Embed Size (px)
Citation preview

Maciej Jędrzejczyk MD, PhD
Department of Diagnostic Imaging,
2nd Division of Warsaw Medical Univeristy

Introduction to chest radiology
Chest X-ray anatomy
A litle bit of CT and PET
Common general findings
Common pathologies
US – is it useful?
Summary

Imaging methods
- Chest X-Ray (CXR) - Computed Tomography (CT)
- Ultrasound (US) - Scintygraphy (SC) - Positron Emission Tompgraphy (PET) - Magnetic Resonance (MR)

David A. Lisle „Imaging for students”
4th Edition (2012)
www.radiologyassistant.nl

Density:
- Air
- Fat
- Soft tissue
- Bone

How to do it?
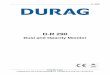
Stator
Rotor
Anode (+)
Cathode (-)

Symetrical and stright localization
of clavicular heads
and spinous processes are
demonstrating a diagnostic
image.
How to do it – patient positioning

How to do it – patient positioning
The patient should be examined at the moment of full inspiration (holding breath). The diaphragm contour should be at the level of the 8th to 10th rib (posterior part ) or 5th to 6th (anterior part).

Negative or positive
Parameter settings:
- high mA to reduce exposure time
- high mA, low kVp for high image contrast
- high kVp for increased photon penetration
NEGATIVE POSITIVE OVERP. UNDERP.

Chest anatomy A-P projection
- Respiratory tract
- Gastrointestinal tract
- Heart and vessels
- Bones
- Muscles
- Others



On the PA chest-film it is important
to examine all the areas where the
lung borders the diaphragm, the
heart and other mediastinal
structures.
These lines and silhouettes are
useful localizers of disease,
because they can be displaced or
obscured with loss of the normal
silhouette.

On a chest film only the outer contours of the heart
are seen.
However it can be helpful to know where the different
compartments are situated.
Left Atrium
Most posterior structure.
Left atrial appendage (in purple) can sometimes be
seen as a small outpouching just below the
pulmonary trunk.
Right Atrium
Receives blood from the inferior and superior vena
cava.
Left Ventricle
Situated to the left and posteriorly to the right
ventricle.
Right Ventricle
Most anterior structure and is situated behind the
sternum.

Chest anatomy lateral projection

Chest anatomy lateral projection
On a normal lateral view the contours of the heart are visible
and the IVC is seen entering the right atrium.
The retrosternal space should be radiolucent.
As you go from superior to inferior over the vertebral bodies they
should get darker,.
The contours of the left and right diaphragm should be visible.
However the left diaphragm can only be seen to a point where it
borders the heart .

Chest anatomy lateral projection
Left Atrium
The upper posterior border of the
heart is formed by the left atrium.
Left Ventricle
Forms the lower posterior border.
Right Ventricle
The lower retrosternal space is
filled by the right ventricle.

Heart dimension (HD<1/2ThD)

The left pulmonary artery runs over the left main
bronchus, while the right one runs in front of the right
main bronchus.
Hence the left hilum is higher than the right.
Both pulmonary arteries and veins can be identified on
a lateral view and should not be mistaken for
lymphadenopathy.
The lower lobe pulmonary arteries extend inferiorly from
the hilum.
They are described as little fingers, because each has
the size of a little finger.
Pulmonary vesels

The mediastinum can be divided into an anterior,
middle and posterior compartment, each with it's
own pathology.
Mediastinal lines
Mediastinal lines or stripes are interfaces
between the soft tissue of mediastinal structures
and the lung.
Displacement of these lines is helpful in finding
mediastinal pathology.
Mediastinum

Superior and inferior
mediastinum
Mediastinum

Hiatal hernia
Mediastinum enlargment

Mediastinum - enlargement
Lympadenopathy - PET

Hilar enlargement
Enlargement of the hili is usually due
to lymphadenopathy or enlarged
vessels.

1. Lymphadenopathy and groundglass
appearance of the lungs.
2. Bilatral lymphadenopathy.
3. Bulky lymphadenopathy.
4. 1-2-3 sign.
5. Nodular lung pattern, no
lymphadenopathy.
6. Hilar and paratracheal
lymphadenopathy.
Hilar enlargement

Lung fissures

Lung fissures

The right lung lobes

The right lung lobes

The right lung lobes

The left lung lobes

The left lung lobes

Bones – how to count the ribs?

