Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:737-743
Magnetic resonance imaging in clinically isolatedlesions of the brain stemIEC ORMEROD, A BRONSTEIN, P RUDGE, G JOHNSON, D MACMANUS,AM HALLIDAY, H BARRATT, EPGH DU BOULAY, BE KENDAL, IF MOSELEY,SJ JONES, A KRISS, E PERINGER
From the National Hospitalfor Nervous Diseases and the Institute ofNeurology, Queen Square, London, UK
SUMMARY Twenty-seven patients with an isolated brain stem syndrome, thought to be due todemyelination, were examined by magnetic resonance imaging (MRI). A brain stem lesion wasidentified in 25, and clinically silent lesions outside the brain stem were demonstrated in 20. MRIwas more sensitive than evoked potentials in detecting brain stem and other lesions. The scanfindings were compared with those in 23 patients with multiple sclerosis, who had chronic brainstem dysfunction, with particular reference to the distribution of abnormalities and the MRI char-acteristics of the lesions. The relaxation times, T1 and T2, of the lesions were measured by MRI.These values were seen to fall in serial studies of acute lesions, but remained unchanged in thechronic lesions. MRI may therefore allow the age of lesions to be assessed.
Disturbance of brain stem function is frequentlyfound in patients with multiple sclerosis and may bethe presenting symptom.' However, it is not knownwhat proportion of patients presenting with an iso-lated episode of brain stem dysfunction will ulti-mately prove to have multiple sclerosis. Evokedpotentials and x ray computed tomography (CT)have been of limited value in detecting evidence ofmultiple lesions and examination of the cerebrospinalfluid (CSF) does not consistently show an immu-nological abnormality in the central nervous system(CNS) of such patients. Since MRI is a sensitivemethod for detecting plaques in the CNS in patientswith known multiple sclerosis,2 we have studied anumber of patients presenting with signs of brainstem dysfunction and compared the abnormalitiesfound on MRI with those in patients who have clini-cally definite multiple sclerosis and a similar brainstem disturbance.The aim of the study was fourfold. Firstly, to deter-
mine the sensitivity of MRI in identifying lesions
Address for reprint requests: Dr IEC Ormnerod, UniversityDepartment of Clinical Neurology, The National Hospital forNervous Diseases, Queen Square, London WCIN 3BG, UK
Received 3 September 1985.Accepted 16 October 1985
within the brain stem. Secondly, to compare the sitesof the lesions visualised by MRI with the site of dam-age suggested by neurological and neuro-otologicalexamination. Thirdly, to establish the incidence ofclinically unsuspected lesions in parts of the brainother than the brain stem detected by MRI, and tocompare these findings with the results of evokedpotential studies and the examination of the CSF.Fourthly, to study the natural history of the brainstem lesions with particular reference to the changesin MRI parameters.
Methods
I SubjectsThirty patients (aged 17 years to 49 years, mean 27-9 years),in whom there was evidence of isolated brain stem dys-function, were examined. None had a history of neurologicaldysfunction prior to the development of brain stem symp-toms. Subjects aged over 50 years and those with evidence ofvascular disease were excluded. In all patients a diagnosis ofmultiple sclerosis was thought to be possible by the referringneurologist. In addition, 23 patients (aged 24 years to 58years, mean 36 years) with clinically definite multiple sclero-sis were scanned. All had long-standing evidence of brainstem dysfunction. A third group of 50 neurologically normalcontrol subjects (aged 18 years to 60 years, mean 42 years)was also studied. Examinations performed were approvedby the Ethics Committee of The National Hospitals, QueenSquare and Maida Vale and conformed to the guidelines ofThe National Radiological Protection Board.
