
ORAL SURGERY/PAIN CONTROL
The normal serum concentration of glucose is:
• 20-40 mg/dl• 50-70 mg/dl• 80-120 mg/dl• 130-150 mg/dl
Copyr ight © 2001 - DENTAL DECKS
Gen Info
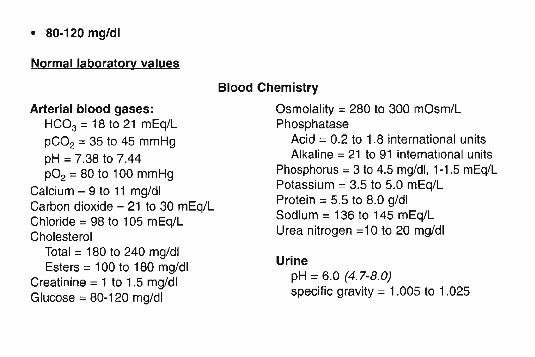
• 80·120 mg/dl
Normal laboratory values
Arterial blood gases:HC03 = 18 to 21 mEq/L
pC0 2 =35 to 45 mmHgpH =7.38 to 7.44p02 = 80 to 100 mmHg
Calcium - 9 to 11 mg/dlCarbon dioxide - 21 to 30 mEq/LChloride = 98 to 105 mEq/LCholesterol
Total = 180 to 240 mg/dlEsters =100 to 180 mg/dl
Creatinine = 1 to 1.5 mg/dlGlucose = 80-120 mg/dl
Blood Chemistry
Osmolal ity =280 to 300 mOsm/LPhosphatase
Acid =0.2 to 1.8 internat ional unitsAlkaline = 21 to 91 international units
Phosphorus = 3 to 4.5 mg/dl, 1-1.5 mEq/LPotassium =3.5 to 5.0 mEq/LProtein =5.5 to 8.0 g/dlSodium =136 to 145 mEq/LUrea nitrogen =10 to 20 mg/dl
UrinepH = 6.0 (4.7-8.0)specific gravity = 1.005 to 1.025
ORAL SURGERYIPAIN CONTROL
What is the proper rate of rescue breathing in an adult?
• 15 times per minute• 12 times per minute• 20 times per minute• 25 times per minute
Copyright @ 2001 - DENTAL DECKS
Gen Info
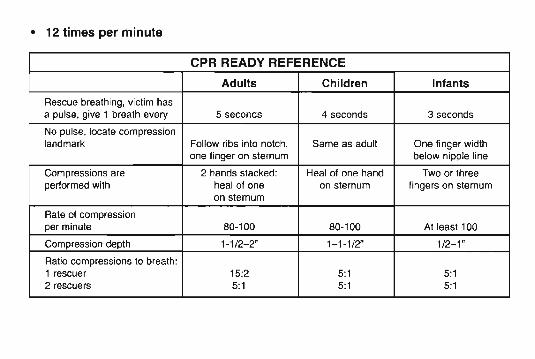
• 12 times per minute
CPR READY REFERENCE
Adults Children Infants
Rescue breathing, victim hasa pulse, give 1 breath every 5 seconds 4 seconds 3 seconds
No pulse, locate compressionlandmark Follow ribs into notch, Same as adult One finger width
one finger on sternum below nipple line
Compressions are 2 hands stacked: Heal of one hand Two or threeperformed with heal 01 one on sternum lingers on sternum
on sternum
Rate 01 compressionper minute 80-100 80-100 At least 100
Compression depth 1-1/2-2" 1-101/2" 1/2-1 "
Ratio compressions to breath:1 rescuer 15:2 5:1 5:12 rescuers 5:1 5:1 5:1
Gen InfoORAL SURGERY/PAIN CONTROL
The American Society of Anesthesiologists would give what ASA classification to ahealthy young patient with an unremarkable medical history and no systemic disease?
• ASA-O• ASA-I• ASA-II• ASA-V
Copyright © 2001 - DENTAL DECKS
• ASA·1
American Society of Anesthesiologists (ASA)Classification of Physical Status
ASA-1 A normal healthy patient
ASA-II A patient with mild systemic disease or signif icant health risk factor (such assmoking, excessive alcohol use, and obesity)
ASA-III A patient with severe disease that is not incapacitating
ASA-IV A patient with severe systemic disease that is a constant threat to life
ASA-V A moribund patient who is not expected to survive without the operation
ASA-VI A declared brain-dead patient whose organs are being removed for donor purposes
ORAL SURGERY/PAIN CONTROL
Which surgical approach listed below is the best to expose the TMJ?
• Preauricular• Submandibular• Both are the same
Copy right © 2001 - DENTAL DECKS
TMJ
• Preauricular
Surgical approaches to the TMJ:• Preauricular: The best incision to expose the TMJ. A perpendicular incision is made
just anterior to the external ear parallel to the superficial temporal artery. The incision extends from one inch above the zygomatic arch to the lower extremity of theear. The condyle is approached from behind . Note: With this approach, care mustbe taken not to damage either the facial nerve or the vessels that richly supply thisarea.
• Submandibular approach (Risdom approach): This is the standard surgicalapproach to the ramus of the mandible and neck of the condyle. It is not the bestapproach for procedures within the joint space itself.
Remember: The most common cause of TMJ ankylosis is trauma. However, ankylosis is the most common complication of rheumatoid arthritis.
ORAL SURGERY/PAIN CONTROLTMJ
What is the best way to palpate the posterior aspect of the mandibular condyle?
• Intraorally• Lateral to the external auditory meatus• Through the external auditory meatus• Any of the above
Copyright @ 2001 - DENTAL DECKS
• Through the external auditory meatus (canal)
The temporomandibular joint should be evaluated for tenderness and noise. Thejoint is palpated laterally (in front of the external auditory meatus) with the mandible ina closed and open position. The joint should also be palpated through the external auditory meatus with the mandible in a closed and open position. Note: The posterioraspect of the condyle is rounded and convex, whereas the anteroinferior aspect isconcave.
When the articular disc (or meniscus) of the joint and condyle of the mandible lackfunctional coordination, you will hear a click when a patient opens his/her mouth.Tenderness and sensitivity should be noted as well as joint noises (clicking and crepitus). The mandibular range of motion should also be determined. The normal range ofmovement of an adult's mandible is about 50 mm (opening) and 10 mm protrusivelyand laterally.
Notes :1. NSAIDs are the first line of treatment for TMJ pain2. Benzodiazepines may be prescribed for significant muscle pain or spasms3. Moist heat to the affected area is helpful (no longer than 15 minutes per applica
tion).4. Educate patient about bruxism and the need to avoid clenching and grinding teeth.
TMJORAL SURGERY/PAIN CONTROL
Which of the following is considered to be the most common cause of TMJ pain?
• Internal derangement• Degenerative joint disease (DJD)• Myotascial pain dysfunct ion (MPD) syndrome• None of the above
Copyright © 2001 - DENTAL DECKS
• Myofascial pain dysfunction (MPD) syndrome
TMJ syndrome is divided into three categories:• Myofascial pain dysfunction (MPD) syndrome: Is considered to be the most
common cause of TMJ pain. It is a disease primarily involving the muscles of mastication.
• Internal derangement: Is defined as an abnormal relationship of the articular discto the mandibular condyle, fossa, and articular eminence (or tubercle) .
• Degenerative joint disease (osteoarthritis): Is the organic degeneration of thearticular surfaces within the TMJ.
Important: The key mechanism for the cause of TMJ disorders is muscle dysfunction (or muscle spasm)
MPD syndrome is believed to be a stress related disorder. This increase in stress produces an increase in mandibular muscle tension and in combination with teeth clenching results in muscle spasm, pain, and dysfunction. Note: MPD often responds to anacrylic night guard (also called an occlusal separator or occlusal appliance) along witha soft diet, limited talking, and elimination of gum chewing. Moist heat applied to theface and nonsteroidal anti-inflammatory agents are also helpful during the acute phase.
ORAL SURGERY/PAIN CONTROL
What is the only direction in which the TMJ can be dislocated?
• Laterally• Medially• Anteriorly• Posteriorly
Copyright © 2001 - DENTAL DECKS
TMJ
• Anteriorly
Internal derangement of the TMJ is present when the posterior band of the articular discis anteriorly displaced in front of the condyle. As the articular disc translates anteriorly,the posterior band remains in front of the condyle and the bilaminar zone becomesabnormally stretched. Often the displaced posterior band will return to its normal position when the condyle reaches a certain point. This is termed anterior displaced withreduction. Note: When the articular disc reduces the patient often feels a pop orclick in the joint.
In some patients the articular disc remains anteriorly displaced at full mouth opening.This is termed anterior displacement without reduction. Note: The articular disc canusually be reduced by inducing downward pressure on the posterior teeth and upwardpressure on the chin, accompanied by posterior displacement of the entire mandible.
Note: The patient who has had reduction of a mandibular dislocation should beinstructed to limit opening of the mouth for two to three weeks.
Remember: The most common cause of restricted mandibular movement is disc interference disorders, which change the relationship of the disc and the condyle.
ORAL SURGERY/PAIN CONTROLImpl/Grfts
All of the following are contraindications to implant placement except one. Which isthe exception:
• The presence of pathology within the bone• The presence of limiting anatomic structures such as the inferior alveolar nerve or
maxillary sinus• Unrealistic expectations of the patient• Poor oral health and hygiene• Patient's inability to tolerate implant procedures• The patient has a pronounced gag reflex• Acute illness or uncontrolled metabolic disease
Copyright © 2001 - DENTAL DECKS
• The patient has a pronounced gag reflex
This may actually be an indication for the consideration of implant placement. Thisis because the patient may not be able to tolerate the placement of a removable prostheses.
Other possible indications for implant placement include:• Resorption of alveolar ridge or other anatomic considerations that do not allow for
adequate retention of conventional removable prostheses.• Patient is psychologically unable to deal with removable prostheses.• Medical condition for which removable prostheses may create a risk (i.e., seizure
disorder). .• Loss of posterior teeth, particularly unilaterally.
Remember :• Implants placed in the maxillary anterior region have the highest failure rate.• Mobility of the implant is regarded as the most common sign of implant failure.
ORAL SURGERY/PAIN CONTROLImpl/Grfts
Which of the following is the most common indication for tooth transplantation?
• Severe decay of a central incisor• Severe decay of a first molar• Severe decay of a third molar• Severe decay of a canine
Copyright © 2001 - DENTAL DECKS
• Severe decay of a first molar
The first molar is atraumatically removed, and the third molar is placed into thesocket. Success of the transplant is most predictable w hen the apices of the roots >of the tooth to be transplanted are ana third to one-ba lf formed with open apices andthe bordering bony plates are intact. Also, you need adequate mesiodistal width of thehost implant site, the absence of acute periapical or periodontal inflammatory states,and the general good oral health of the patient. Note: This is called an autogenoustooth transplantation, meaning a tooth from the same individual is moved toanother site. The most likely cause of failure will be a chronic, progressive externalroot resorption.
Important: The almost universal sequelae of an allogeneic tooth transplant isankylosis and progressive root resorption. An allogeneic tooth transplant meansthat a tooth from one individual is placed in another individual.
Remember: The change in continuity of the occlusal plane observed after ankylosisof a tooth is caused by the continued eruption of the other non-ankylosed teeth andgrowth of the alveolar process.
ORAL SURGERY/PAIN CONTROL Impl/Grfts
Which of the following are requirements for successful implant placement?
• Mucosal seal• Adequate transfer of force• Biocompatibility• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
Important: Mobility of the implant is regarded as the most important sign of implantfailure.
Steps in the assessment of patients prior to implant placement:
1. Dental and medical history2. Clinical examination3. Radiographic examination (panoramic and periapical)
The surgeon and restoring dentist must work together to ensure proper implantplacement and orientation. A surgical stent fabricated to the specifications of therestoring dentist can be helpful to ensure proper implant placement and orientation.Remember: Without proper planning, an implant may be successfully integratedbut impossible to restore.
ORAL SURGERYIPAIN CONTROL
The optimal bone grafting material should be of what origin?
• Foreign• Synthetic• Autogenous• Mixed
Copyright © 2001 - DENTAL DECKS
Impl/Grfts
• Autogenous
Autogenous bone is bone from the same person (from one part of the body toanother). Autogenous grafts (also called an autograft) are usually employed to restorelarge areas of lost mandibular bones following oncological surgery or trauma. Of all thefacial bones resected in oncological surgery, the mandible is the most frequentlyremoved.
The bone marrow for grafting defects in the mandible and maxilla is generallyobtained from the iliac crest. Also used for ridge augmentation.
Notes:1. A costochondrial rib graft may be employed with the cartilaginous portion simu
lating the TMJ and condyle. When used for ridge augmentation a lot of shrinkageis noted.
2. Bone plates, biphasic pins, titanium mesh, and intraosseous wires are used inthe fixation of bone grafts. Sutures are not generally used.
ORAL SURGERY/PAIN CONTROL
Allaplastic grafts are:
Impl/Grfts
• Those where the bone to be grafted to jaw is taken , or harvest from one's own body• Taken from human donors• Inert, man made synthet ic materials• Harvested from animals
Copyright © 2001 - DENTAL DECKS
• Inert, man made synthetic materials
For bone replacement a man made material that mimics natural bone is used . Most oftenhydroxyapatite (HA) is used for augmentation of the mandib le. Hydroxyapatite is a dense , blocompatib le material that can be produced synthetically or obtained from biologic sources such ascoral. The granular or particle form is most commonly used for alveolar ridge augmentation.Note: When placed in a subperiosteal environment, HA bonds both physically and chemically tothe bone.
Some advantages and disadvantages of restructuring an atrophic ridge with hydroxyapatitegranules:
• AdvantagesIt is a simple surgical technique suitable as an office procedure
- No donor site is required to obtain autogenous bone graft material• Hydroxypatite is totally biocompatibie and nonresorbable
• DisadvantagesMigration of the hydroxypatite granulesPoor ridge form (inadequate heigh t)Abnormal coior under the mucosa
- Mental nerve neuropathyExcessive augmentation
ORAL SURGERY/PAIN CONTROLImpl/Grfts
Alloplastic materials used for augmentation genioplasty generally have a tendencyto do what?
• Produce an immunologic response• Be replaced by the host bone• Migrate from the position in which they were placed at the time of surgery• Be rejected
Copyright © 2001 - DENTAL DECKS
• Migrate from the position in which they were placed at the time of surgery
Genioplasty is a procedure by which the position of the chin is surgically altered. Themost common techniques for genioplasty are osteotomy or augmentation with naturalor alloplastic materials.
There are two other problems that are frequently encountered when using alloplasticmaterials for genioplasty:• Erosion of the chin prominence contiguous with the implant.• Unpleasant sensation in the implant region when exposed to cold temperatures.
Note: The best way to enlarge the prominence of the chin for best long-term results isto reposition the lower border anteriorly by osteotomy (horizontal sliding osteotomy).
Remember: Alloplastic grafts are inert, man made synthetic materials. The modernartificial joint replacement procedures uses metal alloplastic grafts. For bone replacement a man made material that mimics natural bone is used. Most often this is a formof calcium phosphate (i.e.. tricalcium phosphate, calcium carbonate, or hydroxyapatite).
ORAL SURGERY/PAIN CONTROL
The most commonly used allogeneic bone is:
• Freeze-dried• Artificial• Neither of the above
Copyright © 2001 - DENTAL DECKS
Impl/Grfts
I
J
• Freeze-dried
Allogeneic grafts (also called allografts or homografts) are composed of tissues takenfrom an individual of the same species who is not genetically related to the patient.They consist of freeze-dried bone and freeze-dried decalcified bone from anothersource (usually cadaver bone).
These grafts are treated to reduce the antigenicity. However, these treatments destroyany remaining osteogenic cells in the graft. These grafts offer a hard tissue matrix only;.!!Jis graft is eventuallv replaced by the bast bone
Important point: The host must produce all of the essential elements in the graft bedfor an allogeneic bone graft to become resorbed and replaced.
The advantages of this type of graft are that it doesn 't require another site of preparation in the host and that a similar bone or a bone of similar shape to that beingreplaced can be obtained.
ORAL SURGERYIPAIN CONTROL
Implants that are surgically inserted into the jawbone are called:
• Endosseous implants• Subperiosteal implants• Transosseus implants
Copyright © 2001 - DENTAL DECKS
Impl/Grfts

• Endosseous implants---They are the most frequently used implants today
Oral Implants can be categorized into three main groups:1. Endosseous Implants are implants that are surgically Inserted Into the jawbone. They are the most
frequently used Implants today. They are further subdivided into root form and blade form implants.2. SUbperiosteal Implants are frameworks specifically fabricated to l it on top of supporting areas in the
mandible or maxilla under the mucoperiosteum.3. Transosseous Implants are implants that are similar to endosseous implants in that they are surgically
inserted into the jawbone. However, these implants actually penetrate the entire jaw so that they actually emerge opposite the entry site, usually at the bottom 01the chin. Note : Their primary ind ication is inthe very atrophic mandible where root form implants may lurther compromise the strength of the jaw.
Remember: Osseo lntegrated implants are anchored directly to lIying bone. This determination is..!!!.ade by radiographic and light microscopic analysis.... -
Root form implants:• Cylindrical in shape, can be threaded or non-threaded. 3 to 5 mm in diameter and 7 to 20 mm in length.
Typically made of titanium. Note : These implants are the most popular.
Blade implants:• Are wedge-shaped or rectangular in cross section. Typically made of titanium as well.
Two basic types of implant placement:1. Submerged - requires a second surgical procedure (two-stage) to uncover the fixture.2. Nonsubmerged - does not require a second surgical procedure (one-stage) .
ORAL SURGERY/PAIN CONTROLImpl/Grfts
Allogeneic grafts (also called allografts) are composed of tissues taken from:
• Another species• An individual of the same species who is not genetically related to the recipient• An individual of the same species who is genetically related to the recipient• The same individual
Copyright @ 2001 - DENTAL DECKS
• An individual of the same species who is not genetically related to the recipient
···Usually cadaver bone
Classification of grafts (or implants)• Autogenous grafts (also called autografts) are composed of tissues taken from the same
Individual. Most frequently used in oral surgery.• Allogenic grafts (also called allografts) are composed of tissues taken from an individual of
the same species who is not genetically related to the patient (usually cadaver bone).• Isogeneic grans (also called isografts or syngenesioplastic grafts) are composed of tissues
taken from an individual of the same species who is genetically related to the recipient.• ~enogeneic imp lants (also called xenografts or heterografts) are composed of tissues taken
from a donor of another species, for example. animal bone grafted to man (also called heterograft). Rarely used in oral surgery.
Note: Rejection of the graft is most common when allografts or xenografts of bone and cartilage are used in oral surgery. Autogenous grafts, although frequently presenting surgical andtechnical problems. do not as a rule involve rejection (or immunological complications).
The ideal graft should:• Be replaced by the host bone.• Withstand mechanical forces.• Produce no immunologic response (or rejection).• Actively assist osteogenic (bone-form ing) processes of the host. The greatest osteogenic
potential occurs with an autogenous cancellous graft and hemopoietic marrow.
FracturesORAL SURGERY/PAIN CONTROL
If the fracture line results in a muscle pull displacing the fractured segment, it istermed a (an):
• Favorable fracture• Unfavorable fracture
Copyright © 2001 - DENTAL DECKS
• Unfavorable fracture
The line of fracture will determine whether muscles will be able to displace the fractured segments from their original position:• If the fracture line prevents the displacement of the fracture by muscle pull, it is
termed a favorable fracture.• If the fracture line results in a muscle pull displacing the fractured segment, it is .
termed an unfavorable fracture.
The following radiographic views are often helpful to evaluate mandibular fractures:• Posteroanterior view• Lateral oblique view• Towne view• Panoramic view
Remember: The control of airway is vital to any treatment of a patient with facial fractures.
ORAL SURGERY/PAIN CONTROLFractures
A patient with a paralyzed left lateral pterygoid muscle is instructed to open hismouth wide. Which direction will the mandible take upon opening?
• To the right• To the left• Straight
Copyright © 2001 - DENTAL DECKS
• To the left
-" The mandible will always deviate to the side of the injury.
