Embed Size (px)
Citation preview


Maharashtra Medical Council Accredited CMEs conducted at BARCHospital since the date of accreditation, March 28, 2011
Date Department Topic Speaker
July 8, 2011 Obstetrics & Cervical Cancer Prevention Dr. Mukesh Gupta
Gynaecology and Management - Dr. Amita Maheshwari
Unveiling New Facts
August 26, 2011 Chembur Dispensary Geriatric Medicine D~ Rekha Bhatkhande
D~ H. K. Hase
D~ Bharat Shah
October 14, 2011 ENT What is New is ENT, D~ Prabodh Karnik
Head & Neck Dr. Pragnya Parikh
Dr. Pankaj Chaturvedi
December 9, 2011 Pediatric Challenges in Dr. Mamta Manglani
Pediatric Infections Dr. Ira Shah
Dr. Anand K. Shandilya
February 3, 2012 Anesthesia CPCR & Organ Transplant Dr. Khusrav B. Bajan
D~ Rahul Pandit
Dr. Sanjay Nagral
March 30, 2012 Surgical Palliative Care for Dr. Mary Ann Muckaden
life-limiting illness D~ P.N. Jain
Dr. Sheila N Myatra
June 1, 2012 Medicine Rheumatology D~ Vikram Londhey
Dr. Balkrishnan
Dr. Sunil Singh
August 3, 2012 Radiology Non Invasive Dr. Hemant Telkar
Vascular Imaging - Dr. Deepak Patkar
Role of a & MRI D~ Susheel Kumar
October 5, 2012 Pathology Update in Laboratory Dr. Varsha Vadera
Medicine Dr. Avinash Phadke
Dr. Prema Varthakavi


1'rom tHe 'Etlitor's 1Jesk.. _-------------------------------------------------------Pulse
This issue of 'Pulse' focuses on 'Renal disease '. The guest article by Dr. Viswanath Billa has
illustrated the objective of BP regulation which is to ensure that enough blood flows to each organ
which is physiologically adequate and not injurious. In the physiological aspects, the Pressure
Natriuresis Curve and its fundamental correlate to the underlying physiological regulation i.e.
increase in salt intake, increase in BP and the role of various regulatory mechanisms like nervous
and renal have been explained in detail. In short, the correlation of cardiovascular and renal
systems, has been explained clearly. In pregnancy, renal disease can get manifest in gestational
hypertension and diabetes. Timing of delivery can prevent the progression of renal disease in such
cases. The women with chronic renal disease who opt for pregnancy are at increased risk of rapid
deterioration of renal function.
As a part of infection control measures, CDC's core guidelines during dialysis procedures are
suggested. In these procedures as there is direct access to the blood stream in haemodialysis and to
the closed peritoneal cavity in chronic ambulatory peritoneal dialysis through various tubings/
catheters, the strict compliance with these guidelines shall help to minimize infection related
complications.
Lastly, a message for the Resident Medical Officers and the Nursing staff with regard to the
generalized care of the hospitalized patients from patient's safety point of view:
1. Use of standardized abbreviations and dose designations.
2. Prompt writing of clear, concise and legible admission orders with date and time and the
legible signature.
~ . 1~v'~(Dr. Amrita Misri)
3. Prevention of nosocomial infections by strict adherence to the Infection control practices.
4. Excellent communication among the physicians, nursing staff and the patients/relatives.
We dedicate this issue of 'Pulse' to our senior colleague, Late Dr. D.K. Iaitley, then Head ofAnaesthesiology and Head Medical Division, whose dedication to Medical Division has alwaysinspired us. Dr. Jaitley has given us the opportunity to work for the 'Pulse'.

(jtUSt.flLrtide=------------------------------------------------------Pulse
What has Salt got to do with Blood Pressure?Dr. Viswanath Billa MD, DM
Associate Professor of Nephrology,Consultant Nephrologist and Transplant Physician, Bombay Hospital
A pioneering observation was made by t NeiChing, in a classicChinese text, dated 100 BCthatlinked, for the first time, hypertension and saltintake. In his treatise he refers to hypertensionas, "the 'hard pulse' resulting from a high saltintake".
This article attempts to study the data availableto date on this subject and current understandingand research that establishes a link between saltas a risk factor to the development ofhypertension. In the course of this paper, asystematic analysis of epidemiologic data,evolutionary correlates, physiological correlatesand randomized control trials has been done, inan attempt to understand this relationship.
Epidemiologic data:Lewis Dahl made some seminal observations onsalt intake and the prevalence of hypertension indifferent geographic areas and races, which waspublished in the American Journal of ClinicalNutrition in 1972. As seen in Fig.1, he noted thatessential hypertension isseen primarily in societies
with average sodium intakes above 100 meq/day(2.3 g sodium); it is rare in societies with averagesodium intakes of less than 50 meq/day (1.2 gsodium).These observations do suggest that thedevelopment of hypertension requires a thresholdlevel of sodium intake.
The most significant modern epidemiologicresearch was the INTERSALTStudy, which was aworldwide study that tested both within andcross-population prior hypotheses on 24 hoursodium excretion and blood pressure.The relationbetween these two variables was studied in10079 men and women aged 20-59, sampledfrom 52 centres around the world based on ahighly standardised protocol and extensive qualitycontrol. The results are depicted graphically in theSodium excretion ranged from 0-2 mmol/24 h(Yanomamo Indians, Brazil) to 242 mmol/24 h(north China). In individual subjects (withincentres) it was significantly related to bloodpressure. Four centres found very low sodiumexcretion, low blood pressure, and little or noupward slope of blood pressure with age. Across
the other 48 centres sodium wassignificantly related to the slope of bloodpressure with age but not to median bloodpressure or prevalence of high bloodpressure. Potassium excretion wasnegatively correlated with blood pressurein individual subjects after adjustment forconfounding variables. As seen in Figs.2&3and Table1, there clearly is a relationshipbetween salt intake and blood pressure inthe subjects of this study. Also, thecomparative data showing saltconsumption and BP between low saltconsuming populations versus the rest ofthe populations studied clearly shows a BPadvantage in the low salt consumingpopulations.
jU
JAPANESE(NORTHERN JAPAN)
E.9 -~ 20 -$
JAPANESE~~ • (SOUTHERN JAPAN)u0z~ • AMERICANS (NORTHERN U.S.)<;:
."~ 10 - -
'";2 • MARSHALL ISLANDERS (PACIFIC)
~4 ESKIMOS (ALASKA)
I I I0 10 20 30 40
% HYPERTENSIVES
Fig.1: Salt intake and hypertension
Vol. 14 November 2012 II

~q_~_t_~· Pulse
Table 1: Comparison of Four Low Sodium Centres and Remaining 48 INTERSALTCentres
Variables Yanomamo Xingu Papua Kenya RemainingNew Guinea 48 centres
Lifestyle Factors24-hour sodium
(mmol-median) <1 6 27 51 160Sodium/potassium
ratio (meadian) <0.01 0.08 0.48 1.8 3.4BMI 21.2 23.4 21.7 20.8 25.2Alcohol drinkers (%) 0 0 8.7 30.7 53.0
Blood pressureSystilic BP(median) 95.4 98.9 107.7 109.9 118.7Diastolic BP (median) 61.4 61.7 62.9 67.9 74.0Hypertensive (%) 0 1.0 0.8 5.0 17.4Systolic slope with age
(mmHg/l0yr) -1.1 +0.6 -1.4 +2.4 +5.0
*Systolic blood pressure (BP)of 140 mm Hg or more, diastolic BPof 90 mm Hg or more, or receivinganthypertensive therapy.
BMI, body mass index. What Dahl published as an observation ofsalt consumption and blood pressure is fairlycongruous to the results of the randomised
A control trial, INTERSALT.;80 mmHg
.~ soli Oddll!:C }0- __ 0 no s ctt odde<l 10 tooa
B.-hdm.aS lI5-lOQ}
W~I~s (~aq)
~=.arsl.(R&rOIO"9n.)(! eQ}6e~g,um (t11Q)Swlt'dH'\
...•Porlu~~1 (:'1119)
Unlleod Stale'S (fi-IOg)
~ 120V)
160
100
7.0-29 40-49
,60-69 AQI
Fig.2: Relationship between salt intake and bloodpressure: age-wise distribution
4O~----------------------------~~~=-36
Dahl, 160slope" +lOmmol Na-+1.0% prevalence
31
28
20
06
02
,207
,259
,300
26 9NaCVd
, , mmol
362 414 466 Nald1~5
Fig.3: Relationship between salt intake and bloodpressure: across diverse races
Why do humans need salt?Sodium is a vital constituent of the body'sionic composition. In order to maintainextracellular fluid volume, 2500 mEq i.e150gm of sodium is necessary. In order totrigger the intracellular action potential300mEq i.e. 18gm of sodium is required. Ifsalt is essential for life, then why does saltcause disease? Is there a finite threshold ofsalt consumption that is essential for healthand anything beyond this becomescounterproductive to good health?
Salt and Human evolution: We now believethat salt has some causal relation with BP.But we have not been able to establish amechanistic link between the two. Medicinehas historically been concerned withmechanistic or 'proximate' answers toquestions of how diseases develop andcause pathology. This approach may notfully explain disease causation. In contrast,evolutionary, or 'ultimate' questions,frequently ask 'why' structures or functionsare as they are. A full explanation of adisease should ideally address both.
II Vol. 74 November 2072

~q_~_t_~·k Pulse
Life evolved as a unicellular organism. This lifeform had a simple process for nutrient deliveryby diffusion across the cell membrane to provideenergy to simple processes of life. As animalsevolved, body size increased, and delivery ofnutrients to cells came to exceed the range ofdiffusion. Simple systems capable of supportingcellular metabolism arose, and natural selectionwent on to shape our staggeringly complex,highly integrated cardiovascular system. In amulticellular organism processes got centralised.There needed to be an organisational structure,no multiplication of responsibility, goodcommunication lines, systems that would deliverinput and carry back the output. i.e. a circulatorysystem. Blood pressure thus became an ernerqent 'property of this system. Blood pressure, however,cannot be reduced to the individual elements ofthe circulation. It is a function of all of themacting in concert; it is an emergent property ofthe entire system. All hierarchically organizedbiological systems have higher order emergentfunctions that depend on, but are not predictablefrom, the structures and functions of lower levels.Because emergent properties are lost when asystem is disaggregated, integrative physiologyis critical to understanding blood pressureregulation.
Human beings are believed to have originated incentral Africa. In this location, far away from anyphysical contact to salt in the environment, wherediet consisted of what could be gotten by huntingand gathering, sodium conserving genotypesevolved. Since the source of sodium was limited,the body's requirement of sodium was regulatedby minimizing losses. As humans migrated outof central Africa, selection pressure for sodiumconservation declined in the cooler, wetterclimates of the northern latitudes and coastalareas of Africa. However, genetic drift ensuredthat ancestral sodium-conserving genotypespersisted. If genes originally selected for sodiumconservation changed the set point of the renalpressure-natriuresis to a higher blood pressurerange when expressed in an environment ofsodium abundance, individuals harboring such
genotypes could be at increased risk of developinghypertension. To explain this phenomenon, JamesNeel proposed the 'thrifty genes' hypothesis. Inprinciple, this hypothesis suggests that any lifeforms genetic makeup improve an organism'sability to conserve nutritional resources obtainedin times of abundance thereby favoring survivalduring times of want. This ensures reproductivesuccessand the survival of that life form. Thus achanged environment posed a challenge to thegenetic framework that was by nowprogrammed to conserve salt. A tradeoff in thisscheme of things was the development ofhypertension.
Physiological explanation: The fundamentalobjective of BP regulation is to ensure thatenough blood flows to each organ, avoidingcompetition between organs, adjusting BP tothe need of that organism at that time point,and helping keep BP at a level where it isphysiologically adequate and not injurious.
Guyton developed a 'Systems Engineering' modelor Physiome, which he called 'SAPHIR'-"aSystems Approach for Physiological Integrationof Renal, cardiac, and respiratory functions"(Fig.4). The idea behind the Physiome is to seethe organism as an integrated system in whicheach organ plays a role.
He then hypothesised the concept of Hierarchyof Control systems and its contribution to BPregulation. He established a temporal patternof this and classified them into,1.short-term (damping), where cardiovascularreflexes regulated blood pressure, mediated bythe nervous system2. intermediate-term (damping) where capillaryfluid shifts, delayed compliance of thevasculature, hormonal controls (Agll, AVP)regulated blood pressure.3. long-term (control), where the kid neymanages overall fluid and solute balance, whichdetermines the baseline level of BP. Thismechanism had infinite gain.
Vol. 14 November 2012 II



f:uest.f!lrtide~~------------------------------------------------------Pulse
00 !!
..•.:l :.= :l'~I
~I
• 1~ 1
: 1: 1~I·,&'• 1J!,• 1~::t:
I '-,1
Aldosteron.<-----
o 0 15 30 I 2 4 8 1632 I 2 4 8 161 2 4 8 16····00
'-v-'~~~Seconds Minutes Hours Doys
Time after sudden change in pressureFig.5: Degree of activation, expressed in terms of feedback gain, ofdifferent pressure control mechanisms following a sudden change inarterial pressure. Note the rapid activation of the nervous mechanisms,the moderately rapid activation of several intermediate pressure controlmechanisms, and the slow but extremely powerful activation of the renal·body fluid presusure control system.
This hierarchy of pressure control systems (Fig.S)very elegantly demonstrates how blood pressureregulatory mechanisms influence BP as a timedependent variable, and how the early responsesare quick to react but inefficient, and the lateresponses are slow to react but more efficient.
The Pressure-Natriuresis Curve is the functionalcorrelate of this underlying physiologicalregulation (Fig.6).
An increase in sodium intake shifts the curve tothe right ensuring that a similar amount ofsodium gets excreted. The tradeoff of thisregulatory mechanism is an increase in bloodpressure. The curve also depicts the infinite gainfeature of the kidney - blood volume - pressureregulator (Fig.7,8,9). Guyton also used this curveto analyse arterial pressure regulation in severalaltered functional and pathological states of thekidney such as reduced kidney mass, Goldblattkidneys and high aldosterone and angiotensinstates.
The concept of Salt Sensitivity: This term is theblood pressure responsiveness to variations inNa intake. There is as yet no biochemical nor
clinical criteria for this trait. However severalfeatures of this state and factors associated withthis state are described in the Tables 2&3.
Randomised control trials to study theassociation between salt intake andhypertensionThere are several ways to determine saltconsumption. While dietary recall appears to 'bea reasonable method, it can be quite erroneous.Measurement of the 24 hr urine excretion of Nais a fairly accurate method to estimate saltconsumption and is based on the principle thatin a steady state, in health or in disease, saltconsumption mirrors salt excretion. (Fig.10).There have been several formulae devised to
tOO
t t t&AI" 0 05 '0
t••
oL...:::~~===~_10 20
SECONDFig.6: Correction of arterial pressure back toward the controllevel by the baroreceptor reflex following an initial abnormalrise in pressure. Note that the feedback gain in this instanceis 1.6 after the reflex has become fully developed.
O~----T---~--~--'---C---~~Z 4 S a .() 01>
HOURSFig.7: Function of the kidney-blood volume feedback controlsystem to correct the arterial pressure back to normal followingan initial abnormal pressure rise. Note that the arterial pressurereturns all the way back to normal and that the feedbackgain is infinite when full correction has occurred.
II Vol. 14 November 2012

ytuSt.9lrtide~---------------------------------------------------Pulse
estimate daily salt excretion from a spot urinesodium.
The relation between salt consumption andhypertension has been studied in several animalmodels.
In Fig.11, salt was added to the usual low Nadiet of chimpanzees and the quantitative effecton average BPin this experiment was substantial.With 5 g salt per day, systolic pressure rose12 mm Hg whereas with a 15 g salt intake thesystolic pressure increased by 26 mm Hg. Whenthe experiment was stopped and the original dietwas restored, the original low blood pressurewas restored.
~ O+-----~~----r_----_r----~~~ 0 ~ ~ ~ARURIAl PRBro~E( Hg l
Fig.S: The pressure-natriuresis Curve
a~ oL-----~~--••~~====~~ _50 100 150
ARTERIAL PRESSURE (mmHg)
Fig.9: Increase in sodium intake & its effects
Table 2: Features of Salts-Sensitive HypertensionEpidemiologic fetures
Black raceObesityAdvanced ageDiabetesRenal dysfunctionUse of cyclosporine
Clinical featuresMicroalbuminuriaAbsence of normal nocturnal decrease inblood pressureAbsence of modulation of blood flow with
sodium loading
The Diet and Systolic Hypertension (DASH) isanother powerful study that studied the effectof salt on blood pressure prospectively. (Fig.12).Unlike the other studies done so far, DASH wasa Sodium intake study. It attempted to answerseveral relevant questions by analysing the effectof a usual north American diet as compared to aDASH diet on a little more than 200 subjects ineach arm. About 40 percent of these subjectswere hypertensive. The DASH diet consisted offruits, vegetables, and low-fat dairy products,that included whole grains, poultry, fish, andnuts, with only small amounts of red meat,sweets, and sugar-containing beverages. In eacharm, 3 subgroups were created with 3.5, 2.3and 1.2gm sodium respectively. The hypothesisgenerating questions were,1. Does reducing the level of sodium from 150
rnrnol/day (S.7 g of salt) to below 100 mrnol/day, lower BPmore than reducing the sodiumlevel only to the recommended limit?
2. Does the DASH diet lower the blood pressurebeyond the level achievable by simplyreducing sodium intake?
3. What is the combined effect of the DASH dietand reduced sodium intake?
The results were interesting. Reducing the sodiumintake from the high to the intermediate level
Vol. 14 November 2012 II

