Embed Size (px)
Citation preview

Lumbar Spine Differential Diagnosis
Jason Zafereo, PT, OCS, FAAOMPTCli i l O th di R h bilit ti Ed tiClinical Orthopedic Rehabilitation Education
1

Objectives
Describe the relevant findings from the history and examination indicating the source of symptoms as:examination indicating the source of symptoms as:
– Contractile tissue – Non-contractile tissue
Nerve Spine
Describe the relevant findings from the history andDescribe the relevant findings from the history and examination indicating a primary impairment of:
– StiffnessWeakness– Weakness
2
CONTRACTILE TISSUE PATHOLOGY
3
Subjective Exam Findings
Chief complaint: LBP Onset (QL): MVA or sustained Onset (QL): MVA or sustained
walking boot use Aggravating: Rolling over in
bed (QL) standing uprightbed (QL), standing upright (Iliopsoas) and walking (QL), coughing - sneezing (QL), sit to stand (ES), stairs (ES)to stand (ES), stairs (ES)
Easing (QL): pressure relief or short term corset use
– Travell and Simons 1992Travell and Simons 1992
4

Subjective Exam Findings--Location
Quadratus lumborum Iliopsoas Rectus Abdominus
Travell and Simons 1992, 19835
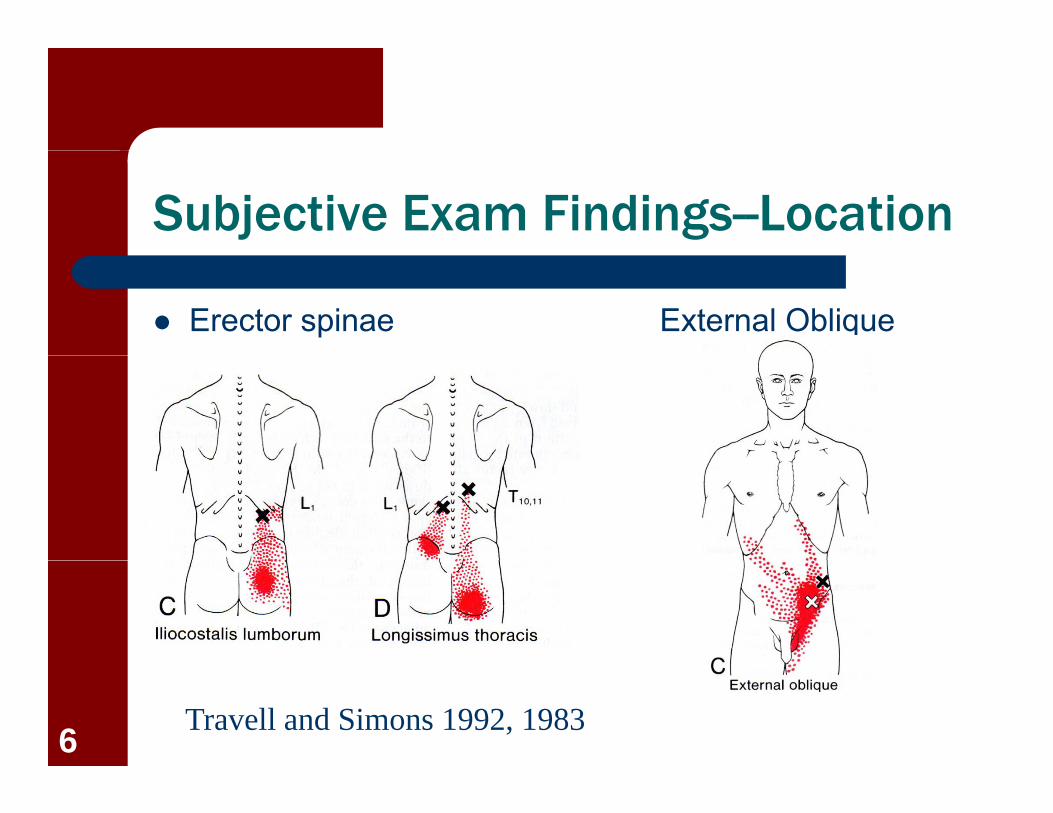
Subjective Exam Findings--Location
Erector spinae External Oblique
Travell and Simons 1992, 19836

Objective Exam Findings
Test ResponseAlignment Elevated ipsilateral crest (QL); Forward trunk g p ( );
lean (Iliopsoas)ROM/Flexibility Restricted flexibility of involved muscle; Active
and Passive ROM painful in opposite directions; LROM significantly limited sagittal plane and contralateral sidebending (QL); marked limitation of flexion (ES)
M scle Pro ocation Testing Painf l possibl eak (no atroph )Muscle Provocation Testing Painful, possibly weak (no atrophy)Palpation 1) Focal tenderness with concordant sign
reproduction (about 3kg of pressure)2) Twitch response2) Twitch response3) Taut band4) Often referred pain (non dermatomal) on
continued (~5sec) pressure7

NON-CONTRACTILE TISSUE PATHOLOGY
8

Nerve
Cauda Equina S dSyndrome
Disc Herniation with R di l thRadiculopathy
Lumbar Spine StenosisStenosis
9

Subjective Exam Findings—Cauda Equina Syndrome
Numbness around the buttocks Walking almost causes urination Walking almost causes urination Burning sensation around the buttocks Numbness in the soles of both feet Numbness in both legs Numbness without pain +LRs ≥ 2, p < 0.05p
– Konno et al, BMC Musc Disorders, 2007
10

Subjective Exam Findings—HNP with Radiculopathy
Age 15-40O t ith lifti Onset with lifting
Pain aggravated with sitting easedwith sitting, eased with standing/walking
Pain with valsalva, cough, laugh, sit to standstand– Magee 2008
11
Subjective Exam Findings—Lumbar Spine Stenosis
No pain or sx improved when sittingsitting
Age>48 years Leg pain>back pain Bilateral symptoms Pain during walking/standing
-LR = 19 +LR = 4 6– -LR = .19, +LR = 4.6 – Pre-test probability = 40%– 4/5 = 76%
5/5 = 99+%– 5/5 = 99+%Katz et al, Arth Rheum, 1995; Cook et
al, 201112

