Embed Size (px)
Citation preview

ORIGINAL PAPER
Daniel De Wolf Æ Tom Vercruysse Æ Bert SuysNico Blom Æ Dirk Matthys Æ Jaap Ottenkamp
Major coronary anomalies in childhood
Received: 7 March 2002 /Accepted: 3 September 2002 / Published online: 15 October 2002� Springer-Verlag 2002
Abstract Major coronary artery anomalies are ex-tremely rare in childhood. We wanted to assess thehistorical and diagnostic features and the therapeuticoptions of three distinct types of coronary arteryanomalies: abnormal origin of the left coronary arteryfrom the pulmonary artery (ALCAPA), coronary fistulaand coronary stenosis. In a retrospective study, 33children with these types of coronary artery disease wereidentified, 15 with ALCAPA, 12 with fistula and six withcoronary stenosis. History, physical examination, ECG,X-ray, echocardiography, angiography, therapy andoutcome were reviewed. ALCAPA showed distincttypical echocardiographic characteristics. Coronary ar-tery fistula could be identified by a typical murmur andechocardiographic evidence of coronary dilatations.Coronary stenosis should be suspected by the clinicalpicture in a specific context. Conclusion: rare coronaryartery anomalies can be accurately diagnosed in child-hood. Timely therapy yields good prognosis.
Keywords ALCAPA Æ Coronary fistula Æ Coronarystenosis Æ Ischaemia
Abbreviations ALCAPA abnormal origin of the leftcoronary artery from the pulmonary artery ÆLV left ventricle
Introduction
In contrast to the adult population, major coronary ar-tery anomalies are extremely rare in infancy and child-hood. Grossly, coronary anomalies in children can becongenital or acquired. Congenital anomalies can beisolated: abnormal origin of left (sometimes right) coro-nary artery from the pulmonary artery (ALCAPA) ac-counting for 0.5% of congenital heart defects [19],coronary fistula accounting for 0.2% of congenital heartdisease [23], abnormal origin and course of coronaryarteries accounting for 0.17% of sudden death in youngpeople [10] and isolated coronary artery stenosis andatresia [24]. Congenital coronary anomalies can be as-sociated with other cardiac anomalies: (congenitallycorrected) transposition of the great arteries, pulmonaryatresia and intact septum, tetralogy of Fallot, truncusarteriosus as the most common. Acquired coronary dis-ease in children occurs in Kawasaki disease [33], throm-bo-embolic disease and familial hypercholesterolaemia.
Ideally, the diagnosis of coronary artery pathology ismade at the initial assessment by the paediatric cardi-ologist, but in daily practice, this is not always the case.We were particularly interested in the assessment of re-ported non-invasive findings during the initial diagnosticevaluation that could have lead to a correct diagnosis ofmajor coronary disease at that time. We relied particu-larly on the original reports. We wanted to emphasisethose features that alarmed clinicians during routinecardiac assessment. The results of subsequent therapy inthe institutions were reviewed.
Patients and methods
Only patients with clinical signs due to major coronary anomalies,necessitating therapy in the majority of cases, were selected. Ex-cluded were patients with other cardiac malformations obscuringthe signs of coronary disease (i.e. pulmonary atresia and intactseptum), patients with (un-) expected coronary problems during theperi-operative course of cardiac surgery (i.e. tetralogy of Fallotwith infundibular course of the left coronary, transposition with
Eur J Pediatr (2002) 161: 637–642DOI 10.1007/s00431-002-1081-y
D. De Wolf (&) Æ T. Vercruysse Æ B. Suys Æ D. MatthysDepartment of Paediatric Cardiology,Ghent University Hospital, De Pintelaan 185,9000 Gent, BelgiumE-mail: [email protected].: +32-9-2402419Fax: +32-9-2403856
N. BlomDepartment of Paediatric Cardiology, CAHAL,Leiden University Medical Centre, Leiden, The Netherlands
J. OttenkampEmma’s Children’s Hospital AMC,Amsterdam, The Netherlands

‘‘surgically difficult’’ coronary anatomy) and patients with coro-nary aneurysms due to Kawasaki disease but without signs ofmyocardial ischaemia.
