Embed Size (px)
Citation preview
387Low Dose Aldosterone Antagonism Reduces Diuretic Requirements in HeartFailureAlexandra Perez1, Larisa H. Cavallari1, Dee Fontana2, Thomas D. Stamos2, Vicki L.Groo1,2; 1Pharmacy Practice, University of Illinois Medical Center, Chicago, IL;2Cardiology, University of Illinois Medical Center, Chicago, IL
Background: The effect of low doses of aldosterone antagonists (AA) on loopdiuretic (LD) dosing in heart failure (HF) has not been reported. If AA have a natriureticeffect at low doses, there is the potential for an unexpected diuresis with continuationof baseline diuretic therapy. The objective of this study was to evaluate the effects ofAA on loop diuretic dose requirements and risk for dehydration/acute renal failure(ARF) in the treatment of heart failure. Methods: We reviewed the medical recordsof HF subjects who where on a LD at the time of AA initiation. Baseline data in-cluded demographics, medications, renal status and co-morbidities. Loop diureticdose changes, renal function and number of hospital admissions for dehydration/ARF over a 12-month period after AA initiation was evaluated. Results: Sixty sub-jects, 60% black, 57% male, mean age 54 were included in the study. Baseline char-acteristics include average BP of 124/73, weight 226 pounds, BUN 19 and, SrCr 1.23mg/dL and 83% had moderate to severe left ventricular dysfunction. Concomitanttherapy included beta-blockers (93%) and ACEI (98%). Furosemide was the onlyLD used. As shown in the table, there was a significant reduction in LD dose overthe 12-months following AA initiation. Diuretic doses were unchanged (NC) in 19(32%) subjects, increased (INC) in 14 (23%) and decreased (DEC) in 27 (45%).The INC/NC group was on a lower LD dose compared to the DEC group at baseline(92 6 53 mg vs. 132 6 69 mg, p 5 0.012). The INC/NC subjects were more likely tohave 2-co-morbidities versus 1 in the DEC group. The DEC group had a significantdecline in renal function at the time of first LD dose change compared to baseline(p ! 0.05). There were 4 hospitalizations due to dehydration/ARF with no significantdifference between DEC and INC/NC groups. Conclusions: Data from this studyshowed that 45% of subjects required a decrease in LD dose over a 12-month periodand 7% of subjects were hospitalized due to dehydration/ARF. Renal dysfunction wassignificant among the DEC group. Careful monitoring of renal function and fluid sta-tus, in addition to potassium, is warranted in this population.
Furosemide Dose Changes
Baseline 1 month 3 months 6 months 12 months
All subjects (mg) 109 6 64 109 6 67 101 6 62 94 6 57 * 89 6 59 *DEC group (mg) 132 6 69 119 6 66 * 98 6 68 y 84 6 54 y 67 6 50 y
* 5 p ! 0.05, y 5 p ! 0.001.
388Comparison of Ultrafiltration, Nesiritide, and Usual Care in AcuteDecompensated Heart FailureSyed Saghir1, Cheryl Bartone2, Raymond Barrows1, Santosh G. Menon2, Eugene S.Chung2; 1Internal Medicine, The Christ Hospital, Cincinnati, OH; 2Heart Failure,Ohio Heart and Vascular Center, Cincinnati, OH
Background: In acute decompensated heart failure (ADHF), the primary clinicalgoal of symptom improvement through volume removal is often not realized anda significant number of patients are discharged with inadequate volume loss. Standardof care is based on loop diuretics, despite lack of conclusive data on longterm safetyand efficacy. Nesiritide (N) is an adjunctive therapy used to rapidly improve symp-toms and promote naturiuresis, while ultrafiltration (UF) is an effective way to re-move fluid in diuretic resistance. We compared usual care (UC), UF, and UC plusN in a case control study. Methods: 25 HF inpatients that underwent UF (Aquadex,CHF Solutions) were selected based on completeness of clinical data. UC and Ngroups were matched for age, gender, ejection fraction, etiology of HF, and creati-nine. The decision to use UF, N or UC was a clinical decision for the attending Car-diologist. Mean UF rate was 325 6 117 (ml/hr), with a mean duration of 38 6 25(hrs). Diuretics were held during UF but not during N infusion. Data were collectedby chart review. Results: There were no significant differences in patient demograph-ics, co-morbidities or baseline laboratory values. Rehospitalizations, pre- and post-treatment laboratories, and weight changes are shown in the table. Conclusion: Inpatients with ADHF, UF appears to be a more effective method to remove volumeand prevent 30 day all cause readmissions than UC or UC plus N, but with relativelygreater increase in BUN and creatinine. A prospective study comparing UF and ad-junctive therapy with N is warranted.
