Embed Size (px)
Citation preview

® National Strength and Conditioning AssociationVolume 29, Number 2, pages 26-37
Keywords: spinal column; stabilization; lovy back pain; transversusabdominis; multifidus
Lumbar Stabilization: An Evidence-BasedApproach for the Athlete With Low Back PainMorey J.Kolber PT,MSPT,CSCS,Kristina Beekhuizen,PhD,CSCSNova Southeastern University,Ft. Lauderdale, Florida
s u m m a r y
This manuscript presents an over-
view of spinal stabilization for the
lumbar spine. Emphasis is placed on
the local stabilization musculature,
which has received considerable
support in the literature. A progres-
sive stabilization program targeting
the local stabilizing musculature is
recommended for the diverse ath-
letic population.
Introduction
A ppruxiinately 60-80% of theadult population will experiencean episode of low back pain
(LBP) at some point in their lives (13.49, 58, 65). The natural history, howev-er, is favorable, as over 80% of individu-als tnay recover independently of treat-ment within 4-6 weeks of initialcomplaints (49. 75). Although the nat-ural history is favorable, the reported re-currence rate of LBP is as high as
58-90%( 13. 29. 49, 72, 73). LBP is onlysecond to the common cold for physi-cian visits, and the costs of LBP in somesocieties exceed that of coronary arterydisease and diabetes combined (49).From an economic standpoint, the totalcost of LBP including societal factors ex-ceeds S40 billion per year (20, 49, 75).
LBP is not limited co the nonathletic pop-ulation, as individuals involved in athleticendeavors may be affected at an equal orgreater frequency than the general popu-lation (6. 15, 23, 50, 58, 64"", 71). Specificsports such as weighdifting and Americanfootball are associated with a higher inci-dence of degenerative conditions, stressfractures, and injuries of the lumbar spinewhen compared to the general population(3, 6, 23. 36, 37, 44). Athletes who per-form sports involving repeated or forcefulloading ot the spine are considerably moreprone to spondylolysis (stre.ss fractures ofthe pars interarticularis) and instability ofthe low back (22. 25, 26, 40, 41, 59, 70).Stress fractures and spinal instability havebeen identified as risk factors for LBP inthe athletic population (22, 56, 37).
Intervention for athletes with LBP isoften based upon the educational dogmaof the trainer, clinician, or strength andconditioning specialist. Differences of
April 2007 • Strength and Conditioning Journal
opinion exist as to what the optimal ex-ercises are for LBP (19). Among inter-ventions for the athlete with LBP, spinalstabilization has received considerableattention and, therefore, will be iht-focus of this discussion. This manu-script will elucidate the research relatingto spinal stabilization, di.scuss muscularchanges associated with lumbar spinedisorders, and propose an evidence-based lumbar stabilization program.Methods of achieving lumbar spine sta-bilization that are applicable to the di-verse recreational and athletic popula-tion will be presented.
Etiology and Risk FactorsThe etiology of LBP is multi-factori;ilwith reports of over 50% of episodes oc-curring tor no apparent reason (43). Riskfactors for LBP related to muscle perfor-mance in the general and athletic popu-lation include delayed mu.scle activation,impaired muscle control, decreased en-durance of the extensor mu.sctilature,and weakness of the extensors whencompared to the flexors (1, 2, 5, 8, 9,45,51, 57, 62). Reports eluding to low backinjuries from weight training, gymnas-tics, rugby, and other sports, such asAmerican football, have been document-ed in the literature (3, 23, 36, 37, 63,64). Football players, in general, increase

their risk of developing low back pain astheir years of involvement with theirsport increases (23). Specific conditionssuch a.s early degenerarive changes andstress fractures of the lumbar spine aremore common in American footballplayers than that of the general popula-tion (3, 23, 36, 37). Low back injurieshave been attributed to the recreationaland competitive weight training popula-tion as well, with low back conditions re-ported at all age groups, including ado-lescents (3. 63). In the authors'observation, athletes in particular are af-(licted with recurrent episodes of LBPdue to the propensity to train throughpain and the inherent focus on perfor-mance outweighing prevention.
DefinitionsGlobal spinal stabilizers: Musculatureprimarily responsible for generatingmovement including the erector spinae.external obliques, quadratus lumborum,and rectus abdominis (4).
Local spinal stabilizers: Musculaturewith intervertebral attachments that arecapable of providing intersegementalstability (61). The multifidus. transver-sus abdominis, and internal obliques areclassified as local stabilizers (61).
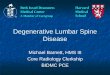
Lumbar multifidus: (Figure 1) Deepspinal musculature responsible forspinal extension and posture when con-tracting bilaterally, and rotation whenacting unilaterally (53, 77). Originatesat the sacrum, iliac spine, and transverseprocesses of the spine, spans 2-4 seg-ments and inserts into the spinousprocesses above the level of origin (42).The multifidus musculature is responsi-ble for lumbar segmental stability as it isable to provide segmental stiffness andcontrol in che neutral zone (29, 55, 76).
Lumbar segrnental itistability: (a) Loss ofcontrol or excessive motion in a seg-ment's neutral zone (57); (b) decreasedcapacity of the stabilizing system tomaintain the neutral zone within physi-ological limits; (c) a loss of stiffness be-
Figure 1. Multifidus muscle group. Lies directly in contact with vertebrae. (Copyright©Primal Pictures Ltd.,www.primalpictures.com)
tween motion segments such that nor-mal loads result in pain or stress (27).Segmental instability may be caused byweakness, degenerative disease, loss ofpassive tension and injury.
Spinal extensors: (Figure 2) Posteriorlylocated musculature of the vertebral col-umn responsible for actively extendingthe spine and eccentrically controllingforward flexion. The erector spinae isthe largest group of spinal extensors(53).
Spinal flexors: Anterior and laterally lo-cated musculature of the pelvis and verte-bral column responsible for actively flex-ing the spine against gravity. The flexorsisometrically contract as a means of stabi-lizing the ribs and pelvis during lifting,pushing, or pulling. Spinal flexors include
the abdominal musculature, p.soas major,and internal/external obliques when act-ing bilaterally (53).
