Embed Size (px)
Citation preview

Long Term Follow-Up after Splenectomy Performed forImmune Thrombocytopenic Purpura (ITP)
Joseph Schwartz,1 Melissa D. Leber,2 Shmuel Gillis,3 Austin Giunta,2 Amiram Eldor,1 andJames B. Bussel2*
1Department of Hematology, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel2Department of Pediatrics, New York Presbyterian Medical Center, New York, New York
3Department of Hematology, Hadassah University Hospital, Hadassah Ein-Karem, Jerusalem, Israel
Splenectomy is the only treatment of ITP known to have “curative” effects in a substantialfraction of patients. However, the true long-term outcome is uncertain and controversialbecause published series have not adjusted for the duration of follow-up. This IRB-approved retrospective study included all patients with ITP who underwent splenectomybetween 1988-1993 at three major medical centers and required a minimum postoperative5-year follow-up. Complete response (CR) was defined as all postsplenectomy plateletcounts >150 × 109/L without treatment; partial response (PR) as platelet counts ≥50 ×109/L without treatment; and failure as platelet counts <50 × 109/L or receiving therapyafter splenectomy. Seventy-five patients identified with ITP underwent splenectomy from1988 to 1993. Three patients died prior to 5-year follow-up, and 56 of the 72 patients (78%)were evaluable with follow-up for five years or longer, median 7.5 years. The immediatepostoperative complete remission rate was 77%; 57% of patients have remained in pro-longed CR. Thirty-seven patients (66%) have not required any therapy after splenectomy.Eight patients had platelet counts >150 × 109/L for 4–8.5 years before relapsing; no clearplateau was attained in the remission curve. There was no operative mortality. Ten pa-tients (18%) reported minor postoperative bleeding episodes. No life-threatening infec-tions, significant heart disease, or pulmonary hypertension developed after splenectomyin the 434 patient-years of follow-up. This study helps to define the long-term results ofsplenectomy for ITP. Am. J. Hematol. 72:94–98, 2003. © 2003 Wiley-Liss, Inc.
Key words: long-term; follow-up; splenectomy; ITP
INTRODUCTION
Immune thrombocytopenic purpura (ITP) is an auto-immune disorder characterized by accelerated plateletdestruction. Antiplatelet autoantibodies bind to platelets,causing phagocytosis by the mononuclear phagocyte sys-tem [1,2]. The approximate incidence is 5–10 per100,000 persons per year [3]. In affected adults, splenec-tomy has been considered to be a second-line therapy forITP in patients who either fail to respond to initial cor-ticosteroids or require continuous treatment to maintain asafe platelet count [2,4,5].
The beneficial effects of splenectomy in successfulcases are removal of the sites of antibody-coated plateletdestruction and/or antiplatelet antibody production [6,7].This duality has made prediction of who will respond tosplenectomy difficult. Attempts to identify factors thatwould predict the success of splenectomy have led toconflicting results among published reports [8–17].
Reported response rates to splenectomy have variedfrom 50% to 80% [2,8–13]. However, the true long-termoutcome response rate is not known because follow-up inmost studies has been relatively short [10,12–14]. Evenin the studies with longer median follow-up, i.e., up to5–7 years, patients with short follow-up (3 months to 1year) were included [9,11,15–17] and could not be dis-tinguished from those with longer follow-up.
*Correspondence to: James B. Bussel, M.D., New York PresbyterianHospital, Weill Medical College, Department of Pediatrics, 525 East68th Street, Room P-695, New York, NY 10021.E-mail: [email protected]
Received for publication 16 May 2002; Accepted 15 October 2002
Published online in Wiley InterScience (www.interscience.wiley.com). DOI:10.1002/ajh.10253
American Journal of Hematology 72:94–98 (2003)
© Wiley-Liss, Inc.

There is also very little information describing latecomplications of splenectomy for ITP other than sepsis.However, in patients with hereditary spherocytosis, therehas been speculation that there might be an acceleratedoccurrence of atherosclerotic events and development ofpulmonary hypertension years after splenectomy [18,19].The purpose of this study was to evaluate the long-termoutcome of splenectomy, defining “long-term” as a mini-mum follow up of 5 years in adults with ITP.
