Embed Size (px)
Citation preview

Living with diabetes within the
framework of Swedish primary
health care:
Somalian and professional perspectives
Anne-Marie Wallin
SCHOOL OF HEALTH SCIENCES, JÖNKÖPING UNIVERSITYDISSERTATION SERIES NO. 6, 2009
f o r s k a r s k o l a n h ä l s a o c h v ä l f ä r d
Living with diabetes w
ithin the framew
ork of Swedish prim
ary health care: Somalian and professional perspectives A
nne-Marie W
allin
Anne-Marie Wallin
Anne-Marie Wallin is a Registered Nurse with a Master of Science degree in Public Health. She has many years of experience as a district nurse and as a public health worker in multicultural settings. She has been coor-dinator around immigrants issues in primary health care in Örebro County Council. Anne-Marie Wallin has developed and carried out projects focusing on spe-cific health needs among immigrants and participated in epidemiological studies specially focused on immi-
grants. She has also had lectures for SFI (Swedish for immigrants) classes regarding health care and lectures in training courses for local-government interpreters in Örebro municipality about the Swedish health care in general.
Owing to the increased immigration during the last twenty years or so means that a lot of health-care professionals within diabetes care will in the future be encounter-ing people with diabetes who are born in countries culturally remote from Sweden. To ensure a high quality of diabetes care for all patients there is a need to acquire deeper knowledge of immigrants experiences of living with the disease and their conceptions of the encounter in diabetes care within primary health care. Therefore the thesis includes both immigrants of Somalian origin and health-care profes-sionals. To the author’s knowledge is this the first published research in Sweden or elsewhere that focuses on immigrants from Somalia with diabetes mellitus.
The findings in the thesis showed that changing lifestyle was considered as a hard work by the patients and a number of barriers was mentioned especially when it comes to eating habits. There was also a variation how they managed the fasting month of Ramadan. Those who fasted did not see the diabetes as an obstacle, oth-ers did so and indicated that fasting was not compulsory for a sick person. Women used more supernatural beliefs than men when they described their experiences in connection with the diagnosis and their health beliefs. Most of the experiences of receiving the diagnosis consisted of ways of managing this information. The pa-tients conceived the diabetes care as being of high quality but they also conceived limitation with the care. They conceived unmet needs such as too long waiting times for appointments, not encountering the same physician every time, lack of contact with specialists and failure to culturally adapt dietary advice. Health-care professionals conceived cultural challenges in the encounter such as managing lan-guage barriers, illiteracy and different traditions such as fasting during Ramadan.
JÖNKÖPING, 2009
ISSN 1654-3602 ISBN 978-91-85835-05-8

School of Health Sciences, Jönköping University
Living with diabetes within the framework
of Swedish primary health care:
Somalian and professional perspectives
Anne-Marie Wallin
DISSERTATION SERIES NO. 6, 2009
JÖNKÖPING 2009

© Anne-Marie Wallin, 2009 ISSN 1654-3602 ISBN 978-91-85835-05-8

To my pillars in life Johnny, Mattias and Hanna


Abstract
Wallin, A-M. 2009. Living with diabetes within the framework of Swedish primary health care: Somalian and professional perspectives. Written in English with a Swedish summary. Dissertation in Nursing. The Research School of Health and Welfare, School of Health Sciences, Jönköping University, SE-55111 Jönköping, Sweden. The overall aim of this thesis was to provide knowledge on the one hand Somalian-born immigrants´ experiences of living with diabetes mellitus (DM) in a new cultural environment, on the other hand their encounter with Swedish diabetic care – this from both their own point of view and that of the health-care professionals. There was an endeavour to describe methodological aspects of the interpreter´s role in respect of the trustworthiness of research performed in multicultural societies. A descriptive design was used, involving three qualitative interview studies with an interpreter (Studies II-IV) and one systematic literature review (Study I). The latter served as a foundation for conducting the interviews with an interpreter and the Matrix Method was used. The same 19 patients with diabetes of Somalian origin participated in Studies II-IV, joined by five health-care professionals in Study IV. The interviews were subjected to qualitative content analysis in the case of Studies II and III, and to phenomenograpic analysis in the case of Study IV.
In Study I, 13 empirical cross-cultural interview studies with an interpreter involved were scrutinized. The findings showed that the interpreter’s role in the research process was given little attention. There was usually no account either of the style of interpreting, the interpreter’s previous experience or the seating arrangements for the interviews. On the other hand most of the studies offered direct or indirect information about the interpreter’s knowledge of the aim of the research or participation in the transcription of the text or data analysis. The most frequent techniques used to established trustworthiness were prolonged engagement and member checks.
A prominent problem for the participants in Study II was to give up traditional eating habits. Difficulty in managing everyday life was mentioned especially by women in connection with the need to keep to the diet regime because of a lack of understanding and support from family and friends. To changing lifestyle was considered as a hard work and a number of barriers was mentioned especially when it comes to eating habits. The findings showed a variation how the participants managed the fasting month of Ramadan. Those who fasted did not see the diabetes as an obstacle, others did so and indicated that fasting was not compulsory for a sick person. In study III the findings showed that women used more supernatural beliefs than men when they described their experiences in connection with the

diagnosis and their health beliefs. Most of the experiences of receiving the diagnosis consisted of ways of managing this information. Commonly mentioned by the participants, irrespective of gender, when they receiving the diagnosis was a attempt to find some advantages, or positive comparison. Other participants tried to repress the diagnosis and doubted it. Most of the participants, irrespective of gender, did not immediately respond with shock or other strong emotion when they received the diagnosis.
In study IV the patients conceived the diabetes care as being of high quality but they also conceived limitation with the care. They conceived unmet needs such as too long waiting times for appointments, not encountering the same physician every time, lack of contact with specialists and failure to culturally adapt dietary advice. Health-care professionals conceived several cultural challenges in the encounter such as managing language barriers, illiteracy and traditions such as fasting during Ramadan.
In conclusion, this thesis generate knowledge which can serve as a foundation to securing the quality of diabetes care for this patient group and contribute to working out local diabetic programmes for patients with another background than the Swedish. In addition the thesis can contribute to making improvements when it comes to working with an interpreter in qualitative interview studies as well as in clinical settings.
Keywords: Cross-cultural interviews, diabetes, experience, encounter, ethnic minority, health beliefs, health-care professionals, interpreter, literature review, qualitative method

Original papers
The thesis is based on the following papers, which are referred to by their Roman numerals in the text: I. Wallin A-M, Ahlström G. Cross-cultural interview study using
interpreters: systematic literature review. Journal of Advanced Nursing 2006, 55(6): 723-735
II. Wallin A-M, Löfvander M, Ahlström G. Diabetes: a cross-cultural
interview study of immigrants from Somalia. Journal of Clinical Nursing, 2007, 16(11C): 305-314
III. Wallin A-M, Ahlström G. From diagnosis to health: a cross-cultural
interview study with immigrants from Somalia. Submitted IV. Wallin A-M, Sidenvall B, Ahlström G. Conceptions of the encounter
in diabetes care on the part of patients of Somalian origin and health-care professionals: a qualitative study. Submitted
The studies I and II have been reprinted with permission of the publishers.


Contents
ABBREVIATIONS 12
DEFINITIONS 12
INTRODUCTION 13
BACKGROUND 15
The encounter between patients and health-care professionals in diabetes care 15
Language barriers in health care 16
Immigration to Sweden 17 Somalis in Sweden 18 Somalia: historical and social background 19
Diabetes Mellitus 20
Living with diabetes 21 Beliefs about health and illness 23
RATIONALE FOR THE THESIS 25
AIMS 26
METHODS 27
Design 27
Systematic literature review (Study I) 28 Material 28 Data collection 28 Data analysis 29
Qualitative interview studies (Studies II-IV) 30 Participants 30 Procedure 31

Data collection 32 Interviews 32
Data analyses 33 Qualitative latent content analysis (Studies II, III) 33 Phenomenographic analysis (Study IV) 34
Ethical considerations 35
SUMMARY OF THE FINDINGS 36
The interpreter’s role as described in qualitative cross-cultural interview studies (Study I) 36
Experiences of everyday life and managing diabetes-related problems (Study II) 37
Experiences of receiving the diagnosis and health beliefs (Study III) 38 Experiences of receiving the diagnosis 38 Beliefs about health 38
Encounters between patients of Somalian origin and health-care professionals (Study IV) 39
The patients´ conceptions 39 The health-care professionals´ conceptions 39
DISCUSSION 41
Reflections of the findings 41 Language 42 Habits and traditions 43 Health beliefs 47
Methodological considerations 48
CONCLUSIONS AND IMPLICATIONS 51
SVENSK SAMMANFATTNING 54
BAKGRUND 54
SYFTE 55

METOD OCH DELTAGARE/STUDIER 55
RESULTAT 56
SLUTSATSER 59
ACKNOWLEDGEMENTS 60
REFERENCES 62

12
Abbreviations
DM Diabetes Mellitus
T1DM Type 1 Diabetes Mellitus
T2DM Type 2 Diabetes Mellitus
Definitions
Asylum seeker: someone who has applied for refugee status and is awaiting a decision on this application (Taylor 2006). Belief: something accepted as true, especially as a tenet or a body of tenets, by people in a cultural group (Purnell & Paulanka 1998). Cross-cultural: a concept which comes from anthropological research in which cultural groups are compared and contrasted with one another (Brink 1999). In a cross-cultural research the participants are usually recruited from a specific country and the research process is conducted with procedures which are ethnically specific or culturally sensitive (Im et al. 2004). Culture: a shared way of life of a group of people that includes beliefs, values, ideas, language, communication, norms and visible expressed forms such as customs, art music, clothing, and etiquette (Papadopoulos 2006). Immigrant: a person born in a another country and settled (in the present case) in Sweden, irrespective of citizenship and reason for immigration (SOU 1999:137). Refugee: a person who is outside his/her country of nationality because of fear of persecution on grounds of race, nationality, religious or political beliefs or gender, sexual orientation or other membership of a particular group and is unable or unwilling to avail himself/herself of the protection of that country (SFS 2005: 716).

13
Introduction
As Sweden is becoming a multicultural society professionals in primary-health care need knowledge about immigrants’ view on health and living with long-term disease. This knowledge is of decisive importance for mutual understanding in the encounter between the immigrant and health-care professional. My own experiences of encounters with immigrant patients both as a district nurse and as a public health worker in multicultural settings have involved both challenges and opportunities. The challenges mostly consisted of language barriers when an interpreter not was present, but sometimes also our different views led to misunderstandings. From these encounters in clinical settings I have learnt that the Swedish health-care professionals and immigrants often have different perspectives on health, illness and treatment. Some patients used biomedical thinking and others folklore understanding, and there is a danger when health-care professionals neglect one at the expense of the other. Through my encounters with people of different ethnic backgrounds I have come to understand the influence of cultural background on many aspects of people’s lives. There needs to be a broad view of quality of care owing to the fact that during the past decades Sweden has changed from a society with a few ethnic groups to one with over a hundred, differing in background, language and religion (Ekblad et al. 2000). One such group are the Somalis. People who migrate from their country of origin to another country are generally healthier than those who do not, but this “healthy migrant effect” tends to wear off with time (Sundquist 2001). Studies in Sweden have found that diabetes was more common among immigrants, especially those born in countries outside Europe (Eliasson & Boström 2006, Wändell et al. 2007). This situation puts new demands on health care professionals. There are many obstacles to the provision of a good quality of care for ethnic minority groups of patients. There is for instance a lack of knowledge and information about different needs and how to deliver appropriate care when language barriers exist (Thomas & Dines 1994). The disease in focus in this thesis is diabetes mellitus (DM), which is a global health problem and the number of people who are affected have increased

14
worldwide (Zimmet et al. 2001). Today T2DM constitutes about 85-90 per cent of all DM cases (Amos et al. 1997, Zimmet et al. 1997, WHO 2006) and ethnic-minority groups have a higher prevalence than their host population (King & Rewers 1993, Carter et al. 1996, Zimmet et al. 1997, Jaber et al. 2003 ). Patients with T2DM are usually the responsibility for primary health-care, and this means that it is of great importance to know more about the encounters between immigrants with this type of DM and health-care professionals at primary health-care centres. Some studies in Sweden have indicated a higher prevalence of DM among Turkish women and immigrants from non-European countries than among Swedish born people (Wändell et al. 2003, Eliasson & Boström 2006, Wändell et al. 2007). In the opinion of Elsiasson and Boström (2006) these differences may be explained by the immigrants´ different conditions of life in Sweden, with social exposure and accompanying unfavourable habits of living. There is a lack of research focusing on health in persons with DM who are refugees and have not been in Sweden long and who come from countries with a culture far removed from the Swedish (Hjelm 1998). It is against this background that the present thesis investigates Somalian immigrants´ experiences of living with DM in Sweden, including their encounter with diabetes care in primary health care and taking into consideration both their own point of view and that of the health-care professionals.

15
Background
The encounter between patients and health-care professionals in diabetes care The essential part of health care is the encounter between a patient and a provider (Esposito 2005). The encounter can be seen as a part of a holistic view and constitutes an intersubjective meeting between two experiencing subjects, the patient and the health-care professional who engage in a true and meaningful confirming dialogue (Dahlberg 1996). It has been shown that the interaction between diabetic patients and health-care professionals is connected with the patients´ metabolic control. Patients with good control experience positive feed-back while those with unsatisfactory control experience a lack of communication with the care team (Wikblad 1991). It has also been shown that important aspects of the patient-professionals relationship are sufficient time for consultations, continuity in the care, the patient’s having the opportunity to ask questions and the professional’s listening to the patients´ concerns (Pooley et al. 2001). In a study where the focus was on patients perception of continuity in the encounter in diabetes care it was found that they saw it in terms of (a) regular reviews with clinical testing and advice over time, (b) having a relationship with a health-care professional who knew and understood them and took time to listen and explain, (c) flexible but consistent co-ordination among staff (Naithani et al. 2006). In another study it was found that patients perceived the diabetes care as superficial and mainly related to metabolic control, whilst the accompanying education consisted of an overwhelming amount of new information, often presented on only one occasion (Wikblad 1991). A Norwegian study has reported the health-care professionals´ frustration at their inability to be patient-centred when they met patients of Pakistani background with T2DM. They found that the patients expected them to adopt an authoritarian style, in total disagreement with their convictions. This made some of the health-care professionals afraid of insulting the patients, which resulted in their giving only diffuse advice to the patients (Fagerli et al. 2005a). In a latter study (Fagerli et al. 2007) the patients´ perspective on the encounter was investigated. They spoke of two dimensions, empathy and caring, and expressed a wish for cultural sensitivity and clarity in advice. The patients who were more integrated into Norwegian took up these two dimensions in relation to what they appreciated about the health-care professionals, whilst those who