A patient who sustained a subcondylar fracture on the left side would be unableto deviate the mandible to the right. This is normally treated by a closed procedureinvolving intermaxillary fixation. This procedure immobilizes the concomitant fractures and corrects the displacement of the jaws associated with the condylar fracturethereby correcting the shift of the midline toward the side of the fractured condyle andthe slight premature posterior occlusion on that side.
ORAL SURGERY/PAIN CONTROLFractures
Which of the following can contribute to the non-healing (non-union) of a fracture?
• Ischemia• Excessive mobility• Interposition of soft tissue• Infection• All of the above
Copyright @ 2001 - DENTAL DECKS
• All of the above
Four reasons that a fracture does not heal:1. Ischemia: The navicular bone of the wrist, the femoral neck, and the lower third of the tibia
are all poorly vascularized and therefore are subject to ischemic necrosis after a fracture.2. Excessive mobility: Healing is prevented and pseudoarthrosis or a pseudo-joint may
occur.3. Interposition of soft tissue: Occurs between the fractured ends.4. Infection: Compound fractures have a tendency to become Infected.
Note: A fat embolism is most often a sequela of fractures.
Inappropriate healing (three types):• Delayed-union: satisfactory healing which requires greater than the normal six week period.
May be caused by infection, interposition of soft tissue or muscle between the fractured segments.
• Non-union: failure of the fractured segments to unite properly. May be caused by infection,improper immobilization, or interposition of soft tissue.
• Mal-union: can be either delayed or complete union in an improper position. May be causedby improper immobilization or imperfect reduction.
FracturesORAL SURGERY/PAIN CONTROL
A mandibular fracture that extends only through the cortical portion of the bone without complete fracture of the bone is called a:
• Simple fracture• Greenstick fracture• Compound fracture• Comminuted fracture
Copyright © 2001 - DENTAL DECKS
• Greenstick fracture
'··Greenstick fractures are closed fractures involving incomplete fractures with flexible bone. Most often seen in children .
The following categories classify mandibula r fractures by describing the condition of thebone fragments at the fracture site and possible communication with the external environment:• Simple - divides a single bone into two distinct parts with no external communica
tion. These are closed fractures with no lacerations of the oral mucosa or facial tissues.
• Compound - fracture commynicates with the outside environment (open fracture).This may occur by laceration of the oral tissues exposing the bone fragments , fracture of the maxilla into the sinuses, or by way of skin lacerations that would exposethe fractured segments. Infection is common.
• Comminuted - multiple fractures of a single bone. They may be simple or compound.
Remember: The most common complication of an open fracture is infection .
FracturesORAL SURGERY/PAIN CONTROL
Which type of bone healing involves both endosteal and periosteal proliferation?
• Primary (bone-fa-bone)• Secondary (space fills in with cal/us)
Copyright © 2001 - DENTAL DECKS
• Primary (bone-to-bone)
The healing of bone can be divided into three overlapping phases:1. Hemorrhage - occurs first and is associated with clot organization and proliferation
of blood vessels. This nonspecific phase occurs during the first 10 days.2. Callus formation - a primary callus is formed in the next 10 to 20 days. A second
ary callus forms in 20 to 60 days.3. Functi nal reconstruc . - mechanical forces are important in this phase..The
haversian systems are lined up according to stress lines. Excess bone is removed.The shape of the bone is molded to conform with functional usage so that bone maybe added to one surface and removed from another. It takes 2 to 3 years to completely reform a fracture.
Secondary bone healing involves mostly endosteal proliferation into the void (thespace between two pieces of bone).
Endosteal proliferation - occurs within a bone_
Periosteal pro lifer urs within the connective tissue covering all bo Ea.Speriosteum.
ExoORAL SURGERY/PAIN CONTROL
Which size suture listed below has the least st rength and the smallest diameter?
• 9-0• 3-0
• 2• 5
Copyright © 2001 - DENTAL DECKS
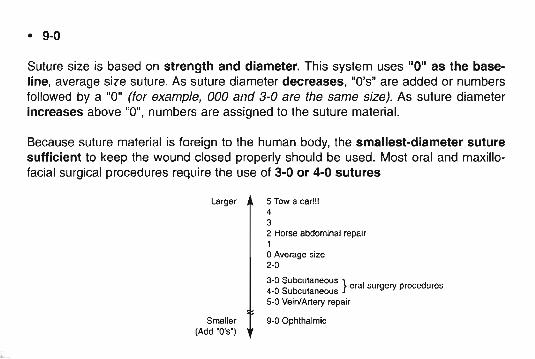
• 9-0
Suture size is based on strength and diameter. This system uses "0" as the baseline, average size suture. As suture diameter decreases , "D's" are added or numbersfollowed by a "0" (for example, 000 and 3-0 are the same size). As suture diameterincreases above "0", numbers are assigned to the suture material.
Because suture material is foreign to the human body, the smallest-diameter suturesufficient to keep the wound closed properly should be used. Most oral and maxillofacial surgical procedures require the use of 3-0 or 4-0 sutures
Larger 5 Tow a car !!!432 Horse abdominal repair1oAverage size2-0
43.0
0SSUbcbuttaneous } oral surgery procedures
- u cu aneous5-0 Vein/Art ery repa ir
Smaller(Add "D's' )
g-OOphthalmic
ExoORAL SURGERYIPAIN CONTROL
Strong apical pressure with a small straight elevator may displace root tips of maxillary premolars and molars into the:
• Submandibular space• Maxillary sinus• Mandibular canal• Infratemporal fossa
Copyright @ 2001 - DENTAL DECKS
• Maxillary sinus
If the root tip is small (2 or 3 mm), noninfected, and cannot be removed throughthe small opening in the socket apex, no additional surgical procedure should beperformed through the socket, and the root tip should be left in the sinus. If the root tipis left in the sinus, measures should be taken similar to those taken when leaving anyroot tip in place. The patient must be informed of the decision and given proper followup instructions.
If a large root fragment or the entire tooth is displaced into the maxillary sinus(antrum), it should be removed. The usual method is a Caldwell-Luc approach. Thisis a surgical procedure in which an opening is made into the maxillary sinus by way ofan incision into the canine fossa above the level of the premolar roots. The tooth orroot is then removed. Important: An oral surgeon to whom the patient should bereferred should perform this procedure.
ExoORAL SURGERY/PAIN CONTROL
Which of the following delay the healing process of an extraction site?
• A patient that has a protein deficiency• A patient on glucocortico id therapy• An older patient• Local infections• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
There are two basic methods of wound healing:1. Primary intention (also called first intention) occurs when wound margins are nicely
apposed. Healing occurs more rapidly with a lower risk of infection, with less scar formationand less tissue loss than wounds allowed to heal by secondary intention. Examples includewell-repaired and well-reduced bone fractures.
2. Secondary intention (also called second intention) occurs when a wound is large and exudative. This site fills in with granulation tissue. Healing is slower and produces more scar tissue than is the case with healing by primary intention. Examples include extraction sockets,poorly reduced fractures, and large ulcers.
Stages of wound healing:1. Inflammatory stage (consists of a vascular and cellular phase) : neutrophils and lymphocytes
predominate.2. Fibroblastic stage (mediated by fibroblasts): collagen and new blood vessels are produced.3. Remodeling stage (collagen fibers continue to increase tensile strength)
Other factors that impair wound healing: foreign material, necrotic tissue, ischemia, and tension.
Remember: 3% hydrogen peroxide is the agent of choice for the debridement of intraoralwounds.
ORAL SURGERY/PAIN CONTROLExo
During extraction of a maxillary third molar, you realize the tuberosity has also beenextracted. What is the proper treatment in this case?
• Remove the tuberosity from the tooth and reimplant the tuberosity• Smooth the sharp edges of the remaining bone and replace and suture the remain
ing soft tissue• No special treatment is necessary• None of the above
Copyright © 2001 - DENTAL DECKS
• Smooth the sharp edges of the remaining bone and replace and suture theremaining soft tissue
A fracture of the maxillary tuberosity most commonly results from extraction of anerupted maxillary third molar - or a second molar if it happens to be the last tooth inthe arch.
If the tuberosity is fractured but intact. it should be manually repositioned and stabilized with sutures.
The complications most often seen after extraction of an isolated residual maxillaryerupted molar are: (-ro.V'\'C)\O>\'S)• Fracture of the tUberosity• Fracture of the floor of the sinus
Important: "Beware of the lone molar"
ExoORAL SURGERY/PAIN CONTROL
In preparing the edentulous mandible for dentures , each of the following may be safely excised except
• A labial frenum• A lingual frenum• The mylohyoid ridge• The genial tubercles• An exostosis
Copyright © 2001 - DENTAL DECKS
• The genial tubercles
The genial tubercles are situated on the lingual surface of the mandible at a pointabout midway between the superior and inferior borders. There are four of them, twoof which are situated on each side and adjacent to the symphys is. Although usually relatively small, they may be fairly large and extend outward from the surface as spinousprocesses. These tubercles are the area of muscle attachment for the suprahyoidmuscles.
Important: If the genial tubercles were removed, the tongue would be flaccid.
Notes:1. When removing the mylohyoid ridge, be careful to protect the lingual nerve.2. When removing a mandibular exostosis (mandibular torus) it is recommended that
an envelop flap design, which has no vertical components, be used.
ExoORAL SURGERYIPAIN CONTROL
While attempting to remove a grossly decayed mandibular molar, the crown fractures. What is recommended next step in order to facilitate the removal of this tooth?
• Use a larger forceps and luxate remaining portion of tooth to the lingual• Separate the roots• Irrigate the area and proceed to remove the rest of the tooth• Place a sedative filling and reschedule patient
Copyright © 2001 - DENTAL DECKS
• Separate the roots"""This can be done with a chisel , elevator, or most easily with a bur.
Teeth with two or more roots often need to be sectioned into single entities prior tosuccessful removal. A popular method of section ing is to make a bur cut between theroots, followed by inserting an elevator in the slot and turning it 900 to cause a break.
The removal of a freshly fractured root is usually attempted by the closed method(without a flap) if there is a likelihood of success. However, it is best to prepare a flapif the technique is not successful within 5 to 10 minutes. Otherwise a half hour can bewasted, the soft and bony tissues can be traumatized, and a flap has to be made anyway.
Teeth are resistant to crush but are not resistant to shear. Therefore :• Place the beaks of the forceps opposite to each other at the same level on the tooth.• The beaks should be applied in a line parallel with the long axis of the tooth.
Remember: When luxating a tooth with forceps , the movements should be firm anddeliberate, primarily to the facial with secondary movements to the lingual. The maxillary first bicuspid is least likely to be removed by rotation forces due to its rootstructure (obviously molars are not removed by rotation).
ExoORAL SURGERY/PAIN CONTROL
While extracting a mandibular third molar, you notice that the distal root tip is missing. Where is it most likely to be found?
• In the infratemporal fossa• In the submandibular space• In the mandibular canal• In the pterygopalatine fossa
Copyright © 2001 - DENTAL DECKS
• In the submandibular space
Important: To prevent this, avoid all apical pressures when removing the roots or root tips ofall mandibular molars. If a mandibular molar root tip is displaced inferiorly, it may either be in themandibular canal or through the lingual cortical plate.
Note: The sybmandibular space usually drains infections from the mandibular bicllspids andmolars because their apices lie below the mylohyoid muscle attachment.
The submandibular space is a potential space of the neck bounded by the oral mucosa andtongue anteriorly and medially; the superficial layer of deep cervical fascia laterally, and thehyoid bone inferiorly. It comprises two spaces, the sublingual and submaxillary spaces, divided by the mylohyoid muscle.
The submental space is the medial part of the submaxillary space. It contains the submentallymph nodes that drain the median parts of the lower lip, tip of the tongue, and the floor ofthe mouth. Usually drains infections from the mandibular incisors and canines because theirapices lie above the mylohyoid muscle attachment.
The sublingual space is the superior part of the submandibular space, containing the sublingualgland and loose connective tissue surrounding the tongue.
Remember: Ludwig's angina.is the most commonly encountered neck space infection (involvesthe sublingu8J, submandibular, and submental spaces).
ExoORAL SURGERY/PAIN CONTROL
Arrange the following five phases of healing of an extraction site in their correct order:
• Replacement of the connective tissue by fibrillar bone• Hemorrhage and clot formation• Replacement of granulation tissue by connect ive tissue and epithelial ization of the
site• Recontouring of the alveolar bone and bone maturation• Organization of the clot by granulation tissue
Copyright © 2001 - DENTAL DECKS

• The correct order of the five phases of healing of an extraction site are:1. Hemorrhage and clot formation2. Organization of the clot by granulation tissue3. Replacement of granulation tissue by connective tissue and epithelialization of the site4. Replacement of the connective tissue by fibrillar bone5. Recontouring of the alveolar bone and bone maturation
Note: Glucocorticoids have been shown to have the greatest effect on granulation tissue (theyretard healing)
The same stages that occur in normal wound healing of soft tissue injuries (inflammation, fibroplasia, and remodeling) also occur in the repair of injured bone. However, osteoblasts andosteoc lasts are also involved to repair damaged bone tissue.
Bone heals by pr imary and secondary intention as does soft tissue.• Primary intention bone repair involves both endosteal and periosteal proliferation This
type of bone repair occurs when either the bone is incompletely fractured or a surgeon closely reapproximates the fractured ends of a bone. Little fibrous tissue is produced with minimal callus formation.
• Secondary intention bone repair involves mostly endosteal proliferation. If fracturedbones remain more than a millimeter apart, this type of repair takes place. A lot of fibroustissue is formed and a callus is formed This callus eventl lally ossifies... .
ExoORAL SURGERY/PAIN CONTROL
If a small communication is made with the maxillary sinus during extraction of a maxillary second molar, what treatment is recommended?
• The sinus communication should be closed with a flap procedure• No additional surgical treatment is necessary• A figure-eight suture should be placed over the tooth socket• None of the above
Copyright © 2001 - DENTAL DECKS
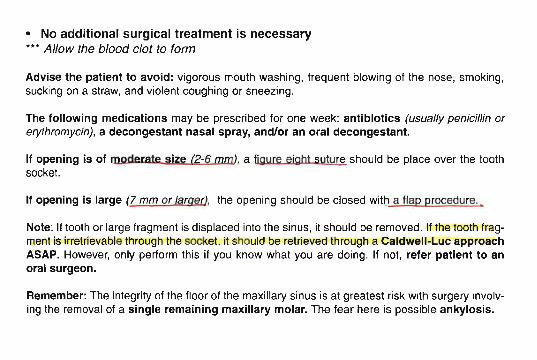
• No additional surgical treatment is necessary*** Allow the blood clot to form
Adv ise the pat ient to avoid: vigorous mouth washing, frequent blowing of the nose, smoking,sucking on a straw, and violent coughing or sneezing.
The following medications may be prescribed for one week: antibiotics (usually penicillin orerythromycin), a decongestant nasal spray, and/or an oral decongestant.
If opening is of moderate size (2-6 rom), a figyre eight suture should be place over the toothsocket.
If opening is large (7 mm or larger), the opening should be closed wittJ a flap procedure.
Note: If tooth or large fragment is displaced into the sinus, it should be removed. If the tooth fragment is irretrievable through the socket, it should be retrieved through a Caldwell·Luc approachASAP. However, only perform this if you know what you are doing. If not, refer patient to anoral surgeon.
Remember: The integrity of the floor of the maxillary sinus is at greatest risk with surgery involving the removal of a single remaining maxillary molar. The fear here is possible ankylosis.
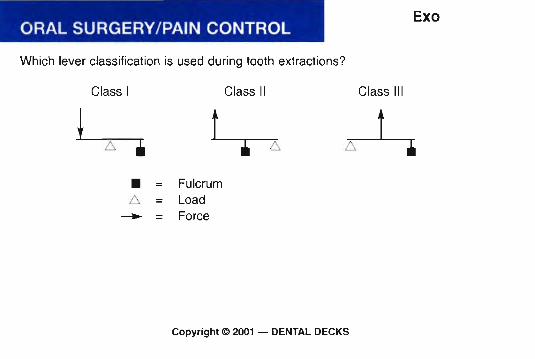
ORAL SURGERYIPAIN CONTROL
Which lever classification is used during tooth extract ions?
Exo
Class I
• =6. =....... =
Class II
FulcrumLoadForce
Class III
Copyri ght © 2001 - DENTAL DECKS
• Class II lever
Teeth are extracted by luxation forces perpendicular to the long axis of the tooth. notby pulling along the long axis . The fulcrum is as close to the apex of the tooth as possible. Note: Rotation forces can be used on single rooted teeth.
Remember: The beak of extraction forceps is designed so that most of the pressureexerted during an extraction is transmitted to the root of the tooth.
ORAL SURGERY/PAIN CONTROL
Which teeth listed below are the most frequently impacted?
• Maxillary can ines• Maxillary third molars• Mandibular third molars• Mandibular premolars
Copyright © 2001 - DENTAL DECKS
Exo
• Mandibular third molars***Followed by maxillary third molars and maxillary canines
Classifications of impactions: One system employs a description of the angulationof the long axis of the impacted third molar with respect to the long axis of the second molar.• Mesioan ul % of all impacted teeth)• Distoangular (6% of all impacted teeth• Vertical (38% of all impacted teeth)• Horizontal (3% of all impacted teeth)***In addition, teeth can also be angled in a buccal or lingual direction. Note: Mostmandibular third molars are angled toward the lingual direction.
Impactions are also classified based on the relationship to bone and tissue:• Soft tissue impacted: impacted by soft tissue only• Partial bony impaction: crown is partially covered by bone• Full bony impaction: tooth completely covered by bone
The most common site for a supernumerary tooth is in the maxillary incisor area.When it occurs here, it is called a mesiodens. These teeth are usually small, pegshaped, and do not resemble the teeth normal to the site. Treatment is surgicalremoval.
ORAL SURGERY/PAIN CONTROLDrugs
Which of the following narcotics is contained in the analgesics Percodan andPercoset?
• Codeine• Oxycodone• Hydrocodone• Morphine
Copyright © 2001 - DENTAL DECKS
• Oxyeodone
This narcotic is also considered to have the highest dependency liability when compared to drugs such as codeine , propoxyphene and pentazocine.
Oxyeodone (contained in Percodan and Percocet) and Hydroeodone (contained inLorcet, Lortab and Vicodin) are 0eioids similar in structllre to mO~FJhine and codeine.• Pereodan (Oxycodone + aspirin) is the strongest pain medication you can prescribe
and have the patient still be ambulatory. Do not take on empty stomach.• Pereoeet (Oxycodone + acetaminophen)• Loreet, Lortab and Vieodin (Hydrocodone + Acetaminophen) all combine a...lli!!::
cotic analgesic and a cough reliever (hydrocodone) with a nonnarcotic analgesic(acetaminophen) for the relief of moderate to severe pain.
Codeine is a narcotic analgesic and antitussive (cough suppressant). It is weaker thanmorphine, less addictive , and less constipat ing. Codeine is usually combined with otherdrugs, for example , Empirin (Aspirin + Codeine) , and Tylenol #2, 3, and 4(Acetaminophen + Codeine)
ORAL SURGERY/PAIN CONTROLDrugs
Acetaminophen and propoxyphene are used together to treat moderate to severepain due to:
• Dental procedures• Headache• Back pain• Arthralgias• Myalgias• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above ( Ol\ ct\JoN)/,CI?10 """ N OPt\ , 1'J 1 (, flo l' o lC Y~HE"~'E
This combination of acetaminophen and propoxyphene is called Darvocet·N or Wygesic. Thesecompounds are mild narcotics and analgesics prescribed for the relief of moderate to severepain, with or without fever. Note : Darvon compound-55 is a combination of aspirin, caffeine, andpropoxyphene.
Acetaminophen (Tylenol) is a non-salicylate analgesic with similar analgesic potency asNSAIDs. Propoxyphene (Oarvon) is an oral synthetic opioid analgesic structurally similar tomethadone. Note: The combination of acetaminophen and propoxyphene produces additiveanalgesia as compared to the same doses of either agent alone.
Notes:1.' cetaminophen has anti retic and anal esic ro erties but no anti-inflammatory proper
ties. It does no e ect clotting time as does aspirin.2. Aspir in is an anti inflammatory, antipyretic and analgesic that is used to relieve headaches,
toothaches, and minor aches and pains, and to reduce fever. The GI tract rapidly absorbs it.3. Talwin compound combines the strong analgesic properties of pentazocine and the anal
gesic, anti-inflammatory, and fever-reducing properties of aspirin. It is used for the relief ofmoderate pain. It does not produce euphoria.