Subjective Exam Findings--Location
L4 L5 S1
13
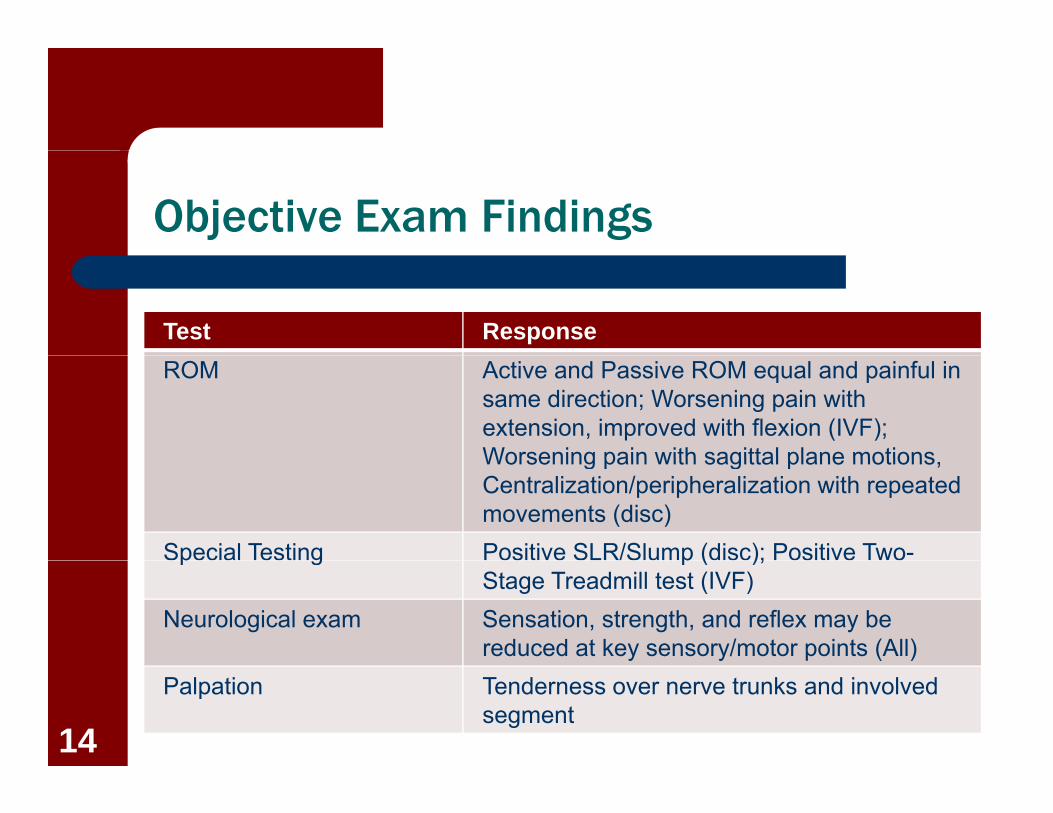
Objective Exam Findings
Test ResponseROM Active and Passive ROM equal and painful in
same direction; Worsening pain with extension, improved with flexion (IVF); Worsening pain with sagittal plane motionsWorsening pain with sagittal plane motions, Centralization/peripheralization with repeated movements (disc)
Special Testing Positive SLR/Slump (disc); Positive Two-p g p ( );Stage Treadmill test (IVF)
Neurological exam Sensation, strength, and reflex may be reduced at key sensory/motor points (All)
Palpation Tenderness over nerve trunks and involved segment
14

SLR
Validity (pooled)SLR S iti it 85– SLR Sensitivity = .85, Specificity = .52
– Crossed SLR Sensitivity 29 S ifi it 88= .29, Specificity = .88
Reliability– SLR K = .70
– Rubinstein and van Tulder, Best Pract & Res Clin Rheum, 2008
– van der Windt et al 201015
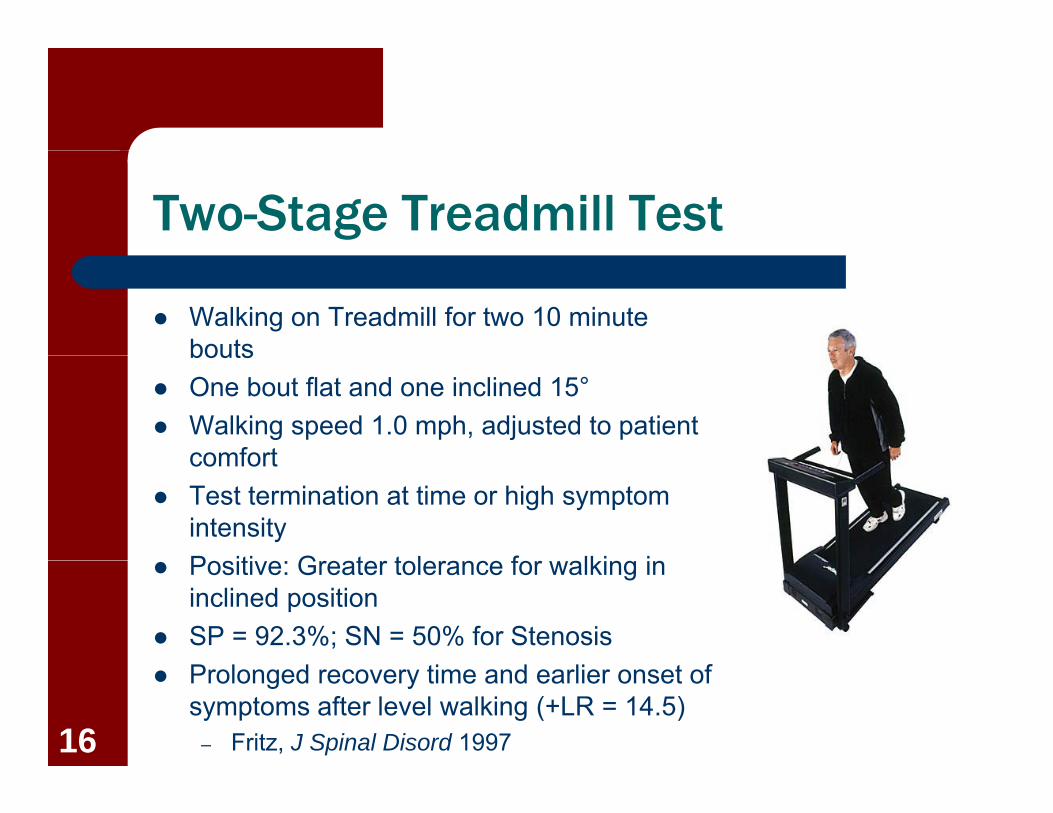
Two-Stage Treadmill Test
Walking on Treadmill for two 10 minute boutsbouts
One bout flat and one inclined 15° Walking speed 1.0 mph, adjusted to patient
comfortcomfort Test termination at time or high symptom
intensityP iti G t t l f lki i Positive: Greater tolerance for walking in inclined position
SP = 92.3%; SN = 50% for Stenosis Prolonged recovery time and earlier onset of
symptoms after level walking (+LR = 14.5)– Fritz, J Spinal Disord 199716

Joint/Disc
Differential diagnosis is difficultdifficult
– Shared pain referral patterns– Inconsistent lumbar coupling
Key to diagnosis lies with cluster testing based on history imaging and ROMhistory, imaging, and ROM findings
17
Subjective Exam Findings--Joint
Age >65P i t d ith Pain not worsened with
– Coughing– Hyperextensionyp– Forward flexion– Extension-rotation
Rising from a chair– Rising from a chair
Pain relieved by recumbency*– 5 of 7 present suggests joint pain (+LR = 2.6-2.8, -LR = .06-
.88) Revel et al, Spine, 1998 Laslett, BMC Musc Dis, 200418