PATIENTS AND METHODS
The study included retrospective analysis of all 75cases of adults with ITP that underwent splenectomybetween 1988 and 1993 in three major medical centers:Cornell University Medical Center in New York; Had-assah Ein-Karem University Hospital in Jerusalem; andThe Tel-Aviv Sourasky Medical Center, Israel. Patientswere identified via ICD9 and CPT coding. ITP was de-fined according to the guidelines of the American Soci-ety of Hematology [4]. Splenectomy was generally per-formed when patients did not respond to medical therapy.This study protocol was IRB approved and followed ateach of the participating medical centers. Medical rec-ords of all patients and their follow-up were sought. Re-peated attempts were made to contact all patients viatheir primary physicians and then directly. Medical in-formation and blood counts were obtained from the pa-tients themselves, their physicians, and/or review of theirhospital and outpatient clinic charts. Information re-ceived from patients was double checked with medicalrecords, i.e., laboratory reports, physician documenta-tion, or hospital charts.
Criteria for response were defined as follows: com-plete response (CR), all post-splenectomy platelet counts>150 × 109/L without ever receiving treatment after sple-nectomy; partial response (PR), all other patients withplatelet counts >50 × 109/L without therapy after sple-nectomy; failure, platelet counts <50 × 109/L or patientswho received therapy after splenectomy.
Data Analysis
Statistical analysis was carried out with the Stat-View4.5 and Prism 3.0 software. Differences were evaluatedby the chi-square test. A two-tailed P value of 0.05 orless was considered as statistically significant. Kaplan–Meier analysis was used to estimate remission rates. Pa-tients relapsing between 2 years, i.e., between 4 and 5years from surgery, were assigned a relapse time of 4.5years.
RESULTS
Seventy-five patients with ITP were identified whounderwent splenectomy between 1988 and 1993 at the
three medical centers. Sixteen patients (21%) were lost to5-year follow-up. Three patients died: two due to malig-nancy (both approximately 36 months after splenectomy)and one due to pre-existing ischemic heart disease (48months after surgery). This left 56 of the 75 patients(75%) who had data available for minimum of 5 yearsafter splenectomy. These 56 patients comprised the studygroup (Table I), and they were followed up to 10.5 yearspostoperatively with a median of 7.5 years. There were434 years of patient follow-up after splenectomy in the56 patients in the study.
In addition to ITP, the medical history of a small num-ber of patients included thyroid disease, connective tissuedisease, cancer, and cardiovascular disease (Table I). Themedian age of the patients at the time of splenectomy was37 years (range, 15–81). Forty-five of the 56 patients(80%) were women. The median interval from diagnosisto splenectomy was 12 months with a range of 0.5–233months (Table I). Forty-one of the 56 patients (73%) hadplatelet counts between 0 and 20 × 109/L prior to surgery,and the median nadir platelet count prior to surgery was14.5 × 109/L.
All patients received steroids as initial therapy for ITP.Twenty-seven patients received only steroids prior tosplenectomy, while 29 patients received additional medi-cations including immunoglobulins (IVIG) [19 patients],vincristine [10], danazol [8], anti-D [3], cytoxan [2], andimuran [1]. All patients received pneumoccocal vaccineprior to the surgery.
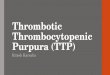
The probability of staying in clinical remission(CR+PR) after splenectomy is shown by Kaplan–Meieranalysis in Figure 1: 73% of the patients were still inclinical remission 5 years post splenectomy, and 62%were in remission 10 years postoperatively.
These data are divided into CR, PR, and failure inTable II.
Complete Remission (CR) Group
Forty-three of the 56 patients (77%) achieved a com-plete remission immediately after splenectomy. Thirty-two patients (57% of the total) remained in a prolongedcomplete remission with a persistently normal plateletcount, never having received any postsplenectomy treat-
TABLE I. Characteristics of Evaluable Patients
Number of patients 56Sex (F/M) 45/11Median age (years) 37 (15–81)Median time from diagnosis to splenectomy (months) 12 (0.5–233)Median follow-up (years) 7.5 (5–10.5)Median platelet counts before splenectomy (109/L) 14.5 (2–90)Other medical conditions presplenectomy
Thyroid disease 5Connective tissue disease 3History of malignancy 2Arteriosclerotic disease 3
Long-Term Follow-Up Splenectomy for ITP 95

ment. Eleven patients, 20% of the total and 25% of thecomplete responders to surgery, relapsed after an initialcomplete response.
Partial Remission (PR) Group
Five (9%) patients achieved a partial remission (PR).All have remained in PR throughout the long-term fol-low-up maintaining platelet count >50 × 109/L.