t::uestJbtide~~------------------------------------------------------Pulse
Table 3 Factors associated with sodium retention
Reduced sodium filtrationDecrease in ultrafiltration coefficientDecrease in single-nephron glomerular
filtration rateIncreased sodium reabsorption
Increase in vasoconstrictor expression:angiotention II, aldosterone, andhyperactive sympathic nervous system
Decrease in vasodilator expression: nitric oxide,kallikrein, dopamine, and vasodilatory
prostaglandinsAltered regulation or altered expression of
sodium channel s in the renal tubules
Fig.10: Comparison of measured andestimated excretion
Kawasaki'S equatfOn Tanaka's equation
N=l36R=O.563
: r ' "":'"
~~f':. "
,/,L--~ --',Estimated Na (mmoVday) Estimated Na(mmoVday)
reduced the systolic blood pressure by 2.1 mmHg (P<0.001) during the control diet and by 1.3mm Hg (P=0.03) during the DASHdiet. Reducingthe sodium intake from the intermediate to thelow level caused additional reductions of 4.6 mmHg during the control diet P<0.001) and 1.7 mmHg during the DASH diet (P<0.01). The effectsof sodium were observed in participants with andin those without hypertension, blacks and thoseofother races, and women and men. The DASHdiet was associated with a significantly lowersystolic blood pressure at each sodium level; andthe difference was greater with high sodium levelsthan with low ones. As compared with thecontrol diet with a high sodium level, the DASHdiet with a low sodium levelled to a mean systolic
Before Treatment period160r---r-:G::-ro-u-ps-------r----,
• Experimental(Na added.n= 10)
o Control(n= 12)
After
II
150140
Systolic 130
C; 120IE 110.se 100::lenen 90ea. Mean"0 80001ii 70 .
60Diastolic
5040~~-r---r-~~-~
oe Dee JunNov91
Mar AugNo... Mar
93 93 93 94Date
Fig.11: Relationship between salt consumptionand hypertension: animal model
92
blood pressure that was 7.1 mm Hg lower inparticipants without hypertension, and 11.5 mmHg lower in participants with hypertension.
Severalpapers and meta analysesof these studieshave come to similar conclusions which have ina scientific manner established credence to the
135
-2.1Coorrot ctier r<-10 -0.8>t
-5.9 : ----.... -4.6
~ 130 (-8.0to-3.71,t. ~ 1~-5'9tO-3'2)t::: : -5.0 :~ '(-7.6Io-2.51t~
~ DASH diet • .•. -2.2
g _13.(-4.4to-O.W'm 125 1-2.61~O.O)· -------.... t(.) -1.7 •(5 (-3.010 -OAIt
~sn 120+----.----r------..
A
High Intermediate
Sodium Level
Low
Oi 85:I:E.s
-1.1
Control die' T~ -0.21t-2.9 : -2.4
~ 1-4.310-1.5,* ~ -2.5 r~-3.JtO-L51t~ , (-4.110 -0.8It
£. 80 DASHdie' ·------.-.(-2.~!~O.4) t
] l-l:;~:O.2) ~~~ 1- 1.9 to -O.1)t
"~o 75+------.-------r--------..B
High Intermediate
Sodium Intake
Low
Fig.12: Effect of salt on blood pressure:DASH model
Vol. 14 November 2012

t:lUStJ1lrticle~~------------------------------------------------------Pulse
IGene \
IB~IOgy I
I Salt sensitivity I
I
PhYSi~9YI
I Pressure-Natriuresis curve IFig.13: Causal relationship between salt consuption & hypertension
I Evolution
hypothesis that salt consumption is linked to thedevelopment of hypertension. Evenlooking at theoutput side, drugs that increase sodium loss likethe thiazides are potent drugs to control bloodpressure.
Seemingly the search for the causal relationshipbetween salt consumption and hypertension byepidemiologic data, evolutionary correlates,physiological correlates, pathological markersand randomized control trials, has come fullcircle. (Fig.13).
What now remains is how effectively we are ableto use this data to implement salt restriction toreduce cardiovascular morbidity and mortality.
1. Lewis K Dahl.The American Journal of ClinicalNutrition 25: February 1972, pp. 231-244.
2. Jeremiah Stamler. Am J Clin Nutrition1997:65(suppl):626S-42S.
Pathology
3. Alan B.Wader.Evolution and Hypertension2007;49;260-265.
4. Effects on blood pressure reduced dietarysodium and dietary approaches to stophypertension (DASH) diet. Frank M.Sacks,NEngl J Med, Vol. 344, No.1, January 4,2001
5. Links Between Dietary Salt Intake, Renal SaltHandling, Blood Pressure, andCardiovascular Diseases Pierre Menton,Physiol Rev 85: 679-715, 2005;
6. Guyton, Coleman, Granger (1972) Ann. Rev.Physiol
7. Subtle acquired renal injury as a mechanismof salt sensitive hypertension. Richard JJohnson. N Engl J Med, Vol. 346, No. 12,March 21, 2002
Vol. 74 November 2072 II

-------------------------------------------------------Pulse
Kidney Disease in PregnancyDr. Gayatri Modi, Dr. Rashmi Singh, P.G.RMOs,
Dr. Santoshi Prabhu, Medical OfficerDepartment of Obstetrics & Gynaecology, BARC Hospital.
Introduction
During normal pregnancy, virtually every organ
system undergoes anatomical and functional
changes. The kidneys also undergo marked
haemodynamic, tubular and endocrine changes.
A failure of these adaptations in women with
renal disease creates a suboptimal environment
for fetal development and increases the risk of
obstetrics complications. Thus, the
understanding of these adaptations plays a major
role in obstetric care as they can appreciably alter
the criteria for diagnosis and treatment of renal
diseases during pregnancy.
Renal Adaptation to Pregnancy
Normally in pregnancy, the kidney length
increases from 1 to 1.5 cm, and kidney volume
increases by up to 30%. There is physiologic
dilatation of the urinary collecting system with
hydronephrosis in up to 80% of women, usually
more prominent on the right side more likely due
to mechanical compression of the ureters
between the gravid uterus and the linea
terminalis. Hydronephrosis of pregnancy is
usually asymptomatic, but abdominal pain, and
rarely obstruction, can occur.
Glomerular filtration increases by 40% to 65%
due to increase in renal blood flow and is
maintained until the middle of the third trimester.
The increase in glomerular filtration rate (GFR)
results in a physiologic decrease in circulating
creatinine, urea, and uric acid levels.
Assessment of Renal Function during Pregnancy
Average serum creatinine decreases from 0.8 mgi
dl to 0.5 to 0.6 mq/d! Hence, a serum creatinine
of 1.0 mq/dl reflects renal impairment in a
pregnant woman. Blood urea nitrogen (BUN)
decreases from an average of 13 mg/dl. Serum
uric acid reaches a nadir of 2.0 to 3.0 rnq/dl by
22 to 24 weeks. Thereafter, the uric acid level
begins to rise, reaching non-pregnant levels by
term which is due to increased renal tubular
absorption of urate. Pregnant women have
normal excretion of an exogenous solute load,
and appropriately conserve sodium when intake
is restricted. The serum sodium typically decreases
by 4 to 5 m mol/l below non-pregnancy levels.
The urinalysis is essentially unchanged during
pregnancy, except for occasional glucosuria.
These are due to increased filtration with less
efficient tubular reabsorption of glucose and
aminoacids. There are no significant differences
by trimester. Albumin constitutes only a small
part of total protein excretion and ranges from
5 to 30 mq/day. Airoldi and Weinstein (2007)
concluded that proteinuria exceeding 300 mg/
day should be considered abnormal.
Renal disorders in pregnancy:
Renal and urinary tract disorders commonly
encountered in pregnancy can be grouped as:
A) Complications unique to pregnancy-e.g.
Diabetes insipidus, Preeclampsia (Gestational
Hypertension).
II Vol. 14 November 2012

-------------------------------------------------------Pulse
B) Pregnancy-induced changes predisposing to. development or worsening of urinary tract
disorders-ego Markedly increased risk ofpyelonephritis.
C) Diseases preceding pregnancy-e.g.Neph rol ith iasis.
D) Renal diseases associated with systematicillness.
Diabetes Insipidus of Pregnancy
Circulating levels of vasopressinase, an enzymethat hydrolyzes arginine vasopressin, are
increased during normal pregnancy. Occasionally,this increase is so pronounced that circulatingantidiuretic hormone (arginine vasopressin)disappears, resulting in the polyuria and
polydipsia of diabetes insipidus presenting duringthe second trimester and disappearing after the
delivery. Affected women may becomedangerously hypernatremic, especially with
cesarean section using general anesthesia and/or water restriction in the delivery room. Thepolyuria can be controlled by the administration
of deamino-8-darginine vasopressin (desmopressin[DDAVPJ), which is not destroyed byvasopressmase.
Preeclampsia and Hemolysis, Elevated Liver
Enzymes, and Low Platelets (HELLP) Syndrome
Preeclampsia is a systemic syndrome specific topregnancy (incidence -3% to 5%), characterizedby the new onset of hypertension and proteinuriaafter 20 weeks of gestation. Several medicalconditions are associated with increasedpreeclampsia risk, including chronic
.hypertension. diabetes mellitus, renal disease,obesity. and antiphospholipid antibodysyndrome.
Renal Changes in Preeclampsia
The pathologic swelling of glomerular endothelialcells, glomerular endotheliosis and loss of the
capillary space is characteristic of preeclampsia
as shown in the figure below. There are deposits
of fibrinogen and fibrin within and under the
endothelial cells, and electron microscopy shows
loss of glomerular endothelial fenestrae. Recent
studies have shown that mild glomerular
endotheliosis also occurs in pregnancy without
preeclampsia, especially in gestational
hypertension. Both renal blood flow and GFR are
low in preeclampsia as compared with normal
pregnancy. Renal blood flow decreases as a result
of high renal vascular resistance. Although acute
renal failure can occur in preeclampsia, typically
proteinuria and renal sodium and water retention
are the only renal manifestations of disease.
Vascular endothelial changes in Pre-eclampsia
Preeclampsia: Diagnosis and Clinical Features
• Hypertension
For the diagnosis of preeclampsia, hypertension
is defined as a systolic blood pressure of 140 mm
Hg or higher or a diastolic blood pressure of 90
mm Hg or higher after 20 weeks of
gestation in a woman with previously normal
blood pressu reo Hypertension shou Id be
Vol. 14 November 2012 III

-------------------------------------------------------Pulse
confirmed by two separate measurements at least2 hours apart.
• Proteinuria
Diagnosis of preeclampsia requires greater than300 mg protein in a 24-hour urine collection.However, the degree of proteinuria is a poorpredictor of adverse maternal and fetaloutcomes, thus heavy proteinuria alone is notan indication for urgent delivery.
• Edema
It is also recognized to be a feature of normal
pregnancy, diminishing its usefulness as a specific
pathologic sign. Still, the sudden onset of severe
edema,especially edema of the hands andface,can be an important presenting symptom
of preeclampsia.
• Uric Acid
Serum uric acid is elevated in most women withpreeclampsia primarily as a result of enhanced
tubular urate reabsorption. Serum uric acid levels
are correlated with severity of preeclampsia and
with adverse pregnancy outcomes, even in
gestational hypertension without proteinuria.
Clinical Features of Severe Preeclampsia
Several clinical and laboratory findings suggestsevere or progressive disease and should promptconsideration of immediate delivery.
• Systolic blood pressure> 160 mm Hg ordiastolic blood pressure> 110 mm Hg on twooccasions at least 6 hr apart while on bedrest.
• Proteinuria >5 g in a 24-hr urine specimen or
• Dipstick proteinuria +2 or more on tworandom urine samples at least 4 hr apart.
• Oliguria « 500 ml urine output over 24 hr)
• Severe headache, mental status changes, orvisual disturbances
• Pulmonary edema or cyanosis
• Epigastric or right-upper quadrant pain
• Hepatocellular injury (transaminase elevationto at least twofold over normal levels)
• Thrombocytopenia « 100,000 plts/rnm")
• Fetal growth restriction
• Cerebrovascular accident
Eclampsia
It is preeclampsia associated with convulsion notattributed to other causes. Sometimes it canoccur without hypertension and proteinuria. Upto one-third of eclampsia occurs postpartum.Radiologic imaging by head computedtomography (CT)or magnetic resonance imaging(MRI) is usually not indicated when the diagnosisis apparent, but typically shows vasogenic edema,predominantly in the subcortical white matterof the parieto-occipital lobes. Eclampsia maycause subtle long-term impairment in cognitivefunction.
HELLP syndrome
Is an acronym for the syndrome of hemolyticanemia, elevated liver enzymes, and low platelets.It is a severe variant of preeclampsia, although itcan occur in the absence of proteinuria. It isassociated with increased maternal and neonataladverse outcomes including eclampsia (6%),placental abruption (10%), acute renal failure(5%), disseminated intravascular coagulation(8%). pulmonary edema (10%), and (rarely)hepatic hemorrhage and rupture.
Maternal and Neonatal Mortality
Maternal death is most often due to eclampsia,cerebral hemorrhage, renal failure, hepatic
Vol. 14 November 2012

------------------------------------------------------Pulse
failure, pulmonary edema, and HELLP syndrome.Worldwide, preeclampsia is associated with a
perinatal and neonatal mortality rate of 10%.Neonatal death is most commonly due toiatrogenic prematurity undertaken to preserve the
health of the mother. Fetal growth restriction asa result of impaired uteroplacental blood flow
or placental infarction. Oligohydramnios andplacental abruption are less common
complications.
Management and Treatment of Preeclampsia
• Timing of Delivery
In women presenting prior to 24 weeks of
gestation, maternal complications and perinataland neonatal mortality are extremely high
(>80%). For this reason, termination is usuallyrecommended. In addition, the presence of non-
reassuring fetal testing, suspected abruptionplacentae, thrombocytopenia, worsening liverand/or kidney function, and symptoms, such asunremitting headache, visual changes, nausea,
vomiting, or epigastric pain are generallyconsidered indications for expedient delivery. In
preeclampsia presenting between 24 and 34weeks of gestation without the above severe
signs and symptoms, postponing delivery mayimprove neonatal outcomes.
• Blood Pressure Management
Acutely, aggressive lowering of blood pressurecan lead to fetal distress or demise, especially ifplacental perfusion is already compromised.
Because of this, antihypertensive therapy forpreeclampsia is usually withheld unless the blood
pressure rises above 150 to 160 mm Hg systolicor 100 to 110 mm Hg diastolic, above which therisk of cerebral hemorrhage becomes significant.
Methyldopa a centrally acting cx2-adrenergicagonist has the most extensive safety data and
appears to have no adverse fetal effects. ~
Adrenergic antagonists are effective without
known teratogenicity or known adverse fetaleffects except atenolol, which has beenassociated with fetal growth restriction.
Labetalol, which result in better preservation ofuteroplacental blood flow because of its cx-
blocking action is used, both as an oral and anintravenous agent. Calcium channel blockers,nifedipine appear to be safe in pregnancy. When
hypertension in pregnancy is complicated by
pulmonary edema, diuretics are appropriate andeffective.Angiotensin converting enzyme ACEinhibitors and angiotensin receptor blockers are
contraindicated in the second and third trimesterof pregnancy, as they produce renal dysfunctionin the fetus, leading to renal dysgenesis, fetal
oliguria and oligohydramnios, pulmonaryhypoplasia, IUGR, and neonatal anuric acuterenal failure (ARF) ultimately leading to death of
the fetus.
• Intravenous Agents for Urgent Blood PressureControl
Severe hypertension in pregnancy occasionallyrequires inpatient management with intravenousagents. Intravenous labetalol is safe and effective.
Use of hydralazine is associated with an increasedrisk of maternal hypotension, maternal oliguria,
placental abruption, and low APGAR scores.
Hence, hydralazine should probably beconsidered second-line and its use limited whenpossible. Nitroprusside carries risk of fetal cyanide
poisoning if used for more than 4 hours and isgenerally avoided.
• Magnesium and Seizure Prophylaxis
Magnesium has been widely used for the
management and prevention of eclampsia.Magnesium sulfate slows neuromuscularconduction and depresses central nervous system
irritability. Women receiving magnesium shouldbe monitored carefully for signs of toxicity,
Vol. 14 November 2012 III

-------------------------------------------------------Pulse
including loss of deep tendon reflexes, flushing,somnolence, muscle weakness, and decreasedrespiratory rate. Such monitoring is especiallyimportant in women with impaired renal functionwho have impaired urinary magnesiumexcretion.
• Management of HELLP Syndrome
Among women in the 24- to 34-week gestationalwindow, whose clinical status appears relativelystable and with reassuring fetal status, expectantmanagement is often a viable alternative.
Gestational Hypertension
Gestational hypertension is defined as the newonset of hypertension without proteinuria after20 weeks of gestation, which resolvespostpartum. Gestational hypertension progressesto overt preeclampsia in approximately 10% to25% of cases. When gestational hypertension issevere, it carries similar risksfor adverse outcomesas preeclampsia.
Chronic Hypertension
History of hypertension prior to pregnancy or ablood pressure above 140/90 mm Hg prior to20 weeks of gestation is suggestive of chronichypertension. Pregnant women with chronichypertension have an increased risk ofpreeclampsia (21% to 25%), premature delivery(33% to 35%), IUGR (10% to 15%), placentalabruption (1% to 3%), and perinatal mortality(4.5%).
However, most adverse outcomes occur inwomen with severe hypertension (diastolic bloodpressure > 11 0 mm Hg) and those withpreexisting cardiovascular and renal disease. Inthe absence of underlying renal disease, the newonset of proteinuria (> 300 mq/day), usually with
worsening hypertension, is the most reliable signof superimposed preeclampsia.
Secondary Hypertension in Pregnancy
Causes of secondary hypertension in pregnancyare renal artery stenosis, primaryhyperaldosteronism, and pheochromocytoma,Renal artery stenosis should be suspected when -hypertension is severe and resistant to medicaltherapy. Hypertension and hyperkalemia fromprimary hyperaldosteronism might be expectedto improve during pregnancy, as progesteroneantagonizes the effect of aldosterone on the renaltubule. Although rare, pheochromocytoma canbe devastating when it first presents duringpregnancy. This syndrome occasionally isunmasked during labor and delivery, when fatalhypertensive crisis can be triggered by vaginaldelivery, uterine contractions, and anesthesia.Maternal and neonatal morbidity and mortalityare much better when the diagnosis is madeantepartum, with attentive and aggressivemedical management. Surgical intervention istypically postponed until after delivery wheneverpossible.
Approach to Management of ChronicHypertension in Pregnancy
Blood pressure control should be optimized priorto conception whenever possible, and womenshould be counselled regarding the risks ofadverse pregnancy outcomes, includingpreeclampsia. Once pregnant, changes inantihypertensive agents may be appropriate andwomen should be followed closely for signs ofsuperimposed preeclampsia.
Goals of Therapy
Medical treatment should be initiated in womenwith newly diagnosed chronic hypertension inpregnancy only if there is evidence of end-organ
III Vol. 14 November 2012

