Embed Size (px)
Citation preview
Lower respiratory tract
• Lungs are axenic (no normal flora)– Pneumonia
• Described by location, pathogen or way contracted
– Pleurisy
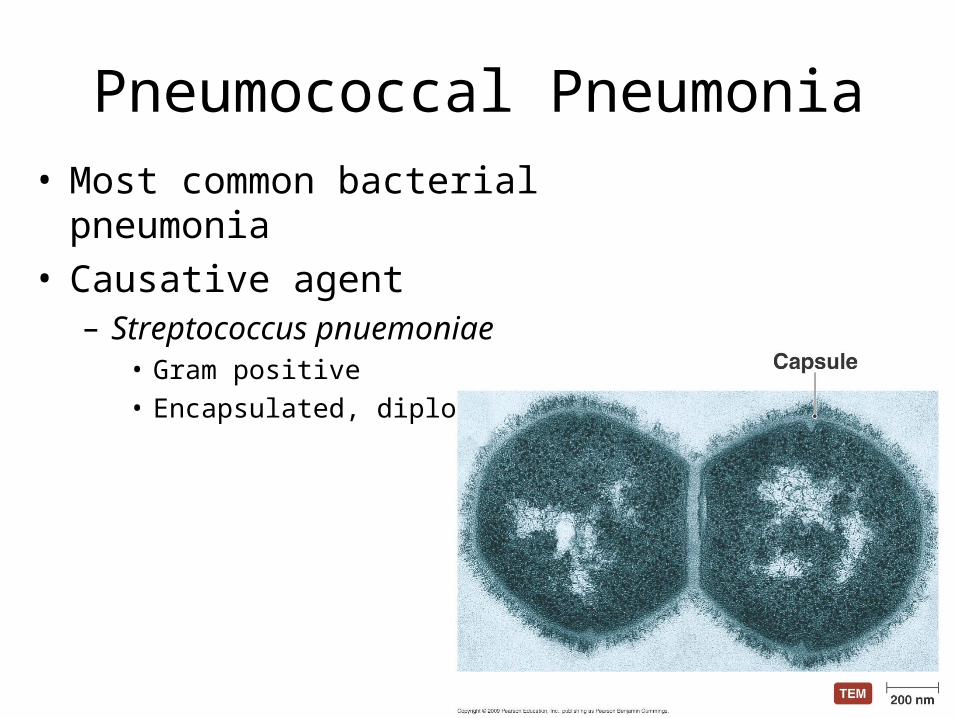
Pneumococcal Pneumonia• Most common bacterial pneumonia• Causative agent
– Streptococcus pnuemoniae• Gram positive• Encapsulated, diplococci
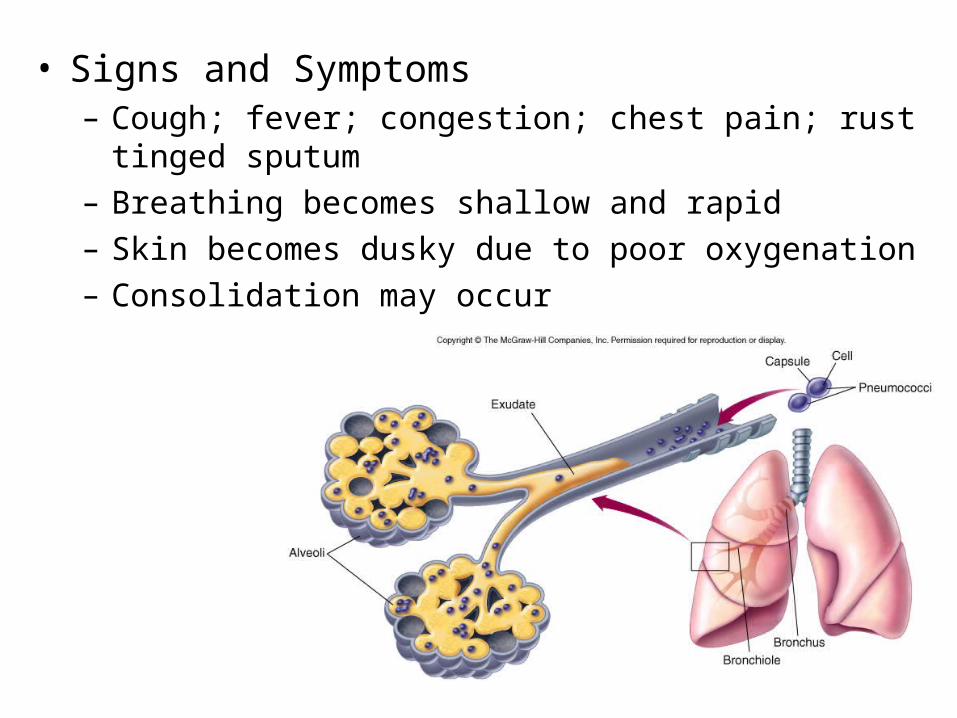
• Signs and Symptoms– Cough; fever; congestion; chest pain; rust tinged sputum– Breathing becomes shallow and rapid– Skin becomes dusky due to poor oxygenation– Consolidation may occur
– Recovery is usually complete• Most strains do not cause permanent damage to
lung tissue
– Complications • Pleural effusions• Septicemia• Endocarditis • Meningitis
• Epidemiology– 75% of healthy individuals carry encapsulated
strain in their throat• Bacterial rarely reach lung • Risk of pneumonia rises when cilia destroyed
• Gram stain of sputum used for diagnosis • Pneumococci confirmed with quelling reaction
• Bacteria that reach alveoli cause inflammatory response
• Adhesions • Capsule• Phosphorylocholine in cell wall• Pneumolysin (cytotoxin)• IGA proteases
