Embed Size (px)
Citation preview
Low Dose Tricks in Kids
Marilyn J. Siegel, M.D
Mallinckrodt Institute of Radiology
Washington University Medical Center
St. Louis, MO
Disclosure of Commercial Interest
I have a financial relationship with a
commercial organization that may have a direct
or indirect interest in the content as follows:
• Siemens Medical Solutions: consultant,
speakers bureau
Learning Objective-To Understand
• Basic CT dose reduction “tricks” in a young population
Background: Pediatric CT Facts
• Up to 11% of CT exams are pediatric
• 33% are in children < 10 years
• 17% are in children 0-5 years old
• This is the population that is most
sensitive to radiation exposure!
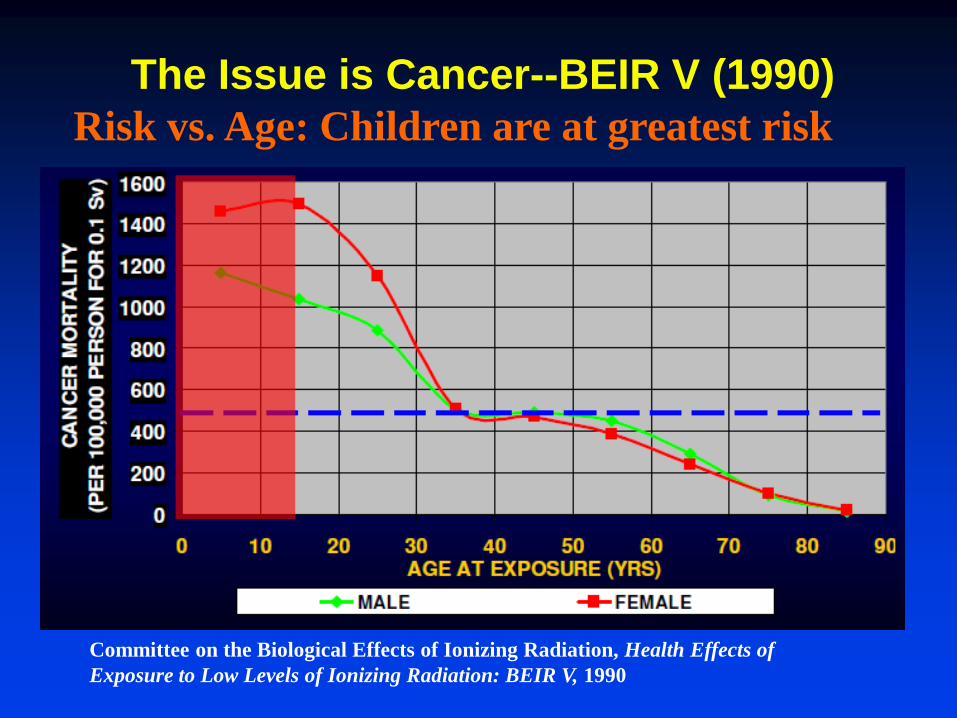
The Issue is Cancer--BEIR V (1990)
Risk vs. Age: Children are at greatest risk
Committee on the Biological Effects of Ionizing Radiation, Health Effects of