737
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

Table I The abnormalities ofevokedpotentials and CSF in patients with clinically isolated brain stem lesions. The patientswere divided on the basis ofthe duration oftheir symptoms. Group I with symptomsfor less than 3 months and Group II withsymptomsfor 9 months or more
VEP AEP SEP CSFoligoclonal
(N = 17) (N = 17) (N = 16) (N = 15)Group INormal 14 14 14 9Abnormal 3 3 2 6
Group II (N = 10) (N = 9) (N = 8) (N = 7)Normal 3 6 6 4Abnormal 7 3 2 3
2 MRIAll the patients studied underwent MRI examination. Thiswas performed with a 0 5 T Picker imaging system (a fewinitial studies were done at 0 25 T), studying protons. Multi-slice imaging protocols were used with inversion recovery
(IR) and spin echo (SE) sequences for the axial scans andadditional sagittal slices were made in most patients. Inmany individuals computer reformatted images of the relax-ation time constants, T, and T2, were made and mea-
surements of these values were taken from both normalbrain stem and from the lesions. The scans were assessedblind by a panel of independent assessors.
3 Neurological assessmentAll patients were examined clinically including assessment ofeye movements, gait and balance. In addition, a full neuro-otological assessment was carried out in those patients withisolated brain stem lesions and in those with definite multiplesclerosis who had brain stem lesions. The latter comprised:(a) DC ENG recording from each eye. Saccadic velocitieswere determined for 300 movements in the horizontal plane.Pursuit was studied in the horizontal plane for target dis-placements of 300 at frequencies of 0-1 to 2 Hz. Nystagmuswas sought in the light and dark in the primary position ofgaze and on displacement of the eye 300 to the left and rightin the horizontal plane or vertically. (b) Opto-kinetic nys-tagmus was assessed using a small rotating drum in the hor-izontal and vertical planes and a full field stimulation in thehorizontal plane. (c) Vestibular function was assessed withbinaural, bi-thermal caloric testing, sinusoidal oscillationsand impulsive rotation in the horizontal plane. The effect offixation was determined for all three methods of inducingthe vestibulo-ocular reflex. (d) Positional nystagmus waselicited by the Hallpike manoeuvre. (e) Pure tone audiome-try and stapedius reflex recording (both ipsi- and contra-laterally).
4 Evoked potential examinationVisual (VEP), auditory (AEP), and median and posteriortibial somatosensory (SEP) evoked potentials were recordedin the majority of subjects in the patient groups (clinicallyisolated lesions of the brain stem and clinically definite mul-tiple sclerosis with brain stem dysfunction). The exam-inations were performed without prior knowledge of theMRI findings and the methods conformed to those pre-viously described.3
5 CSFIn the majority of subjects in the patient groups the CSF wasexamined for the presence of oligoclonal bands.
Results
I MRI, CSF and evoked potentialsThirty patients were examined in whom the diagnosisof a clinically isolated brain stem lesion was made onthe basis of a combination of long tract and brainstem signs, the presence of nystagmus of central ori-gin or an internuclear ophthalmoplegia. Although thediagnosis of demyelination was raised in all patientsof this group at presentation, three patients wereproved to have an alternative diagnosis: one brainstem glioma, one brain stem angioma and one pon-tine haemorrhage. In the remaining 27 patients theage range was 21 to 49 years (mean 315 years), andthe duration of symptoms was 1 week to 12 years(mean 74 weeks). These 27 fell into two clear sub-groups in terms of the duration of their symptoms;group I, with symptoms for less than 3 months andgroup II, with symptoms in excess of 9 months.
Table 2 The incidence and distribution ofMRI abnormalities in patients with multiple sclerosis and those with a clinicallyisolated presentation (Group I, II)
Brain stem Cerebellar Only P Only DC P + DC Any cerebralabnormalities
GroupI(N = 17) 15 2 4 1 8 13GroupII(N= 10) 10 2 1 0 6 7Multiple sclerosis (N = 23) 21 8 2 0 21 23P = Periventricular lesions.DC = Discrete cerebral white matter lesions.