389Screening for New Diagnosis of Heart Failure in Primary Care Clinics UsingElectronic Health Record and the Impact of Diabetes MellitusW.H. Wilson Tang1, Anil Jain2, C. Martin Harris2; 1Cardiovascular Medicine,Cleveland Clinic, Cleveland, OH; 2Medicine, Cleveland Clinic, Cleveland, OH
Background: The incidence of heart failure (HF) has largely been derived from pop-ulation-based epidemiological studies. With the implementation of electronic healthrecord (EHR) in the primary care setting, EHR-based screening for new diagnosis ofHF can be a useful strategy. Methods: Since 2001, the Cleveland Clinic PrimaryCare Network (CCPCN) has incorporated EHR into their clinical practice. We re-viewed the problem list and/or encounter diagnosis list of consecutive adult patientswith at least one visit per year in the CCPCN between 2001-5 without prior history ofHF, and stratified according to a documented history of diabetes melltius. Validationby detailed chart review on the incident cases were performed for those diagnosed inthe year 2004 (n 5 114). Results: In our cohort of over 17,518 adult patients, 3,421(20%) had a history of diabetes mellitus. There is a bias in over-reporting in 2001, butbetween 2002-4, a consistent 0.7% incidence of new diagnosis of HF in the overallpopulation has been observed. In the diabetic cohort, a consistently higher incidenceof 1.8-2.2% was observed (see Table). Among the 114 patients with new diagnosis ofHF documented in 2004, 102 (89%) had no prior HF documented in the precedingEHR notes. Conclusion: An EHR-based screening for new diagnosis of HF in theprimary care setting is feasible, and can provide the platform to explore the role ofantecedant risk factors (such as diabetes mellitus) for developing heart failure.
Incidence of HF Identified in HER
Year N (all) HF Incidence (All) N (diabetes) HF Incidence (diabetes)
2001 17,382 1.1% 3,325 2.9%2002 17,264 0.7% 3,252 2.2%2003 17,149 0.7% 3,190 1.9%2004 17,035 0.7% 3,134 1.8%
390Improved Outcomes with Chronic Inodilator Therapy in the Modern HeartFailure PatientShun Kohsaka1, Greg V. Poulin1, Lauren M. Barrash2, Erin Donaho1, MichelleEdwards1, Reynolds M. Delgado1; 1Department of Cardiology, Texas HeartInstitute at St Luke’s Episcopal Hospital, Houston, TX; 2Critical Care Systems,Houston, TX
Introduction: Randomized controlled trials showed increased mortality with intrave-nous inodilator therapy used acutely, intermittently or continuously in patients withacute heart failure (HF) syndromes. However, the appropriate role of intravenous in-odilator in the management of chronic HF is still controversial. In clinical practice, itsuse remains a common but highly variable therapeutic option. Purpose: As new op-tions emerge for the treatment of HF, the available information should be reviewed todetermine safety and outcomes for patients treated with chronic intravenous inodila-tor therapy. Methods: We retrospectively analyzed the outcome of 32 consecutivepatients enrolled for chronic continuous milrinone therapy from January 1, 2004 toMarch 10, 2006. The patients met local Medicare criteria including 20% improve-ment in either cardiac index or pulmonary wedge pressure. Results: Average agewas 60.1 þ/� 14.7 y/o and the population was predominantly male (70.6%). Allthe patients were on beta-blockers at the initiation of infusion. The milrinone was
UC (n 5 25) UF (n 5 25) N (n 5 25)
Mean LOS(days)
4.9 6 3.3 7.2 6 5.9 6.2 6 2.9
Median LOS(days)
4 6 6
30 d HFreadmission(%)
6 (24) 3 (12) 7 (28)
In-Hospitaldeath (%)
0 (0) 1 (4) 0 (0)
Pre Rx Post Rx Pre Rx Post Rx Pre Rx Post RxHct, % 36.7 6 7.2 35.9 6 6.2 34.0 6 4.8 34.2 6 5.5 38.1 6 7.9 35.4 6 6.2Hgb, gm/dl 12.2 6 2.5 12.0 6 2.1 11.3 6 1.5 11.3 6 1.8 12.7 6 2.6 11.8 6 2.2Na, mg/dl 138 6 3.0 137.5 6 2.5 135.3 6 6.5 133.7 6 6.9 136.0 6 4.7 136.5 6 4.0K, mg/dl 4.2 6 0.8 4.1 6 0.5 4.2 6 0.6 4.5 6 0.6 4.3 6 0.7 4.2 6 0.5BUN, mg/dl 34.6 6 23.5 38.8 6 26.0 51.6 6 28.8 61.2 6 34.7* 35.9 6 19.3 37.2 6 21.8Cr, mg/dl 1.8 6 0.8 1.9 6 1.0 1.9 6 0.8 2.2 6 1.1* 1.5 6 0.6 1.5 6 0.7Wt, lbs. 223.1 6 75.7 216.8 6 74.3* 229.7 6 73.3 213.8 6 68.1* 205.6 6 74.1 201.0 6 76.6D Wt (lbs) 6.3 6 7.6 15.8 6 13.6 4.7 6 10.9D Cr O 0.5
(%)6 (24) 11 (44) 5 (20)
*p # 0.01 vs. pre-treatment value; 6 standard deviation.
