Embed Size (px)
Citation preview
Emergenze ipertensive:
quando e come trattare
Lorenzo Ghiadoni, MD, PhD
Dipartimento di Medicina Clinica e Sperimentale, Università di Pisa
UO Medicina d’Urgenza Universitaria, AOUP
European Hypertension Specialist
Physicians in emergency departments (EDs)
frequently triage patients with ‘hypertensive crises’,
as an acute and severe rise in blood pressure (BP)
presenting with highly heterogeneous profiles ranging
from absence of symptoms to life-threatening target
organ damage.
Mancia G, al. Eur Heart J 2013
2013 ESH/ESC guidelines
for the management of arterial hypertension
• The approach in the acute hypertensive setting has not
been well established, in contrast with the evidence-
based recommendations guiding the appropriate
management of chronically elevated BP.
• In addition, a large number of patients in EDs are
affected by chronic hypertension, and do require referral
to outpatient care rather than acute interventions.
• Most importantly, few randomized clinical trials have
addressed the short-term and long-term effects of acute
BP lowering on cardiac and cerebrovascular morbidity
and mortality.
Mancia G, al. Eur Heart J 2013
2013 ESH/ESC guidelines
for the management of arterial hypertension
Acute severe BP rise in the ED
• Few studies have addressed the epidemiology of acute
hypertensive episodes.
• The prevalence of acute hypertensionwas examined in a
retrospective cohort study using administrative data
collected by 114 acute care hospitals from 2005-2007.
• Among 1,290,804 adults, acute hypertension (defined
as SBP ≥180 mmHg in the ED) occurred in 178,131
patients (13.8%).
Shorr AF et al, J Hosp Med. 2012 Mar; 7(3):203-10
Clinical characteristics associated with acute BP rise in
the ED:
• female sex
• obesity,
• coronary artery disease
• somatoform disorder
• high n° of antihypertensive medications
• Non-compliance to treatment
Acute severe BP rise in the ED
Most cases of acute
severe hypertension
in the ED are not life-
threatening and
preventable !!!!
Saguner AM et al. Am J Hypertens. 2010 Jul; 23(7):775-80
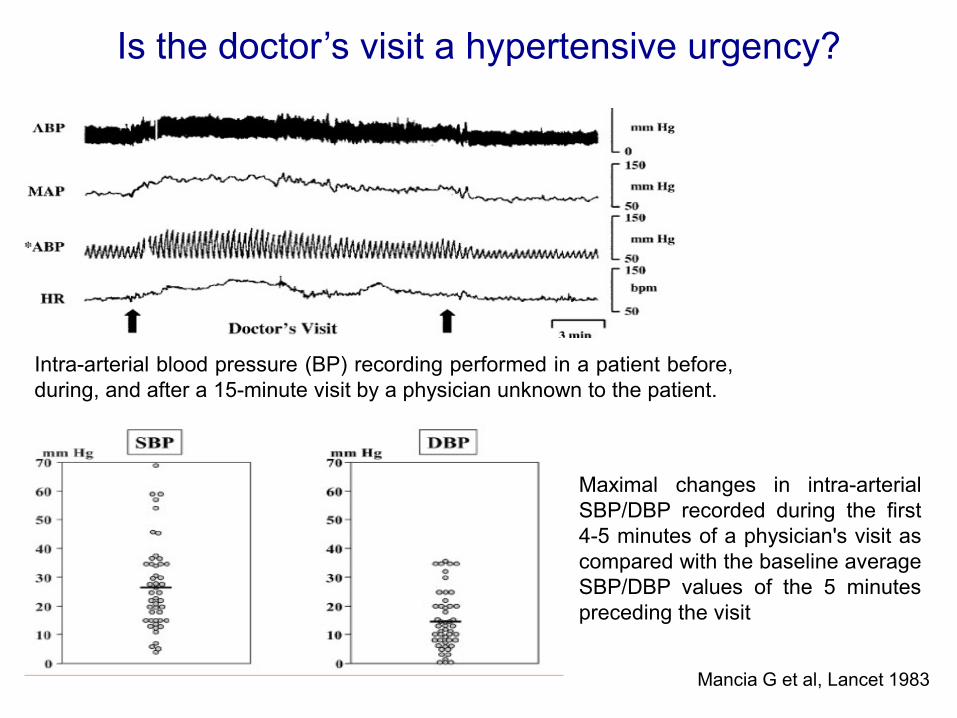
Mancia G et al, Lancet 1983
Intra-arterial blood pressure (BP) recording performed in a patient before,
during, and after a 15-minute visit by a physician unknown to the patient.