Ormerod, Bronstein, Rudge et al738
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

Magnetic resonance imaging in clinically isolated lesions of the brain stem
Fig 1 An inversion recovery image in a patient with anisolated VI nerve palsy. The lesion (arrowed) is deeply sited,presumably involving the VI nervefibres.Group I There were 17 patients within this group;the age range was 21 to 48 years (mean 29-8 years)and the duration of symptoms was between one weekand 3 months (mean 3-6 weeks). Full evoked potentialstudies were performed in all but one patient who didnot have SEPs. CSF was examined in all but twopatients. The VEPs were abnormal in three patientsindicating a lesion remote from the brain stem and an
Fig 3 Inversion recovery images. The sagittal (a), and axial(b) cuts demonstrate the lesion (arrowed) extending into theponsfrom thefloor ofthefourth ventricle. The patient hadbilateral VIIpalsies and a horizontal gaze palsy.
oligoclonal pattern was found in the CSF in sixpatients (table 1). Only three patients had an abnor-mal AEP and in two the SEP was abnormal; theseabnormalities could have been due to a single brainstem lesion and did not help to clarify the diagnosis.Two of the 17 patients in this group had normal MRIscans of the brain stem; one of these had evidence ofperiventricular lesions in the supra-tentorial sections.Neither of these two patients had abnormal evokedpotentials. In all, 13 of the 17 patients showed abnor-malities outside the brain stem (table 2). In the twopatients with a single lesion in the brain stem but noother lesions supra-tentorially detected by MRI, onehad an oligoclonal CSF and one an abnormal VEP.Group II This group comprised 10 patients (aged 22to 49 years, mean 31-8 years) in whom demyelinationof the brain stem was suspected although symptomshad been present for 9 months or longer. Theduration of brain stem symptoms ranged from 9months to 12 years (mean 46-5 months). All thepatients had evidence of brain stem lesions on theirscans (table 2). Eight patients had a full set of evokedpotential studies; in four either the AEP, the SEP, orboth indicated a lesion in the brain stem (table 1). Inseven patients MRI showed lesions outside the brain
Right eye
R30"
Left eye
Fig 2 A spin echo image in a patient with a VII nerve palsy.The laterally placed lesion (arrowed) is presumed to havedamaged the VII nervefibres.
Fig 4 ENG in a patient with bilateral internuclearophthalmoplegia (the MRI is shown in Figure 5). There isfailure ofadduction ofboth left (A) and right (B) eyes.
739
(
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

740
V.
Fig 5 Axial scans in a patient with a bilateral internuclearophthalmoplegia. The lesion is seen on thefloor ofthefourthventricle on the spin echo (a), inversion recovery (b), T1 (c)and T2 (d) images.
stem and in six of these the VEPs were also abnormal.In one patient where the MRI failed to reveal addi-tional, subclinical, abnormalities the VEP was abnor-mal. In seven patients the CSF was examined andoligoclonal bands were demonstrated in three, all of
Ormerod, Bronstein, Rudge et alwhom had MRI evidence of cerebral lesions.Normal control subjects Of the 50 subjects in thisgroup, three had abnormalities on MRI; in two therewere a small number of discrete lesions within thecerebral white matter; in the third there were wide-spread lesions indistinguishable from those seen indefinite multiple sclerosis. There was nevertheless ahighly significant difference (p < 0 001, chi square)between the cerebral MRI changes in patients ofgroups I and II and the controls.
2 Correlation ofsite of the MRI lesion in the brainstem andphysical signsfor groups Iand IIThere was a good correlation between the presence ofa VI nerve palsy and the lesion seen on the MRI scanwhich was either in the floor of the 4th ventricle ordeeper in the pons, presumably involving the nucleusof the VI nerve or its fibres respectively (fig 1). Alesion was seen in one of these sites in all six patientswith a VI nerve palsy. Similarly, in all of the eightpatients with VII nerve palsies lesions were seen at anappropriate site within the brain stem, including thethree with bilateral VII palsies. In the cases with clini-cal evidence of an isolated VII palsy the MRI lesionswere more lateral in the region where the VII nervefibres pass laterally (fig 2).
Horizontal gaze palsies were present in threepatients and in each case lesions were visualised in anarea of the brain stem which could have included theparamedian pontine reticular formation (PPRF), anarea thought to be responsible for the generation ofsaccades.A combination of these three clinical abnormalities
was not infrequently seen. Three patients had com-bined VI and VII nerve lesions. Another patient had
Fig 6 Axial spin echo images, at 2 levels through the lateral ventricles, showing clinically unsuspected lesions (arrowed) in apatient with an acute clinical brain stem lesion (a, b). Comparable sections (c) in a patient with clinically definite multiplesclerosis show similar but more extensive lesions.
