Embed Size (px)
Citation preview

M. JESSUPM. JESSUP
Tenth International Symposium
HEART FAILURE & Co.CARDIOLOGY SCIENCE UPDATE FEMALE DOCTORS SPEAKING
ON FEMALE DISEASES
Milano9 - 10 aprile 2010

Genders and Heart Failure: Difference and Analogies
Prognostication Assessment in Heart Failure Women:
Do we have enough skill?
Mariell Jessup MD, FAHA, FACC
Professor of Medicine
University of Pennsylvania
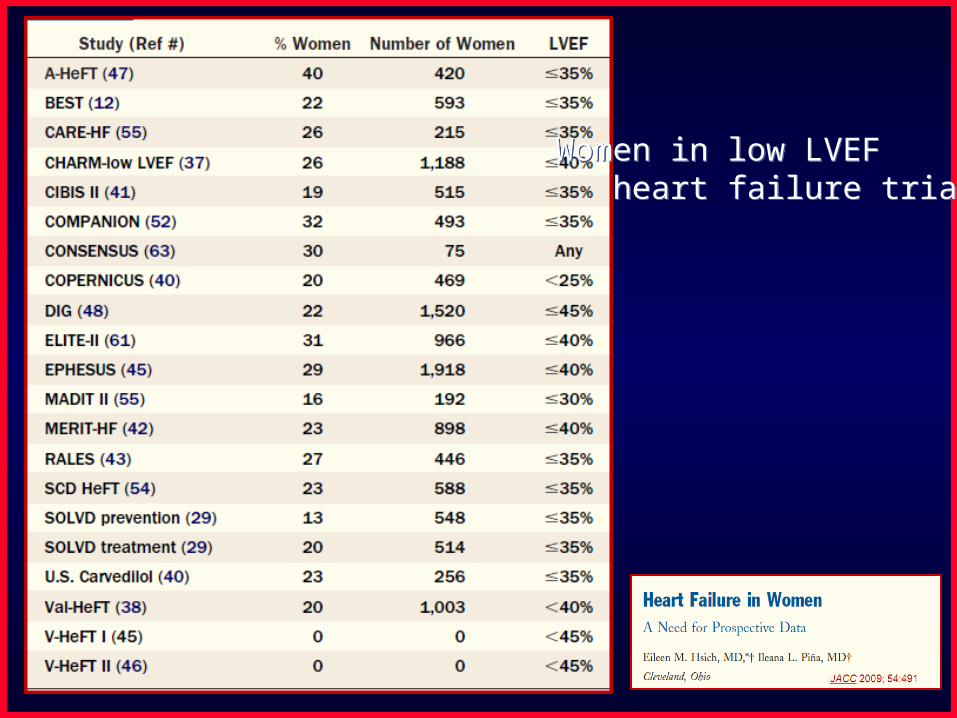
Women in low LVEF heart failure trials.Women in low LVEF heart failure trials.

1063 persons45% survival at 5 years
Circ Heart Failure 2008; 1:91-97
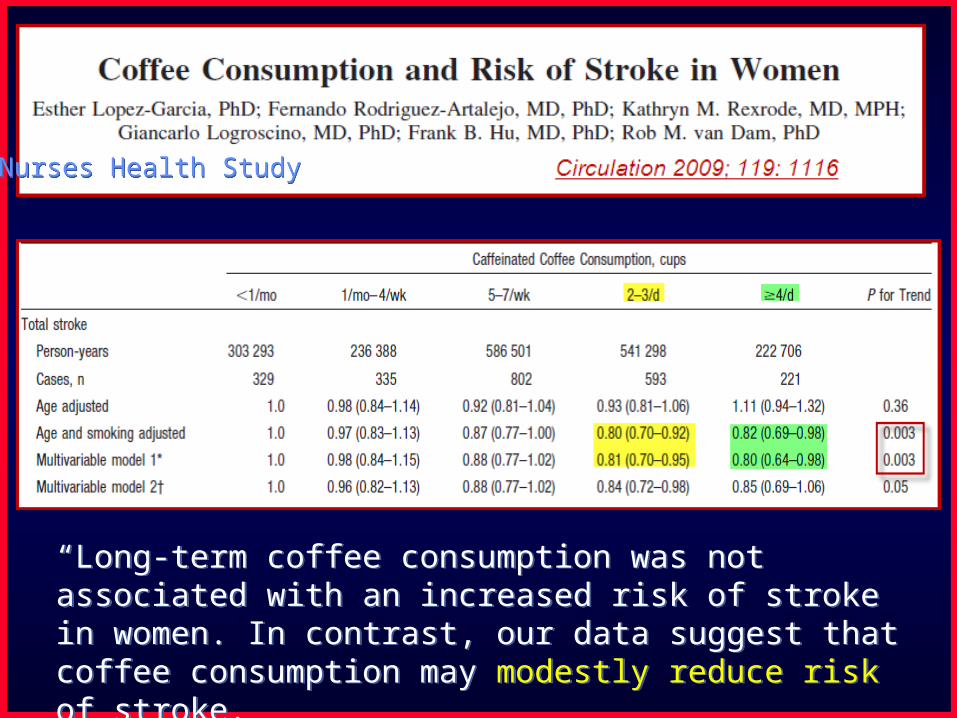
“Long-term coffee consumption was not associated with an increased risk of stroke in women. In contrast, our data suggest that coffee consumption may modestly reduce risk of stroke.
“Long-term coffee consumption was not associated with an increased risk of stroke in women. In contrast, our data suggest that coffee consumption may modestly reduce risk of stroke.
Nurses Health StudyNurses Health Study

