-
By .Dr.Vinayak.M.Nadiger
**
-
Coronary arteryCoronary artery is a vasa vasorum that supplies
the heart.
Coronary comes from the latinCoronariusMeaning Crown.*
*
-
Coronary arteryThe coronary artery arises just superior to the
aortic valve and supply the heart
The aortic valve has three cusps
#left coronary (LC), #right coronary (RC) #posterior
non-coronary (NC) cusps.
*
*
-
Each artery arises from respective aortic sinuses
- Right coronary sinus(anterior)(RCA) - Left coronary sinus(left
posterior)(LCA) - Non-coronary sinus(right posterior)(No coronary
artery)The coronary arteries and their major branches are
sub-epicardially locatedLCA ostium -4.7mm(Range 1.0 -8.5)RCA
ostium-3.7mm(Range 0.5 -7.0)RCA takes off at right angle and LCA
takes off at more acute angles
*
-
*
-
*
-
*
-
Right coronary arteryOriginates from right coronary sinus of
Valsalva Courses through the right AV groove between the right
atrium and right ventricle to the inferior part of the septum
*
*
-
Branches of RCA*Conus branchSINU NODAL BRANCHAV Nodal Branch
*
*
-
Conus branch 1st branch supplies the RVOTSinus node artery 2nd
branch - SA node.(in 40% they originate from LCA)Acute marginal
arteries-Arise at acuteangle and runs along themarginof the right
ventricle above the diaphragm.Branch to AV nodePosterior descending
artery : Supply lower part of the ventricular septum & adjacent
ventricular walls.
Arises from RCA in 85% of case.
*
*
-
Proximal - Ostium to 1st main RV branchMid - 1st RV branch to
acute marginal branchDistal - acute margin to the crux
*
-
Right coronary anatomyAOLARCACONUS BR RCASAN1234RCAAM*
*
-
RCAAMAM*
*
-
Area of distributionRT CORONARY ARTERY----1)Right
atrium2)Ventriclesi) greater part of rt. Ventricle except the area
adjoining the anterior IV groove.ii) a small part of the lt
ventricle adjoining posterior IV groove.3)Posterior part of the IV
septum4)Whole of the conducting system of the heart, except part of
the left br of AV bundle *
*
-
DOMINANCEDetermined by the arrangement that which artery reaches
the crux & supply posterior descending artery
The right coronary artery is dominant in 85% cases.
8% cases - - circumflex br of the left coronary artery
7% both rt & lt coronary artery supply posterior IVseptum
& inferior surface of the left ventricle-here it is balanced
dominance.
*
*Whichever artery crosses the crux of the heart and gives off
the posterior descending branches is considered to be the dominant
coronary artery.*
-
Left coronary artery Arises from left coronary cuspsTravels
between RVOT anteriorly and left atrium posteriorly.Almost
immediately bifurcate into left anterior descending and left
circumflex artery.Length 10-15mm
*
*The venous drainage of the heart is carried out by 3 types of
vesselsCoronary sinus Larger vein draining 75% of total coronary
flow. It drains from left side of heart.Anterior coronary veins
drains from right side of heartThebesian veins- drians blood from
myocardium into concerned chambers of heart.
*
-
*
*37% OF PATIENTS HAVE TRIFURCATION OF LEFT coronary artery, with
an intermediate or ramus medianus artery arising between the LAD
and circumflex coronary artery.*
-
LEFT CORONARY ARTERY*
*
*
-
For practical purposes is a continuation of the LMCAPasses to
the left of pulmonary trunk and travels into the upper portion of
IV sulcus.As it turns around the pulmonary artery and begins its
downward course the LAD forms a 90* angle often highlighted by
origin of 2nd diagonal .
*
-
LAD BRANCHES1) Diagonals2) Septals3) RV branches4) Terminal
branch
*
-
Proximal - Ostium to 1st major septal perforator or 1st diagonal
artery whichever is firstMid - 1st perforator to D2 (90 degree
angle)Distal - D2 to end
*
-
Departs at a sharp angle from LM to run posteriorly along the AV
groove towards the crux cordis.Reaches crux only in 16% casesCourse
nearly mirrors that of RCA.
*LCx supplies 15-25% of LV (40-50% in dominant LV)*
-
Proximal - Ostium to 1st major obtuse marginal branchMid - OM1
to OM2Distal - OM2 to end
*
-
LT CORONARY ARTERY1) Left atrium.2) Ventriclesi) Greater part of
the left ventricle, except the area adjoining the posterior IV
groove.ii) A small part of the right ventricle adjoining the
anterior IV groove.3) Anterior part of the IV septum.4) A part of
the left br. Of the AV bundle.*
*
-
Coronary Venous Anatomy of the HeartThe cardiac veins can be
grouped into the following categories, according to the region
being drained: the CS and its tributaries , the anterior cardiac
veins, the thebesian veins.
*
*
-
*
*
-
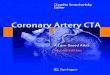
Normal coronary venous anatomy on volume-rendered images from
contrast materialenhanced coronary CT angiography. (a)
Anterolateral view of the heart shows the anterior interventricular
vein (AIV) coursing through the anterior interventricular sulcus
parallel to the left anterior descending artery (LAD). It continues
as the great cardiac vein (GCV) in the left atrioventicular groove
along with the left circumflex artery (LCX).
*
*
-
Posteroinferior view of the heart shows the GCV continuing as
the CS, which finally drains into the right atrium (RA). Also shown
are the posterior interventricular vein (PIV) accompanying the
posterior descending artery (PDA), the posterior vein of the left
ventricle (PVLV), and the left marginal vein (LMV) accompanying the
obtuse marginal artery (OMA).