Failure Group
Nineteen patients (34%) failed splenectomy. In eightpatients (14.3%), there was no response to the operation.The other 11 patients initially had a complete response(normal platelet count) and subsequently relapsed. Threepatients failed in the first 2 years, two patients relapsedafter 4–5 years, three patients after 5–6 years, and threepatients between 6 and 8.5 years after splenectomy(Fig. 1).
All 19 patients in the failure group received predni-sone after splenectomy, 11 received IVIG, 5 receivedvincristine, 3 received danazol, 3 received Cytoxan, and1 received imuran. The eight primary failure patients,who did not have any response to the splenectomy, werealso refractory to medical therapy after splenectomy. Ofthe 11 patients with late failure, 5 responded to steroids.
There were six cases (11%) in which accessory spleens
were identified and removed. One was in a primary fail-ure patient, and five were in patients with late failure; ofthese five patients. Those five patients relapsed 1, 4, 5,and 8 years after splenectomy. The platelet count rosefollowing the removal of the accessory spleens only inthe two patients who had normal platelet counts for >4years after initial splenectomy before relapse.
Young age at splenectomy, defined as �37 years,which was the median age, had a trend toward a positiveoutcome for splenectomy (P � 0.07). A good responseto splenectomy was not related to the time between di-agnosis and splenectomy or to patient gender (Table III).When the failure group patients were subdivided intothose who failed to respond immediately and those whoresponded initially and later relapsed, none of these vari-ables was predictive in either subgroup.
There were no perioperative deaths. Six patients (10%)experienced transient postoperative complications, in-cluding infections, subphrenic abscesses, and minorwound hematomas. Hemorrhagic symptoms consisted ofecchymoses and petechiae were noted in 10 patients(18%) in the follow-up period, all but one of which werein the failure group. There were no major or internalhemorrhages. There were no cases of overwhelming postsplenectomy infections (OPSI). Two patients sufferedfrom chronic sinusitis after the surgery. One patient un-responsive to surgery was found to have a positive anti-nuclear factor antibody post-operatively, but none devel-oped SLE. Of three patients with ITP in association withconnective tissue disease, two failed to respond to sple-nectomy and one had a PR. The five patients with ITPwho had thyroid disease and underwent splenectomy had2 CR, 1 PR, and 2 failures. Two patients developed ce-rebrovascular accidents (CVA) after surgery. One was 66years old at the time of splenectomy and had diabetesmellitus and hyperlipidemia. She was in CR for 4 years,relapsed, and shortly afterward had a CVA. The otherhad had a history of Hodgkin’s disease at age 36. Shereceived chemotherapy and radiation and achieved last-
TABLE III. Outcome After Splenectomy: Influence of Age,Duration of ITP, and Sex
Parameter
Response to splenectomy
CR + PR Failure
Age at splenectomy (years)>37 (n � 29) 16 13�37 (n � 27) 21 6
�2 3.187; P � 0.074Diagnosis–splenectomy interval (months)
>12 (n � 28) 20 8�12 (n � 28) 17 11
�2 0.717; P � 0.397Sex
Female (n � 45) 28 17Male (n � 11) 9 2
�2 1.514; P � 0.218Fig. 1. Kaplan–Meier curve of remission rate (CR+PR) in 56adults with ITP following splenectomy.
TABLE II. Response to Splenectomy
Immediatepost-operative
Long-termfollow-up
Therapypost-operative
No therapypost-operative
Completeremission
43 (77%) 32 (57%) — 32 (57%)
Partialremission
5 (9%) 5 (9%) — 5 (9%)
Failure 8 (14%) 19 (34%) 19 (34%) —Total 56 56 19 (34%) 37 (66%)
96 Schwartz et al.

ing remission from her Hodgkin’s lymphoma. She un-derwent splenectomy for ITP at age 42 with primaryfailure and developed a CVA 3 years after the surgerywhile maintaining normal platelet counts on steroidtherapy. No significant heart disease or pulmonary hy-pertension developed after the surgery in any of the pa-tients. One patient with coronary artery disease pre-existing splenectomy died 4 years after surgery.