16
were less integrated took up the two dimensions in relation to what they found lacking in the encounter. Lack of empathy and caring in the encounter reduced the patients´ trust in health-care professionals and also their interest in opening up and engaging in shared decision-making (Fagerli et al. 2007).
Language barriers in health care Communication is central to ensuring a care which is safe, efficient and equitable (Green et al. 2005). Communication is an organized, patterned system of behaviour that regulates and makes possible all professional-patient interaction (Andrews & Boyle 2008). Communication skills such as listening, questioning, touch, paraphrasing and body language are used, especially by nurses in developing a trusting relationship with patients (McCabe & Timmins 2006). Language is the primary means of interpersonal communication (Luckmann 1999, Munoz & Luckmann 2005). It is used to express ideas, feelings and emotions, to negotiate and to communicate information and, reactions (Luckmann 1999, Munoz & Luckmann 2005). Effective communication implies mutual understanding of the meaning attached to the messages (Andrews & Boyle 2008). Spoken language is the feature of every society, but people also communicate in nonverbal ways with the body, which vary across cultures (Luckmann 1999, Maltby 1999, Munoz & Luckmann 2005, Andrews & Boyle 2008). It is estimated that two-thirds of all communication is nonverbal, by means of bodily gestures, facial expressions, eye movement and eye contact (Luckmann 1999, Munoz & Luckmann 2005). The quality of communication between patient and health-care professional is vital. Attitude, style of speech and interaction during the encounter in combination with written information can be of decisive importance with regard to treatment outcome (National Board of Health and Welfare 2004). Barriers to communication may arise when patients and health-care professionals do not share the same culture, ethnicity, socio-economic background or educational background (Luckmann 1999, Munoz & Luckmann 2005, Andrews & Boyle 2008). The greatest challenge in cross-cultural communication in health care occurs when the patient and the health-care professionals speak different languages (Cioffi 2003, Andrews & Boyle, 2008). Language barriers have been shown to aggravate both stress and a sense of helplessness among nurses (Murphy & Clark 1993). Language barriers between health-care professionals and immigrant patients have been documented by several authors (Murphy & Clark 1993, Hjelm et al. 1998, Robinson & Gilmartin 2002, Gerrish et al. 2004, Hultsjö & Hjelm

17
2005, Thyli et al. 2007). Despite these barriers professionals interpreters were seldom or never used (Gerrish 2001, Gerrish et al. 2004, Fagerli et al. 2005b, Thyli et al. 2007), from which resulted misunderstanding and inadequate care (Gerrish 2001, Gerrish et al. 2004, Fagerli et al. 2005b). Communication is the key to patient-centred care, where the emphasis is on listening to what the patient has to say (Rhodes & Nocon 2003). When the patients and the health-care professionals differ in ethnicity, skills in cross-cultural consultation will be needed. There may be different expectations regarding the encounter, and there may be need of an interpreter (McAllister & Farquhar 1992). Trained interpreters, as compared with non-trained ones, have been found to improve clinical care in that there have been fewer errors of interpretation and greater patient satisfaction (Hornberger et al. 1997, Flores 2005, Karliner et al. 2007). Given the choice, patients choose professional interpreters (Ngo-Metzger et al. 2003, Edwards et al. 2005).
Immigration to Sweden There exist no established and distinct definition of the concept “immigrant” (SOU 1999:137). In the 1950s the word “foreigner” was used for a person who was not born in Sweden. Later this term was changed to “immigrant” in official documents as the thinking was that this change of words would imply a welcoming to participate in the new society. However, the change has not resulted in any improvement as ´immigrants´ represent a broader category than “foreigner” and the term follows to the next generation, i.e. the second generation of immigrants (Allwood & Franzén 2000). In this thesis I follow the National Public Health Committee defining an immigrant, irrespective of citizenship and reason for immigration, as a person born in an another country and now settled in Sweden (SOU 1999:137). During and after the Second World War, Sweden became an immigrant country instead of an emigrant country (Svanberg & Tydén 1992, Lundh & Ohlsson 1999, SCB 2004, Swedish Migration Board n.d.-a). During the post-war period up to 1970s the immigration was dominated by labour immigrants from the Nordic countries and from other European countries (Svanberg & Tydén 1992, Lundh & Ohlsson 1999, Bäärnhielm et al. 2005, Swedish Migration Board n.d.-a). New immigration rules were introduced in 1967, making immigration to Sweden for labour market reasons restricted for immigrants outside the Nordic countries (Swedish Integration Board 2006). From the early 1980s the number of asylum seekers increased from year to year and reached its peak in 1992 during the war in the former Yugoslavia, with a

18
total of 84000 applications (Swedish Migration Board 2008a). During the 1980s the largest groups of asylum seekers were from Lebanon, Iraq and Iran, and from the 1990s to 2007 from former Yugoslavia, Iraq and Somalia (SCB n.d-a., Swedish Migration Board 2008b). Today immigration is dominated by refugees and asylum seekers and close relatives (Svanberg & Tydén 1992, Lundh & Ohlsson 1999, SCB 2004). Immigrants are not a homogenous group. There are different ethnic groups as well as differences within the groups. Immigrants differ in ethnic, demographic and cultural background, socio-economic status, reasons for immigration and time of residence (SOU 1999:137, Ekblad 2000). Furthermore, individuals from the same country may have differ in education, religion, values and traditions (SOU 1999:137). Thus immigration has caused Sweden to become a multicultural society with over a hundred groups of people of different ethnical background (Ekblad et al. 2000). More than 13 per cent of the present-day population are foreign-born (SCB n.d.-b).
Somalis in Sweden Somalis are one of the most recent immigrant groups in Sweden. Only two per cent of those who have migrated to Sweden have been here for more than 10 years (Swedish Integration Board 1999). It was at the beginning of 1960s that the first immigrants from Somalia arrived in Sweden. The reason for immigration in this decade was studies or marriage (Nordström 1993). In connection with the civil war in Somalia in the early 1990s one to two million people fled their home country. Mostly they went to the USA, Canada and the United Kingdom, but some came to Sweden (Johnsdotter 2007). The majority of Somalis in Sweden came during this period but Somalis do still come as asylum seekers (Nordström 1993, Swedish Integration Board 1999, Swedish Migration Board 2008a, 2008b). The number of Somalis in Sweden is slightly more than 21 000 (SCB 2007) and approximate 8 200 have Swedish citizenship (SCB 2008). Most of the Somalis in Sweden live in Stockholm, Malmo and Gotenburg. In terms of age Somalis are a young immigrant group, about 54 per cent are under 30 years of age, while only 19 per cent are over 40 and only 0,1 per cent are older than 65 (SCB 2008). The Somalis are heterogeneous group, including people who are highly educated and people who are illiterate, townspeople and country people, wealthy people and less wealthy people (Swedish Integration Board 1999).

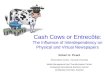
Somalia: historical and social background Somalia is situated in the zone commonly referred to as the Horn of Africa in the northeastern part of the African continent. It has the Indian Ocean to the east, the Gulf of Aden to the north and Ethiopia and Kenya as neighbouring countries to the west and south-west respectively (Figure 1). Somalia has a history of political conflict going back to 1969 when General Mahammad Siad Barré seized power and established a military dictatorship. Before the civil war began in 1991 the population of Somalia was approximately seven million (Scuglik et al. 2007). Somalia has one of the most homogeneous population in Africa, 85 per cent being described as Somalis. The official language is Somali but Arabic, Italian and English are also spoken (CIA 2008). The present written form of the Somali language was adopted in 1972 (Scuglik et al. 2007). Somalia is a clan-based society where political, economic and social welfare are influence by membership of the patrimonial clan family (Carroll et al. 2007).
Figure 1. Map of Africa with location of Somalia and neighbouring countries The Somali family represents values of legal marriage, honesty, good behavior, respect for elders, co-operation and group responsibility (Scuglik et al. 2007). The health-care system in urban areas in pre-war Somalia consisted of Western-style clinics and hospitals, and in rural regions “traditional” or “cultural” doctors were more common (Carroll et al. 2007). Most Somalis are Muslims and fasting during the month of Ramadan is one of the five pillars of Islam (Salti et al. 2004, Smide 2006). A person who fasts during Ramadan must refrain from eating, drinking, use of oral medications and smoking from dawn to sunset (Qureshi 2002, Al-Arouj et al. 2005). However, there are no restrictions of food or fluid intake from sunset to down (Al-Arouj et al. 2005, Smide, 2006). During Ramadan most people consume two meals per day, one after sunset (Iftar or Iftari) and the other before dawn
19

20
(Suhur or Sehri) (Qureshi 2002, Al-Arouj et al. 2005). The evening meal consist of extra sweet and savoury foods during the Ramadan (Barber et al. 1979, Qureshi 2002, Smide 2006). Fasting is not obligatory according to Islamic roles if it will have harmful consequences for the individual. People with diabetes fall into this category because they are at high risk for various complications if the pattern and amount of their food and fluid intake is markedly altered (Al-Arouj et al. 2005).
Diabetes Mellitus The World Health Organization (WHO) estimates that more than 180 million people worldwide suffer from DM and the figure is expected to increase to 366 million by 2030 (Wild et al. 2004, WHO 2006). Most cases will be T2DM, which is associated with a sedentary lifestyle and obesity (Zimmet et al. 2001). The “developing” world will to an increasing extent be faced with this challenge because of expected demographic changes and transitions to a lifestyle similar to that in industrialized nations (Renders et al. 2000, Green et al. 2003). Besides populations of developing countries, minority groups and population groups in industrialized countries with unfavourable living conditions are those who face the greatest risk of getting diabetes (King & Rewers 1993, Zimmet, 2000). In Sweden the prevalence of known diabetes has been estimated as 3-4 per cent of the population (Berger et al. 1998, Lundman & Engström 1998, Berger et al. 1999, National Board of Health and Welfare 1999), which is to say approximately 300,000 individuals (National Board of Health and Welfare 1999, Eliasson & Boström 2006). T1DM represents 10-15 per cent of all diabetes in Sweden and 30,000 – 40,000 are affected, of whom about 7,000 are children. T2DM, on the other hand, is common after the age of 50. Half of the approximately 250,000 people with this type are over 65 (Eliasson & Boström 2006). A higher prevalence of DM has been reported among immigrants from non-European countries than among Swedish born people (Wändell et al. 2003, Eliasson & Boström 2006, Wändell & Gåfvels 2007, Wändell et al. 2007). DM is a chronic disease in which the body has deficiency of and/or a resistance to insulin (Jerreat 2004, WHO 2006). Characteristic symptoms are thirst, polyuria, blurring of vision and weight loss. However, often symptoms are not severe, or may be absent, for which reason hyperglycaemia may go for a long time undiscovered (Alberti & Zimmet 1998). Hyperglycaemia is a common effect of uncontrolled diabetes and over time many of the body’s systems, especially the nerves and blood vessels are affected (WHO 2006). The two major classes of DM are type 1 (T1DM) and type 2 diabetes mellitus (T2DM)

21
(Guthrie & Guthrie 2002, Loveman et al. 2003, WHO 2006). In 1980 the Expert Committee on Diabetes mellitus named them besides T1DM and T2DM also insulin-dependent diabetes mellitus (IDDM) and non-insulin diabetes mellitus (NIDDM). The terms T1DM and T2DM were omitted in 1985 but as of 1998 they have been retained (Alberti & Zimmet 1998). T1DM is characterized by a lack of insulin production due to a cell-mediated auto-immune destruction of pancreatic beta-cells, and the person affected is totally dependent on injected insulin to survive (Jerreat 2004, Peters Harmel & Mathur 2004). Approximately 75 per cent of people who develop T1DM do so before 30 years of age (Peters Harmel & Mathur 2004). T2DM on the other hand, which accounts for over 90 per cent of cases globally, is characterized by insulin resistance and/or abnormal insulin secretion, either of which may predominate (Zimmet 1999, Zimmet et al. 2001). Initially and sometimes throughout their lives, people with this form of diabetes do not require insulin to achieve satisfactory diabetic control (Peters Harmel & Mathur 2004). If the control of blood glucose is not achieved by means of diet or oral hypoglycaemic agents, insulin is used (Zimmet et al. 2001). The risk of developing T2DM increases with age, obesity and lack physical activity (American Diabetes Association 2003) and the disease develops gradually over a long period, with vague symptoms or none at all (Green et al. 2003). T2DM is more common in people with a family history of the disease (American Diabetes Association 2003). T2DM is still a disease of the middle-aged and elderly but there is accumulating evidence to indicate that onset in those under 30 is common. For example in Japan T2DM is more common among children than T1DM (Alberti et al. 2004). Probably T2DM will occur more frequently among younger people in the future because overweight is increasing in this population worldwide (Eriksson et al. 2001). Persons with T2DM in Sweden are mostly handled by general practitioners (GP) and district nurses in primary health care, who have special training in diabetes care. These GP and nurses usually work in teams and see patients regularly. The nurse can see patients independently and it is also common that patients see paramedical staff, e.g. dieticians (Holmström & Rosenqvist 2005).
Living with diabetes Being diagnosed as having a chronic disease such as diabetes is distressing for the majority of people (Beeney et al. 1996). Commonly emotions in reaction to the diagnosis include stress, shock, sadness, fear, despair, anger, anxiety depression and denial (Beeney et al. 1996, Gillibrand & Flynn 2001, Kralik et al. 2001, Burns & Skelly 2005). In a study of newly diagnosed diabetes patients three main routes to diagnosis were found. These routes, which differed in their

22
effect on patients’ emotional reactions to the diagnosis were “suspected diabetes”, “illness” and “routine”. Those patients who had suspected diabetes showed no emotional reaction to the diagnosis, while those within the `routine´ road described the most varied emotional reactions. Some felt shocked and a little scared, others felt grateful or were glad that their diabetes had been diagnosed. The most prevalent emotional reactions among those on the ´illness´ route was amazement or a sense of relief: thinks might have been worse (Peel et al. 2004). DM being a chronic disease, those afflicted with it have to adjust and integrate it into their daily life (Dalal 2000). They have to make lifestyle changes such as dietary adjustments, exercising regularly, adherence to both medication and blood sugar testing and going for medical check-up. For some these changes can be demanding (Hörnsten 2004). Also the family will need to make adjustments as they, too, `live with diabetes´ (Guthrie & Guthrie 2002). The goal of the treatment is to prevent acute and long-term complications and to maintain a high quality of life (National Board of Health and Welfare 1999, Loveman et al. 2003). People with diabetes need to maintain control over it in order to prevent complications, therefore it is the duty of the health-care professionals to educate and encourage them to make informed decisions in their everyday lives (Van Dam et al. 2003). People with diabetes need also to know and understand their disease, their role as decision-makers and how to take responsibility for the day-to-day diabetes care. Self-management education is essential for the attainment of these goals throughout life and should be adjusted to individuals needs (National Board of Health and Welfare 1999, Funnell & Anderson, 2002, Loveman et al. 2003). When the disease is under control the patient can be confident and independent, feeling a sense of freedom (Edwall et al. 2008). Living with diabetes generates psychological stress. Persons with diabetes must continually pay attention to managing their regimen. This involves eating, sleeping, physical activity, intake of medication and maintenance of an acceptable blood glucose level. In addition a person with diabetes balances between hyperglycemia and the attendant fear of diabetes complications and hypoglycemia and the fear of acute complications (Rubin & Peyrot 2001). Living with diabetes has been described by some people in terms of lack of freedom, restrictions, and sense of uncertainty about the future (Lundman 1990, Callaghan & Williams 1994, McCord & Brandenburg 1995, Koch et al. 1999, Popoola, 2005). Others have spoken of it in terms of struggling with changed health situation and worries about the future (Burns & Skelly 2005, Penckofer et al. 2007) or in terms of stress due to the constant demand for vigilance (Koch et al. 1999). It has been found that Arabic-speaking immigrants living in Sweden find it difficult to cope with their diabetes. On the other hand