Exposure to Low Levels of Ionizing Radiation: BEIR V, 1990
"Make a habit of two
things -- to help, or at least do no harm“
Hippocrates, The Epidemics
Low Dose Tricks in Kids: 6 Basic Pillars
1. Use CT appropriately
2. Limit number of contrast phases
3. Adjust mA and kV for body size
4. Increase the collimation
5. Increase the pitch
6. Shield sensitive organs
1. Appropriate Utilization
• Justify the study-is it needed?
• Avoid repetitive studies
• Use ultrasound or MRI when they
offer comparable or more information
–BUT not always possible
• Benefit needs to outweigh risk
Step 2: Limit Number of Contrast Phases
• Key concept: venous phase imaging
suffices for tumor and trauma CT
• Key concept: arterial phase imaging
suffices for vascular lesions (rings,
coarctation and sequestration)
• You don’t routinely need multiphase
imaging
• You don’t need non-contrast scans
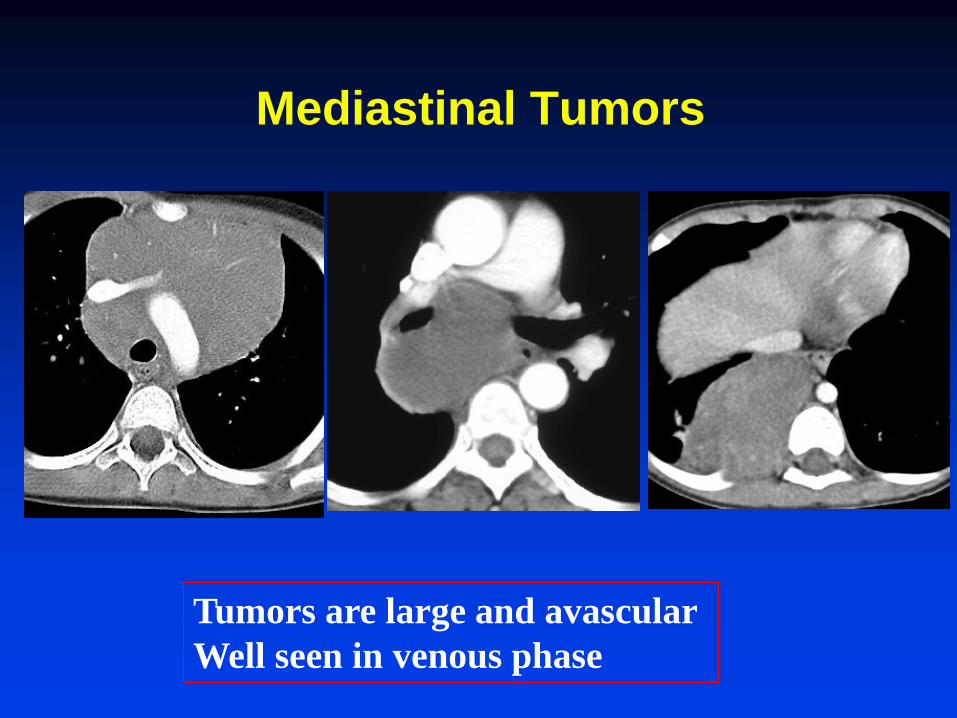
Mediastinal Tumors
Tumors are large and avascular
Well seen in venous phase
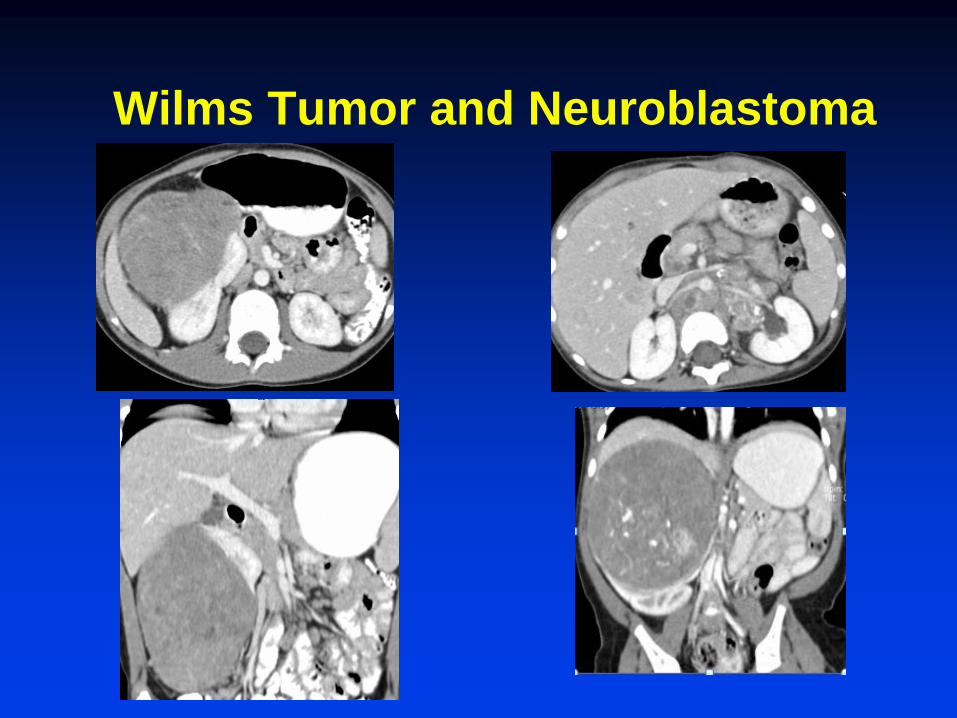
Wilms Tumor and Neuroblastoma
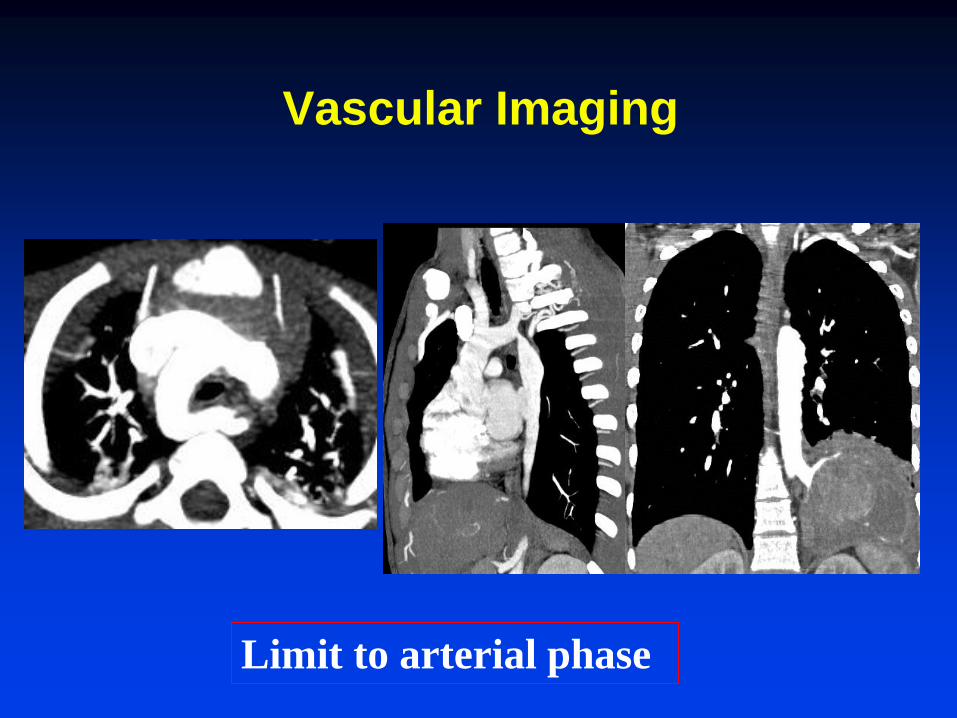
Vascular Imaging
Limit to arterial phase
Exception is the Liver
• Dual phase scanning mandatory
for characterization of tumors
–HA phase: 12 to 15 sec
–PV phase: 55 to 60 sec
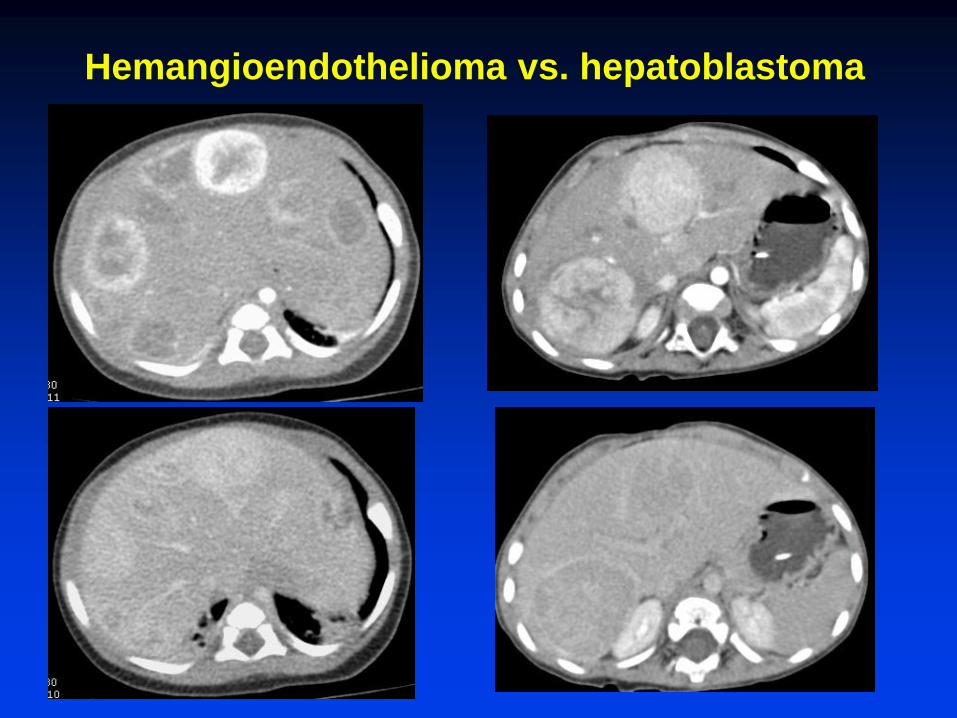
Hemangioendothelioma vs. hepatoblastoma
3. Adjust mA and kVp for body size
• Dose and mA: linear relationship
–50% decrease in mA = 50% dose decrease
• Dose and kVp: exponential relationship
–120 to 80 kVp = 30% to 50% dose decrease
The Challenge is how to select the best parameters
• Basic approaches-published charts OR automated technology