DISCUSSION
Since first introduced more than 50 years ago by Kaz-nelson [20], splenectomy continues to be the only “cu-rative” treatment for patients with ITP. The immediatepostoperative response is in approximately 80–85% ofpatients [2,11,13,14]. The long-term response rate is lesswell defined and has been variably estimated to be in therange of 50–80% [8–16]. While there are more than 40reports of the long-term outcome of splenectomy, onlyfive reports [9,11,15–17] had a median follow-up >5years. Moreover, all five included patients whose follow-up was as short as 6–12 months; none analyzed the re-sponse to splenectomy as a function of time from sur-gery, and none provided individual patient data.Therefore, the true long-term response rate to splenec-tomy remains unknown.
The aim of this study was to evaluate the long-termoutcome of splenectomy, arbitrarily requiring a mini-mum follow-up of 5 years. At one center (NYPH) codingfor splenectomy in the medical record was only availablebeginning in 1988 so that only patients who underwentsplenectomy from 1988 to 1993 were included. This re-sulted in the number of patients available for accrualbeing 75. Only five of the more than 40 published reportsincluded more splenectomized patients [10–14].
Encompassing 56 patients, all of whose follow-up was�5 years (median 7.5 years, range 5–10.5 years), 77% ofthe patients responded immediately after the surgery;66% of patients achieved a long-term satisfactory re-sponse, complete or partial, during the study period notreceiving any therapy and always maintaining a plateletcount �50 × 109/L. The Kaplan–Meier probability esti-mates were similar with a 73% stable remission (plateletcount always >50 × 109/L, never any need for treatment)at 5 years and 62% at 10 years after surgery. Eight pa-tients (14%) relapsed 4–8.5 years after the operation. TheKaplan–Meier analysis (Fig. 1) indicates that as timefrom splenectomy increases, the success rate for an ex-cellent response steadily decreases. It is not clear if aplateau was achieved, suggesting a reduction in the rateof relapses.
Despite those late relapses, our study shows long-termsustained remission in 66% of cases, none of whom re-quired any additional treatment. This is a far better out-come than any other treatment modality of ITP. High-
dose dexamethasone showed limited and transientresponse [21], dapsone has been used successfully in40–50% of patients [22], danazol is beneficial in 20–40%of patients [23], and vinca alkaloids showed even lowertransient response rate [24]. None induced an unmain-tained CR in more than 10% of cases.
One limitation for data interpretation arising from thefact that 16 patients (21%) were lost to follow-up prior to5 years. Although those 16 patients’ outcome may limitthe overall data interpretation, taking into account widerange of outcomes in the missing patients would notsubstantially change the results reported here. For ex-ample, if 13 of the 16 missing patients had a remission,this would result in a 70% sustained response ratewhereas if only 5 of the 16 achieved a lasting remission,this would only lower the overall long-term response ratefrom 66% to 58%. Hence, the long-term response rate at5–10 years postoperative after splenectomy is 60–70%.
The incidence of an accessory spleen in relapsed pa-tients is 9–22% [9,11,25], as it was in this series (11%).After accessory splenectomy, two patients out of sixwent into complete remission. As was noted by others[2,26–28] response to accessory splenectomy was onlyseen in those patients who relapsed �4 years after initialsplenectomy.
Many studies have attempted to identify prognosticfactors for response to splenectomy in patients with ITPwithout consistent findings among the published reports.In our series, we evaluated the age at splenectomy, timefrom diagnosis to splenectomy, and sex of the patients.Although none of these factors had a significant associa-tion with outcome, there was tendency for younger age tobe a positive predictive factor (P � 0.07), as was re-cently shown by two other reports [29,30]. In our study,due to the long interval between splenectomy and assess-ment of outcome, the specific details of the preoperativeresponse to steroids or other medical therapy (IVIG)were often unavailable.
Splenectomy caused no surgical mortality or signifi-cant morbidity. There was a 10% postoperative morbid-ity, which included mostly hematoma and infection ofthe surgical incision, as was seen in other series [8,14].Our series, which included 434 patient-years post-sple-nectomy, had no cases of overwhelming post-splenec-tomy infection (OPSI).