4. The most appropriate time to administer the initial dose of an analgesic to control postoperative pain is before the effect of the local anesthetic wears off.
ORAL SURGERY/PAIN CONTROL
Diazepam (Valium) can be used for:
• Candida albicans infections• Sedation induction• Hypothyroidism diagnosis• Myasthenia gravis
Copyright © 2001 - DENTAL DECKS
Drugs

• Sedation Induction
Benzodiazepinessuch as diazepam (Valium), chlordiazepoxide (Librium), lorazepam (Ativan),clonazepam (Rivotri/), f1urazepam (Dalmane), temazepam (Restoril) , triazolam (Halcion),alprazolam (Xanax), and midazolam (Versed) are medications that are frequently prescribed forthe symptomatic treatment of anxiety and sleep disorders. They produce their effects via specitic receptors involving GABA. Benzodiazepines are the most effective oral sedative drugs usedin dentistry.
Benzodiazepines, particularly diazepam and chlordiazepoxide are frequently prescribed forpreoperative sedation. These drugs are tranquilizers and are " sed to produce consciollSsedation in anxious patients. Diazepam is more potent than chlordiazepoxide, These drugs do notproduce hangovers like barbiturates and other sedative drugs. Note: Do not use these drugsduring the first trimester of pregnancy.
Important: Be careful when administering any sedative drug to a patient who is taking a phenothiazine drug (i.e., Chlorpromazine , Fluphenazine , Prochlorperazine). These drugs willpotentiate the action of sedative drugs.
Notes:1. Chloral hydrate is a sedative and hypnotic that is widely used for pediatric sedation.2. Emotional stress decreases the rate of absorption of a drug when given orally.
ORAL SURGERY/PAIN CONTROLDrugs
Ultrashort-acting barbiturates produce loss of consci ousness by depression of the:
• Medulla oblongata• Ascending portion of the reticular activating system• Substantia nigra• Descend ing portion of the reticular activating system
Copyright © 2001 - DENTAL DECKS
• Ascending portion of the reticular activating system
The reticular activating system is a functional (rather than morphologic) system in the brainessential for wakefulness , attent ion, concentration, and introspection. 8. network of nerve fibersin the thalamus . hypothalamus , brain stem, and cerebral cortex contribute to the system .
Ultrashort-acting barbiturates: 84~m+ts" StJ.d1)r-~~'c:;s• Thiopental (Pentothal)• Thiamylal (Surital)• Methohexital (Brevital)
Short-acting barbiturates:• Pentobarbital (Nembutal)• Secobarbital (Seconal)
Long-acting barbiturates:• Phenobarbital
(Generally not used in oral surgery)
Important: Barbiturates are contraindicated in patients with respiratory disease or those whoare pregnant.
Note: Physical dependence is likely to develop with barbiturates if abused . The dependencehas a strong psychological as well as physical basis. Sudden withdrawal from high doses can befatal.
ORAL SURGERY/PAIN CONTROL
All of the following drugs are anticholinergic, except.
• Atropine• Benztropine• Scopolamine• Fenfluramine• Trihexyphenidyl• Dicyclomine• Glycopyrrolate• Ipratropium• Probanthine
Copy right © 2001 - DENTAL DECKS
Drugs
• Fenfluramine"'Fenfluramine is an anorexigenic agent
All ant icholinergic drugs interfere with the bind ing of acetylcholine at its receptor. The mostcommon method for categorizing anticholinergic drugs is to identify the ionization state of nitrogen (i.e., tertiary or quaternary) because this affects the drug's ability to penetrate the CNS.Atropine, scopolamine, benztropine, dicyclomine, and trihexyphenidyl are all tert iary compounds, while glycopyrrolate , ipratropium, and probanthine are quaternary. Note: As a general rule, lertiary compounds penetrate the CNS more read ily than do quaternary (i.e., ionized)compounds. One exception to this rule is atro pine, which at normal doses penetrates the CNSpoorly.
The principal therapeutic uses of anticho linergic drugs in dentistry are:• To decrease the flow of saliva during dental procedures• To decrease the secretion from respiratory glands during general anesthesia•••Atrop ine is the most commonly used anticholinergic drug for these purposes. Scopolaminepenetrates the CNS more readily than atropine but is rarely used.
Notes:1. A patient premedicated with atropine will exhibit mydriasis (dilated pupils)2. Atropine is contraind icated for nursing mothers and for patients with glaucoma.
ORAL SURGERY/PAIN CONTROLDrugs
Which of the following are physiolog ical symptoms of a patient taking barbiturates?
• Slurred speech• Shallow breathing• Sluggishness• Fatigue• Disorientation• Lack of coordination• Dilated pupils (mydriasis)• All of the above
Copyright © 2001 - DENTAL DECKSI
J
• All of the above
Barbiturates have two major effects:1. Sedative (which decreases anxiety)2. Hypnotic (which helps sleep)
Barbiturates depress the central nervous system, and this will last 3 to 8 hoursdepending on the dose. The barbiturates of choice for the dentist usually are the shortacting variety because the onset of sedation is short (approx. 30 minutes to an hour)and the duration of effect (3 to 4 hours) is more than sufficient for most dental procedures.
The following drugs should be avoided in a patient taking barbiturates: phenothiazines,alcohol, antihistamines, and antihypertensives. These drugs will enhance the eNSdepression of the barbiturates.
Note: After IV administration of an ultrashort-acting barbiturate (for example Brevital orPentothal), the last tissue to become saturated as a result of redistribution is fat(as compared to liver, brain, and muscle tissue).
Remember: Barbiturates are metabolized in the liver and are excreted by the kidney.
ORAL SURGERY/PAIN CONTROLDrugs
Of the following drugs, which is most likely to cause seizures as an adverse reaction?
• Aspirin• Morphine• Meperidine• Acetaminophen
Copyright ~ 2001 - DENTAL DECKS
• Meperidine (Demerol)" ' Note: This adverse effect is very rare
Meperidine (Demerol) is a potent narcotic analgesic prescribed for the relief of moderate to severe pain and as a cough suppressant. It is probably the mostly widely usednarcotic in American hospitals . It compares favorably with morphine, the standard fornarcotic analgesics. Meperidine is the most abused drug by health professionals.Note: It produces slight euphoria but no miosis.
Morphine is the standard drug to which all analgesic drugs are compared. It causeseuphoria, analgesia, and drowsiness along with miosis and respiratory depression.
ORAL SURGERY/PAIN CONTROL
Clinically, scopolamine is used to:
Drugs
• Prevent nausea and vomiting associated with motion sickness• Reduce salivation and excess bronchial secretions prior to surgery• Reduce spastic states in parkinsonism• Produce sedation and as a pre-anesthetic medication• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above***Scopolamlne is very effective for the prevention of motion sickness and this indication represents its most common clinical use.
Scopolamine, like atropine, is generally used in surgery as a premedication for itsantimuscarinic properties, usually in combination with an oplold or barbiturate.
When you premedicate a patient with Scopolamine, the following effects will be prolonged (similar to premedication with Morphine) :• Amnesia• Psychic sedation• Decreased salivation
Notes:1. Reduction of secretions occurs by competitive blockade of acetylcholine and other
cholinergic stimuli at cholinergic receptors sites on salivary and bronchial glands.2. Antagonism of acetylcholine on the sphincter and ciliary body in the eye, produces
mydriasis (dilation of pupils)
ORAL SURGERY/PAIN CONTROLDrugs
Therapeutic anticoagulation is administered to patients with all of the followingexcept
• Postmyocardial infarction• Cerebrovascular thrombosis• Asthma• Pulmonary thrombosis
Copyright © 2001 - DENTAL DECKS
• Asthma
Medical consultation is always indicated before oral surgery if the patient is currently receivinganticoagulant or antiplatelet therapy.
Anticoagulants include dicumarol , heparin , antithrombin III, enoxaparin, and warfarin.Remember: Aspirin and NSAID's both Inhibit platelet aggregation and if given to a patient taking an anticoagulant already, the effects can be life-threatening.
Important point for oral surgery: A patient who is on anticoagulant therapy (whether it is warfarin, heparin, aspirin, or an NSAID) will mostly likely have a prolonged prothrombin time{p r ) and bleeding time. For elective extractions, this patient should stop taking the anticoagulant for two to three days prior to extractions. Always check with the patient's attending physician before recommending this.
When oral surgery is performed on these patients the following steps may help to preventhemorrhage from occurring:
• Hemostatic agent placed within the socket• Multiple sutures in the surgical area• Intraoral pressure packs• Ice packs (extraoral)• The avoidance of mouth rinses• Soft diet
ORAL SURGERYIPAIN CONTROL
How long should one wait before obtaining a biopsy of an oral ulcer?
• 4 days• 7 days• 14 days• 30 days
Copyright © 2001 - DENTAL DECKS
Biopsy
• 14 days
Almost all oral ulcers caused by trauma will heal within 14 days. Therefore, anyulcer that is present for 2 weeks or more should be biopsied.
Biopsy is also indicated in the following instances:• Pigmented lesions (black/brown)• When tissue is associated with paresthesia, this is often an ominous sign.• If a lesion suddenly enlarges, it should be biopsied.
Note: Always aspirate a central bone lesion to rule out a vascular lesion. If a lesionseems compressible, pulsatible, blue, or a bruit is heard, beware of a vascular lesionand biopsy only under controlled hospital setting.
A stethoscope is used to listen for a bruit.
ORAL SURGERY/PAIN CONTROL
Which of the following are indications for biopsy?
Biopsy
• A lesion that persists for more than two weeks with no apparent etiologic basis• Persistent hyperkeratotic changes in surface tissues• Bone lesions not specifically identified by clinical and radiographic findings• A lesion that has the characteristics of malignancy• An inflammatory lesion that does not respond to local treatment after 14 days
(such as removing local irritant)• A persistent swelling , either visible or palpable, beneath relatively normal tissue• All of the above are indications for biopsy
Copyright © 2001 - DENTAL DECKS
• All of the above are indications for biopsy
Biopsy technique and surgical principles:
• Anesthesia: Block local anesthetic techniques are employed when possible; if not,infiltration may be used but the solution should be injected at least 1 cm away fromthe lesion.
• Tissue stabiization: Use fingers or clamps.• Hemostatsis: Gauze compresses (avoid high speed suction) .• Incision: Sharp scalpel.• Extent of incision: Obtain some normal tissue adjacent to lesion if possible.• Handling of tissue: Use a traction suture through the specimen, not tissue forceps
to avoid specimen trauma.• Specimen care: After removal, the tissue should be immediately placed in 10% for
malin solution that is at least 20 times the volume of the surgical specimen. Note:No other solution is acceptable.
ORAL SURGERY/PAIN CONTROL
Which of the following is not an indication for exicisional biopsy?
Biopsy
• A small lesion (less than 1 em in diameter)• A lesion that can be removed completely without traumatizi ng the tissue• When there is a suspicion of malignancy• A pigmented or small vascular lesion
Copyri ght © 2001 - DENTAL DECKS
• When there is a suspicion of malignancy
***This would be an indication for incisional biopsy.
An incisional biopsy is a biopsy that samples only a particular or representative part ofthe lesion. If the lesion is large or has different characteristics at different locations,more than one area of the lesion may need to be sampled.
Other Indications: If the area under investigation appears difficult to excise becauseof its extensive size (larger than 1 em in diameter) or hazardous location.
An excisional biopsy implies removal of the entire lesion at the time the surgical diagnostic procedure is performed. A perimeter of normal tissue surrounding the lesion isalso excised to ensure total removal.
ORAL SURGERY/PAIN CONTROLBiopsy
Which of the following is the fixative of choice used for a routine biopsy specimen?
• Hydrogen peroxide• Sodium hypochlorite• 10% formalin• Saline
Copyright © 2001 - DENTAL DECKS
• 10% Formalin
After removal, the tissue should be immediately placed in 10% formalin solution (4%formaldehyde) that is at least 20 times the volume of the surgical specimen. The tissuemust be totally immersed in the solution, and care should be taken to be sure that thetissue has not become lodged on the wall of the container above the level of formalin.
Types of biopsies:• Incisional - take only part of lesion } most often used for oral lesions• Excisional - entire lesion is removed• Needle - aspirational biopsy• Exfoliative cytology - pap smear
Remember: A negative incisional biopsy report of a highly suspicious oral lesionsuggests that another biopsy specimen is necessary in view of the clinical impressions.The key is a highly suspicious oral lesion.
Disord/CondORAL SURGERY/PAIN CONTROL
Rheumatic fever is:
• Inflammation of joints (arthritis) and the spleen (splenomegaly) resulting from astreptococcal infection, usually of the throat.
• Inflammation of joints (arthritis) and the parotid glands (parotitis) resulting from astaphylococcal infection, usually of the middle ear
• Inflammation of the jo ints (arthritis) and the heart (carditis) resulting from a streptococcal infection, usually of the throat.
• Inflammation of the joints (arthri tis) and the thyroid gland (goiter) resulting from astaphylococcal infection, usually of the blood.
Copyright © 2001 - DENTAL DECKS
• Inflammation of joints (arthritis) and the heart (carditis) resulting from a streptococcalinfection, usually of the throat. .
Rheumatic fever is a com Iication of an acute stre tococcal infection, almost always apharyngitis (sore throatLThe offending agent i re tococca 0 a so known as~
!" A, B-hemolytic StreptoCOCCIJS Although rheumatic fever may follow a streptococcal infection, itis not an infection. Rather, it is an inflammatory reaction to an infection, affecting many partsof the body such as joints, heart, and skin.
Rheumatic fever is most common in children (5-15 years old). The onset is usually sudden.Typically, symptoms begin several weeks after the disappearance of a streptococcal sore throat.The major symptoms of rheumatic fever are join pain (arthritis), fever, chest pain, or palpitations caused by heart inflammation (carditis), jerky, uncontrollable movements (Syndenham 'schorea), a rash (erythema marginatum) , and small bumps (nodules) under the skin. The treatment is penicillin and rest.
Heart inflammation (carditis), disappears gradually, usually within five months. However, it maypermanently damage the heart valves, resulting in rheumatic heart disease. The valve betweenthe left atrium and ventricle (mitral valve) is most commonly damaged. The valve may becomeleaky (mitral valve regurgitation), abnormally narrow (mitral valve stenosis) , or both. Note: thepulmonary valve is rarely Involved.
Note: A history of rheumatic fever should lead the dentist to an in-depth dialogue history seeking the presence of rheumatic heart disease (RHO). If RHD is present, antibiotic coverage is indicated to minimize the risk of subacute bacterial endocarditis (SSE).
ORAL SURGERY/PAIN CONTROLDisord/Cond
Management of an acute asthmatic ep isode occurring during oral surgery includes allof the following except
• Terminate all dental treatment• Position the patient in an erect or semi-erect position• Patient should administer their own bronchodilator using an inhaler• Administer nitroglycerin• Administer oxygen• Monitor vital signs
Copyright © 2001 - DENTAL DECKS
• Administer nitroglycerin" ' Nitroglycerin is given in the management of a patient having chest discomfort (possibleanginal attack)
Note: In most severe asthmatic attacks or when the patient's bronchodilator is ineffective, epinephrine (0.3 ml of a 1:1,000 dilution) can be injected 1M or SC.
Asthma is a syndrome consisting of dyspnea, cough, and wheezing caused by bronchospasm,which results from a hyperirritability of the tracheobronchial tree. There are two types: allergicasthma (most common form) and id iosyncrati c asthma.
Avoid the use of the following drugs : Aspirin, NSAID's, barbiturates, narcotics, and erythromycin (if patient is taking theophylline).
Important: Nitrous oxide is safe to administer to people with asthma and is especially indicated for patients whose asthma is triggered by anxiety. If pat ient is tak ing steroids, consult physician for the possible need for corticosteroid augmentation.
Note: The inhalation of a selective beta2-agonist (terbuta line, albuterol) is the preferred treatmentfor an acute asthmatic attack.
Status asthmaticus is the most severe clinical form of asthma, usually requiring hospitalization,that does not respond adequately to ordinary therapeutic measures. If not managed properly,chronic part ial airway obstruction may lead to death from respiratory acidosis (which is produced by hypoxemia and hypercapnea) .
Disord/CondORAL SURGERY/PAIN CONTROL
Which of the following are the most common causes of dehydration?
• Fever• Vomiting• Diarrhea• Heat exhaustion• All of the above
Copyri ght © 2001 - DENTAL DECKS
• All of the above···Dehydration may also occur as a result of burns, diabetes insipidus, or an acute infection.
Important: One of the cardinal signs of dehydration is polydipsia (excess ive thirst)
Dehydration is the loss of water and important blood salts like potassium (K-) and sodium (Ne').Vital organs like the kidneys, brain, and heart can't function without a certain amount of waterand salt.
Initially, a patient suffering from dehydration will clinically demonstrate only dryness of the skinand mucous membranes.
However, as dehydration progresses, the turgor (or fullness) of the skin is lost. If dehydrationpersists, oli guria (reduced urine output) occurs as a compensation for the fluid loss. More severe£!egrees of fluid loss are accompanied by a shift of water from the intracellular space to the extracellular space a process that causes severe cell dvsfunction, particularly in the brain.Systemic blood pressure falls with continuous dehydration, and declining perfusion eventuallyleads to death.
Fluids in several forms should be continually urged on the patient. In severely dehydrated individuals, they must get to the hospital right away. IV fluids will quickly reverse dehydration, andis often life saving in young children and infants.
Disord/CondORAL SURGERY/PAIN CONTROL
Which of the following are important points to remember in the management of a diabetic patient?
• Defer surgery until diabetes is well-controlled; consult physician• Schedule an early morning appointment and avoid lengthy appointments• Consult physician if any questions concerning modification of the insulin regimen
arise• Watch for signs of hypoglycemia• Treat infections aggressively• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the abovet '1Pt '!
Diabetes Mellitus is a complex disorder involving mostly carbohydrates (glucose) and lipidsowing primarily to a relative or complete lack of insulin secretion by the beta cells of the pancreas.
People with well-controlled diabetes are no more susceptible to infections than people without diabetes, but they have more difficulty containing infections (this is caused by altered leukocyte function).
Patients who take insulin daily and check their urine regularly for the sugar and ketones (controlled diabetics) usually can be treated in the normal manner without additional drugs or dietalterations.
Important: If any doubt exists as to the patient's medical status, consultation with the patient'sphysician is indicated. Do not assume anything.
Note:• The treatment of choice for hypoglycemia in an unconscious diabetic patient is IV injection
of 50% dextrose in water.• The treatment of choice for hypoglycemia in a conscious diabetic is the administration of an
oral carbohydrate (orange juice , cola beverages, candy bars, etc.)
Remember: Glossopyrosis (burning sensation in the tongue) and glossodynia (pain in thetongue) are symptoms that are seen in the diabetic patient. This is caused by the degenerationof the myelin sheaths of peripheral nerves.
Disord/CondORAL SURGERY/PAIN CONTROL
Atel ectasis can result from which of the following after a patient has undergone oralsurgery?
• Inactivity after surgery• Postoperative narcotic analgesics• An endotracheal tube which was misplaced during the oral surgery procedure• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
Atelectasisis is the collapse of a lung. It is the most common anesthetic complicationoccurring within the first 24 hours after surgery under general anesthesia. Symptomsinclude diminished breath sounds , fever, and increas ing dyspnea. Note: Prolongedatelectasis can lead to pneumonia.
Pneumothorax is the presence of air in the pleural cavity. It can occur as a postoperative complicat ion of aspiration of liquid vomitus into the trachea and the bronchi. Theonset of pneumothorax is accompanied by a sudden , sharp chest pain, followed by .difficult, rapid breathing , cessation of normal chest movements on the affected side,tachycardia, a weak pulse, hypotension, diaphoresis, and elevated temperature, pallor,dizziness, and anxiety.
Notes:1. Pneumonitis (inflammation of the lung) and atelectasis are two of the most com
mon causes of fever in a patient who has had general anesthesia.2. The most common post-op complication of outpatient general anesthesia is nau
sea.