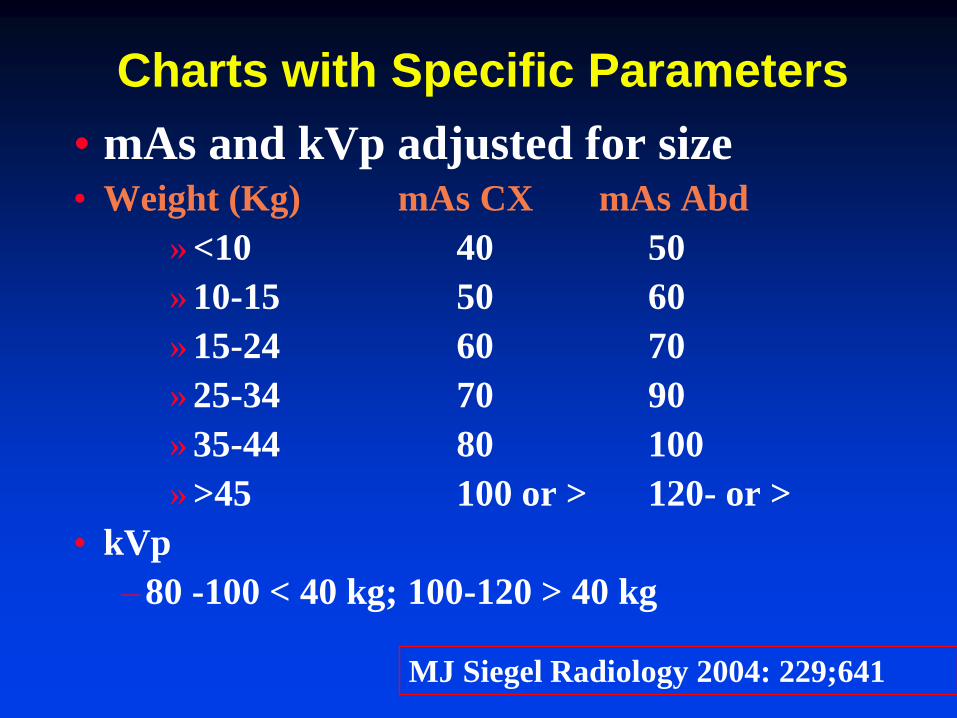
Charts with Specific Parameters
• mAs and kVp adjusted for size • Weight (Kg) mAs CX mAs Abd
» <10 40 50
» 10-15 50 60
» 15-24 60 70
» 25-34 70 90
» 35-44 80 100
» >45 100 or > 120- or >
• kVp
–80 -100 < 40 kg; 100-120 > 40 kg
MJ Siegel Radiology 2004: 229;641
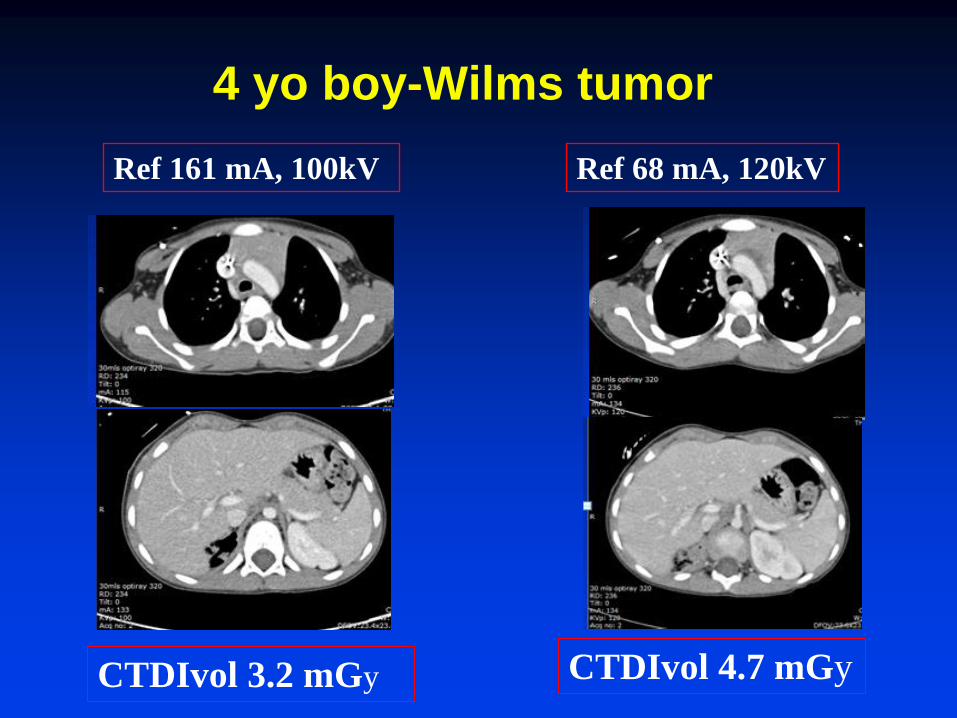
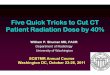
Ref 161 mA, 100kV Ref 68 mA, 120kV
CTDIvol 3.2 mGy CTDIvol 4.7 mGy
4 yo boy-Wilms tumor
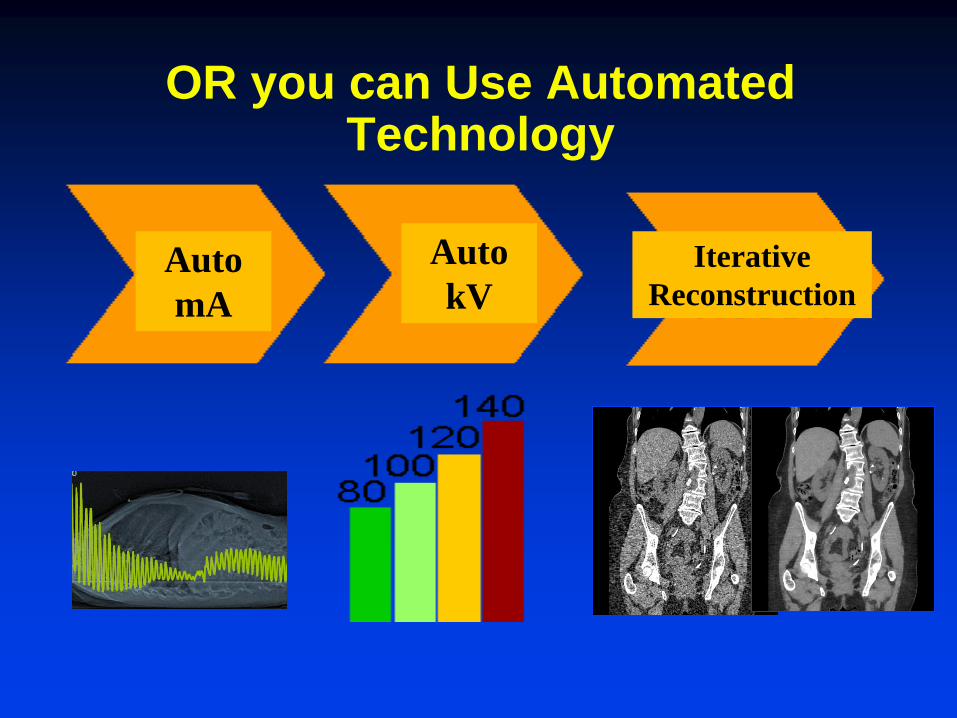
OR you can Use Automated Technology
Iterative
Reconstruction
Auto
kV Auto
mA
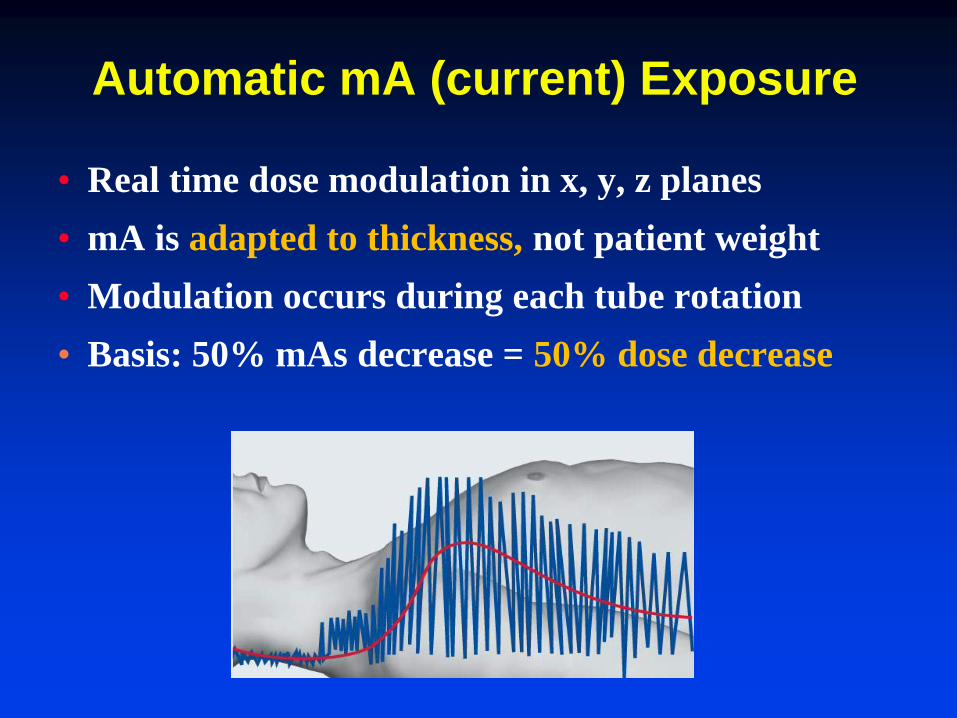
Automatic mA (current) Exposure
• Real time dose modulation in x, y, z planes
• mA is adapted to thickness, not patient weight
• Modulation occurs during each tube rotation
• Basis: 50% mAs decrease = 50% dose decrease