An increased incidence of atherosclerotic events in-cluding heart disease, CVA, and pulmonary hypertensionhave been described after splenectomy, which may bedue to abnormal erythrocytes may remaining longer inthe circulatory system, initiating platelet activation[18,19,31,32], as well as post-splenectomy thrombocyto-sis. Recently, Ahn et al. [33] suggested that there was anincreased risk of dementia caused by microinfarcts insubsets of ITP patients, especially if potentiated by a risein the platelet count after splenectomy. Such mechanisms
Long-Term Follow-Up Splenectomy for ITP 97

may be aggravated in the presence of pre-existing coro-nary heart disease or hemolytic disorders [18,32]. Thelow incidence of heart disease in the series reported hereis mitigated by both the inclusion of only two males overthe age of 50 and the absence of hemolytic disorders. Ourseries had only 3 patients who developed thromboticevents (1 cardiac and 2 CVA). The possibility of anincreased risk of long-term thrombotic complications inpatients with ITP requires further evaluation.
In conclusion, splenectomy generally appears to besafe and effective for the treatment of ITP. Prediction ofoutcome is difficult in individual cases but the immediateresponse rate was 77%, with 57% of patients staying inprolonged CR and 66% in CR+PR at a median of 7.5years postoperatively. The information developed herewill allow a more informed decision about the risks andbenefits of splenectomy in patients with ITP.
REFERENCES
1. Bussel JB, Cines D. Immune thrombocytopenic purpura, neonatal al-loimmune thrombocytopenia and post-transfusion purpura. In: Hoff-man R, Benz EJ, Shattil S, Furie B, Cohen HJ, Silverstein LE, Mc-Glave P, editors. Hematology: basic principles and practice. NewYork: Churchill Livingstone; 2000. p 2096–2114.
2. Berchtold P, Mcmillan R. Therapy of chronic idiopathic thrombocy-topenic purpura in adults. Blood 1989;74:2309–2317.
3. Fredriksen H, Schmidt K. The incidence of idiopathic thrombocyto-penic purpura in adults increases with age. Blood 1999;3:909–913.
4. George JN, Woolf SH, Raskov GE, Wasser JS, Aledort LM, BallemPJ, Blanchette VS, Bussel JB, Cines DB, Kelton JG, Lichtin AE,McMillan R, Okerbloom JA, Regan DH, Warrier I. Idiopathic throm-bocytopenic purpura: a practice guideline developed by the explicit meth-ods for the American Society of Hematology. Blood 1996;88:3–40.
5. Portielje JE, Westendorp RG, Kluin-Nelemans HC, Brands A. Mor-bidity and mortality in adults with idiopathic thrombocytopenic pur-pura. Blood 2001;97(9):2549–2554.
6. Karpatkin S, Stick N, Siskind GW. Detection of splenic antiplateletantibody in idiopathic thrombocytopenic purpura. Br J Haematol 1972;23:166–176.
7. Siegel RS, Rae JL, Barth S, Coleman RE, Reba RC, Kurlander R,Rosse WF. Platelet survival and turnover: important factors in predict-ing response to splenectomy in immune thrombocytopenic purpura.Am J Hematol 1989;30:206–212.
8. Shaw JHF, Clark MA. Splenectomy for immune thrombocytopenicpurpura: Auckland experience 1979–87. Austr N Z J Surg 1990;59:123–126.
9. Naouri A, Feghali B, Chabal J, Boulez J, Dechavanne M, Viala JJ,Tissot E. Results of splenectomy for idiopathic thrombocytopenic pur-pura. Acta Haematol 1993;89:200–203.
10. Akwari OE, Itani KMF, Coleman RE, Rosse WF. Splenectomy forprimary and recurrent immune thrombocytopenic purpura. Ann Surg1987;206:529–541.
11. Mazzucconi MG, Arista MC, Peraino M, Chistolini A, Felici C, Fran-cavilla V, Macale E, Conti L, Gandolfo GM. Long-term follow-up ofautoimmune thrombocytopenic purpura (ATP) patients submitted tosplenectomy. Eur J Haematol 1999;62:219–222.
12. Pizzuto J, Ambriz R. Therapeutic experience on 934 adults with idio-pathic thrombocytopenic purpura: multicenter trial of the CooperativeLatin American Group on Hemostasis and Thrombosis. Blood 1984;64:1179–1183.
13. Fenaux P, Caulier MT, Hirshauer MC, Beuscart R, Goudemend J,Bauterrs F. Reevaluation of the prognostic factors for splenectomy inchronic idiopathic thrombocytopenic purpura: a report on 181 cases.Eur J Haematol 1989;42:259–264.
14. Stasi R, Stipa E, Masi M, Cecconi M, Scimo MT, Oliva F, Sciarra A,Perrotti AP, Adomo G, Amadori S, et al. Long-term observation of 208adults with chronic idiopathic thrombocytopenic purpura. Am J Med1995;98:436–442.