Spinal neutral zone: Range of displace-ment near the spine segments' neutralposition where minimal resistance is re-quired of the osteoligamencous struc-tures. The neutral zone may increasewich injury, articular degeneration, lossof passive stiffness, weakness, or inhibi-tion of the stabilizing musculature (57).When the neutral zone Is increased, thespine may become unstable (57).
Spinal stabilization exercises: Exercisesdesigned to recruit muscles capable ofenhancing stability of the spine(l 1) andstiffness through training muscular acti-vation patterns. Spinal stability is desir-able for prevention of aberrant mobility
April 2007 • Strength and Conditioning Journal

Figure 2. Spinal extensor musculature of the low back. (Copyright ® Primal PicturesLtd., www.primalpictures.com)
at the neutral zone, decreasing pain andimpairment associated with instability,and decreasing injury risk.
Transversus abdominis: (Figure 3) Trans-versely oriented deep abdominal respon-sible for local stabilization. Originates atthe inner surface of the lower 6 ribs, di-aphragm, thoracolumbar fascia, andiliac crest and inserts at the linea albadeep to the rectus abdominis (42). Theaction of the musculature is to draw theabdominal wall in coward the spinemaintaining levels of intra-abdominalpressure and imparting tension to thethoracolumbar and sacroiliac spine (32-34,55,56,61).
DiagnosisDespite technological advances, theidentification of a specific cause of LBP
may be indefinable (27, 46, 49, 52, 68,69), and che pursuit of valid methods todiagnose and treat LBP remains a re-search priority. Although a multitude ofconditions exist, it is not uncommon forthe source of an individual's LBP to re-main elusive despite diagnosis (52, 68,69). Common clinical diagnoses includebut are not limited to: osteoarthritis,discogenic disorders, spinal stenosis,joint abnormalities, facet and sacroiliacdisorders, ligament sprains, musclestrains, spondylolysis, and spinal insta-bility. Mechanical diagnosis of LBPbased on classifying patients into rele-vant subgroups using diagnostic algo-rithms and testing clusters (13, 46, 49.68, 69, 74, 78-80) has shown promisein the areas of discogenic disorders (14,79), facet disorders (78,79), and sacroil-iac syndromes (79, 80). Methods to di-
agnose the cause of LBP, however, arebeyond the scope of this manuscript.
Deficits in strength, size, density, coor-dination, and activation of the lumbarstabilizing musculature lollowing a lowback injury or episode of LBP have beenaffirmed in rhe literature (1, 10, 11,15-18, 35, 38, 39, 47, 60. 61, 66, 67),lending credibility to approaches de-signed to strengthen and stabilize thelumbar spine following injury.
Spinal StabilizationInterventions for the athlete with LBPoften include a confrontational ap-proach, whereas the athlete will contin-ue to participate in training to tolerance;however, the athlete is often encouragedto push beyond their limits throughsport-specific functions, and intrinsicmuscle stabilization does not present atraining priority. Routines to treatand/or prevent LBP include general ex-ercise, a graduated return to sport-spe-cific tasks, spinal conditioning, andspinal stabilization exercises. Individu-als designing programs for the athletewith LBP may or may not prescribespinal stabilization as part of the condi-tioning program, as the focus is often toreturn to sport-specific training. Evi-dence is compelling to justify spinal sta-bilization exercises for the individualwith LBP due to the associated loss ofmuscle function, atrophy, and weaknessalong with the preventative benefits sub-stantiated in the literature (5-9, 11,
28-31.33-35,45,51,57,62,77).
Spinal stabilization essentially consistsof both static and dynamic stabilization.When lifting or pu.shing heavy objectswe position our spine in a rigid mannerto increase torque and stabilize thetrunk, which is referred to as static stabi-lization and requires activity primarilyof the global stabilizers. Dynamic stabi-lization on the other hand is presentthrough both neurological activation ofthe muscular system, direct muscle ca-pabilities, and passive tension. Dynamicstabililization requires coordinated rc-
April 2007-Strength and Conditioning Journal

cruitment of the local stabilization mus-culature (61). Following injury the dy-namic stabilization system is often af-fected (28-30, 33, 34).
The goals of spinal stabilization are to(a) increase the capacity of the muscularstabilizing system to maintain the neu-tral zone of the spine within its physio-logical limits (29, 55, 56, 61, 76); (b) in-crease the low back's tolerance to insulithrough the conditioning of key muscu-lature; (c) restore muscle size, strength,and endurance; (d) re-establish coordi-nated muscle activity as required for pre-vention of recurrence and restoration offunction (11, 28); and (e) reduce painassociated with spinal instability.
Structures Responsible forStabilizationStabilization of the spine Is achievedthrotigh passive structures and the neur-al/muscular systems. The passive struc-tures are often insufficient for stabiliza-tion during dynamic activities thatchallenge the spines neutral zone, par-ticularly among individuals with LBP.Due to the relative insufficiency of thepassive stabilizers the muscular stabiliz-ers must therefore fulfill the need forstabilization; however, in the individualwith LBP, this function Is often sup-pressed or inhibited.
The passive structures, including liga-ments, capsules, and osseous structures,provide stabilization through tension,bone congruence, and reflex activationof the stabilizing musculature. Injury,degenerative changes, and adaptivelengthening of the passive structuresmay reduce their ability to provide nor-mal stiffness and reflex muscle activa-tion (66, 67), thus compromising sta-bility. When stability is compromised ata specific segment or multiple seg-ments, the neutral zone increases. Thisincrease can potentially (a) increasepain, (b) increase injury risk throughsuppressed function of refiex stabilizers,and (c) decrease sport performance andfunction.