• Prevention – Pneumococcal vaccine
• Treatment– Antibiotics successful if given early
• Penicillin (some resistance) • Erythromycin, cephalosporin and chloramphenicol
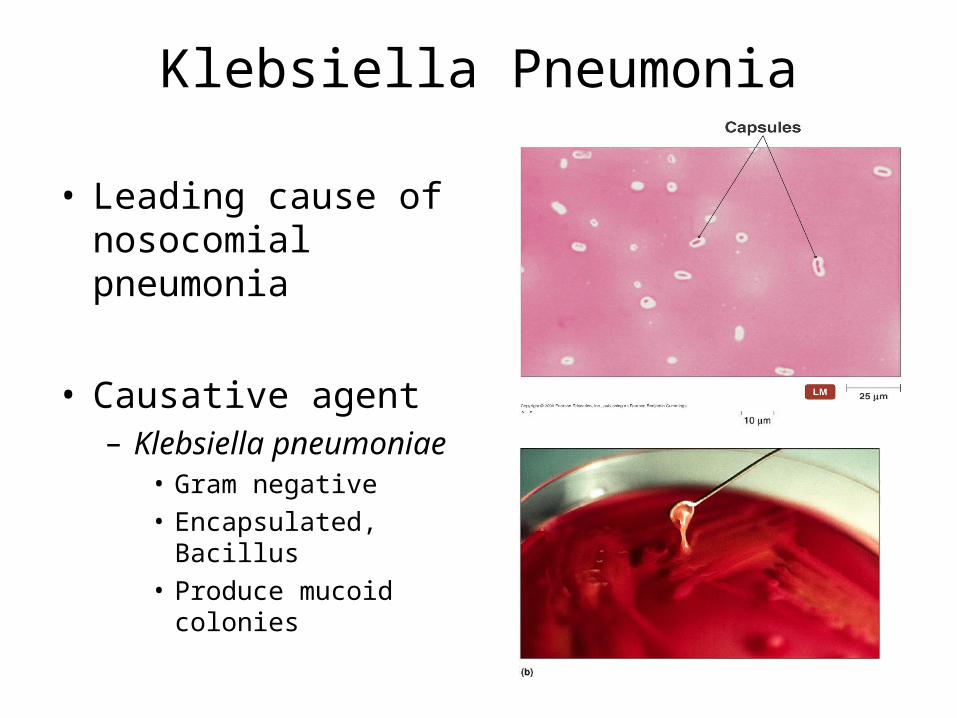
Klebsiella Pneumonia
• Leading cause of nosocomial pneumonia
• Causative agent– Klebsiella pneumoniae
• Gram negative• Encapsulated, Bacillus• Produce mucoid colonies
• Signs and Symptoms:– Typical pneumonia symptoms combined with
a thick, bloody sputum and recurrent chills
– Organism causes tissue death• Leads to formation abscess in lung or other tissues • Endotoxin can trigger shock and disseminated
intravascular coagulation
• Epidemiology– Endogenous – Difficult for K. pneumoniae to infect lungs of
healthy persons • Leading causes of nosocomial death• Also causes UTI, meningitis and wound infections
– Diagnosed with chest x-ray and sputum culture
• Prevention – No vaccine available – Employ good aseptic technique
• Treatment– Antimicrobial treatment limited
• Cephalosporin combined with an aminoglycoside• Tissue damage and release of endotoxin can cause
