Embed Size (px)
Citation preview
1J Med Adv Clin Case Rephttps://www.jmaccr.com
1 INTRODUCTION
The genus Chryseobacterium belongs to the Flavobacteri-aceae family, first described by Vandamme, et al., in 1994 [1]. Chryseobacterium indologenes is a non-fermentative, catalase-positive, indole-positive, oxidase-positive, aerobic gram-negative rod [2]. C. indologenes is usually found in environmental sources such as soil, water, and food sources. These organisms may colonize the hospital water supply and may be associated with infections in immuno-compromised. Major risk factors noted in reported C. indologenes infections are prolonged hospitalization, immuno-compromised patients, patients with indwelling catheters or devices, and patients on prolonged broad-spectrum antibiotics [3,4]. It is also associat-ed with carrying multidrug-resistant genes. We report a geriat-ric patient with asymptomatic urinary tract infection (UTI) due to multidrug-resistant C. indologenes without the documented risk factors and died post-cardiac surgery due to septic shock with low cardiac output syndrome.
2 | CASE PRESENTATION
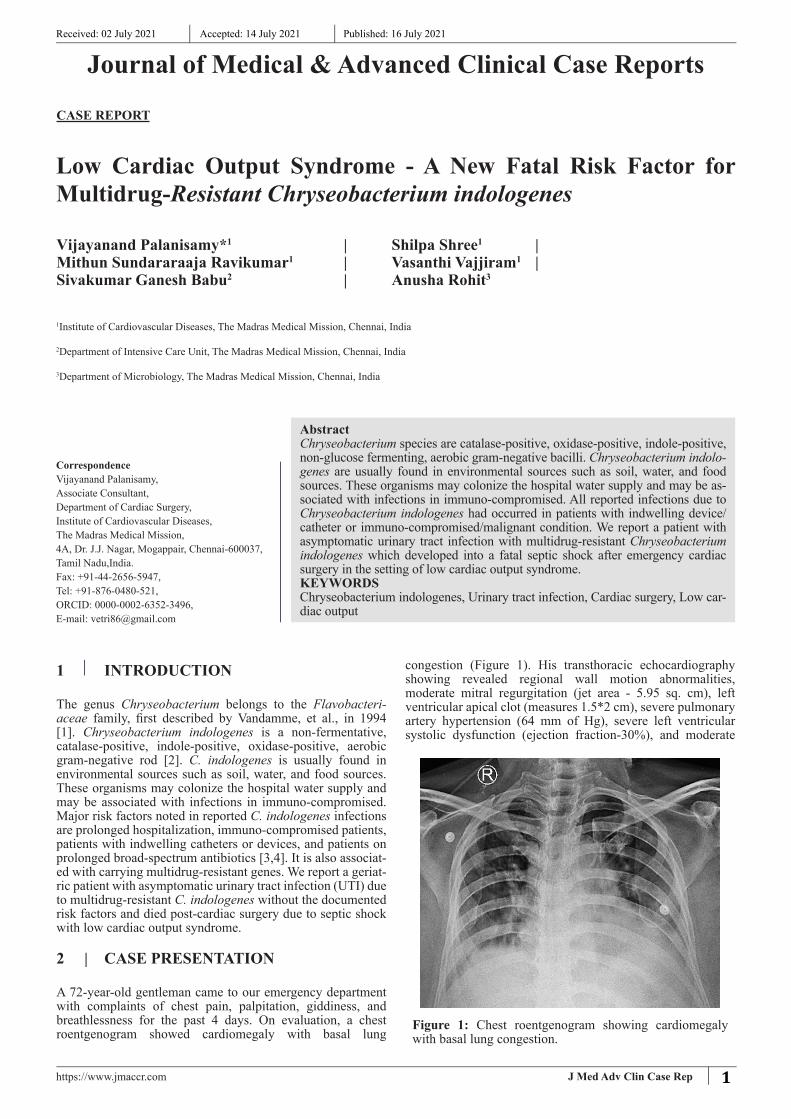
A 72-year-old gentleman came to our emergency department with complaints of chest pain, palpitation, giddiness, and breathlessness for the past 4 days. On evaluation, a chest roentgenogram showed cardiomegaly with basal lung
congestion (Figure 1). His transthoracic echocardiography showing revealed regional wall motion abnormalities, moderate mitral regurgitation (jet area - 5.95 sq. cm), left ventricular apical clot (measures 1.5*2 cm), severe pulmonary artery hypertension (64 mm of Hg), severe left ventricular systolic dysfunction (ejection fraction-30%), and moderate
CASE REPORT
Received: 02 July 2021 Accepted: 14 July 2021 Published: 16 July 2021
Low Cardiac Output Syndrome - A New Fatal Risk Factor for Multidrug-Resistant Chryseobacterium indologenes
| Shilpa Shree1 | | Vasanthi Vajjiram1 |
Vijayanand Palanisamy*1
Mithun Sundararaaja Ravikumar1
Sivakumar Ganesh Babu2 | Anusha Rohit3
1Institute of Cardiovascular Diseases, The Madras Medical Mission, Chennai, India
2Department of Intensive Care Unit, The Madras Medical Mission, Chennai, India
3Department of Microbiology, The Madras Medical Mission, Chennai, India
Journal of Medical & Advanced Clinical Case Reports
CorrespondenceVijayanand Palanisamy,Associate Consultant,Department of Cardiac Surgery,Institute of Cardiovascular Diseases,The Madras Medical Mission,4A, Dr. J.J. Nagar, Mogappair, Chennai-600037,Tamil Nadu,India.Fax: +91-44-2656-5947,Tel: +91-876-0480-521,ORCID: 0000-0002-6352-3496,E-mail: [email protected]
AbstractChryseobacterium species are catalase-positive, oxidase-positive, indole-positive, non-glucose fermenting, aerobic gram-negative bacilli. Chryseobacterium indolo-genes are usually found in environmental sources such as soil, water, and food sources. These organisms may colonize the hospital water supply and may be as-sociated with infections in immuno-compromised. All reported infections due to Chryseobacterium indologenes had occurred in patients with indwelling device/catheter or immuno-compromised/malignant condition. We report a patient with asymptomatic urinary tract infection with multidrug-resistant Chryseobacterium indologenes which developed into a fatal septic shock after emergency cardiac surgery in the setting of low cardiac output syndrome.KEYWORDSChryseobacterium indologenes, Urinary tract infection, Cardiac surgery, Low car-diac output