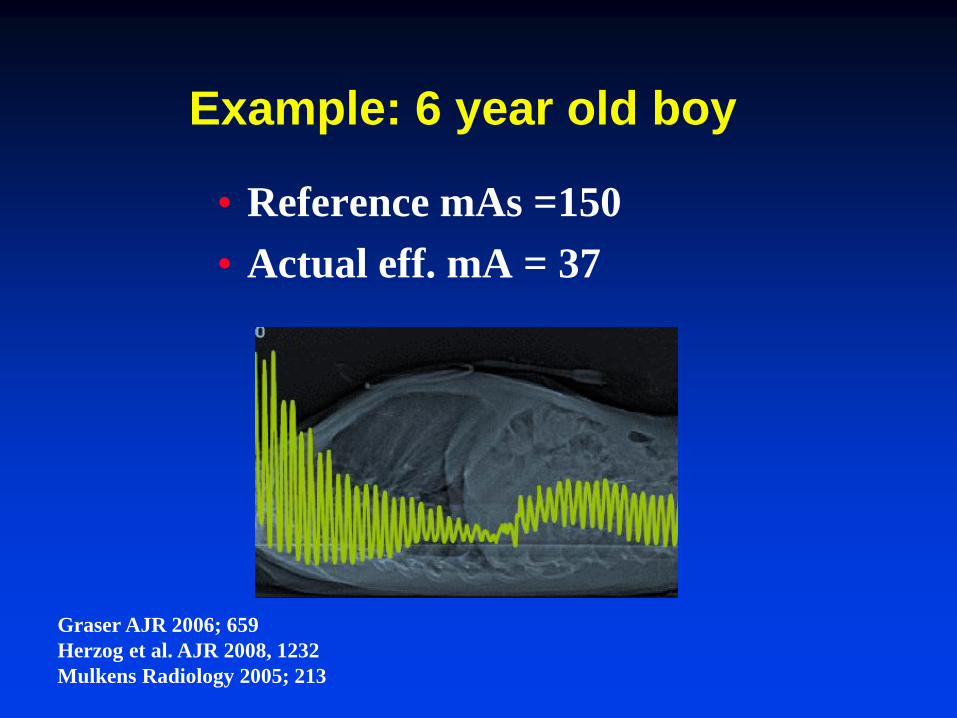
Example: 6 year old boy
• Reference mAs =150
• Actual eff. mA = 37
Graser AJR 2006; 659
Herzog et al. AJR 2008, 1232
Mulkens Radiology 2005; 213
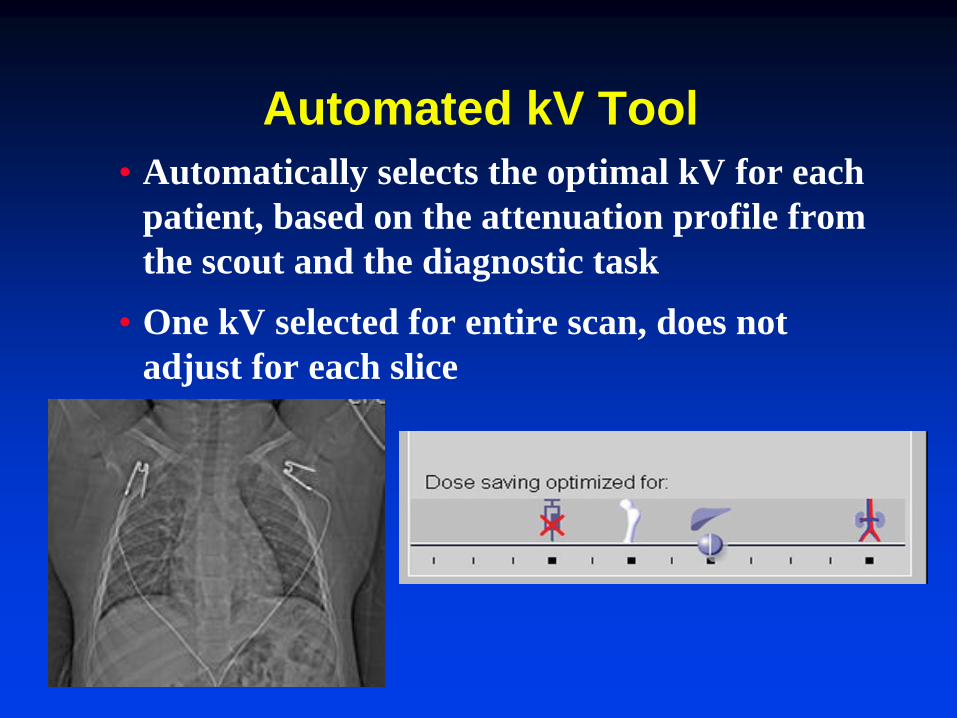
Automated kV Tool
• Automatically selects the optimal kV for each
patient, based on the attenuation profile from
the scout and the diagnostic task
• One kV selected for entire scan, does not
adjust for each slice
Auto KV-Clinical Tests
• Tested in > 150 children day 1-18 years
• 26 had prior scans without auto kV
• Results
–with auto kV mean CTDI vol 3.7 mGy
–without mean CTDIvol 5.9 mGy
–Mean dose reduction= 2.1 mGy
–Great quality images
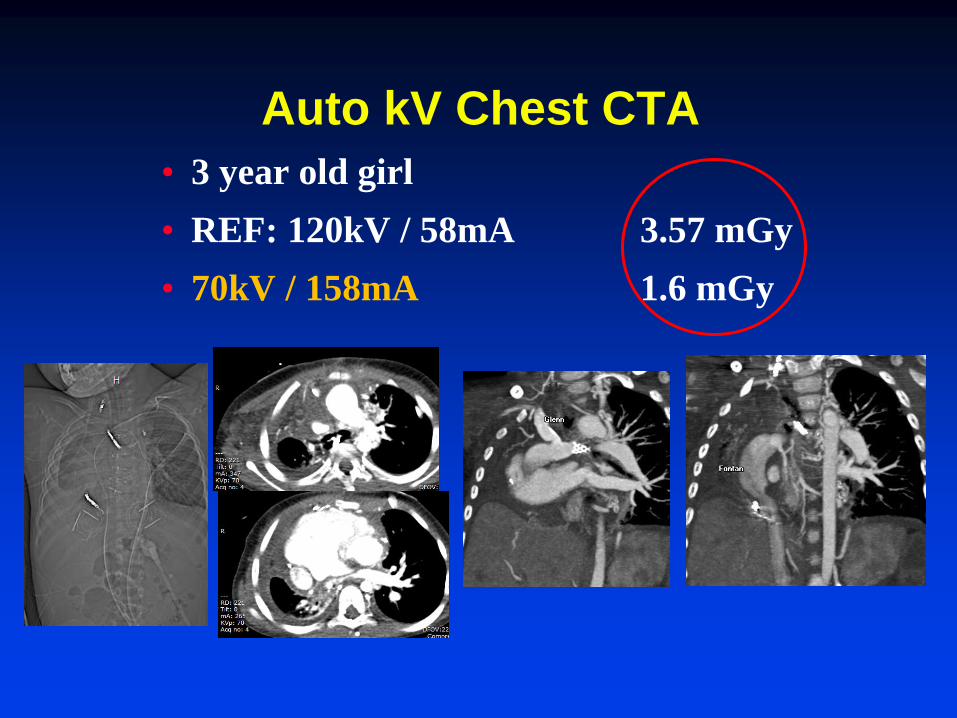
Auto kV Chest CTA
• 3 year old girl
• REF: 120kV / 58mA 3.57 mGy
• 70kV / 158mA 1.6 mGy
Step 4: Increase the collimation
• Detector collimation