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

Magnetic resonance imaging in clinically isolated lesions of the brain stem
ing from the floor of the IV ventricle into the pons (fig° o 3), presumably involving the VII nerve fibres at the
0° genu, as well as the PPRF or the part of the VI nervenucleus concerned with conjugate horizontal gaze.
0 An internuclear ophthalmoplegia was seen in sevencases five of which were bilateral (fig 4) and the areaof the medial longitudinal fasciculus (MLF) wasinvolved in five cases (fig 5). However in one patiento with an internuclear ophthalmoplegia no lesion was
0 o apparent in the brain stem on MRI and in anotherthere were so many lesions that no anatomical local-isation was possible.
* * Four of the six patients with upbeat nystagmus had0.0*a lesion in the floor ofthe IV ventricle, a site known to
*a*[o Acute | be associated with this abnormality;4 in two other* * Chronic patients with this sign, there was a solitary lesion in. Chronic the medulla in one and no lesion was apparent in the
-J~* *.- other. All nine patients with abnormalities of the sta-* pedius reflex had pontine lesions. There was no con-
500 . 700 goo ' 1100 ' 1300 sistent site of lesions in patients who had pursuitT900ms 1100 13 defects, including unilateral pursuit abnormality, or
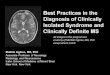
Ti1 /ms caloric dysfunction.Fig 7 A scatter plot ofT1 versus T2for acute and chronicbrain stem lesions. There is little overlap between the twogroups. The mean and standard deviations are shown ofTand T2for normal brain stemfrom the control subjects.
a complete horizontal gaze palsy together with bilat-eral VII palsies; the MRI lesion was midline, extend-
130-
0
0
--SD
0 5 10Time (weeks)
3 Comparison oflesions seen on MRI in Groups Iand II andpatients with definite multiple sclerosisThere was remarkable similarity in the distribution ofthe brain stem lesions between the patients whopresented with clinically isolated lesions and thepatients with multiple sclerosis. The floor of the IVventricle and cerebral aqueduct were the most fre-
1300-
1100-
.E 900-
7-
700-
15 20
0 0 E
_a_ -~0
0 5 10
Tirme (weeks)15 20
Fig 8 A plot of T1 ofacute brain stem lesions against timefrom the onset ofbrain stem symptoms. Serial measurementsfrom the same lesion arejoined together. The mean (M) andstandard deviation (SD) ofthe T1 values ofthe chroniclesions are shownfor comparison.
Fig 9 A plot of T2 ofacute brain stem lesions against timefrom the onset ofbrain stem symptoms. Serial measurementsfrom the same lesion arejoined together. The mean (M) andstandard deviation (SD) of the T2 values ofthe chroniclesions are shownfor comparison.
250
225
200
E 175EI-
150-
125-
100-
741
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

742quent sites for the lesions. Of the 25 patients withMRI evidence of clinically isolated brain stem lesions,10 had a lesion in one of these sites compared with 18of 21 patients in the group of clinically definite multi-ple sclerosis. In the supra-tentorial cuts changes wereagain most frequently seen around the ventricles inboth the patients with clinically isolated lesions andwith clinically definite multiple sclerosis. Peri-ventricular changes were seen in all 23 patients withmultiple sclerosis and in 19 of the 27 (70%) patientswith clinically isolated brain stem lesions (table 2).These changes were of similar distribution in thesetwo groups although the abnormalities seen inpatients presenting with clinically isolated lesionswere less extensive than those seen in patients withestablished multiple sclerosis (fig 6).
4 Evolution of the brain stem lesionsContrast in the MR images is multi-parametric and ismainly dependent on the proton density and therelaxation times T1 and T2.5 We thereforereformatted the images to produce computed imagesofT1 and T2, as observations of intensity alone wouldnot allow the contribution of these parameters to thesignal intensity to be assessed. Measurements takenof the brain stem lesions showed that the acute lesionsusually had elevated T1 and T2 values relative tothose seen in the chronic brain stem lesions (fig 7),which were in turn higher than those recorded fromthe normal brain stem in our control group. Onfollow-up examination the MR characteristics of theacute lesions were seen to fall towards those seen inthe chronic lesions (figs 8, 9). T1 and T2 of the chroniclesions showed no significant change over a 3 monthperiod.
