Embed Size (px)
Citation preview

ARTICLE IN PRESS
1350-9462/$ - se
doi:10.1016/j.pr
�CorrespondE-mail addr
Progress in Retinal and Eye Research 24 (2005) 333–354
www.elsevier.com/locate/prer
Longitudinal changes in the visual field and optic disc in glaucoma
Paul H. Artes, Balwantray C. Chauhan�
Department of Ophthalmology and Visual Sciences, Dalhousie University, 2nd floor, Centennial Building, 1278 Tower Road,
Halifax, Nova Scotia, Canada B3H 2Y9
Abstract
The nature and mode of functional and structural progression in open-angle glaucoma is a subject of considerable debate in the
literature. While there is a traditionally held viewpoint that optic disc and/or nerve fibre layer changes precede visual field changes,
there is surprisingly little published evidence from well-controlled prospective studies in this area, specifically with modern
perimetric and imaging techniques. In this paper, we report on clinical data from both glaucoma patients and normal controls
collected prospectively over several years, to address the relationship between visual field and optic disc changes in glaucoma using
standard automated perimetry (SAP), high-pass resolution perimetry (HRP) and confocal scanning laser tomography (CSLT). We
use several methods of analysis of longitudinal data and describe a new technique called ‘‘evidence of change’’ analysis which
facilitates comparison between different tests. We demonstrate that current clinical indicators of visual function (SAP and HRP)
and measures of optic disc structure (CSLT) provide largely independent measures of progression. We discuss the reasons for these
findings as well as several methodological issues that pose challenges to elucidating the true structure–function relationship in
glaucoma.
r 2004 Elsevier Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334
1.1. Glaucoma: detection and progression of damage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334
1.2. Variability, change and diagnosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334
1.3. Importance of elucidating structure–function relationships in glaucoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
2. Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
2.1. Types of structure–function relationships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
2.2. Metrics of progression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
2.2.1. Subjective grading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
2.2.2. Event-based analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
2.2.3. Trend-based analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
3. Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
4. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
4.1. Glaucoma patients and healthy controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
4.2. Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
4.2.1. Static automated perimetry (SAP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
e front matter r 2004 Elsevier Ltd. All rights reserved.
eteyeres.2004.10.002
ing author. Tel.: +1902 473 3202; fax: +1 902 473 2839.
ess: [email protected] (B.C. Chauhan).

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354334
4.2.2. High-pass resolution perimetry (HRP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
4.2.3. Confocal scanning laser tomography (CSLT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
4.3. Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337
4.3.1. Progression with event-based analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 338
4.3.2. ‘Evidence of change’ (EOC) analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339
5. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 341
5.1. Event-based analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 341
5.2. EOC analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 343
5.2.1. Comparison between sensitivity and pattern deviation-based EOC analyses. . . . . . . . . . . . . . . . . . . . . . 343
5.2.2. Comparison of global EOC scores between SAP, HRP and CSLT . . . . . . . . . . . . . . . . . . . . . . . . . . . . 344
5.2.3. Simulations with randomly re-ordered data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 344
5.2.4. Sectorial visual field and optic disc changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 345
5.2.5. Relationship between visual field progression with SAP and HRP . . . . . . . . . . . . . . . . . . . . . . . . . . . . 346
5.2.6. Relationship between visual field and optic disc progression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 346
5.3. Baseline predictors of progression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 347
6. Case examples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 347
7. Discussion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 347
7.1. Visual field and optic disc changes: findings from these studies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 347
7.2. Clinical and biological measures of progression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351
7.3. Methodological issues in correlating functional and structural changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351
8. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 353
1. Introduction
1.1. Glaucoma: detection and progression of damage
Open-angle glaucoma is an age-related optic neuro-pathy that causes loss of retinal ganglion cells (RGCs).The pathogenesis of glaucoma has been linked to theaction of intraocular pressure (IOP) on the optic disccausing glaucomatous optic disc cupping and visual fielddefects (Hoskins and Kass, 1989; Epstein, 2004). Thereis no universally accepted definition of glaucoma,however, it is likely to represent a series of syndromesthat precipitate in glaucomatous damage. A diagnosis ofglaucoma is made after careful assessment of the opticdisc, visual field, a measurement of IOP and inconsideration of ocular, systemic and demographicfactors. The choices and degree of treatment dependon the initial level of field and disc damage as wellas on factors such as the patient’s lifestyle and lifeexpectancy.Clinically the visual field is measured most often using
conventional static automated perimetry (SAP), thoughother techniques such as high-pass resolution perimetry(HRP) (Frisen, 1987), frequency doubling technology(FDT) perimetry (Johnson and Samuels, 1997) andshort-wavelength automated perimetry (SWAP) (Sam-ple and Weinreb, 1989; Johnson et al., 1989) are also
used. The optic disc is examined clinically withophthalmoscopy and can be documented using conven-tional photography or one of the newer imagingtechniques such as confocal scanning laser tomography(CSLT) (Zinser et al., 1989). While the pattern andmode of progression of the visual field and optic dischave been studied and described by many authors usingtechniques from kinetic perimetry to SAP (Hart Jr. andBecker, 1982; Mikelberg and Drance, 1984; Mikelberget al., 1986; Chauhan et al., 1990; Spry and Johnson,2002; Nicolela et al., 2003) and from ophthalmoscopicexaminations and disc photography (Pederson andAnderson, 1980; Tuulonen and Airaksinen, 1991; Air-aksinen et al., 1992; Zeyen and Caprioli, 1993) to CSLT(Kamal et al., 1999; Chauhan et al., 2001), determiningwhether the visual field or the optic disc have changed inindividual patients remains one of the most challengingaspects of glaucoma management.
1.2. Variability, change and diagnosis
Central to the task of determining glaucomatousprogression is the distinction of true change fromvariability. Variability of measurements with SAPand CSLT has been studied extensively. Knowledgeof the biological variability of measurements in ahealthy population allows the clinician to determine

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 335
the likelihood that the visual field or optic disc showsigns of damage. While this approach is logical, thediagnostic accuracy of a technique will depend on theoverlap in a measurement of the visual field or optic discbetween groups of unselected glaucoma patients andhealthy subjects. The diagnostic accuracy also dependson the criteria by which subjects were selected into thestudy. If, for example, the criteria include an abnormalvisual field, it is not surprising that a measure of thevisual field will yield high diagnostic accuracy. Likewise,if optic disc appearance is part of the inclusion criteria,then it is not surprising that a measure of the optic discwill appear to provide good separation between thepopulations. Because the definition of glaucoma invari-ably includes the appearance of the optic disc and/orvisual field, independent assessments of the diagnosticaccuracy of these tests is difficult.Traditionally it is thought that the task of making a
diagnosis of glaucoma based on the visual field and/orthe optic disc (i.e., based on the probability of theobserved values being within normal limits) is distinctfrom determining the presence of progression. However,an alternative approach is to regard any change of thevisual field or the optic disc that exceeds normal ageingas a diagnostic sign, irrespective of whether themeasurements are within or outside the statisticallydefined normal limits. For example, the optic disc in apatient suspected of glaucoma may change, yet stillremain within the large range of physiological between-subject variability. In such cases, the evidence of changecan be used a diagnostic sign. Likewise, detectablechange over time in the visual field can be highlysuggestive of disease, even though the various visualfield indices may appear well within normal limits.
1.3. Importance of elucidating structure– function
relationships in glaucoma
Glaucoma is likely a disease that is modulated bymany factors. This may be related to the fact that thereis a wide range of optic disc appearances and visual fielddefects which can be classified as glaucomatous. Asdiscussed above, in many cases the appearance of thevisual field or optic disc alone may not be sufficient foraccurate diagnosis. In such cases, the clinical evidence isstronger if the optic disc appearance can be corrobo-rated with the visual field and vice-versa. Similarly,when optic disc change is suspected over time, corre-sponding changes in the visual field may strengthen thelevel of clinical information. Whether visual field andoptic disc changes in longitudinal studies occur intandem is one of the subjects of this paper.Elucidating the relationship between a functional and
structural test, or indeed two functional tests, is alsoimportant to determine the relative utility of the tests atthe different stages of disease. For example, it is
frequently thought that optic disc examination orquantification has more utility during the earlier stagesof the disease than SAP, while psychophysical tests mayhave greater utility during the later stages of the disease.It is also thought that SWAP may have more utility thanSAP in early glaucoma, but less so in the advancedstages, owing to the limited dynamic range of SWAP(Demirel and Johnson, 2000).Finally, elucidating the structure–function relation-
ship in glaucoma is scientifically important in determin-ing the order of changes during the disease process.Determining this information in different sub-types ofglaucoma, for example based on optic disc appearance(Nicolela et al., 2003), may shed light on the nature ofprogression and may eventually allow a more tailoredapproach to treatment.
2. Review
2.1. Types of structure– function relationships
Correlating visual function to a structural parameterderived from the optic disc, or nerve fibre layerappearance, and visual function in a populationdescribes the strength of such a relationship at onepoint in time. An often-made assumption is that thiscross-sectional relationship is a useful ‘first approxima-tion’ for the longitudinal relationship between functionand structure in individual patients. For example, theslope of the relationship between, say, the visual fieldmean deviation in SAP and the neuroretinal rim areaacross a population is used as the postulated change ofthe visual field and optic disc in individuals observedover time. The use of cross-sectional data to predictlongitudinal behaviour in individual patients may not beappropriate, even though statistically strong relation-ships can be derived from cross-sectional data. Thevalidity and usefulness of this approach, specificallywhen dealing with individual patients in a clinicalfollow-up, requires investigation.
2.2. Metrics of progression
Visual field and optic disc changes have beenmeasured using a variety of methods that range froma subjective clinical judgement based on only twoobservations to complex statistical analyses of manyobservations in time. Study outcomes depend criticallyon the metric of progression used, and there is noexternal standard by which the performance of thesemetrics can be judged (see Section 7.2).
2.2.1. Subjective grading
Subjective grading of changes in the visual field(Werner et al., 1988; Spry and Johnson, 2002) and optic