permanent damage to lungs • High fatalities even with treatment
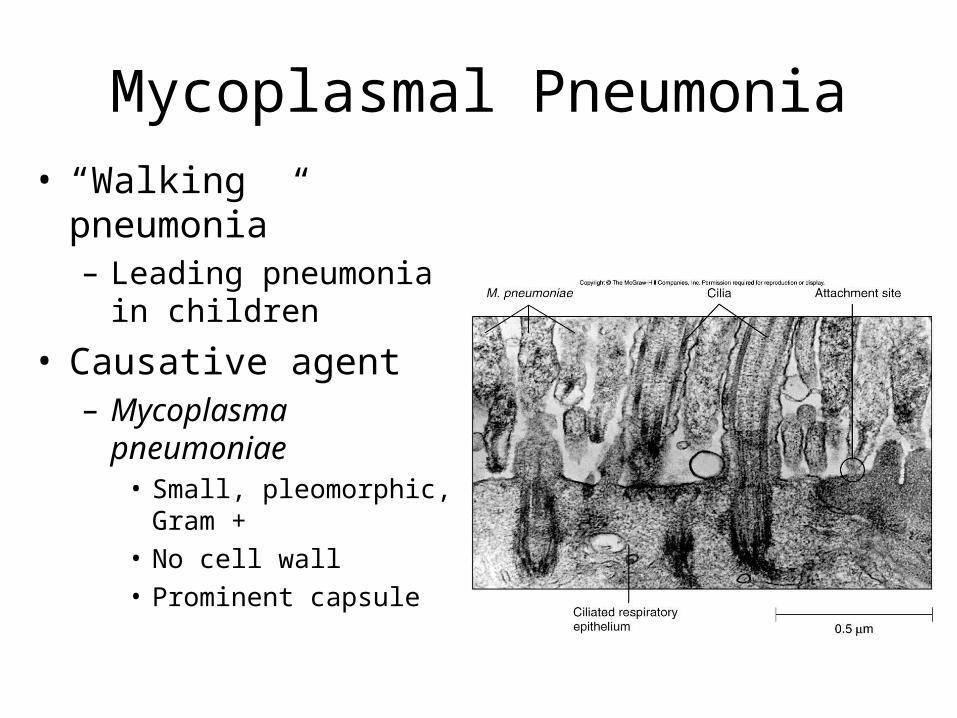
Mycoplasmal Pneumonia• “Walking pneumonia”
– Leading pneumonia in children
• Causative agent– Mycoplasma
pneumoniae• Small, pleomorphic,
Gram + • No cell wall• Prominent capsule
• Signs and Symptoms– Onset is gradual
• 1-4 week incubation period
– First symptoms include• Fever, headache, muscle pain, fatigue, sore throat
and excessive sweating • atypical for pneumonia• Persistent dry cough for several weeks
• Organism attaches to receptors on epithelium– Adhesion protein – Interferes with cilia, cells die and slough off– Capsule protects it from phagocytosis – Inflammation initiates thickening of bronchial and
alveolar walls• Causes difficulty in breathing
• Epidemiology– Spread through aerosol droplets
• Survive for long periods in secretions
– Grow slowly in culture • 2-6 weeks for “fried egg” colonies to appear
– Diagnosis difficult• Serological tests required
• Prevention and treatment– No practical prevention
• Avoid crowding in schools and military facilities• Aseptic technique
