Embed Size (px)
Citation preview

MAARPU - A convergence initiative to improve Health & Nutrition Status of Women & Children
•

Empowering lives through convergence
• Department for Women Development and Child Welfare
• Government of Andhra Pradesh
INTRODUCTION The Govt.of Andhra Pradesh is providing various services related to Health & Nutrition to Mother & Child in the rural and urban areas with a special focus on poor by involving various departments like Medical & Health, ICDS, IKP, PR, RWS, MEPMA etc,.
Each department is working with their own targets on entitlements. Though there is a improvement in the Health & Nutrition status of women & Children, the decline of MMR & IMR and malnutrition is not up to the expected level. There is need to improve significantly, to achieve MMR & IMR reduction as a part of the millennium development goals (MDG).

5
Low Birth Weight Children
% of Children with Low Birth Weight (NFHS - 3, 2005-06)
19.4 18.7 17.2
16.1
21.5
0
5
10
15
20
25
Andhra Pradesh
Karnataka Tamilnadu Kerala India
% of children born with low birth weight in A.P. is
19.4% which is highest among the southern
states

6
52
4551
27
4643
3844
27
3740
3741
2933
INDIA AP KARNATAKA KERALA TAMILNADU
NFHS-1(1992-93) NFHS-2 (1998-99) NFHS-3 (2005-06)
% of Underweight Children under 3 years
There is no improvement in nutrition status of children 0-3 yrs
from NFHS 2 to NFHS 3

The percentage of anaemic pregnant women has increased from 42% to 56%
from 1998- 99 to 2005-06
Malnutrition amongst Women in AP
42
49
57
20
5056
60
53
33
58
Andhra
Pradesh
Karnataka Tamil Nadu Kerala India
NFHS-2 NFHS-3

Maternal Mortality Ratio
• There was a fall of 31% in MMR in AP from 2003 to 2009 due to increase in institutional deliveries
• The aim is to reduce MMR to 70 by end of 12th Plan

71
63
53
12
53 58 57
50
14
37 42 41
35
12
22
INDIA AP KARNATAKA KERALA TAMILNADU
SRS-1997 SRS-2005 SRS-2012
Infant Mortality Rate
• AP has not made much progress in reduction of IMR which is a matter of concern
•The aim is to reduce IMR to 25 by end of 12th Plan

Anaemia: The percentage of anaemic pregnant women has increased from 42% to 56%
from 1998- 99 to 2005-06
Status of Malnutrition amongst Women in A.P.
42
49
57
20
5056
60
53
33
58
Andhra
Pradesh
Karnataka Tamil Nadu Kerala India
NFHS-2 NFHS-3
BMI : The nutritional status among the women in the State shows that more than one-
third of them are below 18.5. Between 1998-99 and 2005-06, there is a marginal decline
of 4% of women who are having BMI below 18.5

Proposed Goals for the State
Parameters Present
Status
MDG
(2015)
12th Plan
(2016-17)
Low-Birth Weight (%) 19.4 -- 10
Under Weight (%) 37 24 20
Anaemia (%) 57 -- 30
IMR (per 1,000 live births) 41 24 25
MMR (per 1,00,000 live births) 134 75 70
Poor Awareness on Government Health & Nutrition Programes among the public
Lack of Public Awareness on Importance of Nutrition /Balanced Diet
Poor Coordination & Convergence with all line Departments to Provide effective health care to the ANCs/PNCs/Children
Strong Myths & Misconceptions among the Public due to Illiteracy, Ignorance
MCH Tracking is not up to the mark & Lack of follow up action
Delay in identification of Highrisk cases and poor ANC checkups Lack of proper planning, Supervision & monitoring of field level health activities by PHC & Higher level supervisory staff.
Identified Challenges in Maternal & Child Health Care

To achieve the above said tasks allied departments like Medical & Health, ICDS, IKP, PR, RWS, MEPMA etc. need to converge through a programme called
“MAARPU”

Evolution of “Maarpu”
• The Chief Secretary held a meeting with the Group of Secretaries, on 16th August 2012 to discuss the way forward to achieve the MDGs • to initiate convergence in service delivery among the
welfare departments
• to develop a behaviour change in the community and the functionaries towards a sustainable demand based and participatory mode
• By leveraging the existing strengths in – Strong institutions of District Collectors
– Self Help Groups & VO
Maarpu 14
Maarpu (Go Ms 249)
• Combine the strengths of all the depts. – Human resources
(Health & ICDS) – Community resources
(ASHAs & SHGs)
• Over arching monitoring and tracking – District Collectors – Cluster Convergence
Officers – SPHOs, CDPO, Area
Coordinators
15
8 Components of “Maarpu”
1. Focused monitoring of 20 key interventions to reduce IMR, MMR & Malnutrition
2. Convergence in service delivery at habitation level
3. Convergent Behavioral change communication (BCC)
4. Monitoring of the 20 Key Interventions
5. Participation of SHG & Village Organizations (Vos)
6. Use of Maternal and Child Protection (MCP) card.
7. Synchronization
8. Administrative structure for convergence