23
the cultural and language barriers they encountered in diabetes care are less of a problem for them (Sahle Stattin 2001). Certain differences have been found between women and men in respect of living with diabetes. In Koch and co-workers´ studies (Koch et al. 1999, 2000) women indicated that the disease had restricted their lives, while men indicated that it had a positive effect on their lives. Also in two other studies women indicated more hindrance in their daily activities than men did (Fitzgerald et al. 1995, Wenzel et al. 2005). Further, Swedish women were found to be more worried than men about long-term complications. Men, on the other hand, were more troubled by the limitation of personal freedom the disease caused. In contrast to the recently mentioned studies, women more often had something positive to say about having diabetes than men did (Gåfvels 1997). In a study by McCord & Brandenburg (1995) the participants indicated positive features of their having contracted diabetes: the felt that it had led them to a healthier and/or happier lifestyle.
Beliefs about health and illness Beliefs about health and illness are culturally constructed and affect patients’ decisions regarding their choice of self-care treatment (Helman 2001, Daly et al. 2002, Munoz & Luckmann, 2005). For health-care professionals it is important to have knowledge and an understand of the health beliefs of their patients to ensure optimum care (Hawthorne et al. 1993, Hodes 1997, Greenhalgh et al. 1998, Jobanputra & Furnham 2005). The sick person’s initiative with regard to managing a disease is dependent of his or her perception of the disease and its causes (Dalal 2000). Consequently there is an increasing need to understand the beliefs of the patients (Esposito 2005). In a Swedish study one quarter of the health-care professionals in diabetes care spoke of lack of knowledge about differences between Swedish born and immigrant diabetic patients’ beliefs about health and illness (Hjelm et al. 1998). In most cultures beliefs about health and illness are part of a complex body of inherited folklore influenced by notions from media, the Internet and the medical model (Helman 2001). Lay theories of health and illness are often set in relation, in the literature, to Helman’s (2001) division of the aetiology of ill health into four domains. These domains are: within the individual, in the natural world, in the social world and in the supernatural world. In most cases these lay theories are multicausal, involving all four of the domains. In the case of the domain designated within the individual is a question of bodily malfunction. In the case of the natural world it is a question of the natural environment, living as well as inanimate. Common in this domain are climate

24
condition such as cold, heat, wind, rain, snow, or damp. In the case of the social world other people are blamed for the illness - people believed to possess the power to harm others. In the case of the supernatural world illness is ascribed to the direct action of supernatural entities, such as gods, spirits or ancestral shades (Helman 2001). Helman (2001) points out that individual and natural explanations for health and illness are more prominent in industrialized countries whilst social and supernatural explanations are more prominent in non-industrialized countries. Several studies have investigated differences in beliefs about health and illness among minority ethnic groups as compared to the majority population. For example in a study from the USA the participants (White, Black, Latinos and Asians) had to rate the importance of 37 possible causes of illness. All participants irrespective of background, rated natural and supernatural causes as the most important factors but participants from the minorities cited supernatural causes significantly more often than did participants from the majority population (Landrine & Klonoff 1994). Furnham and co-workers (1999) tested Helmans theory (2001) in a cross-national study in three countries, the UK, Uganda and South Africa. In accordance with Helman’s theory supernatural and social explanations of health were more prominent among the Ugandan and South African participants than among the British. Also in a later study supernatural explanations of health and illness were found to be more important among British Indian immigrants than among British Caucasians. However, psychological factors, self-responsibility and physical vulnerability were the most accepted type of explanation of health and illness among these groups (Jobanputra & Furnham 2005). In a recent study among Ugandan men and women the beliefs about health and illness were mainly attributed to individual and social factors but nature and supernatural factors were also mentioned (Hjelm & Nambozi 2008). In a Swedish study both Yugoslavian born females and Swedish-born females put forward individual factors as causes of diabetes (Hjelm et al. 1999). In another study, men born in Sweden, Arabic countries and the former Yugoslavia also described health mainly in relation to individual and social factors (Hjelm et al. 2005). In summary, some studies have shown that in non-industrialized countries people mostly use supernatural and social explanations for health and illness while individual explanations are more salient in non-industrialised countries.

25
Rationale for the thesis
Sweden has become a multicultural society owing to the increased immigration during the last twenty years or so and has over a hundred ethnic groups. DM is a growing health problem worldwide and studies have indicated a higher prevalence of DM among immigrants from non-European countries than among Swedish-born people. This means that health-care professionals within diabetes care will in the future be encountering people with diabetes who were born in countries culturally remote from Sweden. Little has been written about how to work with interpreters into cross-cultural research. In addition, members of immigrant groups who are not fluent in the majority language often have been excluded from research, which lead to an inaccurate portrayal of immigrants health-care needs. In summary: to ensure a high quality of diabetes care for all patients in Sweden there is a need to acquire deeper knowledge of immigrants´ experiences of living with a chronic disease such as DM and immigrants´ and health-care professionals´ perceptions of the encounter in diabetes care within primary health care. Therefore this thesis includes both immigrants of Somalian origin and health-care professionals. There is no previous published research - either in Sweden or elsewhere - that focuses on immigrants from Somalia with DM.

26
Aims
The overall aim of this thesis was to provide knowledge about on the one hand Somalian-born immigrants´ experiences of living with diabetes mellitus (DM) in a new cultural environment, on the other hand their encounter with Swedish diabetic care – this from their own point of view and of the health-care professionals. Further, there was an endeavour to describe methodological aspects of the interpreter’s role in respect of the trustworthiness of research performed in multicultural societies. The thesis is presented in four studies based on the following four specific aims:
I: To review how the interpreter's role is described in empirically based qualitative cross-cultural interview studies and how trustworthiness is determined.
II: To describe how persons from Somalia with DM experience everyday living in Sweden and how they manage diabetes-related problems, with inclusion of a gender perspective.
III: To investigate how immigrants from Somalia living in Sweden experiences the diagnosis and to describe their beliefs about health.
IV: To describe how patients of Somalian origin and health-care professionals perceived the encounter in diabetes care at primary health-care centres.
In this thesis, by `cross-cultural study´ is meant a study where the participants and the researcher do not have a common language and therefore an interpreter was used during the interviews.

27
Methods
Design The thesis has a descriptive design with qualitative methods in three of the studies (Studies II-IV) and one study (Study I) is a systematic literature review. The latter study (Study 1), which focuses on qualitative cross-cultural interview studies with an interpreter involved, served as a foundation for conducting the interview with the participants of Somalian origin since here, too, an interpreter was involved. The design and methods are presented in Table 1. Two of the empirical studies (Studies II, III) focus on individuals of Somalian origin diagnosed as having DM and the other (Study IV) not only on these participants but also on professionals at primary health care centres. Table 1. Design and methods used in the studies in the thesis Study Design Data collection Data
analysis 1 Systematic
literature review
Systematic review of qualitative interview studies with an interpreter involved (n = 13)
Garrard’s Matrix Method
II Descriptive Qualitative
Semi-structured interviewwith adult persons of Somalian origin with DM. An interpreter was involved in the interviews (n = 19)
Latent content analysis
III Descriptive Qualitative
See study II Latent content analysis
IV Descriptive Qualitative
Semi-structured interviewwith adult persons of Somalian origin with DM (same participants as in study II and III) and health-care professionals in diabetes care (n = 19 participants of Somalian origin, 5 health care professionals)
Phenomeno-graphic analysis
Qualitative research is defined by Munhall (2001, p 68) as “involving broadly stated questions about human experiences and realities, studied through sustained contact with persons in their natural environments, and producing rich, descriptive data that help us to understand those persons´ experiences”. In

28
a qualitative research the researcher seeks a close involvement with the persons under investigation, so as to see the world through their eyes (Bryman 2004). There were several reasons for choosing this approach. First, descriptive design and qualitative methods are suitable when the population are unstudied or little is known about the phenomenon to be investigated (Morse & Field 1995, Brink & Wood 1998). Second, qualitative methods are essential for identifying and confirming intangible and unknown aspects of humans and when describing and understanding a phenomenon from the emic perspective (Morse & Filed 1995, Patton 2002). Third, qualitative research is the primary method for gaining new knowledge greater understanding of the complex multicultural world (Leininger 1998).
Systematic literature review (Study I)
Material In order to allow the participants of Somalian origin to fully express themselves the author decided to conduct the interview with aid of an interpreter. Since the author had no experience to working with an interpreter in a research setting it was important to investigate how other researchers had described the interpreter’s role in qualitative cross-cultural interview studies and how they had determined trustworthiness. Therefore a systematic review was conducted in respect of these matters before conducting the interviews with the participants of Somalian origin (Studies II-IV). Inclusion criteria with regard to the review items were the following: (1) qualitative cross-cultural interview studies with an interpreter involved; (2) published in peer-reviewed journals in English; (3) abstract available to judge whether the study was relevant. A total of thirteen studies fulfilled the criteria and of these four were conducted in Canada, two each in the USA and the UK and one each in Australia, Lithuania, South Africa, Sweden and Vietnam. The studies were published during the period 1988 - 2004 and four of them were conducted in countries foreign to the authors.
Data collection In order to obtain an overview of qualitative cross-cultural interview studies conducted with aid of an interpreter a systematic literature search was carried out during October-November 2004. Studies were identified through systematic searches in the following electronic databases: CINAHL, ERIC,

29
PsycINFO, PubMed, Sociological abstract and Your Journals @Ovid. Several search terms were used in combination and the searches in each database included all the years covered at that time. The search terms were: 1) “interpreter” in combination with “qualitative interview”, “qualitative research”, “migration study”, “immigrant stud”٫, “immigration study”, “cross-cultural intervie”٫, “cross-cultural study”, “immigrant”, “immigrants”, “immigration”, “migration”, “focus group”, “validity”, “trustworthiness”, “threats to validity” and “threats to trustworthiness”. 2) “bilingual” in combination with “validity and interview”, and “trustworthiness and interview”. 3) “translator” in combination with “validity” and “trustworthiness”. 4) “cross-language” in combination with “research”. After the exclusion of duplicates and of studies not related to the aim of the present study, 10 studies remained, and they were supplemented with three found by means of a manual search of the included studies´ reference lists. Consequently 13 studies were included in the review.
Data analysis To investigate how the interpreter’s role was described in previous qualitative cross-cultural interview studies and how trustworthiness was determined, a review matrix was used to scrutinize the studies. The Review Matrix is the central part of the Matrix Method, which is both a structure and process for analysing/scrutinizing literature (Garrard 1999, 2007). The purpose of the Review Matrix is to provide a structure for creating order and comparing the information from the literature (Garrard 1999, 2007). Writings of experienced cross-cultural researchers were reviewed first. From this the following topics were developed to be used in the analysis of the thirteen studies: (1) Number of interpreters included in the study; (2) Background of the interpreter(s) (gender, age and cultural background); (3) Style(s) of interpreting and seating arrangements during the interviews; (4) Competence of the interpreter(s) (previous experience of interpreting, respect and trust on the part of the group being studied); (5) Extent of participation of the interpreter(s) in the research process (Know(s) the aim of the research? Take(s) part in the transcription of the text and in the data analysis?); (6) Is/Are the interpreter(s) visible or invisible in the research study? (What term is used with reference to the interpreter(s): “with”, “through”, “assistance” (etc.)? Is/Are the interpreter(s) present in the text through the use of the third person in the translation and in the quoted remarks of the participants? Was the/each interpreter interviewed about his or her opinions and are these documented in the publication?); and finally (7) Established trustworthiness was in this study reviewed in accordance with Lincoln and Guba’s (1985) methods for demonstrating credibility:

30
prolonged engagement, triangulation and member check. An example of the analysis of the seven topics is shown in Table 2. Table 2. Example of analysis from the topics included in the review matrix Author(s) (year), Country Somerville (2001), United Kingdom Topics Numbers of interpreters OneBackground of interpreter(s) Gender available Interpreting style(s) and seating during the interviews
Not available
Competence of interpreter(s) The interpreter was unknown for the participants. Not available whether the interpreter had previous experience of interpretation
Extent of participation of interpreter(s) in the research process
Only available that the interpreter had information about the project
Interpreter(s) visible or invisible in the study Invisible. The author expressed that she did interviews using an interpreter. Quoted passages not in the third person and the interpreter is not interviewed in the study
Trustworthiness Triangulation by investigators and member check with only one of the participants due to limited interpreter time
Qualitative interview studies (Studies II-IV)
Participants The participants were recruited from six primary health care centres in two towns in Sweden. These six centres´ districts are characterized as multicultural areas. Inclusion criteria for participation for the diabetic persons were the following: Somalian-speaking adults (>18 years) diagnosed as having had diabetes for at least six months. If the person had other diseases these should have been stable during the past year. Contact was made with the district nurse who cared for diabetic patients at each primary health care centre to get access to data in the medical records of the persons who fulfilled the inclusion criteria.

31
For the health-care professionals the inclusions criteria were: district nurses or general practitioners responsible for diabetes care at primary health-care centres who are, or have been, in contact with at least five Somalian-speaking patients with diabetes (Study IV). This in order to avoid preconceived opinions based on too narrow experience. Thirty-nine individuals, 33 persons with diabetes and six health-care professionals, who fulfilled the inclusion criteria were invited to participate. Ten of the 33 diabetic persons declined and four could not be reached (7 men and 7 women). Five of 6 eligible health-care professionals, 4 nurses and 1 general practitioner (all women), were willing to participate, the other could not be reached. Thus there were 19 participants in Studies II, III and 24 in Study IV. All of the participants of Somalian origin had T2DM with duration 1-13 years (mean 7 years). Most of them (11) were treated with oral anti-diabetes drugs, five with a combination of tablets and insulin, two with insulin and one only with diet. Eleven were women and eight were men, aged from 30 to 83 years (mean 55 years). They had lived in Sweden between 1-14 years (mean 10 years) and nearly all of them, (16) had received their diagnoses in Sweden.
Procedure The potential participants received a letter (in Somali in the case of the persons of Somalian origin) with information about the research project. After three to four days they were contacted by phone by the author – or by an interpreter in the case of language barrier. They were given additional information about the study, were assured that participation was voluntary and were guaranteed confidentiality, and then they were asked if they were willing to participate. If they agreed to participate an appointment for the interview was booked. The participants had the opportunity to choose the place of the interview. Most of the interviews with the persons with diabetes were conducted in their homes although five preferred secluded but public places, one at a primary health care centre and one at the interviewer’s workplace. The interviews with the health-care professionals were all performed in a secluded place at their workplaces. The interviews were tape-recorded after permission from the interviewee and lasted about two hours with the persons with the diabetic persons and about one hour with the health-care professionals. Written notes were taken in the case of two participants (persons with diabetes) who refused tape-recording. All interviews were transcribed verbatim in Swedish and also expressions of emotions were noted.

32
Data collection
Interviews All the data collection in Studies II-IV was carried out by means of face-to-face qualitative semi-structured interview of a conversational nature based on an interview guide. The purpose of the qualitative research interview is to understand experiences from the interviewee’s perspective. The knowledge which is obtained is created by interaction between the interviewer and the interviewee (Kvale 1996). The interview guide lists the questions or topics that are to be explored during the interview and ensures that these remain the same in the case of each person interviewed (Patton 2002). The main question for the interview in Study II was: “What is it like to live with diabetes?” In Study III the following two main questions were asked: “What was your experiences of receiving the diagnosis”? and “What do health means to you ”? In Study IV the main question put to the patients with diabetes was: “What are your experiences of the encounter with the diabetes care at primary health-care center”? and to the health-care professionals: “What are your experiences of the encounter with patients with diabetes of Somalian origin”? The intention during the interviews was to encourage the participants to speak freely without interruption. Follow-up questions were formulated in accordance with how comprehensively the person answered the main question(s). Frequently used follow-ups questions in the qualitative studies were: “Can you tell me more?”, “Can you explain?”, “What did you feel then?” ”What did you think then?” and “What did you do then?”. Interviews with aid of an interpreter Two professional interpreters - one man and one woman, both originally from Somalia - were recruited for interpretation during the interviews. The point of having interpreters of different sexes was to give the participants the opportunity to choose the sex of the interpreter. Both interpreters were experienced local-government interpreters but neither of them had previously worked as an interpreter in qualitative research interviews. There were several reason why the interviews were conducted with aid of an interpreter. First, participants may feel less confident and intelligent if the interviews are not conducted in their first language (Murray & Wynne 2001). Second, conducting the interviews in the participants´ first language maximizes the quality of data (Twinn 1998). Third, what is said must of course be understandable to the participants and use of their own language is ideal in this respect (Berg 2004). Finally, this thesis could not have been properly accomplished without the aid of an interpreter in the interviews because many of the participants of Somalian origin were not fluent in Swedish.