Between 1990 and 2001, 33 children (16 female, 17 male) withmajor coronary artery anomalies were identified in two tertiaryunits for Paediatric Cardiology and Surgery, accounting for ap-proximately 6000 operations and interventions during that period(0.5% of paediatric heart defects requiring surgery or intervention).The median age at diagnosis was 5 months (range 1 day to 14years), the median follow-up was 3.5 years (range 2 months to 10years). In a retrospective survey, data which appeared generallyavailable were gathered (Table 1). In the patient history, the reasonfor referral to the hospital or paediatric cardiology unit was noted.In the ECG protocol, signs of myocardial ischaemia (broadQ-waves in I, aVL, V4–6 or T inversion and/or ST depression) orhypertrophy were looked at. In the protocol of the initial echo-cardiography, attention was paid to the description of the mitralvalve papillary muscles (echodensity), mitral incompetence, leftventricular (LV) dysfunction, coronary artery dilatation (subjectivesizing) and abnormal coronary artery colour flow.
Results
The results of the 33 children are presented in Table 1.The most important diagnostic findings are summarisedin Table 2. The results were divided into three sub-
groups: ALCAPA (n=15), coronary artery fistula(n=12), and coronary artery stenosis and/or thrombosis(n=6). In Table 2, the diagnostic features of the AL-CAPA group were also compared to those of a group of11 children with dilated cardiomyopathy (6 male) with amedian age of 2 years at presentation (range 1 day to 14years). ALCAPA is an important differential diagnosisin children with dilated cardiomyopathy.
The ALCAPA group was very young compared tothe others (median 3.5 months). The most prominentsymptoms consisted of respiratory problems and feedingdifficulties. A heart murmur together with signs of heartfailure was encountered in the majority of patients aswere ECG signs of ischaemia. Echo findings showed LVdysfunction with mitral incompetence and papillarymuscle echodensity. In the majority of the patients,subjective sizing disclosed a right coronary dilatation.Only in 50% of the patients was the ALCAPA demon-strated on the initial echocardiogram (by direct visuali-sation of the origin on 2-dimensional echo, or by anabnormal diastolic colour Doppler signal in the pul-monary artery). Angiography to confirm the diagnosiswas performed in all but two patients (in our most recent
Table 1 Patient dataCoronary arteryanomalies
ALCAPA Coronaryfistula
Coronary stenosis/thrombosis
Male (n) 8 7 2Female (n) 7 5 4Age at diagnosis (months) 3.5 46 14.5Follow-up (months) 30 13.5 17.5
Reason for referral including:Respiratory symptoms (n) 11 2 2Heart failure (n) 5 0 0Feeding problems (n) 11 2 1Heart murmur (n) 8 11 1Effort-related irritability (n) 2 0 5Shock (n) 0 0 1
Physical examinationSigns of heart failure (n) 9 0 3Heart murmur (n) 11 10 3
X-ray:Cardiomegaly (n) 14 6 3Pulmonary congestion (n) 2 0 1
ECG:Ischaemia (n) 9 1 3Hypertrophy (n) 10 4 4Normal (n) 1 7 2
Echo:Mitral incompetence (n) 10 1 2Papillary muscle density (n) 9 0 2Abnormal LV function (n) 12 2 4Coronary dilation (n) 10 12 1Abnormal origin (n) 8 0 0
Therapy:Surgery (n) 14 4 4Intervention or medical (n) 0 4 1None (n) 1 4 1Interval presentation/therapy <1 week 1 month 1 monthComplications pre- and post (n) 1 0 1Redo therapy (n) 0 1 0Residual: LV dysfunction (n) 2 0 1Residual: mitral incompetence (n) 6 1 1
638

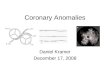
experience) (Fig. 1). In 14 patients, surgery consisting ofdirect re-implantation of the coronary artery in 12 andconnection by tunnel in two was initiated within 1 week.One child died 36 h after surgery due to intractable heartfailure. The others survived with acceptable residual le-sions: mild heart failure lasting beyond 6 months in twopatients and mild mitral incompetence in six. All thesurvivors were asymptomatic. When the patients of theALCAPA group were compared to a group of patientswith dilated cardiomyopathy, papillary muscle echo-density and right coronary artery dilatation (even bysubjective sizing) were clearly distinctive diagnostic fea-tures (Table 2).A total of 12 patients were diagnosed with coronary fis-tula. Their median age was 46months. Almost all patientspresented with and were referred for a murmur, withoutsigns of overt heart failure. On physical examination, themurmur was described as continuous in almost all pa-tients. Ischaemia on ECG was rare. In contrast to theALCAPAgroup, coronary dilatation on echowas seldomaccompanied by echocardiographic features of LV
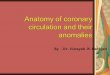
dysfunction. Increased echodensity of mitral valve pap-illary muscle was absent. In 11/12 patients, fistulous flowto the heart chambers could be identified by colourDoppler alone. The connection was left coronary to rightatrium in three, left coronary to right ventricle in four,right coronary to right atrium in one and right coronaryto right ventricle in four. Eight patients were treated; intwo a conservative approach was chosen due to the smallsize of the fistula (spontaneous closure inone1), one re-fused treatment and one is awaiting elective catheter oc-clusion. Of the eight patients treated, four underwentsurgical closure and four underwent coil occlusion(Fig. 2), depending on the institution’s preference. Clo-sure was uneventful in all eight patients, but in one patientre-intervention was necessary because of residual fistulawith mitral incompetence after initial surgery. All treatedchildren were asymptomatic at last follow-up.
