Embed Size (px)
Citation preview

LMNL VS. UMNL
DAYNA RYAN, PT, DPTWINTER 2012

GENERAL TERMINOLOGY
PNS: motor units and associated sensory connections
• Includes cranial nerves
CNS: brain and spinal cord
Sign = an objective finding revealed upon physical examination
Symptom = (subjective) functional components of a disease perceived by a patient and expressed in a patient’s history

• Peripheral nerve conditions• Bell’s Palsy• Guillain-Barre• Charcot-Marie-Tooth Disease• Polio and post-polio syndrome• Diabetic polyneuropathy• Alcoholic polyneuropathy• Hansen’s Disease (leprosy)
• Mixed peripheral nerve / spinal cord conditions
• Myotrophic lateral sclerosis (ALS)• Tabes dorsalis

LOWER MOTOR NEURON LESIONS
Most common signs/symptoms: pain and weakness
Muscle weakness
• Paralysis (plegia) = total or severe loss of voluntary contraction
• Paresis = mild or partial loss of voluntary contraction characteristic of LMNLs
Atrophy – common feature of many neuromuscular disorders
-if you don’t use it u lose it.
Hypertrophy
• Compensatory activation of synergistic muscles to support weakened muscles may result in “compensatory hypertrophy)
• Causes muscle imbalance, and can lead to pain.

MUSCLE HYPERACTIVITY
Fasciculations = rapid, fine, painless contraction of groups of muscle fibers
• Visible but not strong enough to move limbs• Commonly seen in anterior horn cell disorders=motor cells
(e.g. ALS)
Cramps = painful muscle spasms
• When violent, referred to as convulsions • Clonic: alternating contraction and relaxation• Tonic: sustained contraction=charley horses• Also associated with anterior horn cell disorders

TETANY
= involuntary muscle twitching, spams, or cramps occurring as a result of a hyperexcitable peripheral nerve
**can also occur in CNS disorders
• Fibrillation: small, asynchronous contractions occurring in a single skeletal muscle fiber
• Too small to see (need an EMG to detect)• Present following denervation and with some myopathies
• Myotonia: delayed capacity for relaxation in skeletal muscle (tone disorder)
• Contracture: tightness or restricted ROM across a joint (common for Parkinson's, due to basal ganglia)

LMNL CHARACTERISTICS
Muscle Fatigability (myasthenia)
• Decreased muscle endurance because cannot recruit because of lack of innervation
Hypotonia: decreased muscle tone
• Increased risk of subluxation (shoulders, scoliosis)
Abnormal Sensation
• Often an early presenting sign of PNS dysfunction• Paresthesias = tingling or “pins and needles” sensations
Decreased or absent DTRs
• Due to disrupted reflex arc (motor or sensory path) • Myopathies exhibit this because muscle cannot respond to
the nerve impulse

SENSORY ABNORMALITIES THAT ACCOMPANY LMNLS•Anesthesia: Loss of feeling or sensation, especially the loss of pain.•Hypesthesia: Decreased sensitivity to sensory stimulation; also called hypoesthesia.•Paresthesia: Abnormal sensation such as burning, pricking, tickling, or tingling, especially occurring spontaneously.•Hyperesthesia: Exaggerated unpleasant sensitivity to touch or other non-noxious sensory stimuli.

SENSORY ABNORMALITIES THAT ACCOMPANY LMNLS
Hypalgia: Diminished sensitivity to painful stimuli:; also called hypoalgia.
Hyperalgia: Excessive sensitivity to painful stimuli.
Causalgia: sensation of persistent, severe burning of the skin, often accompanied by hypersensitivity to touch and temperature and trophic skin changes

*EXAM*: UPPER MOTOR NEURON LESIONSSpasticity = velocity-dependent increased muscle tone accompanied by hyperactive DTRs
• Any damage to the corticospinal tract causes spasticity (crosses at medulla pyramids)
• Predominantly in anti-gravity muscles (UE flexors, LE extensors)• Caused by lack of inhibition to control excitability of alpha motor neurons
Rigidity = increased resistance to passive stretch that is velocity independent and uniform throughout ROM
-much harder to stretch than spasticity
• Occurs in basal ganglia and extrapyramidal disorders• Cogwheel: rhythmic, interrupted resistance (Parkinson’s=only really sever)• Decorticate: usually from lesions in the thalamus, cerebral white matter, or
internal capsule• Decerebrate: from lesions in midbrain or diencephalon