–routine imaging: > 1mm
–angiography: 0.6-0.75 mm
Goal: To get the highest resolution with the lowest radiation exposure
Step 5: Increase the Pitch
• Pitch: linear impact on dose
• Increase pitch 50% = decrease dose 50%
• For single source CT: pitch 1-1.5 suffices
• For dual source: pitch 3.4 is possible
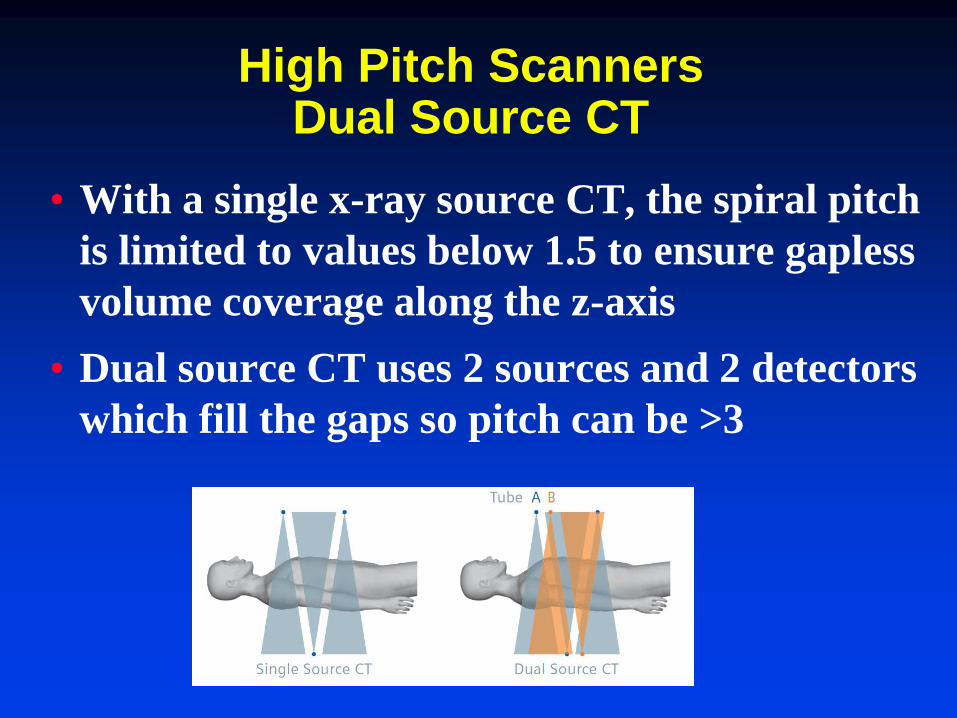
High Pitch Scanners Dual Source CT
• With a single x-ray source CT, the spiral pitch
is limited to values below 1.5 to ensure gapless
volume coverage along the z-axis
• Dual source CT uses 2 sources and 2 detectors
which fill the gaps so pitch can be >3
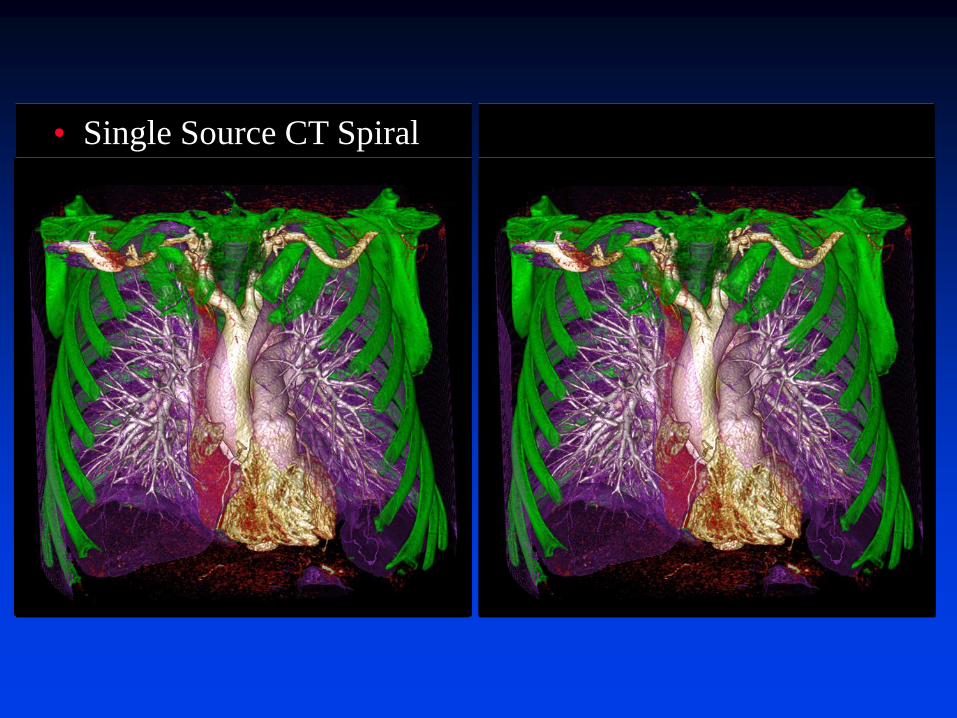
• Single Source CT Spiral •Dual Source CT Flash Spiral
• Pediatric: > 4s, sedation
• Whole Body: >10 seconds
• Pediatric: < 1s, no sedation
• Whole Body : 4 seconds 3 2 1 Scan 3 2 1 Scan