– Antibiotic treatment• Penicillins are ineffectual (WHY?)• Antibiotics of choice are tetracycline and erythromycin
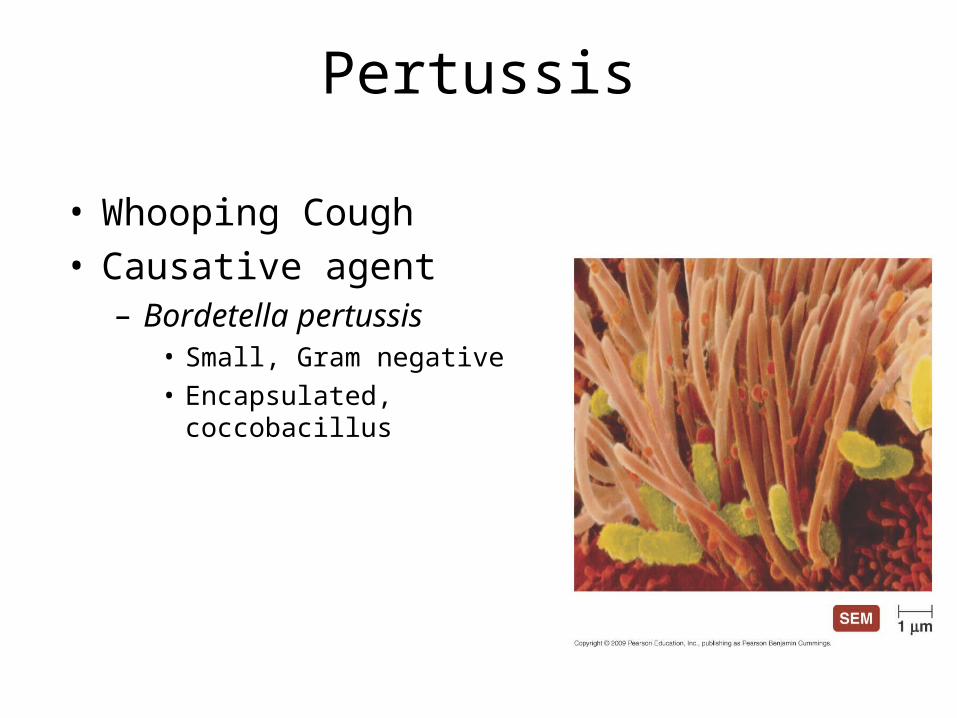
Pertussis
• Whooping Cough• Causative agent
– Bordetella pertussis• Small, Gram negative• Encapsulated, coccobacillus
• Signs and Symptoms:– Catarrhal stage – cold symptoms (1-2 weeks)
– Paroxysmal stage – severe coughing (2-4 weeks)• Coughing followed by characteristic “whoop”• May cause vessels in eyes to rupture • Cyanosis• Vomiting, diarrhea and seizure may occur
– Convalescent phase –persistent cough (months)
• Pathogen enters respiratory tract and attaches to ciliated cells– Produces 2 forms of adhesions
• Colonizes upper and lower respiratory tract
– Produces numerous toxic products • Mucus secretion increases and cilia action decreases• Cough reflex is only mechanism for clearing
secretions• Decreased blood flow and WBC activity
• Epidemiology– Spreads via infected respiratory droplets– Highly contagious – Most infectious during runny nose period– Classically disease of infants– Often overlooked as a persistent cold in adults
– High risk of secondary infections!