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354336
disc (Collaborative Normal-Tension Glaucoma StudyGroup, 1998; Heijl et al., 2002) has been used tocategorize progressing and non-progressing eyes. In thistype of assessment, there is minimal, if any, standardiza-tion of the criteria used for change. Advantages of thisapproach are the similarity to real clinical practice andease of use. There are significant limitations, includingthe often reported poor inter-rater and intra-rateragreement (Werner et al., 1988; Varma et al., 1992;Viswanathan et al., 2003; Azuara-Blanco et al., 2003).Classifications are usually binary (normal/glaucomatousor stable/progressing) although a wider scale of ratingsmay provide more informative classifications. Finally,subjective grading does not use the analytical potentialof many modern perimeters and imaging devices.
2.2.2. Event-based analysis
In this form of analysis, a follow-up examination iscompared to a baseline of a single or mean of two ormore examinations. This approach is used commonly inthe analysis of visual field data and is availablecommercially in the Statpac programme (Heijl et al.,1991) of the Humphrey Field Analyser (HFA, CarlZeiss Meditec Inc., Dublin, CA). It is also used in theanalysis of CSLT images in the Topographical ChangeAnalysis (TCA) of the Heidelberg Retina Tomograph(HRT, Heidelberg Engineering GmbH, Dossenheim,Germany). With visual fields, the changes (i.e. thedifferences between baseline and follow-up examina-tions) are compared to the test–retest variability from aseparate sample of patients. If the observed changesexceed the test–retest limits (typically estimated byempirical 5th and 95th percentiles), actual change islikely to have occurred. In contrast, the TCA analysis ofHRT data evaluates the significance of the observedchanges between baseline and follow-up with referenceonly to the individual patient’s variance at a particularlocation, and not to values derived from a population(Chauhan et al., 2000).Progression is then defined on the basis of a somewhat
arbitrarily chosen cut-off, for example a given numberof test locations with a given amount of change on agiven number of consecutive follow-up examinations.The typically binary nature of this approach (stable/progressing) is subject to limitations similar to thosediscussed for subjective grading (Section 2.2.1).
2.2.3. Trend-based analysis
In this approach, regression analysis of a dependentvariable, such as visual field sensitivity or neuroretinalrim area is performed on follow-up time. The choice ofdependent variables is considerable, varying from highlylocalized to global ones. Trend-based analyses can bevery powerful, especially when many observationsare available. Because regression techniques implicitlyaccount for the variability within each subject (as
compared to event-based analyses which for visual fieldanalysis are usually based on test–retest variability in asample of patients), they have the potential to detectsubtle progression which may not be apparent in event-based analyses, but generally at the expense of moreexaminations and/or follow-up time (Vesti et al., 2003).Trend-based approaches are also available in visual fieldanalysis programs such as Statpac (Heijl et al., 1991),Progressor (Viswanathan et al., 1997) and Peridata(Peridata Software GmbH, Hurth, Germany).Similar to event-based analysis, the definition of
progression using this approach is arbitrary and canbe based on the number of visual field locations showinga given magnitude of slope and/or statistical signifi-cance.
3. Purpose
The paper describes a comprehensive investigation onprogression in glaucoma in a group of patients withopen-angle glaucoma who were followed in a prospec-tive study for several years. We also report data from acohort of healthy controls followed identically. We havedeveloped a new method of analysing progression calledevidence of change (EOC) to facilitate the comparisonbetween different tests and describe the use of this metricas well as of others to elucidate the relationship betweenchanges in the visual field and optic disc using SAP,HRP and CSLT.
4. Methods
4.1. Glaucoma patients and healthy controls
This paper reports on data from 84 patients with aclinical diagnosis of open-angle glaucoma, and 41healthy controls, followed in a prospective longitudinalstudy. Patients were recruited consecutively from theglaucoma clinics of the Eye Care Centre at the QueenElizabeth II Health Sciences Centre while the controlswere enrolled from a local telephone company, seniors’groups and local church organizations in Halifax, NovaScotia. The study was approved by the institutionalResearch Ethics Committee, and all participants gavewritten informed consent. Patients were included ifthey had a clinical diagnosis of open-angle glaucomawith optic nerve and visual field damage compatiblewith glaucoma. Controls had intraocular pressureo21mmHg and a normal eye examination. Subjectswere excluded from the study if the refractive errorexceeded 5D equivalent sphere or 3D of astigmatism, orif their best-corrected visual acuity was worse than 6/12.The demographic details of both subject groups aregiven in Table 1.

ARTICLE IN PRESS
Table 1
Details of patient and control samples (medians and ranges)
N Age (yr) Follow-up (yr) Number of exams Baseline MD (dB)
Glaucoma 84 62.7 (31–88) 7.4 (2–9) 14 (5-18) �4.0 (+0.4, �14.9)
Control 41 57.2 (34–76) 7.5 (2–9) 7 (5–16) �0.2 (+1.5, �4.2)
Fig. 1. Stimulus used in high-pass resolution perimetry. The space-
averaged luminance of the bright core and the dark borders equal that
of the background.
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 337
If both eyes of a subject were eligible, one randomlyselected eye of each subject was assigned the study eyeand examined at intervals of 6 months. At each session,SAP, HRP, and CSLT were performed. For the analysisreported in this paper, subjects were included if datafrom at least five sessions were available. We did notattempt to exclude data from any subject for failing tomeet arbitrary reliability criteria. The reason for thefewer median number of examinations in the controlscompared to patients (but a similar follow-up time) isthat the follow-up of the controls was planned initiallyfor only for 5 years, however, we subsequently extendedthe study and ‘re-recruited’ these subjects. In contrast,the glaucoma patients were followed continuously. Bothgroups were followed identically at 6-monthly intervals.Our analyses took account of these differences in follow-up (see Section 4.3).
4.2. Tests
4.2.1. Static automated perimetry (SAP)
SAP was carried out using the Humphrey FieldAnalyzer (Carl Zeiss Meditech, Dublin, CA). Through-out the follow-up, the field was examined with the 30-2program using the full-threshold strategy and a Gold-mann size III stimulus (subtending 0.431). Although allpatients were examined with the 30-2 program (76locations), all analyses reported in this paper were basedon the 52 test locations of the 24-2 test (excluding thetwo blind spot locations).
4.2.2. High-pass resolution perimetry (HRP)
HRP was carried out using the Ring program ofthe Ophthimus system (HighTech Vision, Goteborg,Sweden). The technique is described in full elsewhere(Frisen, 1987). In brief, this program examines 50 testlocations of the central visual field using a single-reversalstaircase technique with a ‘vanishing optotype’ stimulusthat contains predominantly high spatial frequencies(Fig. 1). The size of the stimuli is varied in 12 discretesteps of 0.1 log (step size 1.26) while the stimulusMichelson contrast of 0.25 is kept constant.
4.2.3. Confocal scanning laser tomography (CSLT)
The Heidelberg Retina Tomograph (Heidelberg En-gineering GmbH, Dossenheim, Germany) was used toacquire three-dimensional topography images of theoptic disc. The technique is described in detail elsewhere
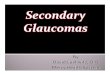
(Zinser et al., 1989; Chauhan, 1996). In brief, the deviceacquires 32 confocal images from different focal planesin the optic nerve head and the peripapillary retina. Thetopography of these structures is then reconstructedfrom the image series. At each session, three scans of10� 101, centred at the optic disc were obtained andaveraged to derive mean topography and reflectanceimages. Using the Heidelberg Eye Explorer software(version 1.4.0.1), an experienced observer (BCC) thendrew a contour line to coincide with the optic discmargin and reviewed all images in the series to ensureadequate alignment. In cases in which the automaticalignment algorithm had failed, we used the optionalmanual alignment feature of the software whichprompts the user to identify at least four landmarkssuch as vessel bifurcations. The stereometric parametersoptic disc and rim area based on the standard referenceplane (both global and sectoral, see Section 4.3.2.2) aswell as the probability maps of the TopographicalChange Analysis (TCA) were exported. Fig. 2 shows anexample of the probability maps of the TCA and thecorresponding optic disc topographies in four follow-upexaminations.
4.3. Analyses
We assessed progression with both event- and trend-based methods. The rationale and methodology of theseanalyses is described below.