Focus on 20 key interventions and its monitoring
1. Early Registration of Pregnancy 2. Ante Natal Checkups (ANCs) 3. Maternal Nutrition 4. Identification of high-risk pregnancies & ensuring appropriate referral 5. Birth Planning 6. Institutional delivery 7. Early initiation of breastfeeding 8. Exclusive breastfeeding for six months 9. Post Natal Care and Newborn Care 10. Immunization 11. Growth Monitoring 12. Complementary feeding & Child Nutrition 13. Management of ARI & Diarrhoea 14. Strengthening of referral system 15. Family Planning 16. Maternal & Infant Death Reviews 17. Sanitation & Hygiene 18. Age at Marriage 19. Adolescent Girls 20. Gender Sensitization
Convergence Committees for monitoring &
implementing the converging efforts
1. Village Level Convergence Committee
2. PHC Level Meetings
3. Cluster Level Convergence Committee (CLCC)
4. District Level Convergence Committee

The Committees will review
• Progress of Key interventions
• Behavior change in the community
• Service delivery for health care & nutrition
The Committees will meet once in a month

Village Level Convergence Committee Members of the VLCC
• Sarpanch Chairperson • Panchayat Secretary Special Invitee • VRO Special Invitee • SC/ST Women Ward Members Members • Women MPTC/ZPTC/MPP President living in the village Members • President of Village Education Committee Member • ANM Member • AWWs Member • ASHAs Member • VO Chairperson Member-Convener The Committee meeting will be held preferably on every 2nd Tuesday of the month or on 4th Tuesday to enable the ANMs to attend the VLCC meetings.

The agenda for the VLCC meeting
• Action Taken Report of previous meeting.
• Health and Nutrition Services availed by women and children with a focus on registration of all ANCs, follow up of children with Severe Acute Malnourishment (SAM) and underweight children, maternal or infant death.
• Nutrition & Health Days (NHDs 1 and 2)
• Health and Nutrition behavior of the community with focus on preventing child marriage and gender-selective abortions, encouraging deliveries in government institutions and spreading awareness about JSSK benefits.
• Early initiation of breast feeding, exclusive breast feeding for 6 months and complementary feeding from 6 months to 3 years.
• social and other issues like gender sensitization,
• Action plan for the next month.

Roles and Responsibilities of Village Level
Functionaries: ASHA
• Visit all households and sensitize pregnant women and their family members
• Should prepare the list of beneficiaries for ANC, immunization etc. Efforts should be made to bring the people who are missed in previous meetings.Special attention in mobilising SAM children along with their mother and father
AWW
• AWWs will display information about the day fixed for the VLCC at the Gram Panchayat building, AWC etc.
• Prepare the list of beneficiaries for ANC, immunization and other health services. Provide supplementary nutrition to the pregnant and lactating women & children aged 6 months to 6 years.
• Counsel pregnant women, mothers, adolescent girls on health and nutrition.Monitor growth and make a list of under-nourished and SAM children.
Prepare the MAARPU report in Format 6.

Roles and Responsibilities of Village Level Functionaries:
MPHA(F)(ANM) • Shall update the field register. • Shall keep adequate number of Maternal and Child Protection(MCP) cards and issue them to all the pregnant women registered for ANC. • Counsel mothers & family members, especially husbands, about care to be taken during pregnancy. • Inform families about EDD, birth planning, referral services, PNC care etc. • Make a list of high risk pregnancies. • Emphasize the importance of immunization and child health care. • Provide health education to adolescent girls. • Ensure display of IEC/BCC material. Prepare the MAARPU reports in Formats 2 to 5.

Roles and Responsibilities of Village Level Functionaries:
PRI • Gram Panchayat is responsible for: • Chlorination of water sources and cleaning of overhead tanks once in 15 days. • Fixing pipeline leakages and closure of pit taps etc. • Solid and liquid waste management. • Cleaning of street drainages. • Encourage use of sanitary latrines. • The PRIs shall support ASHA and AWW in mobilising the parents of malnourished children, and the husband of each pregnant woman. The Panchayat Secretary may prepare the Maarpu report in Format 7.

Monitoring Formats for the VLCC meeting:
The VLCC will review the issues of health and nutrition services and behavioural change, as per the Monitoring and Reporting Format 1.
For facilitating this review,information will be provided by the ANM in Formats 2 to 5 pertaining to Maternal Health, Child Health, Sick children and mortality, if any; by the Anganwadi Worker in Format 6; by the Panchayat Secretary in Format 7; and by the Village Organisation in Format 8. The ANM may obtain print-outs from MCTS or use her Field Register to provide the information listed in Formats 2 and 3 and need not prepare the Formats separately.
Based on the VLCC review, a report in Format 1 will be submitted by the ANM to the Medical Officer of the PHC.