• Clinical– Age– Gender– Etiology– HR/BP– BMI– Respiratory Rate– HF Signs/Symptoms– Recent Hospitalization– LVEF– Atrial Fibrillation– VT/VF
• Comorbidities– Cancer/PVD/CVA– Diabetes Mellitus– Smoking/COPD/Sleep Apnea– Alcohol– Liver Disease– Depression– Dialysis
• Functional– NYHA Class Prior to Admit and 30 day
• Laboratory - Admit and D/C– Sodium– BUN/Cr– Total Bilirubin– AST/ALT/Albumin– Hgb/WBC/RDW/%Lymphs– Uric acid– Cholesterol– BNP– Troponin
• Medications/Device - Admit and D/C– Diuretics - Type and Daily Dose– ACEI– ARB– CCB– B blocker– Aldosterone Blockers– Hydralazine/Nitrate– Statin– ASA/NSAID/Clopidogrel– Digoxin– BiV ± ICDs– Inotrope Use
Prognostic Predictors in HF

Goldberg, Jessup Circulation 2007; 116:360

ADHERE® CART: Predictors of Mortality
SYS BP 115SYS BP 115n=24,933n=24,933
SYS BP 115SYS BP 115n=24,933n=24,933
SYS BP 115SYS BP 115n=7,150n=7,150
SYS BP 115SYS BP 115n=7,150n=7,150
6.41%6.41%n=5,102n=5,1026.41%6.41%
n=5,102n=5,10215.28%15.28%N=2,048N=2,04815.28%15.28%N=2,048N=2,048
21.94%21.94%n=620n=620
21.94%21.94%n=620n=620
12.42%12.42%n=1,425n=1,42512.42%12.42%n=1,425n=1,425
5.49%5.49%n=4,099n=4,0995.49%5.49%
n=4,099n=4,0992.14%2.14%
n=20,834n=20,8342.14%2.14%
n=20,834n=20,834
BUN 43BUN 43N=33,324N=33,324
BUN 43BUN 43N=33,324N=33,324
Greater thanLess than
2.68%2.68%n=25,122n=25,122
2.68%2.68%n=25,122n=25,122
8.98%8.98%n=7,202n=7,2028.98%8.98%
n=7,202n=7,202
Cr 2.75Cr 2.752,0452,045
Cr 2.75Cr 2.752,0452,045
Highest to Lowest Risk CohortOR 12.9 (95% CI 10.4-15.9)
Fonarow GC, et al. Risk stratification for in-hospital mortality in heart failure using classification and regression tree(CART) methodology. JAMA. 2005;293:572-580.
33,324 patients!
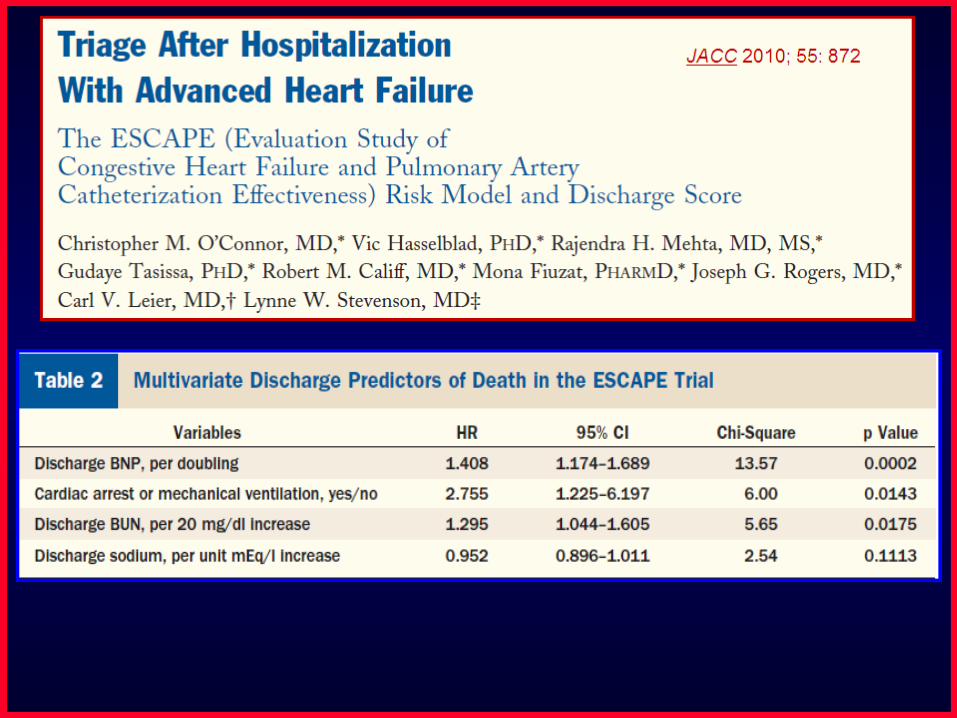