ORAL SURGERY/PAIN CONTROL
Chronic bronchitis is primarily a disease of:
• Alcoholics• Cigarette smokers• Miners• Patients with a family history of allergy
Copyright © 2001 - DENTAL DECKS
Disord/Cond
• Cigarette smokers
Chronic Bronchitis is clinically defined as productive cough occurring for at leastthree months of the year for at least two consecutive years. This condition has astrong association with cigarette smoking (90% of all cases occur in smokers). Thebronchial glands are enlarged, causing excess secretion of mucus. Chronic bronchitis often leads to Cor pulmonale (enLargement of the right ventricle of the heart). airway narrowing, and obstruction along with the squamous metaplasia of the bronchialtree.
Important: Patients with chronic bronchitis may be predisposed to lung cancer (bronchogenic carcinoma).
Remember: Patients with chronic bronchitis (or any COPD) can have difficulty duringoral surgery. Many of these patients depend on maintaining an upright posture tobreathe adequately. They frequently experience difficulty breathing if placed in analmost supine position or if placed on high-flow nasal oxygen.
Disord/CondORAL SURGERY/PAIN CONTROL
Which tw o diseases below cause more than 60% of all cases of end-stage renal dis-ease in the United States? .
• Diabetes• Leukemia• High blood pressure (hypertension)• Pernicious anemia
Copy right © 2001 - DENTAL DECKS
• Diabetes• High blood pressure (hypertension)
End-stage renal disease (ESRD) is a condition in which there is a permanent and almost complete loss of kidney function. The kidney functions at less than 10% of its normal capacity. In endstage renal disease, toxins slowly build up in the body. Normal kidneys remove these toxins(i.e., urea and creatin ine) from the body through urine.
Patients with ESRD:• Are often on steroid therapy• Are more susceptible to post-op infections• Have an increased tendency to bleed"'When oral surgical procedures are undertaken on these patients, meticulous attention togood surgical technique is necessary to decrease the risks of excessive bleeding and infection.
Some important points to remember when treating patients with renal insufficiency and thoseon hemodialysis:• Avoid the use of drugs that are metabolized or excreted by the kidney.~ Do not use NSAID's (they are ne hrotoxic .
"' . p e d orm oral surgery e day after dialysis~ Consult physician for possibie prophylactic antibiotics.
Disord/CondORAL SURGERYIPAIN CONTROL
Which of the following is the most common cause of bleeding disorders?
• Polycythem ia vera• Thrombocytopenia• Myelofibrosis• Chronic myelocytic leukemia
Copyright © 2001 - DENTAL DECKS
• Thrombocytopenia
Thrombocytopenia is an abnormal condition in which the number of platelets isreduced. This condition is common in people with Idiopathic thrombocytopenic purpura (ITP) in which case an autoimmune disease causes very low platelet counts.
Clinical features:• Spontaneous appearance of purpuric or hemorrhagic lesions of the skin which may
vary in size from tiny, red pinpoint petechiae to purplish ecchymoses and even massive hematomas. Patients also exhibit a bruising tendency.
• Nosebleeds, GI bleeding, urinary tract bleeding.• Severe and often profuse gingival hemorrhage.• Petechiae also occur on the oral mucosa.
Important:Two concerns with doing surgery on these patients:• Post-operative hemorrhage caused by a decrease in blood platelets.• Patients with the chronic form may be on steroids and have adrenal insufficiency.
They may be unable to handle the stress of extractions.
Disord/CondORAL SURGERY/PAIN CONTROL
All of the following are causes of metabolic alkalosis except.
• Use of diuretics (thiazides, furosemide, ethacrynic acid)• Vomiting• Chronic renal failure• Overact ive adrenal gland (Cushing's syndrome or use of corticosteroids)
Copyright © 2001 - DENTAL DECKS
• Chronic renal failure
An abnormality in one or more of the pH control mechanisms can cause one of two major disturbances inacid-base balance.1. Ac idosis: is a condition in which the blood has too much acid (or too little base , frequently resulting in a
decrease in blood pH. When the pH of the blood falls be ow normal, which is around 7.3, the centralnervous system becomes so depressed that the person first experiences disorientation and later maybecome comatose. Note: The normal blood bicarbonate-carbonic acid ratio is 20:1. A 10:1 ralio indicates uncompensated acidosis. Severe acidosis always occurs during CPR.
2. Alkalosis: is a condition in which the blood has too much base (or too little acid); occasionally resultingin an Increase In blood pH. The major effect on the body is overexcitability of the nervous system. Thismay result in tetany (tonic spasm).
Depending on the cause ot the condition, acidosis or alkalosis may be respiratory or metabolic.
Metabolic acidosis is eJCcessilli blood acidity characterized by an inappropriately low level of blc'trf i&nate In theblood. Major causes include chronic renal failure, diabetic ketoacidosis, lactic acidosis. poisons and diarrhea.
Respiratory acidosis is excessive blood acidiw caused by a buildup of carbon dioxide in the blood as aresult of poor lung function or slow breathing (decrease in respiratory rate). Major causes include hypovenliIalion, emphysema, chronic bronchitis, severe pneumonia, pulmonary edema, and asthma. Treatmentof acidosis is ingestion of sodium bicarbonate.
Metabolic alkalosis is a condition in which the blood is alkaline because of an inappropriately high level ofbicarbonate. Major causes include vomiting acidic gastric contents or as a result of ingesting alkaline drugs.
Respiratory alkalosis is a condition in which the blood is alkaline because rapid or deep breathing resyltsJo a low blood carbon dlgx ide level Major causes include ItYperve nt ilatiQrl (from anxiety), pain, cirrhosis of the liver, low levels of oxygen in the blood (high altitude) , and aspirin overdose. Note: It is much lesscommon than respiratory acidosis. Treatment of alkalosis is ingestion of ammonium chloride.
ORAL SURGERY/PAIN CONTROLDisord/Cond
Diabetes Mellitus Type 2 is associated with all of the following characteristics. except:
• Normal or increased insulin synthesis• Onset in adulthood• Autoimmune origin• Associated with obesity• Rare ketoacidosis
Copyright © 2001 - DENTAL DECKS
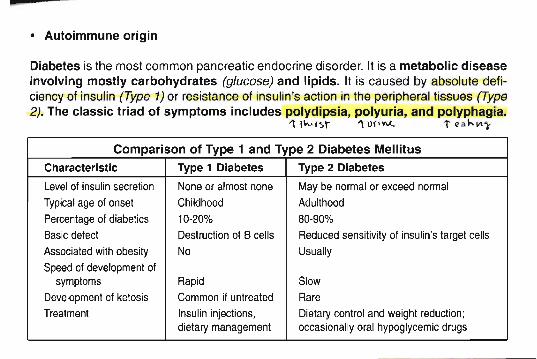
• Autoimmune origin
Diabetes is the most common pancreatic endocrine disorder. It is a metabolic diseaseinvolving mostly carbohydrates (glucose) and lipids . It is caused by abso lute deficiency of insulin (Type 1) or resistance of insulin's action in the peripheral tissues (Type2). The class ic triad of symptoms includes polydipsia, polyuria, and polyphagia.
" i\-V f ~r "\ UI'V\.(.. t ~a hV' ')-
Comparison of Type 1 and Type 2 Diabetes Mellitus
Characteristic Type 1 Diabetes Type 2 Diabetes
Level of insulin secretion None or almost none Maybe normal or exceed normalTypical age of onset Childhood AdulthoodPercentage of diabetics 10·20% 80·90%
Basic defect Destruction of B cells Reducedsensitivity of insulin's target cells
Associated withobesity No UsuallySpeed of development of
symptoms Rapid SlowDevelopment of ketosis Common if untreated RareTreatment Insulin injections, Dietary control and weight reduction;
dietarymanagement occasionally oral hypoglycemic drugs
Disord/CondORAL SURGERY/PAIN CONTROL
A serious condition in which the quantity of blood pumped by the heart each minute(cardiac output) is insufficient to meet the body's normal requirements for oxygenand nutrients is called:
• Heart block• Ventricular tachycardia• Congestive heart failure• Atrial fibrillation
Copyright © 2001 - DENTAL DECKS
• Congestive heart failure (CHF)
Usually the left ventr icle fails first, soon followed by right-sided failure. The commonsigns of CHF include :• Exertional dyspnea• Paroxysmal nocturna l dyspnea (patient wakes up gasp ing for air)**" These are the earliest and most common signs• Peripheral edema (swollen ankles)• Cyanosis• Orthopnea (sitting or standing in order to breathe comfortably)• High venous pressure
Patient treatment and dental management considerations:• Prolonged rest• Administration of oxygen• Digitalis (patients are prone to nausea and vomiting)• Diuretics/vasodilators (patients are prone to orthostatic hypotension; avoid exces
sive epinephrine)• Dicumarol (patients may have bleeding problem)
ORAL SURGERY/PAIN CONTROL
The unpleasant sensation of difficulty in breathing is called:
• Hypercapnea• Dyspnea• Hypocapnea• Apnea
Copyright © 2001 - DENTAL DECKS
Disord/Cond
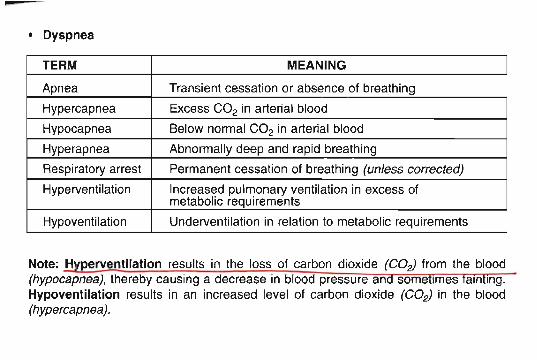
• Dyspnea
TERM MEANING
Apnea Transient cessation or absence of breathing
Hypercapnea Excess CO2 in arterial blood
Hypocapnea Below normal CO2 in arterial blood
Hyperapnea Abnormally deep and rapid breathing
Respiratory arrest Permanent cessation of breathing (unless corrected)
Hyperventilation Increased pulmonary ventilation in excess ofmetabolic requirements
Hypoventilation Underventilat ion in relation to metabolic requirements
Note: H perventilation results in the loss of carbon dioxide (COz) from the blood(hypocapnea), thereby causing a decrease in blood pressure an some irnes am Ing.Hypoventilation results in an increased level of carbon dioxide (COz) in the blood(hypercapnea).
Disord/CondORAL SURGERY/PAIN CONTROL
All of the following statements concerning hemophilia are true, except:
• Hemophilia A and B are inherited as a sex-linked recessive trait by which malesare affected and females are carriers.
• Bleeding time is abnormally prolonged• The majority of people afflicted with hemophilia have Type A and are under the age
of 25.• The signs, symptoms and clinical manifestations include excessive bleeding from
minor cuts, epitaxis, hematomas, and hemarthroses.• Chronic complications include impaired renal function and osteoarthritis.
Copyright © 2001 - DENTAL DECKS
---------------- - - - - - - - - - - - - - - ------ --
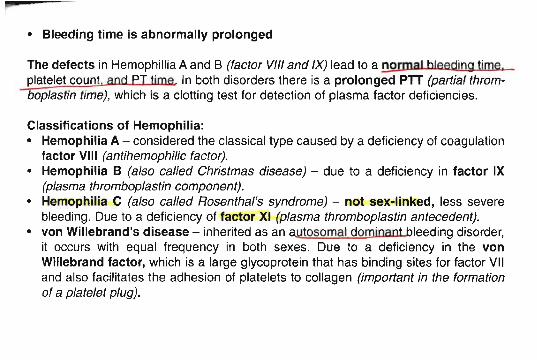
• Bleeding time Is abnormally prolonged
The defects in Hemophillia A and B (factor VIII and IX) lead to a normal bleeding time.platelet count. and PT time In both disorders there is a prolonged PTT (partial thromboplastin time), which is a clotting test for detection of plasma factor deficiencies.
Classifications of Hemophilia:• Hemophilia A - considered the classical type caused by a deficiency of coagulation
factor VIII (antihemophilic factor).. • Hemophilia B (also cal/ed Christmas disease) - due to a deficiency in factor IX
(plasma thromboplastin component).• Hemophilia C (also cal/ed Rosenthal's syndrome) - not sex-linked, less severe
bleeding. Due to a deficiency of factor XI (plasma thromboplastin antecedent).• von Willebrand's disease - inherited as an autosomal dominant bleeding disorder,
it occurs with equal frequency in both sexes. Due to a deficiency in the vonWillebrand factor, which is a large glycoprotein that has binding sites for factor VIIand also facilitates the adhesion of platelets to collagen (important in the formationof a platelet plug).
Disord/CondORAL SURGERYIPAIN CONTROL
Chronic obstructive pulmonary disease (COPO) is a group of disorders characterizedby airflow obstruction during respiration. Which one of those disorders listed belowis marked by dyspnea and wheezing expiration caused by episodic narrowing of theairways?
• Bronchial asthma• Chronic bronchitis• Emphysema• Bronchiectasis
Copy right © 2001 - DENTAL DECKS
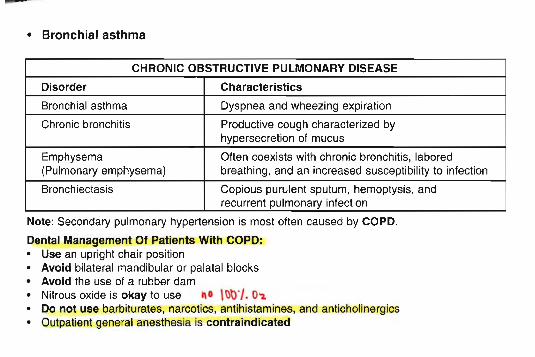
• Bronchial asthma
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Disorder Characteristics
Bronchial asthma Dyspnea and wheezing expiration
Chronic bronchitis Productive cough characterized byhypersecretion of mucus
Emphysema Often coexists with chronic bronchitis , labored(Pulmonary emphysema) breathing, and an increased susceptibility to infection
Bronchiectasis Copious purulent sputum, hemoptysis, andrecurrent pulmonary infection
Note: Secondary pulmonary hypertension is most often caused by COPD.
Dental Management Of Patients With COPD:• Use an upright chair position• Avoid bilateral mandibular or palatal blocks• Avoid the use of a rubber dam• Nitrous oxide is okay to use ,,0 \t)~r/. 0"2.• Do not use barbiturates, narcotics, antihistamines, and anticholinergics• Outpatient general anesthesia is contraindicated
Disord/CondORAL SURGERYIPAIN CONTROL
Which type of shock listed below is most often associated with severe trauma andreactive peripheral vasodilation?
• Hypovolemic shock• Cardiogenic shock• Septic shock• Neurogenic shock• Anaphylactic shock
Copyright © 2001 - DENTAL DECKS
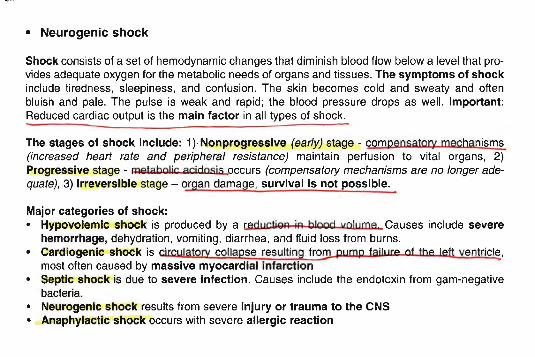
• Neurogenic shock
Shock consists of a set of hemodynamic changes that diminish blood flow below a level that provides adequate oxygen for the metabolic needs of organs and tissues. The symptoms of shockinclude tiredness, sleepiness, and confusion . The skin becomes cold and sweaty and oftenbluish and pale. The pulse is weak and rapid; the blood pressure drops as well. Important:Reduced cardiac output is the main factor in all types of shock .
The stages of shock include: 1)·Nonprogressive (early) stage - compensatory mechanisms(increased heart rate and peripheral resistance) maintain perfusion to vital organs, 2)Progressive stage - I+Iptabo1ic acidosis occurs (compensatory mechanisms are no longer adequate), 3) Irreversible stage - organ damage , survival Is not possible.
Major categories of shock:• Hypovolemic shock is produced by a red!lc' iQR iR bloOd volume Causes include severe
hemorrhage, dehydration , vomiting, diarrhea, and fluid loss from burns.• Cardiogenic shock is circulatorv collapse resulting froQl.. pump failllrP of the left ventricl~ ,
most often caused by massive myocardial infarction• Septic shock is due to severe infection. Causes include the endotoxin from gam-negative
bacteria.• Neurogenic shock results from severe injUry or trauma to the CNS• Anaphylactic shock occurs with severe allergic reaction
ORAL SURGERY/PAIN CONTROL
All of the following are elements of general anesthesia except.
• Analgesia• Relaxation• Hyperpyrexia• Hyporeflexia• Narcosis
Copy right @ 2001 - DENTAL DECKS
Anesth
• Hyperpyrexia (an elevated body temperature)
The four elem ent s of genera l anesthesia are:1. Analg es ia (the Jack of pain without loss of consciousness). Note: The best monitor of the
level of analgesia is the verbal response.2. Relaxat ion3. Hyporeflexia (weakening of the reflexes)4. Narco sis
"'Only analgesia, relaxation, and hyporeflexia are met by using local anesthetics. Narcosis canonly be reached when local anesthetics are given in a toxic dose or IV.
Notes:1. The medulla is the last area of the brain to be depressed during general anesthesia. This area is
the most vital part of the brain and contains the cardiac, the vasomotor, and respiratory centers ofthe brain.
2. The most reliable sign of "oxygen want " while monitoring a patient during general anesthesia isan increased pulse rate. Cyanosis may also be present.
3. The emergency most frequently experienced during outpatient general anesthesia is respiratoryobstruction.
4. The best anesthetic technique used in oral surgery to avoid aspiration of blood or other debris whena patient is under general anesthesia is endotracheal Intubation with pharyngeal packs.
5. A patient with an acute resp iratory Infection is contraindicated for general anesthesia.6. The eyes are taped shut prior to draping a patient before surgery to prevent .comeal abrasion.
ORAL SURGERY/PAIN CONTROL
A complete blood count (CSC) includes:
• Hematocrit• Hemoglobin• White blood cell count• Red blood cell count• All of the above
CoPvrlght © 2001 - DENTAL DECKS
Anesth
• Total leukocytes (WBC's)Normal = 5,000-10 ,OOO/mm3
Dental Infection = 15,000-20,000/mm3
• Total erythrocytes (RBC's)- Normal men = 5.0 (4.5-6.0)x106/mm3
- Normal women =4.5 (4.3-5.5)x1()6/mm3
• All of the above
The CBC and urina lys is are two tests that should be done before deciding whether to use a general anesthetic for surgical procedures on a patient. Note : If a bleeding problem is suspected the PIT (partialthrombop lastin time) should also be evaluated.
Complete blood co unt (CBC) inc ludes:• Hematocrit (the volume percentage of
red blood cells in whole blood)- Normal men = 45-50 percent- Normal women = 40-45 percent
• Hemoglobin- Normal men = 14-18 g1dL- Normal women = 12-16 g1dL
Important: The mini mal acceptable val ue fo r the hematocrit is 30 percent for elective surgery.
Normal values for coagulati on:• Template bleeding time = 1 to 9 minutes• Prothrombin time (PT) = 11 to 16 seconds (compared to normal control)• Partial thromboplastin time (PIT) = activated, 32-46 seconds (compared to normal control)• Platelets =140,000 to 440,OOO/ml
Urine values :• pH =6.0 (4.7-8.0)• specific gravity = 1.005 to 1.025
ORAL SURGERY/PAIN CONTROL
Stage I of anesthesia describes which level of sedation?
• Unconscious sedation• Conscious sedation
Copyright © 2001 - DENTAL DECKS
Anesth
• Conscious sedation
Geude l's stages of anesthesia:
• Stage I (amnesia and analgesia) - begins with the administration of anesthesia and continues to the loss of consciousness. Respiration is quiet, though sometimes irregular, andreflexes are still present.
• Stage II (delirium and excitement) - begins with the loss of consciousness and includesthe onset of total anesthesia. During this stage the patient may move his limbs, chatter incoherently, hold his breath, or become violent. Vomiting with the attendant danger of aspirationmay occur. The patient is brought to Stage III as quickly and smoothly as possible.
• Stage III (surgical anesthesia) - begins wi th establishment of a regular pattern of breathing and total loss of consciousness and includes the period during which signs of respiratoryor cardiovascular failure first appear. This stage has four planes.