Maximal changes in intra-arterial
SBP/DBP recorded during the first
4-5 minutes of a physician's visit as
compared with the baseline average
SBP/DBP values of the 5 minutes
preceding the visit
Is the doctor’s visit a hypertensive urgency?
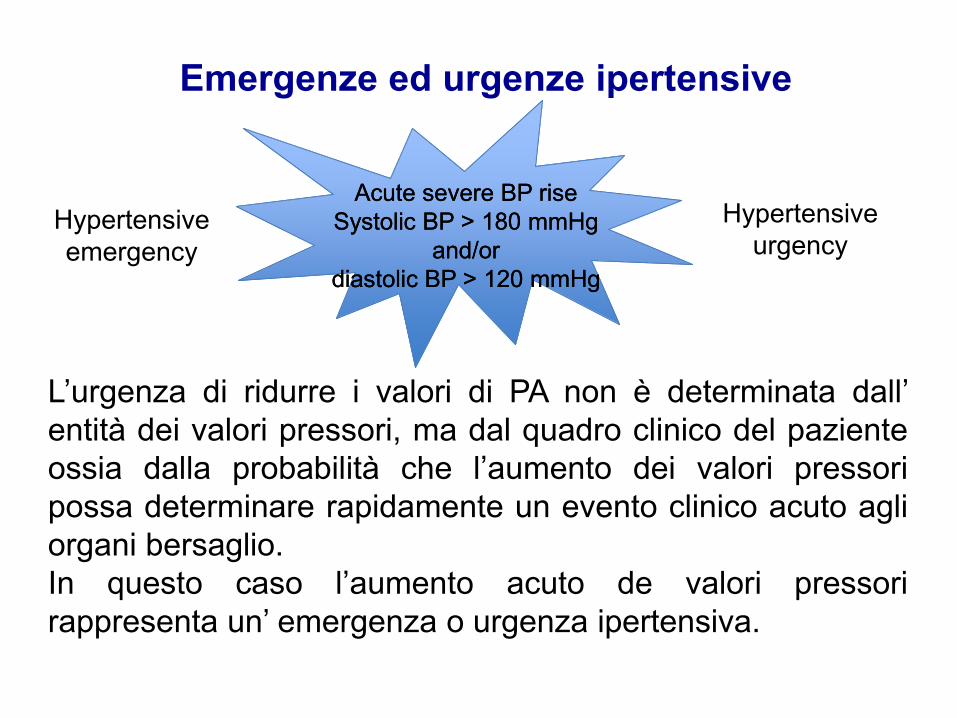
Emergenze ed urgenze ipertensive
L’urgenza di ridurre i valori di PA non è determinata dall’
entità dei valori pressori, ma dal quadro clinico del paziente
ossia dalla probabilità che l’aumento dei valori pressori
possa determinare rapidamente un evento clinico acuto agli
organi bersaglio.
In questo caso l’aumento acuto de valori pressori
rappresenta un’ emergenza o urgenza ipertensiva.