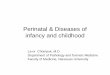
Six patients were diagnosed with coronary occlusion(stenosis and/or thrombosis). Median age at diagnosiswas 14.5 months. Effort irritability was the major reasonfor referral (present in five patients). On physical ex-amination, three patients showed clear signs of heartfailure, and three a heart murmur. On X-ray, cardio-megaly and pulmonary congestion were seen in threechildren and one child respectively. The ECG showedsigns of ischaemia in only 3/6 patients. Echocardiogra-phy showed mitral incompetence with increased echo-density of the papillary muscles in two patients,abnormal LV function in four, and dilated coronaryarteries in only one patient. Angiography was performedin all six patients. Diagnoses were: coronary arterythrombosis in a neonate with familial antithrombin IIIdeficiency, left coronary ostial stenosis in a child 2months after an uneventful arterial switch procedure(normal origin of the coronary arteries), left coronaryartery stenosis due to kinking in a 10-year-old afterneonatal arterial switch and ventricle septal defect clo-sure, one bilateral coronary ostial stenosis in a child withWilliams syndrome, one left coronary artery stenosis ina child with familial supravalvar aortic stenosis, and onebilateral coronary stenosis in a patient with untreatedKawasaki disease (Fig. 3). One child died after heart
Table 2 Diagnostic features.(DCM dilated cardiomyo-pathy, +++ = 100%,++ = 50%, + = 25%–50%,– = 0%–25%, 0 = 0%)
ALCAPA/DCM Fistula Stenosis/thrombosis
SymptomsRespiratory ++/++ ) 0Feeding ++/++ ) )Irritability )/) 0 ++
ExaminationHeart failure ++/+++ 0 ++Murmur ++/) ++ ++ECG ischaemia ++/) ) ++
EchocardiographyMitral incompetence ++/++ ) +Papillary muscle echodensity ++/0 0 )LV dysfunction ++/+++ ) ++Coronary dilatation right ++/0 ++ )Intracardiac fistulous colour flow 0 ++ 0
Fig. 1 Injection of contrast in the pulmonary artery duringtemporary balloon occlusion of the left pulmonary artery showsfilling of the proximal part of the left coronary artery (ALCAPA)
639

catheterisation (myocardial infarction 12 h post-proce-dure), two underwent internal mammary bypass surgery(Fig. 3), one coronary ostial plasty, one coronary arte-rioplasty, and one medical therapy (anticoagulation inthe child with antithrombin III deficiency). Of the fivesurvivors, only the child with Kawasaki disease showeddiminished LV function, another showed mild residualmitral incompetence. All children became asymptomaticafter treatment.
Discussion
Coronary artery anomalies are rare in children. Coro-nary artery anomalies with clinical expression are evenmore exceptional. Important coronary anomalies asso-ciated with a congenital heart malformation can influ-ence the clinical picture, without dominating it, as is thecase in pulmonary atresia with intact septum [15,16].Other silent coronary anomalies, on the other hand,eventually create technical difficulties during correctivesurgery in specific types of heart disease, increasing
surgical morbidity and mortality, as in the arterialswitch operation. Finally, coronary anomalies that areisolated or associated with other diseases can dominatethe clinical picture. In our retrospective study, we ana-lysed the clinical presentation, diagnosis and treatmentof patients belonging to this last group.