Figure 1: Chest roentgenogram showing cardiomegaly with basal lung congestion.

2
J Med Adv Clin Case Rephttps://www.jmaccr.com
support. He was on continuous ventilation with the same supports on the first postoperative day (POD). His urine culture sensitivity showed the colonization with over 100,000 CFU/ml growth of multidrug-resistant C. indologenes (Figure 5).The organism was sensitive only to Co-trimoxazole with high Minimum Inhibitory Concentrations (MIC’s) to carbapenems, beta-lactamase inhibitors, fluoroquinolones, aminoglycosides, and colistin (Table 1). Urologist and infectious disease physician advice were obtained and treated accordingly. He had a drop in urine output on the second POD for which acute peritoneal dialysis was initiated. As his general condition improved on the third POD, he was extubated. On 4th POD, he had an episode of tachypnea with hypoxia, for which he was reintubated. On the same day, his hemodynamics became unstable and the patient was declared dead due to septic shock (procalcitonin - 8.12 ng/ ml) added to low cardiac output syndrome.
3 | DISCUSSION
Chryseobacterium indologenes have been identified in the past few years as an emerging multidrug-resistant pathogen causing hospital-acquired infections. C. indologenes can cause a wide range of infections, such as bacteremia, sepsis, pneumonia, shunt infection, urinary tract infection, keratitis, and infection of the central nervous system [5]. After widespread use of colistin and tigecycline, the prevalence of infections due to C. indologenes has been on the rise [3]. The organism resideseven in chlorinated water supplies, hence poses a serious threatto cause health care associated infection in a high-riskpatient. According to the literature, identified risk factorsfor encountering C. indologenes infection were the presence
right ventricular dysfunction (Tricuspid annular plane systolic excursion - 11 mm) (Figure 2, Figure 3A, Figure 3B, Figure 4A, Figure 4B). The coronary angiography showed triple vessel coronary artery disease. On pre-operative evaluation, he was diagnosed with asymptomatic bacteriuria for which urine was sent for culture sensitivity and started on a prophylactic antibiotic. Due to ongoing chest pain and continued breathlessness despite medical management, he was planned for an emergency high-risk cardiac surgery. Intraoperatively, his bladder was catheterized with a silicone urinary catheter in view of UTI. He underwent left ventricular apical clot removal, Dor’s ventriculoplasty, mitral valve repair, and coronary artery bypass grafting. He was shifted to the postoperative intensive care unit with inotropic support and intra-aortic balloon pump
Figure 2: Transthoracic echocardiography showing mitral regurgitation (jet area -5.95 sq.cm)
Figure 3: Left ventricular apical clot. A) Transthoracic echocardiography four-chamber view showing left ventricular apical clot measuring 1.5*2 cm size; B) Transesophageal echocardiography three-dimensional short-axis image showing the apical clot
Figure 4: Transthoracic echocardiography. A) M mode showing Ejection fraction - 30%; B) Continuous wave doppler showing right ventricular systolic pressure - 54.27 mm Hg.