• Stage IV (premortem) - signals danger. This stage is characterized by pupils that are maximally dilated and skin that is cold and ashen. Blood pressure is extremely low, often unrneasurable. Cardiac arrest is imminent. Remember: The eyes appear greatly enlarged in sizeand nonreactive to bright light when functional circulation to the brain has stopped.
- ~~---- ---- - --- - - - - - - ---'
ORAL SURGERY/PAIN CONTROL
Which of the following will produce neurolept anesthesia?
• Neuroleptic agent + narcotic analgesic• Neuroleptic agent + nitrous oxide• Neuroleptic agent + narcotic analges ic + nitrous oxide• Narcotic analgesic + nitrous oxide
Copyright © 2001 - DENTAL DECKS
Anesth
• Neuroleptic agent + narcotic analgesic + nitrous oxide
Neurolept anesthesia is a state of neurolept analgesia and unconsciousness, produced by the combined administration of a narcotic analgesic and a neurolept ic agent,together with the inhalation of nitrous oxide and oxygen.
-)(Neurolept analgesia only produces an unconscious state if nitrous oxide is alsoadministered. (see below)
Neuroleptic agent + narcotic analgesic = neurolept analgesia(Droperidol) (Fentanyl) (conscious)
Under the influence of this combination, the patient is sedated and demonstratespsychic indifference to the environment yet remains conscious and can respond toquestions and commands.
Neurolept + nitrous oxide = neurolept anesthesiaanalgesia in oxygen (unconscious)
Induction of anesthesia is slow, but consciousness returns quickly after the inhalation of nitrous oxide is stopped.
AnesthORAL SURGERY/PAIN CONTROL
Inadvertent intravascular injection of a local anesthetic with a vasoconstrictor maycause which of the following clinical signs?
• Nervousness• Tremors• Dizziness• Blurred vision• Excitation and/or depression of the eNS• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above
These signs may be followed by:• Drowsiness• Convulsions• Unconsciousness• Possible respiratory arrest
Remember: Injections should always be made slowly with aspiration to avoidintravascular injection. This will prevent systemic reaction to both local anestheticandvasoconstrictorused in many solutions. The presence of a vasoconstrictor doesnot prevent an intravascular injection or systemic absorption. The acute intravenous toxicity of a local anesthetic agent with a vasoconstrictor may be higher thanthat of the anesthetic agent by itself. If drowsiness is apparent after administration ofa local anesthetic, then the reaction is probably due to the toxic effect of the anesthetic as opposed to a psychogenic reaction.
Note: In local anesthesia, the depression of respiration is a manifestation of thetoxic effects of the solution.
AnesthORAL SURGERY/PAIN CONTROL
All of the following are advantages of using nitrous ox ide analgesia except
• Rapid onset and recovery• Pleasant induction• It is a complete pain reliever• Nonirritating to the GI tract
Copyri ght © 2001 - DENTAL DECKS
• It is a complete pain reliever
Other advantages of using nitrous oxide analgesia include:
• Good analgesia • It has virtually no adverse effects• It is nonflammable in the absence of hypoxia• It is suitable for all ages and therapeutic • It is tltratable and produces euphoria
for many medically compromised patients
Nitrous oxide is a colorless, nonirritating gas with a pleasant, mild odor and taste. It has a blood/gaspartition coefficient of 0.47 and is thus poorly soluble in blood. It is excreted unchanged by thelungs. It is the oldest gaseous anesthetic in use today. It is the only inorganic substance used as ananesthetic. Its primary disadvantage as a general anesthetic is its lack of potency.
Notes:• Nitrous oxide should be stored under pressure in steel cylinders painted blue.• Oxygen is stored in green tanks.
Disadvantages of nitrous oxide (N~) analgesia:• There is a "misuse" potential with both patients and dentists.• It is not a complete pain reliever; a local anesthetic is still required to do most dental procedures.• The most common patient complaint is nausea.• Diffusion hypoxia may occur; make sure you give 100% oxygen at the end of dental procedure
to prevent it. Important: The inhalation of 100% oxygen is contraindicated for a person who haschronic obstructive pulmonary disease.
AnesthORAL SURGERY/PAIN CONTROL
The initial event in a vasovagal syncope episode is the stress- induced release ofincreased amounts of catecholamines that cause all of the following except
• A decrease in peripheral vascular resistance• Tachycardia• Sweating• Bradycardia
Copy right © 2001 - DENTAL DECKS
• Bradycardia
"'Bradycardia appears after the initial event in a vasovagal syncope episode.
The most common emergency seen after the use of local anesthetics is syncope(fainting) . The patient may complain of feeling a generalized warmth with nausea andpalpitations.
As blood pools in the periphery, a drop in blood pressure appears , with a corresponding decrease in cerebral blood flow. The patient will then complain of feeling dizzy orweak. Compensatory mechanisms attempt to maintain adequate blood pressure, butthey soon fatigue, which leads to vagally mediated bradycardia. Once the blood pressure drops below levels necessary to sustain consciousness , syncope occurs.
Placing the patient in a supine position together with the administration of 100% oxygen is often all that is required. Additional treatment is based on symptoms.
Note: The primary airway hazard for an unconscious dental patient in a supine position is tongue obstruction. Remember: Head tilVchin lift.
AnesthORAL SURGERY/PAIN CONTROL
Which of the following is the maximum allowable dose for 2% lidocaine with 1:100,000epinephrine?
• 2.0 mg lidocaine/per lb.• 3.5 mg lidocaine/per lb.• 6.0 mg lidocaine/per lb.• 7.0 mg lidocaine/per lb.
Copyright © 2001 - DENTAL DECKS
• 3.5 mg lidocaine/per lb.
For example: 70 lb. Patient x 3.5 mg =245 mg (maximum allowable dosage) + 36 mg(amount of Lidocaine in 2% carpule) = approximately 7 carpules.
Note: 1 kg =2.2 pounds
For carbocaine without epinephrine, the maximum allowable dose is 3.0 mgllb.
Remember:The maximum allowable dose of epinephrine that can be administered to a cardiacrisk patient is 0.04 m9:. In terms of local anesthetics this would be equivalent to:
1 carpule (1.8 cc) with anesthetic cone. 1:50,0002 carpule (3.6 cc) wi anesthetic cone. 1:100,0004 carpule (7.2 cc) wi anesthetic cone. 1:200,000
ORAL SURGERYIPAIN CONTROLAnesth
The following signs are indicative of a patient having which type of reaction (a somato genic reaction or a psychogen ic reaction) ?
• Nausea• Pallor and cold perspirat ion• Widely dilated pupils• Eyes rolled up• Brief convuls ions
Copyright © 2001 - DENTAL DECKS
• A psychogenic reaction···A psychogenic reaction is caused by psychological factors rather than physical factors(drugs)
Vasovagal syncope, a psychogenic reaction, is the most commonly experienced complicationassociated with the use of local anesthetic solutions. The clinical signs closely resemble those ofshock. These psychogenic reactions readily respond to placing the patient in a supine position.
The foll owing dru gs, when administered on e hour prior to the dental appointment , are safe andeffective ways to allay the fears of an apprehensive adult dental patient and possibly avoid apsychogenic reaction in the dental chair:• Diazepam (Valium): 5-10 mg orally (PO)• Pentobarbital (Nembutal): 50-100 mg orally (PO)• Secobarbital (Seconal): 50-100 mg orally (PO)• Promethazine (Phenergan): 25 mg orally (PO)
···Note dosa ges and route of admin istration.
These drugs are not recommended un less you have experience with them and can handle anycomplications that may happen from their use.
Note: A somato genic reaction is the development of a reaction from an organic pathophysiologic cause.
AnesthORAL SURGERYI PAIN CONTROL
Phlebitis of a vein after administration of IV valium is usually attributed to the presence of which of the following in the mixture?
• Hydroquinone• Water• Alcohol• Propylene glycol
Copyright © 2001 - DENTAL DECKS
• Propylene glycol
Phlebitis (also called thrombophlebitis), which is irritation or inflammation of a yeio. issometimes seen after IV administration of valium. This is usually attributed to the presence of propylene glycol in the mixture .
Phlebitis is more likely to occur if a vein in the hand or wrist is used and may be morecommon following repeated injections, especially in heavy smokers, the elderly, andwomen taking oral contraceptives.
Clinical observations of phlebitis:• The vessel feels hard and thready or cord-like• The site is extremely sensitive to pressure• The surrounding area may be erythematous and warm to the touch• The entire limb may be pale, cold, and swollen
Treatment: Elevate limb, apply moist heat, and possibly use anticoagulants.
AnesthORAL SURGERY/PAIN CONTROL
Postoperative hypotension may be due to the effect of:
• Transfusion reactions• A fat embolism• The anesthetic or analgesics on the myocardium - >~wr to~ ...o~ fl\ t..""{o1l..
• Liver failure• Anaphylaxis• All of the above
Copyright © 2001 - DENTAL DECKS
• All of the above***It is usually due to the effect of the anesthetic or analgesics on the myocardium.
The treatment is narcan (a narcotic antagonist) if hypotension is due to narcotics . Useatropine (an anticholinergic) if bradycardia is present.
Note: Postoperative~ension is most often due to post-op pain. Treat with narcotics and sedatives. Other causes include hypercarbia (greater than normal amountsof carbon dioxide in the blood), or administration of a vasopressor or catecholamineagents.
AnesthORAL SURGERY/PAIN CONTROL
All of the following drugs can reduce salivary flow during dental treatment. Which one,however, works by reducing anxiety and sensitivity during the procedure?
• Scopolamine• Atropine• Local anesthesia• Benztropine
Copyright © 2001 - DENTAL DECKS
• Local anesthesia
Local anesthesia acts by reducing sensitivity which therefore reduces the anxiety andstress related to treatment; salivation is also decreased.
Scopolamine, atropine and benztropine are anticholinergic drugs. Not only do theydecrease the flow of saliva, but also decrease the secretion from respiratory glandsduring general anesthesia.
AnesthORAL SURGERY/PAIN CONTROL
Which of the following is a peculiar thermal alteration that occurs during surgery insusceptible persons?
• Malignant hypothermia• Heat stroke• Malignant hyperthermia• Hyperreflexia
Copyright © 2001 - DENTAL DECKS
• Malignant hyperthermia
Malignant hyperthermia is an autosomal dominant inherited cond ition, occurring inpatients undergoing general anesthesia. It is characterized by a sudden, rapid risein body temperature assoc iated with signs of increased muscle metabolism, such astachycardia , tachypnea, sweating, and cyanosis; increased carbon dioxide production;and usually muscle rigidity. It occurs usually in apparently healthy children and youngadults at an average age of 21 years . There is no sex differential.
Treatment includes the admin istration of Dantrolene and 100% oxygen , coo ling procedures, and the correction of acidosis and hyperkalemia. People who have malignanthyperthermia are informed of their condition and advised that one-half of their firstdegree relatives are likely to have the trait.

ORAL SURGERY/PAIN CONTROL
Ketamine is most common ly used to obtain:
• Neuroleptanesthesia• Local anesthesia• Dissociat ive anesthesia• Regional anesthesia
Copyright © 2001 - DENTAL DECKS
Anesth
• Dissociative anesthesia
Ketamine hydrochloride (Kela/ar) is a rapid acting, non-barbituate , parenterally admin~anesthet ic that produces dissociative anesthesia. Dissociative anesthesia ischaracterized by analgesia and amnesia wi th out the loss of respiratory fllOction Or.
"pharyngeal and laryngeal reflexes. The patient appears to be awake, but detachedfrom the environment and unresponsive to pain. Ketamine administration produces acatatonic state in which the patient does not respond to noxious stimuli .
Ketamine is particularly useful for brief, minor surgical procedures and for the inductionof inhalation anesthesia .in pediatric geriatric and disturbed patients The onset ofaction is about 1 minute after IV injection and 5 minutes after 1M injection. The durationof anesthesia is about 5 to 10 minutes for IV, and 10 to 20 minutes for 1M. Recoverytakes much longer. There are no known antagonists.
Ketamine:• Increases secretions of the salivary and bronchial glands• Increases BP, muscle tone and heart rate, but not respirations• Side effects include: hypertension, increased pulse and delirium
AnesthORAL SURGERY/PAIN CONTROL
Which drug listed below is most commonly used to attain general anesthesia?
• Valium• Chloral Hydrate• Phenergan• Brevital
Copyright © 2001 - DENTAL DECKS
• Brevital (Methohexital)
Brevital is an IV barbiturate and is prescribed for the induction of anesthesia in shortsurgical procedures as a supplement to other anesthetics . 1.1 is metabol ized in the liver
..and excreted by the kidney Brevital induction is characterized by being rapid andthere is also rapid recovery. The side effect most often seen is hiccoughs. This isbelieved to be caused by rapid injection of the Brevital. Note: A primary advantage ofIV sedation is the ability to titrate individualized dosage.
The general anesthetics most frequently used are inhalation alone, barbiturates alone,barbiturates with oxygen, and nitrous in combination with a more potent agency suchas halothane. In addition, a local anesthetic is sometimes used for vasoconstriction andto decrease the amount of barbiturate used in lengthy procedures.
Note:The most effective agent in the initial treatment of respiratory depression dueto overdose of barbiturates is oxygen under positive pressure.
Some reasons to use sedation :• For a patient who is very apprehensive or scared• To decrease stress in a medically compromised patient• To perform several procedures on a patient who is extremely anxious
ORAL SURGERY/PAIN CONTROL
All of the following are considered to be what type of anesthetic?
• Nitrous Oxide• Cyclopropane• Ethylene• Halothane• Isoflurane• Methoxyflurane
Copyright © 2001 - DENTAL DECKS
Anesth
• Inhalation anesthetics
Inhalation anesthetics are drugs inhaled as gases or vapors. These diverse drugs arerelatively simple lipophilic molecules, ranging from the inorganic agent nitrous oxide(N20 ) to ethers such as ethyl ether, hydrocarbons such as cyclopropane and halogenated hydrocarbons such as halothane.
Administration of an inhalation anesthetic (except nitrous oxide) is usually preceded by intravenous or intramuscular administration of a short acting sedative hypnoticdrug, often a barbiturate. The procedure almost always requires endotracheal intubation.
Cyclopropane, halothane and methoxyflurane are inhalation general anestheticsthat have a relatively low therapeutic index, but their clinical safety is greatly increasedby the extreme ease in reversing tissue concentration . General anesthesia withhalothane is commonly preceded by administration of atropine to reduce salivation andbronchial secretions caused by halothane.
The rapidity of anesthesia with an inhalation anesthetic agent is primarily related toits degree of blood solubility.
Inhalation anesthetics are absorbed and primarily excreted through the lungs.
AnesthORAL SURGERY/PAIN CONTROL
All of the following are contraindications to the use of nitrous oxide excep t.
• Hypoxemia• Respiratory disease• Children• Emotional instability• Contagious diseases
Copyright © 2001 - DENTAL DECKS
• Children
*** Nitrous oxide is very appropriate for use on a child who is fearful and timid.
Nitrous oxide is contraindicated in patients with:1 Hypoxemia - an abnormal deficiency of oxygen in the arterial blood2. Respiratory disease (emphysema, asthma , upper respiratory obstruction)3. Emotional instability4. Contagious diseases (can't sterilize entire tube)
Nitrous oxide is a gas used as an anesthetic in surgery. It provides light anesthesia and is deliveredin various concentrations with oxygen. Nitrous oxide alone does not provide deep enough anesthesiafor major surgery, for which it is supplemented with other anesthetic agents. It is often given for induction of anesthesia, preceded by the administration of a barbiturate or an analgesic narcotic. Inductionand recovery are both rapid. Note: Sedation can rapidly be reversed when using inhalation as theroute for administration of drugs.
Nitrous oxide is the only safe conscious sedation technique for the pregnant patient (use onlyin second and third trimester). Barbiturates, narcotics, and tranquilizers all pass the placental barrier.Note: Elective extractions in pregnant patients is contraindicated.
The most common complication associated with nitrous oxide sedation is a behavioral problem(laughing, giddy). .
The difference between conscious sedation and general anesthesia as far as patient response isconcerned: the patient retains all his reflexes under conscious sedation, but not under general anesthesia.
AnesthORAL SURGERYIPAIN CONTROL
Which local anesthetic listed below may possibly manifest its toxicity clinically by initialdepression and drowsiness rather than stimulation and convuls ion?
• Lidocaine• Procaine• Benzocaine• Tetracaine
Copyright © 2001 - DENTAL DECKS
• Lidocaine
The initial effect upon the brain for local anesthetics is usually stimulation and then depression.However, it is also possible that the excitatory phase of the reaction may be extremely brief ormay not occur at all. This is true especially with lidocaine and mepivacaine. With theseagents, patients exhibit drowsiness. Also note that lidocaine and mepivacaine can also showcross-allergy.
Allergic reactions to amide type local anesthetics are rare but may occur as a result of hypersensitivity to the local anesthetic agent itself or due to an allergy to methylparaben or otherpreservatives used in many solutions. These reactions are characterized by cutaneouslesions of delayed onset or urticaria, edema, and other manifestations of allergy.
Amide type local anesthetics undergo biotransformation in the liver by microsomal enzymes butsome is excreted unchanged (10-20%). Ester type local anesthetics undergo rapid biotransformation in the blood plasma. The major portion of this inactivation process occurs within theblood through hydrolysis to paraaminobenzoic acid by the enzyme pseudocholinesterase.Patients with pseudocholinesterase inactivity are unable to detoxify ester type agents at a normal rate. Amide type anesthetics are recommended in these patients.
Important: For those patients allergic to both ester and amide type local anesthetics,Diphenhydramine is a safe and effective alternative.
AnesthORAL SURGERY/PAIN CONTROL
How many milligrams of epinephrine are in each cartridge (1.8 cc) of 2% lidocainewith 1:100,000 epinephrine? •
• 0.018 mg• 18 mg• 0.036 mg• 36 mg
Copyright © 2001 - DENTAL DECKS
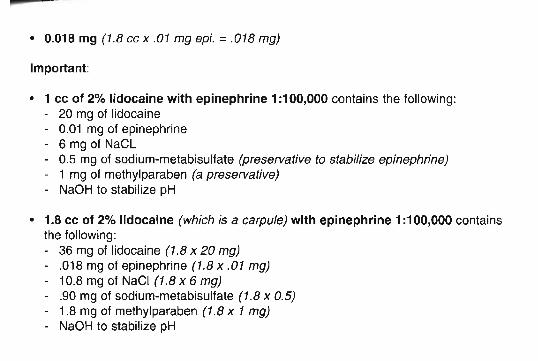
• 0.018 mg (1.8 cc x .01 mg epi. = .018 mg)
Important:
• 1 cc of 2% lidocaine with epinephrine 1:100,000 contains the following:- 20 mg of lidocaine- 0.01 mg of epinephrine- 6 mg of NaCL- 0.5 mg of sodium-metabisulfate (preservative to stabilize epinephrine)- 1 mg of methylparaben (a preservative)- NaOH to stabilize pH
• 1.8 cc of 2% lidocaine (which is a carpule) with epinephrine 1:100,000 containsthe following:- 36 mg of lidocaine (1.8 x 20 mg)- .018 mg of epinephrine (1.8 x .01 mg)- 10.8 mg of NaCI (1.8 x 6 mg)- .90 mg of sodium-metabisulfate (1.8 x 0.5)- 1.8 mg of methylparaben (1.8 x 1 mg)- NaOH to stabilize pH
AnesthORAL SURGERY/PAIN CONTROL
Which two of the following are useful for sedation and analgesia only?
• Halothane• Methoxyflurane• Cyclopropane• Nitrous oxide• Ethylene
Copyright © 2001 - DENTAL DECKS
• Nitrous oxide• Ethylene
Nitrous oxide: 10-20% (maximum 35%)-rapid induction and recovery.
Ethylene: 25-35%--rapid induction and recovery, not used often due to explosivenessand disagreeable odor.
Agents useful for surgical anesthesia:
Cyclopropane: 20-35% for stage 3, rapid induction and recovery, good muscle relaxant, sensitizes heart to catecholamines.
Halothane: 3% induction and 1-2% maintenance, relatively slow induction and recovery. Not a good muscle relaxant. Side effects include sensitizing heart to the catecholamines, hypotension and cardiac arrhythmias. Not a good analgesic, used as anadjunct. Note: Halogenated hydrocarbons are associated with liver damage if toxicdoses are used.