33
Out of the basis of knowledge acquired in previous cross-cultural studies (Study I) the interviews with participants of Somalian origin with an interpreter involved were carried out in the follow way. Before the interviews a meeting was held with the interpreters to clarify the aim of the research project, the research questions and the interpreter’s role during the interview (Jentsch 1998, Murray & Wynne 2001, Adamson & Donovan 2002). Baker and co-workers (1991) discussed consecutive and simultaneous interpreting. In the case of the former one person speaks at a time, in the case of the latter the interpreter is speaking at the same time as the interviewer or the interviewee (Baker et al. 1991). The latter style is not recommended for a one-to-one conversation since it can be distracting for all parties involved. This style involves a greater risk of error in that the interpreter is subjected to more stress and fatigue than in the case of the consecutive style (Westermeyer 1990). Therefore the style of interpreting during the interviews in Studies II-IV was consecutive, and just the essential meaning of what was said was translated (i.e. the translation was not word-by-word). In most cases the interviewer and interpreter sat side-by side facing the interviewee. The interpreters were not previously known to most of the interviewees. Two participants did not want an interpreter at all, instead their husband/wife helped to translate when necessary.
Data analyses
Qualitative latent content analysis (Studies II, III) Content analysis or qualitative content analysis (Polit & Beck 2004) is a widely used qualitative method for analysing text data (Hsieh & Shannon 2005). Content analysis has a long history. As long ago as the eighteenth century the method was used in Scandinavia to analyse hymns and sermons (Rosengren 1981). It has long been used in communication, journalism, sociology and psychology. In nursing the method is mostly used in psychiatry, gerontological and public health studies (Elo & Kyngäs 2007). Initially the method dealt with manifest quantitative description of communication but has over the years expanded to include interpretation of latent content (Graneheim & Lundman 2004). The method focuses on human communication and is concerned with meanings, consequences and context, the goal being to provide knowledge and understanding of the phenomena under study (Downe-Wamboldt 1992). The analysis may be performed on a manifest or latent level, where the manifest is a question of the visible or obvious components of a text, while the latent is question of the underlying meaning (Baxter 1991, Downe-Wamboldt 1992, Berg 2004, Krippendorff 2004). Graneheim and Lundman (2004) state that both manifest and latent content analysis are concerned with interpretation but the interpretations vary in depth and level of abstraction.

34
In Studies II and III an inductive latent content analysis was used and the author analysed the interviews separately. The procedure of the analysis started with the reading of the interview transcripts several times to obtain an overall picture. Then the text was sorted into two content areas, i.e. interview text addressing a specific topic (Graneheim & Lundman 2004). In Study II the content areas were (1) experiences of living with diabetes in everyday life and (2) management of diabetes in everyday life. In Study III they were (1) experiences of receiving the diagnosis and (2) beliefs about health. Next, the text in each content area was divided into meaning units, which were pasted up in a table in a Word document. The analysis continued with condensation of the meaning units, preserving the core. Thereafter the condensed meaning units were inductively labelled with codes. Next the codes were compared concerning differences and similarities and abstracted into sub-themes and themes. Finally the credibility of the findings was in Studies II and III confirmed by the co-author/s who performed a co-assessment of the analysis. There followed a discussion between all the authors where subthemes/themes were refined until the most plausible interpretation was attained. To further strengthen the interpreted findings these were also presented and discussed in depth with one of the interpreter and the author (AMW).
Phenomenographic analysis (Study IV) Phenomenography was developed by a research group in the Department of Education at the University of Gothenburg in the 1970s (Marton 1981). It is like phenomenology in that the object of research is in both cases human experience and awareness, but there is a difference of focus. In phenomenology the focus is on essence, on the most invariant meaning, while in phenomenography it is on variation in the world as experienced (Marton 1996, Sjöström & Dahlgren 2002). In phenomenography the aim is to describe the qualitatively different ways in which people experience, perceive, conceptualise and understand various aspects of an phenomena in the world around them (Marton 1986, Marton & Ming Fai 1999). These different ways of understanding are presented in the form of conceptions and descriptive categories (Marton & Yan Pong 2005). Phenomenography makes a distinction between the first-order perspective, which focuses on objective reality, and the second-order perspective, which focuses on how people experience and conceive the world (Marton 1981, Marton & Booth 1997). The phenomeographic approach has been used extensively to investigate learning and teaching, and during the last ten years it has been increasingly used in health and nursing research (Mårtensson 2002, Skärsäter 2002, Holmström et al. 2003, Schröder, 2006). In Study IV the interviews for each participant group were analysed separately. The analysis was carried out in the following phases: (1) The interviews were

35
read several times in their entirety to obtain an overall picture; then in a further reading, statements describing the participants perceptions of the encounter in diabetes-care were identified and labelled in the margin. (2) The different statements were compared and then grouped together on the basis of similarities and differences. In this phase preliminary conceptions were generated and labelled in the margin. (3) The preliminary conceptions were compared with each other and with the statements and were grouped into preliminary descriptive categories. (4) The focus was then shifted from the relations between the conceptions to the relations between the preliminary descriptive categories. To assure that the descriptive categories were in agreement with and represented the conceptions these were scrutinized and the final descriptive categories in each participants group emerged (Marton, et al. 1993, Schröder 2006). (5) To achieve a high degree of trustworthiness, the third researcher (GA), experienced in phenomenographic analysis, scrutinized each step of the analysis. The results were then discussed by this researcher and the author (AMW) until consensus was achieved.
Ethical considerations The empirical studies (II-IV) were approved by a Regional Ethical Review Board in Sweden. These studies have been guided by the four basic ethical principles: autonomy, beneficence, non-malfeasance and justice (Northern Nurses´ Federation 2003, World Medical Association 2004). During the whole research process reflections on the principles of beneficence and non-malfeasance have been central. When a researcher from the majority population studies a minority group, there is a risk of unconscious affronts to the participants through the neglect of culture-specific norms (Hjern 1995). To avoid this the author sought advice from a culturally competent standby person as well as one of the interpreters. Suspecting that the participants might be vulnerable through having been victims of violence and acts of cruelty, the researchers (AMW, GA) took the decision, on a research-ethical basis, not to ask more than was absolutely necessary for the study. Participants might find unmotivated questions invasive and upsetting. Autonomy was achieved in that all the participants were given written and oral information (in Somali to the participant of Somalian origin) about the aim of the research project, voluntary participation and the right to terminate the participation at any time without explanation. Confidentiality was guaranteed and the transcribed interviews have no personal identification. The participants gave their informed consent. To show respect for the principle of non-malfeasance no request for written informed consent was asked for - because in more collectivized cultures like the Somalian, trust and good faith depend one’s

36
word rather than one’s signature (Marshall & Rossman 2006). The participants had no direct benefit of this research but had indirect benefit in that the results provide health-care professionals with increased knowledge concerning those who are culturally different, the aim being to ensure high-quality health care for all. The local-government interpreters involved in the research are under an obligation to follow the Official Secrets Act and have the same professional code of secrecy as persons working in health care. This and other ethical guidelines constitute what the Legal, Financial and Administrative Services Agency as ´Good interpreting practice` (Legal, Financial and Administrative Services Agency 2004, Niska 2004).
Summary of the findings
The main findings of each of the four studies involved in the thesis are presented in this section. More detailed findings are available in each paper (I-IV).
The interpreter’s role as described in qualitative cross-cultural interview studies (Study I) In almost all of the reviewed studies, the involvement of an interpreter was reported in the method section, and the number of interpreters varied from one to five. In four studies it was made clear that some but not all of the interviews were performed with the aid of an interpreter. The most common form to describing the interpreter’s background was with respect to gender and culture. Only in one study was the style of interpreting clearly described, and the seating arrangement during the interviews was not described in any of the studies. In more than half of the studies nothing was said about the interpreter’s previous experience of interpreting. However, in most of the studies there was direct or indirect information about the interpreter’s knowledge of the aim of the research or participation in the transcription of the text or data analysis. In nearly all the studies the researchers attempted to render the interpreter(s)

37
invisible in the research process. The most frequent techniques used to established trustworthiness were prolonged engagement (devoting enough time to learn about the culture and building a relationship of trust with the ethnic group in question) and member checks.
Experiences of everyday life and managing diabetes-related problems (Study II) The findings concerning the patients´ experiences of everyday living and how they manage diabetes-related problems produced four themes and 11 subthemes (Table 3). Table 3. The participants’ experiences and management of everyday life.
Themes Sub-themesExperiences of distress in everyday life
Physical deterioration has changed thingsGiving up activities and habits Need for strict everyday management Difficulty in managing everyday life
Everyday life continues as before
Maintaining religious practicesNot feeling ill
Comprehensibility giving a feeling of control
Becoming acquainted with warning signs from the body and coping with them Permitted to restrain from fasting during Ramadan
Being compliant Must do as they sayDifficulty of doing as they say Being dependent on others
A prominent problem for the participants was to give up traditional eating habits. They also felt restricted by having to test blood sugar levels, keep to a prescribed diet and take medicine at set times. Their everyday life was filled with worries, chiefly regarding high blood sugar levels but there was also a fear of dying from the complications of diabetes. Difficulty in managing everyday life was mentioned especially among women in connection with the need to keep to a strict diet, because of a lack of understanding on the part of family and friends (Table 3. Experiences of distress in everyday life). The participants had different opinions about celebrating Ramadan, the fasting month. One opinion was that the disease did not provide any hindrance to it, and those who held this opinion continued to fast and maintained that fasting and drugs could be combined (Table 3. Everyday life continues as before). Another opinion expressed by the participants was that they were permitted to restrain from

38
fasting because it was not compulsory for someone who has an disease (Table 3. Comprehensibility giving a feeling of control). Following the advice of health-care professionals and changing one’s lifestyle was considered hard work. The participants mentioned a number of barriers to changes in lifestyle, chiefly when it came to eating habits (poor financial situation, prescribed diet with no taste to it, effort required to give up traditional food and follow the ‘plate model’) but also with respect to physical exercise (cold climate in winter discouraging going for a walk) (Table 3. Being compliant).
Experiences of receiving the diagnosis and health beliefs (Study III)
Experiences of receiving the diagnosis Several of the participants indicated that they had had symptoms for several years before receiving the diagnosis, but few had suspected diabetes. Most of the experiences of receiving the diagnosis consisted of ways of managing this information. Above all among women there was acceptance of what is fated, and these participants used religious terms when speaking of their experiences to the diagnosis. Commonly mentioned by the participants, irrespective of gender, was a attempt to find some advantages, for instance that diabetes is a well-known disease which can be treated with medicine. There was also positive comparison, such as that T2DM is not as dangerous as T1DM. Other participants tried to repress the diagnosis and doubted it – something that is treated only with diet, not with drugs, cannot be a real disease.
Beliefs about health The participants explained their health beliefs in several ways. Health was explained, irrespective of gender as absence of disease. Health and disease were opposite poles and could not exist at the same time. Health was also associated with a properly functioning body. The women spoke in terms of the body’s having to function and be active, the men spoke in terms of being free from pain. There were both women and men who saw health as a state of general well-being, involving being happy and carefree, being respected and not being in conflict with other people. The women spoke also of independence and the ability to do housekeeping, while the men spoke of the ability to go to work. It was also said – more often by women than by men – that health was fated by a higher power. Common used terms for illustrate this were “God gives health” and “Health always comes from above”.

39
Encounters between patients of Somalian origin and health-care professionals (Study IV) The analysis of the interviews with the patients and health-care professionals in respect of the encounter in diabetes care gave rise to three descriptive categories for the patients conceptions and two for the health-care professionals (Table 4). Table 4. Descriptive categories of the encounter in diabetes care Patients Health-care professionals
Confidence in the care Skilful teaching Successful self-care Cultural challenges in diabetic care Care not culturally adapted
The patients´ conceptions The patients conceived the health-care professionals as competent, sensitive, always accommodating and helpful and communicated in an understandably way. They conceived the care as being characterized by a close relationship between themselves and the health-care professionals. They experienced carefully performed medical examination, treatment and education in self-care. They conceived themselves supported by the individual care they received. Further, they conceived that the regular follow-ups gave confidence and security, and to have access to an interpreter. They experienced that the health care system in the new country was well-organized and that the care was of high quality, all the more so in comparison with that to be found in their country of origin (Table 4. Confidence in the care). They received advice about diet, exercise and about management of medication and blood sugar control and conceived it important to follow these advice (Table 4. Successful self-care). The participants conceived limitations with the care too. They conceived unmet needs such as too long waiting times for appointments, lack of contact with a specialist and not encountering the same physician. They also conceived that the dietary advice they had received from the diabetic team was not culturally adapted (Table 4. Care not culturally adapted).
The health-care professionals´ conceptions Health-care professionals conceived that skilful teaching in the case of people from Somalia implied the same process as in the case of patients with diabetes

40
in general. They started by building up a confiding relation with the patient and conceived the education as a step-by-step process beginning with identification of an inappropriate life-style and then giving advice how to change unsuitable habits. In their teaching they used different tools such as pictures and the “plate model”. Motivation, support, and encouragement were conceived as being central aspects of their teaching of self-care to the patients. The health-care professionals conceived the communication of information about self-care as being facilitated by getting relatives involved, because these people could not only help the patients to understand the information but also enhance the patients´ motivation with regard to self-care. They also conceived that Somalian patients with diabetes, as compared to Swedish born ones, needed more knowledge about severe diabetic complications and overweight and high blood pressure as risk factors (Table 4. Skilful teaching). The health-care professionals also conceived cultural challenges in their encounter with the patients, such as language barriers, illiteracy and different traditions such as fasting during Ramadan. They involved an interpreter in their communication with the patients, which was conceived as a limitation because of their lack of direct contact with the patients. When it came to illiterate patients they conceived a need to improvise. They also conceived that they needed more comprehensive knowledge of Somalian food so they could give culturally adapted advice (Table 4. Cultural challenges in diabetic care).