Figure 3. Transversus abdominis. Arrows point to the transversely oriented musclefibers that lie deep to the rectus abdominis. (Copyright © Primal PicturesLtd., wwvi'.primalpictures.com)
It is generally agreed upon that all of thespine muscles may play a role in ensuringspinal stability (8, 21, 27) during high-level activity, such as lifting heavy weightsor competitive sports. In the healthyspine, the trunk musculature functions tocontrol and initiate movement, respondto loading and postural perturbations,provide stiffness, minimize aberrantmovements, and provide a stable base foractivity. While all muscles of the trunkplayarolein stability to some degree, cer-tain muscles have a more specializedfunction than others. Stabilization of thelumbar spine is achieved through musclesclassified as either having local (deep andintrinsic) or global stabilizing function.The local spinal stabilizers have receivedconsiderable attention in the literaturedue to their ability to prevent movement
outside the spines neutral zone. Addi-tionally, re.search indicates that local sta-bilization abilities are suppressed follow-ing an episode of LBP, specifying theneed to address these muscles. In the au-thors' experience, athletes invariably re-ceive some form of spinal stabilization aspare of their conditioning routines; how-ever, the focus is often on the large globalstabilizers and deficient in the area oflocal stabilization.
The global stabilizers include the rectusabdominis, spinal extensors, externalobliques, quadratus lumborum. andpsoas muscles. The global stabilizersfunction in response to voluntary effortduring the initiation of spinal move-ment and during challenging activitiesthat require a stiff spine.
April 2007 • Strength and Conditioning Journal

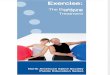
Figure 4. Fatty infiltration (white regions identified by*) of the multifidus in an indi-vidual with chronic low back pain.The multifidus (*) is located deep to theerector spinae (arrows).
Much accencion in the literature hasbeen focused on the spinal extensors,particularly the erector spinae (2, 5, 7,24, 62), which will be the primary glob-al stabilizer lending itself to discussionin this manuscript. The spinal extensorsserve to extend the lumbar spine, main-tain the natural lordosis, and stabilizethe spine in the closed packed positionduring lifting and other activities re-quiring lumbar stabilization. Evidencesuggests that there is decreased en-durance and measurable atrophy of thespinal extensors in the LBP population(10, 35, 39, 54). Weakness of the spinalextensors relative to the spinal flexors in-creases an individual's risk for develop-ing LBP (45). In addition, a decreasedrertex response of the extensors in reac-tion to movement when compared to
m
the flexors may predispose one to injury(9). Lastly, evidence suggests that in-creasing the strength of the spinal exten-sors may decrease the likelihood of de-veloping LBP (5. 24, 51).
The local stabilizers' function is to pro-vide a stable base in preparation or antici-pation of crunk and extremity move-ments. The local stabilizers fulfill the roleof stabilizing the spine when the integrityof the spine's neutral zone is challenged.In the healthy spine, muscle contractionof the local stabilizers is automatic andprecipitated by movement of the extremi-ties or trunk, unlike the injured spinewhereas the activation is suppressed or de-layed. The local stabilizers include themultifidus (Mult), transversus abdominis(TrA), and internal obliques.
April 2007 • Strength and Conditioning Journal
The Mult is a deep intrinsic spinal mus-cle that will maintain posture, extend,and rotate the spine. Additionally, chcMult contracts in anticipation of trunkand extremity movement to provide astable base. In the healthy lumbar spine,the Mult provides stabilization locallyby minimizing movement of the spinalcolumn and maintaining the theoreticalneutral zone (55, 66, 67, 76^. Evidencesuggests that the Mult imdergoes patho-logical changes following an episode ofLBP, such as suppressed activation, atro-phy, fatty infiltration (Figure 4), andweakness (U, 30, 29, 38, 47, 60, 77).
The TrA functions to flatten and com-press the abdominal wall. The 7rA is in-variably activated in anticipation oftrunk and extremity movement to pro-vide stability of the lumbar spine(31-34) similar to the Mult. Weaknessor delayed activation of the'IrA may di-rectly affect local spinal stabilization as aresult. Research has reported reducedactivation ability of the TrA in the LBPpopulation (16, 31, 33, 34) as well as de-creased recurrence rates of LBP on thosewho are able to restore their ability tocontract the TrA (28).
Among clinicians and strength and con-ditioning specialists, it is generallyagreed upon that all of the muscles sur-rounding the spine provide stabilizationto some degree during physical activity.While the authors agree that a compre-hensive approach to spinal stabilizationand conditioning is necessary in the ath-letic population, specific muscles re-quire attention in the athlete with LBP.The erector spinae. Mult, and TrA havereceived much attention in the literaturedue to their stabilizing abilities and as-sociated deficits following an episode ofLBP. Therefore, these select muscles willbe the focus of this discussion.
Stabilization ProgramIndividuals with LBP will recover atvarying time frames depending upon thenature ol thetr injury, diagnosis, andability to recover without aggravation of

(a) Supine abdominal draw exercise with natural lordosis using a pressure cuffto monitor positioning, (b) Supine abdomi-nal draw exercise with natural lordosis and simultaneous upper and lower extremity flexion.
cheir condition. Due to the competitivenature of athletics, known risk factorsfor LBP, and prevalence of LBP, spinalexercises are invariably incorporatedinto both training and rehabilitationprograms.
The proposed stabilization program in-c! udes 3 progressive stages. The programfocuses on the local stabilization muscu-lature in phase one, with progressionInto the final stage, which incorporatesche global stabilizers. Progressionthrough the 3 stages is dependent uponthe athlete's abilities, pain level, andstage of injury. In cases where the stabi-lization program is used for prevention,ihe athlete may progress on a timelinebased on their abilities to master the ex-ercises. Individual progression, however,will vary as the initial tasks may require alew sessions in some individuals due tosuppressed muscle activity associatedwith LBP.
This program is recommended as part ofa comprehensive individualized condi-tioning program. It should be per-iormed daily during stage 1 since neuralactivation is essential to mastering therequired tasks. The program can then bedecreased to 3 times a week during stage3 since the athlete will typically return
to premorbid activities at this time andwill be performing the routine as part ofa comprehensive program.
Stage 1All participants begin the program withstage 1, which includes 3 progressive ex-ercises. An individual's level of condi-tioning will not directly influence theirabilicy to activate the local musculaturefollowing an episode of LBP; therefore,stage 1 is of primary importance. Theinitial goal of stage 1 is to activate thelocal stabilizing muscles without com-pensation by the large global stabilizers.This stage requires neural activation andmuscle coordination. The final goal ofstage 1 involves maintaining a co-con-traction of che local stabilizers while per-forming rapid alternating extremitymovements in the sagittal plane.