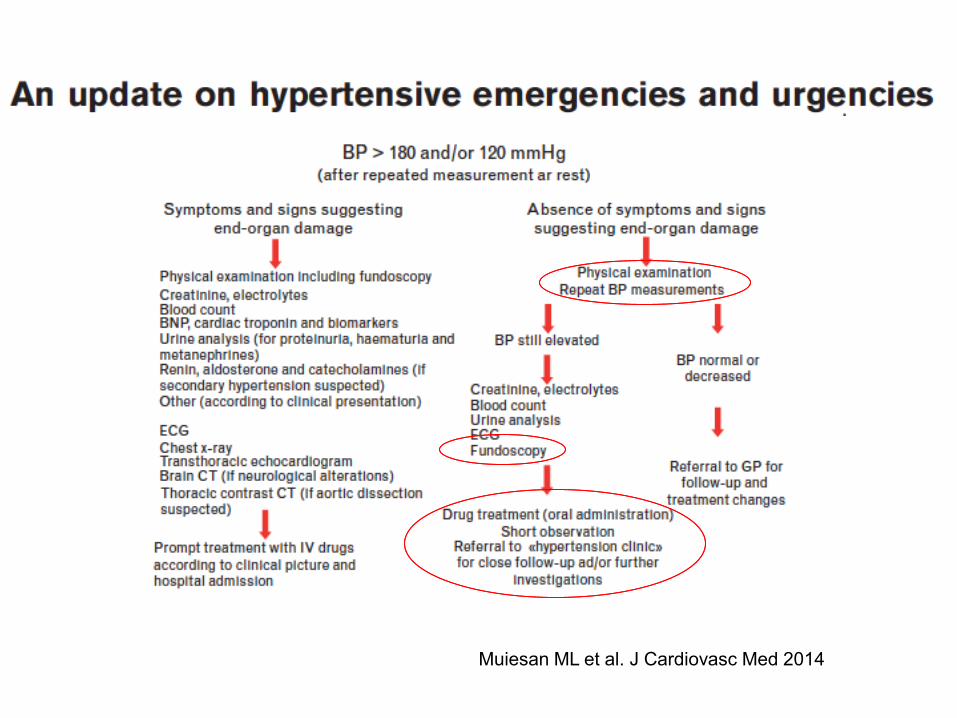
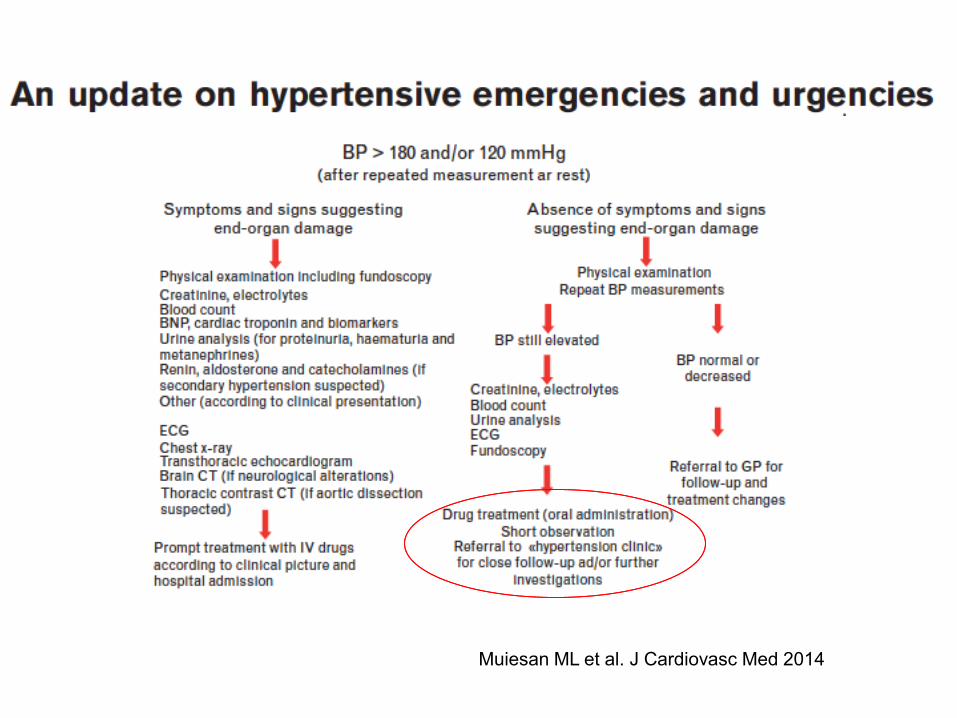
Hypertensive
emergency
Hypertensive
urgency
Acute severe BP rise
Systolic BP > 180 mmHg
and/or
diastolic BP > 120 mmHg
Acute severe BP rise
Systolic BP > 180 mmHg
and/or
diastolic BP > 120 mmHg
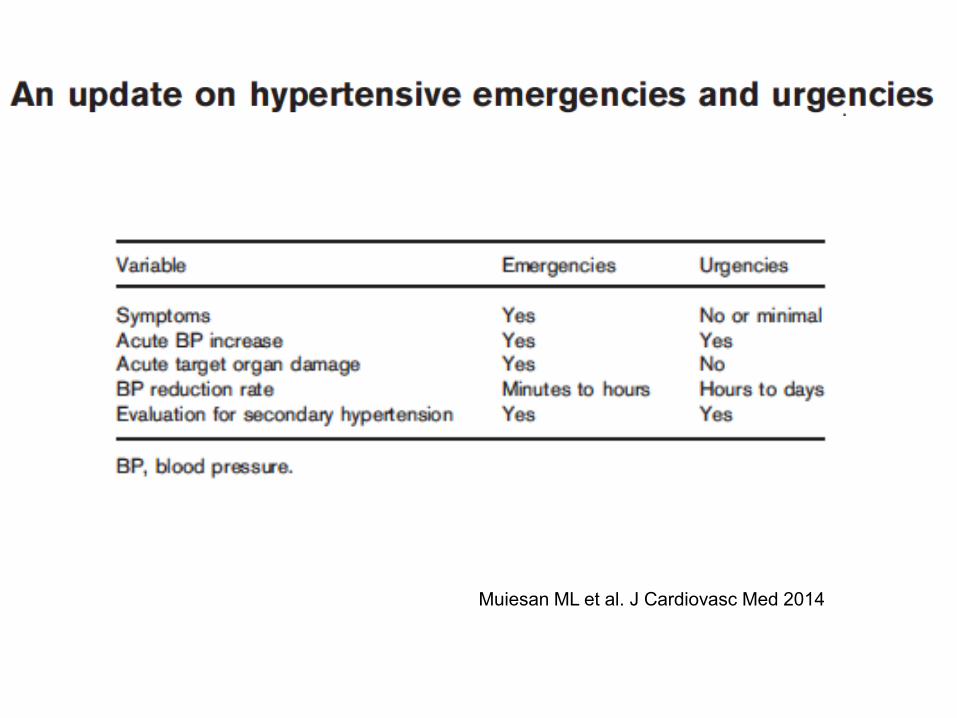
Muiesan ML et al. J Cardiovasc Med 2014
Muiesan ML et al. J Cardiovasc Med 2014
Most common presentations of hypertensive emergencies
in the ED are:
• pulmonary oedema and congestive heart failure
• cerebral infarction
• hypertensive encephalopathy
and also include:
intracranial haemorrhage, aortic dissection, myocardial
infarction, malignant hypertension, sympathetic crises
(cocaine toxicity/pheochromocytoma) and eclampsia.
The aim of treatment is to avoid an acute worsening of
organ damage and further long-term complications
Muiesan ML et al. J Cardiovasc Med 2014
• The choice of the best drug(s) with the better benefit–risk ratio
depends on the correct recognition of the clinical picture and the
consideration of comorbidities.
• Several rapid-acting intravenous agents are available for the
treatment of hypertensive emergencies and the choice is mainly
related to the clinical manifestation of end-organ damage
• The effect of these drugs should be carefully monitored in a proper
setting, in order to avoid an excessive velocity of BP reduction
• Sublingual nifedipine is not recommended.