Methoxyflurane: 1-3%, slow induction and recovery, good muscle relaxant, sensitizesthe heart to catecholamines, respiratory depressant , good analgesic.
Note: Ventricular fibrillation is least likely to occur during anesthesia with nitrous oxide.The principal danger associated with the use of nitrous oxide anesthesia in concentrations exceeding 80% is hypoxia.
ORAL SURGERY/PAIN CONTROLAnesth
During an inferior alveolar nerve block injection, the needle passes through themucous membrane and the buccinator muscle and lies lateral to the:
• Masseter muscle• Temporalis muscle• Medial pterygoid muscle• Lateral pterygoid muscle
Copyright © 2001 - DENTAL DECKS
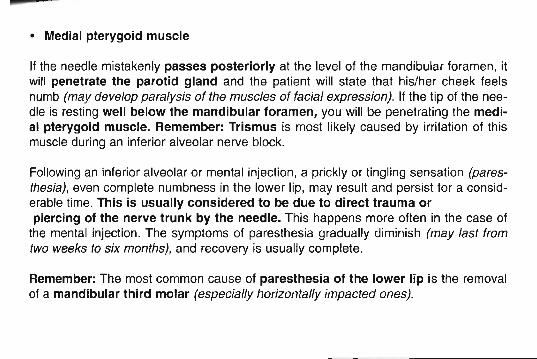
• Medial pterygoid muscle
If the needle mistakenly passes posteriorly at the level of the mandibular foramen, itwill penetrate the parotid gland and the patient will state that his/her cheek feelsnumb (may develop paralysis of the muscles of facial express ion). If the tip of the needle is resting well below the mandibular foramen, you will be penetrating the medial pterygoid muscle. Remember: Trismus is most likely caused by irritation of thismuscle during an inferior alveolar nerve block.
Following an inferior alveolar or mental injection, a prickly or tingling sensation (paresthesia), even complete numbness in the lower lip, may result and persist for a considerable time. This is usually considered to be due to direct trauma orpiercing of the nerve trunk by the needle. This happens more often in the case of
the mental injection. The symptoms of paresthesia gradually diminish (may last fromtwo weeks to six months), and recovery is usually complete.
Remember: The most common cause of paresthesia of the lower lip is the removalof a mandibular third molar (especially horizontally impacted ones).
AnesthORAL SURGERY/PAIN CONTROL
From the choices listed below, what are the two most important steps in the initialmanagement of a laryngospasm?
• Administering epinephrine• Applying oxygen under positive pressure• Administering succinylcholine• Placing the patient in the Trendelenburg position
Copyright © 2001 - DENTAL DECKS
• Applying oxygen under positive pressure• Administering succinylcholine
A patient under general anesthesia loses the laryngeal reflex. If blood and saliva collect near the voca l cords, this stimulates the patient to go into spasm (laryngospasm)and the vocal cords will close. When this happens , air cannot pass through and hencethe problem.
Note: Succinylcholine is a skeletal muscle relaxant that is used when performingendotracheal intubation and endoscopy procedures.
AnesthORAL SURGERY/PAIN CONTROL
All of the following are reasons that vasoconstrictors are included in local anestheticsexcept
• They prolong the duration of action of the local anesthetic• They reduce the chance of an allergic reaction to the local anesthet ic• They reduce the toxicity because less local anesthet ic is necessary• They reduce the rate of vascular absorption by causing vasoconstriction• They help to make the anesthesia more profound by increasing the concent ra
tions of the local anesthet ic at the nerve membrane.
Copyright © 2001 - DENTAL DECKS
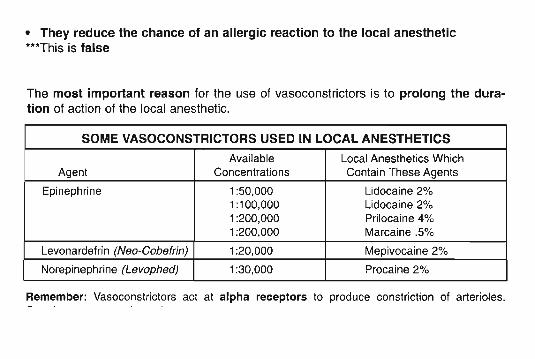
• They reduce the chance of an allergic reaction to the local anesthetic***This is false
The most important reason for the use of vasoconstrictors is to prolong the duration of action of the local anesthetic.
SOME VASOCONSTRICTORS USED IN LOCAL ANESTHETICS
Available Local Anesthetics WhichAgent Concentrations Conta in These Agents
Epinephrine 1:50,000 Lidocaine 2%1:100,000 Lidocaine 2%1:200,000 Prilocaine 4%1:200,000 Marcaine .5%
Levonardef rin (Neo-Cobefrin) 1:20,000 Mepivocaine 2%
Norepinephrine (Levophed) 1:30,000 Procaine 2%
Remember: Vasoconst rictors act at alpha receptors to produce constriction of arterioles.
AnesthORAL SURGERY/PAIN CONTROL
After receiving an injection of a local anesthetic containing 2% lidocaine with 1:100,000epinephrine, the patient loses consciousness. Which of the following is the most probable cause?
• Acute toxicity• Allergic response• Syncope• Hypervent ilation syndrome
Copy right © 2001 - DENTAL DECKS
• Syncope***Caused by transient cerebral hypoxia
Proper management of syncope:• Place patient in supine position with feet slightly elevated .• Establish airway (head tilt/chin lift)
- Administer 100% oxygen via face mask. O2 is indicated for treatment all types ofsyncope except hyperventilation syndrome.
• Monitor vital signs and support patient.- Pupils may dilate from brain not getting oxygen.
• Maintain your composure. Apply cool, wet towel to patient's forehead.• Follow-up treatment.
• Determine factors causing unconsciousness.
Remember: Hyperventilation in an anxious dental patient leads to carpodedal spasm(a spasm of the hand, thumbs, foot, or toes).
ORAL SURGERY/PAIN CONTROL
Local anesthetics depress small, nonmyelinated nerve fibers:
• First• Last• At the same time as large, myelinated nerve fibers• After the large, myelinated nerve fibers
Copyright © 2001 - DENTAL DECKS
Anesth
• First
***Local anesthetics depress large, myelinated nerve fibers last.
Variations in susceptibility of nerve fibers to local anesthetics are dependent on thediameter of the nerve and the distance between the nodes of Ranvier.
Clinically, the general order of loss of function is as follows:• Pain• Temperature (cold and warmth)• Touch/pressure• Proprioception• Skeletal muscle tone (motor)
Note: Nerves regain function in reverse order.~-_.::......----------
ORAL SURGERY/PAIN CONTROL
Nitrous oxide works on the:
• Peripheral Nervous System (PNS)• Central Nervous System (e NS)• Autonomic Nervous System (ANS)
Copyright © 2001 - DENTAL DECKS
Anesth
• Central Nervous System (eNS)
Nitrous oxide is the only inorganic gas used by the anesthesiologist. Room air contains 21% oxygen; you must make sure that the patient receives at least this muchoxygen. Maximal safe concentrations of nitrous oxide (70% nitrous / 30% oxygen)produce intoxication, analgesia, and amnesia.
Nitrous oxide is carried in the bloodstream in physical solution. There is no metabolism or degradation of nitrous oxide in the body. It is excreted solely via the lungs,unchanged. High blood levels of nitrous oxide can be achieved quite quickly. It is nontoxic to body tissues. The only toxicity with the use of nitrous oxide is the lack of oxygen that could result from the operator's error. The gag reflex is only slightly obtundedwith nitrous oxide analgesia. It is believed that nitrous oxide has its main effects onthe ~icylar activating system and the limbic system.
Remember:• The first symptom of nitrous oxide analgesia is tingling of the hands.• Nausea is the most common side effect of nitrous oxide analgesia.• The correct total liter flow of nitrous oxide/oxygen is determined by the amount
necessary to keep the reservoir bag 1/3 to 2/3 full.
ORAL SURGERY/PAIN CONTROL
What is usually the first clinical sign of mild lidocaine toxicity?
• Itching• Nervousness• Vomiting• Sleepiness
Copyrig ht © 2001 - DENTAL DECKS
Anesth
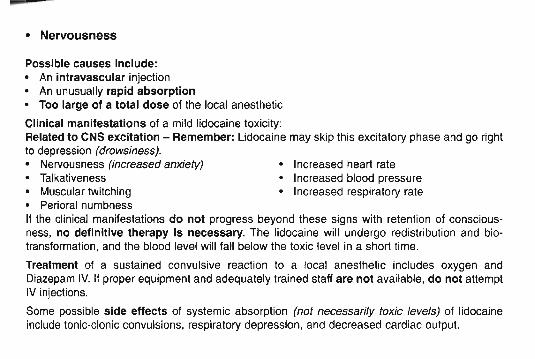
• Increased heart rate• Increased blood pressure• Increased respiratory rate
• Nervousness
Possible causes Include:• An intravascular injection• An unusually rapid absorption• Too large of a total dose of the local anesthetic
Clinical manifestations of a mild lidocaine toxicity:Related to CNS excitation - Remember: Udocaine may skip this excitatory phase and go rightto depression (drowsiness).• Nervousness (increased anxiety)• Talkativeness• Muscular twitching• Perioral numbnessII the clinical manifestations do not progress beyond these signs with retention of consciousness, no definitive therapy is necessary. The lidocaine will undergo redistribution and biotransformation, and the blood level will fall below the toxic level in a short time.
Treatment of a sustained convulsive reaction to a local anesthetic includes oxygen andDiazepam IV. If proper equipment and adequately trained staff are not available, do not attemptIV injections.
Some possible side effects of systemic absorption (not necessarily toxic levels) of lidocaineinclude tonic-clonic convulsions, respiratory depression, and decreased cardiac output.
ORAL SURGERY/PAIN CONTROL
Local anesthetics are most effective in tissues that have what pH?
• Below 7• Above 7• Below 4• Makes no difference what the pH of the tissue is
Copyright © 2001 - DENTAL DECKS
Anesth
• Above 7
Local anesthetics are alkaloid bases that are combined with acids to form water-soluble salts. Above pH 7 (alkaline) you get hydrolysis of the anesthetic salts. Remember:The potential action of all local anesthetics depends on the ability of the anesthetic salt to liberate the free alkaloidal base (the non-ionic lipophilic molecule). Thepotency of local anesthetics increases with increasing lipid solubility.
As pH of the solution (tissue) goes down and the hydrogen ion concentration isincreased, the cationic (water-soluble) form rises and free base form goes down.Conversely, as the pH is increased and hydrogen ion concentration is decreased, thefree base (fat-soluble) form increases and the cationic form decreases. This free baseform readily penetrates the lipid rich nerve.
Remember: Inflammation and infection cause the tissues to be acidic. The cationic(water-soluble) form of the anesthetic predominates (there is less free base available).Therefore, the penetration of the membrane is lessened and the anesthetic has pooreffectiveness.
AnesthORAL SURGERY/PAIN CONTROL
Which of the following is that phase of anesthesia that begins with the administrationof anesthetic and continues until the desired level of patient unresponsiveness isreached?
• Amnesia• Induction• Maintenance• Recovery
Copyr ight © 2001 - DENTAL DECKS
• Induction
The depth of general anesthesia (by inhalation) varies with the partial pressure (tension) of the anesthetic agent in the brain, and the rates of induction and recoverydepend upon the rate of change of tension in this tissue (also blood supply to the lungs,pulmonary ventilation, and the concentration of the anesthetic influence the rate ofinduction). The signs and stages of anesthesia are most likely to be seen with an anesthetic that has a slow rate of induction.
Notes :1. Maintenance is the process of keeping a patient in surgical anesthesia2. Recovery is the phase of anesthesia commencing when surgery is complete and
the delivery of the anesthetic is terminated and ending when the anesthetic has beeneliminated from the body.
3. The behavior of patients under general anesthesia suggests that the most resistant part of the eNS is the medulla oblongata (cardiac, vasomotor, and respiratory centers of the brain).
4. The most controllable route for administration of a general anesthetic is inhalation.~ 'MIlS\ ["o lA.trotbb~
AnesthORAL SURGERY/PAIN CONTROL
Which vein listed below is the optimum site for IV sedation for an outpatient?
• Median basilic vein• Median cephalic vein• Median antebrachial vein• Angular vein
Copyright © 2001 - DENTAL DECKS
• Median cephalic vein
This vein lies in the lateral aspect of the antecubital fossa (anterior to the elbow). Avoidentering the brachial artery. If the artery is entered, the following symptoms willappear: immediate burning at the site of the injection, the arm will appear blotchy, andthe pulse in the arm will be weak compared to the other arm.
IV sedation:• Usually done with a 21 gauge needle• Popular drug is Valium (Diazepam)• The rate of injection of Valium is 1 ml/minute
- 1 ml of injectable Valium contains 5 mg of Valium• Injection is discontinued when the eyelids droop (ptosis)
Three common signs indicating when the correct level of sedation has been reachedwhen using Valium:
1. Blurring of vision2. Slurring of speech3. 50% ptosis of the eyelids (this is called Verrill's sign)
Remember: Valium is contraindicated for use in a patient with a history of narrowangle glaucoma.
ORAL SURGERY/PAIN CONTROL
All of the following local anesthetics are amides except
• Prilocaine• Bupivacaine• Lidocaine• Procaine
Copyright © 2001 - DENTAL DECKS
Anesth
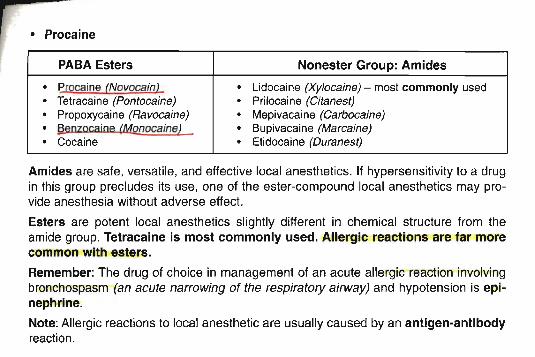
• Procaine
PABA Esters Nonester Group: Amides
• Procaine (Novocainl • Lidocaine (Xylocaine) - most commonly used
· Tetracaine (Pontocaine) · Prilocaine (Citanest)
· Propoxycaine (Ravocaine) · Mepivacaine (Carbocaine)
· §.enzocaine (Monocaine) · Bupivacaine (Marcaine)• Cocaine • Etidocaine (Ouranest)
Amides are safe, versatile, and effective local anesthet ics. If hypersens itivity to a drugin this group precludes its use, one of the ester-compound local anesthetics may provide anesthesia without adverse effect.
Esters are potent local anesthetics slightly different in chemical structure from theamide group. Tetracaine is most commonly used. Allergic reactions are far morecommon with esters.
Remember: The drug of choice in management of an acute allergic reaction involvingbronchospasm (an acute narrowing of the respiratory airway) and hypotension is epinephrine.
Note: Allergic reactions to local anesthetic are usually caused by an antigen-antibodyreaction.
AnesthORAL SURGERY/PAIN CONTROL
All of the following may prevent a patient from developing a vasovagal syncopal reaction after the use of a local anesthetic except:
• Slowing injecting the anesthetic solution• Watching the patient's color change during the injection• Using a topical anesthetic prior to administration of the local anesthetic• Injecting the anesthetic solution as quickly as possible• Using a low concentration of vasoconstrictor• Premedicating extremely anxious patients• Sympathetic, but confident handling of the patient
Copyright © 2001 - DENTAL DECKS
• Injecting the anesthetic solution as quickly as possible
The most common cause of a transient loss of consciousness in the dental office isvasovagal syncope. This generally is due to a series of cardiovascular events whichare triggered by the emotional stress brought on by the anticipation of or delivery ofdental care.
Prevention of vasovagal syncopal reactions involves proper patient preparation.
Remember: Any signs of an impending syncopal episode should be quickly treated byplacing the patient in a fully supine position or a position in which the legs are elevated above the level of the heart (Trendelenburg position) and by placing a cool, moisttowel on the forehead.
Important: The most common early sign of syncope is pallor (flushed).
AnesthORAL SURGERY/PAIN CONTROL
How will a larger than normal functional residual capacity affect nitrous oxide sedation?
• Nitrous oxide sedation will happen much quicker• Nitrous oxide sedation will take longer• Functional residual capacity does not effect nitrous oxide sedation
Copyright @ 2001 - DENTAL DECKS
• Nitrous oxide sedation will take longer
The functional residual capacity is the amount of air remaining in the lungs at the endof the normal expiration. Note: This air is used to provide air to the alveoli , which willaerate the blood evenly between breaths .
Note: Pulmonary volumes and capac ity are about 20 to 25% less in females than inmales and are greater in large and athletic persons. Nitrous oxide sedation will varyaccordingly.
AnesthORAL SURGERY/PAIN CONTROL
How do local anesthetics effect the nerve membrane?
• They increase potassium flux• They increase the membrane excitability by Increasing the membrane's perme
ability to sodium ions• They decrease the membrane's permeability to sodium ions and reduce the mem
brane excitability• They increase the calcium and chloride flux
Copyright @ 2001 - DENTAL DECKS
• They decrease the membrane's permeability to sodium ions and reduce themembrane excitability
Most local anesthetics act directly on the activation gates of the sodium channels , making it much more difficult for these gates to open. This decreases sodium membranepermeability, and therefore reduces membrane excitab ility. When the excitability hasbeen reduced below a critical level, a nerve impulse fails to pass through the anesthetized area (depolarization does not occur). Note: K+ FLUX remains unchanged .
Remember:Na+-K+shift:
When Na+enters the nerve =depolarizationWhen K+exits the nerve =repolarization
Important Points:1. Local anesthetics reversibly block nerve impulse conduction and produce
reversible loss of sensation at their administration side.2. The site of action of local anesthetics is at the lipoprotein sheath of the nerve.
ORAL SURGERY/PAIN CONTROLAnat
When a patient attempts protrusion, the mandible deviates markedly to the left.Which muscle listed below is unable to contract?
• Buccinator muscle• Temporalis muscle• Right lateral pterygoid muscle• Left lateral pterygoid muscle
Copyright © 2001 - DENTAL DECKS
• Left lateral pterygoid muscle
"'With lateral pterygoid injury, the mandible will deviate toward the side of injury.
The mandible will also deviate.!9ward the side of injury with:• Aokylosis of the condyl~ t **The most common cause of TMJ ankylosis is trauma)• A unilateral condylar fracture-- -The mandible will deviate away from the affected side with:• Condylar hyperplasia (**'Malocclusion is also a common occurrence with this
injury)
Remember: The lateral pterygoids (right and left) acting together are the prime protractors of the mandible.
Important: In addition to opening and protruding, the lateral pterygoids move themandible from side to side. For right lateral excursive movements, the left lateralpterygoid muscle is the prime mover and vice versa.
ORAL SURGERY/PAIN CONTROLAnat
Which artery listed below supplies the mucosa of the hard palate posterior to the maxillary canine?
• Sphenopalatine artery• Greater palatine artery• Posterior superior alveolar artery• Nasopalatine artery
Copyright © 2001 - DENTAL DECKS
• Greater palatine artery
The descending palatine artery gives rise to the greater and lesser palatine arteries, whichpass through the greater and lesser palatine foramina, respectively, and supply the hard andsoft palates . In addition to the soft palate, the lesser palatine artery also helps supply the tonsils (along with the tonsillar artery, a branch of the facial artery). Note : The greater palatineartery sends a branch to anastomose with the nasopalatine branch of the sphenopalatineartery in the incisive foramen to supply the mucosa of the hard palate anterior to the maxillarycanine.
<,
Innervation of the soft tissue of the posterior two-thirds of the hard palate is derived from thegreater (anterior) palatine nerve. It emerges into the hard palate by way of the greater palatineforamen and passes forward approximately halfway between the alveolar crest and the midline.It supplies the soft tissues of the palate as far anteriorly as the canine tooth where it overlaps withbranches from the nasopalatine nerve. It is necessary to anesthetize the greater palatine nerveif extractions or surgical procedures are contemplated in this area of the palate.
To anesthetize the greater (anterior) palatine nerve, you need to deposit local anesthetic at thegreater palatine foramen. The greater palatine foramen is situated between the second andthird maxillary molars about 1 cm from the palatal gingival margin toward the midline.