RIGIDITY FROM BRAIN INJURY
Fredericks & Saladin book “Pathophysiology of the Motor Systems”

UPPER MOTOR NEURON LESIONS
Hypotonia: associated with cerebral or spinal shock, followed by an increase in spasticity
Muscle Weakness/Generalized Fatigue
• significant atrophy is rare since reflex activity is still present
Poor Coordination
• Loss of fractionation• Movement timing: increased reaction time & increased
movement time (time to build up contraction and complete movement)
• Involuntary movements (tremors, choreas, athetosis, etc)

UPPER MOTOR NEURON LESIONS
Associated reactions = unintentional movement of one limb that often occurs during the intentional movement of another limb
Ataxia = unsteadiness, incoordination, or clumsiness of movement
• Movement is jerky and unprecise• Difficulty regulating force, direction, and velocity of movement• Common in cerebellar lesions
Apraxia = inability to perform a goal-directed motor activity in the absence of paresis, ataxia, or disturbance of muscle tone
Sensory deficits – larger areas compared to PNS lesions

BRAIN STEM

Lesion Discriminative Touch and Proprioception
Pain and Temp
Upper midbrain Loss is all contralateral Loss is all contralateral
Posteriolateral medulla or lower pons
Not affected in face because tracts and nuclei are superior to medulla. Not affected in body because tracts are more medial.
Pain and temp loss ipsilateral in face (CNV uncrossed) and contralateral in body.
Medial medulla or lower pons.
Medial lemniscal axons cross midline in lower medulla so have contralateral loss in body.
Spinalthalamic, Contralateral face affected from second order neurons from CNV
Posterolateral upper pons or midbrain after all tracts from body have crossed midline
Contralateral in body. Proprioception is ipsilateral in face (only the CNVprop fibers have not crossed at this level).
Contralateral in face and body

BRAINSTEM LESIONS


BRAINSTEM LESIONS

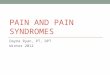
BELL’S PALSY
Innervation to upper face is bilateral
Innervation to lower face is unilateral (from opposite hemisphere)
“a” is Bell’s Palsy
“b” is stroke
Person in a and b requested to smile and close eyes

BELL’S PALSY: ETIOLOGY
• Unknown in most cases
• May be secondary to viral infection causing swelling in auditory canal or exposure to cold temperatures
• In a small number of cases, secondary to acoustic neuroma impinging on nerve

BELL’S PALSY: SIGNS & SYMPTOMS
• Motor: flaccidity• Mouth droops• Nasolabial fold is
flattened• Eyelid does not close
• Sensory: • Decreased taste on
ipsilateral tongue
• ANS:• Decreased tearing (dry
eye)
Characteristic Smile

BELL’S PALSY: INCIDENCE AND ONSET
• Incidence is 20/100,000 in US each year (affects 20,000-100,000 people in US / year)
• Typical onset is overnight• Onset more common between 20-40 y.o.
(increased incidence with increased age)• Increased risk in diabetics and pregnant women
and people with MS

BELL’S PALSY: MEDICAL TREATMENT
• High-dose corticosteroids for 5 days followed by a tapered dose for another 5 days
• Antiviral medications, e.g. acyclovir• Because of positive association between HSV and
Bell’s Palsy• Improves outcomes when paired with corticosteroids
• Eye patch, artificial tears (methylcellulose eye drops every 4 hours)
• Gentle massage and gentle heat occasionally used• PT for muscle retraining only if problems persist

DIABETIC POLYNEUROPATHYAffects PNS axons primarily (some demyelination)
Etiology: disrupted microcirculation
Onset:
• After long duration diabetes• In diabetics who have had diabetes for 25+ years, 50% have
this condition
• Occurs in insulin-dependent and non-insulin dependent diabetes
Some regeneration with control of diabetes

DIABETIC POLYNEUROPATHY
Characteristics
• Large nerve fiber involvement (most common)• painless paresthesias in feet and lower legs• decreased vibration and proprioception sense• decreased DTRs
• Small nerve fiber involvement• deep aching pain in legs and burning feeling in feet• decreased touch, pain, and temperature sensations• nocturnal pain and paresthesias