Discussion
Reflections of the findings Living with diabetes meant a lack of freedom but also worries about the future. Changing one’s lifestyle was hard work and involved overcoming barriers. The findings in this thesis confirm the findings of previous research to the effect that the encounter between patients and health-care professionals is central in the diabetes care (Gåfvel & Lithner 1996, Esposito 2005). In a cross-cultural encounter communication is a main aspect of the interaction between health-care professionals and patient, the aim being to ensure that the care is safe and of high quality. If the diabetic patient is living in a new cultural environment there is most often a language barrier when it comes to the encounter with health-care professionals. On the other hand, studies have shown that difficulties in communication can exists even when patients and health-care professionals share a common language (Wiman & Wikblad 2004, Efraimsson et al. 2006). But the situation is more problematic when there is a triad consultation where an interpreter is involved - or, worse when an interpreter is not involved despite being required (Björk Brämberg 2008). The findings are discussed with reference to three aspects generated from the main findings and related to encounters: language, habits/tradition and health beliefs (Figure 2).
Habits and traditions
Encounter Health beliefs
Language
Figure 2. Aspects of importance for cross-cultural encounters
41

42
Language The patients did not mention any language problems in connection with their encounter with health-care professionals. They appreciated having access to an interpreter, which health-care professionals conceived necessary for providing information in a comprehensible way (Study IV). This finding differs from that of a Norwegian study where interpreters were seldom used in the consultation between health-care professionals and Pakistani-born persons with T2DM (Fagerli et al. 2005b), also from that of a study involving English-speaking district nurses and South Asian patients (Gerrish 2001). In Sweden, immigrants are legally entitled to be assisted by an interpreter, free of charge, in their contact with authorities (Niska 2004). The interpreter is booked in advance by the health-care professionals and the interpreter is usually unknown to the patient (Fatahi et al. 2005). The interpreter’s role is to be a neutral creator of a bridge to understanding and to balance support between patients and health-care professionals (Fatahi et al. 2008). Use of an interpreter means that the patient and the health-care professional have no direct contact with each other, which was conceived as a limitation by the health-care professionals (Study IV). Sometimes the health-care professionals were uncertain as to whether all the information had been communicated to the patients (Study IV). Not trusting interpreters to transmit intended messages accurately has been found before (Lee et al. 2005, Abbe et al. 2006, Rosenberg et al. 2008). However, when a consultation involves an interpreter it is the health-care professional’s duty to make sure that all the information has been translated correctly. To prevent incorrect interpretation and misunderstanding, health-care professionals should speak in short and clear sentences, pausing to check on patients´ understanding and asking them to repeat back (Glasser 1983, Phelan & Parkman 1995, Green et al. 2005). To communicate through an interpreter was conceived as demanding because it was time-consuming and concentration was needed all the time (Study IV). The time factor has been emphasized in an English and a Swedish study where an interpreter was involved (Greenhalgh et al. 2006, Fatahi et al. 2008). When interpreters were asked about problems they encounter they indicated lack of time as an important obstacle to an effective contact between patients and health-care professionals (Fatahi et al. 2005, Greenhalgh et al. 2006). In a triad encounter more time is needed simply because three people are involved instead of two, and the cultural distance between the patients and health-care professionals increase the need for more time. Not having sufficient time affects the quality of care provided for immigrant patients (Fatahi et al. 2005). Both advantages and disadvantages were experienced when it came to using relatives as interpreters (Study IV). It was conceived as an advantage to use

43
relatives as interpreters when they were more skilled in Swedish than the professional interpreter. On the other hand relatives could be regarded as not being neutral and as neglecting to translate all that the health-care professionals said (Study IV). This is in agreement with the findings of several other studies where family interpreters have been perceived as selective and less accurate in their information-giving than professional interpreters (Murphy & Clark 1993, Ekblad et al. 2000, Rosenberg et al. 2008). Communication is central to ensuring a safe, patient-centered and equitable care and therefore a high-quality interpreter service is crucial (Green et al. 2005). A review showed that optimal communication, patient satisfaction and very few interpreter errors occur when patients have encountered trained professional interpreters or bilingual health-care professionals (Flores 2005). Other studies have reported that when trained interpreters are involved in the encounter in health care the quality of interpretation is significantly higher than when the interpreting is done by relatives or by staff with no interpretation training (Hornberger et al. 1996, Bischoff et al. 2003). In addition, when patients have a choice, they choose professional interpreters rather than relatives (Ngo-Metzger et al. 2003). To sum up. The patients with diabetes of Somalian origin conceived no language barrier in the encounter with health-care professionals – they appreciated having access to an interpreter. The health-care professionals conceived communicating through an interpreter necessary but time-consuming, and the interpreter stood in the way of direct contact with the patient. Sometimes the staff conceived uncertainty whether all the information had been communicated and made understandable to the patients. Both advantages and disadvantages were conceived to use of relatives as interpreters. It was conceived as an advantage to use a relative if he or she was skilled in the language, but a disadvantage was that relatives were not neutral and were selective in their translation.
Habits and traditions Living with diabetes require lifestyle chances which participants regarded as hard work. Obstacles to changes in food habits were dietary advice not culturally adapted, difficulty of giving up traditional food, tastelessness of the prescribed diet and poor financial situation (Studies II, IV). This is in accordance with what other researchers have found when investigating dietary intake and barriers to dietary adherence among T2DM patients (El-Kebbi et al. 1996; Nthangeni et al. 2002). An English study on West Indian persons with diabetes and a Norwegian one on Pakistani-born persons with diabetes showed that traditional food habits were not sufficiently taken into consideration in advice on diabetes management (Scott 1998, Fagerli et al. 2005b). In a study

44
among African American the general perception was that `eating healthfully´ meant giving up part of their cultural heritage and trying to conform to the dominant culture. The participants also spoke the poor taste of ´healthy´ food and of the expenses to buying such food (James 2004). Making dietary adjustments, can be difficult when support is lacking from people around. In Study II, especially women described difficulties in adhering to the prescribed diet when support and understanding from family and friends was lacking. Similar results have been found in earlier studies (El-Kibbi et al. 1996, Dye et al. 2003) and specifically among women (Samuel-Hodge et al. 2000). Wives were involved in the consultation with married men because it was likely that they did the cooking (Study IV). The findings of this thesis indicate that it is important to involve husbands of women patients so that they become aware of the importance of adherence to the prescribed diet and will offer support. It has previously been shown that patients with a high level of family support for diet self-care have reported fewer barriers to following the diet regime (Wen et al. 2004). If patients are to have a good chance of adhering to dietary advice it must be culturally adapted. The health-care professionals conceived that they tried to accomplish such adaptation but really needed more knowledge of Somalian food for this purpose (Study IV). Many health-care professionals see the failure to follow diet advice as a simple failure of patients´ will-power or an unwillingness to change behavioural patterns (Vijan et al. 2004). Instead, it probably has to do with advice’s not being culturally appropriate (Nthangeni et al. 2002), and indeed the Somalian patients in Studies II and IV revealed that they were uncertain about what they could eat of their traditional food. If health-care professionals are to be able to give culturally adapted dietary advice to their immigrant patients they must have knowledge about food combination patterns in different cultures and the process of adaptation to a new food patterns. Kocturk-Runefors (1991) has developed a model for food combination patterns, involving a distinction between staple foods, (e.g. potato, rise, bread, etc.), complementary foods (meat, fish, vegetable, milk, cheese, eggs, legumes etc.) and accessory foods (fats, herbs, spices, sweets nuts, fruits, drinks). The staple and complementary foods are designated basic foods. It is these foods that people first think of when asked what they eat. The main culinary role of the accessory foods is to enhance the taste and presentation of the basic foods. Adaptations to a new dietary pattern proceed in a continuum where identity and taste form the two extreme poles. When new foods are incorporated into the diet the taste aspect is given priority. The change begins with accessory foods, which includes the sweetest and fattiest food of a culture and the level of

45
cultural prejudice is low because they are not considered real foods. The higher up we go in the hierarchy of foods, the greater our attachment. It takes a long time to incorporate new basic foods into the diet because the cultural identification with these foods is stronger (Kocturk-Runefors 1991). This is something health-care professionals need to know so that they can give dietary advice better adapted to patients´ cultural backgrounds. The model can be used to better understand the complexity to adapt new dietary patterns. For the patients involved in the present thesis it was importance to celebrating Ramadan and they did not see their diabetes as a problem in this respect, but health-care professionals conceived it as a problem (Studies II, IV). This goes against the findings of a study where the majority of Arabic females considered Ramadan as less important in Sweden because of the disruption of the extended family or kin group (Hjelm et al. 2003). However, one reason to maintain this tradition can be that the fasting preserves one’s identity and contributes to the consolidation of the feeling of togetherness within the ethnic group in a new country (Jonsson et al. 2002). In the case of the present thesis there was a variation in how the fasting month was managed. Those who did not fast indicated that a person who is a Muslim and has a disease is exempt from fasting (Study II). This was the position of the women, and they considered that fasting also took away a lot of energy – and being without food for so many hours was not good for a person with diabetes. Men’s decision to fast or not depended upon when Ramadan occurs (Study II). Since Ramadan is lunar-based its occurs eleven days earlier from year to year (Benaji et al. 2006). Thereby the duration of the daily fast varies from a few up to 18 hours a day (Aadil et al. 2004, Al-Arouj et al. 2005, Benaji et al. 2006). Those who were fasting changed the timing for their drug intake during Ramadan but they received no information from the health-care professionals about how to manage this and no follow-ups during the fasting period (Studies II, IV). For their part, the health-care professionals were given divergent advice as to how they should handle the patient’s habit of fasting during Ramadan. There is no agreement among researchers as to whether it is safe or not for a person with DM to fast (Barber et al. 1979, Davidson 1979, Sulmani et al. 1988, Salti et al. 2004, Al-Arouj et al. 2005, Benaji et al. 2005, Elhadd & Al-Amoudi 2006). Therefore it is the duty of health-care professionals to prepare patients for it but also inform both the patients and their families that fasting most of time is risky (Benaji et al. 2005). However, Al-Arouj and co-workers (2005) have made some recommendations for fasting for Muslim diabetes patients. Supporting these recommendations are an expert panel of diabetologists from several Muslims countries. It is recommended that a patient should not decide to fast without considering the possible risk involved and thoroughly discussing it with his or her doctor. If patients insist on fasting they

46
should undergo pre-Ramadan assessment and receive both education and instructions related to physical activity, meal planning, blood glucose monitoring and dosage and timing of medications. Follow-ups during the fasting period are recommended as reducing the risk of complications (Al-Arouj et al. 2005). This shows the need of evidence-based guidelines in diabetes care for immigrants in Sweden about fasting during Ramadan, in order to prevent complications and promote relevant self-care. When it comes to the key habit physical activities in living with diabetes, it emerged that the participants tried to follow the advice of daily exercise but mentioned the cold climate in the winter as preventing going for walks (Study II). However, the health-care professionals conceived the willingness among diabetes patients of Somalian origin to take exercise as being less than among Swedish-born diabetes patients. The patients’ low motivation for physical activities during the winter puts pressure on the health-care professionals to find alternative activities. Furthermore, the health-care professionals conceived that there were sometimes limitations in communication regarding the need of a changed life-style, in particular concerning older patients and the need for more walking (Study IV). When patients are struggling to make both dietary and physical chances the health-care professionals should encouraged them to put physical activity first since this generates a sense of well-being and motivation to self-manage (Malpass et al. 2008). To sum up. Changing lifestyle was regarded by the patients as a difficult task - especially to changing food habits, because the advice they received was not culturally adapted. Health-care professionals conceived that they tried to give advice adapted to the patients´ culture but needed to know more about Somalian food to be able to give the best advice. The patients found it difficult to follow the advice when support from the family was lacking. To give the patients more change of changing their diet there is a need for the health-care professional to understand food combination patterns in different cultures and the process of adaptation to new food patterns. The model which Kockturk-Runefors (1991) has developed can be a tool for health-care professionals to understand the complex process of such adaptation. To maintain fasting during Ramadan was important, and those who fasted did not see their diabetes as a problem in this respect –but health-care professionals conceived it as a problem. The patients received no instructions about dosage and timing of medications and no appointments for follow-ups during the fasting period. Going by the findings of this thesis there would seem to be a need to develop recommendations for patients with diabetes who fast in Sweden.

47
Health beliefs In Study III the participants described health mostly in terms of individual factors as proposed by Helman (2001). It was explained from a pathogenic perspective as absence of disease, as having a well-functioning body or no bodily pain. Having good health was the most important thing in life (Study III). These findings are consistent with those of previous Swedish studies concerning women and men born in Arabic counties, former Yugoslavia and Sweden (Hjelm et al. 2003, 2005). Also in a Canadian study both health-care professionals and patients described health in terms of individual factors such as being emotionally and physically well (McKague & Verhoef 2003). The patients contributing to this thesis also described health in terms of general well-being. It was very much a question of being independent - living in one’s own flat, being able to do the housework, being able to work. Having good habits and sleeping well were also associated with health (Study III). Similar findings were found in McKague and Verhoef´s study (2003): health was described in terms of an ability to function at a variety of levels, including sleeping and eating well and going to work. Having the ability to go to work and to take care of the household were also the most frequently cited attributes of health among a British Greek population (Papadopoulos 2000). Health was besides individual factors also attributed to social factors such as being respected and not being in conflict with other people (Study III). These findings correspond with those of three Swedish studies where first European and then European and non-European cultural differences in beliefs about health and illness were investigated (Hjelm et al. 1999, 2003, 2005). Supernatural factors were also mentioned in connection with health. It was more common among women than men to mention such factors. Common statements were of the type “Health always comes from above” and “God gives health”, but there were also statements to the effect that God can take it back again too. Health and illness depended on God’s will (Study III). In addition, comparable findings have been reported in an ethnographic study on both sexes concerning ten elderly older Arabian Gulf Muslims. In that study the participants indicated that health and illness come from Allah (Ypinazar & Margolis 2006). Also in a study among Kashmiri men with diabetes in Leeds Naeem (2003) found that many of them believed that having diabetes was “Allah’s will”. Thus health was mostly believed to be dependent on individual factors such as having a well-functioning body, having good habits, being independent and having the ability to work. To some degree health was also believed to be dependent on social and supernatural factors. It has been suggested by Helman (2001) that social and supernatural factors are more prominent in the case of

48
people from non-Western countries, but such was not the case when it came to the Somalian participants referred to in this thesis. Perhaps they have incorporated Westerns beliefs since they are exposed to Western culture every day.
Methodological considerations There are special ethical and methodological issues that have to be considered when interviewing people in a vulnerable situation such as people with a chronic disease (Davies et al. 1998), not least if there is a language barrier (Edwards 1998, Temple & Young 2004, Squires 2008). The patients participating in the present research exhibited varying degrees of difficulty in expressing themselves in Swedish but they still chose to take part and share their experiences. Giving these persons a voice can be viewed as particularly important from a research- ethical and methodological standpoint. Immigrants not fluent in the majority language are seldom included in qualitative research, possibly because they do not fit into the traditional interviewee profile, are not articulate and reflective because of language difficulties (Esposito 2001). Though it is a limitation that the interviews with the participants of Somalian origin had to be performed with the aid of an interpreter, it did give these people the opportunity to express themselves in their first language, whereby they probably felt more confident when being interviewed. As Berg (2004) reminds us, the language must of course be understandable to the persons who are interviewed – which means that this thesis could not have been accomplished without the aid of an interpreter. To minimize the threats to credibility involved in using interpreter (Kapborg & Beterö 2002) the interviewer met the interpreters before the interviews in advance to discuss the aim of the study, research questions and their role during the interviews. Further, in Studies II-IV there is a detailed description of the interpreter’s part in the interviews. The interviews with the participants of Somalian origin (Studies II-IV) were transcribed and analysed only in Swedish, which also could have influenced credibility. On the other hand in a study where both Chinese and English languages were involved the author found that no significant differences in the data analysis (Twinn 1997). Another way to minimize the risk of bias due to the interviewing procedure with an interpreter, the research started with a method study in order to review the knowledge in this area (Study I). The Matrix Method was used to analyse the studies involved in the review, this method being conductive to a systematic and trustworthy analysis (Garrard 1999, 2007). Certain decisions based on the methodological literature (Study I) were made before the start of

49
the interviews, and they are described thoroughly in the respectively qualitative interview studies (Studies II-IV). In Study I credibility was strengthened by means of the specific criteria concerning which studies were to be included in the review. The literature search strategy and the analysis of the studies were conducted by the same author (AMW) but when hesitation arose in the analysis the second author (GA) was consulted. Despite well-prepared interviews there were two participants of Somalian origin that did not want an interpreter, instead their wife/husband translated when necessary – and this may have influenced the trustworthiness of the studies (Twinn 1997). In addition, written notes were taken in the case of two interviews because the interviewees did not want to be tape-recorded. This could have interfered with listening attentively (Patton 2002). However, during these interviews the interviewer checked repeatedly with the interviewees to confirm what was said. After the interviews the written notes were also followed up with the interpreter. For ethical reasons it was left to the patient to decide where the interview should take place. Eleven patients chose to be interviewed in their own home, five in secluded public places, one at a primary health care centre and one at the interviewer’s workplace. Whether this had an influence on the findings was not specifically studied. It is probable that being able to choose where the interview was to be meant that the participants felt confident and comfortable. In Study IV only five health-care professionals were interviewed, this being the number who met the inclusion criteria. Though more subjects may well have generated a greater variety of perceptions, the existent material is rich. The participants’ unique stories provided vivid descriptions. Therefore this study has an important place in enhancing the understanding of the encounters between the patients and health-care professionals. A limitation is that the participants of Somlian origin were interviewed only once. The decision to stop at just one interview per participant was based on the fact that it is not uncommon that refugees are unwilling to participate in research studies (Samarsinghe & Arvidsson 2002). However, an additional interview would have offered the chance of obtaining more expanded information (Patton 2002). The selection was of all eligible patients with diabetes from well-defined geographical areas rather a long distance from each other, and it was judged that this sample was sufficient to achieve transferability to other immigrants from Somalia.