What is important?

What is important?
Stuctures – leadpoints:
- heart position,
- contour of diagphragms,
- liver shadow,
- gas bubbles,
- hila positions,
- aorta contour.

How to read it?

How to read it?
Lung parenchyma

What is important?
Hidden areas
There are some areas that need
special attention, because pathology
in these localizations can easily be
overlooked:
- apical zones
- hilar zones
- retrocardial zone
- zone below the dome of diaphragm
These areas are also known as the
hidden areas.

Here is an example of
a large lesion in the
right lower lobe, which
is difficult to detect on
the PA-film, unless
when you give special
attention to the
hidden areas.

Notice the subtle
increased density in the
area behind the heart
that needs special
attention (red arrow).
This was a lower lobe
pneumonia.

Anatomical variant
Vena azygos lobe
A common normal variant is the
azygos lobe.
The azygos lobe is created when
a laterally displaced azygos vein
makes a deep fissure in the upper
part of the lung.
On a chest film it is seen as a fine
line that crosses the apex of the
right lung.

Anatomical variant?

Technique

mAs
kVp
slice thickness
(beam collimation)
pitch (table speed per
gantry rotation/beam
collimation)

Native CT
Contrast enhanced CT
CT angiography
Perfusion imaging
HRCT
Reconstructions

Pilot

Windows

CE-CT anatomy

Planar reconstructions

HRCT – special technique
dedicated to lung diseases
- narrow slice width is used (usually <1 mm)
- high spatial resolution image
reconstructions algorithms are implemented
- minimized filed of view (not necessery in
modern CT-machines)
- mAs elevated to reduce noise signals
(radiation dose is elevated as well!).

Secondary lobule is the basic anatomic and fuctional
unit of pulmonary structure.
It is the smallest lung unit surrounded by connective
tissue septa and is made up of few pulmonary acini,
that contain the alveoli.
The secondary lobule is supplied by terminal bronchiole
in the center, that is parallelled by the centrilobular
artery.
Pulmonary veins and lymphatics run in the periphery of
the lobule within the interlobular septa.

Centrilobular area is the central part of the secundary
lobule.
It is usually the site of diseases, that enter the lung
through the airways ( i.e. hypersensitivity pneumonitis,
respiratory bronchiolitis, centrilobular emphysema ).
Perilymphatic areas the peripheral part of the
secundary lobule.
It is usually the site of diseases, that are located in the
lymphatics of in the interlobular septa ( i.e. sarcoid,
lymphangitic carcinomatosis, pulmonary edema).

Focal septal thickening in lymphangitic
carcinomatosis and small nodular lesions
(metastasis).

PET = radiology + nuclear medicine

PET – characterization of lesion (ca within
atelectasis).
PET-CT can detect malignancy in
focal pulmonary lesions of
greater than 1 cm with
sensitivity of about 97% and
specificity of 78%.
False-positive findings in the
lung are seen in granulomatous
disease and rheumatoid
disease.
False negatives are seen in low
grade malignant tumors like
carcinoid and alveolar cell
carcinoma and lesions of less
than 1 cm.

PET – monitoring therapy



Lung abnormalities mostly present as
areas of increased density, which can
be divided into the following patterns:
- consolidation,
- atelectasis,
- nodule or mass,
-interstitial changes.
Less frequently areas of decreased
density are seen as in emphysema or
lung cysts.


Consolidation Consolidation is the result of replacement of air in the
alveoli by transudate, pus, blood, cells or other
substances.
The key-findings on the X-ray are:
•ill-defined homogeneous opacity obscuring vessels ,
•silhouette sign - loss of lung/soft tissue interface,
•air-bronchogram,
•extention to the pleura or fissure, but not crossing it,
•no lung volume loss.
Form of consolidation - pattern of distribution:
•diffuse - perihilar (batwing) or peripheral (reversed
batwing),
•lobar or focal.
•multiple - usually multiple ill-defined densities.