Exercise 1 (Figure 5a) is referred co asthe supine abdominal draw. The athleteis asked to lie on their back with theirhips and knees flexed 45 degrees, assum-ing a natural lordosis of the lumbarspine. A blood pressure cuff inflated to30—40 mm hg is placed under theirspine. Once in position, the athlete isasked to draw their abdomen in and up.The athlete is asked not to hold theirbreath and to maintain the natural lor-
dosis by avoiding the desire to flattenthe back during this task. The read-outon the pressure cuff should remain rela-tively constant throughout the exercise.Flattening the back and not maintainingthe desired lordosis will result in a rise inthe pressure read-out, which is thenused as a signal for the athlete to resumethe lordotic position. 1 his exercise acti-vates both the TrA by drawing in the ab-domen and the Mult by maintaining thelordosis. This exercise is held for 10 rep-etitions of 30 second durations. Oncemastered the co-contraction performedin this exercise is utilized for the pro-gressions in the remainder of the exer-cise program.
Exercise 2 involves maintaining the co-contraction of the TrA and Mult whileperforming rapid alternating arm flex-ion for a dtiration of 1 minute for 3—5sets. Research has identified a feed-for-ward anticipatory contraction of the TrAand Mult in response to upper and lowerextremity movements (32-34). Onceupper extremity (UE) motions are toler-ated, the athlete is instructed to performrapid alternating hip flexion of approxi-mately 6-12" while maintaining a co-contraction of the TrA and Mult. Oncethe athlete is able to maintain a co-con-traction of the TrA and Miilc during
April 2007 • Strength and Conditioning Journal

Figure 6. (a) Quadruped position with co-contraction of the transversus abdominis and multifidus. (b) Quadruped position withco-contraction and simultaneous upper and lower extremity extension.
movements of the upper and lower ex-tremities, the task is mastered and theathlete can advance to the next exercise.
Exercise 3 (Figure 5b) requires the ath-lete to maintain the co-contraction andnatural lordosis while rapidly alternat-ing the arms and hips into flexion whilelying on their back. The procedure in-volves simultaneously raising the leftarm and right lower extremity (LE) fol-lowed by raising the right UE and leftLE. This is carried out for 3 sets of 20repetitions or durations of I minute for3-5 repetitions. The athlete can advanceto stage 2 once they demonstrate theability to maintain the co-contraction ofthe TrA and Mult while performing ex-tremity movements in the supine posi-tion and without complaints of pain.
Stage 2The progression to stage 2 involves exer-cises that require a co-contraction of theTrA and Mult during the assumption ofadditional positions, with the added re-cruitment of the erector spinae, shoul-der, and hip extensor musculature.
Exercise 1 (Figure 6a) requires the indi-vidual to assume a quadruped positionwhile maintaining a co-contraction ofthe local stabilizers. The individual is
asked to raise the arms forward into flex-ion alternating rhythmically from theright to the left arm. Once this is mas-tered, LEs are brought into relative hipextension while maintaining the localco-contraction.
Exercise 2 (Figure 6b) involves alter-nately raising their upper and lower ex-tremities simultaneously (right armwith left leg. then left arm and right leg)while maintaining the co-contraction ofthe TrA and Mult. When performed ac-cording to the recommendations out-lined, this exercise will activate both thelocal and global stabilizers. The exerciseis typically performed for 3 sets of 20repetitions or 10 10-second holds. Theindividual .should demonstrate the abil-ity to maintain a steady position withminimal sway while strictly holding aco-contraction of the TrA and Multprior to advancing co the next exercise.
Exercise 3 involves performing the sameexercise described in exercise 2 with theaddition of ankle cuff weights. Anklecuff weights will challenge the stabiliz-ing musculature by increasing muscleactivation when raising the teg, as weli asthrough the relative imbalance of weightbetween the upper and lower extremi-ties.
Stage 3The final stage requires the participantto maintain the abdominal draw andnatural lordosis co-contraction duringthe performance of exercises designedto recruit global stabilizers. The 3 exer-cises described in stage 3 are consideredto be of equal challenge and may beperformed as tolerated by the individ-ual using principles of exercise progres-sion.
Exercise 1 (Figure 7) requires the in-dividual to assume the prone positionwhile lying flat on a table. The partic-ipant first assumes the abdominaldraw, then begins extending che spineoff the mat to their end-range limit ofextension while maintaining the ab-dominal draw. The feet are not stabi-lized as this exercise is designed to beperformed in a controlled manner,primarily seeking the effort of thespinal extensors. This exercise may beadvanced by adding pillows under thewaist to increase the range of motionof the exercise, by extending the armsoverhead, or by adding cuff weights tothe wrists while holding the armsoverhead.
Exercise 2 (Figure 8) requires the in-dividual to perform the "side bridge"
April 2007 • Strength and Conditioning Journal

Figure 7. Prone trunk extension with abdominal draw.
Figures. Side bridge exercise while maintaining abdominal draw.
exercise (48) traditionally used tostrengthen the quadratus lumborum.Participants are required to lie onilieir side with the legs extended. Theexercise requires the individual to lift
their hips off the table to a levelwhere their body is straight and sup-ported by their weight-bearing armand feet. Individuals are instructed tomaintain the TrA-Mult co-contrac-
tion and hold the position for a dura-tion of 10 seconds for a total of 10repetitions. This exercise is per-formed on both the right and leftsides. To advance this exercise, theparticipant is instructed co repetitive-ly reach cheir arm straight out to thefronc (Figure 9a) and then toward theceiling (Figure 9b) while maintainingthe side bridge position with a TrA-Mult co-contraction.
Exercise 3 (Figure 10) require.s cheindividual to stand on an unstablesurface, such as a balance board,which will recruit the stabilizationmusculature through postural per-turbations. While standing on theunstable surface, the participant isinstructed to assume a position ofslight knee and hip flexion whilemaintaining a co-contraction of chelocal stabilizers. During the exercise,the individual is instructed to rapidlyalternate arm flexion while maintain-ing their balance and position. Thisexercise is advanced by using dumb-bells during the arm movement. Thisexercise is usually performed for aduration of 1 minute for 2-5 repeti-tions. As the exercise is mastered theweights may be increased and theeyes may be closed to further chal-lenge the local stabilizers.