Discussion
Until the early 1970s methods of diagnosing multiplesclerosis depended upon the clinical demonstration oftwo or more lesions in the central nervous system in apatient with symptoms for 1 year or more, in whomthere was a relapsing and remitting course and whereno other cause was found to account for their disabil-ity.6 Since then evoked potential methods have beendeveloped which may demonstrate clinically silentlesions and most neurologists now utilise these meth-ods to assist in the diagnosis of multiple sclerosis. Thepresence of oligoclonal bands in the CSF is character-istic of multiple sclerosis and some diagnosticclassifications7 include these and evoked potentialabnormalities in assessing the certainty of the diagno-sis. However, neither the evoked potential abnormal-ities, nor those of the CSF are specific to multiplesclerosis. Imaging of the cerebral hemispheres andbrain stem, by conventional CT scanning, has been
Ormerod, Bronstein, Rudge et aldisappointing in multiple sclerosis even using highdose contrast enhancement in an attempt to localiselesions where the blood brain barrier is defective.8MRI was first reported to be of value in detectingplaques in the brain in 1981,8 9 an observation whichhas been confirmed by other groups2 10 and thisstudy.Of more clinical concern, however, is the patient
who presents with an isolated lesion in his first epi-sode. Patients presenting with optic neuritis have ahigh chance of developing multiple sclerosis duringtheir lifetime and many studies have followed largegroups of such patients.11 On the other hand, patientspresenting with isolated brain stem lesions have notbeen followed systematically to determine whetherthey subsequently develop the disease. The fewfollow-up data that are available suggest thatpatients, for example with VI nerve palsies, have asmall risk of subsequently developing multiple sclero-sis.12
In this study we found a high proportion of ourpatients have MRI changes in the brain similar tothose seen in established multiple sclerosis. It isimportant to note that our patients were highlyselected and cannot be taken as representative of thegeneral population developing isolated cranial nervepalsies, in that they have already been referred to aneurological institute because a neurologist thoughtthe lesion was most likely to be central. This auto-matically excludes a large number of patientspresenting to a general physician with, for example,VI or VII nerve palsies or nystagmus. Be that as itmay, in this study evoked potential studies were oflimited value in detecting remote lesions in patientspresenting acutely although rather better in thosewho have had their disorder for a number of years.CSF examination was abnormal in a higher propor-tion of acute lesions but the presence of oligoclonalbands is not specific to multiple sclerosis. In contrastto this, MRI detected multiple lesions in the brain inover 70% of patients and demonstrated the lesion inthe brain stem in all but three cases. The questionarises as to the specificity of these lesions. Althoughlesions of similar appearance can be seen in patientswith vascular disease, especially over the age of 50years,13 we tentatively suggest that in the presentstudy multiple sclerosis is the most likely diagnosis. Incomparing the scans of the patients with clinically iso-lated brain stem lesions and those with establishedmultiple sclerosis there are striking similarities. Inparticular the periventricular lesions which are socharacteristic of the disease from pathologicalstudies"4 were seen in both groups of patients, theoccipital horns and trigones being most frequentlyinvolved. Similarly, the discrete white matter lesionswere indistinguishable. These findings support the
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from

Magnetic resonance imaging in clinically isolated lesions of the brain stem
concept that many of the patients with apparently iso-lated lesions have multiple sclerosis. Proof must awaitlong term follow-up.