Consolidation

Consolidation One must differentiate between acute
consolidation and chronic consolidation!
In chronic disease we think of:
• neoplasm with lobar or segmental post-
obstructive pneumonia,
• chronic post-infection diseases like
organizing pneumonia (OP) or chronic
eosinophilic pneumonia, which both present
with multiple peripheral consolidations,
• in sarcoidosis sometimes the
granulomatous noduli are so small and
diffuse that they can present as
consolidation (veolar sarcoidosis).

Consolidation

Consolidation
Batwing
- bilateral perihilar distribution of
consolidation.
The sparing of the periphery of the lung is
attributed to a better lymphatic drainage in
this area.
It is most typical for pulmonary edema, both
cardiogenic and non-cardiogenic.
Sometimes it is seen in pneumonias.
Reverse Batwing
- peripheral or subpleural consolidation.
It is frequently seen in chronic lung disease.

Consolidation

Silhuette sign
This is a very important sign. It enables us
to find subtle pathology and to locate it
within the chest.
The loss of the normal silhouette of a
structure is called the silhouette sign.

ARDS – diffuse consolidations
(periferal distribution).

Increased lung attenuation is called ground-glass-
opacity (GGO) - hazy increase in lung opacity
without obscuration of underlying vessels.
We deal with consolidation if the increase in lung
opacity obscures the vessels.
In both ground glass and consolidation the
increase in lung density is the result of
replacement of air in the alveoli by fluid, cells or
fibrosis.
In GGO the density of the intrabronchial air
appears darker as the air in the surrounding
alveoli.
This is called the 'dark bronchus' sign
In consolidation, there is exclusively air left
intrabronchial.
This is called the 'air bronchogram'.

Ground-glass opacity
- Is due to filling of the alveolar spaces with pus,
edema, hemorrhage, inflammation or tumor cells.
- as well as thickening of the interstitium or
alveolar walls below the spatial resolution of the
HRCT as seen in fibrosis.
So it either be the result of air space disease
(filling of the alveoli) or interstitial lung disease
(i.e. fibrosis).
The location of the abnormalities in ground glass
pattern can be helpfull:
- upper zone predominance: respiratory
bronchiolitis, PCP.
- lower zone predominance: UIP, NSIP, DIP.
- centrilobular distribution: hypersensitivity
pneumonitis, respiratory bronchiolitis

Treatable or not treatable?
Ground-glass opacity is nonspecific,
but highly significant finding since 60-80% of
patients with ground-glass opacity on HRCT have
an active and potentially treatable lung disease.
In the other 20-40% of the cases the lung disease
is not treatable and the ground-glass pattern is the
result of fibrosis.

Low Attenuation pattern
Abnormalities that result in decreased
lung attenuation or air-filled lesions:
- emphysema,
- lung cysts (LAM, LIP, Langerhans cell
histiocytosis),
- bronchiectasis,
- honeycombing.
Most diseases with a low attenuation
pattern can be readily distinguished on
the basis of HRCT findings.

Low Attenuation pattern
Upper lung zone preference is seen in:
- inhaled particles: pneumoconiosis (silica
or coal),
- smoking related diseases (centrilobular
emphysema,
- respiratory bronchiolitis (RB-ILD),
- langerhans cell histiocytosis,
- hypersensitivity pneumonitis,
- sarcoidosis.
Lower zone preference is seen in:
- UIP
- aspiration
- pulmonary edema
Central distribution is seen in sarcoidosis and
cardiogenic pulmonary edema.
Peripheral distribution is mainly seen in
cryptogenic organizing pneumonia (COP),
chronic eosinophilic pneumonia and UIP.

Low Attenuation pattern
Emphysema typically presents as areas of
low attenuation without visible walls as a
result of parenchymal destruction.
Centrilobular emphysema - most common
type with irreversible destruction of
alveolar walls in the centrilobular portion of
the lobule (associated with smoking).
Panlobular emphysema - affects the whole
secondary lobule with lower lobe
predominance (alpha-1-antitrypsin
deficiency, and long-last smokers).
Paraseptal emphysema - adjacent to the
pleura and interlobar fissures - isolated
phenomenon in young adults, or in older
patients with centrilobular emphysema.