ARTICLE IN PRESS
Fig. 2. Baseline and subset of follow-up examinations in an eye with progressive enlargement of the cup. Probability maps of the Topographical
Change Analysis (top) and corresponding topography images (bottom) showing the expanding cup (red) and decreasing neuroretinal rim (green and
blue).
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354338
4.3.1. Progression with event-based analyses
4.3.1.1. Rationale. Event-based change analyses are avaluable clinical tool for detecting progression. Com-pared to trend analyses, event-based methods mayrequire fewer tests to alert clinicians to the possibilitythat change may have taken place. They may also bebetter suited to detect episodic changes after a period ofstability (Spry and Johnson, 2002).It is not meaningful to compare sensitivities between
different tests unless their respective specificities areequal. A test that has lower specificity (i.e. falsely flagsprogression where no true change has taken place) islikely to be more sensitive to change compared to a testwith high specificity. The ideal approach to compareprogression rates, therefore, would be to equalize thespecificities with each test. However, owing to the lackof an external standard, this is difficult to achieve withreasonable confidence. Owing to sampling variation, thelimits of test–retest variability derived in one sample ofpatients may not be identical to those that would havebeen derived from another sample, yet even smalldifferences in specificity are likely to have a large effecton the tests’ sensitivity to change. A meaningfulcomparison of progression rates, based on empiricaldata, is therefore very difficult to make.In the studies described below, we therefore assessed
the agreement between tests after deriving sets of criteriawith similar progression rates. The likely specificity ofthese criteria can be estimated by examining the rate ofimprovement (positive change), assuming (a) thatgenuine improvements do not occur, and (b) that chanceimprovements are similar in frequency and magnitude tochance deterioration. The first assumption, of course, isnot always valid. Patients may, for example, showlearning effects that manifest as visual field improve-ment. Similarly, not all positive height changes at the
optic disc are necessarily due to chance as changes in theoptic nerve head due to glaucoma may lead to negativeas well as positive height changes. However, by treatingall positive changes as chance events we are likely tounderestimate (rather than overestimate) the truespecificity of the tests.
4.3.1.2. Methodology. With the visual field tests (SAPand HRP), our event-based analyses were similar to theGlaucoma Progression Analysis (GPA, Carl-Zeiss Med-itech, Dublin, CA) of the HFA. These analyses compareeach location in the follow-up visual field examination,point by point, to the respective baseline of two earlierexaminations. In our analysis, locations at which theobserved change exceeded the 5th or 95th percentilelimits of test–retest variability (estimated in a separategroup of glaucoma patients), probable deterioration orimprovement were marked with black or white triangles,respectively. We based our criteria for visual fielddeterioration or improvement on the number of testlocations identified in this analysis on at least threeconsecutive examinations (Fig. 3).In the present study, the change probability analyses
were based on pattern deviation. By adjusting forchanges in the general height of the visual field(estimated by the 85th percentile of the total-deviationvalues), pattern deviation analyses aim to distinguishlocalized progression from diffuse changes over time.These analyses would therefore be expected to beresistant against overall visual field changes that maybe caused by conditions other than glaucoma (e.g.development of cataract (Bengtsson et al., 1997)).However, it is important to note that by disregardingany non-focal visual field change, pattern deviationanalyses may also underestimate the true amount ofglaucomatous visual field progression.

ARTICLE IN PRESS
Fig. 3. Example of progression analysis with pattern deviation change probability analyses. Locations with probable deterioration from baseline are
marked by black triangles, those with probable improvement by white triangles. Circles show locations with deterioration on three consecutive tests.
Criteria for progression (change in three consecutive tests) were first met in 8/97 (4 locations) and in 7/98 (5 locations).
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 339
Optic disc change was identified with the probabilitymaps of TCA. This analysis, described in detailelsewhere (Chauhan et al., 2000) establishes the statis-tical significance of surface height changes from base-line. The mean topography images (resolution 256� 256pixels) are condensed to topographical probability mapscontaining 64� 64 superpixels. Superpixels with statis-tically significant height change (po0:05) in threeconsecutive probability maps are marked in red (fornegative height changes) or green (positive change)(Fig. 2). The criteria for change were described in termsof the largest cluster of red superpixels within the opticdisc boundary. To account for the large physiologicalvariation in optic disc size, we expressed the size of thiscluster as a percentage relative to the total number ofsuperpixels within the contour line. With all three tests,positive and negative changes were evaluated separately.
4.3.1.3. Description of study. We derived three sets ofcriteria (subsequently referred to as ‘least conservative’,‘intermediate’, and ‘most conservative’), so that thenumber of progressing patients at the end of the follow-up period were similar between the three tests. Kaplan-Meier survival curves were then established for bothprogression and improvement. To visualize the agree-ment between the three tests, we plotted area-propor-tional Venn diagrams (Chow and Ruskey, 2004) inwhich the rectangular areas and their overlap areproportional to the number of patients who wereclassified as progressing with each combination of thethree techniques.
4.3.2. ‘Evidence of change’ (EOC) analyses
4.3.2.1. Rationale. The ‘evidence of change’ (EOC)analyses were established to summarize the strength of
the statistical evidence for change in longitudinal visualfield and optic disc data. The objective of these analysesis to enable a fair comparison of the utility of these testsin detecting progression of glaucoma. Rather thancomparing absolute changes (for example, the loss ofvisual field sensitivity over time in dB/year, or the loss ofneuroretinal rim area in mm2/year), the EOC analysescompare the strength of the evidence that the measure-ments have changed over time. This is accomplished byrelating the magnitude of the observed trend (‘signal’) tothe observed variability of the measurements (‘noise’).One convenient measure of the ‘signal-to-noise ratio’between the absolute amount of change and thevariability of the measurements is the statistical sig-nificance of the trend. A statistically significant trendmeans that any systematic change in the data is unlikelyto have arisen by chance, i.e., that it is likely that sometrue change has taken place. The EOC analyses weretherefore based on an ordinal grading of the statisticalsignificance (p-value) of the trend.Although they are related, there is a critical difference
between the absolute amount of change and thestatistical EOC. The former depends solely on thepatient and the nature of the disease, while the latterdepends also on the tools with which we measure visualfunction and optic disc topography. For example, agiven trend in the data (‘signal’) may have arisen purelyby chance if the variability of the measurements (‘noise’)was high, and we can therefore not be confident that themeasured trend reflects some genuine alteration in themeasured variable (low EOC). If the measurements hadlower variability, the same amount of change would beless likely to have occurred by chance, yielding greaterconfidence (better evidence) that the underlying variablehas truly changed. A hypothetical example for the

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354340
relationship between the change, variability, and statis-tical significance is given in Fig. 4. Owing to its lowvariability, test A generates a high EOC score. With testB, the larger variability of the measurements make itplausible that the trend has arisen by chance, eventhough the rate of decline appears much higher thanwith test A. Because the objective of the EOC analyses isto compare the effectiveness of different tests indetecting change, it is important that these analysesreflect both on the amount of change that is taking place(the ‘signal’) as well as on any factors that relate to ourability to measure this change (e.g. the ‘noise’ ofmeasurement error).Data from various tests are also difficult to compare
owing to the differences between the tests’ samplingstrategies. The visual field tests in our study (SAP andHRP), for example, examine approximately 50 testlocations in the central visual field, while severalthousand discrete measurements are obtained with eachCSLT mean topography. To establish a commonframework within which a fair comparison betweenthe tests could be carried out, while preserving the
Fig. 4. Comparison between two hypothetical visual field tests. Owing to its l
test B (right), even though the absolute rate of change in A (�1 dB/yr) is les
Fig. 5. Visual field sectors for SAP (left) and HRP (centre) and correspondin
to the inferior optic disc sectors, the central visual field sectors to the tempor
disc, and the inferior visual field to the superior optic disc sector. The fixation
shaded in black and are excluded from the analysis.
sensitivity of the analyses to localized changes, the EOCanalyses were based on a subdivision of the visual fieldand optic disc into several corresponding sectors whichwere then evaluated separately.
4.3.2.2. Methodology. From several schemes thathave been proposed for the correspondence betweenfunctional and structural measures (Weber and Ulrich,1991; Garway-Heath et al., 2000), we selected thescheme proposed by Junemann et al. (Junemannet al., 2000) for its simplicity and subdivided the visualfield and the optic disc into four corresponding sectors(Fig. 5).For the visual field tests, we calculated the pattern
deviation at each test location based on previouslypublished normative data (Heijl et al., 1987; Wall et al.,2004). The pointwise values were then averaged toobtain the mean pattern deviation values within eachvisual field sector. The series of mean pattern deviationvalues of each of the four visual field sectors were thenevaluated for statistically significant trends as describedbelow. The analyses were based on pattern deviation in
ower variability, test A (left) generates greater evidence of change than
s than in B (�2 dB/yr).
g optic disc sectors (right). The superior visual field sectors correspond
al optic disc sector, the temporal visual field sectors to the nasal optic
points are marked by crosses, the blind spot areas of the visual field are