Subjective Exam Findings--Joint
Positive Extension-Rotation testtest
Age ≥ 50 Best when walking Best when walking Best when sitting Pain is paraspinal
– 3 of 5 present suggest relief with ZJ block (+LR 9.7)
– Extension-Rotation test (SN = te s o otat o test (S100%)
– Laslett et al, Spine J, 200619
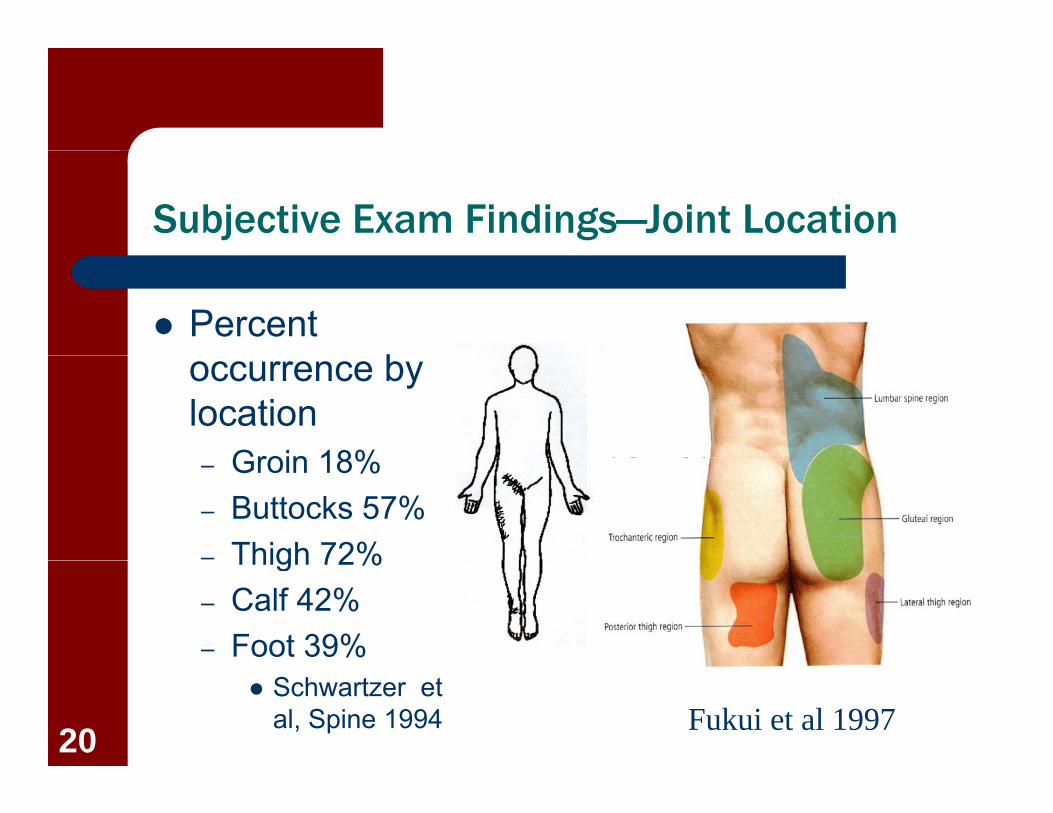
Subjective Exam Findings—Joint Location
Percent boccurrence by
locationGroin 18%– Groin 18%
– Buttocks 57%– Thigh 72%Thigh 72%– Calf 42%– Foot 39%
Schwartzer et al, Spine 1994 Fukui et al 199720

Subjective Exam Findings--Disc
Pain while rising from sittingsitting
Young et al 2003
Imaging– Degenerative disc on MRI
(-LR = .21) – Imaging suggestive of g g gg
high intensity zone, endplate changes, or degeneration (+LR > 2) Hancock et al 2007
21
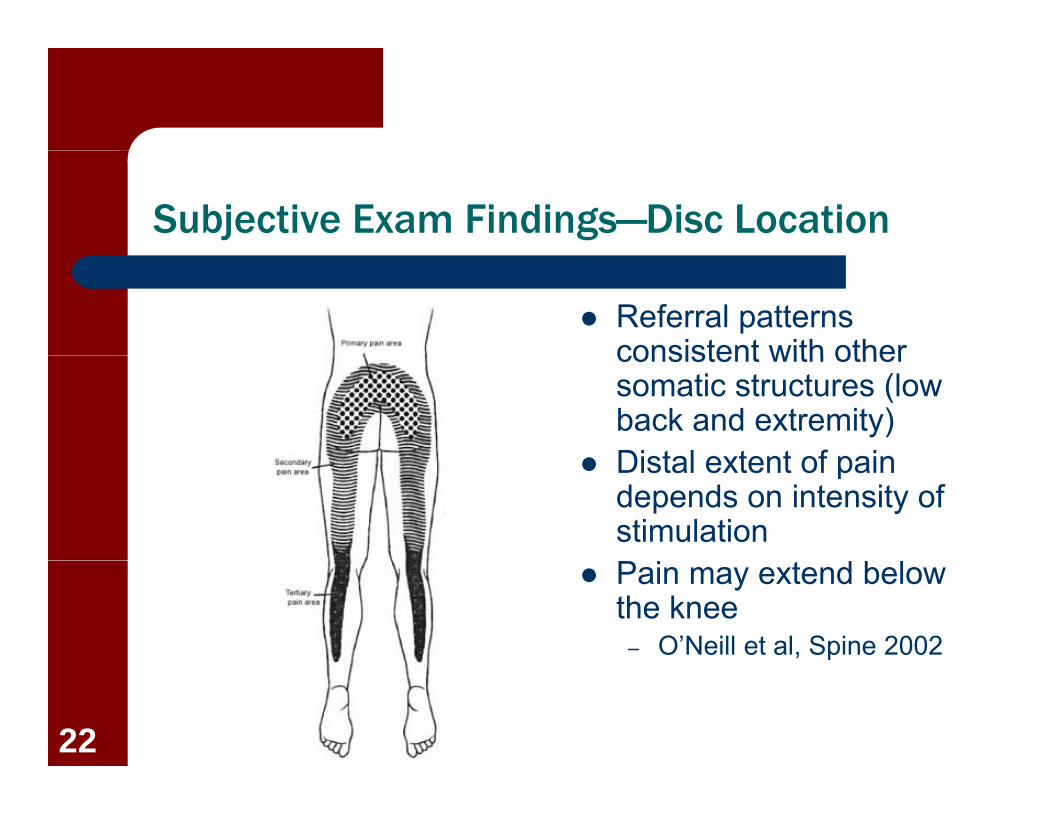
Subjective Exam Findings—Disc Location
Referral patterns consistent with otherconsistent with other somatic structures (low back and extremity)
Distal extent of pain Distal extent of pain depends on intensity of stimulation
Pain may extend below the knee
– O’Neill et al, Spine 2002
22

Objective Exam Findings
Test ResponseROM Active and Passive ROM painful in same
direction; 3-D combined movements most painful (Ext/Rot): Joint; Significant loss of
t i l bilit d i idextension, vulnerability during mid-range flexion/rotation, and centralization yields +LR of 6.7 for disc (Laslett et al. 2006)
Special Tests May have positive dural testing: DiscSpecial Tests May have positive dural testing: DiscPalpation Tenderness over involved jointsAlignment Presence of acute lateral shift or lumbar
kyphosis: Disckyphosis: Disc
23
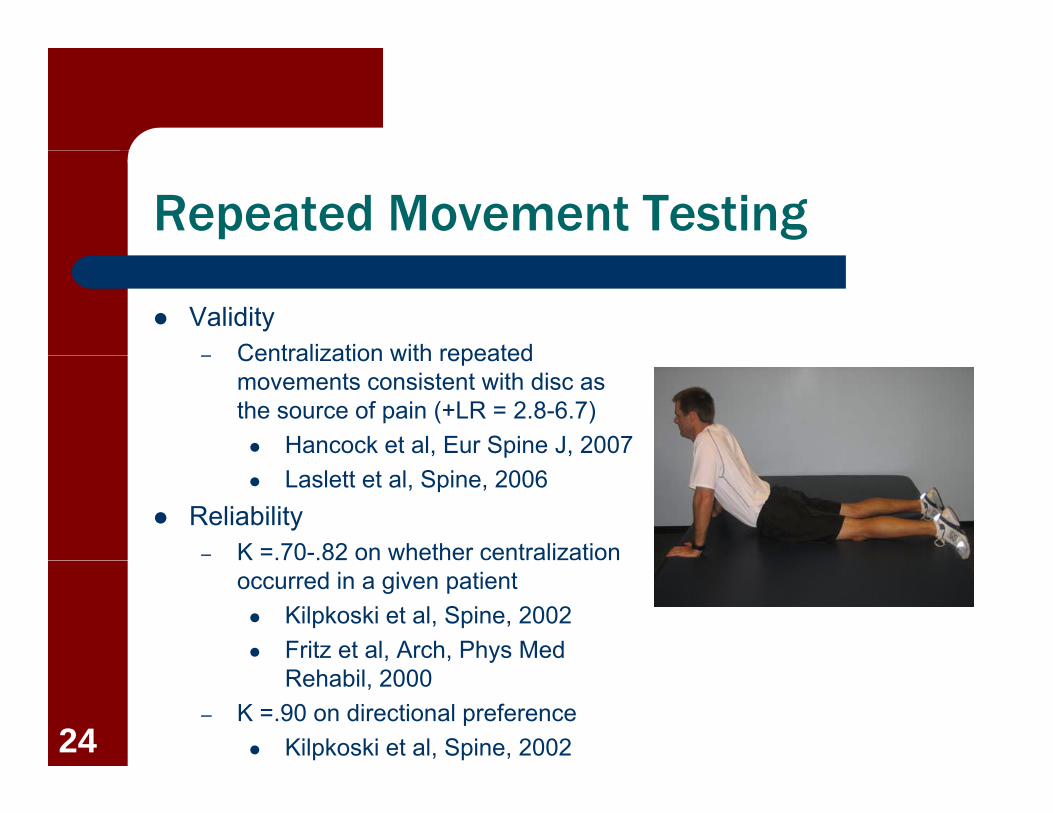
Repeated Movement Testing
Validity– Centralization with repeated– Centralization with repeated
movements consistent with disc as the source of pain (+LR = 2.8-6.7) Hancock et al, Eur Spine J, 2007 Laslett et al, Spine, 2006
Reliability– K =.70-.82 on whether centralization
occurred in a given patient Kilpkoski et al, Spine, 2002 Fritz et al, Arch, Phys Med
Rehabil, 2000– K =.90 on directional preference
Kilpkoski et al, Spine, 200224