15. Jiji RM, Firozvi T, Spurling CL. Chronic idiopathic thrombocytopenicpurpura—treatment with steroids and splenectomy. Arch Intern Med1973;132:380–383.
16. Thompson RC, Moore RA, Hess CE, Wheby MS, Leavell BS. Idio-pathic thrombocytopenic purpura: long-term results of treatment andthe prognostic significance response to corticosteroids. Arch InternMed 1972;130:730–737.
17. Den Ottolander GJ, Grataama JW, De Koning J, Brand A. Long-Termfollow-up study of 168 patients with immune thrombocytopenic pur-pura. Scand J Hematol 1984;32:101–110.
18. Schilling RF. Spherocytosis, splenectomy, strokes and heart attacks.Lancet 1997;350:1677–1678.
19. Hoeper MM, Niedermeyer J, Hoffmeyer F, Flemming P, Fable H.Pulmonary hypertension after splenectomy? Ann Intern Med 1999;130:506–509.
20. Kaznelson P. Verschwinden der hemorrhagischen Diathese bie einemFalle von “essentieller Thrombopenie” nach Milzexstirpation: splenogenethrombolytische purpura. Wien Klin Wochenschr 1916;29:1451–1554.
21. Stasi R, Brunetti M, Pagano A, Stipa E, Masi M, Amadori S. Pulsedintravenous high-dose dexamethasone in adults with chronic idiopathicthrombocytopenic purpura. Blood Cells Mol Dis 2000;26:582–586.
22. Godeau B, Durand JM, Roudot-Thoraval F, Tenneze A, OksenhendlerE, Kaplanski G, Schaeffer A, Bierling P. Dapsone for chronic auto-immune thrombocytopenic purpura: a report of 66 cases. Br J Hae-matol 1997;97:336–339.
23. Ahn YS, Rocha R, Mylvaganam R, Garcia R, Duncan R, HarringtonWJ. Long-term danazol therapy in autoimmune thrombocytopenia:unmaintained remission and age-dependent response in women. AnnIntern Med 1989;111:723–729.
24. Facon T, Caulier Mt, Wattle E, Jouet JP, Bauters F, Fenaux P. Arandomized trial comparing vinblastine in slow infusion and by bolusi.v. injection in idiopathic thrombocytopenic purpura: a report on 42patients. Br J Haematol 1994;86:678–680.
25. Szold A, Schwartz J, Abu-Abeid S, Bulvik S, Eldor A. Laparoscopicsplenectomies for idiopathic thrombocytopenic purpura. Am J Hema-tol 2000;63:7–10.
26. Wallace D, Fromm D, Thomas D. Accessory splenectomy for idio-pathic thrombocytopenic purpura. Surgery 1982;91:134–136.
27. Ambriz R, Munos R, Quintanar E, Sigler L, Aviles A, Pizzuto J.Accessory spleen compromising response to splenectomy for idio-pathic thrombocytopenic purpura. Radiology 1985;155:793–796.
28. Verrheyden CN, Beart RW, Clifton MD, Phyliky RL. Accessory sple-nectomy in the management of recurrent idiopathic thrombocytopenicpurpura. Mayo Clinic Proc 1978;53:442–446.
29. Fabris F, Tassan T, Ramon R, Carraro G, Randi ML, Luzzatto G,Moschino P, Girolami A. Age as the major predictive factor of long-term response to splenectomy in immune thrombocytopenic purpura.Br J Haematol 2001;112(3):637–640.
30. Kathouda N, Grant SW, Mavor E, Friedlander MH, Lord RV, Achanta K,Essanti R, Mason R. Predictors of response after laparoscopic splenectomyfor immune thrombocytopenic purpura. Surg Endosc 2001;15:484–488.
31. Schilling RF. Estimating the risk for sepsis after splenectomy in he-reditary spherocytosis. Ann Intern Med 1995;122:187–188.
32. Robinette CD, Fraumeni JF. Splenectomy and subsequent mortality inveterans of the 1939–45 war. Lancet 1977;2:127–129.
33. Ahn YS, Horstman LL, Jy W, Jimenez JJ, Cui Y, Escobar MA, BowenB. Vascular dementia among patients with ITP and risk factors [ab-stract]. Blood 2000;196(11):250a.
98 Schwartz et al.