----------------------------------------------------Pulse
damage (proteinuria, cardiomyopathy) or the
blood pressure exceeds 150 to 160 mm Hgsystolic or 100 to 110 mm Hg diastolic.
Similarly, in women already receiving chronic
antihypertensive therapy prior to pregnancy,consideration could be given to tapering or
discontinuing treatment unless blood pressuresexceed these levels.
Acute Kidney Injury in Pregnancy
The most common cause of AKI during
pregnancy is prerenal azotemia due tohyperemesis gravidarum or vomiting from acutepyelonephritis. Occasionally preeclampsia, HELLP
syndrome, and acute fatty liver of pregnancy arecomplicated by acute renal failure. Obstetric
complications such as septic abortion andplacental abruption are associated with severeacute tubular necrosis and bilateral cortical
necrosis. Obstructive uropathy is a rare cause ofrenal failure in pregnancy.
The diagnosis of renal cortical necrosis can be
usually be established by CT scan, whichcharacteristically demonstrates hypodense areasin the renal cortex. The treatment of AKI in
pregnancy is supportive with prompt restorationof fluid volume deficits, and in later pregnancy,
expedient delivery. No specific therapy is effective
in acute cortical necrosis except for dialysis whenneeded. Both peritoneal and hemodialysis havebeen used during pregnancy, however peritonealdialysis carries the risk of impairing uteroplacentalblood flow. Patients with septicemia, mostly
respond to antibiotics and volume resuscitation."Survival is intimately linked with the managementand recovery of the AKI.
Obstructive Uropathy and Nephrolithiasis
If clinical suspicion is high (e.g., marked
hydronephrosis, abdominal pain, elevated serum
creatinine), a Percutaneous nephrostomy may beneeded as a diagnostic and therapeutic trial. If
present, obstruction can be managed withureteral stenting. Circulating levels of 1, 25-
dihydroxyvitamin D3 are increased during normal
pregnancy, resulting in increased intestinalcalcium absorption. Urinary excretion of calciumis also increased, leading to a tendency in somewomen to form kidney stones. Excessive intakeof calcium supplements can lead to
hypercalcemia and hypercalcuria. Calcium oxalate
and calcium phosphate constitute the majority
of the stones produced during pregnancy,presenting with flank pain and lower abdominalpain with hematuria. Premature labor and therisk of infection is increased. Ultrasonography is
the preferred method to visualize obstruction andstones. The management of renal calculi is
conservative with adequate hydration, analgesics
and antiemetics. Thiazide diuretics and
allopurinol are contraindicated. Nephrolithiasiscomplicated by urinary tract infection should be
treated with antibiotics for 3 to 5 weeks, followed
by suppressive treatment after delivery. Most
stones pass spontaneously, but ureteral
catheterization and placement of a ureteral stent
may be needed. Extracorporeal shockwave
lithotripsy has been used during the first 4 to 8
weeks of pregnancy without known adverse
consequences to the fetus.
Urinary Tract Infection and Acute Pyelonephritis
Physiologic hydronephrosis predisposes pregnant
women to ascending pyelonephritis in the setting
of cystitis.
Asymptomatic Bacteriuria is persistent, activelymultiplying bacteria within the urinary tract inasymptomatic women.
Incidence during pregnancy varies from 2 to 7percent. A clean-voided specimen containing
Vol. 14 November 2012 II

------------------------------------------------------Pulse
Antimicrobial Agents Used for Treatment of Pregnant Women with Asymptomatic Bacteriuria are asfollows:
Single-dose treatmentAmoxicillin 3 gAmpicillin 2 gCephalosporin 2 gNitrofurantoin 200 mgTrimethoprim-sulfamethoxazole 320/1600 mg
OtherNitrofurantoin 100 mg four times daily for10 daysNitrofurantoin 100 mg twice daily for 7 daysNitrofurantoin 100 mg at bedtime for 10 days
more than 105 bacteria/ml is diagnostic.Untreated asymptomatic bacteriuria inpregnancy is associated with an increased riskof premature delivery and low birth weight andcan progress to overt cystitis or acutepyelonephritis in up to 40% of patients. Acutepyelonephritis is a serious complication presentswith fevers, loin pain, and dysuria and canprogress to endotoxic shock, disseminatedintravascular coagulation, and acute renal failure.Thus, early detection and treatment ofasymptomatic bacteriuria is recommended. Urineculture is preferred for screening. Screening forasymptomatic bacteriuria is recommendedduring the first prenatal visit and is only repeatedin high-risk women, such as those with a historyof recurrent urinary infections or urinary tractanomalies. If asymptomatic bacteriuria is found,prompt treatment is warranted (usually with acephalosporin) for at least 3 to 7 days. A follow-up culture 2 weeks after treatment is necessaryto ensure eradication of bacteriuria. Suppressive
3-day courseAmoxicillin 500 mg three times dailyAmpicillin 250 mg four times dailyCephalosporin 250 mg four times dailyCiprofloxacin 250 mg twice daily ::Levofloxacin 250 mg dailyNitrofurantoin 50 to 100 mg four times daily;100 mg twice dailyTrimethoprim-sulfamethoxazole 160/800 mgtwo times daily
Treatment failuresNitrofurantoin 100 mg four times dailyfor 21 days
Suppression for bacterial persistence orrecurrenceNitrofurantoin 100 mg at bedtime forremainder of pregnancy
therapy with nitrofurantoin or cephalexin isrecommended for those patients with bacteriuriathat persists after two courses of therapy.Pyelonephritis is usually treated aggressively withhospitalization, intravenous antibiotics, andhydration.
Chronic Kidney Disease and Pregnancy
Women who enter pregnancy with chronic renaldisease are at increased risk for rapid decline ofrenal function and perinatal mortality due topreterm delivery and IUGR.
The physiologic increase in renal blood flow andGFR characteristic of normal pregnancy isattenuated in chronic renal insufficiency. Womenwith mild renal impairment (serum creatinine lessthan 1.4), normal blood pressure, and noproteinuria have good maternal and fetal
Vol. 14 November 2012

-------------------------------------------------------Pulse
outcomes, with Iittle risk for acceleratedprogression toward ESRD or preterm delivery.Initiating pregnancy with a serum creatininegreater than 2.0 rnq/dl carries a high risk foraccelerated decline in renal function both duringand after pregnancy. Among women with aserum creatinine greater than 2.5 rnq/dl, over70% experience preterm delivery, and over 40%experience preeclampsia and terminatingpregnancy does not reliably reverse the declinein renal function.
Renal diseases associated with systematic illness
1) Diabetic Nephropathy and Pregnancy
Pregnancy itself does not impact adversely onprogression of kidney disease, if kidney functionis normal or near normal at the onset. Womenwith diabetic nephropathy are strongly advisedto postpone pregnancy until after renaltransplantation, which improves fertility statusand fetal outcomes, and does not lead toimpaired renal function if allograft function isnormal. ACE inhibitors and angiotensin IIreceptor blockers are contraindicated duringpregnancy. It is known that in utero high sugarexposure in the offspring of diabetic mothersleads to impaired nephrogenesis and reducednephron mass, and this may put the offspring athigher risk for developing renal disease andhypertension in later life.
2) Lupus Nephritis and Pregnancy
With careful planning, monitoring, andmanagement, the majority of patients with SLE-especially those with normal baseline renalfunction-can complete pregnancy without
" serious maternal or fetal complications likepreeclampsia, preterm birth, IUGRand abortion.Women with lupus should postpone pregnancyuntil lupus activity is quiescent andimmunosuppressives are minimized. Prophylactictherapy with steroids does not appear to preventa lupus flare during pregnancy.
Pregnancy in chronic dialysisCurrent management recommendation inwomen on chronic dialysis with pregnancy -Increasing the weekly dialysis dose to 20 or morehours per week to improve neonatal outcomesand longer gestations. This is often attained bydaily nocturnal dialysis. Medications must becarefully reviewed.Erythropoeitin dosing shouldbe adjusted a dose increase of approximately50% to maintain hemoglobin target levels of 10to 11 q/dl.. Antihypertensive therapy should beadjusted for pregnancy to maintain maternaldiastolic pressure at 80 to 90 mm Hg by usingmethyldopa, labetolol, and sustained releasenifedipine. Close monitoring of fetal well-being,in collaboration with an obstetrician, is essentialafter 24 weeks of gestation as early fetal distressIS common.
Pregnancy in the Renal Transplant PatientLindheimer and colleagues (2008) and Hou(2003) recommend that women who haveundergone transplantation satisfy the followingrequisites before attempting pregnancy:
1. They should be in good general health for atleast 2 years after transplantation.
2. There should be stable renal function withoutsevere renal insufficiency-serum creatinine <2mq/dl, and preferably < 1.5 mq/dl., none tominimal proteinuria, no evidence of graftrejection, and absence of pyelocalyceal distensionby urography.
3. Absent or easily controlled hypertension.
4. Drug therapy reduced to maintenance levels.
Vaginal delivery is safe, and cesarean sectionshould be performed only for obstetricalind ications.
Effect of Pregnancy on Renal Allograft Function
Pregnancy itself does not appear to adverselyaffect graft function in transplant recipients,provided baseline graft function is normal andsignificant hypertension is not present.
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
In general, when pregnancy occurs 1 to 2 yearsafter transplant, the rejection rate is similar tothat seen in nonpregnant controls (3% to 4%).
When moderate renal insufficiency is present(serum creatinine >1.5 to 1.7 mq/dl). there is arisk of progressive renal dysfunction,small forgestational age infant and of preeclampsia.
There is increased risk for infections withcytomegalovirus, herpes simplex, andtoxoplasmosis. The rate of bacterial urinary tractinfections is increased (13% to 40%).
Hypertension affects between 30% and 75% ofpregnancies among transplant recipients with riskof Preeclampsia in 25% to 30% .Renal transplantrecipients should be managed aggressively, withtarget blood pressure close to normal-a goal thatdiffers from somewhat higher blood pressuregoals in women with hypertension in pregnancyin the absence of a transplant. Agents of choiceinclude methyldopa, nonselective ~-adrenergicantagonists (i.e. labetalol). and calcium channelblockers.
Cyclosporine (or tacrolimus) and steroids, withor without azathioprine, form the basis ofimmunosuppression during pregnancy.Corticosteroids at low to moderate doses (5 to10 mg/day) are safe. Close monitoring of blood
levels with dosing adjustment are required toavoid risk of acute rejection.
Breast feeding is not recommended In womenon immunosuppressive drugs.
Management of Acute Rejection in Pregnancy
Acute rejection should be suspected if fever",oliguria, graft tenderness, or deterioration inrenal function is noted.
Biopsy of the renal graft should be performed toconfirm the diagnosis.
High-dose steroids remain a mainstay oftreatment of acute rejection during pregnancy,with the risk of fetal malformations and maternalinfections.
Pregnancy Outcome following Kidney Donation
Recent data suggests that these women have alower incidence of full-term deliveries and higherrisk for fetal loss, gestational diabetes, gestationalhypertension, and preeclampsia duringpregnancy.
References
1. Obstetrics & Gynecology Clinics of NorthAmerica, Vol: 37 (2010)
2. Williams Obstetrics, 23rd Edition.3. Practical Guide to High-Risk Pregnancy and
Delivery- Fernando Arias, 3rd Edition.
II Vol. 14 November 2012

----------------------------~-------------------------Pulse
Renal Cell Carcinoma ImagingDr. Amitkumar Choudhari, DNB Student
Dr. Ajay Chaubey, Dr. Surita Kantharia, Medical OfficersDepartment of Radio diagnosis, BARCHospital
Abstract:
Objectives: Review the role of imaging in renal
cell carcinoma with special focus on contrast
enhanced ultrasound imaging.
Methods: The techniques used in evaluation of
renal tumors like urography, ultrasonography, CT
and MRI are discussed.
Result: Cross sectional imaging has heightened
sensitivity of detecting renal masses which may
not be clinically apparent. Imaging also helps in
characterizing and staging renal masses. On
contrast ultrasonography, early and dense
persistent enhancement of the lesion compared
to rest of the renal parenchyma helps making a
confident diagnosis of neoplasm, especially in
patients with renal failure and hypersensitivity
to iodinated contrast media, where iodinated
contrast media are contraindicated and without
exposure to radiation.
Conclusion: Imaging has a major role in
detecting and staging renal tumours, especially,
incidental renal masses.
Introduction
-." Renal cell carcinoma also known as
hypernephroma or Grawitz's tumor,
pathologically adenocarcinoma is the most
common primary renal malignancy in adults. It
accounts for 85% of all malignant renal tumors
and about 3% of all diagnosed neoplasms (1).
It is more common in men and is usually in 5thto
7th decades. Most are sporadic; some may be
associated with syndromes like von HippelLindau
(vHL). Risk factors include smoking, exposure to
petroleum and asbestos.
The classic clinical presentation of flank pain,
hematuria, and a palpable flank mass is
comparatively uncommon (5-10% of cases).
However, clinical symptomatology may be quite
nonspecific-for example, anorexia, tiredness,
weight loss, or fever of unknown origin(2). Other
presentations include varicocele formation (from
tumor thrombus in the left renal vein or the
inferior vena cava [IVC]) and disseminated
malignancy. RCCmay also present with a variety
of paraneoplastic syndromes, such as
polycythemia secondary to excessivesecretion of
erythropoietin, hypercalcemia secondary to
factors regulating calcium, and hepatic
dysfunction (Stauffer syndrome). Distant
metastases may cause symptoms of cough,
hemoptysis, bone pain, seizures, etc. Incidentally
detected tumors in asymptomatic individuals have
been steadily increasing with the dissemination
of imaging techniques, including CT, MR, and
sonography, accounting for approximately 60%
of renal tumors in the 1990s, compared with
approximately 10% in the early 1970s (3,4).
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
Staging Renal Cell Carcinoma (5) TNM Staging System for the KidneyRobson's Staging System for Renal CellCarcinoma Primary tumor (T)
Robson Disease extentStage
I Tumor confined within the renalcapsule
II Tumor spread to perinephric fat oripsilateral adrenal gland
IliA Venous tumor thrombus (renal veinor IVC)
IIIB Regional lymph node metastases
IIIC Venous tumor thrombus andregional lymphadenopathy
IV Direct invasion of adjacent organsoutside Gerota's fascia
IVB Distant metastases
Regional lymph nodes (N)
Stage Definition
Nx Regional lymph nodes cannot beassessed
NO No regional lymph node metastasis
N1 Metastasis in regional lymph node(s)
Distant metastasis (M)
Stage Definition
MO No metastasis
M1 Distant metastases
Stage Grouping
Stage' T1, NO, MO
Stage 1/ T2, NO, MO
Stage 1/, T1 orT2, N1, MO
13, NOor N1, MO
Stage 'V T4, any N, MO
Any T, any N, M1
Stage Definition
TX Primary tumor cannot be assessed
TO No evidence of primary tumor
T1 Tumor 7cm or lessin greatest dimension,limited to the kidney
T1a Tumor 4cm or lessin greatest dimension,limited to the kidney
T1b Tumor more than 4cm but not morethan 7cm in greatest dimension limitedto the kidney
T2 Tumor more than 7cm in greatestdimension, limited to the kidney
T2a Tumor more than 7cm but less than orequal to 10cm in greatest dimension,limited to the kidney
T2b Tumor more than 10cm, limited to thekidney
13 Tumor extends into major veins orperinephric tissues but not into theipsilateral adrenal gland and not beyondGerota's fascia
Ba Tumor grossly extends into the renal veinor its segmental (muscle containing)branches, or tumor invades perirenaland/or renal sinus fat but not beyondGerota's fascia
Bb Tumor grossly extends into the vena cavabelow the diaphragm
Bc Tumor grossly extends into the vena cavaabove the diaphragm or invades the wallof the vena cava
T4 Tumor invades beyond Gerota's fascia(including contiguous extension into theipsilateral adrenal gland)
II Vol. 14 November 2012