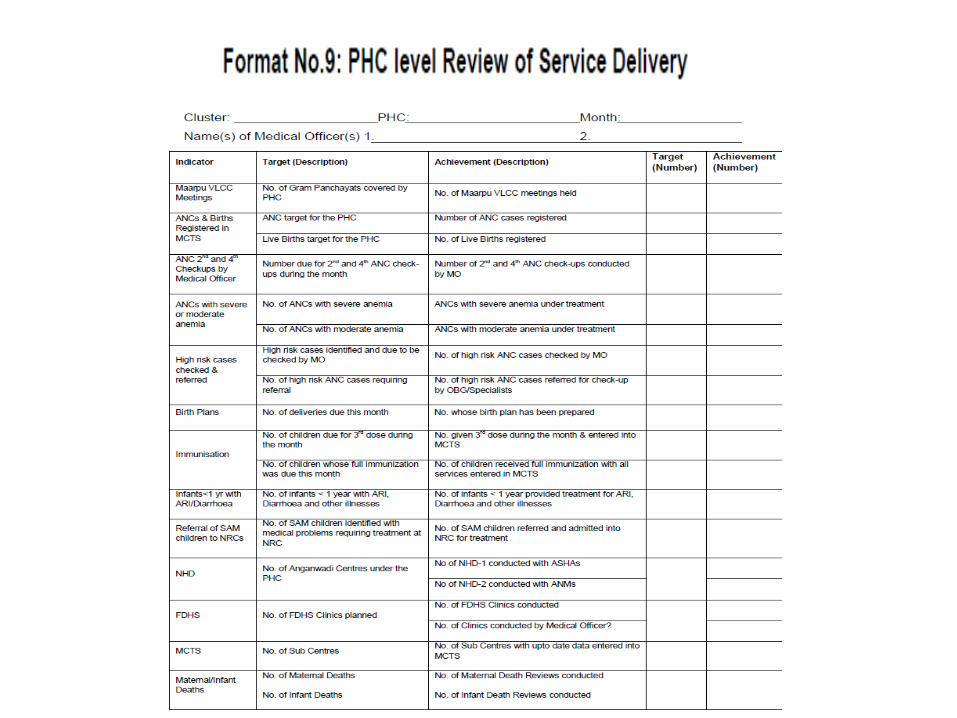
PHC Level Meetings to Review Service Delivery
i. SPHO Chairperson ii. CDPO Vice Chairperson iii. Medical Officer (s) Vice Chairperson iv. Supervisors (ICDS) Member v. CHO/ MPHEO/ PHN /MPHS(M&F) Member vi. AE, RWS Member vii. AE, PR Member viii. APM, IKP Member ix. MPHA (F) (ANM) Member x. ASHA Member xi. AWW Member Monitoring and Reporting Format: The PHC level Monitoring and Reporting Formats may be seen in Part V (Format 9 and 10).

Cluster Level Convergence Committee (CLCC)
This is constituted in each Community Health and Nutrition Cluster
i. Cluster Convergence Officer(nominated by District Collector) Chairperson
ii. Superintendent of Area Hospital /CHC Member
iii. Medical Officers of PHCs in the Cluster Member
iv. Supervisors (ICDS) Member
v. Cluster Coordinators / APM (SERP) Member
vi. Reps of Mandal Mahila Samakhyas Member
vii. SPHO Member Convener
viii. CDPO Member Co-convener
ix. Area Coordinator, IKP Member Co-convener
Monitoring and Reporting Format:The CLCC will consolidate the Format 9 reports on Service Delivery, for all the PHCs in the Cluster. In addition, the CLCC should review the reports of PHCs in Format 10,

District Level Convergence Committee i. District Collector Chairperson ii. Joint Collector Member iii. Cluster Convergence Officers (nom. by District Collector) Member iv. DCHS Member v. Project Officer(RVM) Member vi. CEO(ZP) Member vii. Superintendent Engineer(PR) Member viii. Superintendent Engineer(RWS) Member ix. Representatives of Zilla Mahila Samakhyas Members x. DM&HO Member-Convener xi. Project Director (ICDS) Member-Co-convener


Monitoring and Reporting Format:
The District level Convergence Committee may leverage the following for reviewing the progress and outcomes of Maarpu.
1. Cluster and PHC-wise analysis of MCTS data.
2. Cluster and PHC-wise reports in Format 9.
3. Cluster and PHC-wise report in Format 10.
District level Convergence Committee may consolidate the reports in Formats 9 and 10, and add district-specific issues, strategies and initiatives for submission to the State level Convergence Committee.


Maarpu – Expected Change
• Behavioral Change:
• Change in the role of Community: Recipient mode to Partnership mode
• Service delivery from Programme driven mode to demand driven mode
• Ownership of Public health facilities by the community & Improved health seeking behavior
• Initiate the dialogue on health as priority in the community
• District Collectors involvement:
• Review of 20 interventions at all levels
• Local solutions to address gaps
• Expectation – achieve the goals of NRHM & MDG

Inputs required !, there must be strategies thr’ convergence…..




























