Embed Size (px)
Citation preview

Ultrasound in the assessment of complications of labour
University of Bologna,
Italy
Lodi, 15 Maggio 2010

Outline
Role of ultrasound with:
• Abnormal intrapartum CTG
• Obstructed labour
• Third stage or postpartum disorders

Ultrasound and abnormal CTG
•Abnormal CTG trace is exceedingly frequent during labour
•In few of these cases fetal acidemia is asscociated and expedite delivery is warranted
•US may assist clinician in interpreting abnormal CTG and predicting the risk of fetal hypoxia

Ultrasound and abnormal CTG
Cord compression
Nuchal cord 30% of deliveries
Variable decelerations are common
Risk of asphyxia usually not increased
Doppler Ultrasound are accurate in detecting ≥1 cord circles

Ultrasound and abnormal CTG
Occiput posterior
5-10% of deliveries
Early decelerations are common due to ocular compression (vagal reflex)
Ultrasound are more accurate than digital examination in detecting OP
Orbits

Ultrasound and abnormal CTG
In abnormal CTG due to suspected hypoxia
•Evaluate fetal adaptation/ response to hypoxia and predict the risk of neonatal acidemia
•Document fetal position and station prior to extraction

Doppler Ultrasound and labour hypoxia
Siristatidis C et al, Arch Ob Gyn 2004
Doppler in 70 women in labour monitored with continuous CTG and pulse oximetry;
•Group 1(n=30): normal CTG and O2>40%
•Group 2 (n=40): abnorm CTG and O2 30-40%
•Group 3 (n=20): abnorm CTG and O2<30%
Acidemia significantly more frequent in group C (0/30 vs 1/40 vs 5/20)

Doppler Ultrasound and labour hypoxia
Siristatidis C et al, Arch Ob Gyn 2004
•Group 2 (abnorm CTG and O2 30-40%)
•<PI MCA and >PI umb during vs after contraction
(C/P ratio <1 for O2<37%)
•Group 3 (n=20): abnorm CTG and O2<30%
•<PI MCA and >PI umb during vs after contraction
•>PI MCA and <PI umb after 2 min of O2<30%
After prolonged hypoxia, the brain-sparing effect fails (C/P ratio from < to >1)

Doppler Ultrasound and labour hypoxia
Ghosh et al, Ultras Obst Gyn 2009
Umbilical vein assessment in 52 cases
Double blind design
•26 with abnormal CTG
•8 UV pulsations (6/8 oper deliv for distress)
•18 no UV pulsations (no oper deliv)
•26 with normal CTG
•UV pulsations and oper deliv for distress in none

Ultrasound and abnormal CTG
In abnormal CTG due to suspected hypoxia
•evaluate fetal adaptation/ response to hypoxia and predict the risk of neonatal acidemia
•Document fetal position and station prior to extraction

Ultrasound and abnormal CTG
•Clinical evaluation of fetal head station and position in stage 2 of labour requires much expertise and is highly subjective
•Critical findings to decide how to expedite delivery when indicated
•Ultrasound in labour may assist obstetrician in this task

Intracranial hemorrage in singleton term fetuses and mode of delivery
California database of 583,340 nulliparous singletons deliveries 2500-4000 grms: NEJM341:1709, 1999
incidence OR
Vaginal delivery 1:1900 1,0
Elective CS 1:2750 0,7
CS in labour 1:954 2,0
Vacuum 1:860 2,7
Forceps 1:664 3,4
Failed trial of vacuum/forceps 1:334 5,7

Cranial trauma and intra-partum deaths: Confidential enquiry
BJOG (2005) 112, 619–626
• 37/709 (5%) of intrapartum deaths had cranial injury as a dominant feature
• Sequential instruments in 24 (64%)
• CS after failure of instrumental vaginal delivery in 11 (30%)

Birth simulator: Reliability of transvaginal assessment of fetal head station as defined by the ACOG classification
Dupuis et al: AJOG:(2005) 192, 868–74

Birth simulator:Reliability of clinical assessment
Dupuis et al: AJOG:(2005) 192, 868–74
Residents Attendings
Total errors 32% 25%
High mistaken for low-outlet
22.4% 15.9%
Mid-low mistaken for high
16% 16%

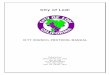
Translabial (infrapubic) ultrasound:
the sagittal viewcaputPubic
symphysis
Fetal skull
Posterior pelvic walls not imaged

Progression angleBarbera: ACOG DVD, 2003

Angle of progression:Kalache et al, UOG March 2009
Inverse probability of successful vacuum or
vagin delivery
•41 pts, stage II, failure to progress
•15 cases with occiput posterior excluded

Head directionHenrich: UOG 2006; 28: 753–760

Progression in the longitudinal plane
<90° 90° >90°
Infrapubic line

p <
.0001
Correlation between sonography of fetal head direction
and digital examinations(Ghi et al: Ultrasound Obstet Gynecol 2009; 33: 331–336)