Interstitial

Interstitial

Interstitial
Interstitial edema usually presents as
reticulation.
A typica l sign are Kerley’s B lines:
1-2 cm long horizontal lines near the
lateral pleura.
The main differential diagnosis of
Kerley B lines is:
- interstitial edema in heart failure,
- lymphangitis carcinomatosa.

Interstitial Most of our knowledge about imaging findings in interstitial lung
disease comes from HRCT.
On HRCT there are four patterns: reticular, nodular, high and low
attenuation.
On a Chest X-Ray it can be very difficult to determine whether there
is interstitial lung disease and what kind of pattern we are dealing
with.
On a CXR the most common pattern is reticular.
The ground-glass pattern is frequently not detected on a chest x-
ray.
The cystic pattern is also difficult to appreciate on a cest x-ray.
When the cysts have thick walls like in Langerhans cell histiocytosis
or honeycombing, it frequently presents as a reticular pattern on a
CXR.

Usual interstitial pneumonia (UIP)
is a form of lung disease characterized
by progressive scarring of both lungs.

Pneumocystis jvr. pneumonia (PCP).

Nodular vs reticular changes.

Atelectasis Atelectasis = lung-collapse
-is the result of loss of air in a lung or part
of the lung with subsequent volume loss
due to airway obstruction or compression
of the lung by pleural fluid or
a pneumothorax.
In many cases atelectasis is the first sign
of a lung cancer!
The key-findings on the CRX are:
• sharply-defined opacity obscuring vessels
without air-bronchogram,
• volume loss resulting in displacement of
diafragm, fissures, hili or mediastinum

Atelectasis Lobar atelectasis
-is an important finding on a chest x-
ray and has a limited differential
diagnosis.
The most common causes of
atelectasis are:
• bronchial carcinoma in smokers,
• mucus plug in patients on
mechanical
ventilation or astmathics (ABPA),
• malpositioned endotracheal tube,
• foreign body in children.
Sometimes lobar atelectasis produces
only mild volume loss due to
overinflation of the other lungparts!

Atelectasis
Right middle lobe atelectasis
Findings:
• blurring of the right heart border
(silhouette sign)
• triangular density on the lateral view
as a result of collapse of the middle
lobe
• usually right middle lobe atelectasis
does not result in noticable elevation
of the right diaphragm.

Atelectasis of RUL

Total atelectasis
Tatelectasis of the right lung due to mucus plugging.
Notice the displacement of the mediastinum to the
right.
Re-aeration on follow-up chest film after treatment
with a suction catheter.
The mediastinum has regained its normal position.

Nodule

Solitary Pulmonary Nodule (SPN) A SPN is defined as a discrete, well-marginated,
rounded opacity less than or equal to 3 cm in
diameter.
It has to be completely surrounded by lung
parenchyma, does not touch the hilum or
mediastinum and is not associated with
adenopathy, atelectasis or pleural effusion.
The differential diagnosis of SPN is basically the
same as of a mass except that the chance of
malignancy increases with the size of the lesion.
Lesions smaller than 3 cm, i.e. SPN's are most
commonly benign granulomas, while lesions
larger than 3 cm are treated as mlignancies.

Nodule
Fleischner Society recommendations for follow-up of nodules
Previous chest radiographs should be reviewed to determine if the lesion has been stable
over 2 years.
If so, no further follow up is necessary, with the exception of pure ground-glass lesions on CT
scans, which can be slower growing.
For lesions with a benign pattern of calcification, further testing is not necessary.
Management of indeterminate lesions greater than 8-10 mm depends on clinical probability of
malignancy, as follows:
Low probability: Serial CT scanning at 3, 6, 12, and 24 months
Intermediate probability: PET-CT, contrast-enhanced CT, transthoracic needle aspiration and/or
transbronchial needle aspiration (TBNA)
High probability: Surgical resection
Any unequivocal growth noted during follow up means that a definitive tissue diagnosis is needed.

