Embed Size (px)
Citation preview

ESPEN Congress Leipzig 2013
LLL Session - Nutritional support in respiratory diseases
New findings of meta-analysis in nutrition interventions for COPD and multimodal approaches
C. Pison (FR)
Nutritional Support in
Respiratory Diseases – LLL 38
New findings of meta-analysis in nutrition
interventions for COPD
and multimodal approaches
Pr. Ch. Pison, MD, PhD
Pulmonary Division
Lung transplantation group
University Hospital, Grenoble
Inserm1055, Grenoble
Joseph Fourier University
Grenoble, France
2 Leipzig, 4th of September 2014

Participation Quality of life - Morbidity
Mortality
FEV1
SpO2
Lungs Oxidant stress,
Hypoxia, Inflammation
Deficiency Systemic Oxidant stress,
Hypoxia, Inflammation
BMI
Skeletal muscles
International Classification of Functioning ICF-2, WHO, 2001
Activities Dyspnea 6 MWD
Obstructive Lung Diseases
3
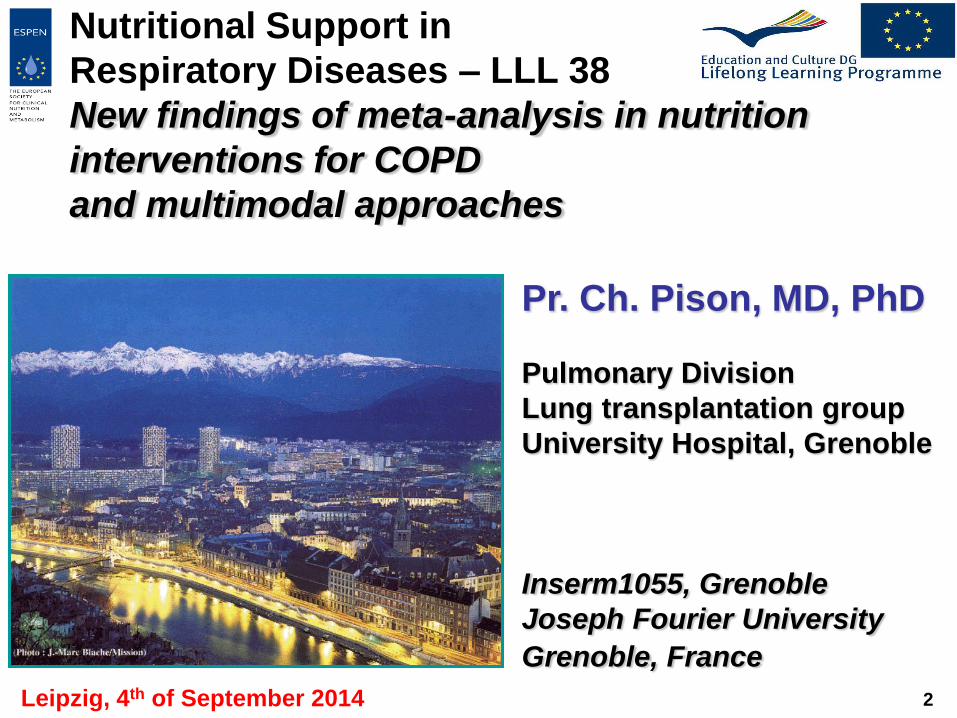
IV: Very Severe III: Severe II: Moderate I: Mild
FEV1/FVC < 70% FEV1 > 80% predicted
FEV1/FVC < 70%
50% < FEV1 < 80% predicted
FEV1/FVC < 70%
30% < FEV1 < 50% predicted
FEV1/FVC < 70% FEV1 < 30%
predicted or FEV1 < 50%
predicted plus chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccination
Add short-acting bronchodilator (when needed)
Add long term oxygen if chronic respiratory failure. Consider surgical
treatments
Therapy at Each Stage of COPD
4

• Depending on their condition COPD patients can need up to 600 kcal /day more than healthy individuals
• “Nutritional supplementation should initially consist of adaptations in the patients’ dietary habits and should be extended to administration of energy-dense supplements”
Baarends et al. Am J Respir Crit Care Med 1997;155:549-54
Baarends et al. 1997;52:780-5
Schols et al. JPEN 1992;16: 364-8
Schols al. Am J Clin Nutr 1991;54:983-7
Nici et al. AJRCCM 2006;173:1390-1413
Nutritional needs in COPD
5

• Acute effects of ONS, fat vs. carbohydrate, 11 subjects
COPD, 62±8 yrs, FEV1 34±12% pred., BMI 22.6±2.3.
Vermeeren et al. AJCN 2001;73:295-301
Post prandial dyspnoea:
fat vs. carbohydrate
250 kcal fat rich oral
supplement
250 kcal carbohydrate rich
oral supplement
6