-------------------------------------------------------Pulse
Radiological Evaluation
Urography
Urography has been used for many years todiagnose renal tumors. Its sensitivity was 80-85%for masses over 3 cm insize and only 10% for
lesions under 3 cm. After the development ofcross sectional imaging techniques its role indetection and work up of solid renalmasses has
decreased and has been replaced mainly bysonography and Uro-CT. Actually it is no
moreproposed in the detection andcharacterization ofmass-like lesions.
Ultrasound
Gray scale sonography
The echostructure or the echogenicity of therenalcarcinoma is correlated to Size,
vascularization, modality of growth (radial orinfiltrative), presenceof cystic or necrotic areas.The echographicpatternis finally connected to the
echogenicity of thesurrounding parenchyma thatcan be increased orsometimes reduced (6).
The tu mor may a ppea r hyperechoic,isoechoic,hypoechoic or of mixed echostructure.Hypoechogenicity is the most frequent
patternand generally it is related to thehypervascularityor to the internal coagulative
necrosis. Hypoechogenicity is observed inpresence of necrotic orhemorrhagic internalareas which are very frequentin major lesions.Anechoic or cystic-like tumors arerare and they
can be related to neoplastic transformation of abenign cyst or to acystocarcinoma. Intratumoral6'r marginal calsifications are observedin about
5-10% of RCC and they appear as spots or focalareas of hypereflectivity associated with posteriorshadowing. Pure isoechoictumours are rare and
they are detected only because they produce abulging of the renal profile or out grow into the
renal sinus. When the carcinoma is largeusually it
appears as an inhomogeneous mass withcomplex mixed echostructure associated todeformation and dislocation of the kidney.
At ultrasonography the differential diagnosisof the renal carcinoma has to be made with somebenign tumors and with so called pseudotumors
or normal variants of the renal anatomy.
The most common benign tumor is
angiomyolipoma (AML) which characteristicallyappears as ahyperechoicmass well distinct from
the adjacent normal parenchyma and withoutanyhypoechoic rim (7,8). In 40% of cases adistantshadowing can be present, which hasnever been observed in hyperechoic appearing
carcinomas. This hyperechogenicity is mainlyrelated to the fatty component of the tumor even
if there are AML with limited adipose tissue butstill hyperechoic. Any renal hyperechoic mass is
very suspicious of AM L, but Iiteratu re data have
shown that hyperechogenicity can be observed
in 30% of carcinomas, especially in small lesions.
For this reason the US diagnosis of AML has to
be confirmed by CT or MR onthe base of
intralesional fat detection.
Oncocytoma, the second most common benign
tumor, cannot be differentiated from the
carcinomaon the basis of ultrasonography.
Insomecasesa central scar can be demonstrated,
but this finding can be observed also in some
malignantlesions (7,9).
Color and Power Doppler
The role of Color- and Power-Doppler in the
detection of renal carcinomas is still under
discussion and the diagnostic gain obtained with
these two modalitiesis limited. The increase of
both diagnosticsensitivity and operator diagnostic
confidence islimited.
Vol. 14 November 2012

----------------------------------------------------Pulse
Doppler flow patterns seen In various renalmasses has been classified by Jinzakiet al.(1 O)asfollows:
Pattern 0: no vascularization
Pattern 1: small and sparse intratumoralcolordots
Pattern 2: penetrati ng pattern with vesselsentering into the mass
Pattern 3: numerous and evidentperipheralvessels (peripheral pattern)
Pattern 4: mixed peripheral andpenetrati ngpattern
Pattern 4 is the most common in the RCC,but itspecific because it can be present also in AMLand on cocytomas. Masses with sparse spotspattern or only peripheral vascularization aremore frequently benign. These Color-Dopplercriteria are inadequate to differentiate a benignfrom a malignant lesion in the clinical practice,but they may only suggest a possible nature ofthe lesion that requires a pathologic confirmation(11). There are few reports regarding the increasein accuracy in the detection of renal tumors usingColor and Power-Doppler imaging associated togray-scale sonography.
On the other side Color and Power-Dopplertechnology is very useful in the characterizationof pseudotumoral aspects, which are verycommon in the kidneys (column of Bertin; adromedary or splenic hump; fetal lobulation; focalareas of hypertrophy). These apparent lessionsshow a normal vascular distribution of the arteriesand veinsthat resembles that of the normalparenchyma.
Contrast Enhanced Ultrasonography
Investigations have shown that contrast-enhanced ultrasound (CEU) may have utility forevaluation of renal masses (12-17). Second-
generation ultrasound microbubble contrastagents are composed of gas-filled lipidmicrospheres measuring approximately 3-51min diameter that are injected IV. When exposedto low-energy ultrasound, the microspheresresonate and produce an acoustic signal thatallows dynamic real-time visualization of tumorvasculature and enhancement characteristics(18).-Ultrasound contrast medium has potentialadvantages over CT and M RI contrast agents inthat CEU agents remain intravascular withoutdiffusing into the interstitial space, allowvisualization of microvasculature, allow highertemporal resolution of ultrasound than of CT orMRI, and carry no known risk of nephrotoxicityor nephrogenic systemic fibrosis in patients withrenal dysfunction(17). The typical contrast agentused in our institute is SonoVue (BraccoSpA,Milan, Italy), which is composed of sulfurhexafluoride gas with a phospholipid shell. Themicrobubbles are metabolized by the liver (shellcomponent) and the gas is exhaled via the lungs.
Imaging Technique
We use the preset contrast mode on ou rmultipurpose ultrasound machine (iU22, PhilipsMedical Systems, Bothell, WA, USA) and acurvilinear transducer operating in the frequencyrange of 2 - 5 MHz which produces images onthe basis of maintenance of microbubbles at lowacoustic pressure.
A 0.5 ml bolus of SonoVue is injected rapidlyfollowed by a 10 ml saline flush. Continuoustimed scanning is started immediately afterflushing with saline. Continuous repeated cineloops are acquired simultaneously over a spanof about 2 minutes after which no contrast signalwas appreciable. Split screen loops are obtainedwhich simultaneously show separate lowmechanical index gray-scale and contrast-onlyimages. A very low acousticpressure (0.05 to 0.09
II Vol. 14 November 2012

-------------------------------------------------------Pulse
Fig.1: Split screen image prior to early arterial phase showing the interpolar renal mass(outlined in red) and the rest of the kidney (contoured in blue) on gray-scale image
Fig.2: Split screen image showing marked enhancement of the renal mass (arrowheads)compared to renal cortex (arrows) on contrast (left) image.
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
Fig.3: Persistently dense contrast enhancement of the mass with a small nonenhancing area (arrow) within representing necrosis.
Fig.4: Split screen image showing the intrahepatic IVC (outlined in red) on gray scale (Right)showing dense intraluminal echogenic thrombus which is avidly enhancing, as visualized on
contrast image (Left), representing tumor thrombosis. L: Liver
II Vol. 14 November 2012

On early phase scanning, the kidney becomeshyperechoic in comparison with the liver (rightside) or the spleen (left side). Later on, the kidneybecomes rapidly hypoechoic if compared withthe adjacent parenchyma and especially with thespleen, which shows a very dense and persistentenhancement. The renal-enhancing effectdecreases as the general contrast concentrationdecreases(19). Unlike iodinated contrast media,CEUS microbubbles are blood pool agents andthere is no pyelographic phase. (Fig.1-3).
------------------------------------------------------Pulse
mechanical index, determining a 40- to 50-mPaderated pressure) is used, with the sound beamfocused at the deeper aspect of the region ofinterest.
Normal Renal Enhancement Pattern onCEUS
The kidney enhances quickly and intensely afterSonoVue bolus injection due to the high renalblood ow. Following enhancement patterns areappreciated:
I. Early arterial phase: Enhancement in thecentral arteries becomes apparent 10 to 15s after contrast injection.
ii. Late arterial or cortical phase: Fewseconds later by enhancement of the renalcortex, whereas pyramids remain echo poor.
iii. Medullary phase: Pyramids gradually fillwith contrast until they are isoechoic withthe cortex.
Pseudotumors
CEUScan be helpful in clarifying some potentialdoubts and sources of misinterpretation ofconventional US. A prominent Bertin column, apersistent fetal lobulation, or a dromedary humpcan be sometimes misdiagnosed as a renal mass.CEUS can be used to assess renal vascularity,cortical thickness, and pyramid spacing. On CEUS
Fig.S: Contrast-enhanced ultrasonographic images in the diagonsis of renal pseudo-tumors
Vol. 14 November 2012 11

-------------------------------------------------------Pulse
Fig.6: Contrast-enhanced ultrasonographic images in the diagnosis of renal pseudo-tumors
Fig.7: Right renal lower polar well defined rounded mass (contoured in figure 6) in acase of chronic renal failure which is isoechoic to the cortex on all phases, consistent
with pseudotumor.
II Vol. 14 November 2012

-------------------------------------------------------Pulse
these pseudo-lesions exactly follow the normal'enhancement pattern of the renal cortex or thepyramid and can thus be differentiated from atrue renal mJSSlesion (20). (Figs.5,6&7).
Solid Renal Tumors
CEUS has a role in differentiating solid renalmasses into benign and malignant. The tumorechogenicity on grey scale, enhancement
Table 1: Bosniak classification of complexrenal cysts adapted to CEUS (26)
Type Description
I Simple cyst. Benign, with no malignantpotential. No further workup.
II Few thin septations or small amount ofperipheral calcification. Weak chance ofmalignancy. Evaluate cyst enhancementwith CEUS. If no enhancement, nofurther follow-up is needed. Ifsubstantial enhancement is observed,assesswith CT. Even if CT is negativefor enhancement, consider US follow-up.
III Many thin septations, several thickseptations, or a small mural nodule.Intermediate chance of malignancy.Evaluate cystenhancement with CEUS.If no enhancement is seen, assesswithCT and follow with US. If substantialEnhancement isseen, consider surgery.Follow-up is mandatory if surgery is notperformed.
IV Many thick septations, large mural" nodule, or mural nodularity. Strong
chance of malignancy. Evaluate withCEUS. If no sonographic enhancementis seen, assesswith CT and follow withUS. If substantial enhancement isseen,consider surgery.
patterns, and degree of enhancement at differentphases are used to differentiate benign andmalignant solid renal mass lesions. CEUSfeaturesof early washout, heterogeneous enhancement,and an enhanced peritumoral rim orpseudocapsulefavor the diagnosis of RCC (21-23). CEUS can also be used to differentiatebetween tumour and bland IVCthrombus relatedto renal cell carcinoma (FigA).
Cystic masses
There is over all 39% and more than 50%incidence of renal cyst in patients older than 50years of age (24). Most of these cysts areincidentally detected.Complex cysts are currentlyclassied according to Bosniak (25). Bosniakclassification suggests malignant potential of acystic mass. This categorization has been basedon CT findings (25) but can be efficaciouslyextrapolated andapplied to CEUS(26) (Table 1).Surgery is recommended for IV and III categories,category II and I are benign.
Computed Tomography
MDCT protocol(27)
In general, 100-150 mL of iodinated IV contrastmedium is used at a flow rate of 2-3 ml./s.Unenhanced images of the liver and kidneys areobtained with 5-mm collimation in 5-mmincrements. Unenhanced images of the kidneysallow detection of calcification or fat in the kidney,enable assessmentof contrast enhancement, andassist in characterizing the lesion. IV contrast-enhanced images targeted on the kidneys areobtained in the arterial, late arterial(corticomedullary and portal venous),nephrographic, and excretory phases at 15-30,45-60, 80-180, and 180 seconds, respectively,after commencement of the IV infusion. Imagingof the liver and the remaining abdominalstructures is performed in the portal venousphase.
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
Unenhanced CT(28)
An initial seriesof unenhanced scansthrough thekidneys should be part of every protocol forevaluation of a suspected renal mass; it providesa baseline from which to measure theenhancement within the lesion after theadministration of intravenous contrast material.This enhancement characteristic is important indistinguishing hyperdense cysts from solidtumors. Because most renal cell carcinomas havea rich vascular supply, they enhance significantlyafter administration of contrast material.Enhancement values of more than 12 HU areconsidered suspicious for malignancy(29).
Most renal cell carcinomas are solid lesions withattenuation values of 20 HU or greater atunenhanced CT (29). Small «3-cm-diameter)tumors usually have a homogeneous appearance,while larger lesions tend to be moreheterogeneous owi ng to haemorrhage ornecrosis. Calcifications are detected in up to 30%of cases of renal cell carcinoma.
Arteriographic Phase(7)The arteriographic phase is performed to evaluatethe arterial anatomy and it occurs 15-30 s afterthe contrast injection. It is characterized by theclear visualization of the large and small vesselssimilar tothose obtained with arteriography. It isparticularly useful in those cases in which aconservativesurgery is planning, because it clearlyshows theanatomic distribution of the renalvesselsand theirrelationship with the neoplasm.
Corticomedullary Phase(7,28)
In the cortico-medullary phase thecontrastmedium is in the glomeruli and in theperitubularcapillaries, but it has not arrived inthe distal tubularlumina and in the interstitium.
An intense corticalenhancement is observed,while the medullaremains hypodense. RCCarecommonly hypodense compared to the cortexand cannot berecognized when they are small.Maximalopacification of the renal veins allowsconfidentdiagnosis of venous extension of thetumor whichcannot be visible in the prosecutionof the study. Insmall hypervascular tumours wit'h -arterio-venousfistulas an early enhancement canbe occasionally observed.
Nephrographic Phase
As contrast material filters through the glomeruliinto the loops of Henle and the collecting tubules,the nephrographic phase of contrastenhancement begins (30). This phase is bestimaged after a scanning delay of at least 80seconds and lasts up to 180 seconds after thestart of injection. In this phase the renal tumorsshow a relatively less contrast enhancementcompared tothe normal adjacent tissue. RCChave a richvascular supply, but lower than normalkidney and acontrast enhancement value of morethan 20 HU with respect to the non-contrast scanis consideredsuspicious for malignancy. When theenhancementis between 10 and 20 HU thediagnostic confidence islower because thesevalues can be observed incomplicated cysts or incystic carcinomas(31).
Excretory Phase
The excretory phase begins approximately 180seconds after the initiation of injection ofiodinated contrast material. The contrast materialis excreted into the collecting system, and as aresult, the attenuation of the nephrogramprog ressively decreases(28). (Fig.8&9).
This phase is occasionally helpful to betterdelineate the relationship of a centrally locatedmass with the collecting system and definepotential involvement of the calices and renal
II Vol. 14 November 2012

-------------------------------------------------------Pulse
pelvis.These data are actually very importantwhen a conservative surgery is pianned. Delayedscanning can also be used in lieu of unenhancedscanning to characterize an incidental renal lesiondetected on a routine contrast-enhanced CTscan(28).
Multiplanar reformatted and 3D volumerendered presentations of the renal phase imagesare helpful in allowing visualization of therelationships of structures, particularly forsurgeons(28,32,33).
MRI Evaluation
MRI is generally only used when optimal CTcannot be performed, as in the case of a severeallergy to iodinated contrast medium orpregnancy. MRI has similar reported overallstaging accuracies to those of CT (34). Itsmultiplanar capability, however, is particularlyuseful for delineating the superior extent oftumor in the IVC(2,35,36).
Coronal and axial conventional T1-weighted (TR/TE, 600/60) and axial dual-echo fast spin-echoT2-weighted (6,000/first -echo TE, 136; second-echo TE, 68) fat-suppressed images of the
Fig.8: Nephrographic phase shows a welldefined rounded heterogenously enhancing
right renal mass (arrowheads).
abdomen are obtained(27). Imagessupplemented by dynamic contrast-enhanced 3Dfast spoiled gradient-recalled echo sequences(FSPGR)help to further delineate the primarytumor and liver lesions and to evaluate anyvascular thrombus identified. In particular, tumor,rather than bland, thrombus is indicated by the
Fig.9b
Axial (Fig.9a) and coronal reformat (Fig. 9b)arterial phase images show abnormallydilated IVC (contoured) with intraluminalthrombus extending from the right renal veinupto the right atrium which showsintramural vascularity (arrowheads),suggestive of tumor thrombus. Same caseas In fig.1 ,2,3,4.
Vol. 14 November 2012

---------------------------------------------------Pulse
presence of enhancing vessels in the
thrombus(27). Multiple dynamic acquisitions canbe used to obtain arterial, nephrogenic, andpyelographiclike images (37-40). MDCT with 3D
reformations and MRI have similar overall stagingaccuracies for RCC(41).
Conclusion
Various imaging modalities can be used forevaluation of renal masses. Ultrasonography isthe primary modality where an incidental renalmass may come to attention. CT and MRI are
the current modalities of choice for preoperativestaging of renal masses. Newer imaging
techniques like contrast enhanced ultrasoundexamination offer an advantage of evaluatingrenal masses, especially, in cases of renal failure
where CT and M R contrast med ia arecontraindicated.
References:
1. Jemal A, Siegel R, Xu J, Ward E. Cancerstatistics, 2010. CA: a cancer journal forclinicians [Internet]. [cited 2011 Jul 20];60(5):277-300. Available from: http://wwwncbi.nlm.nih.gov/pubmed/20610543
2. Choyke PL, Amis ES, Bigongiari LR, BluthEI, Bush WH, Fritzsche P, et. al. Renal cellcarcinoma staging. American College ofRadiology. ACR Appropriateness Criteria.Radiology [Internet]. 2000 Jun 1 [cited 2012Feb 24];215 Suppl:721-5. Available from:http:// u k p m c . a c . u k/ a b st r act/ M ED/11037491
3. Luciani LG, Cestari R, Tallarigo C. Incidentalrena I cell ca rci noma-age a nd stagecharacterization and clinical implications:study of 1092 patients (1982-1997). Urology[Internet]. 2000 Jul [cited 2012 Feb24];56(1 ):58-62. Available from: http://wwwncbi.nlm.nih.gov/pubmed/1 0869624
4. Jayson M, Sanders H. Increased incidenceof serendipitously discovered renal cell
carcinoma. Urology [Internet]. 1998 Feb[cited 2012 Feb 24];51 (2):203-5. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/9495698
5. Vikram R, Casalino DD, Remer EM, ArellanoRS, Bsh 0ff JT, Dig heM, eta I. A CRa ppropriateness criteria: rena I cellcarcinoma staging. Radiology [Internet)": ..·-2011 [cited 2012 Feb 24];Available from:http://ra d i0 logy. rs na. 0 rg/co ntent/6/2/122.short
6. Forman HP, Middleton WD, Melson GL,McClennan BL. Hyperechoic renal cellcarcinomas: increase in detection at US.Radiology [Internet]. 1993 Aug [cited 2012Feb 24]; 188(2):431-4. Availa ble from:http://www.ncbi.nlm.nih.gov/pubmed/8327692
7. Pavlica P, Derchi L, Martorana G. Renal cellcarcinoma imaging. European Urology[Internet]. 2006 [cited 2012 Feb 25];5:580-92. Available from: http://www.sciencedirect. com/science/a rticle/pi i/S 1569905606001291
8. POZZI MUCELLI R, LOCATELLI M.Diagnostica per imrnaqini dell'angiomiolipoma renale: Quadri tipici eatipici. Radiologia medica [Internet]. [cited2012 Feb 25]; 103(5-6):474-87. Availablefrom: http://cat.inist.fr/7 aModele=afficheN&cpsidt= 13896467
9. De Carli P,Vidiri A, Lamanna L, Cantiani R.Renal oncocytoma: image diagnostics andtherapeutic aspects. Journal ofexperimental & clinical cancer research/: CR[Internet]. 2000 Sep [cited 2012 Feb25]; 19(3):287-90. Available from: http://wwwncbi.nlm.nih.gov/pubmed/11144520
10. Jinzaki M, Ohkuma K, Tanimoto A, MukaiM, Hiramatsu K, Murai M, et al. Small solidrenal lesions: usefulness of power DopplerUS. Radiology [Internet]. 1998 Nov [cited2012 Feb 25];209(2):543-50. Available
II Vol. 14 November 2012