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 341
order to minimize the influence of age-related changesand of diffuse losses of visual field sensitivity that maybe caused by non-glaucomatous ocular conditions suchas cataract.For CSLT, we computed the correlation between the
sectoral optic disc rim area (see Section 4.2.3 and Fig. 5)and follow-up time, and no corrections for potentialage-related changes were carried out.The strength of the trends in the four sectors were
evaluated by Spearman’s rank correlation coefficient.Because this coefficient is based on the rank order of themeasurements, there is no requirement for the under-lying change to be linear. Moreover, the rank methodminimizes the influence of outliers. Because the oftenused asymptotic approximations can be inaccurate withsmall samples, we used the exact significance valueswhich state the probability that the measurements couldhave been obtained in the same order purely by chance(Glasser and Winter, 1961). Trends were evaluatedseparately in each sector and graded on an ordinal scaleaccording to their statistical significance (Table 2). Thegrades of the four sectors were then summed into aglobal EOC score (ranging from 0 (very low EOC) to 20(very high EOC)), and the EOC scores for progressionand improvement were evaluated separately. It shouldbe noted that the EOC analyses did not attempt todistinguish between different spatial patterns of pro-gression. A visual field with borderline significant (e.g.p ¼ 0:07) change in three visual field sectors would havebeen assigned an EOC score of 3, the same as a visualfield with more significant change (e.g. p ¼ 0:015) in asingle sector only.
4.3.2.3. Description of studies. As a first step, wecompared the EOC analyses based on sensitivity (rawthreshold) and pattern deviation values. Pattern devia-tion analyses aim to compensate for any ‘overall’changes of the visual field, including any age-relatedphysiological decreases in sensitivity, and negativepattern deviation EOC scores (progression) shouldtherefore occur less frequently than those establishedwith raw threshold values. Also, progression andimprovement scores would be expected to be similar inthe healthy controls.
Table 2
Significance values and corresponding grades of the EOC analysis
Significance (p-value) Grade
p40:1 0
:0:1Xp40:05 1
0:05Xp40:02 2
0:02Xp40:01 3
0:01Xp40:002 4
po0:002 5
Secondly, using the data from glaucoma and controlpatients, we compared the EOC scores of the three tests(SAP, HRP and CSLT). As the EOC analyses evaluateall three tests on a common scale, a direct comparisonbetween the EOC scores reveals which of the threetechniques is, on average, most effective in detectingchange. Further, the topographical distribution ofsectorial EOC scores would be expected to conformand add to what is already known about the spatialpatterns of visual field and optic disc progression. Thecomparison of EOC scores from individual patientsindicates the agreement between different tests, inde-pendent of any criterion that is arbitrarily chosen todichotomize patients into ‘progressing’ or ‘not progres-sing’ categories.Thirdly, we carried out simulation experiments to
validate the EOC approach and to investigate thedistribution of scores under the null hypothesis (absenceof true change over time). In these experiments, the testresults for each patient were randomly reordered withrespect to follow-up time. At each iteration, a newrandom sequence was chosen (random resamplingwithout replacement), and 10 such iterations wereevaluated for each patient. Using this approach, wedid not have to make any assumptions as to thestatistical distribution of our measurements or theinterdependence of trends between different sectorswithin a patient’s visual field and optic disc. The EOCscores of the randomly reordered data were thencompared to the scores of the original data.
5. Results
5.1. Event-based analyses
Fig. 6 shows the Kaplan-Meier survival curves forchange in the glaucoma patients, based on the threecriteria (from least conservative to most conservative)that led to similar numbers of patients classified asprogressing over the follow-up period.The least conservative set of criteria classified
progression in approximately 42% of the glaucomapatients, while the respective figures for the intermediateand most conservative criteria were 25% and 17%,respectively.With all criteria, the agreement between the two visual
field tests (SAP and HRP) was substantially higher thanthat between either of the field tests and CSLT (Fig. 7).The number of patients classified as progressing with allthree tests varied from 16 (least conservative criteria) to3 (most conservative criteria).The same sets of criteria were employed to measure
apparent improvement. While the least conservative setof criteria (1 location with significant pattern deviationimprovement in three consecutive tests) classified a fairly

ARTICLE IN PRESS
Fig. 7. Area proportional Venn diagrams of the classifications with least conservative, intermediate, and most conservative criteria, based on event
analyses. The areas enclosed by each rectangle and their overlap are proportional to the numbers of patients classified as progressing by the respective
tests.
Fig. 6. Kaplan-Meier survival curves for progression (bold line) and improvement (thin line) for SAP, HRP, and CSLT, in glaucoma patients. The
top panels show the results for the least conservative set of criteria with the progression criterion for each test i.e., 1 location each for SAP and HRP
and a cluster of red or green superpixels equivalent in size to 6% of the area within the contour line in the CSLT analysis. The middle and lower
panels show the survival curves for the intermediate and most conservative criteria, respectively. Curves are absent if no events were detected.
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354342

ARTICLE IN PRESS
Fig. 8. Comparison of global EOC scores of visual field change with
SAP and HRP for patients (solid bars) and controls (hollow bars).
Both progression (negative values) and improvement (positive values)
were determined with sensitivity (left) and pattern deviation (right)
analysis. Error bars show the 95% confidence interval of the mean
(shown in one direction only).
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 343
large number of glaucomatous visual fields as improving(16 (19%) and 20 (24%) patients were classified asimproving with SAP and HRP, respectively), the moreconservative criteria classified improvements rarely ornever—indeed only one patient showed apparentpositive change with two locations on SAP. With theCSLT criteria, apparent improvements were morecommon—they occurred in 12, 8 and 2 glaucomapatients, respectively, with the least conservative, inter-mediate, and most conservative criteria.It is interesting to note that the frequency of
improvements varied considerably between the techni-ques, even though the progression rates were equalized.In particular, the ‘improvement’ rate with CSLT wasnoticeably higher (both for patients and controls) thanwith the visual field tests (Table 3). This underscores ourhypothesis that green superpixels cannot simply beinterpreted as ‘chance improvement’ as they arefrequently found in conjunction with red superpixels inthe presence of dramatic alterations in optic disctopography.When we applied the above criteria, derived in
glaucoma patients, to the healthy control group, therewere no statistical differences between the Kaplan-Meiersurvival curves for progression and improvement withany of the three tests (p40:1; log-rank tests). With bothvisual field tests, the progression rate in the controls wasvery low. Even with the least conservative criteria, only4 (10%) and 3 (7%) control subjects had been classifiedas progressing with SAP and HRP at the end of thefollow-up time, and no controls were classified with theintermediate or the most conservative criteria. Similarly,apparent visual field improvement in the controls wasonly detected with the least conservative criterion,occurring in only 1 (2%) and 6 (15%) of controlsubjects with SAP and HRP, respectively. With CSLT,apparent improvement occurred in 4, 2, and 1 controlswith the criteria of 6%, 10%, and 18% of clusteredgreen superpixels within the optic disc boundary.
Table 3
Patients and controls classified as progressing and improving according to
percentages
SAP HRP
Progressing Improving Prog
Patients (n ¼ 84)
Least conservative 35 (42%) 16 (19%) 35 (4
Intermediate 22 (26%) 1 (1%) 20 (2
Most conservative 15 (18%) 0 14 (1
Controls (n ¼ 41)
Least conservative 4 (10%) 1 (2%) 3 (7
Intermediate 0 0 0
Most conservative 0 0 0
5.2. EOC analyses
5.2.1. Comparison between sensitivity and pattern
deviation-based EOC analyses
To enable a comparison between the EOC analysesbased on sensitivity (i.e., the raw threshold values,without any age correction) and those based on patterndeviation (which corrects for age as well as for anyoverall shifts in visual field sensitivity), the averageglobal EOC scores are shown in Fig. 8. For this analysis,EOC scores of progression (negative trends) were givena negative sign and summed across the four sectors. As acontrol analysis, we proceeded similarly for the EOCscores of improvement (positive trends). Both progres-sion and improvement scores were treated indepen-dently from each other.In patients and controls, the pattern deviation-based
analyses gave lower (less negative) progression scores
the 3 criteria with SAP, HRP, and CSLT. Figures in brackets show
CSLT
ressing Improving Progressing Improving
2%) 20 (24%) 35 (42%) 12 (14%)
4%) 0 21 (25%) 8 (10%)
7%) 0 14 (17%) 2 (2%)
%) 6 (15%) 5 (12%) 4 (10%)
0 3 (7%) 2 (5%)
0 3 (7%) 1 (2%)