Muiesan ML et al. J Cardiovasc Med 2014
Muiesan ML et al. J Cardiovasc Med 2014
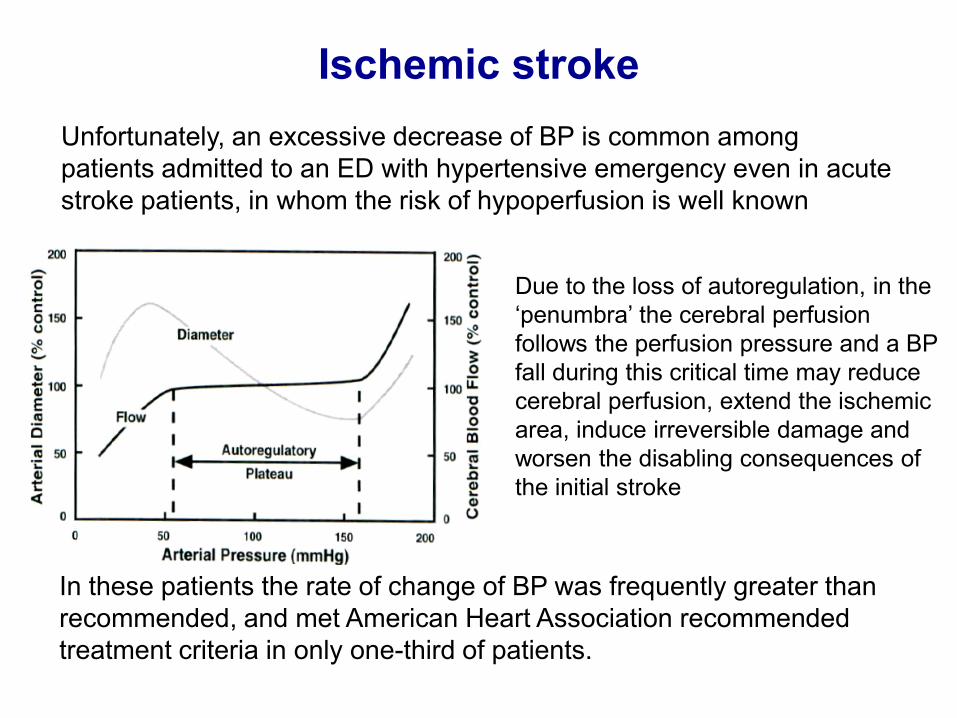
Due to the loss of autoregulation, in the
‘penumbra’ the cerebral perfusion
follows the perfusion pressure and a BP
fall during this critical time may reduce
cerebral perfusion, extend the ischemic
area, induce irreversible damage and
worsen the disabling consequences of
the initial stroke
Unfortunately, an excessive decrease of BP is common among
patients admitted to an ED with hypertensive emergency even in acute
stroke patients, in whom the risk of hypoperfusion is well known
Ischemic stroke
In these patients the rate of change of BP was frequently greater than
recommended, and met American Heart Association recommended
treatment criteria in only one-third of patients.
• The American Stroke Association (ASA) recommend that only BP
values repeatedly > 220/120 mmHg should be treated with either
labetalol or sodium nitroprusside, intravenously, unless there are
other indications for antihypertensive therapy (congestive heart
failure, myocardial infarction, aortic dissection).
• The BP target during the acute phase of an ischemic stroke should
not be a normal BP, but rather:
- 180/105 mmHg diastolic in previously hypertensive patients
- 160–180/90–100 mmHg in previously normotensive patients
Ischemic stroke
AHA/ASA Recommendations for BP Management in Acute Ischemic
Stroke also state that:
• Patients eligible for treatment with intravenous thrombolytics or other
acute reperfusion intervention and SBP 185 mmHg or DBP 110
mmHg should have BP lowered before the intervention.
• A persistent SBP of 185 mmHg or a DBP 110 mmHg is a
contraindication to intravenous thrombolytic therapy.
• After reperfusion therapy, keep SBP below 180 mmHg and DBP
below 105 mmHg for at least 24 h.
Ischemic stroke
AHA/ASA Recommendations for BP Management in Acute Cerebral
Hemorrhages state that:
• if SBP is higher than 200 mmHg or mean arterial pressure (MAP) is
higher than 150 mmHg, consider aggressive reduction of BP
• if SBP is higher than 180 mmHg or MAP is higher than 130 mmHg
and intracerebral pressure (ICP) may be elevated, consider
monitoring ICP and reducing BP to keep cerebral perfusion pressure
between 60 and 80 mmHg.
• if SBP is higher than 180 mmHg or MAP is higher than 130 mmHg
and there is no evidence of or suspicion of elevated ICP, consider
modest BP reduction (e.g. MAP of 110 mmHg or target BP of 160/90
mmHg).