PRIMARY STIFFNESS IMPAIRMENT
25
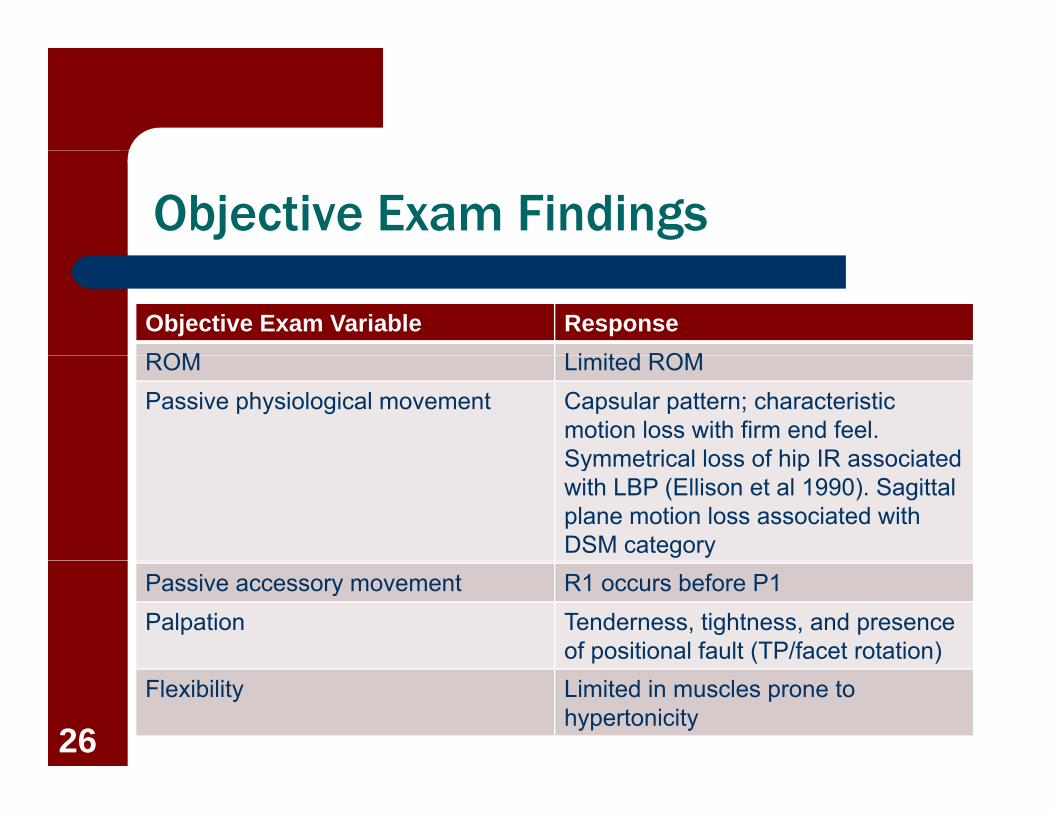
Objective Exam Findings
Objective Exam Variable ResponseROM Li it d ROMROM Limited ROMPassive physiological movement Capsular pattern; characteristic
motion loss with firm end feel. Symmetrical loss of hip IR associatedSymmetrical loss of hip IR associated with LBP (Ellison et al 1990). Sagittal plane motion loss associated with DSM category
Passive accessory movement R1 occurs before P1Palpation Tenderness, tightness, and presence
of positional fault (TP/facet rotation)p ( )Flexibility Limited in muscles prone to
hypertonicity26

Lumbar ROM Diagram
27

Lumbar Cardinal Plane Patterns
28

Reliability of Palpation/Motion Testing
Reliability (pooled)ID f t t (K 53)– ID of osseous structures (K = .53)
– Motion assessment all levels (K = .17)– Pain assessment all levels (K = .42)
Stochkendahl et al, J Manip Phys Ther, 2006
– Most hypomobile segment (K = .71)– Most hypermobile segment (K = .29)
Landel et al, PT 2008
Validity Validity– Poor agreement (K = 0-.04) with MRI
Landel et al, PT 2008 29
Validity of Palpation/Motion Testing
Segmental PA exam findings used to predict response to p pmanipulation or stabilization treatments
– Findings of hypomobility Failure rates were 26% with
manipulation, 74.4% with stabilization
– Findings of hypermobilityg y y Failure rates were 83.3% with
manipulation, 22.2% with stabilization
– Fritz et al Arch Phys Med Rehabil, y ,2005
30