---------------------------------------------------Pulse
from: http://www.ncbi.nlm.nih.gov/pubmed/9807587
11. Wunderlich H, Hindermann W, AI MustafaAM, Reichelt 0, Junker K, Schubert J. Theaccuracy of 250 fine needle biopsies ofrenal tumors. The Journal of urology[Internet]. 2005 Jul [cited 2012 Feb25];174(1):44-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15947574
12. Tamai H, Takiguchi Y, Oka M, Shingaki N,Enomoto S, Shiraki T, et al. Contrast-Enhanced Ultrasonography in the Diagnosisof Solid Renal Tumors. Ultrasound.2005;: 1635-40.
13. Roy C, Gengler L, Sauer B, Lang H. [Role ofcontrast enhanced US in the evaluation ofrenal tumors]. Journal de radiologie. 2008Nov;89(11 Pt 1):1735-44.
14. Wilson SR, Burns PN. Microbubble-enhanced US in Body Imaging: What Role?Radiology. 2010;257(1 ):24.
15. Jiang J, Chen Y, Zhou Y, Zhang H. Clear cellrenal cell carcinoma: contrast-enhancedultrasound features relation to tumor size.European journal of radiology. 2010Jan;73(1):162-7.
16. Fan L, Lianfang D, Jinfang X, Yijin S, YingW. Diag nostic efficacy of contrast-enhanced ultrasonography in solid renalparenchymal lesions with maximumdiameters of 5 cm. Journal of ultrasoundIn medicine!: official journal of theAmerica n Institute of U Itrasou nd InMedicine. 2008 Jun;27(6):875-85.
17. Gerst S, Hann LE, Li D, Gonen M, Tickoo S,Sohn MJ, et al. Evaluation of renal masseswith contrast-enhanced ultrasound: initialexperience. AJ R. American journal ofroentgenology [Internet]. 2011 Oct [cited2011 Oct 13]; 197(4):897-906. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/21940577
18. Hernot S. Microbubbles in ultrasound-triggered drug and gene delivery. Advanceddrug delivery reviews [Internet]. 2008 [cited2012 Feb 25];60(10): 1153-66. Availablefrom: http://www.sciencedirect.com/science/a rticie/pii/sO 169-409x(08)00081-1
19. Nilsson A. Contrast-enhanced ultrasoundof the kidneys. European Radiology. 2004Oct; 14(S8): P104-9.
20. Mazziotti S, Zimbaro F, Pandolfo A,Racchiusa S, Settineri N, Ascenti G.Usefulness of contrast-enhancedultrasonography in the diagnosis of renalpseudotumors. Abdominal Imaging[Internet]. 2010 Apr [cited 2012 Feb26];35(2):241-5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19194642
21. Real-time DDW, Ultrasonography C-enhanced. Renal Cell Carcinoma and RenalAngiomyolipoma. Ultrasound. 2010;:709-17.
22. Ascenti G, Gaeta M, Magno C, MazziottiS, Blandino A, Melloni D, et al. Contrast-Enhanced Second-Harmonic Sonography inthe Detection of Pseudocapsule in Renal CellCarcinoma. Am. J. Roentgenol. [Internet].2004 Jun 1 [cited 2012 Feb 26]; 182(6):1525-30. Available from: http://www.aj ronli ne.org/cgi/content/a bstract/182/6/1525
23. Xiao-qiu D, Yi S, Li-wei XU, Chun-mei XU,Wei BI, Xiao-min W, et al. Contrast-enhanced ultrasound for detection anddiagnosis of renal clear cell carcinoma.2009; 122(2007): 1179-83.
24. Reis M, Faria V, Lindoro J, Adolfo A. Thesmall cystic and noncystic noninflammatoryrenal nodules: a postmortem study. TheJournal of urology [Internet]. 1988 Oct[cited 2012 Feb 26];140(4):721-4.Available from: http://www.ncbi.nlm.nih.gov/pubmed/3418790
Vol. 14 November 2012

-------------------------------------------------------Pulse
25. Bosniak MA. The use of the Bosniakclassification system for renal cysts andcystic tumors. The Journal of urology[Internet]. 1997 May [cited 2012 Jan6];157(5):1852-3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9112545
26. Robbin ML, Lockhart ME, Barr RG. Renalimaging with ultrasound contrast: currentstatus. Radiologic clinics of North America[Internet]. 2003 Sep [cited 2012 Feb26];41 (5):963-78. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14521204
27. Ng CS, Wood CG, Silverman PM, TannirNM, Tamboli P, Sandler CM. Renal cellcarcinoma: diagnosis, staging, andsurveillance. AJR. American journal ofroentgenology [Internet]. 2008 Oct [cited2011 Aug 25];191(4):1220-32. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/l 88061 69
28. Sheth S, Scatarige JC, Horton KM, Corl FM,Fishman EK. Current concepts in thediagnosis and management of renal cellcarcinoma: role of multidetector ct andthree-dimensional CT. Radiographics/: areview publication of the RadiologicalSociety of North America, Inc [Internet].2001 Oct 1 [cited 2012 Feb 25];21 SpecNo(suppl1 ):S237-54. Available from: http:/Ira d iog ra phi cs. rsna. 0 rg/co ntent/2 1/suppl_1/S237.full
29. Silverman SG, LeeBY,Seltzer SE,Bloom DA,Corless CL,Adams DF.Small « or = 3 cm)renal masses: correlation of spiral CTfeatures and pathologic findings. AJR.American journal of roentgenology[Internet]. 1994 Sep [cited 2012 Feb25];163(3):597-605. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8079852
30. Saunders HS, Dyer RB,Shifrin RY,ScharlingES, Bechtold RE, Zagoria RJ. The CTnephrogram: implications for evaluation ofurinary tract disease. Radiographics/: a
review publication ofthe Radiological Societyof North America, Inc [Internet]. 1995 Sep[cited 2012 Feb 25];15(5):1069-85;discussion 1086-8. Available from: http://www.ncbi.nlm.nih.gov/pubmed!7501851
31. Ruppert-Kohlmayr AJ, Uggowitzer M,Meissnitzer T, Ruppert G. Differentiation ofrenal clear cell carcinoma and renal, -papillary carcinoma using quantitative CTenhancement parameters. AJR. Americanjournal of roentgenology [Internet]. 2004Nov [cited 2012 Feb 25];183(5):1387-91.Available from: http://www.ncbi.nlm.nih.gov/pubmed/15505308
32. Urban BA, Ratner LE, Fishman EK. Three-dimensional volume - rendered CTangiography of the renal arteries and veins:normal anatomy, variants, and clinicalapplications. Radiographics/: a reviewpublication of the Radiological Society ofNorth America, Inc [Internet]. 2001 Jan 1[cited 2011 Dec 8];21(2):373-86;questionnaire 549-55. Available from:http://radiographics.rsna.org/content/21/2/373.full
33. Wu nderlich H, Reichelt 0, Schubert R,Zermann DH, Schubert J. Preoperativesimulation of partial nephrectomy withthree-dimensional computed tomography.BJU international [Internet]. 2000 Nov[cited 2012 Feb 25];86(7):777-81.Available from: http://www.ncbi.nlm.nih.gov/pubmed/11069400
34. Beer AJ, Dobritz M, Zantl N, Weirich G,Stollfuss J, Rummeny EJ.Comparison of 16-MDCT and MRI for characterization ofkidney lesions. AJR. American journal ofroentgenology [Internet]. 2006 Jun [cited2012 Feb 25]; 186(6): 1639-50. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/1 6714654
35. Pretorius ES,Wickstrom ML, Siegelman ES.MR imaging of renal neoplasms. Magnetic
Vol. 14 November 2012

-------------------------------------------------------Pulse
Resonance Imaging Clinics Of NorthAmerica. 2000;8(4):813-36.
36. Hilton S. Imaging of renal cell carcinoma.Seminars in oncology [Internet]. 2000 Apr1 [cited 2012 Feb 25];27(2): 150-9.Available from: http://ukpmc.ac.uk/abstract/MED/l0768594.
37. Tuite DJ, Geoghegan T, McCauley G,Govender P, Browne RJF,Torreggiani We.Three-di mensional gadoli niu m-en hancedmagnetic resonance breath-hold FLASHimaging in the diagnosis and staging ofrenal cell carcinoma. Clinical radiology[Internet]. 2006 Jan [cited 2011 Aug30];61 (1):23-30. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16356813
38. Hallscheidt PJ, Fink C, Haferkamp A, BockM, Luburic A, Zuna I, et al. Preoperativestaging of renal cell carcinoma with inferiorvena cava thrombus using multidetector CTand M RI: prospective study withhistopathological correlation. Journal ofcomputer assisted tomography [Internet].[cited 2012 Feb 25];29(1 ):64-8. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/15665685
39. Zhang J, Israel GM, Krinsky GA, Lee VS.Masses and pseudomasses of the kidney:imaging spectrum on MR. Journal ofcomputer assisted tomography [Internet].[cited 2012 Feb25];28(5):588-95. Availablefrom: http://www.ncbi.nlm.nih. gov/pubmed/15480030
40. Choyke PL. Detection and staging of renalcancer. Magnetic resonance imaging clinicsof North America [Internet]. 1997 Feb [cited2012 Feb 25];5(1):29-47. Available from:http://www.ncbi.nlm.nih.gov/pubmed/8995123
41. Hallscheidt PJ,Bock M, Riedasch G, Zuna I,Schoenberg SO, Autschbach F, et al.Diagnostic accuracy of staging renal cellcarcinomas using multidetector-rowcomputed tomography and magneticresonance imaging: a prospective study withhistopathologic correlation. Journal ofcomputer assisted tomography [Internet].[cited 2012 Feb 25];28(3):333-9. Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/15100536.
Vol. 14 November 2072 II
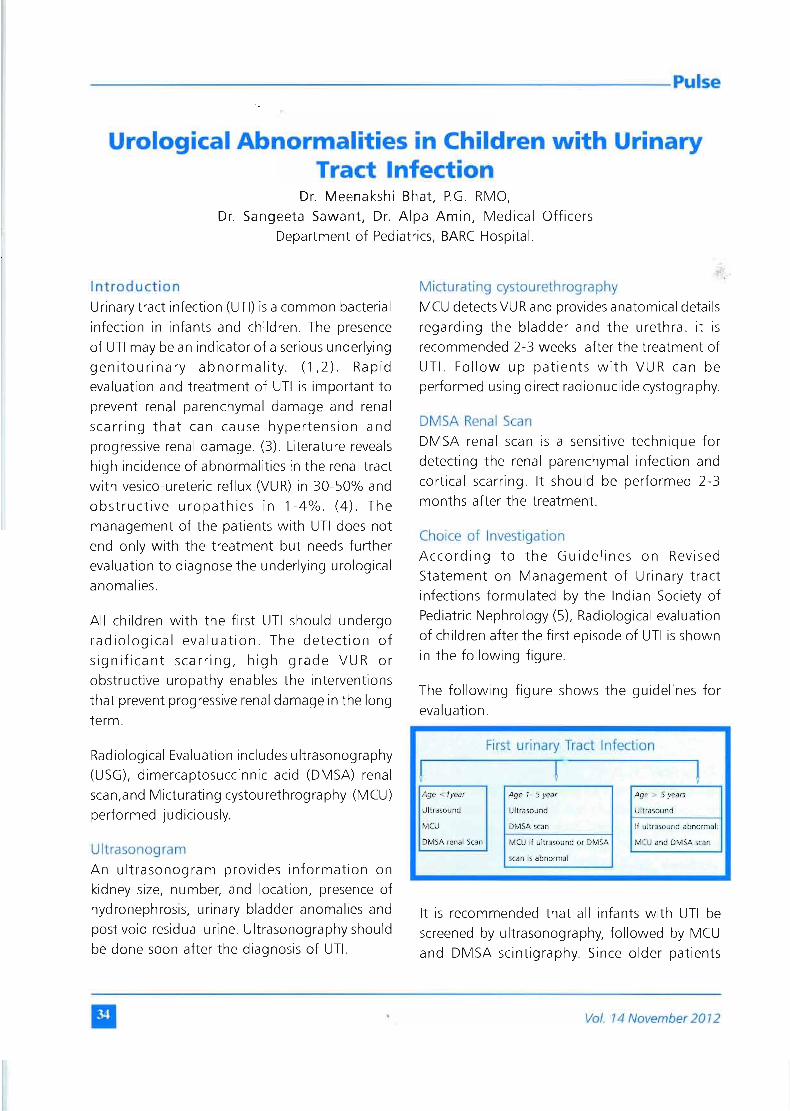
-------------------------------------------------------Pulse
Urological Abnormalities in Children with UrinaryTract Infection
Dr. Meenakshi Bhat, P.G. RMO,Dr. Sangeeta Sawant, Dr. Alpa Amin, Medical Officers
Department of Pediatrics, BARC Hospital.
IntroductionUrinary tract infection (UTI) is a common bacterialinfection in infants and children. The presenceof UTI may be an indicator of a serious underlyinggenitourinary abnormality. (1,2). Rapidevaluation and treatment of UTI is important toprevent renal parenchymal damage and renalscarring that can cause hypertension andprogressive renal damage. (3). Literature revealshigh incidence of abnormalities in the renal tractwith vesico-ureteric reflux (VUR) in 30-50% andobstructive uropathies in 1-4%. (4). Themanagement of the patients with UTI does notend only with the treatment but needs furtherevaluation to diagnose the underlying urologicalanomalies.
All children with the first UTI should undergoradiological evaluation. The detection ofsignificant scarring, high grade VUR orobstructive uropathy enables the interventionsthat prevent progressive renal damage in the longterm.
Radiological Evaluation includes ultrasonography(USG), dimercaptosuccinnic acid (DMSA) renalscan,and Micturating cystourethrography (MCU)performed judiciously.
UltrasonogramAn ultrasonogram provides information onkidney size, number, and location, presence ofhydronephrosis, urinary bladder anomalies andpost void residual urine. Ultrasonography shouldbe done soon after the diagnosis of UTI.
Micturating cystourethrographyMCU detects VUR and provides anatomical detailsregarding the bladder and the urethra. it isrecommended 2-3 weeks after the treatment ofUTI. Follow up patients with VU R ca n beperformed using direct radionuclide cystography.
DMSA Renal ScanDMSA renal scan is a sensitive technique fordetecting the renal parenchymal infection andcortical scarring. It should be performed 2-3months after the treatment.
Choice of InvestigationAccording to the Guidelines on RevisedStatement on Management of Urinary tractinfections formulated by the Indian Society ofPediatric Nephrology (5), Radiological evaluationof children after the first episode of UTI is shownin the following figure.
The following figure shows the guidelines forevaluation.
First urinary Tract Infection
! r !Age < lyear Age 1· 5 year Age> 5 years
Ultrasound Ultrasound Ultrasound
MCU DMSA scan If ultrasound abnormal:
DMSA renal Scan MCU if ultrasound or DMSA MCU and DMSA scan
scan is abnormal
It is recommended that all infants with UTI bescreened by ultrasonography, followed by MCUand DMSA scintigraphy. Since older patients
II Vol. 14 November 20 12