(a) Side bridge exercise with abdominal draw and horizontal upper extremity movement, (b) Side bridge exercise withabdominal draw and horizontal upper extremity movement. [
April 2007 • Strength and Conditioning Journal

Figure 10. Standing stabilization on an unsteady surface maintaining co-contractionof multifidus and transversus abdominis with alternating upper extremityflexion.
ConclusionLBP is a common condition that mayaffect athletes at a greater prevalencethan the general population. Individu-
als involved in program design for theathlete with a current or a past historyof LBP often include the physician,physical therapist, athletic trainer, and
strength and conditioning specialist.While intervention is often sport spe-cific and based on the treatmentprovider's acumen, it is common prac-tice to recommend general stabili/.a-tion exercises. Although general stabi-lization exercises are useful as a meansof spinal conditioning, exercisesspecifically designed Co challenge andactivate the local stabilizers are of pri-mary importance due to the docu-mented pathological changes in thesemuscles following or associated wichLBP, Furthermore, evidence ha.s sub-stantiated the preventative benefits as-sociated with training the local stabi-lizers and the spinal extensors.
Spinal stabilization exercises, when per-formed according to the progressionsrecommended in this manuscript, re-quire no special eqtiipment or space,may be progressed based on the individ-ual's ability and learning curve, and aresafe and applicable for the more com-mon low back conditions experiencedby athletes. Lastly, the stabilization exer-cises recommended may be prescribed aspart of a general conditioning programconsidering the known risk for LBP as-sociated with certain sport.s.
Key Points• Evidence in the literature has identi-
fied the importance of local stabi-lization exercises for the manage-ment of LBP.
• The spinal extensors. Mult, and TrAare adversely affected following anepisode of LBP.
• LBP is associated with reduced IrAand Mult activation.
• LBP is associated with atrophy of theMult and spinal extensor muscula-ture.
• Training the TrA and Mult reducesthe recurrence of LBP. •
References1. AIJ\RANTA, H., H . HURRI, M. HEI.IO-
VAARA, A. SOUKKA, ANO R. H A R U ' .
Non-dynamometric crunk perfor-mance tests: Reliability and normative
April 2007 -Strength and Conditioning Journal

data. Scand. J. Rehabil. Med. 26:211-215. 1994.
2. Alj\R/\NTA, H., S. LUOTO, M. HlXIO-VAARA, AND H. HuRJU. Static back en-durance and the risk of low-back pain.Clin. Biomech. 10:323-324. 1995.
3. ALEXANDER, M . J . Biomechanical as-
pects of lumbar spine injuries in ath-letes: A review. Can. J. Appl. Sport Sci.10:1-20.1985.
4. BkRCMARK, A. Stability of the lumbarspine. A study in mechanical engineer-ing. Acta. Orthopaedica Scandinavica.230:S20-S24. 1989.
5. BllLR[Nc.-S()Ri:N.st)N, R Physical mea-surements as risk factors for low-backcrouble over a one year period. Spine.9:106-119. 1984.
6. BONO, C M . Low-back pain in ach-letes. y. Bone Joint. Surg. Am. 86:382-396. 2004.
7. CARPENTER, D.M., AND B . W . N E L -
SON. Low back strengthening for theprevention and treatment of low backpain. Med. Sci. SportsExerc. 31:18-24.1999.
8. C H O I EWIC:K[, J., ANO S.M. MCGILL.
Mechanical stability of the in vivolumbar spine: Implications for injuryand chronic low back pain. Clin. Bio-mech. (Bristol. Avoti).M:\~\'^. 1996.
9. C H O I E W I C K I , J., S.P. SiLFIES, R.A.
SHAH, H . S . GREENE, N . R Rt;EVi-s, K.
ALVI, AND B . GOLDBERG. Delayed
trunk muscle reflex responses increas-es the risk of low back injuries. Spine.30:2614-2620.2005.
10. COOPER, R.G., W.F. S T CIJ\ IR, AND
M.I. JAY.SON. Radiographic demon-stration of paraspinal muscle wastingin patients with chronic low back pain.Br.J. Rheumatol. 31:389-394. 1992.
11. DANNEELS, L.A., G.G. VANDER-
STRAETEN, D.C. CAMBIER, E.E.
WirvRouw, J. BoRGOis, W.DANKAI-R'IS, AND H.J. DECIJYPER . Ef-
fects of three different training modal-ities on the cross sectional area of thelumbar multifidus muscle in patientswith chronic low back pain. Br. J.Sports Med. 35:186-191. 2001.
12. DE GIROIJ\MO, G. Epidemiology and
social costs of low back pain and fi-
bromyalgia. Clin. J. Pain. 7(Suppl.1):S!-S7. 1991.
13. DELIITO, A., R .E . ERHARD, AND R.W.
BOWI.ING. A treatment based classifi-cation approach to low back syn-drome: Identifying and staging pa-tients for conservative treatment. Phys.r/jcr. 75:470-489. 1995.
14. DoNEUsoN, R., C. APRILL, R. M E D -
CALF, AND W. GRANT. A prospectivestudy of centralization of lumbar andreferred pain: A predictor of sympto-matic discs and anular competence.6>;w. 22:1115-1122. 1997.
15. ENCELHAHirr', M., I. REUTER.J. FREI-
WALD, T. BOHME, AND A. HALBSGUTH.Spondylolysis and spondylolisthesisand sports. Orthopade. 26:755-759.1997.
16. FERREIRA, P H . , M.L. FLRREIR.A, AND
RW. Hoix:i'.s. Changes in recruitmentof the abdominal muscles in peoplewith low back pain. Ultrasound mea-surement of muscle activity. Spine.29:2560-2566. 2004.
17. FKRREIRA, P H . . M.L. FI.RREIRA, C . G .
MAHFR, R . D . HERBERT, AND K. REE-
.SHAUGE. Specific stabilization exercisefor spinal and pelvic pain: A systemat-ic review. Aiist.J. Physiother. 52:79—88.2006.