ALCAPA was the most frequently encountered cor-onary artery anomaly in our series. As clinical signs areatypical, the diagnosis is not always straightforward.Signs of ischaemia together with impaired LV functionon the initial echocardiogram, mitral valve anomalies as asign of myocardial ischaemia [13], and a dilated rightcoronary artery were clues to the diagnosis. Other diag-nostic means, such as myocardial scintigraphy or serialstudies of cardiac enzymes were not routinely performed.Very few published reports are available testing the pro-spective specificity and sensitivity of cardiac enzymes andnuclear studies for the diagnosis of ALCAPA [28]. Ascoring system combining ECG and echocardiographicfeatures gave a high sensitivity and specificity for thedifferential diagnosis of ALCAPA in a series of childrenwith dilated hearts (in the differential diagnosis of dilatedcardiomyopathy) [9]. In our experience, a reasonablysensitive and specific prospective diagnosis of ALCAPAshould be possible in children with dilated and hypoki-netic left ventricles on the basis of the aforementionedclues by any echocardiologist with a high degree of sus-picion of that particular diagnosis. Probably in case ofdoubt only, neonates and infants with a dilated andhypocontractile LV, need angiographic assessment of thecoronary artery origin to confirm or exclude the diagnosisof ALCAPA [17,27]. Treatment is necessary and urgentin all cases of ALCAPA, because even in asymptomaticpatients a conservative approach carries the risk of sud-den death [14]. Surgical treatment consists of establishinga two coronary vessel system, meaning antegrade flow inboth right and left coronary arteries. This can be achievedby direct re-implantation of the coronary artery in theaorta, by a tunnel or bypass [37]. Simple ligation of theorigin of the left coronary artery has been abandoned dueto frequent continued LV dysfunction and the risk of latesudden death [8]. Even in those cases with severe LVdysfunction, surgical correction should be performed.
Fig. 3 Stenosis of the left cor-onary artery as a consequenceof Kawasaki disease. Aftersurgery, note the neat anasto-mosis of the left internalmammary artery with the leftanterior descending coronaryartery, bridging the stenoticsegment
Fig. 2 Injection in the right coronary artery after coil occlusion ofa large coronary fistula, shows the large coronary fistula, distallyoccluded by the coil. Note the tiny native right coronary artery
640

Despite evidence of myocardial scarring, LV functionimproves and normalises in the majority of patients in themonths following successful correction [7, 18, 29, 31,32].Even the sickest children should not be denied the sur-gical option of re-establishing a two-vessel system [12].
Coronary artery fistula was the second most frequentmalformation encountered in our study. These accountfor 0.2% of congenital heart malformations [23]. Themajority of our patients were asymptomatic. The mostfrequently encountered clinical sign was a superficialcontinuous murmur. In cases of important left to rightshunt, cardiac enlargement was noted on X-ray andechocardiography. Coronary dilation on echocardiog-raphy was noted in all patients. Very small fistula ininfants and small children have a reasonable potentialfor spontaneous closure and should be followed con-servatively [30]. In all the others, elective closure hasbeen proposed due to complications later in life, i.e.heart failure, ischaemia and endocarditis [21]. Surgicalligation or interventional closure with simple or de-tachable coils offer comparable excellent short- andlong-term results [11, 21, 26, 38].
Congenital or acquired stenosis or occlusion of thecoronary arteries was the third clinical entity. This is aless homogenous group, although with more pronouncedclinical symptoms than the two former groups (Table 1).All patients were symptomatic, and all presented a clin-ical picture suggesting heart disease. The ECG was ab-normal in 4/6 cases. Echocardiography on the otherhand did not provide direct diagnosis in any of the casesand angiography was necessary. Associated anomalieswere invariably present. The difficulty of diagnosis is il-lustrated by the longer interval between therapy andinitial presentation in the Paediatric Cardiology De-partment (Table 1). Therapy was initiated after a medianinterval of 1 month compared to less than 1 week for thatother potentially life-threatening condition, ALCAPA.
Two patients presented with ostial coronary stenosisaccompanying supravalvar aortic stenosis. The coronaryanomalies are of three different types: concentric ostialthickening, split-like ostial stenosis by fusion of theaortic valve with the supravalvar stenotic ridge anddiffuse coronary narrowing [38]. Signs of effort-relatedirritability and ECG anomalies together with abnormalLV function or mitral incompetence should alert thephysician to possible associated coronary anomaliesunder these conditions. Surgery consists of coronaryostial plasty or bypass [6,35].