50
In the qualitative studies (Studies II-IV) an effort was made to ensure trustworthiness by providing thorough descriptions of data and procedures. The data and procedures were furthermore constantly scrutinized and supervised by an experienced senior researcher. In Study II and III the interviews were subjected to latent content analysis. This method was chosen because it is appropriate both when research findings on a phenomenon are limited (Hsieh & Shannon 2005) and when one is looking for cultural patterns and beliefs (Downe-Wambolt 1992). In Study IV a phenomenographic analysis was chosen since it identifies both similarities and differences, which were under study with regard to how the patients of Somalian origin and the health-care professionals perceived the patient-professional encounter in Swedish diabetes care (Marton 1981, 1986). A basic assumption of the method is that what a group of persons think or understand about a particular phenomenon may vary among them (Wenestam 2000). The foremost strength in this thesis is that immigrants from a non-European country have spoken about their experiences of living with a chronic disease in a new cultural environment and about how they perceive the care they have received. Another strength is that the interviewer had the requisite experience and knowledge to meet immigrant patients as a district nurse in multicultural settings and to make best use of an interpreter. The participants were given sufficient time during the interviews, as well as afterwards, so that any obscurities could be sorted out. Trust and feeling able to speak about their view and experiences concerning living with diabetes were important as the data in the qualitative studies are based on communication with the participants. The interviewer’s pre-understanding as a district nurse in multicultural settings and accustomed to working with interpreters may have influenced the findings both positively and negatively. On the positive side, the interviewer had extensive experiences of communicating through an interpreter. What the interviewer wanted to avoid, however, was that the participants should see the interviewer as a nurse instead as a neutral interviewer and say what they thought the “nurse” interviewer wanted to hear, i.e. give socially desirable answers. As the researcher is the instrument in qualitative inquiry, the researcher credibility is important (Patton 1990, 2002). The researcher’s knowledge of and experience of contact with persons from Somalia made it possible to gain confidence among the study groups. This experience also made it easier to formulate appropriate follow-up questions in the interviews. To further strengthen the credibility of the findings in Studies II and III an in-depth discussion was conducted with one of the interpreters who understands the culture of the participants (Edwards 1998, Tsai et al. 2004). This strategy is recommended when member check cannot be conducted (Adamson &

51
Donovan 2002). There was no dependent relationship between interviewer and participants which could have influenced credibility. Dependability of qualitative data has to do with stability over time (Polit & Beck 2004). In Study I the same search terms were used in the six electronic databases and the search included all the years each database covered at that time (October to November 2004). The studies involved in the review (Study I) were analyzed using the same topics. The same interview guide was used in Studies II-IV for all participants, which means that the same main questions were put to the participants. Further, the interviews in these studies were conducted by the same interviewer. It was an extra advantage to have the same interviewer for both patients and staff as it made it easier to discover differences and similarities between them in Study IV. The fact that more than one interpreter was involved may have resulted in somewhat different interpretations, which could have influenced the dependability of the findings. Transferability has to do with the extent to which the findings can be transferred to other settings or groups (Graneheim & Lundman 2004, Polit & Beck 2004). The findings of Study I can be transferred to other settings or groups where qualitative interview studies are conducted with participants who do not speak the majority language. Whether or not the findings of Studies II-IV can be transferred to other settings or groups is difficult to know. Lincoln & Guba (1985 p 316 ) state that the researcher can only provide the thick description necessary to enable someone interested in making a transfer to reach a conclusion about whether transfer can be contemplated or not. However, the findings in Studies II-IV may be transferred to Somalis with diabetes in the same age range and health-care professionals who live and work in another setting in Sweden. The fact that all health-care professionals were women limits the possibility of transferring the findings to other groups of health-care professionals including men.
Conclusions and implications
The findings in this thesis provide knowledge about how patients of Somalian origin and health-care professionals experienced the encounter in diabetes care as well as about the patients’ health beliefs, experiences of the diagnosis and of everyday life with diabetes (Studies II-IV). Knowledge about to work with an interpreter in research has also been highlighted (Study I).

52
One conclusion drawn from this thesis is that the patients did not conceive any barrier with regard to language, instead they appreciated the interpreter service. The health-care professionals conceived communication through an interpreter as indispensable but also time-consuming, and it was restrictive in that it mean that the patient and the health-care professional were not in direct contact with each other (Study IV). Changing lifestyle was hard work for the patients, particularly when it came to changes in food habits since the dietary advice they received from the health-care professionals was not culturally adapted (Studies II, IV). It was also difficult to follow the dietary advice without family support (Study II). The health-care professionals conceived that they tried to adapt their food advice to the patients´ culture but conceived that they needed more knowledge about Somalian food (Study IV). The patients had different opinion about fasting during Ramadan. Those who fasted maintained that fasting and drugs could be combined; in contrast with the health-care professionals, they conceived it as a problem (Studies II, IV). Others indicated that they were permitted to restrain from fasting since fasting was not compulsory for someone with a disease (Study II). The patients’ health beliefs were mostly described in terms of individual factors such as having a well-functioning body and no disease. To some degree the health beliefs was also defined in terms of social factors such as being respected and not being in conflict with other people (Study III). The knowledge gained from this thesis can be useful in the continuing effort to improve the quality of care adapted to different cultural settings. The following are the main implications:
• Knowledge about working with an interpreter should be a part of all education for health-care professionals and in research schools.
• There is a need of more culturally appropriate dietary advice in
education for health-care professionals working in diabetes care. The model set forth by Kockturk-Runefors (1991) can be a tool for understanding the complex process of adaptation to new food patterns.
• It is of great importance that family become involved in the encounter
in diabetes care to be able to offer support to the patient in adherence to the advice of new and changed habits in everyday life.
• Evidence-based guidelines in diabetes care for immigrants who insist
on fasting during Ramadan, are needed in order to prevent complications and promote relevant self-care.

53
• The health-care professionals need knowledge and understanding of immigrants´ health and illness beliefs to ensure optimum quality of care for diabetes patients.
• There is a need of research in order to acquire knowledge of the interpreters´ experiences and conditions in the interpreter service.

54
Svensk sammanfattning
Bakgrund
Under och efter andra världskriget blev Sverige ett invandrarland istället för ett utvandrarland. Under efterkrigstiden bestod invandringen av arbetskraftsinvandring för att efter år 1967 ersättas av asyl- och flyktinginvandring inklusive deras anhöriga. Denna förändring grundades i att invandringsreglerna av arbetsmarknadsskäl skärptes för utomnordiska medborgare. Den invandring som förekommit till Sverige under de senaste 50 åren har medfört att det svenska samhället idag är ett mångkulturellt samhälle med över hundra etniska grupper med olika bakgrunder, språk och religioner. En av dessa etniska grupper är somalier som kom till Sverige i början av 1990-talet i samband med inbördeskriget i Somalia. Antalet somalier i Sverige är lite mer än 21000 och drygt 8200 av dessa har svenskt medborgarskap. Somalier är en ung invandrargrupp, 54 procent är under 30 år och 19 procent är över 40 år samt endast 0.1 procent är 65 år och äldre. Diabetes Mellitus (DM) utgör ett växande globalt hälsoproblem. Mer än 180 millioner människor runt om i världen är drabbade och antalet beräknas att vara fördubblat till år 2030. De som löper den största risken att drabbas av diabetes är befolkningar i utvecklingsländer, minoritetsgrupper och fattiga i industriländer. Diabetes indelas i två huvudformer, typ 1 diabetes och typ 2 diabetes. Typ 1 diabetes drabbar vanligtvis personer under 30 år medan typ 2 diabetes drabbar oftast personer över 40 år och utgör 85-90 procent av samtliga med diabetes. För att garantera en hög kvalité på vården vid diabetes för alla patienter är det nödvändigt att få kunskap om hur personer, med annan bakgrund än den svenska, upplever att leva med en kronisk sjukdom såsom diabetes. Det är även viktigt att få deras uppfattningar av mötet med svensk diabetesvård i primärvård.

55
Syfte
Det övergripande syftet med avhandlingsarbetet är att generera fördjupade kunskaper om hur personer med somaliskt ursprung och med diabetes lever med sin sjukdom i en för dem ny kultur. Vidare att beskriva hur de uppfattar mötet med den svenska diabetesvården och att beskriva hur vårdpersonal uppfattar mötet med patienter av somaliskt ursprung. Avhandlingens fyra delstudier har följande syften:
1. att granska hur tolkens roll beskrivits i tidigare empiriska kvalitativa intervjustudier samt hur trovärdiga data uppnåtts (Studie 1).
2. att beskriva personer med ursprung från Somalia erfarenheter av att leva med DM och hur de hanterar diabetes relaterade problem. Resultatet analyserades även utifrån ett könsperspektiv (Studie II)
3. att undersöka hur personer med ursprung från Somalia upplevde att få diagnosen diabetes och att beskriva deras hälsouppfattning (Studie III)
4. att beskriva hur patienter med somaliskt ursprung och vårdspersonal uppfattar mötet inom diabetesvården på vårdcentraler (Studie IV).
Metod och deltagare/studier
Avhandlingens design är beskrivande med kvalitativ metod i tre av studierna (Studie II-IV) och en av studierna (Studie I) är en systematisk litteraturstudie (Tabell 1). I den systematiska litteraturstudien (Studie I) inkluderades kvalitativa tvärkulturella intervjustudier med tolk, skrivna på engelska och publicerade i tidskrifter som tillämpar vetenskaplig peer-review granskning. Ett ytterligare kriterium var att ett abstrakt skulle finnas att tillgå för att avgöra huruvida studien uppfyllde de uppsatta kriterierna. I delstudierna II-IV rekryterades deltagarna från sex vårdcentraler i två mellansvenska städer. Inklusionskriterierna för deltagarna med somaliskt ursprung var att de skulle vara somalisktalande vuxna personer (18 år och äldre) och ha haft diagnosen diabetes minst sex månader. Inklusionskriterierna för vårdspersonalen (Studie IV) var distriktssköterska eller distriktsläkare med ansvar för diabetespatienter på vårdcentral som har eller haft kontakt med minst fem somalisktalande diabetespatient. Det sistnämnda för att undvika förutfattade uppfattningar baserade på alltför begränsade erfarenheter.

56
Table 1 Design och metod på de fyra studierna som ingår i avhandlingen Study Design Data collection Data
analysis 1 Systematisk
litteratur-studie
Systematisk litteraturstudie av kvalitativa intervjustudier där tolk används (n = 13)
The Matrix Metod
II DeskriptivKvalitativ
Semi-strukturerade intervju med vuxna personer av somaliskt ursprung med DM typ 2. Vid intervjuerna användes språktolk (n = 19)
Latent innehålls analys
III DeskriptivKvalitativ
Se studie II Latent innehålls analys
IV DeskriptivKvalitativ
Semi-strukturerade intervju med vuxna personer av somaliskt ursprung med DM (samma deltagare som i studie II och III) och vårdspersonal inom diabetesvården (n = 19 personer med diabetes, 5 vårdpersonal)
Fenomeno-grafisk analys
Sammanlagt uppfyllde 39 personer inklusionskriterierna, 33 av dessa var personer med diabetes och sex var vårdpersonal. Av dessa accepterade 19 personer med diabetes (elva kvinnor och åtta män) och fyra distriktssköterskor och en distriktsläkare (alla kvinnor) med ansvar för diabetespatienter att delta i studien. Datainsamlingen för Studie I genomfördes under perioden oktober till november månad 2004 i databaserna Cinahl, Eric, PsycINFO, PubMed, Sociological Abstract och Your Journals @ovid. I Studierna II-IV genomfördes intervjuerna med de somalisk talande deltagarna tillsammans med tolk. Intervjuerna för Studierna II-IV genomfördes på plats som deltagaren själv valt och analyserades med latent innehållsanalys (Studie II, III) och fenomenografi (Studie IV).
Resultat
Resultatet i Studie I visade att tolkens roll var sparsamt beskriven i de 13 inkluderade studierna. Det mest förkommande sättet att beskriva tolken i studierna var att nämna dennes/deras kön och kulturella/nationella bakgrund. I de flesta studierna framgick direkt/indirekt att tolken/tolkarna hade kunskap

57
om syftet med forskningen. Däremot var det inte vanligt att beskriva tolkens placering i förhållande till intervjuaren och den intervjuade och inte heller vilken tolkningsstil som användes. I drygt hälften av studierna fanns ingen information om tolkens tidigare erfarenheter som tolk. Olika tekniker användes för att uppnå tillförlitlighet i studierna. Mest förekommande tekniker var ”prolonged engagement” dvs att forskaren tillbringar tillräckligt lång tid i den kontext där studien genomförs, eller ”member check” eller triangulering antingen genom data, metod eller mellan forskare. I Studie II beskrev patienter med diabetes med somaliskt ursprung sina upplevelser av att leva med diabetes i Sverige och hur de hanterar sjukdomsrelaterade problem. Fem teman framkom i resultatet: ”Upplevda påfrestningar i vardagen”, ”Vardagliga livet fortsätter som förut”, ”Begriplighet ger känsla av kontroll”, och ”Att vara följsam”. Ett huvudfynd var den variation varmed deltagarna hanterade sitt ätande under fastemånaden Ramadan. De deltagare som fastade såg inte diabetessjukdomen som ett hinder för att göra detta medan andra såg den som ett hinder eller angav att fasta inte var obligatorisk för en person med sjukdom. I resultatet framkom såväl likheter som skillnader ur ett könsperspektiv. Kvinnor talade om svårigheter att hantera det dagliga livet när support från familjen saknades, medan män talade om svårigheter att anpassa sig till regelbundna måltider och rutiner. Oavsett kön upplevde deltagarna sig bundna till blodsockerkontroller, dietföreskrifter och till ordinerad medicin. Trots detta försökte deltagarna vara följsamma till de råd och föreskrifter som de erhållit. De nämnde dock svårigheter, framförallt till den föreskrivna maten, som de upplevde som dyr, inte kulturellt anpassad och fattig på smak. I Studie III beskrev patienter med diabetes av somaliskt ursprung sina upplevelser av att få diagnosen samt deras hälsouppfattning. Utifrån deltagarnas berättelser framkom tre teman; ”Existentiella grubblerier”, ”Håller diagnosen ifrån sig”. ”Accepterar det ödesbestämda”, Tre teman framkom även avseende deltagarnas hälsouppfattning. Dessa var: ”Hälsa som frånvaro av sjukdom”, ”Hälsa som allmänt välbefinnande”, och ”Ödesbestämt av högre makt”. Ett av studiens huvudfynd var att kvinnor i förhållande till män framförde en mer övernaturlig hälsouppfattning och även när det gällde upplevelser i relation till att få diagnosen. Hälsa förklarades även som allmänt välbefinnande där kvinnor framförallt talade om att vara oberoende och kunna sköta hushållet medan män talade om förmågan att kunna sköta ett jobb. I Studie IV beskrev patienter med diabetes av somaliskt ursprung och vårdpersonal (diabetessköterskor och distriktsläkare) hur de uppfattade mötet i diabetesvården i primärvården. Både patienterna och vårdpersonalen uppfattade vården som patientcentrerad men patienternas uppfattade även begränsningar