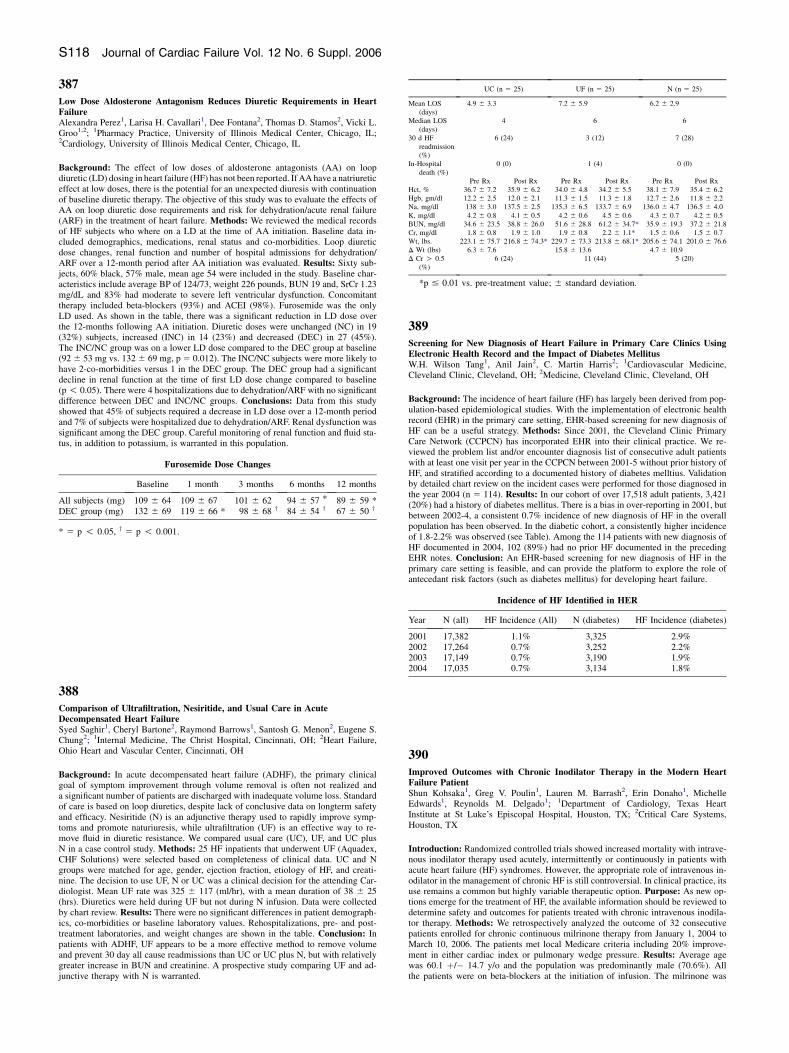
S118 Journal of Cardiac Failure Vol. 12 No. 6 Suppl. 2006







![Aldosterone and dopamine receptors in the kidney: Sites for ...Aldosterone and dopamine receptors 625 with the aldosterone receptor, when measured in vitro [21, 23] (Funder and Adam,](https://img.pdfslide.us/doc/110x75/608977add019a330f10765d3/aldosterone-and-dopamine-receptors-in-the-kidney-sites-for-aldosterone-and.jpg)