Nodule – sign of malignancy

Nodule – sign of malignancy
- Size:
4 - 7mm – 0,9%,
8 – 20mm – 18%,
>20mm – 50%,
>30mm – 75-80%.
- Bronchogram seen- 65% malignant. - Wall thickness (>15 mm), irregular cavitation– 90%. - Contrast enhancement:
>20jH – mal.
<15jH – ben.
- Volume Doubling Time (VDT) - malignant 30-400 days

Multiple lesions Multiple masses
The differential diagnostic list of multiple masses is very
long.
Metastases
Metastases are the most common cause of multiple
pulmonary masses.
Usually they vary in size and are well-defined.
They predominate in the lower lobes and in the
subpleural region.
HRCT will demonstrate the random distribution unlike
other diseases that have a perilymphatic or
centrilobular distribution.

Multiple nodules

Multiple nodules - miliary

Cancer 1. Hilar 2. Nodule 3. Cavity 4. Subpleural 5. Obturative 6. Atelectasis 7. Bronchiectasis 8. Pleural effusion 9. Tumor necrosis 10. Atelectasis and abscess 11. Obturative emphysema 12. Infiltration of mediastinum 13. Pancoast tumor 14. Lymph node involvement 15. Carina infiltration 16. Pericardial infiltration

Cancer

Cancer

Sign of benignity
- large calcifications,
- smooth margins,
- fat,
- spontaneous regression,
- long VDT or stablility over time

Lines and tubes

Lines and tubes and others: endotracheal tube

Lines and tubes and others: peace maker

Heart valves:
- green: pulmonic v.
- blue: aortic v.
- pink: mitral v.
- yellow: tricuspid v.

Heart valves – artificial heart

Heart valves – mitral



Pneumothorax - accumulation of air in the pleural space.
Radiological signs:
Collapse/distortion of the lung
Increase volume of hemithorax
Displacement of mediastiumum
Depressed diaphragm
Increased intercostal space

Pneumomoediastinum and
subcutaneous emphysema

Emphysema

Pneumoperitoneum

Pleural fluid
It takes about 200-300 ml of fluid before it
comes visible on an CXR (figure).
About 5 liters of pleural fluid are present
when there is total opacification of the
hemithorax.

A small right-sided pleural
effusion.

A massive left-sided pleural
effusion.

A loculated (trapped) effusion.


Pleural plaques
They have irregular shapes and do not look like
a lung masses or consolidations.
Some of these opacities are clearly bordering
the chest wall (red arrows).
All these findings indicate that we are dealing
asbestos related pleural plaques:
- bilateral and extensive,
- covering the dome of the diaphragm.

Pleural plaques
Unilateral pleural calcifications are usually
due to:
- infection (TB) ,
- empyema ,
- hemorrhagic .

Mesothelioma


Rib fracture – US is more
sensitive in etection of isolated
rib fracture then CXR.

Atelectasis and air space
consolidation with air
bronchogram of the lower lobe
and pleural effusion.

Empyema with septations
and atelectasis of the lower
lobe on the right side and
atelectasis of the left lower
lobe and echofree pleural
fluid.

Pulmonary embolism with multiple
non vascularized wedge shaped
hypoechoic pleural based lesions

Lung metastases with multiple
hypoechoic masses

CXR: clinical respiratory symptoms/general
check-up/trauma.
CT: detailed charcterization of CXR findings/
oncological chec-up/detection of mets/
staging of ca/characterization of solitary nodule/
trauma.
PET: characterization of nodule/staging/
onkological check-up.
US: detection and estimation of fluid.
Recently - diagnosis of pneumonia

Heart:
- position, size, configuration.
Pulmonary vessels:
- size, position.
Mediastinum:
- trachea, Ao, SVC, AV.

Hila:
- position, size, density.
Lungs:
- contours, lesions/diffuse changes/opacity.
Pleura:
- effusion, pneumothorax, plaques,
thickening, calcifications.

Bones:
- sternum, ribs, spinal collumn
and others.
Diaphragm:
- position, free gas, hernia.
GIT:
- localisation of gas (stomach
buble, colon).

Breast:
- contours, lesions.
Axilla, neck:
- masses.
Lines, tubes and foregin bodies.

Pulmonary embolism
Tuberculosis
Sarcoidosis
Staphylococcal pneumonia
„Inhalation” diseases f.e. siliconosis