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354344
than the sensitivity-based analyses. By compensating forany overall changes of visual field sensitivity (as well asfor the physiological sensitivity losses with age), thepattern deviation analyses are robust to ageing effects aswell as to diffuse elements of visual field progressionthat may be caused by non-glaucomatous conditionssuch as cataract. Therefore as expected, the patterndeviation-based EOC scores of progression and im-provement were very similar in the controls. In contrast,the sensitivity-based EOC scores of the controls wereslightly larger for progression than for improvement,which is likely to reflect ageing effects in the visual field.All further investigations were therefore based onpattern deviation analyses to reduce the potentiallyconfounding effects of ageing. However, by disregardingany diffuse change, the pattern deviation analyses arelikely to somewhat underestimate the true amount ofprogressive visual field change.
5.2.2. Comparison of global EOC scores between SAP,
HRP and CSLT
The EOC analyses were developed to facilitate anobjective comparison between different tests. The meanglobal EOC scores of the three tests are shown in Fig. 9.Not surprisingly, the EOC progression scores of theglaucoma patients were larger than those of the controlsas progressive visual field and optic disc changes areamong the features that define glaucoma. In contrast,the improvement scores were similar in both groups ofsubjects, suggesting that the analyses perform equallywell in both groups, despite the smaller number ofsessions in the control group (Table 1).Comparing the three tests, the negative EOC scores
were slightly larger for CSLT as compared to SAP and
Fig. 9. Mean global EOC scores for progression (negative values) and
improvement (positive values) for patients (solid bars) and controls
(hollow bars) with all tests. Error bars (shown in one direction only)
indicate the 95% confidence interval of the mean.
HRP. Interestingly, this applied to glaucoma patients aswell as to the healthy controls. Also, with CSLT, thenegative EOC scores in the controls were slightly largerthan the positive scores. This suggest a decreasing rimarea measured longitudinally in normal subjects, whichwe believe is the first report of this finding in normalsubjects using modern imaging devices.In the glaucoma patients, the EOC progression scores
with CSLT tended to be larger than those of SAP andHRP. This suggests that, on average, CSLT may bemore effective at detecting progression compared to thevisual field tests. However, as noted above (Section5.2.1), the pattern deviation analyses of the SAP andHRP data compensated for any diffuse components ofvisual field progression and are therefore likely tosomewhat underestimate the true amount of progres-sion. Also, a fair comparison between the three tests isfurther complicated by the fact that there was nocorrection for age-related rim area change with the EOCanalysis of the CSLT data. Altogether, however, thedifferences between the mean EOC progression scores ofthe three tests were neither large nor statisticallysignificant, justifying our approach to equalize theprogression rates of the three tests in subsequentanalyses of test agreement (see Section 5.2.6 below).
5.2.3. Simulations with randomly re-ordered data
The EOC analyses were designed to measure thestatistical strength of a trend in measurements obtainedover time. A strong trend (i.e., a highly significantcorrelation between the measurements and follow-uptime) suggests that there is true change over time ratherthan just random variability. However, some correla-tions will turn out to be statistically significant purely bychance. In order to estimate the EOC scores in theabsence of real change, we conducted simulationexperiments by repeatedly and randomly re-orderingthe original data. By definition, the random re-orderingremoves any true trend in the data, and any significantcorrelations that do arise can be regarded as due tochance. The advantage of this ‘re-sampling’ approach isthat, because real measurements are used, no assump-tions need to be made as to the variability of themeasurements or to the particular shape of theirfrequency distribution.The mean global EOC scores derived from the
simulation experiments are shown in Fig. 10. Asexpected, the simulated scores for progression andimprovement are similar. They are also similar betweenthe three techniques, which underscores the validity ofcomparing the scores of the original data between SAP,HRP, and CSLT. A comparison with Fig. 9 shows thatthe EOC scores for improvement in the original datawere slightly larger than those obtained in the simula-tions. This applied to glaucoma patients as well as tohealthy controls. For the visual fields, a plausible

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 345
explanation is that a few subjects in both groups showedgenuine improvements in the visual fields due to learningeffects, which would have increased the EOC scores of
Fig. 10. Simulated global EOC scores for progression (negative
values) and improvement (positive values) for patients (solid bars)
and controls (hollow bars) with all tests.
Fig. 11. Sectorial EOC-scores for SAP, HRP, and CSLT in glaucoma patien
the results from the original data, the lower panel the results from simulation
95%-confidence interval (shown in one direction only and truncated if large
improvement above their chance level. A similar findingwith CSLT is, however, more difficult to explain as theEOC analyses are based on objective measurements ofneuroretinal rim area. Conceivably, systematic reduc-tions in the height of the reference plane might lead toapparent increases in neuroretinal rim area measure-ments, but this explanation appears more plausible forthe glaucoma patients than for the healthy controls.
5.2.4. Sectorial visual field and optic disc changes
With both SAP and HRP, the EOC scores werelargest in the superior, followed by central and inferiorsectors, and least in the temporal sector (Fig. 11). Asimilar, though perhaps less marked, pattern wasapparent at the optic disc—the inferior, superior andtemporal sectors showed declining rim areas more oftenthan the nasal sectors. Clearly, these topographicaldifferences depend much on how the visual field and theoptic disc are examined. With the visual fields, forexample, there are considerably fewer test locations inthe central and temporal compared to the superior andinferior sectors, and the tests may therefore have less
ts (solid bars) and healthy controls (open bars). The upper panels show
s (10 iterations with randomly re-ordered data). Error bars indicate the
r than the mean).

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354346
power to detect change in the central and temporalsectors compared to the superior and inferior ones.With SAP, the largest positive EOC scores occurred in
the inferior sector of the visual field. While this mightwell be due to sampling variation, an alternativeexplanation is that there are systematic differencesbetween cross-sectional and longitudinal estimates ofvisual field ageing. The normative values underlying thepattern deviation analyses were derived from cross-sectional samples; they are not necessarily valid forlongitudinal observation. With longitudinal observa-tion, for example, subjects gain increasing experiencewith psychophysical tests, and these learning effects maycounteract any age-related losses of sensitivity. Systema-tic differences between longitudinal and cross-sectionalaging effects might therefore have contributed to thetopographical inequalities seen in our control data.
5.2.5. Relationship between visual field progression with
SAP and HRP
The relationship between the EOC scores of SAP andHRP in glaucoma patients and healthy controls is shownin Fig. 12. Points near the origin of the scatterplot arefrom patients who had shown little or no evidence ofprogression with either SAP or HRP while those locatedin the centre or towards the upper right corner of thegraph are from patients with some evidence of progres-sion with both techniques. In both groups of subjects,the relationship between the EOC scores of SAP andHRP was weak. Though the correlation was significantin the glaucoma patients (R ¼ 0:29; p ¼ 0:008), a similarrelationship in the controls did not reach statisticalsignificance (R ¼ 0:27; p ¼ 0:08).With SAP, only 2 of the 41 controls (o5%) showed
an EOC score greater than 3. With HRP, thecorresponding cut-off was an EOC score of 2 (exceededby 1 (2%) control subject). When these cut-offs wereapplied to the glaucoma group, each technique classifiedprogression in 26 patients (31%), and 14 (17%) patients
Fig. 12. Relationship between EOC (progression) scores of SAP and
HRP in glaucoma patients (left) and control subjects (right). A small
amount of random noise has been added to improve the visibility of
overlying data points.
met the criteria with both SAP and HRP. Moreconservative criteria (EOC scores X5 and 6) resultedin even poorer agreement: of 15 (18%) and 16 (19%)glaucoma patients classified as progressing with SAPand HRP, only 6 (7%) met the criteria with bothtechniques.
5.2.6. Relationship between visual field and optic disc
progression
Compared to the weak relationship between the EOCscores of SAP and HRP, the relationships between theEOC scores of either visual field test and those of theCSLT were weaker still (Figs. 13 and 14). Manyglaucoma patients had large EOC scores for theoptic disc but not the visual field, while in other patientsthe opposite was true. Only few patients showedsubstantial EOC scores for both the visual field andoptic disc.We derived three criteria to dichotomize patients
into ‘progressing’ and ‘non-progressing’ groups, basedon EOC scores that gave similar progression rates(Fig. 15). With the least conservative criterion, approxi-mately 40% (33, 33, and 31 patients) were classi-fied as having progressed with SAP, HRP, and CSLT,respectively, while the most conservative criterionclassified approximately 15% of patients as havingprogressed.Fig. 16 shows the agreement between the different
tests, visualized by area-proportional Venn diagrams. Of
Fig. 13. Relationship between SAP and CSLT EOC scores.
Fig. 14. Relationship between HRP and CSLT EOC scores.