18. FLICKER, P.L., J.L. FLECKSTEIN, K.
FERRY, J. PAYNE, C . W A R D , T . MAYER,
R.W. PARKHY, AND R . M . PESHOCK.
Lumbar muscle usage in chronic lowback pain. Magnetic resonance imageevaluation. 5/':nf. 18:582-586. 1993.
19. FOSTER, N . , K. THOMP.SON, D . BAX-
TER, AND J.M. ALL£N. Managemenc of
nonspecific low back pain by physio-therapists in Britain and Ireland. Spine.
24:1332-1342. 1999.20. FRYMOYER, J.W., AND W.L. CATS-
BARIL. An overview of the incidencesand costs of low back pain. Orthop.Clin. North Am. 2:263-271. 1991.
21. GARDNER-MCIRSI:, M.G., LA. STOKILS,
AND J.P. LA!BI E. Role of muscles inlumbar spine stability in maximum ex-tensor efforts./ Orthop. Res. 13:802-808.1995.
22. GARRY, J.P, AND J. MCSHANE. Lum-
bar spondylolysis in adolescent ath-
letes../. Fnm. Pract. 4 7 : 1 4 5 - 1 4 9 .1998.
23. GERHINO, PG., AND P.A. D 'HEMF.-
COURT. Does football cause an increasein degenerative disease of the lumbarspinel* Curr. Sports Med. Rep. 1:47-51.2002.
24. GUNDFWALL, B., M. LlLJFQVlST, ANDT. HANSSON. Primary prevention ofback symptoms and absence fromwork. A prospective randomized studyamong hospital employees. Spine.\8:587-94.1993.
25. HALVORS[:N,T.M., S. NILS.SON, AND
P.H. NAKSI AD. Stress fractures.Spondylolysis and spondylolisthesis ofthe lumbar vertebrae among youngathletes wich back pain. Tidsskr. Nor.Uegefi)ren. 116:1999-2001.1996.
26. HARVEY, J., AND S. TANNER. LOW back
pain in young athletes. A practical ap-proach. Sports Med. 12:394-406.199 L
27. HK:Ks,G.E.,J.M.FRn-z,A.DELm-o,AND S.M. Mc:Gii L. Preliminary'devel-opment of a clinical prediction rule fordetermining which patients with lowback pain will respond to a stabiliza-tion exercise program. Arch. Phys. Med.Rehabil 86:1753-1762. 2005.
28. HiDES, J.A., G.A. JULL, AND C.A.
RICHARDSON. Long-term effects ofspecific stabilizing exercises for first-epi.sode low back pain. Spine.26:E243-E248.2001.
29. HIDES, J.A., C.A. RICHARDSON, AND
G.A. JULL. Multifidus muscle recoveryis not automatic after resolution ofacute, first-episode low back pain.5;>;«?. 21:2763-2769. 1996.
30. HIDES, J.A., M.J. STOKES, M . SAIDE,
G.A. JULL, AND D.H. COOPF.R. Evi-
dence of lumbar multifidus musclewasting ipsilateral to symptoms in pa-tients with acute/subacute low back^•Am. Spine. 19:165-172. 1994.
31. HODGES, P.W., AND C.A. RICHARD-
SON. Ineflicient muscular stabilizationof the lumbar spine associated withlow back pain. A motor control evalu-ation of transverse abdominis. Spine.21:2640-2650. 1996.
32. HODGES, P.W., AND C.A. RICHARD-
SON. Contraction of the abdominal
April 2007 • Strengtfi and Conditioning Journal

muscles associated with movement ofthe lower limb. Phys. Ther. 77:132-141. 1997.
33. HODGES, PW, AND C.A. RICHARD-
SON. Delayed postural contraction oftransversus abdominis in low backpain as.sociated with movement of thelower limb. y. Spinai Disord. 11:46-56. 1998.
34. HODGES, P.W., AND C.A. RICHARD-
SON. Altered trunk muscle recruitmentin people with low back pain withupper limb movement at differentspeeds. Arch. Phys. Med. Rehabil.80:1005-1012. 1999
35. HULTMAN, G., M. NOKDIN, H.SAIWSTE, AND H . OHLSI'N. Body com-
position, endurance, strength, cross-sectional area, and density of MMerector spinae in men with and with-out low back pain. / Spinal Disord.6:114-123. 1993.
36. IwAMOTo, J., H. ABE, Y. TSUKIMURA,
AND K. WAKANO. Relationship be-
tween radiographic abnormalities oflumbar spine and incidence of lowback pain in high school and collegefootball players: A prospective study.Atn. J. Sports Med. 32:781-786.2004.
37. IwAMorti, J., H. ABE, Y. TSUKIMURA,
AND K. WAKANO. Relationship be-
tween radiographic abnormalities oflumbar spine and incidence of lowback pain in high school rugby players:A prospective study. Scand. J. Med. Sci.5/.om. 15:165-168. 2005.
38. KADI R, D.E, D. WARDI AW, AND F.W
SMITH. Correlation between the MRIchanges in the lumbar multifidus mus-cles and leg pain. Clin. Radiol.55:145-149.2000.
39. KANKAANPAA, M . , S. TAIMELA, D .
LAAKSONEN, O . HANNINEN, AND O .
AiRAKSiNEN. Back and hip extensorfatigability in chronic low back painpatients ajid controls. Arch. Phys. Med.
40. KEENE, J.S. LOW back pain in the ath-lete. From spondylogenic injury dur-ing recreation or competition. Post-grad. Med. 74:209-213, 217. 1983.
41. KEENE, J.S., AND D.S. DRUMMOND.
Q
Mechanical back pain in the athlete.Compr. Ther. 11:7-14. 1985.
42. Kr.NDALi., EP., AND E.K. MCCREARY.
Muscles Testing and Function With Pos-ture and Pain (5ch ed). Balcimore,MD: Lippincott Williams & Wilkins,2005. pp. 165-197.
43. KRAMER J. fntervertebraI Disk Diseases(2nd ed.). New York, NY: ThiemeMedical Publishers, 1990. pp. 134.
44. KujAiA, U.M., J.J. SALMINEN, S.
TAIMELA, A. OKSANEN, AND L.