Note: The greater palatine nerve is a branch of the maxillary (eN V-2) nerve.
AnatORAL SURGERY/PAIN CONTROL
Which nerve listed below innervates the facial muscles with motor fibers, the lacrimalgland and salivary glands with parasympathetic fibers, and the anterior tongue withsensory fibers?
• Trigeminal (CN V)• Vagus (CN X)• Facial (CN VII)• Glossopharyngeal (CN IX)
Copyright © 2001 - DENTAL DECKS
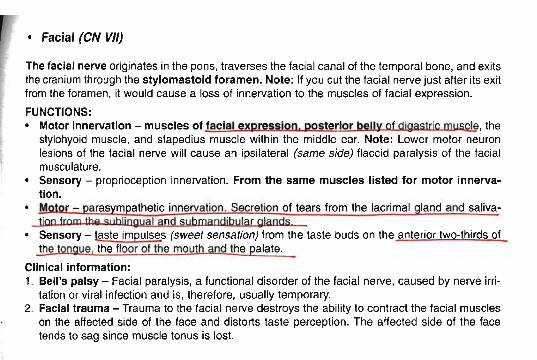
• Facial (eN VII)
The facial nerve originates in the pons, traverses the facial canal of the temporal bone, and exitsthe cranium through the stylomasto id foramen. Note: If you cut the facial nerve just after its exitfrom the foramen, it would cause a loss of innervation to the muscles of facial expression.
FUNCTIONS:• Motor Innervati on - muscles of facial expression, posteri or belly of digastric mu~, the
stylohyoid muscle, and stapedius muscle within the middle ear. Note: Lower motor neuronlesions of the facial nerve will cause an ipsilateral (same side) flaccid paralysis of the facialmusculature.
• Sensory - proprioception innervation. From the same muscles listed for motor innervati on.
o Motor - parasympathetic innervation. Secretion of tears from the lacrimal gland and salivation from the Sl,bljngyal and submandibylar glands
o Sensory - taste impulses (sweet sensation) from the taste buds on the anterior two-thirds ofthe tongue, the floor of the mouth and the palate.
Clinical information:1. Bell 's palsy - Facial paralysis, a functional disorder of the facial nerve, caused by nerve irri
tation or viral infection and is, therefore, usually temporary.2. Facial trauma - Trauma to the facial nerve destroys the ability to contract the facial muscles
on the affected side of the face and distorts taste perception. The affected side of the facetends to sag since muscle tonus is lost.
AnatORAL SURGERY/PAIN CONTROL
All of the following statements conce rning the articular eminence are true except.
• It is also called the articular tubercle• It is convex• It is a ridge that extends mediolaterally just in front of the mand ibular fossa• It is considered to be the non-funct ioning port ion of the temporomandibular joint• It is lined with a thick layer of fibrous connective tissue (fibrocartilage)
Copyright © 2001 - DENTAL DECKS
-------------------------~ ------
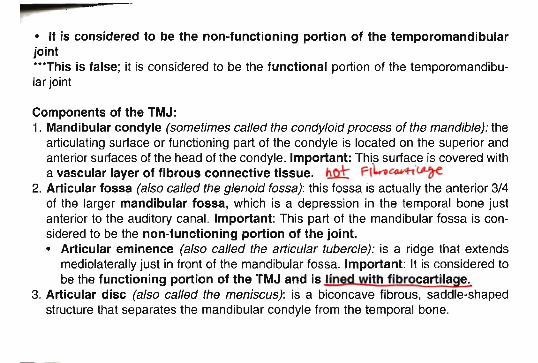
• It is considered to be the non-functioning portion of the temporomandibularjoint---This is false ; it is considered to be the functional portion of the temporomandibular joint
Components of the TMJ:1. Mandibular condyle (sometimes called the condyloid process of the mandible) : the
articulating surface or functioning part of the condyle is located on the superior andanterior surfaces of the head of the condyle. Important: This surface is covered witha vascular layer of fibrous connective tissue. hnt Pl~~'~
2. Articular fossa (also called the glenoid fossa): this fossa is actually the anterior 3/4of the larger mandibular fossa, which is a depression in the temporal bone justanterior to the auditory canal. Important: This part of the mandibular fossa is considered to be the non-functioning portion of the joint.• Articular eminence (also called the articular tubercle): is a ridge that extends
mediolaterally just in front of the mandibular fossa. Important: It is considered tobe the functioning portion of the TMJ and is lin ith fibrocartila e.
3. Articular disc (also called the meniscus): is a biconcave fibrous. saddle-shapedstructure that separates the mandibular condyle from the temporal bone.
ORAL SURGERY/PAIN CONTROL
The internal jugular vein descends through the neck within the:
• Arachnoid sheath• Carotid sheath• Spiral sheath• Dural sheath
Copyright e 2001 - DENTAL DECKS
Anat
• Carotid sheath
The facial vein unites with the retromandibular vein below the border of the mandibleand empties into the main venous structure of the neck, the internal jugular vein.
The internal [uqular vein descends through the neck within the carotid sheath andunites behind the sternoclavicular joint with the subclavian vein to form the brachiocephalic vein. The brachiocephalic veins (right and left) unit in the superior mediastinum to form the superior vena cava , which returns blood to the right atrium of theheart.
The carotid sheath is located at the lateral boundary of the retropharyngeal space atthe level of the oropharynx on each side of the neck deep to the sternocleidomastoidmuscle. It extends from the base of the skull to the first rib and sternum.
Remember: The carotid sheath encloses the carotid arteries, the internal jugular vein,and the vagus nerve.
AnatORAL SURGERY/PAIN CONTROL
The pterygopalatine fossa communicates laterally with the infratemporal fossa byway of:
• The sphenopalatine foramen• The pterygoid canal• The foramen rotundum• The petrotympanic fissure• The pterygomaxillary fissure
Copyright © 2001 - DENTAL DECKS
• The pterygomaxillary fissure -
The pterygopalatine fossa communicates medially with the nasal cavity through thesphenopalatine foramen, posteriorly with the foramen lacerum through the pterygoid canal, superiorly with the skull through the foramen rotundum, and anteriorlywith the orbit through the inferior orbital fissure.
The pterygopalatine fossa is a small space behind and below the orbital cavity. It liesbetween the pterygoid plates of the sphenoid and palatine bone below the apex of theorbit.
Openings into the fossa: Pterygomaxillary fissure, inferior orbital fissure, sphenopalatine foramen, pterygoid canal, pharyngeal canal, and foramen rotundum.
lhe pterygopalatine ganglion lies in the pterygopalatine fossa jllS! belew the mmmlary nerve (Y-?) It receives preganglionic parasympathetic fibers from the facialnerve by way of the reater petrosal nerve. It sends postganglionic parasympathet-ic fibers to the cnmal Ian n g an s In the palate and the nose.
Note: The maxillary nerve (V-2) and the maxillary artery pass through the pterygopalatine fossa.
ORAL SURGERY/PAIN CONTROL
In the head and neck, all the lymph ultimately drains into the:
• Submental lymph nodes• Submandibular lymph nodes• Deep cervical lymph nodes• Retropharyngeal lymph nodes
Copyright © 2001 - DENTAL DECKS
Anat
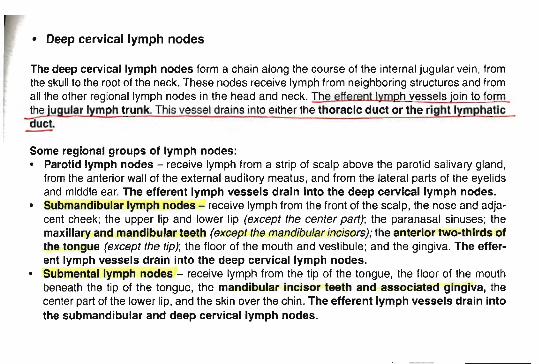
• Deep cervical lymph nodes
The deep cerv ical lymph nodes form a chain along the course of the internal jugular vein, fromthe skull to the root of the neck. These nodes receive lymph from neighboring structures and fromall the other regional lymph nodes in the head and neck. The efferent lymRh vessels join to formthe jugular lymph trunk. This vessel drains into either the thoracic duct or the right lymphatic
dUct.
Some regional groups of lymph nodes:• Parotid lymph nodes - receive lymph from a strip of scalp above the parotid salivary gland,
from the anterior wall of the external auditory meatus, and from the lateral parts of the eyelidsand middle ear. The efferent lymph vessels drain into the deep cervical lymph nodes.
• Submandibular lymph nodes - receive lymph from the front of the scalp, the nose and adjacent cheek; the upper lip and lower lip (except the center part); the paranasal sinuses; themaxillary and mandibular teeth (except the mandibular incisors); the anterior two-thirds ofthe tongue (except the tip); the floor of the mouth and vestibule; and the gingiva. The efferent lymph vessels drain Into the deep cervical lymph nodes.
• Submental lymph nodes - receive lymph from the tip of the tongue, the floor of the mouthbeneath the tip of the tongue, the mandibular incisor teeth and associated gingiva, thecenter part of the lower lip, and the skin over the chin. The efferent lymph vessels drain intothe submandibular and deep cervical lymph nodes.
AnatORAL SURGERY/PAIN CONTROL
Which division of the trigeminal nerve listed below passes through the foramen ovaleand supplies motor innervation to the tensor veli palatini, tensor tympani, musclesof mastication (temporalis, massete r, lateral and medial pterygoids), and the anteriorbelly of digastric and mylohyoid muscles?
• Ophthalmic division (V-1)• Maxillary division (V-2)• Mandibular division (V-3)• None of the above
Copyright © 2001 - DENTAL DECKS
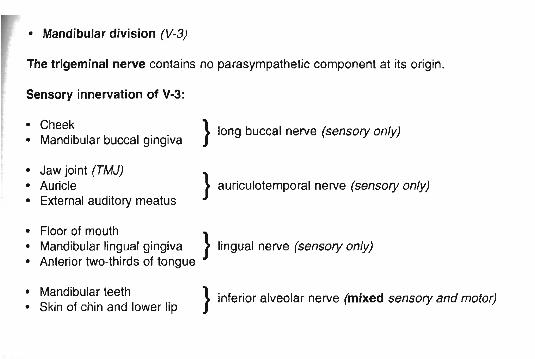
• Mandibular division (V-3)
The trigeminal nerve contains no parasympathetic component at its origin.
Sensory innervation of V-3:
• Cheek• Mandibular buccal gingiva
• Jaw joint (TMJ)• Auricle• External auditory meatus
} long buccal nerve (sensory only)
} auriculotemporal nerve (sensory only).
• Floor of mouth }Mandibular lingual gingiva lingual nerve (sensory only)
• Anterior two-thirds of tongue
• Mandibular teeth• Skin of chin and lower lip
} inferior alveolar nerve (mixed sensory and motor)
AnatORAL SURGERY/PAIN CONTROL
The facial nerve, the retromandibular vein, and the external carotid artery lie within which salivary gland listed below?
• Submandibular gland• Parotid gland• Sublingual gland
Copyright © 2001 - DENTAL DECKS
• Parotid gland
The parotid gland is the largest of the salivary glands and is~Iand. Theparotids are located below and just anterior to the ear. They are diilieiritOdeep and superficiallobes with the stylomandibular tunnel (which encloses the facial nerve) being the dividingline. Therefore, a portion of the parotid lies superficial to the mandibular ramus, and another portion lies deep.
The parotid gland is drained by Stenson's duc t.. which pierces the buccinator muscle andcrosses the masseter muscle where it opens into the vestibule of the mouth opposite the maxIllary second molar.
The parotid gland receives it parasympathetic secretomotor innervation from the 91~SOPharyngeal nerve by way of the lesser petrosal nerve , the otic ganglion, and the auriculotemporal nerve (branch of V-3).
The external carotid artery and its terminal branches within the gland, namely the superficialtemporal and the maxillary arteries, supply the parotid gland. The Ivmphatic drainage of theparotid gland is through the parotid nodes to the deep cervical lymph nodes.
Notes:1. Mumps is a viral disease of the parotid gland. Parotitis is the inflammation of the parotid
gland.2. Von Ebner 's glands are the only other adult salivary glands which are purely serous.
ORAL SURGERY/PAIN CONTROL
The nerve to the mylohyoid muscle is a branch of the:
• Ophthalmic nerve (CN V-1)• Maxillary nerve (CN V-2)• Mandibular nerve (CN V-3)• Facial nerve (CN V/I)
Copyright © 2001 - DENTAL DECKS
Anat
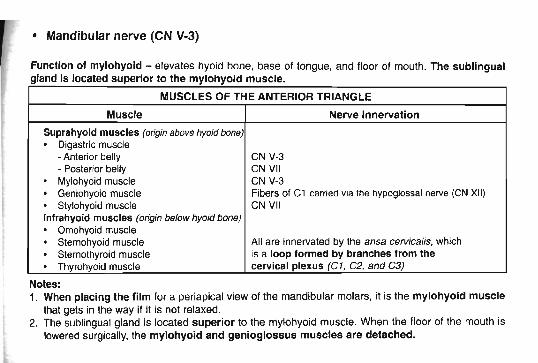
• Mandibular nerve (eN V-3)
Function of mylohyoid - elevates hyoid bone, base of tongue, and floor of mouth. The sublingualgland is located superior to the mylohyoid muscle.
MUSCLES OF THE ANTERIOR TRIANGLE
Muscle Nerve Innervation
Suprahyoid muscles (origin above hyoid bone)
· Digastric muscle• Anterior belly CNV-3• Posterior belly CN VII
· Mylohyoid muscle CN V·3
· Geniohyoid muscle Fibers of Cl carried via the hypoglossal nerve (e N XII)
· Stylohyoid muscle CN VIIInfrahyoid muscles (origin below hyoid bone)
· Omohyoid muscle
· Stemohyoid muscle All are innervated by the ansa cervics tte, which
· Stemothyroid muscle is a loop formed by branches from the
· Thyrohyoid muscle cerv ical plexus (C1, C2. and C3)
Notes:1. When plac ing the film for a periapica l view of the mandibular molars, it is the mylohyoid muscle
that gets in the way if it is not relaxed.2. The sublingual gland is located superior to the mylohyoid muscle. When the floor of the mouth is
lowered surgically, the mylohyoid and genioglossus muscles are detached.
ORAL SURGERYIPAIN CONTROL
Wharton 's duct is associated with the:
• Parotid gland• Submandibular gland• Sublingual gland• Von Ebner's glands
Copyright © 2001 - DENTAL DECKS
Anal
• Submandibular gland
The submandibular glands (sometimes called submaxillary glands) are located in the space (submandibular triangle) bounded by the two bellies of the digastric muscle and the angle of the mandible.The submandibular duct (Wharton 's duct) passes forward along the side of the tongue, beneath themucousmembrane of the floor of the mouth. It is crossed by the lingual nerve and then lies betweenthe sublingual gland and the genioglossus muscle. It opens at the base of the frenulum of thetongue.
Note: These large salivary glands are composed of a mixtyre of serous and mucous acini.
The submandibular glands are innervated by parasympathetic secretomotor fibers from the facialM nerve, which run in the chorda tympani and in the lingual nerve (branch of V-3) and synapse in the
Of)' submandibular ganglion. Note: This Is the same as the sublingual glands. The blood supplycomes from the fac ial artery, which is a branch of the external carotid artery.
Important: During its course, Wharton's duct is closely related to the lingual nerve which eventuallycrosses over it. This is important because if you incise the mucous membranes of the floor of themouth, depending on where you cut, you may expose the lingual nerve, Wharton's duct, and the sublingual gland.
Notes:1. To expose the duct intraorally, only mucous membrane needs to be cut through.2. The best technique for palpation of this gland is bimanual, simultaneous intraoral and extraoral
palpation.3. Lymphadenopathy Is the most common cause of swelling of the tissues in the submandibular
triangle (not cysts, sialoliths , etc.).
ORAL SURGERYIPAIN CONTROLAnat
Branches of which artery listed below supply the maxillary and mandibular teeth?
• Vertebral• Occipital• Maxil lary• Subclavian
Copyright © 2001 - DENTAL DECKS
• Maxillary
Branches of the maxillary artery supply both dental arches. The maxillary teethare supplied by branches of Part 3 (Pterygopalatine part) as follows:• Posterior teeth (molars and premolars) from posterior and superior alveolar arter
ies.• Anterior teeth (canines and incisors) from anterior and middle superior alveolar
arteries.
The mandibular teeth are supplied by the inferior alveolar artery, which is a branch ofPart 1 (Mandibular part).
Note: The maxillary artery supplies the muscles of mastication, the maxillary andmandibular teeth, the palate , and almost the entire nasal cavity.
Remember: The venous return of both dental arches is the pterygoid plexus ofveins.
The external carotid artery supplies most of the head and neck. except for the brain(the brain gets its blood supply from the internal carotid and the vertebral arteries). Theexternal carotid passes through the parotid salivary gland and terminates as the maxillary and superficial temporal arteries. The superficial temporal artery supplies thescalp ·~1'Mr.
ORAL SURGERYIPAIN CONTROLAnat
Which of the following arteries does not accompany the corresponding nerve throughout its course?
• Infraorbital artery• Inferior alveolar artery• Lingual artery• Posterior superior alveolar artery
Copyright © 2001 - DENTAL DECKS
• Lingual artery
The lingual artery arises from the external carotid at the level of the greater horn ofthe hyoid bone and passes deep to the hyoglossus muscle to supply the tongue.
Branches include:• Suprahyoid artery - supplies suprahyoid region• Dorsal lingual artery - remember dorsum of the tongue is the top part that can be
seen easily• Sublingual artery - supplies the floor of the mouth and sublingual gland• Deep lingual artery - supplies the anterior two-thirds of the tongue
The lingual artery supplies blood to the tongue, floor of the mouth, suprahyoid region,sublingual gland, and palatine tonsils.
Important: The inferior alveolar nerve and artery along with the lingual nerve arefound in the pterygomandibular space between the medial pterygoid muscle and theramus of the mandible. The inferior alveolar nerve passes lateral to the sphenomandibular ligament.
Note: The lateral pterygoid muscle forms the roof of the pterygomandibular space.
AnatORAL SURGERY/PAIN CONTROL
Which nerve listed below is the largest of the 12 cranial nerves and is the principalgeneral sensory nerve to the head, particularly the face?
• Vagus (CN X)• Glossopharyngeal (CN IX)• Facial (CN VII)• Trigeminal (CN V)
Copyright © 2001 - DENTAL DECKS
• Trigeminal (eN V)
The trigeminal nerve originates from the brainstem at the inferior surface of the pons. It has tworoots (small motor and large sensory). The large sensory root expands to form the trigem inalganglion (also called the semilunar ganglion) that occupies the trigeminal impression on thepetrous portion of the temporal bone. It is from this ganglion that the three divisions (ophthalmic,maxillary and mandibular) arise. These three divisions exit the skull through openings in thesphenoid bone.
Note: The motor portion of the trigeminal nerve only travels with the mandibular division.The cell bodies of the sensory neurons are found in the trigeminal ganglion.
There are different nuclei (mass of nerve cells) associated with the trigeminal nerve:• Mesencephalic - a nucleus from which fibers run laterally with the mandibular nerve to inner
vate the muscles of mastication. Cell bodies of proprioceptive fibers are located here.• Spinal - a nucleus that receives fibers which mediate pain and temperature for the head
and neck.
Note: If the trigeminal nerve is cut or damaged. there would be a complete loss of sensationin the facial area on the same side ("ipsilateral"). There would also be difficulty in chewing andspeaking.
ORAL SURGERY/PAIN CONTROLAnat
Which of the following teeth could be removed without pain after administration of aninferior alveolar and lingual nerve block?
• All anterior teeth on the side of the injection• Canine and first premolar on the side of the injection• All teeth in that quadrant on the side of the injection• Both premolars and first molar on the side of the injection
Copyright ~ 2001 - DENTAL DECKS
• Canine and first premolar on the side of the injection
You need to give a long buccal injection in order to extract the molars and secondbicuspid. For operative procedures, a long buccal injection may not be needed forthese teeth.
Incisors may need local infiltration for extractions.