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 347
the 60 patients who were classified as progressing with atleast one test, based on the least conservative criteria,only 6 patients met the criterion with all three tests.With the most conservative criteria, 27 patients wereclassified as progressing with at least one test, yet only 2with all three tests.
5.3. Baseline predictors of progression
This analysis was done to establish whether baselinevisual field and optic disc damage were related tosubsequent visual field and/or optic disc progression. Toinvestigate differences between groups, we stratified theglaucoma patients according to their progression statuswith both SAP and CSLT, using the intermediatecriteria described for the event analyses (Section 4.3.1)and the trend analyses with the EOC approach (Section4.3.2). We compared the MD of the baseline visual fieldas well as the rim area deviation (RAD). RAD wascomputed as the difference between the actual rim areaand the rim area expected in a healthy disc of thesame size, expressed in standard deviations from normal(Fig. 17).
Fig. 16. Area proportional Venn diagrams of the classifications with least co
analyses.
Fig. 15. Effect of criterion on progression rate with EOC analyses of
SAP, HRP, and CSLT. The approximate location of the three criteria
are shown on the ordinate (arrows).
Patients with visual field progression tended to havemore advanced disease at baseline compared to thosewho appeared to progress only with the optic disc.Although these differences were statistically significant(po0:05; Kruskall–Wallis), the large overlap betweenthe measurements suggests that baseline damage is not areliable predictor of progression with one or the othertest.
6. Case examples
To illustrate the large variability in the relationshipbetween visual field and optic disc changes found inthese studies, three case examples are presented. In thefirst (Fig. 18), there is evidence of visual field change, butthere appears to be no change in the optic disc. In thesecond example (Fig. 19), there was unequivocal concen-tric enlargement of the optic cup while the visual field atappeared stable. In the final example (Fig. 20), the visualfield and optic disc changes occurred in tandem.
7. Discussion
7.1. Visual field and optic disc changes: findings from
these studies
Assessing glaucomatous progression is one of themost important challenges that face clinicians andscientists. Important patient management decisions,such as to modify therapy, depend on good evidenceof whether the disease, as measured by visual field andoptic disc changes, is stable or progressing. Clinicalstudies comparing therapeutic modalities also requirereliable and robust measures of change.Correlating functional and structural changes in
glaucoma has both clinical and scientific importance.For example, the temporal sequence of visual field andoptic disc changes can influence the management of
nservative, intermediate, and most conservative criteria, based on EOC

ARTICLE IN PRESS
Fig. 17. Baseline MD (A, C) and Rim Area Deviation (RA; B, D) in glaucoma patients, stratified by progression according to event analyses (A, B)
and trend analyses (C, D). With each analysis, the intermediate criteria were chosen to dichotomize the patients into progressing and non-progressing
groups. The group labeled ‘none’ did not meet the criteria for progression with either SAP or CSLT. Patients in the ‘OD only’ group progressed
according to CSLT, but not with SAP, while those in the ‘VF only’ group progressed with SAP but not with CSLT.
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354348
individual patients, while determining their correlationin a group of patients in scientific studies may shed somelight on the nature of disease progression and therelative efficacy of various tests used for measuringvisual function and structural parameters in the opticdisc or retinal nerve fibre layer.Our studies show that, with both trend and event
analyses of clinical data, the relationship between visualfield and optic disc changes is remarkably poor. Thisdoes not imply that the actual relationship betweenstructural and functional change is weak. Rather, ourcurrent clinical measures of visual field and optic discchange may fail to accurately reflect the true relation-ship. Over the average follow-up period of 7 years,change manifested either predominantly in the visualfield or predominantly in the optic disc, and only fewpatients showed disc and field change to a similar extent.In fact, even between the two psychophysical tests in ourstudy (SAP and HRP), correlations over time weresurprisingly weak. This means that, in clinical practice itis unlikely that changes in the visual field can becorroborated with those observed in the optic disc, orvice versa. One important related finding with both the
trend and event analyses was that the agreementbetween visual field and optic disc progression did notappear to improve with the choice of stricter progressioncriteria. This means that a patient with definiteprogressive visual field change was no more likely toshow concurrent optic disc change than a patient withless definite visual field change, and vice versa. Evidenceof visual field progression, for example, ought not bedisregarded because no optic disc changes were notedduring the same period. Similarly, signs of optic discprogression may need to be interpreted irrespective ofwhether concurrent visual field progression was or wasnot present. The case examples 1 and 2 illustrate thispoint.With both trend and event analyses, we showed the
large variation in the progression rates obtained withdifferent criteria. It is important to realize that there isno a priori reason for selecting one such criterion overanother. The choice between different criteria involvesan essentially arbitrary balance between sensitivity andspecificity, neither of which are known or are easilydetermined. Indeed, because the rate of progression is acontinuous variable, a simple yes/no criterion is unlikely

ARTICLE IN PRESS
Fig. 18. Three sets of visual fields and optic disc images from a 6 year follow-up of the left eye of a study patient. The visual field shows both
enlargement of deepening of existing scotomas in both the superior and inferior visual field (A). Reflectivity (B) and topography (C) images from
CSLT show extensive cupping of the optic disc but no apparent change. Visual field mean deviation and optic disc rim area over the follow-up (D).
Arrows indicate time points of the illustrated examinations.
Fig. 19. Three sets of visual fields and optic disc images from a 8 year follow-up of the right eye of a study patient. The visual field appears
unchanged (A). Reflectivity (B) and topography (C) images from CSLT show a concentric enlargement over time. Visual field mean deviation and
optic disc rim area over the follow-up (D). Arrows indicate time points of the illustrated examinations.
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 349

ARTICLE IN PRESS
Fig. 20. Three sets of visual fields and optic disc images from a 7.5 year follow-up of the right eye of a study patient. The visual field shows an
unequivocal change with the development and expansion of a dense paracentral scotoma close to fixation (A). Reflectivity (B) and topography (C)
images from CSLT show a focal thinning of the superior temporal rim and development of a nerve fibre layer defect. Visual field mean deviation
(which does not adequately describe the visual field change) and optic disc rim area over the follow-up (D). Arrows indicate time points of the
illustrated examinations.
P.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354350
to convey all relevant information contained in the data.In situations where binary classifications are required(for example in the comparison of survival curvesbetween two different treatments), it may be prudentto utilize a range of criteria that bracket the largeinterval between highly sensitive and highly specificclassifications.Under the assumption that genuine improvements do
not occur (or, at any rate, occur very rarely), the eventrates for positive change (which we referred to asimprovement) may be regarded as an approximation ofa criterion’s specificity. This assumption, though, maynot be valid. With visual fields, some patients may showgenuine improvement owing to learning effects. Simi-larly, in the optic disc, tissue losses in one location maywell lead to topographical elevation in another. In fact,clusters of green superpixels are often highlighted in theTCA adjacent to areas of significant depressions in opticdisc topography. However, by treating the ‘improve-ment’ events as a proxy measure of false-positivedecisions, we are likely to underestimate (rather thanoverestimate) the true specificity of our criteria. Fromthis viewpoint, the low rate of apparent improvements(Fig. 6, Table 2) suggests that all but the leastconservative criteria yielded fairly high specificity.Simple and objective criteria for visual field and optic
disc progression are indispensable in many clinicalstudies, and further research with both empirical long-itudinal studies, studies of test–retest variability, andcomputer simulation will be needed to further developand evaluate such criteria. Equally important, however,is an understanding that any criterion may fail inindividual cases. Such criteria therefore support, ratherthan replace, considered judgments by experiencedclinicians. For example, unequivocal visual field changenear fixation may involve fewer than the three testlocations stipulated by the criteria of the Early ManifestGlaucoma Trial (Heijl et al., 2002).The EOC analyses showed that the three tests
detected similar amounts of progression. While theEOC progression scores tended to be slightly higherwith CSLT, this finding applied to both glaucomapatients and healthy controls and may be related tophysiological changes with age. With the visual fieldEOC scores, the pattern deviation calculations accountfor ageing changes, but no age correction was attemptedfor the EOC analysis performed on optic disc rim area.In addition, our choice of pattern deviation as the inputto the EOC analyses of SAP and HRP was likely to givea conservative estimate of visual field progression, asany diffuse visual field changes are neutralized in thisanalysis. It does not follow from this finding that CSLT