Common Motor Patterns
Ventral hyperactive
Dorsal hyperactive musculaturehyperactive
musculature– Hip adductors
musculature– Triceps surae– Hamstrings
– Rectus femoris– TFL– Iliopsoas
– Lumbar erector spinae
– Quadratus Iliopsoas– Oblique
abdominals
lumborum
31
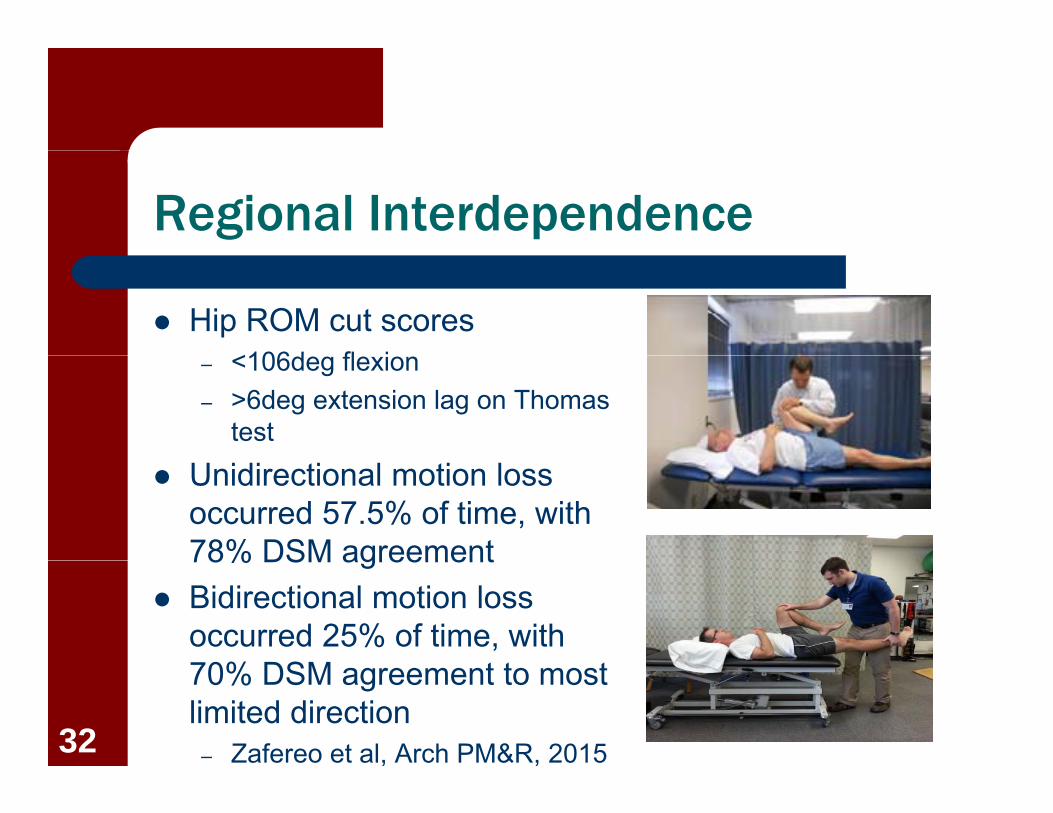
Regional Interdependence
Hip ROM cut scores<106d fl i– <106deg flexion
– >6deg extension lag on Thomas test
Unidirectional motion loss occurred 57.5% of time, with 78% DSM agreement78% DSM agreement
Bidirectional motion loss occurred 25% of time, with 70% DSM t t t70% DSM agreement to most limited direction
– Zafereo et al, Arch PM&R, 201532

PRIMARY WEAKNESS IMPAIRMENT
33
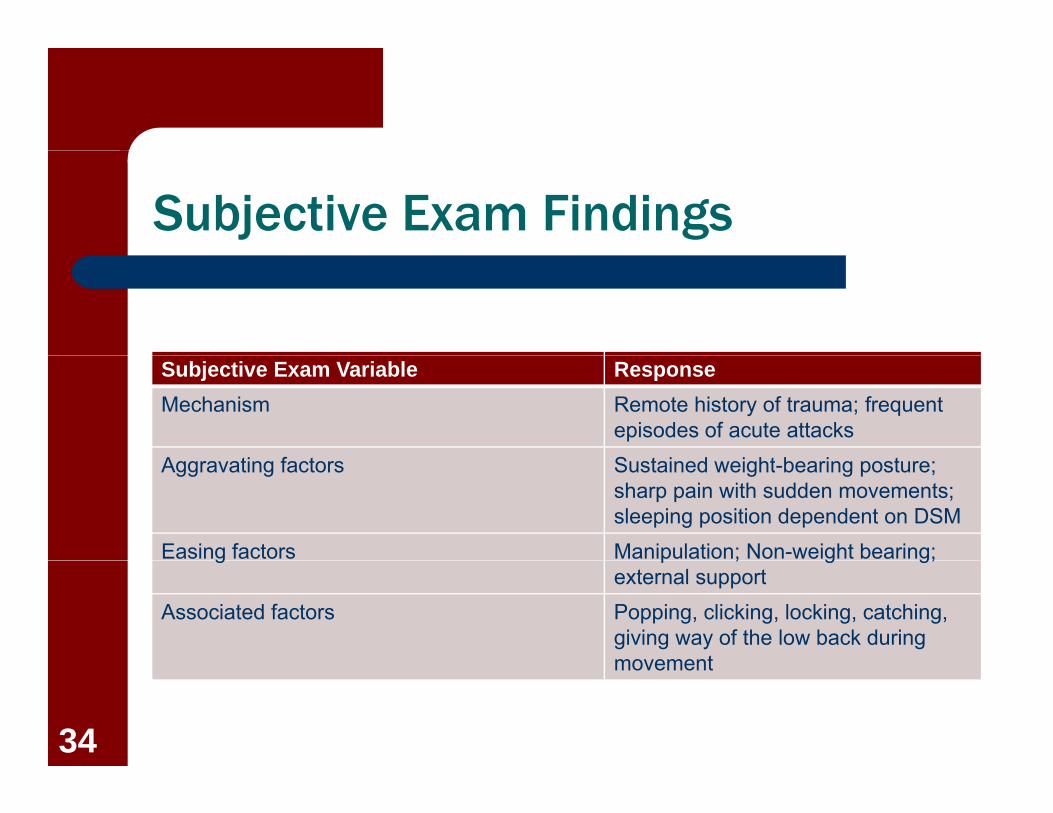
Subjective Exam Findings
Subjective Exam Variable ResponseMechanism Remote history of trauma; frequent
episodes of acute attacksA ti f t S t i d i ht b i tAggravating factors Sustained weight-bearing posture;
sharp pain with sudden movements; sleeping position dependent on DSM
Easing factors Manipulation; Non-weight bearing; g p ; g g;external support
Associated factors Popping, clicking, locking, catching, giving way of the low back during movementmovement
34
Objective Exam Findings
Objective Exam Variable ResponseActive movements Full general mobility with aberrant motion;Active movements Full general mobility with aberrant motion;
hinging, pivoting, fulcruming*. Greater ROM in lying than in sitting/standing
Passive physiological Full with decreased resistance to end range. ass e p ys o og camovement
u t dec eased es sta ce to e d a geLumbar pain with hip ROM testing*.
Passive accessory movement
Increased neutral zone and shear
Special Testing Positive Prone instability test; Positive leg raise tests*; Positive BKFO*
Strength testing Weakness/poor coordination TRA, multifidus, g g pHip extension/abduction (Nadler et al 2001)
Palpation Atrophy of multifidus segmentally; Paraspinal muscle guarding/hypertrophy*35

Defining Aberrant Movement
Altered Lumbopelvic RhythmForward bending: Hip>lumbar in first third; lumbar>hip during last– Forward bending: Hip>lumbar in first third; lumbar>hip during last third
– Extension: Lumbar>hip in first third; hip>lumbar during last third Gower’s sign Gower s sign Deviation from sagittal plane Instability catch, shake, or judder
P i f l f ti Painful arc of motion
Fair to excellent (K=.35-.89) agreement for individual signs Substantial (K=.65) agreement for at least 1 sign Biely et al, 201436

Identification of Radiographic Lumbar Instability
Age <37 years Total extension >26deg Any hypermobility of
the lumbar spinethe lumbar spine Lack of hypomobility of
the lumbar spine* Lumbar flexion
>53deg** +LR = 12 8; LR = 72* +LR = 12.8; -LR = .72
Fritz et al., Eur Spine J 200537