More not always better!
• Energy intake, 568 kcal/d vs. 800 kcal/d, 2 severe depleted
groups of COPD, 19 vs. 20, 8-weeks in-pulmonary rehabilitation
Broekhuizen et al. British Journal of Nutrition 2005;93:965-71
7

Weekes et al. Thorax 2009;64:326-31
+ 194 kcal/d, + 11.8 g protein/d vs. Controls
no changes in muscle strength and respiratory function
St Georges + 10. 1, MRC score + 1 , ADL score + 1.5
Nutritional intervention
8

Nutritional support
in COPD treatment - Guidelines
• 2006 ERS /ATS guidelines. Nici et al. AJRCCM
2006;173:1390-1413
– BMI < 21
– involuntary weight loss: >10% during last 6 months or
>5% in the past month)
– depletion in FFMI, <16 males, <15 females
• 2010 SPLF guidelines. RMR 2010;27:522-48
– No attempt to lose weight
– Rehabilitation > nutritional supplementation in any cases,
especially if under nutrition
• 2014 – ERS statement on Nutrition and COPD
9

• Risk of nutritional depletion in subjects, even normal weighted,
undergoing Pulmonary Rehabilitation
Steiner et al. Thorax 2003;58:745-51.
Goris et al. The British journal of nutrition 2003;89:725-31.
Slinde et al. Clinical nutrition 2003;22:159-65.
Creutzberg et al. Nutrition 2003;19:120-7
Weekes et al. Thorax 2010;64:326-31
Nutritional support:
essential during rehabilitation
10

11
Nutritional intervention

Nutritional intervention
changes body weight, kg
17 studies,
8 combined
with
exercise,
increased
body
weight

13
Nutritional intervention
changes fat-free mass, kg

14
Nutritional intervention
changes in 6-MWD, m

Nutritional intervention alone
is not enough
15
ORGAN FAILURE
SPECIFIC DISTURBANCES Hypoxia, Acidosis,
Oxidative stress,
Growth factor impairments …
Evans WJ et al.
Clin Nutr 2008

Schols et al. AJRCCM 1995;152;1268-74
• Patients 233, FEV1 35 ± 5 %
• Duration 8 weeks, in-patient rehabilitation
• Intervention - exercise + education
- exercise + education + nutrition + placebo
- exercise + education + nutrition + anabolic steroids
• Results
• Increase in body weight with nutrition alone
& anabolic steroids
• Enhanced increase in FFM / Pi-max with anabolic steroids
Exercise training: - endurance
- low impact conditioning exercises
- no strength training
Multimodal Intervention
16
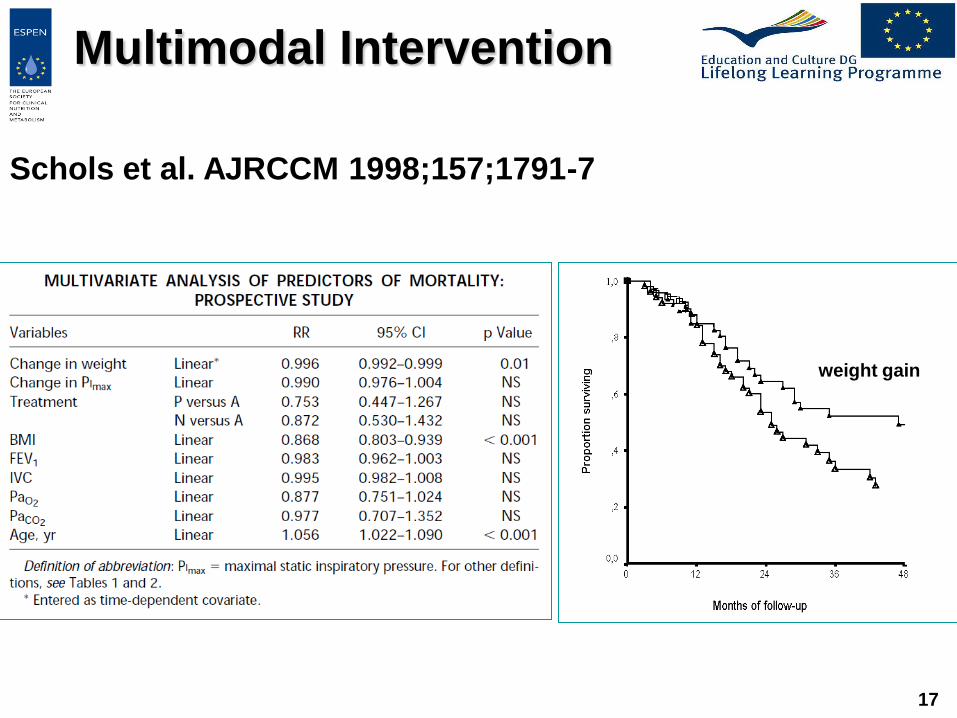
Schols et al. AJRCCM 1998;157;1791-7
weight gain
17
Multimodal Intervention
• Patients 102, 66±9 yrs, FEV1 58±17 %, BMI 26.1±4.4
97, 67±9 yrs, FEV1 60±15 %, BMI 27.3±4.7
Wmax < 70%, 20% depleted
• Duration 2 years
• Intervention 4 months home multimodal intervention,
20 maintenance care
versus usual care
• Results
• 4 months: better FFM, QoL, Wmax, endurance, MRC
dyspnea score, hand grip, 6MWD
• 2 years : better QoL, MRC score, endurance, 6MWD 18
INTERCOM. van Wetering et al. J Am Med Dir Assoc
2010;11:179-187
Multimodal Intervention