JAAKKOLA. Subject characteristics andlow back pain in young athletes andnon-athletes. Med. Sci. Sports Exerc.24:627-632.1992.
45. LEE, J.H., Y. Hosi IINO, K. NAKAMU-
RA, Y. KARiYA, K. SAIIA, .AND K. I IO.
Trunk muscle weakness as a risk factorfor low back pain. A 5-year prospectiveitudy. Spine. 24:54-57. 1999.
46. LONG, A., R. DONELSON, AND T.
FuN( .̂ Does it matter which exercise?A randomized controi trial of exercisefor low back pain. Spine. 29:2593-2602. 2004.
47. MA-ITILLA, M . , M . HURME, H .
ALARANTA, L. PALJARVI, H . KAUMO, B.
FAi.cK, M. LKH'LO, S. EINOIA, AND M .
JARVINEN. The multifidus muscle inpatients with lumbar disc herniation.A histochemical and morphometricanalysis of intraoperative biopsies.Spine. 11:732-738. 1986.
48. McGii L, S.M., A. CHILDS, AND C
Lll'BSON. Endurance times for lowback stabilization exercises: Clinicaltargets for testing and training from anormal database. Arch. Phys. Med. Re-habil. 8Q:94\~944. 1999.
49. M C K E N / I E R.A., AND S. MAY. The
Lumbar Spine: Mechanical Diagnosisand Therapy (2nd ed.). Waikanae, NewZealand: Spinal Publications NewZealand Ltd, 2003.
50. McTlMONEY, C.A., AND LJ. MiCHEU.Current evaluation and management ofspondylolysis and spondylolisthesis.Curr. Sports Med Rep. 2:41^6. 2003.
51. MooNFY, V., M. KRON, P RUMMER-
I'lELD, AND B. HoiMES. The effect ofworkplace based strengthening on lowback injury rates: A case study in the
April 2007 • Strength and Conditioning Journal
strip mining industry./ Occttp. Rehab.5:157-167.1995.
52. NAOIEMSON, A. Advances in low-backpain. Clin. Orthop. 200:266-278.1985.
53. NoRKiN, C . C , AND P.K. LEVANGE.
Joint Structure and Function. A Com-prehensive Analysis (2nd ed.). Philadel-phia: F.A. Davis Company, 1992.pp. 125-162.
54. ODDSSON, L .L , J.E. GIPHART, R.J.
Buijs, S.H. ROY, H . P TAYLOR, AND
C.J. DH LUCA. Development of new
protocols and analysis procedures forthe assessment of LBP by surfaceEMG techniques./. Rehabil. Res. Dev.34:415-26.1997.
55. O'SuLLivAN, P., G.D. PHYIY, L.T.TWOMEV, AND G.T ALUSON. Evalua-tion of specific stabilizing exercise inthe treatment of chronic low back painwith radiologic diagnosis of spondylol-ysis or spondylolisthesis. Spine. 22:2959-2967. 1997.
56. O'SULLIVAN, PB., L. TWOMEY, ANDG.T. ALLISON. Altered abdominalmuscle recruitment in patients withchronic back pain following a specificexercise intervention./O5/'7'. 27:114-124. 1998.
57. PANJABI, M . The stabilizing system ofthe spine. Part 1 fiinction, dysfunction,adaptation, and enhancement. J.Spinal Disord. 5:383-389. 1992.
58. PRKNIICI: W.E. Rehabilitation Tech-niques in Sports Medicine. St. Louis,MO: Times Mirror/Mosby CollegePublishing, 1990. pp. 47, 151,164-168.
59. RALSTON, S. AND M . WI.IR. Suspect-
ing lumbar spondylolysis in adolescentlow back pain. Clin. Pediatr. (PhiLi.).37:287-293.1998.
60. RANTANEN, J., M . HLIRME, B. FALCK,
H. ALARANTA, E NYKVST, M . LEHIO,
S. EiNOiA, AND H. KALIMO. The lum-
bar multifidus mu.scle five years aftersurgery for a lumbar intervertebral discherniation. .,S>/nr. 18:568-74. 1993.
61. RICHARDSON, R.A., C.J. SNIJDKRS,
J.A. HIDES, L. DAMEN, M.S. PAS, AND
J. STORM. The relationship betweenthe transverse abdominis muscles.

sacroiliac joint mechanics, and lowback pain. Spine. 27:399^05. 2002.
62. RissANEN, A., M. HELIOVAARA, H .
ALARAN'I'A, S. TAIMEIA, E. MALKIA, P
KNEKT, A. REUNANEN, AND A. AROMAA.
Does good trunk extensor performanceprotect against back related disability?/LiehabiL Med. 34:62-66. 2002.
63. RissFR. W.L. Musculoskeletal injuriescaused by weight training. Guidelinesfor prevention. Clin. Pediatr. 29:305-310.1990.
64. Ro.ssi, R, AND S. DRAGONI. Lumbarspondylosis and sports. The radiologi-cal findings and statistical considera-tions. Radiol. Med (Torino). 87:397-400. 1994.
65. SCHMID'I, CO. , AND T. KOH! MANN.What do we know about the symp-toms of back pain? Epidemioiogical re-sults on prevalence, incidence, pro-gression and risk factors. Z. Orthop.Lhre. Grenzgeb.U3:292-29S. 2005.
66. SoioMoNow, M., B.H. ZHOLU R.V.
BAR/VITA, Y. LU, AND M . HARRIS. Bio-
mechanics of increased exposure tolumbar injury caused by cyclic loading:Part I. Loss of reflexive muscular sta-bilization. Spine. 24:2426-2434.1999.
67. SoLOMONOw, M., B.H. ZHOU, M .
HARRIS, Y. LU, AND R.V. BARATTA.
The ligamento-muscular stabilizingsystem of the spine. Spine. 23:2552—2562. 1998.
68. SnTZIUl, WO. Scientific approach tothe assessment and man^ement of ac-tivity-related spinal disorders. A mono-graph for clinicians. Report of theQuebec Task Force on Spinal Disor-ders, ^/-iw. 12:sl-s59. 1987.