Identification of Radiographic Identification of Radiographic Instability
SpondylolysisO l d– One-legged hyperextension test had low to moderate sensitivity (50% 73%)sensitivity (50%–73%) and low specificity (17%–32%)
Spondylolisthesis Spondylolisthesis– Lumbar SP palpation had
high specificity (87%–100%) d d t t100%) and moderate to high sensitivity (60–88)
Algarni et al, 201538
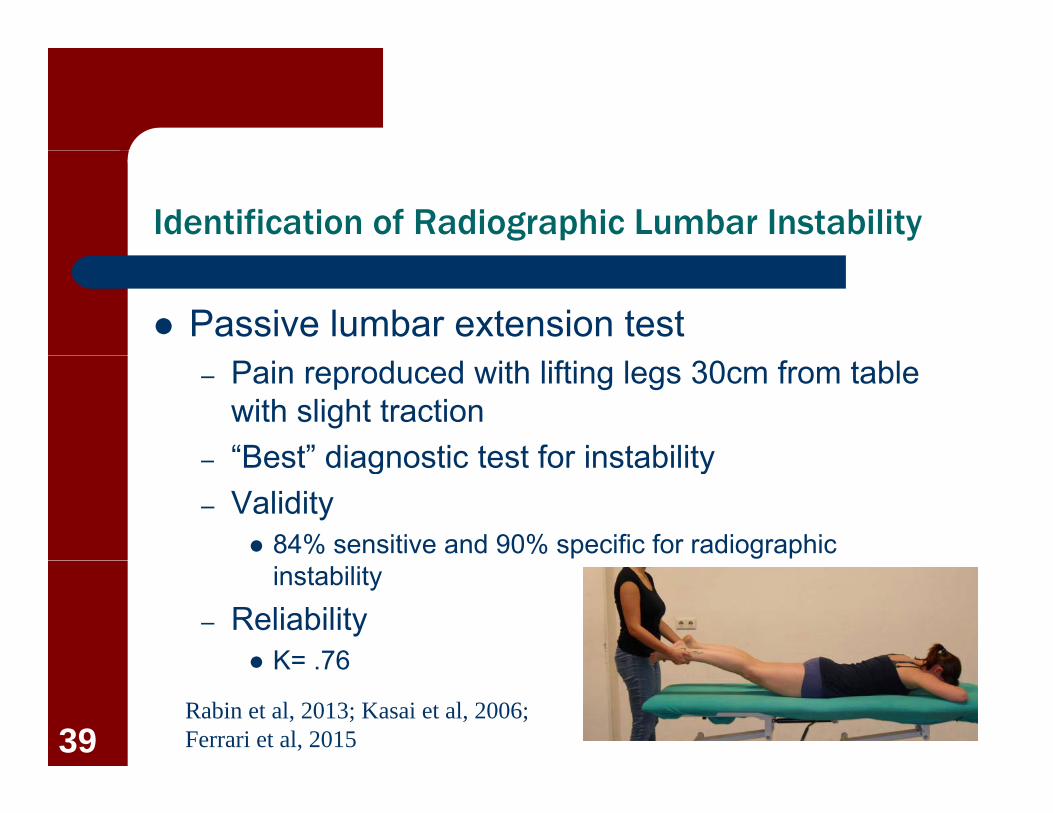
Identification of Radiographic Lumbar Instability
Passive lumbar extension test– Pain reproduced with lifting legs 30cm from table
with slight traction“Best” diagnostic test for instability– Best diagnostic test for instability
– Validity 84% sensitive and 90% specific for radiographic
instability
– Reliability K= 76 K= .76
Rabin et al, 2013; Kasai et al, 2006; Ferrari et al, 201539
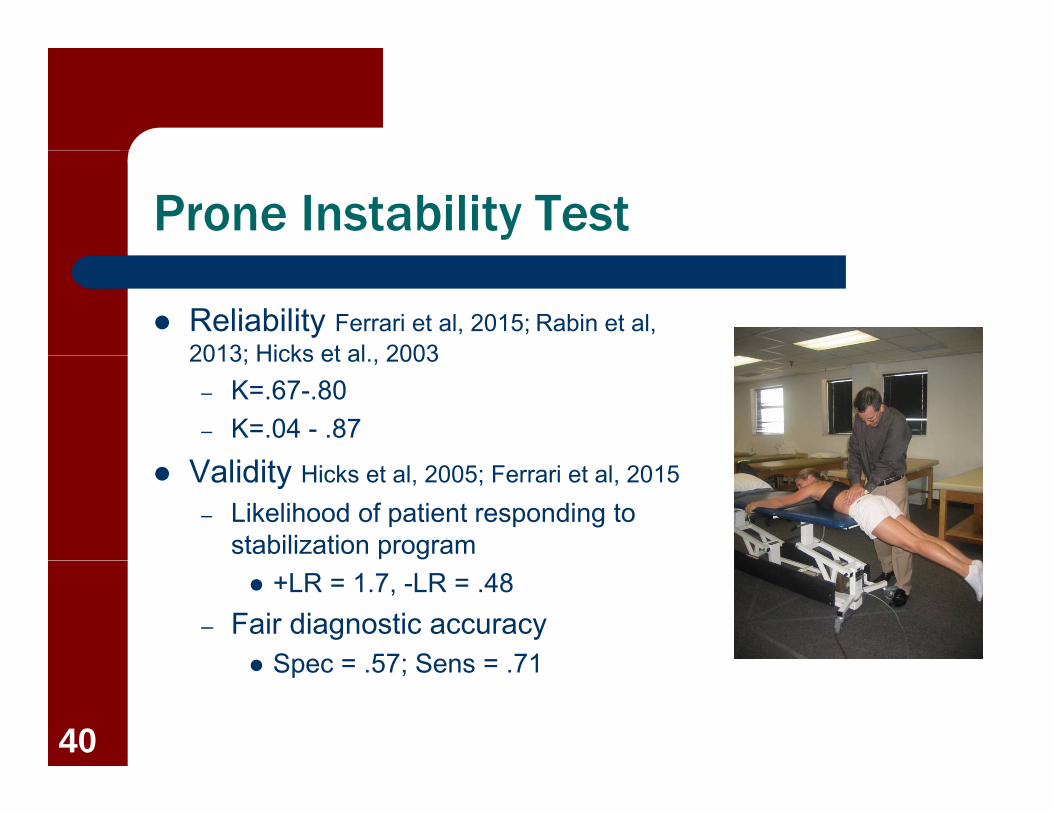
Prone Instability Test
Reliability Ferrari et al, 2015; Rabin et al, 2013; Hicks et al 20032013; Hicks et al., 2003
– K=.67-.80– K=.04 - .87
Validity Hicks et al, 2005; Ferrari et al, 2015– Likelihood of patient responding to
stabilization program +LR = 1.7, -LR = .48
– Fair diagnostic accuracy Spec = 57; Sens = 71 Spec = .57; Sens = .71
40