One patient showed coronary artery stenosis as acomplication of untreated Kawasaki disease. The inci-dence of severe coronary artery stenosis or occlusion is4% in untreated Kawasaki disease [33]. In these patients,echocardiographic visualisation of coronary aneurysmswill guide the diagnosis, which can be confirmed bymyocardial scintigraphy or angiography [4]. Our patientwas treated with bilateral internal mammary bypass.Recent reports suggest that percutaneous balloon angi-oplasty could be of equal benefit in post-Kawasakicoronary stenosis [33,41].
Two patients were diagnosed with symptomatic cor-onary artery stenosis after uneventful arterial switch fortransposition of the great arteries out of a total numberof 231 arterial switch operations performed during thatperiod. Coronary artery malpositions are common intransposition of the great arteries. Some of them com-plicate the arterial switch procedure, resulting in in-creased morbidity and mortality due to peri-operativemyocardial ischaemia or infarction [20]. Nevertheless,coronary artery stenosis has been described even after anuneventful arterial switch procedure. Angiographicstudies post-arterial switch report between 3%–10%unexpected coronary artery stenoses [5,34]. Nuclearstudies with thallium and positron emmission tomog-raphy report even higher numbers of perfusion deficits inthese patients [3,39]. The importance of these defects inasymptomatic patients is unclear [40], but some haverelated the incidence of unexpected sudden death afterarterial switch to stenosis of the left main coronary ar-tery [36]. Ostial reconstruction or bypass surgery hasbeen suggested for symptomatic patients [6,22].
The results of coronary artery surgery in infants andchildren are encouraging for the overall group of chil-dren with coronary artery stenosis, provided arterialgrafting is used. The long-term patency of arterial graftsin children is excellent, exceeding 80% after a 10-yearfollow-up in contrast to venous bypass grafts with a 10-year patency of less than 40% [22,41]. This groupshowed less recovery of left ventricular function, sug-gesting the difference between continuous low coronaryperfusion (as in ALCAPA and coronary fistula), com-pared to acute stenosis, especially in children withatypical complaints.
Our last patient suffered a coronary thrombosis as aconsequence of antithrombin III deficiency. This is ex-tremely rare, even including other possible coagulationdisorders [1, 2,25]. Timely medical treatment could re-verse the ischaemic process. Keeping the diagnosis inmind in children with heart failure and a familial historyof coagulation disorder can be lifesaving.
In our retrospective survey we did not encounter anypatients with congenital coronary ostial atresia beingresponsible for severe neonatal heart failure [24] or ananomalous course of the coronary artery out of thefacing sinus of Valsalva being responsible for suddendeath [10].
References
1. Abdurrahman L, Schwartz S, Beekman R (1999) Thromboticocclusion of the main stem of the left coronary artery in aneonate. Cardiol Young 9: 189–191
2. Beattie S, Norton M, Doll D (1997) Coronary thrombosis as-sociated with inherited protein S deficiency: a case report.Heart Lung 26: 76–79
3. Bengel F, Hauser M, Duvernoy C, Kuehn A, Ziegler S, Stoll-fuss J, Beckmann M, Sauer U, Muzik O, Schwaiger M, Hess J(1998) Myocardial blood flow and coronary flow reserve lateafter anatomical correction of transposition of the great ar-teries. J Am Coll Cardiol 32: 1955–1961
641

4. Bjorkhem G, Evander E, White T, Lundstrom N (1990)Myocardial scintigraphy with 201thallium in pediatric cardiol-ogy: a review of 52 cases. Pediatr Cardiol 11: 1–7
5. Bonnet D, Bonhoeffer P, Piechaud JF, Aggoun Y, Sidi D,Planche C, Kachaner J (1996) Long-term fate of the coronaryarteries after the arterial switch operation in newborns withtransposition of the great arteries. Heart 76: 274–279