Head direction and vacuum Henrich et al: Ultrasound Obstet Gynecol 2006; 28: 753–760
Ghi et al: Ultrasound Obstet Gynecol 2009; 33: 331–336
Direction1-3
tractions4
tractions Failure
Up (n=18) 18 0 0
Horizontal-down (n=14)
6 7 1

midline
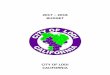
Translabial ultrasound:
the axial view

Correlation between sonography of fetal head rotation and digital examinations (occiput
anterior only)
< 45°
> 45°
Not seen
p <
.0001

Predicting the success of operative vaginal delivery
< 90°
Difficult
(< +2 cms)
Easy
(> +3 cms)
> 90°
longitudinalTransverse
(if occiput anterior)
Easy
(> + 3cms)
< 45°
midline

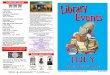
Caveat:the posterior occiput
orbits
LOP

Head direction difficult to
assess
Rotation < 45° frequently seen with high station
Translabial ultrasound in occiput posterior

Outline
Role of ultrasound with:
• Abnormal intrapartum CTG
• Obstructed labour
• Third stage or postpartum disorders

Ultrasound and obstructed labour
Confirming clinical diagnosis of obstructed labour
Demonstrating head malposition as a possible cause
Assisting the physician in the choice between operative vaginal delivery and CS

1.Confirming diagnosis of obstructed labour
Clinical vs sonographic diagnosis
Cervical dilatation
Head station

Persistent posterior occiput
2.Demostrating head malposition in obstructed labour

Frequency of posterior occiputPonkey et al: Obstet Gynecol 2003;101:915
%
Overall 5,5
Para 0 7,2
Para 1+ 4,0
p<.001

Probability of spontaneous vaginal delivery with persistent
occiput posterior
AuthorPara 0 (%)
Para 1+ (%)
Floberg et al, 1987 27 -
Fitzpatrick et al, 2001 29 55
Ponkey et al, 2003 26 57

Posterior occiput:maternal morbidity
Ponkey et al: Obstet Gynecol 2003;101:915
Variable OA OP p
3-4th degree tear 6.7 18.2 <.001
Excessive blood loss* 9.9 13.6 <.001
Post-partum infection 0.8 2.2 <.001
Fever 1.1 4.7 <.001
* > 500 ml vaginal delivery, > 1000 ml CS

Posterior occiput: fetal morbidityCheng et al: Obstet Gynecol 2006;107:837–44
OA OP OR (IC 95%)
Apgar 5’ < 7 1.9 3.8 1.50(1.17-1.91)
Acidemia 0.5 1.8 2.92 (1.84-4.62)
Meconium 22.7 32.3 1.29 (1.17-1.42)
Fetal trauma 0.8 1.4 1.77 (1.22-2.57)
NICU 3.1 5.6 1.57 (1.28-1.92)
Neonatal morbidity 6.0 10.7 1.45 (1.24-1.65)

Encephalopathy in term infantsBadawi: BMJ 1998; 317:1154
Variable OR IC 95%
Sentinel event 4,44 1,30-15,22
Posterior occiput 4,29 1,74-10,54
Operative delivery 2,34 1,16-4,70
Emergency CS 2,17 1,01-4,64
Elective CS 0,17 0,05-0,56

Errors in the clinical prediction of occiput prior to oper delivery
Akmal et al: Ultrasound Obstet Gynecol 2003; 21: 437–440
% error
Overall 26.6
Anterior occiput 17%
Lateral or posterior occiput 46%

Frequency of occiput posteriorAkmal et al: Ultrasound Obstet Gynecol 2004; 24: 425
Cervical dilatation OP (%)
3-5 cm 33%
6-9 34%
10 cm 19%
Delivery 7%

Probability of persistent occiput posterior at delivery
Akmal et al: Ultrasound Obstet Gynecol 2004; 24: 425
21
32
44
0
10
20
30
40
50
60
70
80
90
100
3-5 cm 5-9 cm 10 cm

Prediction of persistent occiput posterior at deliveryBlasi et al, Ultrasound Obstet Gynecol
spine
23/84 OPStage 1 and 2
anterior spine (n=16)
OP at delivery =0/16
posterior spine (n=7)
OP at delivery =6/7

Outline
Role of ultrasound with:
• Abnormal intrapartum CTG
• Obstructed labour
• Third stage or postpartum disorders

SecondamentoUltrasound and 3rd stage

Normal Placental “separation”
•Multiphasic>monophasic
•Down-up 90% of cases
•Blood flow cessation between basal placenta and myometrium soon after delivery of the fetus

US and abnormal 3rd stage Krapp et al, Ultras Obst Gyn 2000
•57 physiologic separation
•Cessation of blood flow uterus-placenta after fetus delivery
•5 manual or instrumental removal of placenta (4 accreta)
•Persistence of blood flow in 4 cases of accreta

Ultrasound and postpartum disorders
In cases of haemorrhage
•Diagnosis of retained tissue and placenta
•Correct placement of balloon for uterine atony

Ultrasound and postpartum disorders
correct X incorrect

…thank you!!