Common Motor Patterns
Dorsal hypoactive musculaturemusculature
– Gluteals
Ventral hypotonic musculature
– Tibialis anterior– Toe extensors– Peronei– Vasti
Rectus abdominus– Rectus abdominus
41
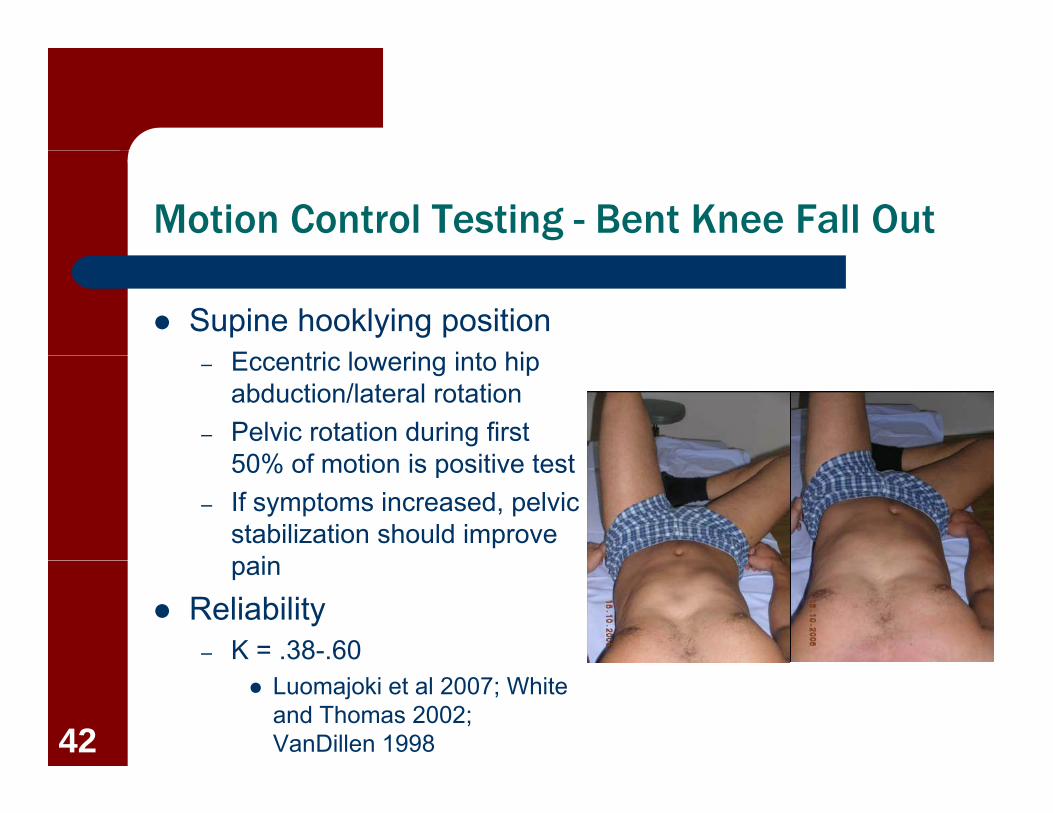
Motion Control Testing - Bent Knee Fall Out
Supine hooklying positionE t i l i i t hi– Eccentric lowering into hip abduction/lateral rotation
– Pelvic rotation during first 50% f ti i iti t t50% of motion is positive test
– If symptoms increased, pelvic stabilization should improve
ipain
Reliability– K = .38-.60
Luomajoki et al 2007; White and Thomas 2002; VanDillen 199842
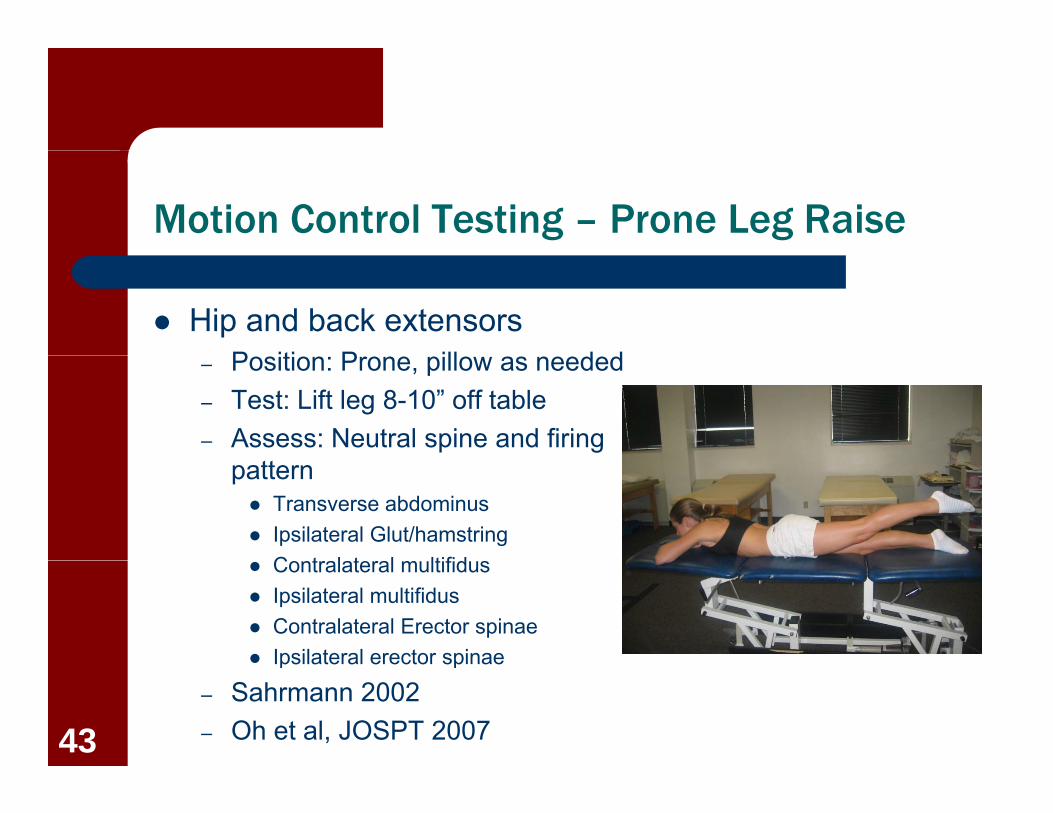
Motion Control Testing – Prone Leg Raise
Hip and back extensorsP iti P ill d d– Position: Prone, pillow as needed
– Test: Lift leg 8-10” off table– Assess: Neutral spine and firing
pattern Transverse abdominus Ipsilateral Glut/hamstring
C t l t l ltifid Contralateral multifidus Ipsilateral multifidus Contralateral Erector spinae Ipsilateral erector spinaeIpsilateral erector spinae
– Sahrmann 2002– Oh et al, JOSPT 200743

Motion Control Testing – Prone Leg Raise
Reliability of hip extension testextension test
– K = .72-.76 for agreement on deviation in frontal, t itt ltransverse, or sagittal plane Murphy et al 2006
Gluteus maximus time to contraction significantly reduced by pelvic y pcompression
– Takasaki et al 200844

Strength Testing-Hip Extensors
Static double leg b id ibridging– Reliability
ICC= 84 ICC=.84
– Expected holds Patients with LBP =
76.7secs Patients without
LBP=172.9secs (after 2 mins, unilateral)
– Schellenberg et al, Am J Phys Med Rehabil 200745

Motion Control Testing – Sidelying Leg Raise
Gluteus medius/minimusP iti Sid l i ith b th– Position: Sidelying with both legs fully extended, neutral hip, relaxed ankle, top arm off the tableoff the table
– Test: Frontal plane hip ABD smooth and easyS b tit ti U t ll d– Substitutions: Uncontrolled and rapid, Flexion/IR of hip, and forward rolling of pelvis, trunk shouldertrunk, shoulder
46