6. Bonnet D, Bonhoeffer P, Sidi D, Kachaner J, Acar P, Villain E,Vouhe P (1999) Surgical angioplasty of the main coronaryarteries in children. J Thorac Cardiovasc Surg 117: 352–357
7. Brezinski D, Harrison J, Hanson M, Wilson J, Van Trigt P,Bashore T (1994) Ischemic hibernating myocardium demon-strated by positron emission tomography in anomalous originof the left coronary artery from the pulmonary artery. AmHeart J 128: 181–185
8. Bunton R, Jonas R, Lang P, Rein A, Castaneda A (1987)Anomalous origin of left coronary artery from pulmonary ar-tery. Ligation versus establishment of a two coronary arterysystem. J Thorac Cardiovasc Surg 93: 103–108
9. Chang R, Allada V (2001) Electrocardiographic and echocar-diographic features that distinguish anomalous origin of theleft coronary artery from pulmonary artery from idiopathicdilated cardiomyopathy. Pediatr Cardiol 22: 3–10
10. Davis J, Cecchin F, Jones T, Portman M (2001) Major coro-nary artery anomalies in a pediatric population: incidence andclinical importance. J Am Coll Cardiol 37: 593–597
11. De Wolf D, Terriere M, De Wilde P, Reidy J (1994) Emboli-zation of a coronary fistula with a controlled delivery platinumcoil in a 2-year-old. Pediatr Cardiol 15: 308–310
12. Del Nido P, Duncan B, Mayer J, Wessel D, La Pierre R, JonasR (1999) Left ventricular assist device improves survival inchildren with left ventricular dysfunction after repair ofanomalous origin of the left coronary artery from the pulmo-nary artery. Ann Thorac Surg 67: 169–172
13. Donnelly W (1987) Ischemic myocardial necrosis and papillarymuscle dysfunction in infants and children. Am J CardiovascPathol 1: 173–188
14. George J, Knowlan D (1959) Anomalous origin of the leftcoronary artery from the pulmonary artery in an adult. N EnglJ Med 261: 993–998
15. Giglia T, Mandell V, Connor A, Mayer J, Lock J (1992) Di-agnosis and management of right-ventricular dependent coro-nary circulation in pulmonary atresia with intact ventricularseptum. Circulation 86: 1516–1528
16. Hanley F, Sade R, Blackstone E, Kirklin J, Freedom R, NandaN (1993) Outcomes in neonatal pulmonary atresia with intactventricular septum: a multi-institutional study. J Thorac Car-diovasc Surg 105: 406–427
17. Houston A, Pollock J, Doig W, Gnanapragasam J, JamiesonM, Liley S, Murtagh E (1990) Anomalous origin of the leftcoronary artery from the pulmonary trunk: elucidation withcolour Doppler flow mapping. Br Heart J 63: 50–54
18. Jin Z, Berger F, Uhlemann F, Schroder C, Hetzer R, Alexi-Meskhishvili V, Weng Y, Lange P (1994) Improvement in leftventricular dysfunction after aortic reimplantation in 11 con-secutive paediatric patients with anomalous origin of the leftcoronary artery from the pulmonary artery. Early results of aserial echocardiographic follow-up. Eur Heart J 15: 1044–1049
19. Keith JD (1959) The anomalous origin of the left coronaryartery from the pulmonary artery. Br Heart J 21: 149–161
20. Li J, Tulloh R, Cook A; Schneider M, Ho S, Anderson R(2000) Coronary arterial origins in transposition of the greatarteries: factors that affect outcome. A morphological andclinical study. Heart 83: 320–325
21. Mavroudis C, Backer C, Rocchini A, Muster A, Gevitz M(1997) Coronary artery fistulas in infants and children: a sur-gical review and discussion of coil embolization. Ann ThoracSurg 63: 1235–1242
22. Mavroudis C, Backer C, Duffy C, Pahl E, Wax D (1999) Pe-diatric coronary artery bypass for Kawasaki congenital, postarterial switch, and iatrogenic lesions. Ann Thorac Surg 68:506–512
23. McNamara JJ, Gross RE (1969) Congenital coronary arteryfistula. Surgery 65: 59–69
24. Musiani A, Cernigliaro C, Sansa M, Maselli D, De Gasperis C(1997) Left main coronary artery atresia: literature review andtherapeutical considerations. Eur J Cardiothorac Surg 11: 505–514