-------------------------------------------------------Pulse
(1 -5 year old) with significant reflux and scars or'Urinary tract anomalies are likely to showabnormalities on ultrasonography, a MCU isadvised in patients having abnormalities on eitherof the above investigations. Children older than5 years are screened by ultrasonography andfurther evaluated only if this is abnormal.
However patients with recurrent UTI at any ageshould undergo detailed imaging withultrasonography, MCU and DMSA scintigraphy.
Our Experience:
Following the above guidelines we evaluated 57cases of UTI in children, in the department ofPediatrics, BARC Hospital.
Aim & Objectives
The Aim of this study was to determine numberof patients having underlying urologicalabnormalities and the specific type ofabnormality.
The diagnosis of UTI was based on Signs andsymptoms of UTI such as fever, pain in abdomen,dysuria, urinary frequency and urine microscopyshowing more than 10 WBCs per high powerfield of centrifuged urine sample or any growthin the urine specimen.
Table 1 : Age group and sex distribution
Age Number Percentage (%)
< 1year 12 20.691 -5 year 34 58.62>5year 12 20.69Total 58 100
Table 2 : Sex incidence
Sex Number Percentage
Male 21 36.21Female 37 63.79Total 58 100
We observed that majority of the children withUTIwere in the age group of 1 -5 years (58.62%).(Tablel).Of all cases 36.71% were males and63.79% were females. The male to female ratiowas 1: 1.8 showing female predominance.(Table2).
Symptomatology
In our study, 36.2% children presented with onlyfever, fever with associated urinary complaintslike dysuria, frequency, urgency and pain inabdomen was seen in 52.6%, while 12% casesdid not have fever.
Investigations
Urine microscopy was positive for more than 10pus cells in all the patients. Urine culture donein all the cases was positive in 63.16%. Theorganism isolated (Table- 3) were E. coli (75%),klebsiella (11.11 %), proteus (11.11 %) andenterobacter (2.78%).
Table 3 : Organisms isolated from urine cultures
Organism isolated Number Percentage (%)
E.coli 27 75
Klebsiella 4 11.11
Proteus 4 11.11
Enterobacter 1 2.78
All patients received appropriate antibiotics for10 - 14 days to control the infection andunderwent full urological investigations.
Radiological Evaluation
All children were subjected to the radiologicalevaluation as perthe Guidelines. Ultrasonographywas performed in all children. DMSA scan wasperformed in 82.57% and 72.41 % weresubjected to Micturating Cystourethrogram.
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
Observations
Urological abnormalities were observed In41.38% cases. Abnormalities were morecommon (70%) in children less than five yearsof age.
Table 4 . Type of Urological Structural anomalies in
*- had associated VUR.
Ultrasound performed in all casesdemonstratedabnormality in 31.03%. The abnormalitiesdetected were hydronephrosis, post void residue,small kidney with scar, calculus withhydronephrosis and ectopic kidney.
DMSA scan revealed renal scarring in 27.7% ofcases. Scarring was seen in children secondaryto Vesicoureteric reflux. Primary scarring withoutany abnormality was seen in only one case.
MCU was abnormal in 38.09% of cases. Theabnormalities detected on MCU wereVesicoureteric reflux (VUR)in 26.19% (Table -5).
Table 5 : Grades of VUR in children
VUR Number Male FemaleGrade 3and below 7 2 5Grade 4 and above 5 4 1
The other anomalies detected werePosterior urethral valve (Zcases);Bladder neck obstruction (1 case)andureterocele (1 case).
After the control of UTI, thesechildren were appropriately manageddepending upon the anomalydetected. They are under regularfollow up in the Pediatric OPD.Children with VUR are regularyfollowed up with ultrasonographyand renal scan. Children with renalscar are under follow up yearly forgrowth, hypertension, renal size andfunction. Those with bowel andbladder dysfunction are managed forthe same.
Conclusion
We observed that in children with UTI,urological abnormality was present in
41.38%. Hence even a single confirmed UTIshould be taken seriously, especially in youngchildren, due to the potential for renalparenchymal damage. Early intervention toidentify and treat them should be carried out soas to prevent serious kidney damage.
Reference:
1. National collaborating centre forWomen's and Children's health. Urinarytract infection in children, diagnosis,treatment and long term management.RCOGPress,London 2007 .available fromwww.Rcpch.ac.uk/Research/ce/Clinical -Aud it/U rinary-tract -infection.
II Vol. 74 November 20 72
Number Male FemaleVesicoureteric reflux (VUR) 11 5 6Posterior urethral valve( PUV) 2 2 -
PUjunction obstruction (PUJ) 2 2 0Ureterocele * 1 1Calculus with hydronephrosis 1 1Bladder neck obstruction withbil hydronephrosis withureteral dilatation 1 1Abnormal urethral meatus 1 1Ectopic kidney 1 1Bladder dysfu nction(post void residue) 2 1 1Extra renal pelvis 1 1Renal scar without otherabnormality 1 1Total 24 11 12

------------------------------------------------------Pulse
2. Chang SL,Shortliffe LD. Pediatric Urinarytract infections.Pediatr c/in North Am.
2006; 53:379-400.
anomalies causing the urinary tractinfection in the children attended thepediatric surgery clinic at the Maternityand Child Teaching Hospital, AI-Qadisiya,Iraq. The N Iraqi J Med. 2011; 7:9-14.3. Joseph TP, Sreekumaran MI, Varma KK.
Incidence of urological anomalies inchildren with urinary tract infections inIndia. Pediatr Surg Int. 1996; 11:566-569.
5. Revised Statement on Management ofUrinary tract infections. The IndianSociety of Pediatric Nephrology. IndianPediatrics. 2011; 48: 709-17.4. Aboud MJ, Kadhim MM. the
microorganism and underlying urological
Alarming facts about Kidney failure
• The kidney has a higher blood flow than brain, liver and heart.
• 50 gallons of blood are filtered through 140 miles of tubes and millions of filters
within the kidney each day.
• The kidneys continue to perform until they have lost 75-80% of their function.
• Lifestyle related disorders like diabetes and hypertension are important causes
of Kidney failure.
• Almost 66% kidney failure occurs due diabetes or hypertension.
• Approximately 7.85 million people suffer from chronic kidney failure in India.
• There were over 1, 50,000 patients were waiting for Kidney transplant in Indiaat the end of 2011.
Vol. 14 November 2012 II

------------------------------------------------------Pulse
Renal Disease and AnaesthesiaDr. Jalpa Kate, P.G.RMO, Dr. Shrividya Chellam, Medical Officers
Department of Anaesthesiology, BARCHospital
Introduction:The kidneys are responsible for a number ofessential functions including water conservation,electrolyte homeostasis, acid base balance, andseveral hormonal functions. When the kidneysare involved in a disease process, some or all ofthese functions may be affected. Knowledge ofhow the kidneys perform these importantfunctions, aids in the understanding ofthe clinicalpresentation, signs and symptoms, andtreatment of renal diseases.
Renal disease is often discovered incidentally,during a routine medical evaluation though somepatients may present with clear evidence of renaldysfunction. Acute as well as chronic renaldisease impairs response to anaesthesia andsurgery. Certain anaesthetic agents and drugs caninduce alteration in renal function.
Relevant Anatomy & Physiology:
Kidneys are paired vital organs. Each kidneyconsists of approximately a million nephrons,which are the functional units of kidney. As theplasma flows along the nephron, virtually all thefluid and solutes are reabsorbed by a number ofactive and passivetransport systems. The kidneysreceive approximately 15% to 25% of totalcardiac output, or 1 to 1.25 Lof blood per minutethrough the renal arteries. A unique feature calledauto-regulation, maintains renal blood flowwhen the mean arterial pressure ranges from60 mm Hg and 160 mm Hg. Interestingly, thekidneys are able to tolerate substantial insultswhile maintaining adequate function despite thistheoretic vulnerability to ischemia.
Renal function tests
Table 1: Tests Used to Evaluate Renal Function
Test Normal ValueGlomerular Filtration RateBlood urea nitrogen 10-20mg/dLSerum creatinine 0.7-1.5 rnq/dl,Creatinine clearance 110-150mU minProteinuria (albumin) < 150 me/day
Renal Tubular Function and/or IntegrityUrine specific gravityUrine osmolalityUrine sodium excretion 1.003-1.030Glucosuria 38-1400mOsm/LEnzymuria <40 mEq/LN-Acetyl-a-glucosaminidasea-Glutathione- 5- tra nsferase
Factors That Influence InterpretationDehydrationVariable protein intakeGastrointestinal bleedingCatabolismAdvanced ageSkeletal muscle massAccurate timed urinevolume measurement
Multiple and severe insults are required to causean injury severe enough to manifest a clinicallyrelevant decrease of renal function. The mostcommon cause of perioperative renal injury isischemia-reperfusion injury. Drugs like certainantibiotics, radiocontrast dyes, NSAIDS can alsoimpair kidney function (Table 2).
II Vol. 14 November 2012

-------------------------------------------------------Pulse
Table 2: Nephrotoxins Commonly Found in the Hospital Setting
EXOGENOUS ENDOGENOUS
Antibiotics (Aminoglycosides, cephalosporins, Calcium (hypercalcemia)amphotericin B, sulfonamide, tetracyclines, vancomycin) Uric acid (hyperuricemia and
hyperu ricosuria)
Anesthetic agents (Methoxyflurane, enflurane) Myoglobin (rhabdomyolysis)Nonsteroidal anti-inflammatory drugs Hemoglobin (hemolysis)(Aspirin, ibuprofen, naproxen, indomethacin, ketorolac) Bilirubin (obstructive jaundice)
Chemotherapeutic-immu nosuppressive agents Oxalate crystals(Cisplatinum, cyclosporin A, methotrexate, mitomycin, Paraproteinsnitrosoureas, tacrolimus)Contrast media
Acute renal failureThis syndrome is a rapid deterioration in renalfunction that results in retention of nitrogenouswaste products (azotemia). it can be divided intoprerenal, renal, and post-renal types dependingon its cause. Prerenal azotemia results from anacute decrease in renal blood flow. Renalazotemia is usually due to intrinsic renal disease,renal ischemia, or renal toxins. Postrenalazotemia is the result of urinary tract obstructionor disruption. Both prerenal and postrenalazotemia are readily reversible in their initialstages but with time progress to renal azotemia.The course of acute renal failure varies widely,but the oliguria typically lasts for 2 weeks and isfollowed by a diuretic phase marked by aprogressive increase in urinary output. Urinaryfunction improves over the course of severalweeks but may not return to normal for up to 1year.
Chronic renal failure
This syndrome is characterized by a progressive.and irreversible decline in renal function over the·~courseof at least 3-6 months. The most commoncauses are hypertension, diabetes, chronicglomerulonephritis, and polycystic renal disease.The full manifestations of this, often referred toas uremia are seen only after the GFRdecreasesbelow 25 rnl/rnin. Patients with clearances below10 ml/min (often said to have end-stage renal
disease) are dependent on dialysis for survivaluntil they receive a successful kidney transplant.
Pathophysiological changes in renal diseases
1) Fluid and electrolyte derangement:Usually certain degree of salt and waterretention is seen. Patient are unable tocompensate for extrarenal fluid lossese.g. diarrhea, vomiting or fever and maydevelop low blood pressure. Potassiumexcretion from body is impaired.
2) impaired calcium absorption leads toosteoporosis.
3) Anemia
4) increased bleeding tendencies due toimpaired function of platelets
5) Cardiovascular system:Most of the patients have high bloodpressure.
Accelerated atherosclerosis may lead toischemic heart disesases like angina,myocardial infarction.
6) immune function is deranged; hencethese patients are prone to infection.
7) Gastrointestinal abnormalities:Bleeding in gastrointestinal tract is seen.Delayed gastric empting leads toanorexia, nausea and vomiting.
Vol. 14 November 2012

-------------------------------------------------------Pulse
8) Neurological abnormality:Peripheral neuropathy characterized bysensory complaints like tingling,numbness, paraesthesia reducedsensations etc are seen in early phaseswhich may later progress to weakness inthe muscles of extremities.
9) Endocrinal changes: renal failure patientswith d ia betes may have red ucedmetabolism of insulin leading to reducedrequirement of insulin.
Drug metabolism and renal diseases
With progressive renal disease, drug excretiongets delayed and active metabolite canaccumulate in body. Also some drugs maythemselves be toxic to kidneys and hence doseadjustment as per renal function (GFR) isrequired.
Following are alterations seen in patients withrenal disease
1) Delayed absorption due to delayedgastric empting
2) Distribution of drug in body may bederanged.
3) Protein binding of drugs is altered.
4) Drugs eliminated by kidneys will haveprolonged elimination half life in body.
Anaesthesia in patients with renal diseases
Anaesthesia aimsMaintain normal blood volumeMaintain normal BPAvoid nephrotoxic drugsAvoid drugs which depend mainly onkidneys for elimination
Preoperative evaluation
Patient's medical history: Establish cause of renalfailure, duration and need for dialysis. Associatedconditions like diabetes, hypertension and heartdiseasesneed to be noted. Conditions associatedwith renal failure (mentioned above) need to benoted too.
Preoperative laboratory investigations:
1) Complete blood count- hemoglobin(Iow- decreased red blood cell synthesis,increase breakdown of red cells), Whiteblood cell count- raised suggest infection,platelet count.
2) Blood glucose level- diabetes is the mostcommon cause for renal impairment. ., .
3) Renalfunction tests- blood urea nitrogen,serum creatinine are raised. Creatinineclearance calculated from creatininevalue helps in dose adjustment.
4) Serum electrolytes- most commonlyserum potassium value are raised.
5) Coagulation study- mainly clotting study.
6) ECG- for ischemia, arrhythmia orelectrolyte dysfunction.
7) X ray chest- signs of fluid overload.
8) Arterial blood gas- evaluate acid basestatus.
9) Liver function test- if major surgery isplanned.
Preoperative optimization:
1) Treatment of anemia.
2) Evaluation and treatment of associatedcardiac diseases.
3) Normalize blood pressure.
4) Correct serum potassium levels ifabnormal.
5) Dialysis if evidence of fluid overload-lower limb edema, pleural effusion.
6) Control of diabetes.
Preoperative premed ication:
1) Antihypertensive medication continued.
2) Aspiration prophylaxis with an H2 blockermay be indicated in patients with nausea,vomiting, or gastrointestinal bleeding.Metoclopramide, 10 mg orally or slowlyintravenously, may also be useful inaccelerating gastric emptying, preventing
Vol. 14 November 2012

-------------------------------------------------------Pulse
nausea, and decreasing the risk ofaspiration
3) Preoperative use of sedatives should beindividualized. Alert patients who arerelatively stable can be given sedatives toallay anxiety especially who are havingischemic heart disease.
4) Patients on hemodialysis should undergodialysis during the 24 hours precedingelective surgery.
5) The preoperative presence of acoagulopathy may be treated.
Monitoring during surgery and anaesthesia:
Noninvasive monitors-
ECG, noninvasive BP, pulseoximetry,capnogaphy, neuromuscular block,Temperatu re.
Invasive monitors-Central venous pressure (fluid status), Arterial line(ABG, invasive BP Monitoring). hourly urineoutput, blood sugar by finger prick in diabeticpatients, nasogasric tube. Pulmonary arterialpressure in selected patients.
General Anaesthesia:
Anaesthesia drugs in renal disease:
Fluid administration:Fluid therapy should be cautious in these patients,as these patients can be in fluid overload, and ifrequired central venous monitoring may be doneto guide fluid replacement.
Regional Anaesthesia:Adequacy of coagulation should be consideredand the presence of uremic neuropathiesexcluded before regional anesthesia is performedin these patients. Dose of local anaesthetics maybe reduced by 25% because of altered proteinbinding and lowered seizure threshold.
Post operative pain relief:Managing postoperative pain IS important inthese patients. Paracetamol can be used safelyin patients with deranged renal function. Nonsteroidal anti-inflammatory drugs (NSAIDs) arebest avoided due to their nephrotoxic potential.Opioids can be used for postoperativepain. Possibility of prolonged half life of thesedrugs in view of impaired renal excretionespecially morphine must be considered. Weakopioids, like tramadol, can be used with dosemodification and monitoring. Regionalanaesthesia too, in the absence of coagulopathy,can provide adequate pain relief. Hypotension
Drug class Safe Use with caution Avoid
Induction agents Propofol Thiopental sodium,ketamine
Sedatives Midazolam,diazepam,lorazepam,alprazolam
Narcotics Fentanyl, Morphine, Pethidineremifentanil Alfentanil
Muscle relaxants atracurium, Vecuronium, doxacurium,cis-atracu rium, Rocuronium, pancuroruum.
succinylcholi ne,. .
rruvacunum prpecuroruum,d-Tubocurarine
Analgesics Paracetamol NSAIDS
Vol. 14 November 2012 III

-------------------------------------------------------Pulse
associated with neuraxial block has to be avoidedsince it can compromise renal blood flow.
Perioperative problems which can beencountered in patients with renal disease:
1) Bleeding- platelet function defect
2) Fluid overload
3) Hypo/ hypertension
4) Inadequate recovery from neuromuscularblocking agents
5) Worsening of renal function.
6) Difficult intravenous access
Conclusion:
The kidney plays a central role in implementingand controlling a variety of homeostaticfunctions. Renaldysfunction can occur asa directresult of surgical or medical disease, prolonged
reduction in renal oxygen delivery, nephrotoxininsult, or a combination of these factors. Theemphasis in the care of these patients ispreservation of the remaining renal function,which is best accomplished by maintainingnormovolemia, judicious fluid administration,dialysis with its implications, avoidingnephrotoxic drugs and drug dose reduction toavoid prolong effect. Thus although anaesthesiain patients with renal impairment are challenging,careful approach towards management canresult in successful outcome.
References:
1) Miller's Anaesthesia, Seventh edition, pg 2105-2134.
2) Clinical anesthesiology, G. Edward Morgan,Jr., fourth edition, pg 742-756.
3) Clinical anesthesia, Paul G. Barash, sixthedition, pg 1347-1374.
Historical references to Kidney stones
• Hippocrates (470/460 B.C.-380/360 B.C.) makes reference to kidney stones in thefamous Hippocratic Oath as follows: "I will not cut persons labouring under thestone, but will leave this to be done by men who are practitioners of this work."
• Louis Napoleon, n=phew of Napoleon Bonaparte, lost the Franco-Prussian War of1870 due wholly or in part from impaired kidney function resulting from kidney stoneformation.
Vol. 14 November 2012