Motion Control Testing – Sidelying Leg Raise
Interrater Reliability– Reported as poor to
acceptable Rabin et al, JOSPT 2013; ab et a , JOS 0 3;
Davis et al, JOSPT 2011
Validity– +LR 2.68-4.59 in
discriminating development of LBP in pasymptomatic population Nelson-Wong et al, JOSPT
2009 and Clin Biomech 200847
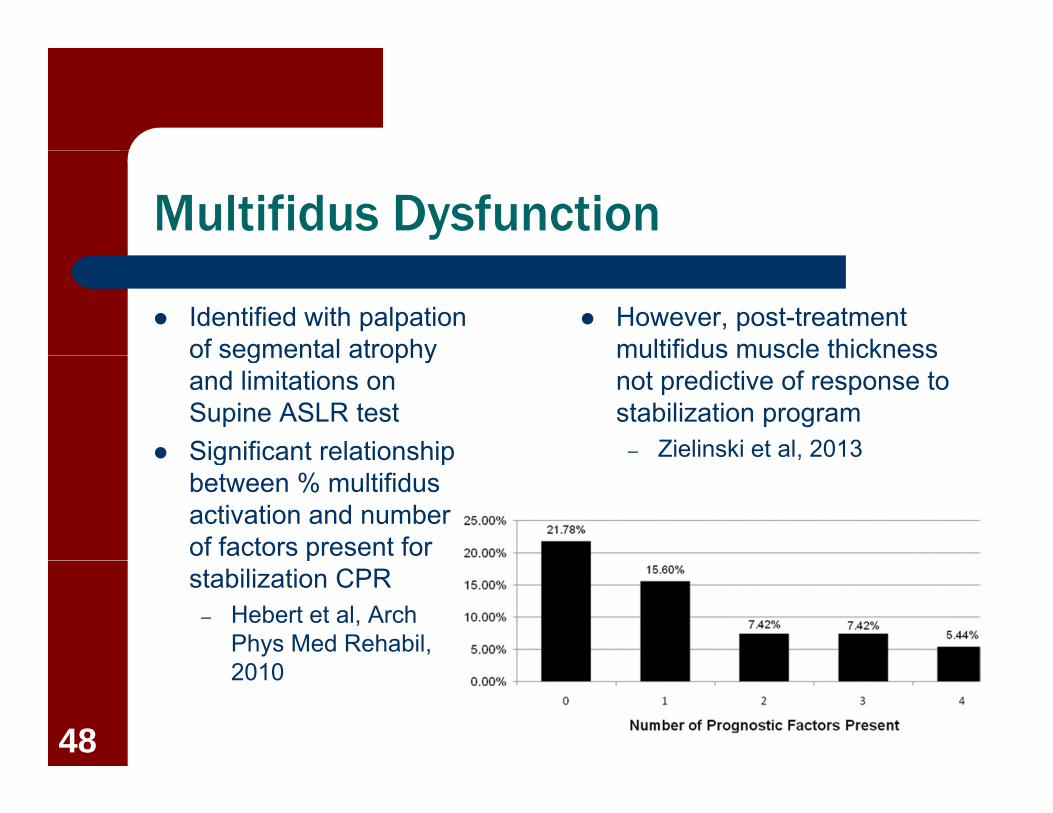
Multifidus Dysfunction
Identified with palpation of segmental atrophy
However, post-treatment multifidus muscle thicknessof segmental atrophy
and limitations on Supine ASLR test
Significant relationship
multifidus muscle thickness not predictive of response to stabilization program
– Zielinski et al, 2013 Significant relationship between % multifidus activation and number of factors present for
,
pstabilization CPR
– Hebert et al, Arch Phys Med Rehabil, 20102010
48

Strength Testing-Trunk Extensors
Prone double SLR highly correlated with developmentcorrelated with development and persistence of LBP
– Males <30secs– Females<29secs
Prone chest raise cut scoresMales >31secs– Males >31secs
– Females >33secs
Reliability (ICC=.90)
– Arab et al, Clin Rehabil 2007
49

Motion Control Testing – Supine Leg Raise
ProcedureSt bili t 40 H
Successful completion of this test not an indication of– Stabilizer to 40mmHg
– Drawing in with relaxed normal breathing
this test not an indication of high TRA activation on US imaging
Grooms et al 2013 Test
– Maintain pressure at 40-43mmHg with the
– Grooms et al, 2013
gfollowing movements Heel slide 3 inch march SLR (8-10”)
50
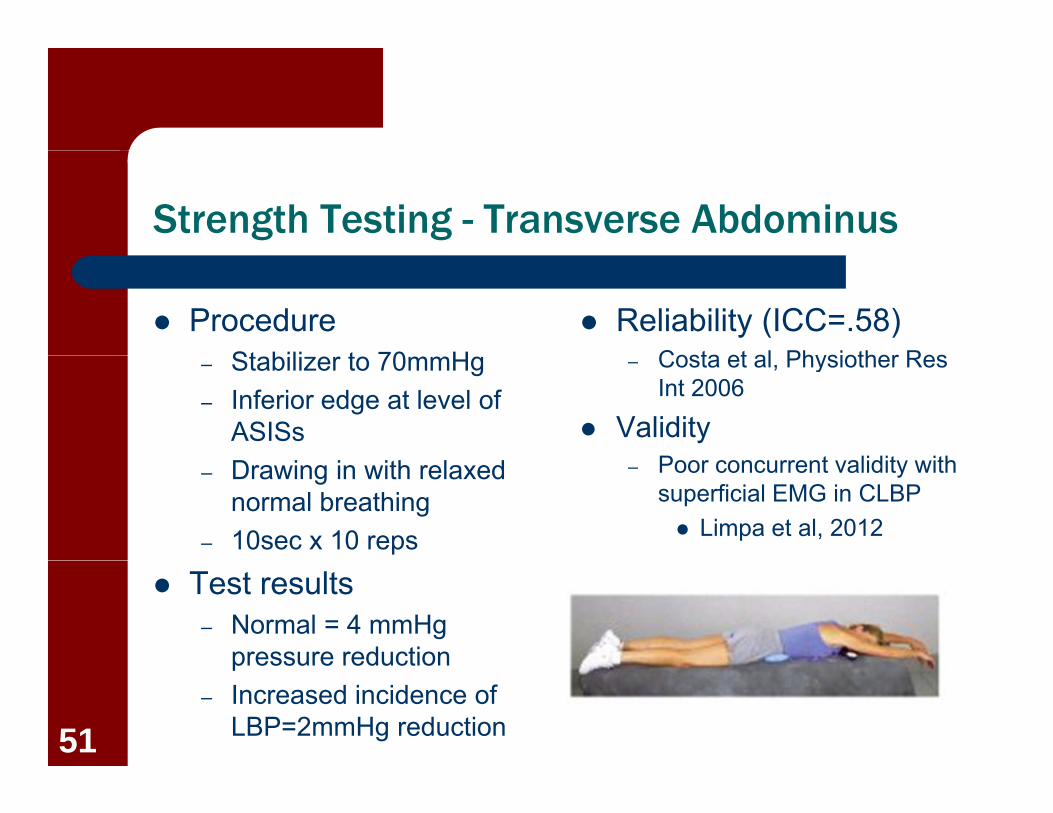
Strength Testing - Transverse Abdominus
ProcedureSt bili t 70 H
Reliability (ICC=.58) Costa et al Physiother Res– Stabilizer to 70mmHg
– Inferior edge at level of ASISs
– Costa et al, Physiother Res Int 2006
ValidityP t lidit ith– Drawing in with relaxed
normal breathing– 10sec x 10 reps
– Poor concurrent validity with superficial EMG in CLBP Limpa et al, 2012
Test results– Normal = 4 mmHg
pressure reductionpressure reduction– Increased incidence of
LBP=2mmHg reduction51

Strength Testing – Trunk Flexors
Double leg loweringG t lik lih d f CLBP if– Greater likelihood of CLBP if anterior pelvic tilt above 50deg hip flexion in males
60d hi fl i i f l 60deg hip flexion in females– Youdas et al, PT 2000
Prone planking– Expected holds
Patients with LBP = 28.3secs Patients without
LBP=72.5secs– Schellenberg et al, Am J Phys Med
Rehabil 200752

Summary of Stabilization Findings
Examples of Motion Control Testing
3/6 positive findings used as criteria for prescribingControl Testing
– Lumbopelvic rhythm– Pattern of motion lumbar
as criteria for prescribing stabilization program
Significant improvements sidebending/rotation toward paraspinal bulk
– Passive Hip ROM
g pin pre-post testing, pain, disability
Luomajoki et al 2010– Active leg raises (sagittal)– Active leg raise (frontal)– Bent knee fall out
– Luomajoki et al 2010
Bent knee fall out
53