58
med vården. Dessa handlade om allt för långa väntetider för att få träffa vårdpersonal, att inte få träffa samma läkare på vårdcentralen, att inte bli remitterad till specialist samt att de givna kostråden inte var kulturellt anpassade. Tre beskrivningskategorier framkom; ”Har förtroende för vården”, ”Lyckad egenvård”, och ”Vården inte kulturellt anpassad”. I vårdpersonalens uppfattningar om mötet med patienter av somaliskt ursprung framkom två beskrivningskategorier; ”Kompetent undervisning” och ”Kulturella utmaningar i diabetesvården”. I den sistnämnda beskrivningskategorin uppfattade vårdpersonalen språkbarriär, krav på att samtalen måste genomföras med tolk, och traditioner såsom Ramadan. Sammanfattningsvis visar resultatet i denna avhandling att patienterna upplevde svårigheter i att förändra livsstil, framförallt att förändra tidigare matvanorna eftersom deras uppfattning var att kostråden de erhållit inte var kulturellt anpassade (Studie II, IV). De beskrev även svårigheter att följa förskrivna kostråd när support saknades från familjemedlemmarna (Studie II). Hälso- och sjukvårdspersonalens uppfattning var dock att de försökte att anpassa kostråden till patientens kulturella bakgrund men att de behövde ökade kunskaper om somalisk mat/livsmedel (Studie IV). Att fasta under Ramadan var viktigt för en del av patienterna och de upplevde inte sin sjukdom som ett hinder för att genomföra fastan, vilket hälso- och sjukvårdspersonalen uppfattade som ett problem (Studie II, IV). Ingen medicinförändring och inga uppföljningsbesök bokades in för patienterna under fastemånaden (Studie IV). När patienterna beskrev sina upplevelser i samband med diagnosen framkom emotionella känslor i form av chock och rädsla hos dem som inte hade misstänkt att de hade diabetes. Det fanns också de som tvivlade på att diagnosen var korrekt och de som försökte förtränga att de hade diabetes efter beskedet. Den mest framträdande upplevelsen i samband med diagnosbeskedet var dock att acceptera det ödesbestämda. När patienterna beskrev hälsouppfattningar var dessa huvudsakligen relaterade till individuella faktorer såsom att vara frisk utan några sjukdomar och att ha en fungerande kropp (Studie III). Hälso- och sjukvårdspersonalen uppfattade språket som ett hinder i mötet med patienterna och använde tolk, vilket uppfattades som tidskrävande men också som en begränsning eftersom ingen direkt relation med patienterna kunde etableras. Patienterna å andra sidan uttalade inga språkhinder, utan uppskattade istället tillgången till tolkservicen i mötet. Hälso- och sjukvårdspersonalen uppfattning var att det fanns både fördelar och nackdelar att använda anhöriga som tolk. En fördel att använda anhöriga som tolk var när dessa behärskade det svenska språket. Nackdelar var att de inte var neutrala och därmed för selektiva i sin tolkning. Det fanns också en misstro bland hälso- och sjukvårdspersonalen huruvida tolkarna översatte all information till patienterna (Studie IV).

59
Slutsatser
Slutsatser som kan dras från resultatet i denna avhandling är att det finns ett behov av utbildningsinsatser om andra kulturers matvanor/traditioner för hälso- och sjukvårdspersonal som arbetar inom diabetes vården. Här kan Kockturk-Runefors (1991) modell vara ett verktyg för att förstå den komplexa process som det innebär att anpassa sig till nya matvanor. Vidare behöver kunskaper om att arbeta med tolk vara en del i grundutbildning av hälso- och sjukvårdspersonal men även på forskarnivå. Det finns även ett behov av att applicera och tillämpa evidensbaserade riktlinjer i praktiken för att förebygga komplikationer och främja relevant egenvård för patienter som insisterar att fasta under Ramadan. För att säkerställa en optimal vård för diabetes patienter med annan bakgrund än svensk behöver hälso- och sjukvårdspersonal kunskap om och förståelse för patienternas hälso- och sjukdomsuppfattning. Det är av stor betydelse att involvera anhöriga i diabetesvården så att de kan ge patienten det stöd som denne behöver för att kunna vara följsam till nya och förändrade vanor i vardagen.

60
Acknowledgements
I would like to express my deep gratitude to the people who have inspired, supported and guided me during the composition of this thesis. In particular, I would like to thank the following: First of all, the persons of Somalian origin with diabetes and the health-care professionals who participated in the studies and openly and generously shared their experiences with me, as also the interpreters for their invaluable assistance. Without you, this thesis would not exist. Professor Gerd Ahlström, my main supervisor, for having faith in me and my work and for providing never-ending encouragement and support, including guidance in research methods and constructive criticism. You were always there for me. Professor Birgitta Sidenvall, my co-supervisor during the later phase of my studies, for constructive criticism, revisions of my English, encouraging support and kindness. Associate Professor Monica Löfvander, my co-author in one of the studies, for constructive advice and kindness. Professor Peter Engfeldt, for support and the introduction of my research at primary health care centres in the two towns where the studies in this thesis were performed. Professor Bengt Fridlund, for scrutinizing my work at the final seminars. Thank you for your constructive and valuable comments. All my fellow PhD students at the School of Health Sciences, Jönköping University. Particular thanks and warm hugs to Marit Silén, Mari Golsäter and Linda Johansson, for both serious discussion and many a good laugh during these years together. You made me think and you helped me relax. I wish you all continued success with your studies and I do hope our friendship will continue.

61
Sally Hultsjö, for your friendship and for all the lunches together where we discussed Life. I wish you all continued success with both your life and your studies and I do hope that we can continue our friendship despite many miles between us in the future.
The staff at the School of Health Sciences. I would especially like to thank Ingrid Widäng, my contact person, for practical help and friendship, and Siv Honkala for friendship during my years in Jönköping. I do hope our friendship will be lasting despite the fact that I am now leaving Jönköping. Malcolm Forbes, for eminent revisions of my English. It has been like Christmas to read your comments. The staff at Jönköping University Library, Örebro University Library and the Medical Library, Örebro University Hospital, for fine service. Thomas Falck, my manager at the Department of Community Medicine and Public Health in Örebro, who gave me leaves so that I could fulfil my research. Evelina and Amanda, my neighbour’s lovely children, who have always been there with comments and laughter. I promise that from now on you will have your “grandmother” back again in your lives. All my friends — none mentioned, none forgotten — who have accepted that I have not been very social during my years of study. I promise that there will be improvement in the future. My father and mother, Gunnar and Christina; my sisters, Iren and Margaretha, and my brothers, Lars-Gunnar and Bertil, with their families, for always being there with love and not letting me ignore the “real” world. Finally, the most important persons in my life: my beloved husband, Johnny, for all the love, support and understanding despite a lot of problems related to hard work and separation during the weekdays over the last two years; and my wonderful son and daughter-in-law, Mattias and Hanna, for always believing in me and for your tolerance with me during these years. For financial support, I want to thank the School of Health Sciences, Jönköping University, the Research Committee of Örebro County Council and the Department of Community Medicine and Public Health, Örebro County Council.

62
REFERENCES
Aadil, N., Houti, IE. & Moussamih, S. (2004) Drug intake during Ramadan. British Medical Journal 329, 778-782.
Abbe, M., Simon, C., Angiolillo, A., Ruccione, K. & Kodish, ED. (2006) A survey of language barriers from the perspective of pediatric oncologists, interpreters, and parents. Pediatric Blood Cancer 47(6), 819-824.
Adamson, J. & Donovan, JL. (2002) Research in Black and White. Qualitative Health Research 12(6), 816-25.
Alberti, KG. & Zimmet, PZ. (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabetic Medicine 15(7), 539-553.
Alberti, G., Zimmet, P., Shaw, J., Bloomgarden, Z., Kaufman, F., Silink, M., for the consensus workshop group. (2004) Type 2 diabetes in the young: the evolving epidemic. The International Diabetes Federation Consensus Workshop. Diabetes Care 27(7), 1798-1811.
Allwood, CM. & Franzén, EC. (2000) Intercultural encounters. In: Allwood CM. & Franzén, EC. (Eds.), Intercultural encounters. A basic book for psychologists and social workers, pp.15-38. (In Swedish). Natur och Kultur.
Al-Arouj, M., Bouguerra, R., Buse, J., Hafez, S., Hassanein, M., Ibrahim, MA., Ismail-Beigi, F., El-Kebbi, I., Khatib, O., Kishawi, S., Al-Madani, A., Mishal, AA., Al-Maskari, M., Nakhi, AB. & Al-Rubean, K. (2005) Recommendations for management of diabetes during Ramadan. Diabetes Care 28(9), 2305-2311.
American Diabetes Association. (2003) Screening for Type 2 diabetes. Diabetes Care 26 (Suppl 1), S21-S24.
Amos, A., McCarty, DJ. & Zimmet, P. (1997) The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabetic Medicine 14 (Suppl 5), S7-S85.
Andrews, MM. & Boyle, JS. (2008) Transcultural concepts in nursing. Fifth Edition. Philadelphia, Wolters Kluwer Health / Lippincott Williams & Wilkins.
Baker, P., with Hussain, Z. & Saunders, J. (1991) Interpreters in Public Services: Policy and Training. London, Venture Press.
Barber, SG., Fairweather, S., Wright, AD., Fitzgerald, MG. & Malins, JM. (1979). Muslims, Ramadan, and diabetes mellitus. British Medical Journal 2, 46-47.

63
Baxter, LA. (1991) Content analysis. In: Montgomery, BM. & Duck, S. (Eds.), Studying interpersonal interaction, pp. 239-253. New York and London, The Guildford Press.
Beeney, LJ., Bakry, AA.& Dunn, SM. (1996) Patient psychological and information needs when the diagnosis is diabetes. Patient Education and Counseling 29(1), 109-116.
Benaji, B., Mounib, N., Roky, R., Aadil, N., Houti, IE., Moussamih, S., Maliki, S., Gressier, B. & El Ghomari, H. (2006) Diabetes and Ramadan: review of the literature. Diabetes Research and Clinical Practice 73(2), 117-125.
Berg, B.L. (2004) Qualitative Research Methods For The Social Sciences. Fifth Edition. Boston, Pearson Education, Inc.
Berger, B., Stenström, G., Chang, YF. & Sundkvist, G. (1998) The prevalence of diabetes in a Swedish population of 280,411 inhabitants. A report from the Skaraborg diabetes registry. Diabetes Care 21(4), 546-548.
Berger, B., Stenström, G. & Sundkvist, G. (1999) Incidence, prevalence, and mortality of diabetes in a large population: a report from the Skaraborg Diabetes Registry. Diabetes Care 22(5), 773-778.
Bischoff, A., Bovier, PA., Isah, R., Francoise, G., Ariel, E. & Louis, L. (2003) Language barriers between nurse and asylum seekers: Their impact on symptom reporting and referral. Social Science & Medicine 57(3), 503-512.
Björk Brämberg, E. (2008) To be an immigrant and a patient in Sweden. An individualised perspective. (Dissertation) (In Swedish) Department of Health Sciences and Social Work, Växjö University.
Brink, PJ. (1999) Transcultural versus cross-cultural. Journal of Transcultural Nursing 10(1), 7.
Brink, PJ. & Wood, MJ. (1998) Advanced Design In Nursing Research. Second Edition. Thousand Oaks, Sage Publications, Inc.
Bryman, A. (2004) Social Research Methods. Second Edition. Oxford, University Press.
Burns, D. & Skelly, AH. (2005) African American women with type 2 diabetes: meeting the daily challenges of self care. The Journal of Multicultural Nursing 11(3), 6-10.
Bäärnhielm, S., Ekblad, S., Ekberg, J. & Ginsburg, BE. (2005) Historical reflections on mental health care in Sweden: The welfare state and cultural diversity. Transcultural Psychiatry 42(3), 394-419.
Callaghan, D. & Williams, A. (1994). Living with diabetes: Issues for nursing practice. Journal of Advanced Nursing 20(1), 132-139.
Carroll, J., Epstein, R., Fiscella, K., Gipson, T., Volpe, E. & Jean-Pierre, P. (2007) Caring for Somali women: Implications for clinical-patient communication. Patient Education and Counseling 66(3), 337-345.

64
Carter, JS., Pugh, JA. & Monterrosa, A. (1996) Non-insulin dependent diabetes mellitus in minorities in the United States. Annals of Internal Medicine 125(3), 221-232.
CIA. World Factbook. (October 2008) Somalia. Retrieved 30 October 2008 from: https://www.cia.gov/library/publications/the-world-factbook/geos/so.html.
Cioffi, RN. (2003) Communicating with culturally and linguistically diverse patients in an acute setting: nurses´ experiences. International Journal of Nursing Studies 40(3), 299-306.
Dahlberg, K. (1996) Intersubjective meeting in holistic caring: a Swedish perspective. Nursing Science Quarterly 9(4), 147-151.
Dalal, AK. (2000) Living with a chronic disease: healing and psychological adjustment in Indian society. Psychology and Developing Societies 12(1), 67-81.
Daly, J., Davidson, P., Chang, E., Hancock, K., Rees, D. & Thompson, DR. (2002) Cultural aspects of adjustment to coronary heart disease in Chinese-Australians: a review of the literature. Journal of Advanced Nursing 39(4), 391-399.
Davidson, JC. (1979) Muslims, Ramadan, and diabetes mellitus. (Letter). British Medical Journal 2, 1511-1512.
Davies, E. A., Hall, S. M., Clarke, C. R., Bannon, M. P., & Hopkins, A. P. (1998). Do research interviews cause distress or interfere in management? Experience from a study of cancer patients. Journal of the Royal College of Physicians of London 32(5), 406-411.
Downe-Wamboldt, B. (1992) Content analysis: method, applications and issues. Health Care for Women International 13(3), 313-321.
Dye, CJ., Haley-Zitlin, V. & Willoughby, D. (2003) Insights from older adults with type 2 diabetes: Making dietary and exercise changes. The Diabetes Educator 29(1), 116-127
Edwall, L-L., Hellström, A-L., Öhrn, I. & Danielson, E. (2008) The lived experience of the diabetes nurse specialist regular check-ups, as narrated by patients with type 2 diabetes. Journal of Clinical Nursing 17(6), 772-781.
Edwards, R. (1998) A critical examination of the use of interpreters in the qualitative research process. Journal of Ethnic and Migration Studies 24(1), 197-208.
Edwards, R., Temple, B. & Alexander, C. (2005) User’s experiences of interpreters. Interpreting 7(1), 77-95.
Efraimsson, E., Sandman, PO. & Rasmussen, BH. (2006) ` They were talking about me´- elderly women’s experiences of taking part in a discharge planning conference. Scandinavian Journal of Caring Sciences 20(1), 68-78.