DIABETIC POLYNEUROPATHY
Screening/Examination Tests
• NCVs• Monofilament screening with 5.07 / 10 gm. filament• Vibration
Complications
• Diabetic ulcers (reducing WB helps)• 50% of non-traumatic amputation in US are in diabetic patients

ALCOHOLIC POLYNEUROPATHY
Affects PNS axon and myelin
Characteristics
• Distal muscle weakness and atrophy• Sensory involvement greater in LEs than in UEs• Pain and paresthesias in distal legs and soles of
feet (this does not typically happen in the diabetic polyneuropathy)
• Aching in calf muscles• Decreased ankle reflexes and poor sensation in
feet

ALCOHOLIC POLYNEUROPATHYCause
• Insidious onset and slow progression• Exacerbations may occur• Sensory signs and symptoms before motor• Mild case = mild aching in calf and feet• Severe case = severe motor and sensory signs
Prognosis
• with abstinence and improved nutrition, a slow, incomplete recovery may occur
• considerable discomfort may remain

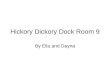
STOCKING-GLOVE PATTERN OF SENSORY IMPAIRMENT

CHARCOT-MARIE-TOOTH (CMT) DISEASEAlso known as:
• Hereditary Motor and Sensory Neuropathy Type I (HMSN) OR
• Peroneal Muscular Atrophy
Lesion site = PNS axon and PNS demyelination, anterior horn cell and dorsal root ganglion
Onset
• Hereditary• Late childhood or adolescence for CMT1• Adulthood for CMT2 (less severe with minimal sensory
loss)• Slowly progressive

CHARCOT-MARIE-TOOTH (CMT) DISEASE
Characteristics
• Pes cavus foot deformity (high arch) and hammer toes
• Symmetric weakness and atrophy in intrinsic foot, peroneal, and anterior tibialis muscles
• Weakness and atrophy rarely go above knee or elbow
• Paresthesias are common• Lead to foot drop (see steppage gait pattern)• Normal lifespan – most remain ambulatory
throughout their lives

CHARCOT-MARIE-TOOTH DISEASEFoot deformity: high arch pes cavus foot deformity with hammer toes

TABES DORSALIS
Lesion site: dorsal roots & posterior columns of lumbosacral and lower thoracic S.C.
Etiology: From syphilis
Diagnosis based on:
• Neuroimaging is normal• Abnormal tibial sensory NCVs• CSF has elevated protein level
Significant sensory loss!

TABES DORSALISCharacteristics
• Unilateral or bilateral presentation• Diminished proprioception and vibration in legs• Sensory ataxia of gait • Areflexia• Touch, pain, and temperature sensation are intact• Aching / paresthesias (radicular distribution)• May also have:
• Autonomic disturbances (bladder atony(incontinence), papillary abnormalities, impotence)
• Later onset of distal muscle weakness and atrophy (if anterior horn cells become involved)

HANSEN’S DISEASE (LEPROSY)
Lesion site: Peripheral nerves
Etiology: Mycobacterium leprae infection
Two forms:• Tuberculoid
• Primarily superficial nn
• Leprous• Weakness - symmetric• Sensory loss• Skin lesions

GUILLAIN-BARRE SYNDROME (GBS)
Alternate Name: Acute Inflammatory Demyelinating Polyradiculoneuropathy = AIDP
• Many variants of the syndrome exist
Lesion site
• PNS myelin (secondary axonal degeneration in many patients)
Etiology
• autoimmune disorder with unknown trigger (may be secondary to an upper respiratory or GI infection)

GUILLAIN-BARRE SYNDROME (GBS)
Primary Characteristics
• Weakness• typically symmetric, beginning in distal LE muscles and
ascending through body rapidly including facial muscles• facial and palatal weakness is common ( in about 50% of
cases)
• Paresthesias (usually transient)• Diminished or absent DTRs• Flaccid muscle tone

GUILLAIN-BARRE SYNDROME (GBS)
Early symptoms
• difficulty with walking• paresthesia in toes (commonly 1st symptom)• muscle tenderness (tender to touch)
About 50% have respiratory involvement
• up to 30% of GBS patients require mechanical ventilation during the acute phase
Dysarthria=slurring of words, dysphagia=difficulty swallowing, and diplopia=double vision develop in severe cases