JACC 2010; 55: 872JACC 2010; 55: 872

JACC 2008; 52:347-56 48, 612 patients
The Prognostic Value of Maximal Oxygen Consumption
0
20
40
60
80
100
0 6 12 18 24
Duration of Follow-up (Mo)
Cu
mu
lati
ve S
urv
ival
(%
) VO2 > 14 ml/Kg/min
VO2 ≤ 14 ml/Kg/min (listed)*
VO2 ≤ 14 ml/Kg/min (not listed)*
Circulation 1991;83:778-786
* p<0.005 for VO2 ≤ 14 vs > 14

O’Neill et al. Circulation 2005; 111:2313

2331 patients 28% womenNYHA II-IVLow LVEF
2331 patients 28% womenNYHA II-IVLow LVEF
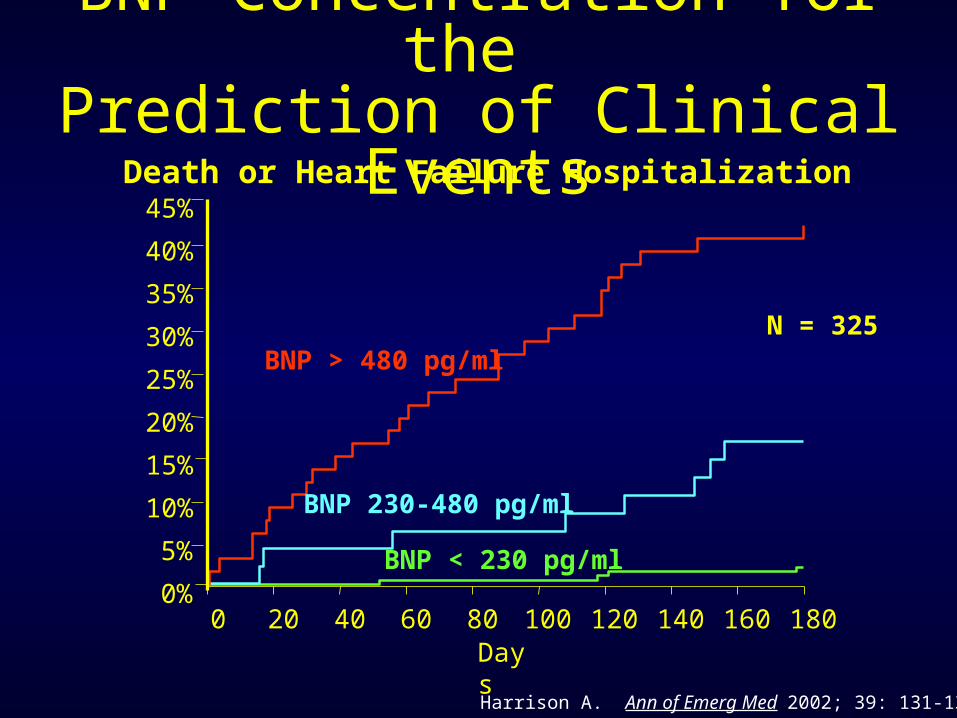
BNP Concentration for the Prediction of Clinical Events
Harrison A. Ann of Emerg Med 2002; 39: 131-138)
0 20 40 60 80 100 120 140 160 1800%
5%
10%
15%
20%
25%
30%
35%
40%
45%
BNP < 230 pg/ml
BNP 230-480 pg/ml
BNP > 480 pg/ml
Death or Heart Failure Hospitalization
Days
N = 325