69. SPI 1ZER, W.O. Approach to the prob-lem. J)>«f.l2:s9-sll.1987.
70. STANDAERT, C.J., S.A. HERRING, B.
HA[ I'I:RN, AND O . KING. Spondyloly-
sis. Phys. Med. Rehabil. Clin. N. Am.11:785-803.2000.
71. TRAINOR, T.J., AND M.A. TRAINOR.
Etiology of low back pain in athletes.Curr. SportsMed. Rep. 3:41-46. 2004.
72. TROUP, J.D., J.W. MAIU-IN, AND D.C.
LLOYD. Back pain in industry: Aprospective survey. Spine.6:61 -69.1981.
73. VAN DEN HOOGEN, H.J.M., B.W.
KOES, J.T.M. VAN ElJEK, L.M.BouTER, AND W. DF.VU.LE. On the
course of low back pain in generalpractice: A one year follow-up study.Ann. Rhejim. Dis. 57:1.3-19. 1998.
74. VON KoKFK, M. Studying the naturalhistory of back pain. i^/n^. 19:s2041-s2046. 1994.
75. WADDFLL, G . A new clinical model forthe treatment of low back pain. Spine.12:632-644. 1987.
76. WiLKF, H.J., S. WOLF, L.E. CLAES,
M. ARAND, AND A. WIESEND. Stabili-
ty increase of the lumbar spine withdifferent muscle groups. A biome-chanical in vitro study. Spine. 20:192-198. 1995.
77. YosHiJL^RA, K., Y. SHIRAI, Y. NAKAYA-
MA, AND S. UESAKA. Histochemical
changes in the multifidus muscle in pa-tients with lumbar intervertebral discherniation. Spine. 26:622-626. 2001.
78. YOUNG, S., AND CN. AI'RILL. Charac-
teristics of a mechanical asse.ssment forchronic lumbar facet joint p a i n . /Manual Manipulative. Ther. 8:78-84.2000.
79. YOUNG, S., C . APRILL, AND M .
LASLEIT. Correlation of clinical exam-ination characteristics with threesources of chronic low back pain.,?/)mf./3:460-465. 2003.
80. YOUNG, S., M . LASU'II', C N . AJ'RILL,
AND C. KELLY. The sacroiliac joint:Comparing physical examination anddiagnostic block arthrography. / Or-thop. Sports Phys. Ther. 30:A34. 2000.
Acknowledgments: The authors wouldlike to thank Meg Guglielmino PT,CSCS, and Hector Perez PTA, NSCA-CPT for their assistance with the pic-tures.
Kolber
Morey J. Kolber is an assistant professorat Nova Southeastern University in Ft.Lauderdale, Florida.
Beekhujzen
Kristina Beekhuizen is an assistant pro-fessor at Nova Southeastern University inFt. Lauderdale, Florida.
THE SECRET IS OUT...Velocity Enhanced Resistance Training
JUMP HIGHERHIT HARDERRUN FASTERTHROW FARTHER
f/r/if£ss
April 2007- Strength and Conditioning Journal

© National Strength and Conditioning AssociationVolume 29, Number 2, pages 38-39
C e r t i f i c a t i o n C E U Q u i z
Lumbar Stabilization: An Evidenced-BasedApproach for the Athlete With Low Back PainNote: This quiz may be used by the CSCS- and NSCA-Certified Personal Trainer to acquire 0.5 CEUs.Certified Athletic Trainers will receive 1 CEU for completing this CEU Quiz.BOC Approved Provider #:P2301-1 • The article for this quiz begins on page 58
1.
2.
3.
4,
5.
The INITIAL goal of a Stage 1 stabilization program for LBPemphasizes which of the following?A. activation of local stabilizers without compensation
by the global stabilizersB. activation of global stabilizers without compensation
by the local stabilizersC. maintain co-contraction of local stabilizers with the
global stabilizersD. maintain co-contraction of global stabilizers with the
local stabilizers
Which of the following musculatures isometrically con-tract to stabilize the ribs?A. global spinal stabilizersB. local spinal stabilizersC. spinai flexorsD. 5pinal extensors
Before progressing to Stage 2 of a stabilization programfor LBP, an individual must be able to perform extremitymovements pain-free in the supine position while main-taining
A. the co-contraction of the transverse abdominis andmultifidus muscles.
B. spinal stabilization during prone trunk extension for30 seconds.
C. spinal stabilization during standing on an unsteadysurface for 30 seconds.
D. the co-contraction of the local stabilizers while in thequadruped position.
An increase in the neutral zone of the spine caused by adegenerative change in the supporting passive structurespotentially results in which of the following?A. increased function of the stabilizersB. decreased number of ligamentsC. decreased injury risk .D. increased pain
Which of the following muscles is classified as a global sta-bilizer of the lower back?A. multifidusB. internal obliquesC. quadratus lumborumD. transverse abdominis
6.
7.
9.
10.
Which of the following musculatures specifically providesintersegmental stability?A. global spinal stabilizersB. local spinal stabilizersC. spinal flexorsD. spinal extensors
Which of the following describes the number of recom-mended exercises and the number sessions per week of aStage 1 stabilization program for LBP?
Number of exercisesA. 3B. 7C. 3D. 7
Sessions per week
7337
Which of the following muscles is classified as a local stabi-lizer of the lower back?
A. psoas majorB. external obliquesC. quadratus lumborumD. transverse abdominis
Which of the following is a Stage 3 exercise of a stabiliza-tion program for LBP that strengthens the quadratus lum-borum muscle?
A. side bridgeB. quadruped positionC. prone trunk extensionD. supine abdominal draw
Which of the following are goals of spinal stabilization ex-ercises to reduce low back pain?
I. improvefunctionII. restore muscle sizeIII. minimize coordinationIV. decrease insult tolerance
A. I and II onlyB. land lVon lyC. l land l l lon lyD. Ill and IV only
The answers to this quiz will appear in Vol. 29(3).
Answers to the CEU Quiz in Vol. 29(1) of the Strength and Conditioning Journal
1.B; 2.A; 3.A; 4.C; 5.B; 6.B; 7.C; 8.A; 9.A; 10.A
April 2007 • Strength and Conditioning Journal