-------------------------------------------------------Pulse
Urine Protein ElectrophoresisDr. Nitin Chikhale P.G.RMO, Dr. Uma Chaturvedi Medical Officer,Dr. Richa Patel DNB Student, Dr. Susan Cherian Medical Officer
In kidneys, the glomerular capillary wall ispermeable to substances with molecular weightof 20 kDa or less.' A normal adult excretes up to150 mg/24hr of protein in urine.' Normal urinaryproteins consist of about 2/3 plasma proteins and1/3 protein derived from the urinary tract. Oncein filtrate, low molecular weight proteins arereabsorbed and metabolized by the proximaltubule cells. This is most readily seen in two-dimensional electrophoretic map.'
Proteinu ria: 1.2
Proteinuria is defined as urinary protein excretionof more than 150 mg per day. Microalbuminuriacan be a sign of early renal disease, especially indiabetic patients. In microalbuminuria, 30 to 150mg protein is excreted per day.
Types of proteinuria: '.2
Proteinuria can be transient (intermittent),orthostatic (relate to sitting / standing) orpersistent (a Iways present). Intra nsientproteinuria, protein in urine disappears when theunderlying cause is resolved.
In orthostatic proteinuria, protein excretion IS
normal when the patient is lying down but isincreased when a person is sitting or standing. Itoccurs in approximately 2 to 5 percent of youngpeople, but is unusual in people over the age of30.
Persistent proteinuria can be further defined asglomerular, tubular or overflow. The mostcommon type is glomerular proteinuria withalbumin as the primary urinary protein. This type
of proteinuria is caused by increased filtration ofalbumin and other macromolecules across theglomerular basement membrane.
Tubular proteinuria results when malfunctioningtubule cells no longer reabsorb proteins in thefiltrate; low molecular weight proteins such as~2 microglobulin and immunoglobulin lightchains dominate over albumin.
In overflow proteinuria, low molecular weightproteins overwhelm the ability of the tubules toreabsorb the filtered proteins. Bence-Jonesproteinuria is the classicexample of overflow (andalso tubular) proteinuria. Quantitativemeasurement of Bence Jones proteins anddetermination that they are monoclonal, aid inthe diagnosis of various disorders includingmultiple myeloma - the malignant proliferationof plasma cells.
Urine protein electrophoresis:'
Urine protein electrophoresis (UPEP) is utilizedto detect the type and concentration of variousproteins in urine. The test provides informationabout the location and degree of damage withinthe nephron. Urine immunofixationelectrophoresis (UIFE)helps to determine the typeof protein detected by UPEP.Urine electrophoresisshould be performed whenever it may be ofclinical value to identify the proteins in urine inorder to evaluate the nature or extent of renal
Normal Urine electrophoresis
'Y ce-I Albumin
Vol. 14 November 2012

-------------------------------------------------------Pulse
damage. But on the other hand, it is importantto know that the patient with renal tubulardisease may also have protein excretions withinthe normal range.
A typical pattern of highly concentrated normalurine contains a small amount of albumin and atrace of transferrin, no other discrete peaks areusually visible.
There are several relatively benign conditionswhich cause significant increase of plasmaproteins in the urine. These include pregnancy,exercise, postu ra I hematu ria and ma rchhematuria. The patterns in these conditionstypically mirror serum electrophoretic pattern.
Trace amount of proteins in urine are importantin the monitoring of some disease states. Theearly stages of diabetic renal disease aremonitored by following the excretion of serumalbumin. The upper limit of normal for urinarymicroalbumin is 20-30 mg/day. Urinarymicroalbumin is typically measured by using lowlevel immunodiffusion plates.
Electrophoretic pattern of urinary proteins:"• Glomerular proteinuria: albuminuria is
hallmark (making up 60 to 90% of totalproteinuria)
• Tubular proteinuria: low molecular weightproteins predominate with total urine proteinrarely> Zq/d -• Impaired tubular reabsorption of low
molecular weight proteins, or
• Overproduction of low molecular weightproteins, such as light chains in myeloma.
Glomerular proteinurua (urine sample)
Iy a-1 Albumina-2
Tubular proteinuria (urine sample)
I y B a-2 a-1 Albumin
• Selective proteinuria expressed as clearance ofIgG over clearance of transferrin is reliableindicator of severity and reversibility ofabnormalities of glomerular proteinuria; patientswith highly selective proteinuria have mildertubulointerstitial damage, improved prognosisand better response to therapy:
Selectivity index (51) = urine IgG / serum IgG xserum transferrin / urine transferrin,
• 51 < 0.10 : Highly selective;
• 51 > 0.11 and d" 0.20 : Moderately selective;
• 51 > 0.21 : Nonselective.
A. AL Amyloidosis C. Nephrotic SyndromeB. Multiple Myeloma
y a alb a alb y
Vol. 14 November 2012
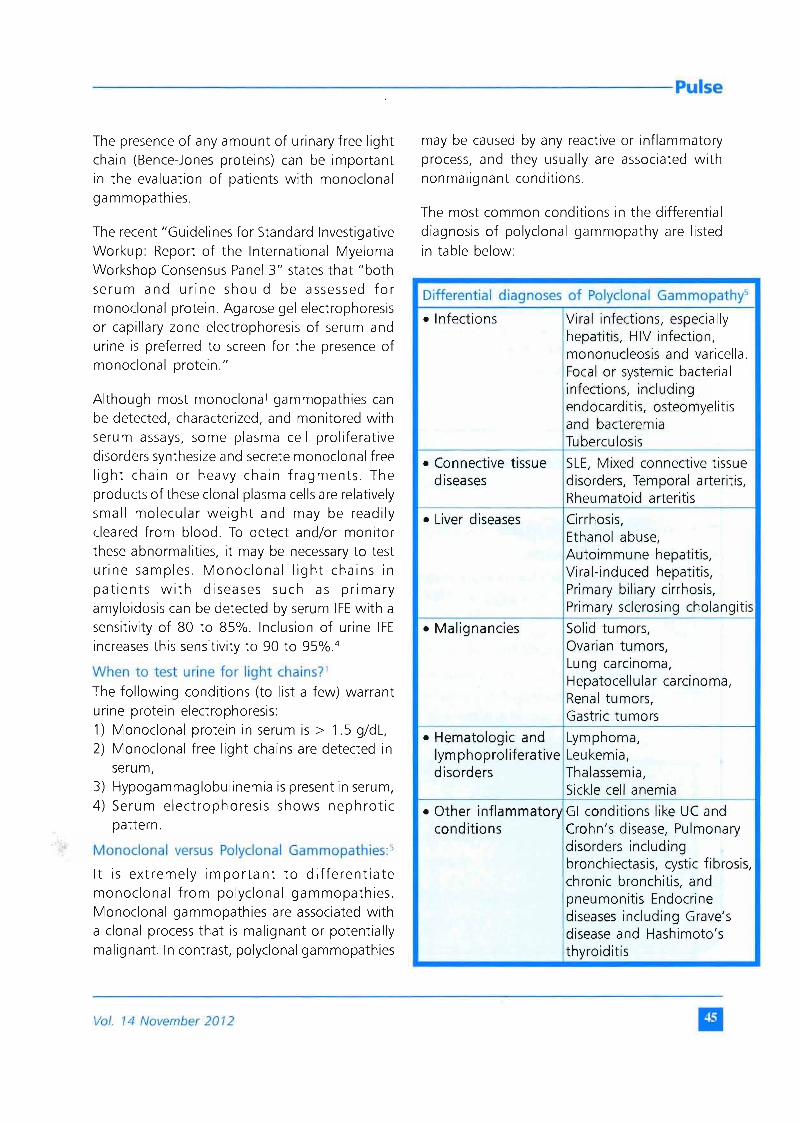
------------------------------------------------------Pulse
The presence of any amount of urinary free lightchain (Bence-Jones proteins) can be importantin the evaluation of patients with monoclonalgammopathies.
The recent "Guidelines for Standard InvestigativeWorkup: Report of the International MyelomaWorkshop Consensus Panel 3" states that "bothserum and urine should be assessed formonoclonal protein. Agarose gel electrophoresisor capillary zone electrophoresis of serum andurine is preferred to screen for the presence ofmonoclonal protein."
Although most monoclonal gammopathies canbe detected, characterized, and monitored withserum assays, some plasma cell proliferativedisorders synthesize and secrete monoclonal freelight chain or heavy chain fragments. Theproducts of these clonal plasma cells are relativelysmall molecular weight and may be readilycleared from blood. To detect and/or monitorthese abnormalities, it may be necessary to testurine samples. Monoclonal light chains inpatients with diseases such as primaryamyloidosis can be detected by serum IFEwith asensitivity of 80 to 85%. Inclusion of urine IFEincreases this sensitivity to 90 to 95%.4
When to test urine for light chains?'The following conditions (to list a few) warranturine protein electrophoresis:1) Monoclonal protein in serum is > 1.5 q/dl,2) Monoclonal free light chains are detected in
serum,3) Hypogammaglobulinemia is present in serum,4) Serum electrophoresis shows nephrotic
pattern.
Monoclonal versus Polyclonal Garnrnopathies:>
It is extremely important to differentiatemonoclonal from polyclonal gammopathies.Monoclonal gammopathies are associated witha clonal process that is malignant or potentiallymalignant. In contrast, polyclonal gammopathies
may be caused by any reactive or inflammatoryprocess, and they usually are associated withnonmalignant conditions.
The most common conditions in the differentialdiagnosis of polyclonal gammopathy are listedin table below:
Differential diagnoses of Polyclonal Garnrnopathy"
• Infections Viral infections, especiallyhepatitis, HIV infection,mononucleosis and varicella.Focal or systemic bacterialinfections, includingendocarditis, osteomyelitisand bacteremiaTuberculosis
• Connective tissue SLE, Mixed connective tissuediseases disorders, Temporal arteritis,
Rheumatoid arteritis
• Liver diseases Cirrhosis,Ethanol abuse,Autoimmune hepatitis,Viral-induced hepatitis,Primary biliary cirrhosis,Primary sclerosing cholangitis
• Malignancies Solid tumors,Ovarian tumors,Lung carcinoma,Hepatocellular carcinoma,Renal tumors,Gastric tumors
• Hematologic and Lymphoma,Iymphoproliferative Leukemia,disorders Thalassemia,
Sickle cell anemia
• Other inflammatory GI conditions like UC andconditions Crohn's disease, Pulmonary
disorders includingbronchiectasis, cystic fibrosis,chronic bronchitis, andpneumonitis Endocrinediseases including Grave'sdisease and Hashimoto'sthyroiditis
Vol. 14 November 2012 II

---------------------------------------------------------Pulse
References:
1) Aigars Brants. Urine protein electrophoresis:Latest Consensus Statements,Recommendations and Testing options. In:newsletter by Sebia Inc.,Norcross,GA;Separation 2009; 1(10): 1-2. Downloadedfrom:www.sebia-usa.com/files/newsletter10-1.pdf
2) Richard A. McPherson, Jonathan Ben-Ezra,Shourong Zhao. BasicExamination of Urine.In: Henry's clinical diagnosis andManagement by Laboratory methods, 21 sted.,W.B.Saunders Comp,2006
3) Mitchell H. Rosner and W. Kline Bolton.Renal Function Testing. American journal ofKidney diseases 2006;47(1): 174-183.
4) A.c. Roden, K.S.Lockington, L.J.Tostrud andJ.A. Katzmann. Urine protein electrophoresisand immunoelectrophoresis usingunconcentrated or minimally concentratedurine sample. Am J Clin Pathol2008;130:141-145.
5) KyleRA. Sequence of testing for monoclonalgammopathies. Arch Pathol Lab Med.1999; 123: 114-8.
Keep your kidneys healthy and save your heart
• Keeping fit and active
• Keep regular control of your blood sugar level
• Monitor your blood pressure
• Eat healthy and keep your weight in check
• Maintain a healthy fluid intake
• Do not smoke
• Do not take over-the-counter pills on a regular basis
• Check your kidney function if you have one or more of the 'high risk' factors
• you have diabetes
• you have hypertension
• you are obese
• you or one of your family members suffers from kidney disease
• Reduced kidney function and increased protein loss are both important and recently
discovered risk factors for heart disease.
• The kidneys and the heart are closely linked.
• The heart and kidneys also have common risk factors for poor function -smoking, high
blood pressure, diabetes and high blood lipids.~ A
II Vol. 14 November 2012

-------------------------------------------------------Pulse
Tertiary Hyperparathyroidism Following Chronic Renal Failure- A Case Report
Dr. Jayesh Kalbhande, Dr. Yogesh Shejul, Dr. Pallavi Bhandarkar, Medical Officers, Thyroid Clinic
Dr. Shrividya Chellam, Medical Officer, Department of Anaesthesiology BARCHospital
Introduction
Nowadays, patients with chronic renal failureundergoing dialysis are on the rise and thereforecases of secondary hyperparathyroidism arecommon. However, cases of tertiaryhyperparathyroidism are relatively rare. Wepresent here a case of tertia ryhyperparathyroidism and discuss thepathophysiology and different treatment optionfor secondary and tertiary hyperparathyroidism.
Case Report
A 39 yr old male patient, known case of chronicrenal failure, was on regular hemodialysis. Hehad been diagnosed with hypertension at theage of 21 years and his renal biopsy showedchronic proliferative glomerulonephritis. Hiskidney function had deteriorated gradually andhe was put on regular hemodialysis since 24 yearsof age. He had received a cadaveric renaltransplant at the age of 27 yr but had developedsevere respiratory tract infection within 6 monthof transplant. His immuno-suppressant therapy
was stopped due to severe infection as a lifesaving measure and thus he ended up withrejection of the transplanted kidney which hadto be removed and he was put back on regularhemod ialysis thereafter.
He presented with loss of appetite, easyfatigueability and severe bone pain. He was onregular erythropoietin injections, vitamin D andcalcium supplements and his hypertension waswell controlled with prazocin.
His blood test reports were as follows:
Dexa scan showed severe osteoporosis in entireskeleton with high risk for fracture. TechnetiumMIBI scan for parathyroid gland uptake showedincreased uptake in left lower parathyroid gland.His Technetium pertechnetate and tetrofosminscan showed increased uptake in right lowerparathyroid gland. In view of above, Tertiaryhyperparathyroidism with polyglandularhyperplasia was diagnosed.
Test Performed Normal Range Patient's values Year wise
2005 2006 2007Serum parathyroid hormone 12 to 72 pg/ml 1823 2627 212025 hydroxy cholecalciferol 7.6 to 75 ng /ml - - 42.7Serum calcium 8.5 - 10.5 mq/dl - 10.2 10.7Serum Phosphorus 3.5 -5.5 mq/dl - 6.2 6.3Serum alkaline phosphatase 30-150U/L - - 380Serum Albumin 3.5 - 5.5 mq/dl - - 4.2Serum creatinine 0.2-1.5mg % - - 11.5
Vol. 14 November 2012

------------------------------------------------------Pulse
He underwent total parathyroidectomy but halfof one parathyroid gland was implanted back inthe right sternocleidomastoid muscle undergeneral anesthesia. Histopathology of all fourparathyroid gland showed hyperplasia of chiefcells.
Post operatively, this patient developed severehypocalcemia due to 'hungry bone syndrome'which was treated with calcium gluconateinfusion. He also developed thrombosis of rightarterio-venous fistula with right subclavian veinthrombosis which was managed with Inj. Heparinand closure of right arteriovenous fistula.
Gradually, he recovered completely and four yearssince his surgery, serum parathyroid hormonelevels are normal. He does not have any bonepain and his stamina has improved though he isstill on regular hemodialysis.
Discussion
The parathyroid glands are four pea-sized glandslocated on the thyroid gland in the neck.Although their nomenclature seems similar, thethyroid and parathyroid glands are entirelydifferent glands, each producing distincthormones with specific functions. Theparathyroid glands secrete parathyroid hormone,a polypeptide that helps maintain the correctbalance of calcium and phosphorous in the body.PTH is involved in the homeostasis of bonemetabolism and regulates the level of calcium inthe blood, release of calcium from bone,absorption of calcium from the intestine, andexcretion of calcium in the urine
The pathophysiology of secondary and tertiaryHPT
Chronic renal failure (CRF)causes abnormalitiesin the renal tubular absorption of phosphatewhich lead to reduced phosphate excretion and
hyperphosphatemia. Also, renal conversion of25-hydroxycholecalciferal to 1, 25-dihydroxycholecalciferol which is active form ofvitamin D is impaired. Thus it leads to deficiencyof active vitamin D resulting in decreasedintestinal absorption of calcium andhypocalcemia. Hyperphosphatemia, low vitaminD and hypocalcemia together stimulatesincreased formation and release of parathyroidhormone. As a consequence of prolongedhypocalcemia, parathyroid chief cell hyperplasiaoccurs and PTHsecretion increases.
Secondary HPT (SHPT)occurs most commonly"secondary" to chronic renal failure (CRF).Hencesecondary HPT is frequently referred to as renalHPT.Estimates suggest that as many as 90% ofpatients with CRFdevelop this diseaseby the timehemodialysis is initiated. Other causes ofsecondary HPTinclude osteomalacia, rickets, andmalabsorption.
Initially, the secretion of parathyroid hormoneby hyperplastic chief cells is regulated by negativefeedback by calcium acting on calcium receptorlocated on chief cells. Thus normocalcemia orhypercalcemia suppresses PTH formation.However, as a result of prolonged hypocalcemiaand stimulation, chief cells become autonomousand they secrete parathyroid hormone in spiteof high level of serum calcium which leads tohypercalcemia and resembles primary HPT.Thiscondition is called "tertiary HPT".
99mTc-sestimibi scintigraphy
Secondary hyperparathyroidism result inhyperplasia of all 4 parathyroid glands. Thesensitivity of imaging modalities such as 99mTc-sestimibi scintigraphy and ultrasound is poor inpatients with multiple gland disease. This isevident in our case where Technetium MIBI scanand Technetium pertechnetate tetrophosmin
II Vol. 14 November 2012