25. Peeters S,VandenplasY, JochmansK,BougatefA,DeWaeleM,De Wolf D (1993) Myocardial infarction in a neonate with he-reditary antithrombin III deficiency. Acta Paediatr 82: 610–613
26. Reidy J, Anjos R, Qureshi S, Baker E, Tynan M (1991)Transcatheter embolization in the treatment of coronary arteryfistulas. J Am Coll Cardiol 18: 187–192
27. Sanders S, Parness I, Colan S (1989) Recognition of abnormalconnections of coronary arteries with the use of Doppler colorflow mapping. J Am Coll Cardiol 13: 922–926
28. Schlemmer M, Pachinger O, Sochor H, Strigl E, Salzer-MuharU, Wimmer M (1988) Value of myocardial scintigraphy ofcoronary artery anomaly in the differential diagnosis of pedi-atric cardiomegaly. Wien Klin Wochenschr 100: 792–799
29. Schwartz M, Jonas R, Colan S (1997) Anomalous origin of leftcoronary artery from pulmonary artery: recovery of left ven-tricular function after dual coronary repair. J Am Coll Cardiol30: 547–553
30. Sherwood M, Rockenmacher S, Colan S, Geva T (1999)Prognostic significance of clinically silent coronary artery fis-tulas. Am J Cardiol 83: 407–411
31. Shivalkar B, Borgers M, Daenen W, Gewillig M, Flameng W(1994) ALCAPA syndrome: an example of chronic myocardialhypoperfusion? J Am Coll Cardiol 23: 772–778
32. Stern H, Sauer U, Locher D, Bauer R, Meisner H, Sebening F,Buhlmeyer K (1993) Left ventricular function assessed withechocardiography and myocardial perfusion assessed withscintigraphy under dipyridamole stress in pediatric patients afterrepair for anomalous origin of the left coronary artery from thepulmonary artery. J Thorac Cardiovasc Surg 106: 723–732
33. Sugimura T, Yokoi H, Sato N, Akagi T, Kimura T, IemuraM, Nobuyoshi M, Kato H (1997) Interventional treatmentfor children with severe coronary artery stenosis with calci-fication after long-term Kawasaki disease. Circulation 96:3928–3933
34. Tanel R, Wernovsky G, Landzberg M, Perry S, Burke R (1995)Coronary artery abnormalities detected at cardiac catheter-ization following the arterial switch operation for transpositionof the great arteries. Am J Cardiol 76: 153–157
35. Thistlethwaite P, Madani M, Kriett J, Milhoan K, Jamieson S(2000) Surgical management of congenital obstruction of theleft main coronary artery with supravalvular aortic stenosis.J Thorac Cardiovasc Surg 120: 1040–1046
36. Tsuda E, Imakita M, Yagihara T, Ono Y, Echigo S, TakahashiO,KamiyaT (1992)Late death after arterial switch operation fortransposition of the great arteries. Am Heart J 124: 1551–1557
37. Turley K, Szarnicki R, Flachsbart K, Richter R, Popper R,Tarnoff H (1995) Aortic implantation is possible in all cases ofanomalous origin of the left coronary artery from the pulmo-nary artery. Ann Thorac Surg 60: 84–89
38. Van Son, Edwards W, Danielson G (1994) Pathology of cor-onary arteries, myocardium, and great arteries in supravalvularaortic stenosis. Report of five cases with implications for sur-gical treatment. J Thorac Cardiovasc Surg 108: 21–28
39. Vogel M, Smallhorn J, Gilday D, Benson L, Ash J, WilliamsW, Freedom R (1991) Assessment of myocardial perfusion inpatients after the arterial switch operation. J Nucl Med 32:237–241
40. Yates R, Marsden P, Badawi R, Cronin B, Anderson D, TynanM, Maisey M, Baker E (2000) Evaluation of myocardialperfusion using positron emission tomography in infants fol-lowing a neonatal arterial switch operation. Pediatr Cardiol 21:111–118
41. Yoshikawa Y, Yagihara T, Kameda Y, Taniguchi S, Tsuda E,Kawahira Y, Uemura H, Kitamura S (2000) Result of surgicaltreatments in patients with coronary-arterial obstructive diseaseafter Kawasaki disease. Eur J Cardiothorac Surg 17: 515–519
642



















![g y : OpenA g i o A Angiology: Open Access€¦ · 30/07/2015 · coronary anomalies and is found in 0.017–0.03% of patients undergoing coronary angiography [1,2]. However, it](https://img.pdfslide.us/doc/110x75/5fd73119d977e33c90666d22/g-y-opena-g-i-o-a-angiology-open-access-30072015-coronary-anomalies-and.jpg)