3
J Med Adv Clin Case Rephttps://www.jmaccr.com
of indwelling devices/implant, malignancies, prolonged hospitalization, prolonged broad-spectrum antibiotics use, and immuno-compromised state. Our patient had neither a urinary catheter nor any other described risk factors, the only risk factors we may have been able to ascertain were old age, low cardiac output syndrome, prolonged cardiopulmonary bypass time (182 min). Only on pre-operative workup, the patient was found to have UTI with multidrug-resistant C. indologenes resistant to even quinolones. Despite optimal medical stabilization, the patient continued to be symptomatic. His LV apical clot also poses a serious threat of stroke. Therefore, we planned to go ahead with surgery after explaining the high risk involved. Preoperatively patient was not on a urinary catheter. Intra-operatively, we used a silicone catheter to catheterize the bladder, as silicone catheter resists biofilm formation i.e, the key step for colonization of C. indologenes.The results of the SENTRY antimicrobial surveillance program [6] showed that a) the most active agents are the quinolones (gatifloxacin and levofloxacin), and trimethoprim-sulfamethoxazole (> 95% susceptibility) b) Ciprofloxacin, piperacillin, cefepime, ceftazidime, and rifampin showed reasonable activity (85% susceptibility) c) vancomycin, chloramphenicol, linezolid, and glycopeptides are not appropriate to treat. C. indologenes is resistant to
carbapenems and cephalosporins due to class A betalactamase and class B carbapenem hydrolyzing beta-lactamase activity. Its resistance is rapidly evolving; commonly used antibiotics against the Gram-negative organisms, such as cephalosporins, aminoglycosides, and imipenem were documented to be ineffective against C. indologenes. Our isolate also showed a similar susceptibility pattern with resistance to cephalosporins, carbapenems, aminoglycosides, and fluoroquinolones, and susceptibility to co-trimoxazole only. The mortality rate varies from study to study in C. indologenes infection. A study from Taiwan with 215 patients [3] revealed that in-hospital mortality rates due to bacteraemia were 63.6% and pneumonia was 35.25%. Even though it is low virulent; it may lead to severe life threatening infections in the setting of low cardiac output syndrome.
4 | CONCLUSIONS
Being a beta-lactamase producer, C. indologenes emerges as one of the serious multi-drug resistant nosocomial pathogens. As empirical antibiotic therapy won’t cover this pathogen, earlier prompt identification of C. indologenes and assessing its susceptibility pattern is crucial in the management of these patients. Even though it is less virulent, it can cause severe life threatening infections in case of multi-drug resistance and heart failure with low cardiac output as in our patient.
5 REFERENCES
1. Bhagawati G, Bhardwaj A, Sajikumar R, et al. (2019)Bacteremia by Chryseobacterium indologenes in apatient with lung cancer: A clinical and microbiologicalinvestigation. Indian J Crit Care Med 23: 157-159.
2. Izaguirre-Anariba DE, Sivapalan V (2020)Chryseobacterium indologenes, an Emerging Bacteria: A Case Report and Review of Literature. Cureus 12: e6720.
3. Chen FL, Wang GC, Teng SO, et al. (2013) Clinical andepidemiological features of Chryseobacterium indologenesinfections: Analysis of 215 cases. J Microbiol ImmunolInfect 46: 425-432.
4. Atici S, Ünkar ZA, Erdem K, et al. (2016) Ventilator-associated pneumonia caused by Chryseobacteriumindologenes: A rare infant case and review of the literature.Springerplus 5: 1741.
5. Christakis GB, Perlorentzou SP, Chalkiopoulou I, et al.(2005) Chryseobacterium indologenes non-catheter-related bacteremia in a patient with a solid tumor. J ClinMicrobiol 43: 2021-2023.
6. Kirby JT, Sader HS, Walsh TR, et al. (2004) Antimicrobialsusceptibility and epidemiology of a worldwide collectionof Chryseobacterium spp: Report from the SENTRYAntimicrobial Surveillance Program (1997-2001). J ClinMicrobiol 42: 445-448.
Figure 5: Agar showing oxidase-positive, non-fermenting yellow colonies of Cryseobacterium indologenes.A) MacConkey agar; B) Blood agar; C) Chocolate agar
Antibiotics MICs InterpretationAmikacin > 64 RCefipime > 64 RCefoperazonesulbactum > 64 R
Ceftazidime > 64 RCiprofloxacin > 4 RGentamicin > 16 RImipenam > 16 RLevofloxacin > 4 RMeropenam > 16 RNetilmycin Disk diffusion done RNorfloxacin Disk diffusion done ROfloxacin Disk diffusion done RPiperacillintazobactum > 128 R
Tigecycline 4 ISTrimethoprim/sulfamethaoxazole 40 S
Table 1: Blood culture and sensitivity report with minimum inhibitory concentration values
MICs: Minimum inhibitory concentrations; R: Resistant; IS: Intermediate sensitivity; S: Sensitivity. Culture shown growth of more than 1,00,000 cfu/ml of C.indologenes