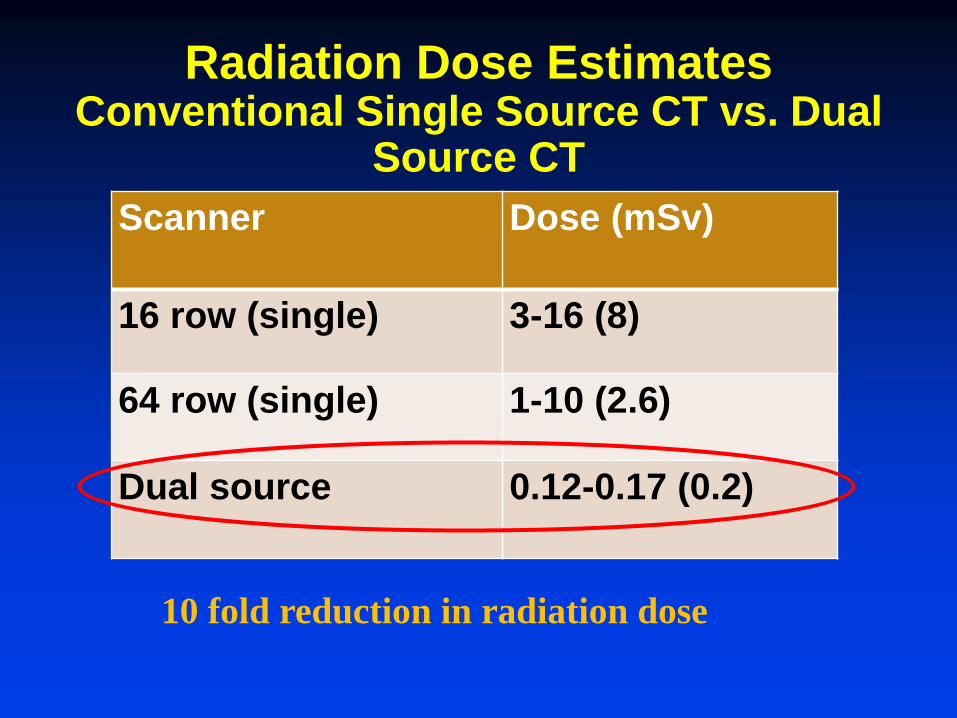
Radiation Dose Estimates Conventional Single Source CT vs. Dual
Source CT
Scanner Dose (mSv)
16 row (single) 3-16 (8)
64 row (single) 1-10 (2.6)
Dual source 0.12-0.17 (0.2)
10 fold reduction in radiation dose
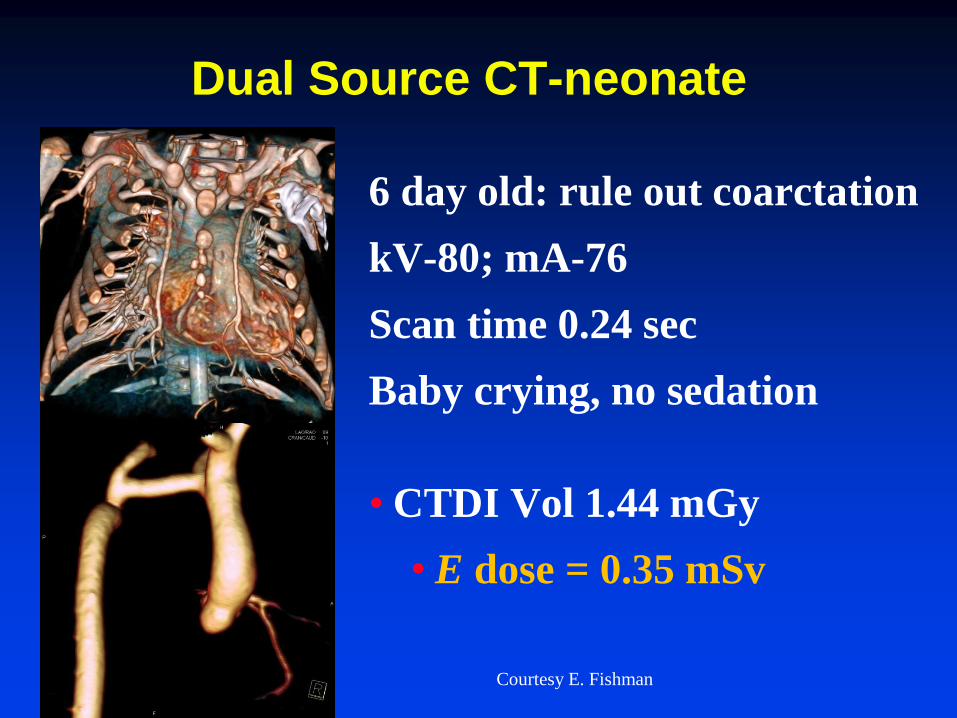
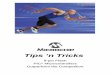
Dual Source CT-neonate
6 day old: rule out coarctation
kV-80; mA-76
Scan time 0.24 sec
Baby crying, no sedation
• CTDI Vol 1.44 mGy
• E dose = 0.35 mSv
Courtesy E. Fishman
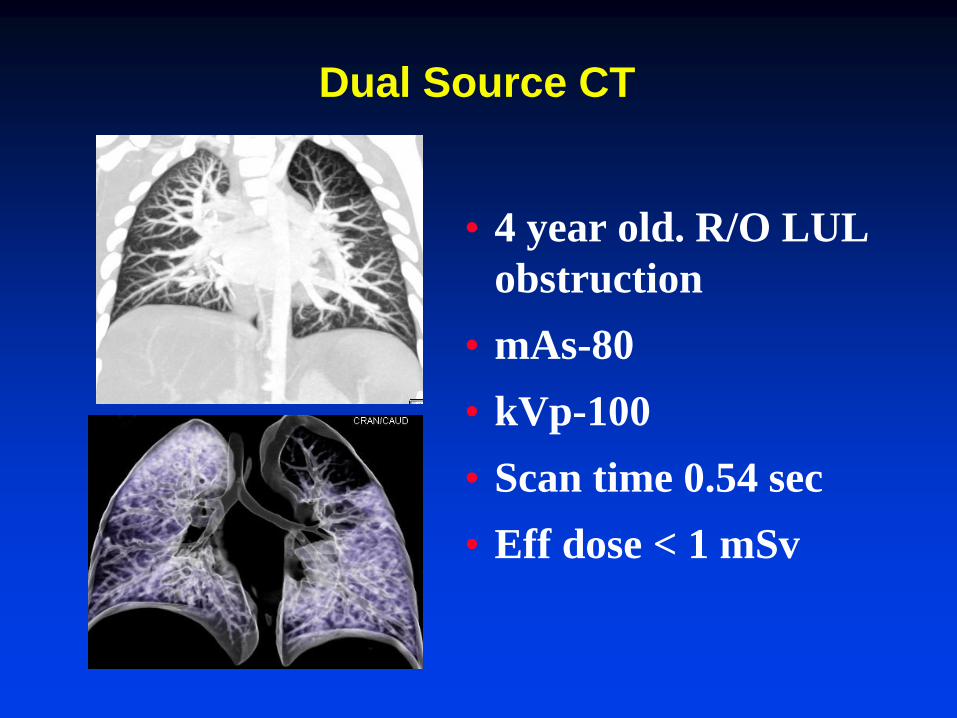
Dual Source CT
• 4 year old. R/O LUL
obstruction
• mAs-80
• kVp-100
• Scan time 0.54 sec
• Eff dose < 1 mSv
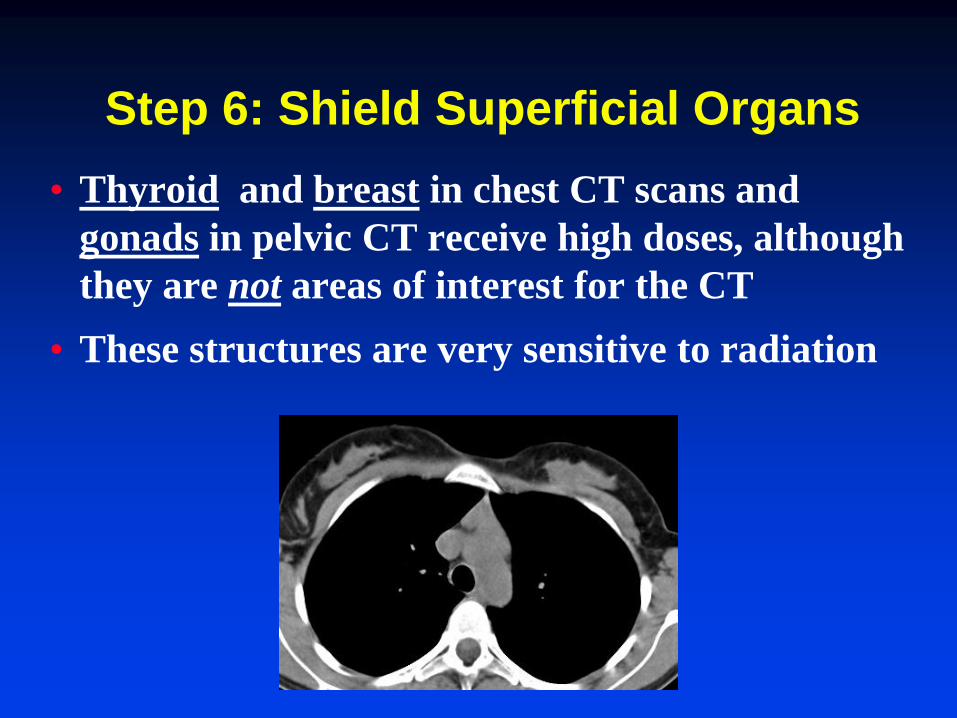
Step 6: Shield Superficial Organs
• Thyroid and breast in chest CT scans and
gonads in pelvic CT receive high doses, although
they are not areas of interest for the CT