Note: An injection into the parotid gland (capsule) when attempting to administer aninferior nerve block may cause a Bell's palsy facial expression (paralysis of the forehead muscles, the eyelid and of the upper and lower lips on the same side of the facethat the injection was given).
Remember: The bone of the maxilla is more porous than that of the mandible, therefore, it can be infiltrated anywhere. The only place where the mandible is porous is atthe incisive fossa.
ORAL SURGERY/PAIN CONTROLAnat
The stylomandibular ligament of the TMJ is a band of cervical fascia that runs fromthe styloid process of the sphenoid bone to the:
• Mandibular condyle• Ramus of the mandible• Angle of the mandible• Lingula of the mandible
Copyright © 2001 - DENTAL DECKS
• ligament suspens ion• durability of the fibrocartilage
• Angle of the mandible***Posterior border of the mandible
Thereare 3 ligaments associated with the TMJ. These ligaments support and reinforcethe TMJ and are involved in complex jaw movements.• One or ligame . The temporomandibular ligament (also called the laterallig-
ament or cramomandibular ligament) runs from the articular eminence to themandibular condyle. It provides direct support to the capsule. This ligament prevents posterior and inferior displacement of the condyle.
• Two accessory ligaments:The stylomandibular ligament separates the infratemporal region anteriorly fromthe parotid region behind. It runs from the styloid process of the sphenoid bone tothe angle of the mandibleThe sphenomandibular ligament is attached to the spine of the sphenoid boneand lingula on medial surface of the mandible .
The TMJ is protected by:• the muscles of mastication• synovial fluid
ORAL SURGERY/PAIN CONTROLAnat
Which salivary gland listed below is the smallest and contains both serous andmucous acini?
• Submandibular gland• Parotid gland• Sublingual gland
Copyright © 2001 - DENTAL DECKS
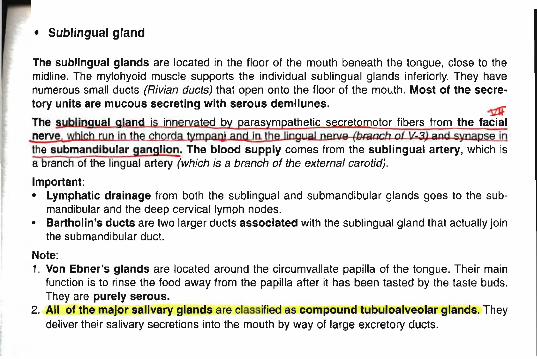
• Sublingual gland
The sublingual glands are located in the floor of the mouth beneath the tongue, close to themidline. The mylohyoid muscle supports the individual sublingual glands inferiorly. They havenumerous small ducts (Rivian ducts) that open onto the floor of the mouth. Most of the secretory units are mucous secreting with serous demllunes. ~
The §.Ubllngual gland is innervated by parasympathetic secretomotor fibers from the facialnerve, which run in the...ctlo.rda tympaw and !Q. the lingual nerue (branch o f 11- 3,1 and synapse inthe submandibular ganglion. The blood supply comes from the sublingual artery, which isa branch of the lingual artery (which is a branch of the external carotid).
Important:• Lymphatic drainage from both the sublingual and submandibular glands goes to the sub
mandibular and the deep cervical lymph nodes.• Bartholin's ducts are two larger ducts associated with the sublingual gland that actually join
the submandibular duct.
Note:1. Von Ebner 's glands are located around the circumvallate papilla of the tongue. Their main
function is to rinse the food away from the papilla after it has been tasted by the taste buds.They are purely serous.
2. All of the major salivary glands are classified as compound tubuloalveolar glands. Theydeliver their salivary secretions into the mouth by way of large excretory ducts.
ORAL SURGERY/PAIN CONTROL
Which two arteries listed below supply blood to the TMJ?
• Facial artery• Lingual artery• Superficial temporal artery• Deep auricular artery
Copyright @ 2001 - DENTAL DECKS
Anat
• Superficial temporal artery• Deep auricular artery"""The deep auricular artery is a branch of the maxillary artery."·"Both the superficial temporal artery and the maxillary artery are terminal branches of the external carotid artery.
I/JThe auriculotemporal nerve. which is a branch of the mandibular division of thetrigeminal nerve, provides the major sensory innervation to the posterior port ion ofthe TMJ. Note: Pain is transmitted in the capsule and the periphery of the disc by theauriculotemporal nerve.
1,/3The nerve to the masseter (called the masseteric nerve), also a branch of themandibulardivision of the trigeminal nerve,carries a few sensory fibers to the anteri-or portion of the TMJ. ---Remember: Muscles acting on the joint:• Masseter• Pterygoids (medial and lateral)• Temporalis• Digastric
ORAL SURGERYIPAIN CONTROLAnat
Which artery listed below supplies the tongue?
• Palatine artery• Inferior alveolar artery• Lingual artery• Vertebral artery
Copyright © 2001 - DENTAL DECKS
~-----
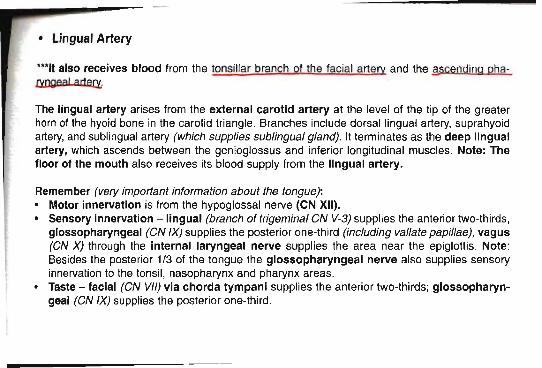
• Lingual Artery
***'t also receives blood from the tonsil lar branch of the facial artery and the -sscending pha~ngea l artert:
The lingual artery arises from the external carotid artery at the level of the tip of the greaterhorn of the hyoid bone in the carotid triangle. Branches include dorsal lingual artery, suprahyoidartery, and sublingual artery (which supp lies sublingual gland). It terminates as the deep lingualartery, which ascends between the genioglossus and inferior longitudinal muscles. Note: Thefloor of the mouth also receives its blood supply from the lingual artery.
Remember (very important information about the tongue):• Motor innervation is from the hypoglossal nerve (eN XII).• Sensory Innervat ion - lingual (branch of trigeminal eN V-3) supplies the anterior two-thirds,
glossopharyngeal (CN IX) supplies the posterior one-third (including vallate pap illae), vagus(CN X) through the internal laryngeal nerve supplies the area near the epiglottis. Note:Besides the posterior 1/3 of the tongue the glossopharyngeal nerve also supplies sensoryinnervation to the tonsil, nasopharynx and pharynx areas.
• Taste - facial (CN VII) via chorda tympani supplies the anterior two-thirds; glossopharyngeal (CN IX) supplies the posterior one-third.
AnatORAL SURGERY/PAIN CONTROL
Which of the following statements concerning the hypoglossal nerve (eN XII) aret rue?
• It is a motor nerve supplying all of the intrinsic and extrins ic muscles of thetongue, except the palatoglossus, which is supplied by the vagus nerve
• It leaves the skull through the hypoglossal canal medial to the carotid canal andjugular foramen
• It passes above the hyoid bone on the lateral surface of the hyoglossus muscledeep to the mylohyoid muscle
• It loops around the occipital artery and passes between the external carotid arteryand internal jugular vein
• In the upper part of its course, it is joined by C1 fibers from the cervical plexus• All of the above statements are true concerning the hypoglossal nerve
Copyright © 2001 - DENTAL DECKS
• All of the above statements are true concerning the hypoglossal nerve
Lesions of the hypoglossal nerve:• Unilateral lesions of the hypoglossal nerve result in the deviation of the protruded
tongue towards the affected side. This is due to the lack of function of thegenioglossus muscle on the diseased side.
• Injury of the hypoglossal nerve eventually produces paralysis and atrophy of thetongue on the affected side with the tongue deviated to the affected side.Dysarthria (inability to articulate) may also be found.
Important: If the genioglossus muscle is paralyzed, the tongue has a tendency tofall back and obstruct the oropharyngeal airway with risk of suffocation.
ORAL SURGERY/PAIN CONTROL
Which paranasal sinuses are the largest?
• Frontal• Ethmoidal• Maxillary• Spheno idal
Copyright © 2001 - DENTAL DECKS
Anat
• Maxillary
Located within the frontal, ethmoid, maxillary, and sphenoid bones are a series ofmucous membrane-lined air spaces called the paranasal sinuses. The sinuses lighten the skull and enhance the resonance of the voice.
Clinical signs of acute maxillary sinusitis:• Severe pain . constant and localized• Tenderness to percussion of the maxillary posterior teeth• A mucopurulent exudate• Any unusual motion or jarring accentuates the pain• Tenderness over the anterior sinus wall
Antibiotics used to treat sinus infections:• 8mp jci!!l!J - for sinusitis due to upper respiratory infections• Penicillin - for sinusitis caused by odontogenic foci• Amoxicillin - for sinusitis caused by odontogenic foci
Note: The maxillary sinus is innervated by the maxillary division of the trigeminal nerve(eN V-2).
"--- - - - - - - - - - - - - - - - - - - - - -
ORAL SURGERY/PAIN CONTROLAnat
The TMJ is the articulation between the condyle of the mandible and the squamousportion of the: -
• Spheno id bone• Temporal bone• Ethmoid bone• Zygomatic bone
Copyright © 2001 :- DENTAL DECKS
• Temporal bone
Each condyle is elliptically shaped (they are not symmetrical nor identical) with theirlong axis oriented mediolaterally. The articular surface of the temporal bone is composed of the concave articular fossa (also called the glenoid fossa or mandibularfossa) and the convex articular eminence (or tubercle). Note: This area is the functional and articular portion of the TMJ and is covered by fibrocartilage.
The articular disc (or meniscus) is a fibrous. saddle shaped structure that separatesthe condyle and the temporal bone. The disc varies in thickness: the thinner, centralintermediate zone separates thicker portions called the anterior band and posteriorband. Posteriorly, the disc is contiguous with the posterior attachment tissues calledthe bilaminar zone. The bilaminar zone is a vascular. innervated tissue that plays animportant role in allowing the condyle to move forward.
The disc and its attachments divide the TMJ into superior and inferior spaces.
AnatORAL SURGERY/PAIN CONTROL
Which nerve below supplies motor function to the buccinator muscle?
• Trigem inal nerve (CN V)• Facial nerve (CN VII) .• Vagus nerve (CN X)• Glossopharyngeal nerve (CN IX)
Copyright © 2001 - DENTAL DECKS
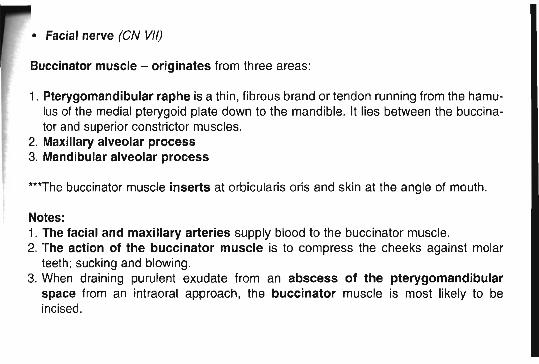
• Facial nerve (eN VII)
Buccinator muscle - originates from three areas:
1. Pterygomandibular raphe is a thin, fibrous brand or tendon running from the hamulus of the medial pterygoid plate down to the mandible. It lies between the buccinator and superior constrictor muscles.
2. Maxillary alveolar process3. Mandibular alveolar process
***The buccinatormuscle inserts at orbicularis oris and skin at the angle of mouth.
Notes:1. The facial and maxillary arteries supply blood to the buccinator muscle.2. The action of the buccinator muscle is to compress the cheeks against molar
teeth; sucking and blowing.3. When draining purulent exudate from an abscess of the pterygomandibular
space from an intraoral approach, the buccinator muscle is most likely to beincised.
AnatORAL SURGERY/PAIN CONTROL
A posterior superior alveolar nerve block (tuberosity injection) will provide anesthesiafor:
• The second and third molars along with the mucoperiosteum of the palate• The first and second molars along with the mucoperiosteum of the palate• The first , second, and third molars but not the mucoperiosteum of the palate• The first, second, and third molars along with the mucoperiosteum of the palate
Copyright © 2001 - DENTAL DECKS
• The first, second, and third molars but not the mucoperiosteum of the palate
***For extraction of any or all of the three molar teeth, a greater palatine injectionshould be given to anesthetize the mucoperiosteum of the palate
The PSA injection (tuberosity injection) does not always anesthetize all of the rootsof the maxillary first molar tooth. Therefore, if anesthesia of this tooth for eitherrestorative dentistry or extraction is required, an infiltration injection also should be performed over the second premolar tooth.
Note: Patients experience few subjective signs of anesthesia after receiving a posterior superior alveolar nerve block, as compared to an inferior alveolar nerve block(numb lip).
Important: If a patient's face becomes distended and swollen after a posterior superior alveolar nerve block, the following treatment is recommended:
• Place cold packs and pressure on the affected side• Explain to the patient that he/she may become black and blue on that side
***This is caused by an intravascular injection.
ORAL SURGERY/PAIN CONTROL
The maxillary first molar is innervated by the:
• Anterior superior alveolar and middle superior alveolar nerves• Middle superior alveolar and posterior superior alveola r nerves• Posterior superior alveolar and inferior alveolar nerves• Midd le superior alveolar and palatine nerves
Copyright © 2001 - DENTAL DECKS
Anat
• Middle superior alveolar and posterior superior alveolar nerves
The PSA innervates the distobuccal root of the first molar and distal to it (secondmolar and third molar).
The MSA innervates the mesiobuccal root of the first molar and the two bicuspids.
The ASA (anterior superior alveolar nerve) innervates the canine and incisors.
Remember: In order to extract the maxillary first molar, you must numb both the PSAand MSA nerves as well as the greater (anterior) palatine nerve for palatal anesthesia(soft tissue).
ORAL SURGERY/PAIN CONTROLAnat
Which cran ial nerve listed below provides motor innervation that allows for movementof the mandible?
• Trigeminal (CN V)• Olfactory (CN I)• Facial (CN VII)• Vagus (CN X)
Copyright @ 2001 - DENTAL DECKS
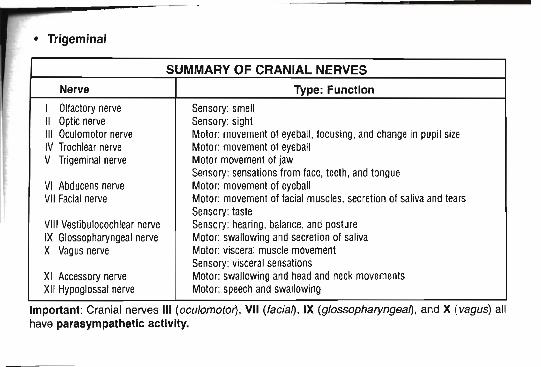
• Trigeminal
SUMMARY OF CRANIAL NERVES
Nerve Type: Function
I Olfactory nerve Sensory: smellII Optic nerve Sensory: sightIII Oculomotor nerve Motor: movement of eyeball, focusing. and change in pupil sizeIV Trochlear nerve Motor: movement of eyeballV Trigeminal nerve Motor movement of jaw
Sensory: sensations from face, teeth , and tongueVI Abducens nerve Motor: movement of eyeballVII Facial nerve Motor: movement of facial muscles. secretion of saliva and tears
Sensory: tasteVIII Vestibulocochlear nerve Sensory: hearing, balance, and postureIX Glossopharyngeal nerve Motor: swallowing and secretion of sal ivaX Vagus nerve Motor: visceral muscle movement
Sensory: visceral sensationsXI Accessory nerve Motor: swallowing and head and neckmovementsXI I Hypoglossal nerve Motor: speechand swallowing
Important: Cranial nerves III tocutomoton, VII (facia~ , IX (glossopharyngea~ . and X (vagus) allhave parasympathetic activity.
ORAL SURGERY/PAIN CONTROLAdren Cart
Which of the following is a metabolic disorder caused by a chronic excess of glucocortlcolds?
• Cushing's syndrome• Addison's disease• Cretinism• Grave's disease
Copyr ight © 2001 - DENTAL DECKS
• Cushing's Syndrome
Four Causes:1. Iatrogenic - caused by chronic therapeutic use of steroids in high doses.2. Abnormal production of ACTH by the pituitary 2..
3. Abnormal production of cortisol by the adrenals,' usually caused by an adrenaltumor (this is the most common cause of Cushing 's Syndrome).
4. Certain non-pituitary neoplasms can produce ACTH (cortisol is normally producedin response to ACTH, therefore excess cortisol is produced).
Characteristics of the patient with Cushing's Syndrome:• Decreased glucose tolerance• Supraclavicular fat pads or " Buffalo hump"• Central obesity or "truncal obesity"• Round "moon" face• Muscular atrophy• Poor wound healing; minor infections may become systemic and long-lasting• The skin may be abnormally pigmented and fragile
Important: The patient's cardiovascular status must be evaluated and treated if necessary prior to surgery.
ORAL SURGERY/PAIN CONTROLAdren Cort
A 52-year-old woman requests removal of a painful mandibular second molar. She tellsyou that she has not rested for two days and nights because of the pain. Her medicalhistory is unremarkable, except that she takes 20 mg of Prednisone daily for erythema multiforme. How do you treat this patient?
• Have patient discontinue the Prednisone for two days prior to the extraction• Give steroid supplementation and remove the tooth with local anesthesia and
sedation• Instruct the patient to take 3 grams of amoxicillin one hour prior to extraction• No special treatment is necessary prior to extraction
Copyright © 2001 - DENTAL DECKS
• Give steroid supplementation and remove the tooth with local anesthesia andsedation
Note: The fear here is that the patient may not have sufficient adrenal cortex secretion(adrenal insufficiency) to withstand the stress of an extraction without taking additionalsteroids. (This holds true for any patient who has been treated for any disease withsteroid therapy.)
Prednisone is a glucocorticoid prescribed as an anti-inflammatory agent.
Remember: Erythema multiforme is a hypersensitivity syndrome characterized bypolymorphous eruption of skin and mucous membranes. Macules, papules , nodules,vesicles, or bullae and target ("bull's-eye-shaped'? lesions are seen. A severe form ofthis condition is known as Stevens-Johnson syndrome. These patients may bereceiving moderate doses of systemic corticosteroids and therefore may be unable towithstand the stress of an extraction. Consultation with their physician is absolutelynecessary before treating these patients.
Adren CortORAL SURGERY/PAIN CONTROL
A person who has been on suppressive doses of steroids will:
• Never regain full adrenal cortical tunctlon .• Take as much as a year to regain full adrenal cortical function• Take as little as a week to regain full adrenal cortical function• Take usually a couple of days to regain full adrenal cortical function
CopyrIght © 2001 - DENTAL DECKS
• Take as much as a year to regain full adrenal cortical function
The following guidelines may help determine if a patient's adrenal function is suppressed, however , if any doubt exists, consult the patient's physician before performing surgery.• People on small doses (5 rng Predisone/day) will have suppress ion when they have
been on the regimen for a month.• People taking equivalence of 100 mg cortisol/day (20-30 rna Predn;sone/dCij() will
have abnormal cortical function in a~• Short-term therapy (1-3 days) of even high dose steroids will not alter adrenal cor
tical function.• A person who has been on su ssive doses of steroids will take as much as a
year to regain full adrenal cortical function.-Remember: Stress or fatigue may cause an adrenal crisis in a patient that has suppressed adrenal function.
ORAL SURGERYIPAIN CONTROL
How much hydrocortisone is secreted by the adrenal cortex daily?
• About 1 mg• About 100 mg• About 20 mg• About 200 mg
Copyright ~ 2001 - DENTAL DECKS
Adren Cort
• About 20 mg
During stress the cortex can increase the output to 200 mg daily.
Remember: Patients taking steroids or people with disease of the adrenals will havedecreased abjlit¥ to produce more glucocorticoids (hydrocortisone) in times of stress(extractions). The reason for this is as follows: Secretion of glucocort icoids is stimulated by ACTH, a hormone produced in the anterior pituitary. The pituitary responds tostress by increasing ACTH output and therefore glucocort icoid production increases.A relative lack of glucocorticoids will also increase output of ACTH. An overabundanceof circulating systemic steroids will inhibit production of ACTH. Patients on large dosesof steroids repress ACTH production which leads to atrophy of adrenal cortex.