• Prevention – Immunization
• Combined with Diphtheria and tetanus toxoids
• DTaP
• Treatment– Primarily supportive – Erythromycin may reduce infectivity if given early
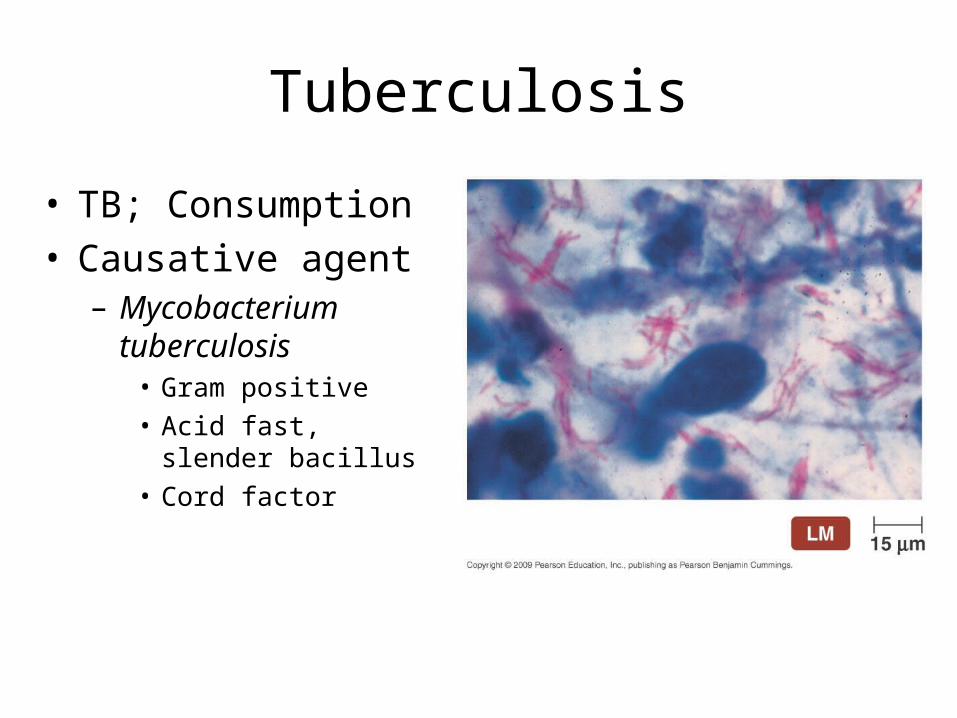
Tuberculosis
• TB; Consumption • Causative agent
– Mycobacterium tuberculosis
• Gram positive• Acid fast, slender
bacillus• Cord factor
• Signs and Symptoms– Chronic illness– Initial symptoms:
• Minor cough and mild fever
– Progressive symptoms:• Fatigue; night sweats; weight loss; chest pain and
labored breathing • Chronic productive cough
– Sputum often bloody
• 3 types of tuberculosis:– Primary TB- initial case of tuberculosis disease– Secondary TB - reactivated – Disseminated TB- tuberculosis involving multiple
systems
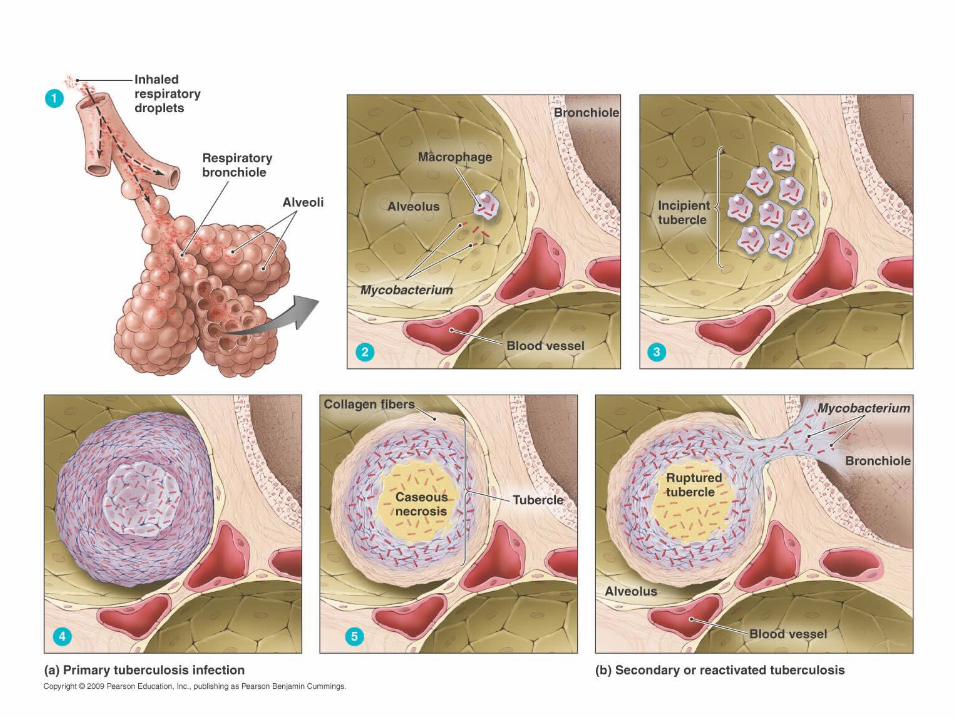