19
INTERCOM. van Wetering et al. J Am Med Dir Assoc
2010;11:179-187
Multimodal Intervention
INTERCOM muscle wasted
INTERCOM muscle non-wasted
Usual Care muscle non-wasted
Usual Care muscle wasted

Casaburi et al. Am J Crit Care Med 2004;170;870-8
20
47 male patients
with COPD, mean
FEV1 = 40%
randomized,
double blind,
controlled
4 groups,
resistance
exercise, 100 mg
testosterone
IM/week, 10 weeks
Multimodal Intervention
testosterone
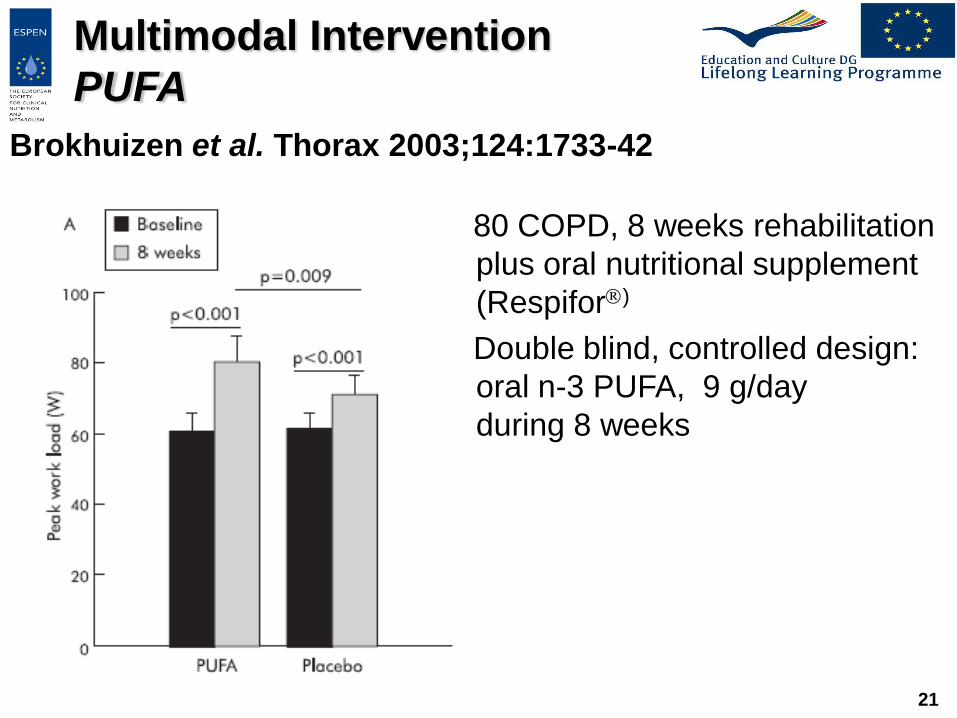
Brokhuizen et al. Thorax 2003;124:1733-42
21
80 COPD, 8 weeks rehabilitation
plus oral nutritional supplement
(Respifor)
Double blind, controlled design:
oral n-3 PUFA, 9 g/day
during 8 weeks
Multimodal Intervention
PUFA