-------------------------------------------------------Pulse
scan showed uptake in different parathyroid
gland. However, it is a useful investigation inpatients with recurrent hyperparathyroidismwhere there is a single functioning parathyroid
gland in which case accuracy of localization is ashigh as 95-100%.
Goals of SHPT Treatment
The ultimate goals of treating SHPT are tonormalize mineral metabolism, prevention orreversal of osteitis fibrosa cystica and
maintenance of bone strength. The markers ofcalcium «;». phosphorus (P), vitamin D and PTH
are used as surrogate measures of diseaseprogression.
1. Target range of serum P 3.5-6.0 rnq/dl
2. Target range of serum Ca 8.4-10.0 rnq/dl
3. Target range of PTH 60-180 pg/ml
In chronic renal failure, bones are resistant toaction of parathyroid hormone as a result of
uremia. Therefore, they require more than normallevel of parathyroid hormone to maintain
homeostasis. Excessive suppression ofparathyroid hormone in CRF can lead todecreased turnover of bone, called as adynamic
bone disease. Therefore, Target range ofparathyroid hormone is kept at 2 -3 times normalvalue in CRF.
Vitamin D therapy
One of the first abnormalities noted on evaluation
may be an isolated increase in PTH. If the PTHconcentration exceeds the target range, theserum 25 (OH) cholecalciferol concentration
should be measured and if that is found to be <30 nq/ml. then dietary deficiency of Vitamin D isdiagnosed and ergocalciferol (vitamin D2)
therapy should be initiated.
If the concentration of 25(OH) cholecalciferol is
> 30 ng/ml and the PTH concentration exceeds
the target range, then inadequate conversion ofvitamin D to active form secondary to CRF isdiagnosed and an activated vitamin D agent
should be initiated.
Of the active form of vitamin D, Calcitriol was
the first agent available. It has the same structureas endogenous activated vitamin D3 [1,25 (OH)
cholecalciferol] and therefore the samepharmacological actions. It stimulates gut and
parathyroid Vitamin D receptors (VDR). Becauseof its affinity for intestinal VDR, calcitriol has the
greatest propensity to increase serum calciumconcentrations. It is especially useful when theserum calcium level is less than the mid-point of
the target range.
Paricalcitol (19-nor-1,25(OH)2D2) and
doxercalciferol (1a-(OH) vitamin D2) are vitamin
D agents that have less affinity for the intestinalreceptors and have been shown to cause a lower
incidence of hypercalcemia. Therefore, they arethe d rugs of choice in presence ofhyperpa rathyroid ism with hyperca Icem ia.
Doxercalciferol is a vitamin D2 pro-drug, 1a (OH)cholecalciferol, and requires activation by hepatic
25-hydroxylase. Therefore, doxercalciferol shouldnot be used in patients with hepatic dysfunction.
Efficacy of therapy for SHPT is generally measuredby the degree of suppression of PTH. Active formsof vitamin D appear to provide greatersuppression of PTH than doxercalciferol,paricalcitol and cinacalcet.
Dietary phosphate restriction
Hyperphosphatemia generally becomes prevalentas the GFR declines to < 30 ml/min/1.73 m2.Dietary phosphate restriction is one of the firstinterventions recommended to lower serumphosphate concentrations. Foods that are highin phosphate content include dairy products,
Vol. 14 November 2012

-------------------------------------------------------Pulse
meats, beans, dark sodas, beer, and nuts. Manyfoods that are high in phosphorus are alsoprimary sources of protein, particularly meats.Generally, patients are instructed to reduce theirintake of or avoid foods that are high inphosphorus but not high in protein. Examplesof foods to avoid include cheese, milk, ice cream,beer, and dark sodas.
Phosphate binding agents
Phosphate binding agents decrease serumphosphate concentrations by binding to dietaryphosphate in the gut, forming an insolublecomplex that is excreted in the feces. Optimally,these agents are administered with food and aregenerally taken three times daily with meals.Phosphate binders from different classes may becombined to achieve target concentrations ofphosphorus and calcium. In fact, the combineduse of a calcium-containing phosphate binderand a non-calcium-containing phosphate bindermay reduce the serum phosphorus level whilemaintaining the calcium concentration. Likewise,the use of one or more non-calcium-containingphosphate binders (e.g., sevelamerhydrochloride) may be needed for patients withhyperphosphatemia with concurrenthypercalcemia.
Calcimimetic agents
It acts by binding to and modifying the calciumsensing receptor(CaR) on the chief cell of theparathyroid gland. This change causes anincreased sensitivity of the receptor to seru mcalcium. Cinacalcet is effective in decreasing PTHconcentrations and maintaining calcium andphosphorus concentrations. It can be used incombination with phosphate binders and vitaminD agents. An increase in serum calcium resultsin rapid diminution of parathyroid hormone (PTH)secretion via activation of the CaR in theparathyroid and enhanced calciuria via activationof the CaR present in the thick ascending limb of
the loop of Henle. Calcimimetics bind to the CaRand result in a marked shift in the calciumresponse curve, reflecting overactivation of theCaR and resulting in suppression of serum PTH.Optimum dose is 30 to 180mg per day. However,it is known to cause hypocalcemia andhyperphosphatemia as hypercalcemic and ahypophosphatemic effect of parathyroidhormone is absent.
,~,
Indications for parathyroidectomy in patientswith secondary HPT
Calciphylaxis
Medical observation not possible
Failure of maximal medical management with:Hyperca Icem ia, Hyperca Icu ria
PTH > 800 pg/m L
Hyperphosphatemia (with calcium x phosphorus>70)
Osteoporosis
Symptoms: pruritus, pathologic bone fracture,ectopic soft tissue calcifications, bone pain.
Surgical Approach
The most commonly accepted approaches inthese patients are
Subtotal parathyroidectomy - it involvesremoval of 3 and 1/2 parathyroid gland with112 gland is left in situ.
2 Total parathyroidectomy with autotransplantation - It involves removal of all 4parathyroid gland with autotransplantationof 1f2 of one parathyroid gland into thenondominant forearm orsternocleidomastoid.
Intraoperative parathyroid hormone monitoring(ioPTH)
Studies have shown that ioPTH testing dependson renal function and PTH assay specificity. A50% drop from the baseline ioPTH is considered
II Vol. 14 November 2012

-------------------------------------------------------Pulse
predictive of sufficient parathyroid tissueresection. Depending on the specificity of theassay,an adequate drop in ioPTH levels (>50%)may not be seen for up to 30 minutes aftercurative resection because of CRFand delayedPTHclearance. Lack of consensus guidelines forioPTH monitoring in patients with tertiary HPTand skepticism over the potential impact on theoverall successrate of parathyroidectomy has ledsome groups to abandon the routine use of thisadjunct.
Radioguided parathyroidectomy
Another state of the art advance that facilitatesintraoperative management of patients withsecondary and tertiary HPT is application ofradioguided techniques. Patients are injectedwith 10 mCi of 99mTc-sestamibi approximately1 to 2 hours before surgery. A gamma probe isthen utilized to identify parathyroid glandsintraoperatively.
Minimally invasive parathyroidectomy ( MIP )
During the last two decades, several techniquesfor minimally-invasive parathyroidectomy havebeen developed, including open approaches(open minimally-invasive parathyroidectomy),Endoscopic pa rathyroidectomy, mi ni ma Ilyinvasive video-assisted parathyroidectomy(MIVAP), The term "minimally invasive" shouldbe reserved to a procedure that allows thesurgeon to perform a traditional operationthrough an access that minimizes the trauma ofsurgical exposure and dissection. Open MIPindicates parathyroid procedures performedthrough a small incision, usually less than 2.5-3cm.
Endoscopic parathyroidectomy (EP)
Total EPwas first described by Gagner in 1996.It is carried out entirely under a steady gas flow,using a 5 mm endoscope introduced through acentral trocar and two or three additional trocars
for needlescopic instruments. All endoscopictechniques are characterized by continuous C02insufflation or mechanical external retraction tomaintain the operative space for dissection andtrocar positioning.
Minimally - invasive video - assistedparathyroidectomy (MIVAP)
MIVAP was firstly described by Miccoli et al. Asmall (1.5-2.0 cm) skin incision is performedbetween the cricoid cartilage and the sternalnotch, in the midline. The thyroid lobe isseparated from the strap muscles with smallconventional retractors (Farabeuf retractors),which are also used to maintain the operativespace. At this point, the endoscope (5 mm, 30°)and the small surgical instruments are introducedthrough the single skin incision without usingany trocar. After identification, the affectedparathyroid gland is bluntly dissected underendoscopic vision by using dedicated spatulasand a spatula shaped aspirator.
Anaesthesia in CRFand SHPT patients
Administrating general anesthesia to an anuricpatient on hemodialysis is a challenge and hasits own attendant risks. Nephrotoxic agents anddrugs which depend entirely on the kidneys fortheir elimination such as diclofenac,aminoglycosides, pancuronium etc should beavoided. Patients need pre-operativehemodialysis which increases the risk ofcoagulation abnormalities. Therefore heparin freehemodialysis is preferred. Often, dehydrationpost dialysis leads to hypotension especially afterinduction of anesthesia. Incidences of fluidoverload, congestive cardiac failure and delayedemergence from anesthesia are higher in suchpatients as also post operative hypocalcemia,laryngeal spasm and tetany and need for postoperative ventilatory support.
Vol. 14 November 2012 II

----------------------------------------------------Pulse
Hungry bone syndrome
The postoperative hypocalcemia probably resultsfrom acute reversal of the PTH-inducedcontribution of bone resorption to maintain theserum calcium concentration. In the hightu rnover state associated withhyperparathyroidism, PTH increases boneformation and resorption with a net efflux ofcalcium from bone. Sudden withdrawal of PTHin such patients causes an imbalance betweenosteoblast-mediated bone formation and
osteoclast-mediated bone resorption andperhaps other changes affecting calcium fluxes,
leading to a marked net increase in bone uptakeof calcium, phosphate and magnesium and thus
causing severe, persistent and prolongedhypocalcemia.
Conclusion
Thus, HPT is a complex and challenging
condition. Metabolic parameters such as calcium,phosphate, PTH, and vitamin D must bemaintained within target ranges to prevent bonedisease and extraskeletal calcification, decrease
cardiac disease risk, and maintain homeostasisof other body systems. Additionally, all of theseparameters need to be controlled simultaneouslyto be successful.
Low calcium
Low phosphorus
Treatment
Calcium Carbonate
High doses of Vitamin D
High CalciumLow Phosphorus
TreatmentSevelamerCinacalcetLow dose of Vitamin D orDoxercalciferol, Paricalcitol
Control of calcium and phosphorus during
treatment
Further reading
• Secondary and Tertiary Hyperparathyroidism:
state of art surgical management. Susan C.
Pitt Surgical Clinics of North America, volume
89, (2009) 1227-1239
• Minimally invasive video - assisted
parathyroidectomy (MIVAP) for secondary
hyperparathyroidism: report of initial
experience, Piero F. Alesina, The AmericanJournal of Surgery (2010) 199,851-855
• Evaluation of Hypercalcemia in Relation to
Hyperparathyroidism, Phillip K. Pellitteri,
Otolaryngologic Clinics of North America -Volume 43, Issue 2 (April 2010)
• Clinical Practice Guideline for the
Management of Secondary
Hyperparathyroidism in Chronic Dialysis
Patients, Guideline Working Group, Japanese
Society for Dialysis Therapy, TherapeuticApheresis and Dialysis volume 12(6):514-525(2008)
Low calciumHigh Phosphorus
TreatmentCalcium carbonateLow dose of Vitamin D
High CalciumHigh Phosphorus
TreatmentSevelamerLow dose of Vitamin D orDoxercalciferol, ParicalcitolConsider Parathyroidectomy
Vol. 14 November 2012

---------------------------------------------------------Pulse
Infection Control MeasuresDr. Amrita Misri, Convener Infection Control Committee
CDC's Core Interventions for Dialysis Blood Stream Infection Prevention. - -
What Healthcare Providers Can Do:1. Chlorhexidine for skin antisepsis:Use an alcohol-based chlorhexidine (>0.5%) solution as the firstline agent for skin antisepsis, particularly for central line insertion and during dressing changes.Povidone-iodine, preferably with alcohol, or 70% alcohol are alternatives.2. Catheter hub cleansing: Cleanse catheter hubs with an appropriate antiseptic after the cap isremoved and before accessing.3. Antimicrobial ointment or chlorhexidine-impregnated sponge dressing: Apply bacitracin/gramicidin/polymyxin B ointment or povidone-iodine ointment to catheter exit sites during dressingchange OR use a chlorhexidine-impregnated sponge dressing.
What Healthcare Institutions Can Do:1. Surveillance and feedback using National Health Safety Network: Conduct monthly surveillancefor Blood stream infections and other dialysis events and enter National Center for Emerging andZoonotic Infectious Diseasesevents into CDC's National Healthcare Safety Network. Calculate facilityrates and compare to rates in other facilities using NHSN. Actively share results with front-line clinicalstaff.
2. Hand hygiene surveillance: Perform monthly hand hygiene audits with feedback of results toclinical staff.
3. Catheter carel vascular access observations: Perform quarterly audits of vascular access care andcatheter accessing to ensure adherence to recommended procedures. This includes aseptic techniquewhile connecting and disconnecting catheters and during dressing changes. Share results with front-line clinical staff.
4. Patient education/engagement: Provide standardized education to all patients on infectionprevention topics including vascular accesscare, hand hygiene, risks related to catheter use, recognizingsigns of infection, and instructions for access management when away from the dialysis unit.
5. Staff education and competency: Provide regular training of staff on infection control topics,including accesscare and aseptic technique. Perform competency evaluation for skills such as cathetercare and accessing at least every 6-12 months and upon hire.6. Catheter reduction: Incorporate efforts (e.g., through patient education, vascular accesscoordinator)to reduce catheters by identifying barriers to permanent vascular access placement and catheterremoval.
Vol. 14 November 2012 II

-------------------------------------------------------Pulse
Paper Publications / Presentations / Achievements
Department of Pediatrics
Publication:
Topic: Herpes zoster in a healthy immunocompetent two year old childAuthors: Dr. Sangeeta P. Sawant, Dr. Alpa Amin, Dr. Santosh Kumar
Journal: Pediatric Infectious Disease, Journal of The Indian Academy of Pediatrics Infectious diseaseChapter, 2012. Vol: 4, No.1. Pg.13-14.
Department of Obstetrics and Gynaecology
Ach ievements:
• Dr. Amrita Misri, Head of Unit and in-charge Surgical Services, was conferred Fellowship byIndian College of Obstetricians & Gynaecologists (FICOG) at 55th All India Congress, Banarason January 29, 2012.
Paper Presentations
• Title: Role of pelvic organ prolapse quantification system in uterovaginal prolapseAuthors: Dr. N. Mishra, Dr. Misri, Dr. Joshi, Dr. S. Prabhu, Dr. V. Jadhav.
Presented by: Dr. Nigamanada MishraVenue: 55th All India Congress, Banaras.Date: 28-29 January 2012.
• Title: Diagnostic Accuracy of Hysteroscopy in evaluation of PM bleedingAuthors: Dr. Shilpa Singh, Dr. Bahadur Rao, Dr. N. Mishra, Dr. D.P. Joshi, Dr. S.R. Prabhu, Dr.
Amrita MisriPresented by: Dr. Shilpa Singh (DNB student)Venue: 40th Annual Conference of Mumbai Obstetrics & Gynecological Society, Juhu.Date: January 7-8, 2012.
• Paper bagged Ashok Mehra Endoscopy Prize.
• Title: Role of Hysteroscopy in evaluation of Post menopausal bleedingAuthors: Dr. Shilpa Singh, Dr. Bahadur Rao, Dr. N. Mishra, Dr. D.P. Joshi, Dr. S.R. Prabhu,Dr. Amrita Misri
Presented by: Dr. Shilpa Singh (DNB student)Venue: "The Prize Symposium celebrating the Talent within" by MOGS held at Masina
Hospital, Mumbai.Date: 19th February, 2012.
II Vol. 14 November 2012

<
Clinical Meetings Conducted at BARC HospitalJanuary 2012 - October 2012
DATE Department TOPIC
January 27, 2012 Gynaecology & Obstetrics Role of hysteroscopy in evaluation of postmenopausal bleeding
February 10, 2012 Medicine Tuberculosis: Management Dilemma
February 24, 2012 Surgical Good Prescription Practices in Gastroenterology
March 09, 2012 Pathology Approach to Diagnosis of Multiple Myeloma
April 13, 2012 Radiology Interesting Cases1. Renal Artery Stenosis
2. Acrania
April 27, 2012 Paediatrics Common Dermatological Problems in Childhood
May 11, 2012 Vashi Dispensary 1. Case of breast carcinoma in male patient
2. Case of alopecia universalis in female patient
May 18, 2012 Medicine Cardiology
May 25,2012 Psychiatry Eating Disorders
June 08, 2012 ENT Cochlear Implants - our experience
June 22, 2012 Opthalmology LASIK
July 06, 2012 Medicine ABC of Sleep Disorders
July 13, 2012 Anaesthesia Acute Pain Management
July 20, 2012 NPCIL 1. Radiation: Part of our life
2. Relationship of Cancer and Radiation
3. NPCIL Emloyees' Health Profile
July 27, 2012 Gynaecology & Obstetrics Pregnancy Hypertension
August 10, 2012 Orthopedics Surgical Management of Rheumatoid-Deformities
August 24, 2012 Mandala Dispensary Study of Anaemia at mandala Dispensary
September 14, 2012 Medical Final Evaluation of Jaundice
September28, 2012 Surgical Breast Cancer Screening in CHSS women
Octomber 12, 2012 Psychiatry Conversion Disorder

Chief Editor
Dr. Amrita MisriHead, Obstetrics and Gynaecology and In-Charge, Surgical Services
Medical Division, BARC Hospital
Anushaktinagar, Mumbai - 400 094.
Published by:
Head, Scientific Information Resource Division
Bhabha Atomic research Centre, Trombay, Mumbai - 400 085.