Haemorrhagic stroke
Muiesan ML et al. J Cardiovasc Med 2014
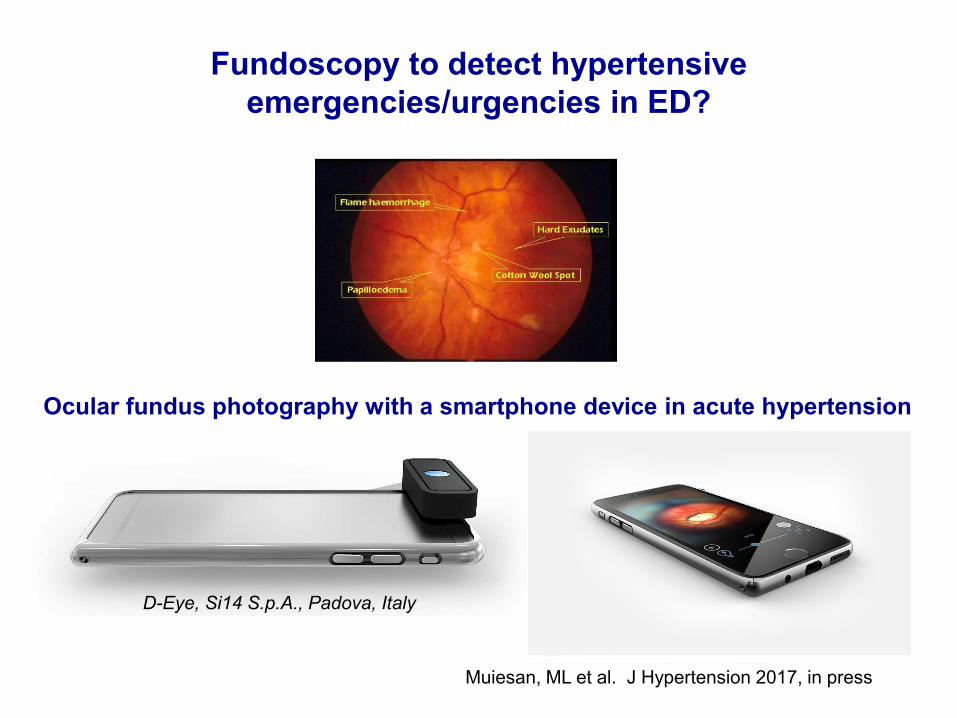
Fundoscopy to detect hypertensive
emergencies/urgencies in ED?
Muiesan, ML et al. J Hypertension 2017, in press
Ocular fundus photography with a smartphone device in acute hypertension
D-Eye, Si14 S.p.A., Padova, Italy
Muiesan ML et al. J Cardiovasc Med 2014
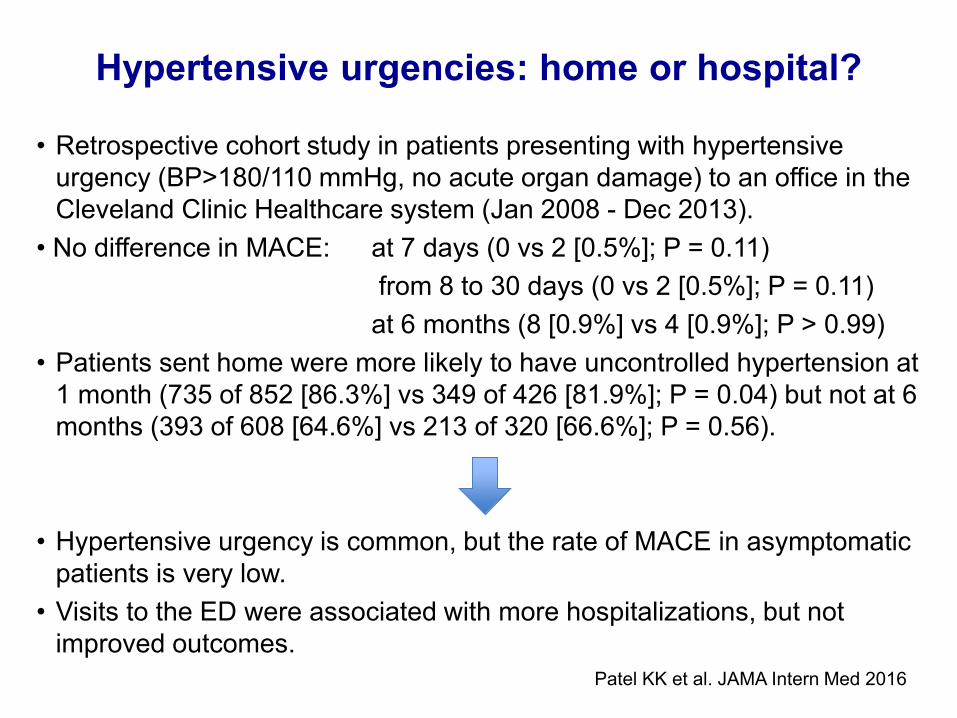
• Retrospective cohort study in patients presenting with hypertensive
urgency (BP>180/110 mmHg, no acute organ damage) to an office in the
Cleveland Clinic Healthcare system (Jan 2008 - Dec 2013).