• Primary TB– Transmitted through respiratory droplets – Pathogens taken up by alveolar macrophages
• fusion of phagosome with lysosomes prevented– Pathogen replicates inside macrophages slowly killing
them– Intense immune reaction occurs
• WBCs surround infected cells and release inflammatory chemicals
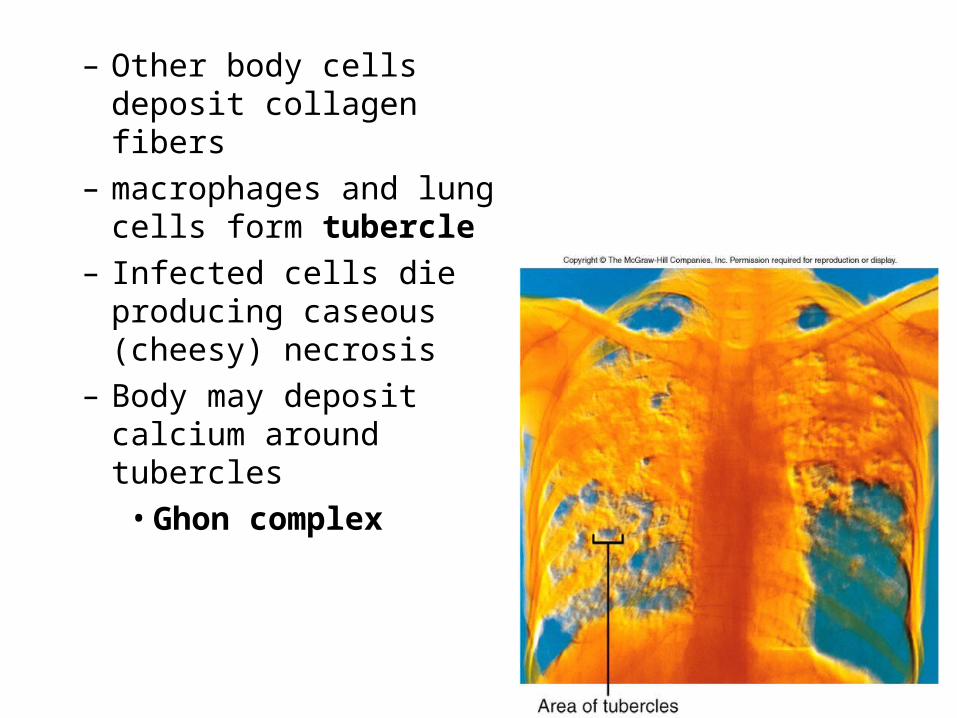
– Other body cells deposit collagen fibers
– macrophages and lung cells form tubercle
– Infected cells die producing caseous (cheesy) necrosis
– Body may deposit calcium around tubercles
• Ghon complex
– Secondary TB • tubercle ruptures and reestablishes active infection• More common in immunosupressed • Leading killer of HIV+ individuals
– Disseminated TB• Some macrophages carry pathogen through blood
and lymph to other sites of body• Bone marrow, spleen, kidneys, spinal cord and
brain