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 351
is, as a rule, more powerful than psychophysical tests indetecting change. The judgment of whether one techni-que is more sensitive to change than another requiresthat the specificities of the competing tests be equalized.Because, in the case of visual field and optic discprogression, there is no independent standard to judgewhether a given patient is changing or not, it is difficultto directly measure the specificity of a test forprogression.The distribution of EOC scores of the four sectors
broadly followed previous findings on visual field andoptic disc progression. With both SAP and HRP,progression occurred mostly in the superior, followedby the inferior and central sectors. This correspondedvery closely to the distribution of EOC scores for theoptic disc. Of note is the relatively large deteriorationrate in the central visual field sectors and the temporaloptic disc. With the 24-2 or 30-2 tests of the HFA, onlysix test locations are located in this functionally veryimportant area. It might be speculated that morethorough testing may have revealed an even largerdegree of change in this area.Clinicians often consider the baseline status of the
visual field or the optic disc as a possible predictor ofsubsequent progression. Many studies have suggestedthat the risk of progression increases with moreadvanced damage at baseline. Although our results withboth trend- and event-based analyses were in generalagreement with these findings (there were statisticallysignificant differences in baseline damage of visual fieldand optic disc when we arbitrarily divided our sampleinto progressing and non-progressing patients), the datahighlight the large overlap between the groups (Fig. 17).The accuracy of using baseline damage to predict therisk of future field progression in individual patients islikely to be poor. With respect to the optic disc, therewas an even greater overlap in the baseline damage (asmeasured by RAD) in progressing vs. non-progressingpatients. The generally held view that severely damageddiscs have ‘no room to progress’ may be supportable inindividual cases, but we were unable to find systematicevidence for this viewpoint—progressing and non-progressing patients had a remarkably wide range ofbaseline disc damage (Fig. 17). However, it is importantto bear in mind that our findings depend largely on thecharacteristics of our study patients who were selectedfor early to moderate visual field damage. Inclusion ofcases with more advanced visual field damage may haveresulted in different findings.
7.2. Clinical and biological measures of progression
Since the primary neuronal damage in glaucoma isloss of RGCs, the ideal study of the relationshipbetween function and structure should be at the levelof the individual RGC and its axon with, say, some form
of single cell electrophysiology or axon conduction velo-city measurements, and intracellular imaging respec-tively. Currently we have no means to conduct this typeof study in vivo. Instead, clinicians and scientists have torely on surrogate measures of functional and struc-tural loss. For visual function, they include mean sensiti-vity, mean deviation and individual pointwise sensi-tivity values using a variety of perimetric tests includingSAP as well as the newer psychophysical techniques. Forstructural measures, these include rim area, cup volumeand retinal nerve fibre layer thickness, among others,obtained with morphometric measurements from opticdisc photographs or modern imaging devices. Currentlywe have little evidence to demonstrate how well theseclinical surrogates represent neuronal integrity, butexperimental studies in monkeys tested functionallyare yielding important information in this area (Har-werth et al., 2002). It is, however, certain that there areconfounding factors in these parameters. For example,experimental studies have shown that in spite ofcomplete optic nerve transection and loss of RGCs theoptic nerve head does not undergo the type of structuralchange in the extracellular matrix that leads to optic disccupping which is the hallmark of clinical glaucoma(Morrison et al., 1990; Agapova et al., 2003). Similarly,visual field measures can be affected by many pre- andpost-retinal factors independent of RGC integrity.Our current clinical measures of function and
structure may ultimately be poor surrogates of neuronalintegrity. How accurately clinical tests represent theintegrity of RGCs probably depends on the parameterbeing measured. For example, it has recently beenargued that nerve fibre layer thickness may be a morelogical parameter to measure than an optic discparameter, such as cup depth or rim area (Schlottmannet al., 2004). On the other hand, other factors, such asfeasibility and inter- and intra-subject variability mayrender a theoretically more appropriate parameter lessuseful clinically. Similarly, psychophysical tests whichare less dependent on pre-retinal factors may provide atruer reflection of RGC activity. Unfortunately, theproof that some techniques provide more relevantinformation than others is often lacking to date andmay be difficult to establish clinically.
7.3. Methodological issues in correlating functional and
structural changes
An important reason to study the temporal relation-ship between functional and structural change inglaucoma is to determine whether one preceeds theother. In clinical study the determination of whetherstructural changes precede functional changes dependson whether a given structural change precedes a changein function that is related to the structural change. Forexample, does a progressive change in the already

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354352
damaged inferior temporal sector of the neuroretinalrim, detected 12 months prior to the detection of changein an already damaged superior nasal visual field, meanthat disc changes precede field change? An equallyplausible interpretation is that the detected optic discchange occurred after some prior visual field progressionthat had taken place before the patient was enrolled inthe study.It is also often assumed that one progressive event
with one technique is equivalent to one progressive eventwith the other. This notion is probably too simplistic.Event-based analyses are founded on statistical rules,based primarily on the variability of measurements. If atest provides low variability compared to the measure-ment range, then it is likely that more progressive eventscan be detected by this technique. Conversely, if the testhas higher variability there will be fewer detectableevents. Because the events are defined statistically, withrespect to measurement variability, they may not berelated to the same biological event in the eye.Furthermore, there is an issue of parity whereby thenumber of progressive events with one technique maynot be equivalent to the number of events with the other.For example, a statistically defined progressive changein the inferior temporal neuroretinal rim may occur atthe same time as a similarly defined change in thesuperior nasal visual field. However, if further events aredetected in the same part of the visual field during thesubsequent examinations, does this imply that the visualfield changes precede optic disc changes (since equiva-lent disc changes were not found) or that optic discchanges occur earlier (since the visual field changes weredetected after the disc change), or that that thefunctional and structural change events are related andbegin at the same time, but occur at different rates?Studying progression with parallel techniques poses
many interpretational problems, not only with respect tocomparing the tests’ efficacy in detecting progression,but also in terms of reflecting the temporal sequence ofclinically measured changes that ensue after RGC injuryin glaucoma. We suggest that while event-based analysesmay have merit when there are a limited number ofobservations, with longer follow-up and frequency ofexaminations the rate of change or its statisticalsignificance may provide more clinically useful informa-tion. In this paper we have described the EOC analysisin an attempt to standardize indices of progressionacross the different techniques. This analysis does notattempt to quantify the amount of progression, but itquantifies the strength of the evidence that change hastaken place.New techniques for detecting the presence and
progression of glaucoma, in addition to novel ideas fordata analysis, are yielding important information andenhancing the care of patients with glaucoma. There are,however, many fundamental questions about glaucoma
progression that cannot be answered by these clinicaltools. In the final analysis we have no independentqualifier of glaucoma or its progression since the class oftests that are used to measure its severity or progressionare the very ones that are used to define it. With theseconstraints, a definition of glaucoma or its progressionis accepted with the caveat that this ‘‘gold standard’’may not be optimal. Hence, when glaucomatousprogression, defined on an event-based analysis ofSAP, is used to evaluate a new psychophysical test, thelatter is by definition at a disadvantage. An independentqualifier, such as a blood test, that can definitivelyclassify progressors and non-progressors does not exist.Our work suggests that the current tools for
monitoring visual field and optic disc change providelargely independent information on progression. Be-cause we lack an independent measure of glaucomatousprogression that in itself does not rely upon a measure offunction or structure, it may be prudent to clearlydistinguish between visual field and optic disc change,rather than referring to ‘glaucomatous progression’.While both these parameters are likely to be useful, ourdata indicate that, within the scope of clinical studies,they have to be regarded as largely independentindicators of glaucomatous change.
8. Future directions
Our laboratory will continue to investigate the natureof glaucomatous progression with current as well asnewer tools for measuring function (such as frequencydoubling perimetry) and structure (such as opticalcoherence tomography and scanning laser polarimetry).Ultimately we feel that measures of progression shouldbe test-specific and that understanding the similaritiesand dissimilarities between these techniques may allowus to determine which biological aspects of progressionare best represented by them. This work will becomplemented by evidence from non-invasive functionaltesting in experimental animals in whom structurallosses can be ascertained with histological analyses.
Acknowledgements
We are grateful to our colleagues, Drs. MarceloNicolela, Raymond LeBlanc and Paul Rafuse for theirclose collaboration and discussions. Subject testing, datacollation and organization was done by Ms. TerryMcCormick and Ms. Donna Hutchison. Dr. TedGarway-Heath provided critical and constructive com-ments on the initial submission. This work wassupported by grants from the Canadian Institutes ofHealth Research (MOP-11357) to BCC and from theNova Scotia Health Research Foundation (MED-727)to PHA.