GUILLAIN-BARRE SYNDROME (GBS)Can occur at any age, but mostly 5th-8th decade
Disease course:
• Maximal onset in less than 4 weeks, many in a few days• Static phase (plateau of 2-4 weeks)• Recovery takes months to years• Recurs in 10% of cases
Weeks
Onset
Static PhaseRecovery

GUILLAIN-BARRE SYNDROME (GBS)• 5% mortality rate• At 6 months, 85% are ambulatory• At 1 year, 20% remain significantly handicapped by
weakness• At 2 years, 8% have not achieved full recovery• Poorer prognosis with:
• onset at an older age• protracted time before recovery begins• need for artificial respiration• significantly decreased amplitude of evoked motor potential
(a sign of axonal degeneration)

POLIO & POST-POLIO SYNDROME (PPS)
Also called: Post-Polio Muscular Atrophy (PPMA)
Lesion site: anterior horn cells (little CN involvement)
Etiology• Polio virus initially.• Existing motor neurons reduce
the number of collateral sprouts resulting in more muscle cell death.
• As motor neurons die with age, there is no redundancy in the system for other motor units to take over, so motor function is decreased.
• NOT due to reactivation of the polio virus.

POLIO & POST-POLIO SYNDROME (PPS)
• Decades after onset of polio (mean of 25 years post-polio onset)
• ¼ to ½ of polio survivors are expected to develop post-polio syndrome (some sources say up to 2/3 of all polio survivors will get PPS)
• more common in women than men• occurs more frequently in those with more severe initial polio symptoms

POLIO & POST-POLIO SYNDROME (PPS)
Signs and Symptoms
Sensation• Not affected• Joint and muscle pain• Intolerance to cold
Motor• Paresis or flaccid
paralysis• Decreased or absent
DTRs=lmn• Decreased endurance for
physical activity
Exercise recommendations:• Never exercise to point of
fatigue (use general body conditioning and low resistance exercises)
• Monitor vitals before and after exercise (remember that respiratory muscles are also affected)
• Caution patient to stop exercise if pain persists or weakness increases

POLIO & POST-POLIO SYNDROME (PPS)Original signs & symptoms
• Asymmetric paralysis• Leg affected more
than arm• More severe
proximally than distally
• No eye muscles involved (CN involvement usually only temporary)
Post-polio S & S• Decreased
strength in previously affected muscles
• New muscle weakness
• Increased muscle atrophy
• Myalgia• Joint pain

AMYOTROPHIC LATERAL SCLEROSIS (ALS)
Also called Lou Gehrig’s Disease
Lesion site: anterior horn cells, lateral corticospinal tract, motor nuclei of brainstem, and motor area of frontal lobe (pre-central cortex)
Etiology unknown except in a few inherited cases

AMYOTROPHIC LATERAL SCLEROSIS (ALS)• LMN signs
• Progressive muscle wasting• Weakness (asymmetric weakness is often presenting
sign)• Fasciculations (especially evident in tongue)• cramps
• UMN signs• Spasticity• Hyperreflexia• Positive Babinski

AMYOTROPHIC LATERAL SCLEROSIS (ALS)
• Most common to see:• Weakness (greater in UEs than in LEs)• Atrophy• Fasciculations• Increased DTRs• Positive Babinski
• Later may see dysphagia and dysarthria• Onset:
• 90% of all cases have onset between 40-70 years of age
• Course is variable and progressive to all striated muscles (except extraocular)
• Death typically secondary to respiratory muscle involvement

AMYOTROPHIC LATERAL SCLEROSIS (ALS)
Prognosis
• Death in 2-5 years commonly from respiratory compromise (mean death is 3-4 years after onset if patient does not get ventilatory support)
• 20% survive more than 5 years• those who have ALS before age 50 generally live
longer

AMYOTROPHIC LATERAL SCLEROSIS (ALS)
• Functions typically preserved throughout disease:• Intellect is not affected• Eye movements• Bowel and bladder control
• Exercise recommended to:• prevent disuse atrophy • maximize strength in remaining innervated muscle cells
• Common problems with swallowing, speech, postural control, and respiration
• Treat pain with modalities such as TENS• Scapulohumeral joints may be affected with increased muscle
weakness . . . Can get glenohumeral joint subluxation