• Epidemiology– 1/3 of world population infected– Annual mortality of ~ 2 million – Estimated 10 million Americans infected
• Rate highest among non-white, elderly poor people– Small infecting dose
• As little as ten inhaled organisms• Not very virulent but high mortality
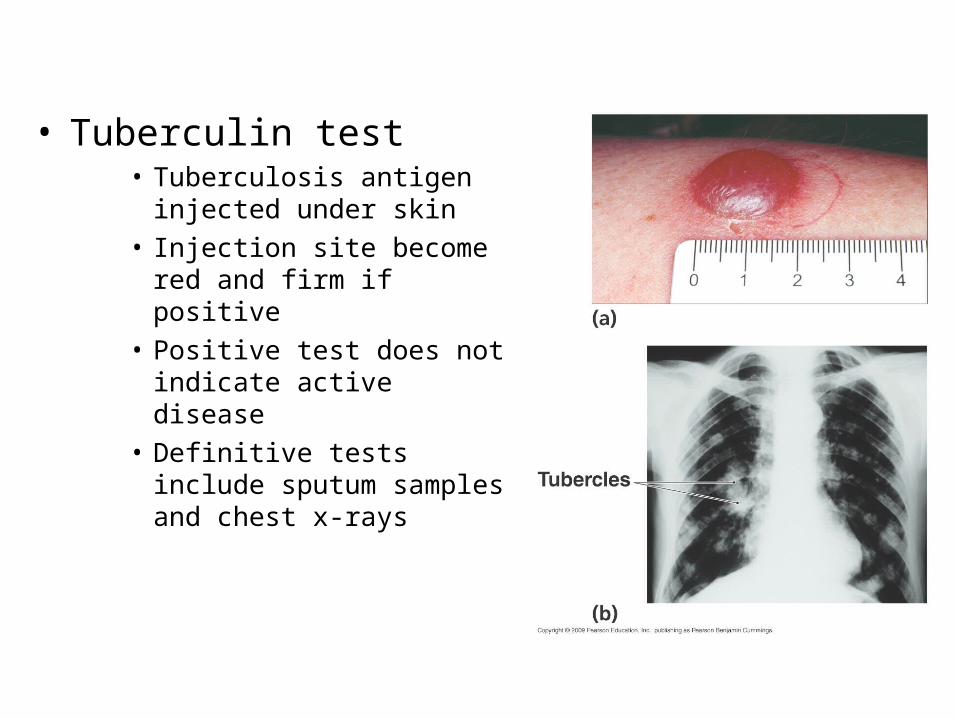
• Tuberculin test• Tuberculosis antigen injected
under skin• Injection site become red and
firm if positive• Positive test does not indicate
active disease• Definitive tests include sputum
samples and chest x-rays
• Prevention – Vaccination used in other parts of the world– Prophylactic antibacterial treatment for exposed
individuals
• Treatment– Antibiotic treatment
• Rifampin, Isoniazid, streptomycin and ethambutol
• MDR strains
• Therapy lasts up to 6 months (DOTS)





