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354 353
References
Agapova, O.A., Kaufman, P.L., Lucarelli, M.J., Gabelt, B.T.,
Hernandez, M.R., 2003. Differential expression of matrix metallo-
proteinases in monkey eyes with experimental glaucoma or optic
nerve transection. Brain Res. 967 (1–2), 132–143.
Airaksinen, P.J., Tuulonen, A., Alanko, H.I., 1992. Rate and pattern
of neuroretinal rim area decrease in ocular hypertension and
glaucoma. Arch. Ophthalmol. 110 (2), 206–210.
Azuara-Blanco, A., Katz, L.J., Spaeth, G.L., Vernon, S.A., Spencer,
F., Lanzl, I.M., 2003. Clinical agreement among glaucoma experts
in the detection of glaucomatous changes of the optic disk using
simultaneous stereoscopic photographs. Am. J. Ophthalmol. 136
(5), 949–950.
Bengtsson, B., Lindgren, A., Heijl, A., Lindgren, G., Asman, P.,
Patella, M., 1997. Perimetric probability maps to separate change
caused by glaucoma from that caused by cataract. Acta.
Ophthalmol. Scand. 75 (2), 184–188.
Chauhan, B.C., 1996. Interpreting Technology. Confocal scanning
laser tomography. Can. J. Ophthalmol. 31, 152–156.
Chauhan, B.C., Drance, S.M., Douglas, G.R., 1990. The use of visual
field indices in detecting changes in the visual field in glaucoma.
Invest Ophthalmol. Vis. Sci. 31 (3), 512–520.
Chauhan, B.C., Blanchard, J.W., Hamilton, D.C., LeBlanc, R.P.,
2000. Technique for detecting serial topographic changes in the
optic disc and peripapillary retina using scanning laser tomogra-
phy. Invest. Ophthalmol. Vis. Sci. 41 (3), 775–782.
Chauhan, B.C., McCormick, T.A., Nicolela, M.T., LeBlanc, R.P.,
2001. Optic disc and visual field changes in a prospective
longitudinal study of patients with glaucoma: comparison of
scanning laser tomography with conventional perimetry and optic
disc photography. Arch. Ophthalmol. 119 (10), 1492–1499.
Chow, S., Ruskey, F., 2004. Drawing area-proportional Venn and
Euler diagrams. In: Graph Drawing: 11th International Sympo-
sium. Perugia (Italy), 2003, Springer, Heidelberg, pp. 466–477.
Collaborative Normal-Tension Glaucoma Study Group, 1998. Com-
parison of glaucomatous progression between untreated patients
with normal-tension glaucoma and patients with therapeutically
reduced intraocular pressures. Am. J. Ophthalmol. 126 (4),
487–497.
Demirel, S., Johnson, C.A., 2000. Isolation of short-wavelength
sensitive mechanisms in normal and glaucomatous visual field
regions. J. Glaucoma. 9 (1), 63–73.
Epstein, D., 2004. Primary open-angle glaucoma. In: Chandler and
Grant’s Glaucoma. Lee and Febinger, Philadelphia, pp. 183–231.
Frisen, L., 1987. A computer-graphics visual field screener using high-
pass spatial frequency resolution targets and multiple feedback
devices. Doc Ophthalmol. Proc. Ser. (49), 441–446.
Garway-Heath, D.F., Poinoosawmy, D., Fitzke, F.W., Hitchings,
R.A., 2000. Mapping the visual field to the optic disc in normal
tension glaucoma eyes. Ophthalmology 107 (10), 1809–1815.
Glasser, G.J., Winter, R.F., 1961. Critical values for the coefficient of
rank correlation for testing the hypothesis of independence.
Biometrica 48 (3/4), 444–448.
Hart Jr., W.M., Becker, B., 1982. The onset and evolu-
tion of glaucomatous visual field defects. Ophthalmology 89 (3),
268–279.
Harwerth, R.S., Crawford, M.L., Frishman, L.J., Viswanathan, S.,
Smith III, E.L., Carter-Dawson, L., 2002. Visual field defects and
neural losses from experimental glaucoma. Prog. Retin. Eye Res.
21 (1), 91–125.
Heijl, A., Lindgren, G., Olsson, J., 1987. Normal variability of static
perimetric threshold values across the central visual field. Arch.
Ophthalmol. 105 (11), 1544–1549.
Heijl, A., Leske, M.C., Bengtsson, B., Hyman, L., Bengtsson, B.,
Hussein, M., 2002. Reduction of intraocular pressure and
glaucoma progression: results from the Early Manifest Glaucoma
Trial. Arch. Ophthalmol. 120 (10), 1268–1279.
Heijl, A., Lindgren, G., Lindgren, A., 1991. Extended empirical
statistical package for evaluation of single and multiple fields in
glaucoma: Statpac2. In: Mills, R.P., Heijl, A. (Eds.), Perimetry
Update 1990/91. Kugler, New York, pp. 303–315.
Hoskins, H., Kass, M., 1989. Primary open-angle glaucoma. In:
Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas. The
C.V. Mosby Company, St. Louis, pp. 277–307.
Johnson, C.A., Samuels, S.J., 1997. Screening for glaucomatous visual
field loss with frequency-doubling perimetry. Invest. Ophthalmol.
Vis. Sci. 38 (2), 413–425.
Johnson, C.A., Adams, A., Lewis, R.A., 1989. Automated perimetry
of short-wavelength mechanisms in glaucoma and ocular hyperten-
sion. Preliminary findings. In: Heijl, A. (Ed.), Perimetry Update
1988/89. Kugler and Ghedini, Berkeley, pp. 31–37.
Junemann, A.G., Martus, P., Wisse, M., Jonas, J., 2000. Quantitative
analysis of visual field and optic disk in glaucoma: retinal nerve
fiber bundle-associated analysis. Graefes Arch. Clin. Exp. Ophthal-
mol. 238 (4), 306–314.
Kamal, D.S., Viswanathan, A.C., Garway-Heath, D.F., Hitchings,
R.A., Poinoosawmy, D., Bunce, C., 1999. Detection of optic disc
change with the Heidelberg retina tomograph before confirmed
visual field change in ocular hypertensives converting to early
glaucoma. Br. J. Ophthalmol. 83 (3), 290–294.
Mikelberg, F.S., Drance, S.M., 1984. The mode of progression of
visual field defects in glaucoma. Am. J. Ophthalmol. 98 (4),
443–445.
Mikelberg, F.S., Schulzer, M., Drance, S.M., Lau, W., 1986. The rate
of progression of scotomas in glaucoma. Am. J. Ophthalmol. 101
(1), 1–6.
Morrison, J.C., Dorman-Pease, M.E., Dunkelberger, G.R., Quigley,
H.A., 1990. Optic nerve head extracellular matrix in primary optic
atrophy and experimental glaucoma. Arch. Ophthalmol. 108 (7),
1020–1024.
Nicolela, M.T., McCormick, T.A., Drance, S.M., Ferrier, S.N.,
LeBlanc, R.P., Chauhan, B.C., 2003. Visual field and optic
disc progression in patients with different types of optic disc
damage: a longitudinal prospective study. Ophthalmology 110 (11),
2178–2184.
Pederson, J.E., Anderson, D.R., 1980. The mode of progressive disc
cupping in ocular hypertension and glaucoma. Arch. Ophthalmol.
98 (3), 490–495.
Sample, P.A., Weinreb, R.N., 1989. Color perimetry for evaluation of
primary open angle glaucoma. Noninvasive Assess. Visual Syst.
Tech. Digest Ser. 7, 32–35.
Schlottmann, P.G., De Cilla, S., Greenfield, D.S., Caprioli, J.,
Garway-Heath, D.F., 2004. Relationship between visual field
sensitivity and retinal nerve fiber layer thickness as measured by
scanning laser polarimetry. Invest. Ophthalmol. Vis. Sci. 45 (6),
1823–1829.
Spry, P.G., Johnson, C.A., 2002. Identification of progressive
glaucomatous visual field loss. Surv. Ophthalmol. 47 (2), 158–173.
Tuulonen, A., Airaksinen, P.J., 1991. Initial glaucomatous optic disk
and retinal nerve fiber layer abnormalities and their progression.
Am. J. Ophthalmol. 111 (4), 485–490.
Varma, R., Steinmann, W.C., Scott, I.U., 1992. Expert agreement in
evaluating the optic disc for glaucoma. Ophthalmology 99 (2),
215–221.
Vesti, E., Johnson, C.A., Chauhan, B.C., 2003. Comparison of
different methods for detecting glaucomatous visual field progres-
sion. Invest. Ophthalmol. Vis. Sci. 44 (9), 3873–3879.
Viswanathan, A.C., Fitzke, F.W., Hitchings, R.A., 1997. Early
detection of visual field progression in glaucoma: a comparison
of PROGRESSOR and STATPAC 2. Br. J. Ophthalmol. 81 (12),
1037–1042.

ARTICLE IN PRESSP.H. Artes, B.C. Chauhan / Progress in Retinal and Eye Research 24 (2005) 333–354354
Viswanathan, A.C., Crabb, D.P., McNaught, A.I., Westcott, M.C.,
Kamal, D., Garway-Heath, D.F., Fitzke, F.W., Hitchings, R.A.,
2003. Interobserver agreement on visual field progression in
glaucoma: a comparison of methods. Br. J. Ophthalmol. 87 (6),
726–730.
Wall, M., Chauhan, B., Frisen, L., House, P.H., Brito, C., 2004.
Visual field of high-pass resolution perimetry in normal subjects.
J. Glaucoma. 13 (1), 15–21.
Weber, J., Ulrich, H., 1991. A perimetric nerve fiber bundle map. Int.
Ophthalmol. 15 (3), 193–200.
Werner, E.B., Bishop, K.I., Koelle, J., Douglas, G.R., LeBlanc, R.P.,
Mills, R.P., Schwartz, B., Whalen, W.R., Wilensky, J.T., 1988. A
comparison of experienced clinical observers and statistical tests in
detection of progressive visual field loss in glaucoma using
automated perimetry. Arch. Ophthalmol. 106 (5), 619–623.
Zeyen, T.G., Caprioli, J., 1993. Progression of disc and field damage in
early glaucoma. Arch. Ophthalmol. 111 (1), 62–65.
Zinser, G., Wijnaendts-van-Resand, R.W., Dreher, A.W., 1989.
Confocal laser tomographic scanning of the eye. Proc. SPIE 1161
(337–344).