• No difference in MACE: at 7 days (0 vs 2 [0.5%]; P = 0.11)
from 8 to 30 days (0 vs 2 [0.5%]; P = 0.11)
at 6 months (8 [0.9%] vs 4 [0.9%]; P > 0.99)
• Patients sent home were more likely to have uncontrolled hypertension at
1 month (735 of 852 [86.3%] vs 349 of 426 [81.9%]; P = 0.04) but not at 6
months (393 of 608 [64.6%] vs 213 of 320 [66.6%]; P = 0.56).
• Hypertensive urgency is common, but the rate of MACE in asymptomatic
patients is very low.
• Visits to the ED were associated with more hospitalizations, but not
improved outcomes.
Hypertensive urgencies: home or hospital?
Patel KK et al. JAMA Intern Med 2016
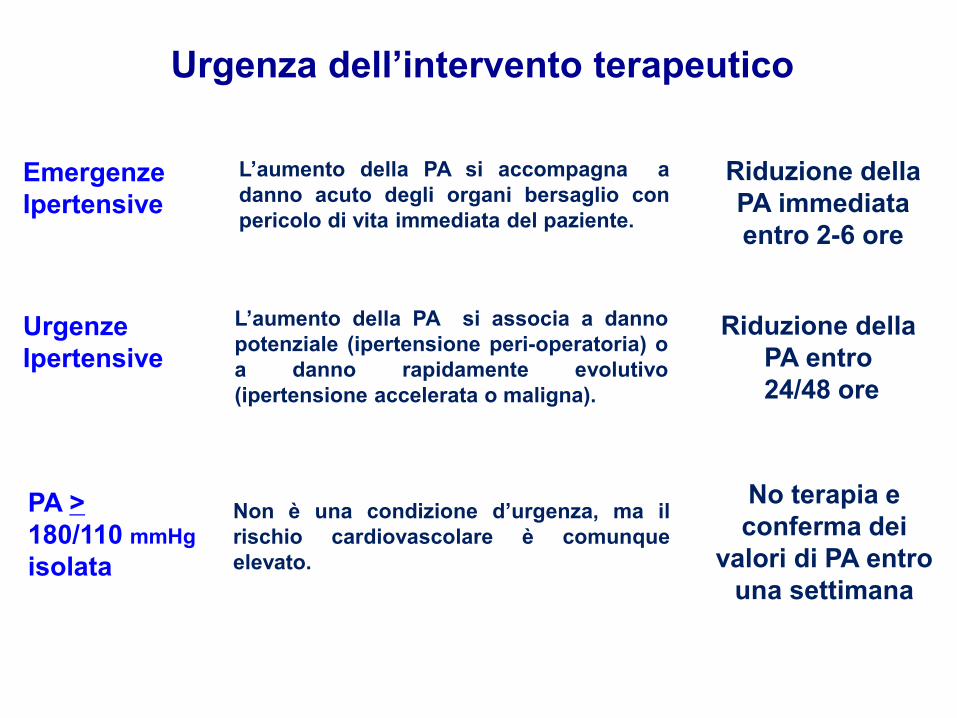
Emergenze
Ipertensive
L’aumento della PA si accompagna a
danno acuto degli organi bersaglio con
pericolo di vita immediata del paziente.
Urgenze
Ipertensive
L’aumento della PA si associa a danno
potenziale (ipertensione peri-operatoria) o
a danno rapidamente evolutivo
(ipertensione accelerata o maligna).
Riduzione della
PA immediata
entro 2-6 ore
Riduzione della
PA entro
24/48 ore
Urgenza dell’intervento terapeutico
PA >
180/110 mmHg
isolata
Non è una condizione d’urgenza, ma il
rischio cardiovascolare è comunque
elevato.
No terapia e
conferma dei
valori di PA entro
una settimana





