If, as seems probable, an estimate of the age oflesions can be made from their T1 and T2 character-istics, it may be possible to determine the time-courseof the cerebral and brain stem abnormalities, anddetermine whether all lesions are accrued simulta-neously in a patient. The origin of the increased T1and T2 of the lesions is not fully established. Oedemaprobably contributes in the acute phase and resolu-tion of oedema and inflammation is the presumedmechanism of the fall in T1 and T2 to values seen inchronic lesions where replacement of myelin by glialfibres is the most prominent histological change.There is evidence that the protons of myelin do notcontribute to the signal obtained from normalbrain"314 and the MR characteristics of chroniclesions are thought to be due to an increase in water,compared with normal white matter, and an alteredphysicochemical environment.The prognostic implications of the cerebral abnor-
malities seen in patients with isolated lesions are not,as yet, determined and it is not possible to make adiagnosis of multiple sclerosis on the basis of dissem-inated lesions on MRI in a patient with a single clin-ical episode. If multiple lesions of different ages weredemonstrated in a patient there would be grounds forassuming that the neurological illness was notmonophasic. Such a finding would suggest a diseasewhich was still active and in which lesions were accu-mulated over a longer period of time, a processknown to occur in multiple sclerosis. The diagnosis ofmultiple sclerosis remains essentially clinical anddemyelinating lesions within the CNS without clinicalsequelae are not sufficient grounds on which to basethe diagnosis. Long term follow-up relating MRIchanges to eventual clinical outcome will reveal thesignificance of such abnormalities. Our results arepart of a prospective study which we hope will resolvethese unanswered problems.
The MRI facility was established by the MultipleSclerosis Society and is also supported by the MedicalResearch Council. We thank Margaret Henry for her
secretarial assistance.
References
Matthews WB, Acheson ED, Batchelor JR, Weller RO.McAlpine's Multiple Sclerosis. Edinburgh, ChurchillLivingstone, 1985.
2 Runge VM, Price AC, Kirshner HS, Allen JH, Partain CL,James AE. Magnetic resonance imagine of multiplesclerosis: a study of pulse-technique efficiency. AJR1984;143:1015-26.
3 Halliday AM, ed. Evoked Potentials in Clinical Testing.Edinburgh, Churchill Livingstone, 1982.
'Fisher A, Gresty M, Chambers B, et al. Primary positionupbeating nystagmus. Brain 1985;106:949-64.
1 Young IR, Bailes DR, Burl M, et al. Initial clinical evalu-ation of a whole body nuclear magnetic resonance(N.M.R.) tomography. J Comp Assist Tomog.1982;6:1-18.
6 McDonald WI, Halliday AM. Diagnosis and classificationof multiple sclerosis. Br Med Bull 1977;33:4-8.
7 Poser CM, Paty DW, Scheinberg L, et al. New diagnosticcriteria for multiple sclerosis: guide lines for researchprotocols. Ann Neurol 1983;13:227-31.
8 Vinuela FV, Fox AJ, Debrun GM, Feasby TE, Ebers GC.New perspectives in computed tomography of multiplesclerosis. AJR 1982;139:123-7.
9Young IR, Pallis CA, Bydder GM, Hall AS, Legg NJ,Steiner RE. Nuclear magnetic resonance imaging inmultiple sclerosis. Lancet 1981 ;ii:1063-6.
Lukes SA, Crooks LE, Aminoff MJ, et al. Nuclear mag-netic resonance imaging in multiple sclerosis. Ann Neu-rol 1983;13:592-601.
l Hutchinson WM. Acute optic neuritis and the prognosisfor multiple sclerosis. J Neurol Neurosurg Psychiatry1976;39:283-9.
12 JA, Younge BR. Paralysis of cranial nerves III, IVand VI. Arch Ophthalmol 1981;99:76-9.
13Ormerod IEC, Roberts RC, du Boulay EPGH, et al.NMR in multiple sclerosis and cerebral vascular dis-ease. Lancet 1984;ii:1334.
14Lumsden CE. The neuropathology of multiple sclerosis.In: Vinken PJ, Bruyn GW, eds. Handbook of ClinicalNeurology, vol 9. Amsterdam: North Holland, 217-9.
15Bottomley PA, Hart HR, Edelstein WA, et al. Normalhuman brain studied by magnetic resonance at 1-5Tesla. Radiology 1984;150:441-6.
16 Pykett IL, Rosen B. Nuclear magnetic resonance: in vivoproton chemical shift imaging. Radiology 1983;149:197-201.
743
Protected by copyright.
on Septem
ber 8, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.49.7.737 on 1 July 1986. D
ownloaded from