JACC 2008; 52:997-1003 NT-proBNP: 1078 pg/ml

In this population of women, higher
baseline blood levels of NT-proBNP were associated with the future development
of SCD, and this relationship was independent of
established risk factors for CHD and/or SCD.
In this population of women, higher
baseline blood levels of NT-proBNP were associated with the future development
of SCD, and this relationship was independent of
established risk factors for CHD and/or SCD.

Stempfle et al. J Heart Lung Transplant 2008;27:222

Mullens et al. Am J Cardiol 2008; 101:1297

Mullens et al. Am J Cardiol 2008; 101:1297
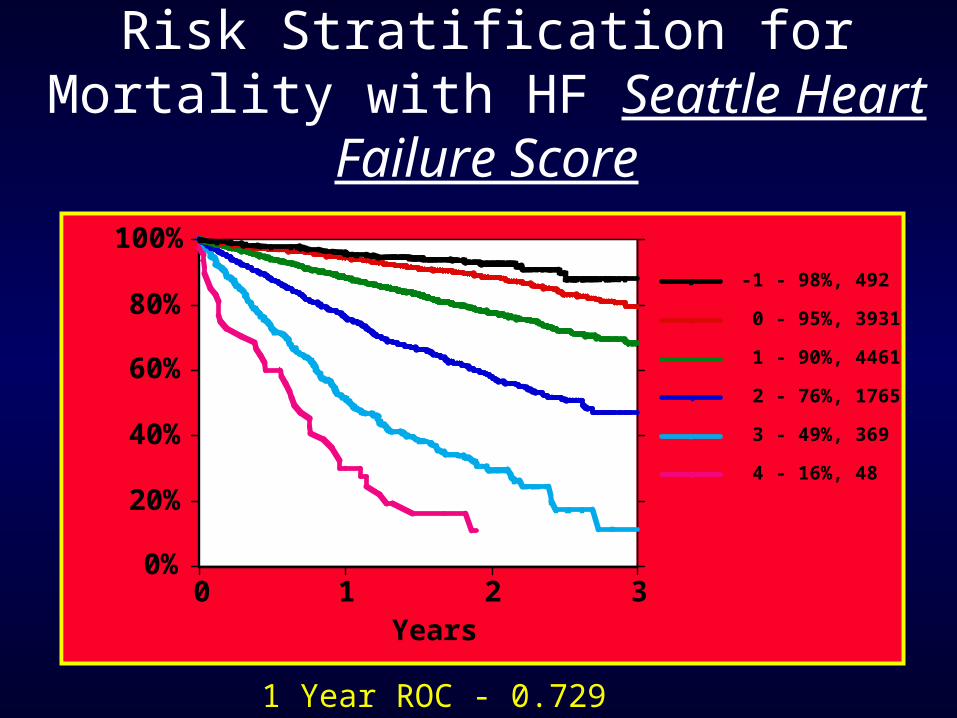
Risk Stratification for Mortality with HF Seattle Heart Failure Score
0%
20%
40%
60%
80%
100%
Surv
ival
0 1 2 3Years
4 - 16%, 48
3 - 49%, 369
2 - 76%, 1765
1 - 90%, 4461
0 - 95%, 3931
-1 - 98%, 492
1 Year ROC - 0.729

Circ Heart Failure 2008; 1:125-133
Health Aging and Body Composition

Aaronson et al. Circulation 1997;95:2660-7
Heart Failure Survival Score

Risk Stratification
I would counsel my heart failure patients to consider advanced therapies (such as VAD or transplant) or discuss end-of-life issues if the predicted annualized mortality rate was:
1. 10-20%2. 20-30%3. 30-40%4. 40-50%5. > 50%6. I would not counsel the patients for either approach