• Patients 60, 66.6±9.6 yrs, BMI 21.5±3.8
62, 65.1±9.6 yrs, BMI 21.4±4.0
• Duration 12 weeks, 12 months follow-up
• Intervention - Education + Exercise + ONS + oral Testosterone
- Education
• Results
• 3 months: increases in body weight, FFM,QF, Hb,
endurance, Wmax, QoL in women
• 15 months : better survival per-protocol analysis
IRAD2 study in Chronic Respiratory Failure
Pison et al. Thorax 2011;66:953-60
22
Multimodal Intervention
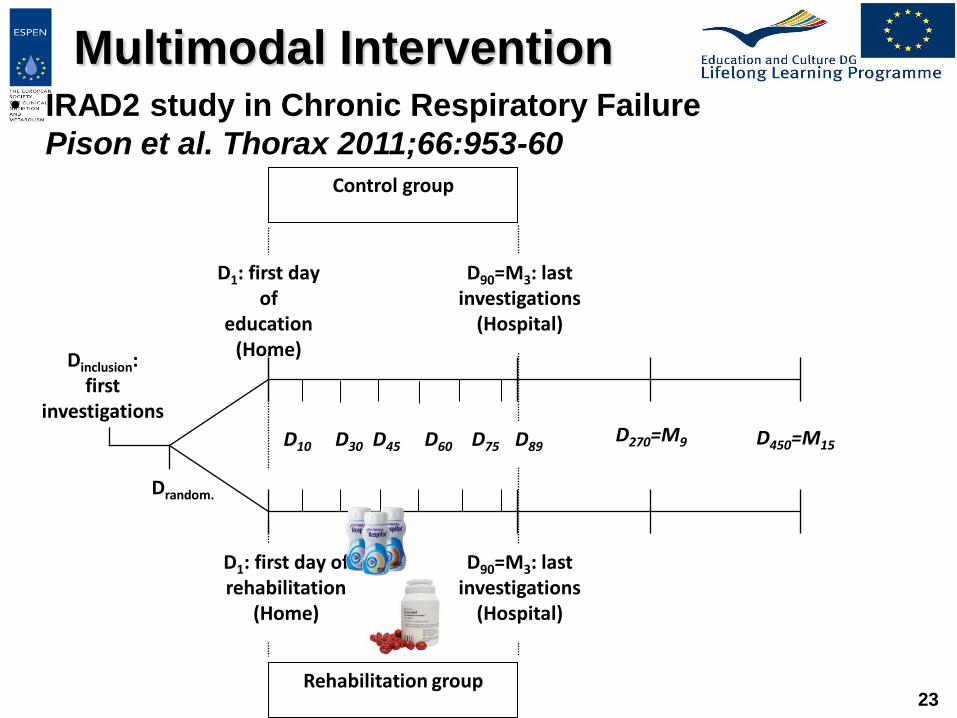
• IRAD2 study in Chronic Respiratory Failure
Pison et al. Thorax 2011;66:953-60
23 Rehabilitation group
Dinclusion: first
investigations
Drandom.
Control group
D10 D30 D45 D60 D75 D89
D1: first day of
education (Home)
D270=M9 D450=M15
D90=M3: last investigations
(Hospital)
D1: first day of rehabilitation
(Home)
D90=M3: last investigations
(Hospital)
Multimodal Intervention

IRAD2 study in Chronic Respiratory Failure
Pison et al. Thorax 2011;66:953-60
24
Multimodal Intervention

IRAD2 study in Chronic Respiratory Failure
Pison et al. Thorax 2011;66:953-60
25
Multimodal Intervention

IRAD2 study in Chronic Respiratory Failure
Pison et al. Thorax 2011;66:953-60
26
Multimodal Intervention

Budweiser et al. Respir Care 2006;51:126-32
27
Multimodal Intervention
NIV

Mineo et al. Eur Respir J 2011;36:408-16
28
Multimodal Intervention
LVRS

Multimodal Intervention
lung transplantation
0
,2
,4
,6
,8
1
0 2 4 6 8 10
Temps, années
après XII-2001, n = 39
avant XII-2001, n = 15
All indications, n = 204
CF, n = 54
0
,2
,4
,6
,8
1
0 2 4 6 8 10
Temps, années
après XII-2001, n = 134
avant XII-2001, n = 68

Multimodal
approach of
undernutrition
Low energy intake
Inactivity
Hypogonadism
Inflammation
Insulin-resistance
Others, hypoxia, ..
Integrated care
Counseling
ONS
Exercise
Androgens
others:
• n-3 FA
• N-acetylcysteine
• anti-TNF
• etc.
Multimodal Intervention

• Patient perspectives and objectives
• Smoking
• Infection
• Respiratory mechanical disadvantages : long-acting
bronchodilators
• Hypoxemia
• Energy intake deficit
• Promotion of Daily Physical Activities
• Modulation of systemic inflammation, omega-3
• Lung volume reduction
• Lung transplantation
Personalized &
Comprehensive Cares
31

Conclusions
• Multimodal Evaluation
• Multimodal Intervention
• Interventions at early and advanced disease, to be
tailored to the patient perspective
• Role of home disease management
32






![Protective ventilation for ALL patients...Cressoni M et al. Am J Respir Crit Care Med 2014,189(2):149–158 Cressoni M et al. Anesthesiology. 2016 Feb 12. [Epub ahead of print] Higher](https://img.pdfslide.us/doc/110x75/6019152bcd2580078d475698/protective-ventilation-for-all-patients-cressoni-m-et-al-am-j-respir-crit-care.jpg)