• These structures are very sensitive to radiation
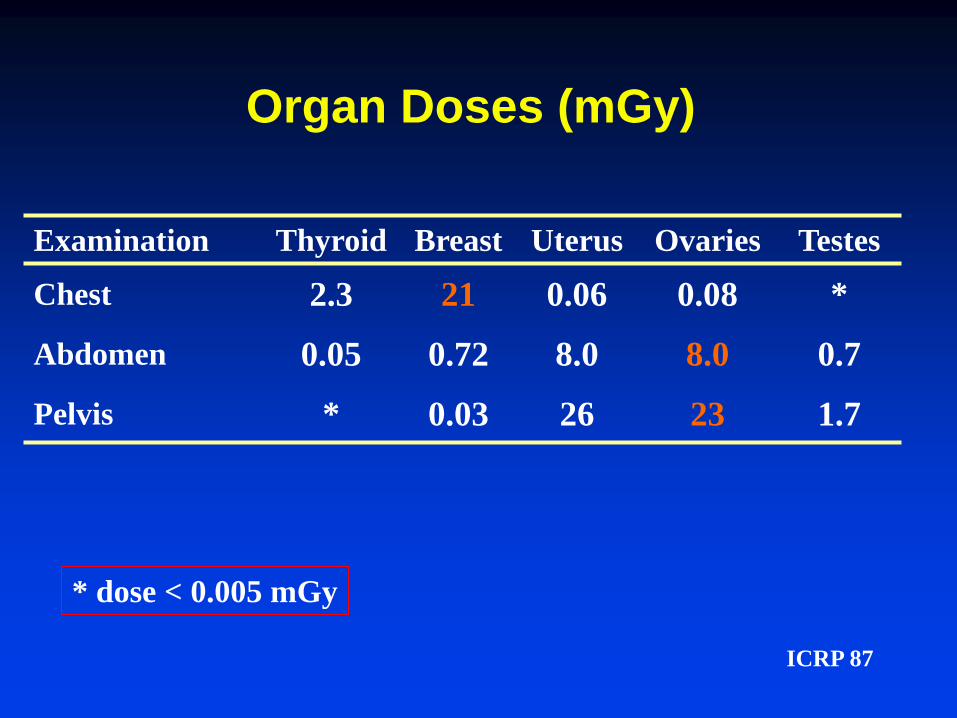
Organ Doses (mGy)
Examination Thyroid Breast Uterus Ovaries Testes
Chest 2.3 21 0.06 0.08 *
Abdomen 0.05 0.72 8.0 8.0 0.7
Pelvis * 0.03 26 23 1.7
* dose < 0.005 mGy
ICRP 87
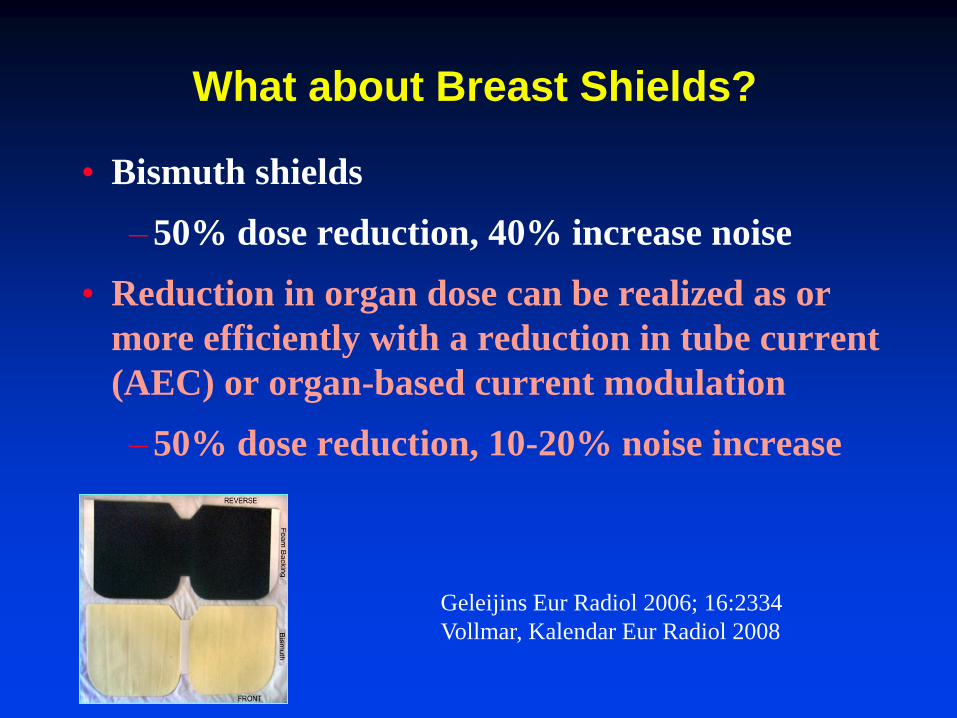
What about Breast Shields?
• Bismuth shields
–50% dose reduction, 40% increase noise
• Reduction in organ dose can be realized as or
more efficiently with a reduction in tube current
(AEC) or organ-based current modulation
–50% dose reduction, 10-20% noise increase
Geleijins Eur Radiol 2006; 16:2334
Vollmar, Kalendar Eur Radiol 2008
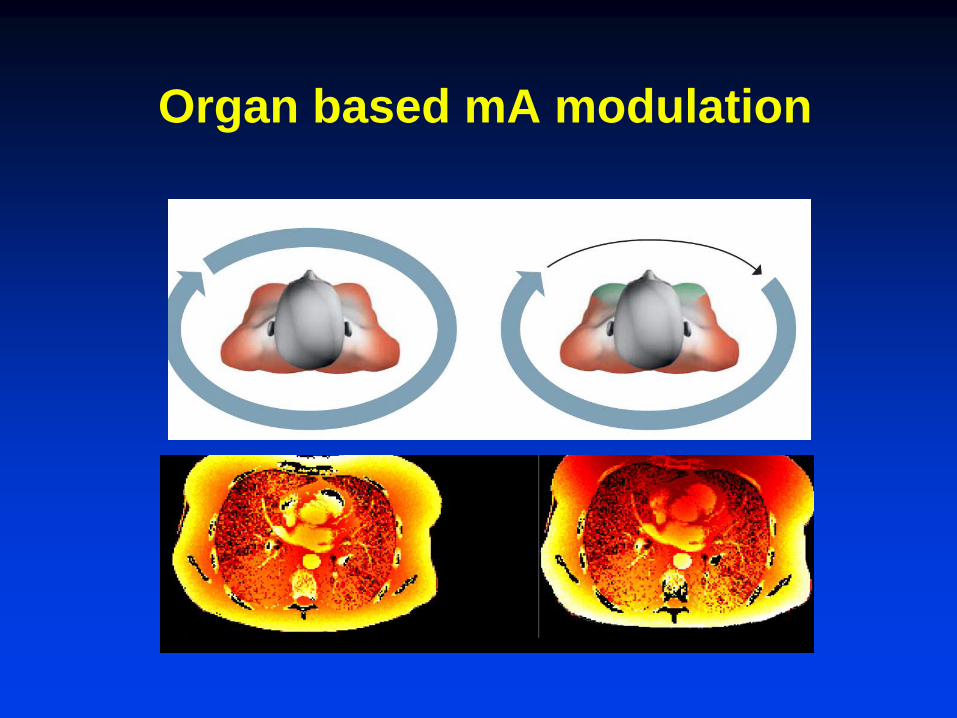
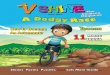
Organ based mA modulation
Pediatric CT
• A challenge but dose reduction is possible using optimized, automated kV, ma, and pitch