*
*
*
-
CS and Its Tributaries The major tributaries of the CS include
(a) the anterior interventricular vein, (b) the GCV, (c) the left
marginal vein and posterior vein, and (d) the middle cardiac vein
or posterior interventricular vein
*
*
-
The anterior cardiac veins are the primary venous return for the
anterior wall of the right ventricle. There are three or four small
veins total, which ultimately drain into the right atrium, although
the pattern of drainage is diverse. Each vein may open directly
into the right atrium, or the veins may coalesce to form a common
venous trunk before emptying into the right atrium
*
*
-
The thebesian veins (venae cordis minimae) are a number of small
veins that drain the subendocardium. They are composed of
endothelial cells and are continuous with the endothelial lining of
the cardiac chambers.
*
*
-
*
*
-
*
*
-
*
*
-
*
-
**
-
Anatomic VariantsCartoon courtesy of Dr. Fred Wu, Childrens
Hospital Boston
**
-
Anatomic VariantsCartoon courtesy of Dr. Fred Wu, Childrens
Hospital Boston
**
-
Classification: Anomalies of origin.Anomalies of
course.Anomalies of termination.Intrinsic
*
-
*
-
*
-
*
-
*
-
*
-
*
-
*
-
*
-
RCA
*
-
*
-
*
-
RCALADLADRCA
*
-
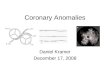
Anomalous origin of the right coronary artery (black arrow) from
pulmonary artery. Note the dilated tortuous coronary artery and
multiple collaterals.
*
-
Volume-rendered image of a Bland-White-Garland syndrome in a
right anterior oblique view. The RCA is dilated. The LAD originates
from the pulmonary artery (arrow) and is also markedly dilated and
tortuous.
*
-
*
-
*
-
Lt. Coronary SinusRCA
*
-
Rt. Coronary SinusLCAPulmonary Trunk
*
-
Rt. Coronary SinusLCARCA
*
-
*
-
Band of myocardial muscle overlying a segment of a coronary
artery.
It is most commonly localized in the middle segment of the LAD
artery
*
-
Myocardial bridging often occurs without overt symptoms.
In some cases, however, myocardial bridging is responsible for
angina pectoris, myocardial infarction, life-threatening
arrhythmias, or even death
*
-
*
*
-
LAD
*
-
Duplication of the LAD artery consists of a short LAD artery,
which courses and terminates in the anterior interventricular
sulcus without reaching the apex, and a long LAD artery, which
originates from either the LAD artery proper or the RCA, then
enters the distal anterior interventricular sulcus and courses to
the apex
*
-
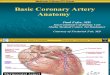
Duplication of LAD seen on volume-rendered image of the heart
(A) and coronary tree image (B). Note a short LAD (black arrow),
which terminates high in the anterior interventricular groove
without reaching the apex and a long LAD (white arrow) which
courses parallel to the short LAD, enters the distal anterior
interventricular groove and supplies the apex.
*
-
LAD
*
-
*
-
*
-
*
-
*
-
Fistula between the RCA and the coronary sinus (CS) depicted by
three-dimensional reconstruction (Panel A) and multiplanar
reformation (Panel B).
*
-
Fistula between the LAD and the right ventricle displayed on
three-dimensional reconstructions (Panel C) and the corresponding
conventional angiogram (Panel D).
*
-
*
-
*
-
*
-
*
-
*
-
*
-
Intrinsic Coronary Arterial Abnormalities
1. Coronary stenosis.Though coronary stenosis is mostly
acquired, congenital coronary stenosis has been describedand can be
ostial (due to a valve-like ridge of the aortic wall or fusion of
the aortic leaflets and aortic wall) or peripheral.
2. Congenital Atresia of the Left Main CA. In this condition
there is complete atresia of the left coronary ostium, so the
entire coronary arterial supply to the heart is derived from the
RCA and its branches. The LAD and LCX are seen in their respective
locations,but they receive blood from the RCA.
-
This is an extremely rare condition and differs from a single
RCA because some of the branches fill retrograde through the
RCA.The collateral circulation from the right to the left coronary
system is usually not sufficient so almost all patients eventually
develop myocardial ischemia.
*
-
3. Coronary Artery Ectasia or Aneurysm. This lesion is defined
as a coronary artery with a diameter of more than 1.5 times the
adjacent normal segment and can be either focal or diffuse.
Coronary aneurysms may be congenital or acquired; in the
acquired group, Kawasaki disease is the most common cause of
aneurysms worldwide.
Congenital aneurysms are more commonly described in the RCA.
Possible complications include myocardial infarction from
embolization of thrombus.
*
-
*
-
*
-
*
*
-
*
*
**
*
*
*
*
*
*
*
*
**
*
*
*
*
*Whichever artery crosses the crux of the heart and gives off
the posterior descending branches is considered to be the dominant
coronary artery.**The venous drainage of the heart is carried out
by 3 types of vesselsCoronary sinus Larger vein draining 75% of
total coronary flow. It drains from left side of heart.Anterior
coronary veins drains from right side of heartThebesian veins-
drians blood from myocardium into concerned chambers of heart.
**37% OF PATIENTS HAVE TRIFURCATION OF LEFT coronary artery,
with an intermediate or ramus medianus artery arising between the
LAD and circumflex coronary artery.**
**
*
*
*LCx supplies 15-25% of LV (40-50% in dominant LV)**
*
*
*
*
*
**
*
*
*
*
*
*
**
**
**
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
**
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*