65
Ekblad, S. (2000) Integration and Public Health, questions for all. (In Swedish). Socialmedicinsk tidskrift 77(1), 2-7.
Ekblad, S., Marttila, A. & Emilsson, M. (2000) Cultural challenges in end-of-life care: reflections from focus groups´ interviews with hospice staff in Stockholm. Journal of Advanced Nursing 31(3), 623-630.
Elhadd, TA. & Al-Amoudi, AA. (2006) Recommendations for management of diabetes during Ramadan. (Comments and responses). Diabetes Care, 29(3) 744-745.
Eliasson, M. & Boström, G. (2006) Chapter 5.2: Major public health problems – diabetes. Scandinavian Journal of Public Health 34(Suppl 67), 59-68.
El-Kebbi, IM., Bacha, GA., Ziemer, DC., Musey, VC., Gallina, DL., Dunbar, V. & Phillips, LS. (1996) Diabetes in urban African Americans. V. Use of discussion groups to identify barriers to dietary therapy among low-income individuals with non-insulin-dependent diabetes mellitus. Diabetes Educator 22(5), 488-492.
Elo, S. & Kyngäs, H. (2007. The qualitative content analysis process. Journal of Advanced Nursing 62(1), 107-115.
Eriksson, J., Lindström, J. & Tuomilehto, J. (2001) Potential for prevention of type 2 diabetes. British Medical Bulletin 60(1), 183-199.
Esposito, N. (2001) From meaning to meaning: The influence of translation techniques on non-English focus group research. Qualitative Health Research 11(4), 568-579.
Esposito, N. (2005) Agenda dissonance. Immigrant Hispanic women’s assumptions and expectations for menopause healthcare. Clinical Nursing Research 14(1), 32-56.
Fagerli, RA., Lien, ME., Botten, GS. & Wandel, M. (2005a) Role dilemmas among health-workers in cross-cultural patient encounters around dietary advice. Scandinavian Journal of Public Health 33(5), 360-369.
Fagerli, RA., Lien, ME. & Wandel, M. (2005b) Experience of dietary advice among Pakistani-born persons with type 2 diabetes in Oslo. Appetite 45(3), 295-304.
Fagerli, RA., Lien, ME. & Wandel, M. (2007) Health worker style and trustworthiness as perceived by Pakistani born person with type 2 diabetes in Oslo, Norway. Health 11(1), 109-129.
Fatahi, N., Hellström, M., Skott, C. & Mattsson, B. (2008) General practitioners´ views on consultations with interpreters: A triad situation with complex issues. Scandinavian Journal of Primary Health Care 26(1), 40-45.
Fatahi, N., Mattsson, B., Hasanpoor, F. & Skott, C. (2005) Interpreters´ experiences of general practitioner-patient encounters. Scandinavian Journal of Primary Health Care 23(3), 159-163.
Fitzgerald, JT, Anderson, RM. & Davis, WK. (1995) Gender differences in diabetes attitudes and adherence. Diabetes Educator 21(6), 523-529.

66
Flores, G. (2005) The impact of medical interpreter services on the quality of health care: a systematic review. Medical Care Research Review 62(3), 255-299.
Funnell, MM. & Anderson, RM. (2002) Working toward the next generation of diabetes self-management education. American Journal of Preventive Medicine 22 (4), Suppl.1, 3-5.
Furnham, A., Akande, D. & Baguma, P. (1999) Beliefs and illness in three countries: Britain, South Africa and Uganda. Psychology, Health & Medicine 4(2), 189-201.
Garrard, J. (1999) Health Sciences Literature Review Made Easy. The Matrix Method. Sudbury, Jones and Bartlett Publishers.
Garrard, J. (2007) Health Sciences Literature Review Made Easy. The Matrix Method. Second Edition. Sudbury, Jones and Bartlett Publishers.
Gerrish, K. (2001) The nature and effect of communication difficulties arising from interaction between district nurses and South Asian patients and their carers. Journal of Advanced Nursing, 33(5), 566-574.
Gerrish, K., Chau, R., Sobowale, A. & Birks, E. (2004) Bridging the language barrier: the use of interpreters in primary care nursing. Health and Social Care in the Community 12 (5), 407-413.
Gillibrand, W. & Flynn, M. (2001) Forced externalization of control in people with diabetes: a qualitative exploratory study. Journal of Advanced Nursing, 34(4), 501-510.
Glasser, I. (1983) Guidelines for using an interpreter in social work. Child Welfare 62, 468-470.
Graneheim, UH. & Lundman, B. (2004) Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today 24(2), 105-12.
Green, A., Christian Hirsch, N. & Pramming, SK. (2003) The changing world demography of type 2 diabetes. Diabetes Metabolism Research and Reviews 19(1), 3-7.
Green, AR., Ngo-Metzger, Q., Legedza, AT., Massagli, MP., Phillips, RS. & Lezzoni, LI. (2005) Interpreter service, language concordance, and health care quality. Experiences of Asian Americans with limited English proficiency. Journal of General Internal Medicine 20(11), 1050-1056.
Greenhalgh, T., Helman, C. & Chowdhury, AM. (1998) Health beliefs and folk models of diabetes in British Bangladeshis: a qualitative study. British Medical Journal 316, 978-983.
Greenhalgh, T., Robb, N. & Scambler, G. (2006) Communicative and strategic action in interprted consultations in primary health care: A Habermasian perspective. Social Science & Medicine 63(5), 1170-1187.
Guthrie, D.W. & Guthrie, R.A. (2002) Nursing management of Diabetes mellitus. A guide to the pattern approach. Fifth Edition. New York, Springer Publishing Company, Inc.

67
Gåfvels, C. (1997) The people behind the disease. A population-based study of life adjustment to insulin-treated diabetes. (Dissertation). Department of Social Medicine and Medicine. Umeå University.
Gåfvels, CM. & Lithner, FG. (1996) Insulin treated diabetic patients. Use of, experience of and attitudes to diabetes care. European Journal of Public Health 6(4), 262-269.
Hawthorne, K., Mello, M. & Tomlinson, S. (1993) Cultural and religious influences in diabetes care in Great Britain. Diabetic Medicine 10(1), 8-12.
Helman, CG. (2001) Culture, Health and Illness. Fourth Edition. London, Arnold.
Hjelm, K. (1998) Migration, health and diabetes mellitus. Studies comparing foreign- and Swedish-born diabetic subjects living in Sweden. (Dissertation) Department of Community Health Sciences, Lund University, Sweden.
Hjelm, KG., Bard, K. & Apelqvist, J. (2005) Beliefs about health and diabetes in men of different ethnic origin. Journal of Advanced Nursing 50(1), 47-59.
Hjelm, K., Bard, K., Nyberg, P. & Apelqvist, J. (2003) Religious and cultural distance in beliefs about health and illness in women with diabetes mellitus of different origin living in Sweden. International Journal of Nursing Studies 40(6), 627-643.
Hjelm, K., Isacsson, Å. & Apelqvist, J. (1998) Health care professionals´ perceptions of beliefs about health and illness in migrants with diabetes mellitus. Practical Diabetes International, 15(8), 233-237.
Hjelm, K., Nyberg, P., Isacsson, A. & Apelqvist, J.(1999) Beliefs about health and illness essential for self-care practice: a comparison of migrant Yugoslavian and Swedish diabetic females. Journal of Advanced Nursing 30(5), 1147-1159.
Hjelm, K. & Nambozi, G. (2008) Beliefs about health and illness: a comparison between Ugandan men and women living with Diabetes Mellitus. International Nursing Review 55(4), 434-441.
Hjern, A. (1995) Migration medicine research: a review. (In Swedish). Stockholm, Medicinska forskningsrådet. Rapport 1995.:1
Hodes, R.M. (1997) Cross-cultural medicine and diverse health beliefs. Ethiopians abroad. The Western Journal of Medicine 166(1), 29-36.
Hornberger, J.C., Gibson, C.D., Wood, W., Dequeldre, C., Corso, I., Palla, B. & Bloch, D.A. (1996) Eliminating language barriers for non-speaking patients. Medical Care 34(8), 845-856.
Hornberger, J., Itakura, H. & Wilson, SR. (1997) Bridging language and cultural barriers between physicians and patients. Public Health Reports 112(5), 410-417.

68
Holmström, I., Halford, C. & Rosenqist, U. (2003) Swedish health care professionals´ diverse understandings of diabetes care. Patient Education and Counseling 51(1), 53-58.
Holmström, IM. & Rosenqvist, U. (2005) Misunderstanding about illness and treatment among patients with type 2 diabetes. Journal of Advanced Nursing 49(2), 146-154.
Hsieh, HF. & Shannon SE. (2005) Three approaches to qualitative content analysis. Qualitative Health Research 15(9), 1277-1287.
Hultsjö, S. & Hjelm, K. (2005) Immigrants in emergency care: Swedish health care staff’s experiences. International Council of Nurses 52 (4), 276-285.
Hörnsten, Å. (2004) Experiences of diabetes care – patients’ and nurses´ perspectives. (Dissertation). Department of Nursing and Department of Public Health and Clinical Medicine, Family medicine, Umeå University, Sweden.
Im, EO., Page, R., Lin, LC., Tsai, HM. & Cheng CY. (2004) Rigor in cross-cultural nursing research. International Journal of Nursing Studies 41(8), 891-899.
Jaber, LA., Brown, MB., Hammad, A., Nowak, SN., Zhu, Q., Ghafoor, A. & Herman, WH. (2003) Epidemiology of diabetes among Arab Americans. Diabetes Care 26(2), 308-313.
James, DC. (2004) Factors influencing food choices, dietary intake, and nutrition-related attitudes among African Americans: Application of a culturally sensitive model. Ethnicity & Health 9(4), 349-367.
Jentsch, B. (1998) The ‘interpreter effect’: Rending interpreters visible in cross-cultural research and methodology. Journal of European Social Policy 8(4), 275-289.
Jerreat, L. (2004) Diabetes for nurses. Second Edition. London, Whurr Publishers Ltd.
Jobanputra, R. & Furnham, A. (2005) British Gujarati Indian immigrants and British Caucasians beliefs about health and illness. International Journal of Social Psychiatry, 51(4), 350-364.
Johnsdotter, S. (2007) “The family tree is long”. Somalian families and the national regulations. In: Olsson, E., Lunqvist, C., Rabo, A., Sawyer, L., Wahlbeck, Ö. & Åkesson, Å. (Eds.), Transnational areas, pp. 115-136. (In Swedish). Umeå, Boréa Bokförlag.
Jonsson, IM., Wallin, AM., Hallberg, LR. & Gustavsson, IB. (2002) Choice of food and food traditions in pre-war Bosnia-Herzegovina: focus group interviews with immigrant women in Sweden. Ethnicity and Health 7(3), 149-161.
Kapborg, I. & Berterö, C. (2002) Using an interpreter in qualitative interviews: does it threaten validity? Nursing Inquiry 9 (1), 52-56.

69
Karliner, LS., Jacobs, EA., Hm Chen, A. & Mutha, S. (2007) Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Services Research 42(2), 727-754.
King, H. & Rewers, M. (1993) Global estimates for prevalence of diabetes mellitus and impaired glucose tolerance in adults. Diabetes Care 16(1), 157-177.
Koch, T., Kralik, D. & Sonnack, D. (1999) Women living with type II diabetes: the intrusion of illness. Journal of Clinical Nursing 8(6), 712-722.
Koch, T., Kralik, D. & Taylor, J. (2000) Men living with diabetes: minimizing the intrusiveness of the disease. Journal of Clinical Nursing 9(2), 247-254.
Kocturk-Runefors, T. (1991) A model for adaptation to a new food pattern: The case of immigrants. In: Furst, EL., Prättälä, R., Ekström, M., Holm, L. & Kjarnes, U. (Eds), Palatable worlds. Sociocultural food studie, pp. 185-192. Oslo, Solum förlag.
Kralik, D., Brown, M. & Koch, T. (2001) Women’s experiences of `being diagnosed´ with a long-term illness. Journal of Advanced Nursing 33(5), 594-602.
Krippendorff, K. (2004) Content analysis. An introduction to its methodology. Second Edition. Thousand Oaks, Sage Publications. Inc.
Kvale, S. (1996) Interviews. An introduction to qualitative research interviewing. Thousand Oak, Sage Publications, Inc.
Landrine, H. & Klonoff, E.A. (1994) Cultural diversity in causal attributions for illness: The role of supernatural. Journal of Behavioral Medicine 17(2), 181-193.
Lee, TS., Lansbury, G. & Sullivan, G. (2005) Health care interpreters: A physiotherapy perspective. Australian Journal of Physiotherapy 51(3), 161-165.
Legal Financial and Administrative Services. (2004) Good interpreting practice. Guidance for authorised interpreters. (In Swedish). Received December 8, 2008 from http://www.kammarkollegiet.se/tolktrans/Godtolk.pdf
Leininger, M.M. (1998) Nature, Rationale, and Importance of Qualitative Research Methods in Nursing. In: Leininger, M.M. (Ed.), Qualitative Research Methods in Nursing, pp.1-25. United States of America, Greyden Press.
Lincoln, Y.S. & Guba, E.G. (1985) Naturalistic Inquiry. London, Sage Publications.
Loveman, E., Royle, P. & Waugh, N. (2003) Specialist nurses in diabetes mellitus. Cochrane Database of Systematic Reviews. Issue 2. Art.No:CD003286.DOI: 10.1002/14651858.CD003286.
Luckmann, J. (1999) Transcultural communication in nursing. Delmar Publishers, Albany.

70
Lundh, C. & Ohlsson, R. (1999) From import of labour migrants to immigration of refugees. Second Edition. (In Swedish). Stockholm, SNS Förlag.
Lundman, B. (1990) Daily livening and coping strategies in insulin-dependent diabetics - Diagnostic reasoning in nursing. (Dissertation). Department of Advanced Nursing and Medicine, University of Umeå, Sweden.
Lundman, B. & Engström, L. (1998) Diabetes and it’s complications in a Swedish county. Diabetes Research and Clinical Practice 39(2), 157-164.
Malpass, A., Andrews, R. & Turner, KM. (2008) Patients with Type 2 diabetes experiences of making multiple lifestyle changes: A qualitative study. Patient Education and Counseling, doi:10.1016/j.pec.2008.08.018.
Matlby, HJ. (1999) Interpreters: A double-edged sword in nursing practice. Journal of Transcultural Nursing 10(3), 248-254.
Marshall, C. & Rossman, G.B. (2006) Designing Qualitative Research. Fourth Edition. Thousand Oaks, Sage publications, Inc.
Marton, F. (1981) Phenomenography – describing conceptions of the world around us. Instructional Science 10, 177-200.
Marton, F. (1986) Phenomenography – a research approach to investigating different understandings of reality. International Journal of Thought 21 (3), 28-49.
Marton, F. (1996) Cognoscon ergo sum – Reflections on reflections. In: Dall´Alba, G. & Hasselgren. B. (Eds.), Reflections on Phenomenography. Towards a methodology? pp. 163-187. Göteborg, Acta Universitatis Gothoburgensis.
Marton, F. & Booth, S. (1997) Learning and Awareness. New Jersey, Lawrence Erlbaum Associates, Inc., Publishers Mahwah.
Marton, F., Dall´Alba, G. & Beaty, E. (1993) Conceptions of learning. International Journal of Educational Research 19, 277-300.
Marton, F. & Ming Fai, P. (1999) Two faces of variation. Paper presented at 8th European Conference for Learning and Instruction August 24-28, 1999, Göteborg University, Göteborg, Sweden.
Marton, F. & Yan Pong, W. (2005) On the unit of description in phenomenography. Higher Education Research & Development 24 (4), 335-348.
McAllister, G. & Farquhar, M. (1992) Health beliefs: a cultural division? Journal of Advanced Nursing 17(12), 1447-1454.
McCabe, C. & Timmins, F. (2006) Communications skills for nursing practice. New York, Palgrave Macmillan.
McCord, EC. & Brandenburg, C. (1995) Beliefs and Attitudes of Persons with Diabetes. Family Medicine 27(4), 267-271.
McKague, M. & Verhoef, M. (2003) Understanding of health and its determinants among clients and providers at an urban community health center. Qualitative Health Research 13(5), 703-717.

71
Morse, J.M. & Field, P.A (1995) Qualitative Research Methods for Health Professionals. Second Edition. Thousand Oaks, Sage Publications, Inc.
Munhall, P.L. (2001) Nursing Research. A Qualitative Perspective. Third Edition. Sudbury, Jones and Bartlett Publishers.
Munoz, C. & Luckmann, J. (2005) Transcultural communication in nursing. Second Edition. Clifton Park, NY : Thomson/Delmar Learning.
Murphy, K. & Clark, JM. (1993) Nurses´ experiences of caring for ethnic-minority clients. Journal of Advanced Nursing 18(3), 442-450.
Murray, CD. & Wynne, J. (2001) Researching community, work and family with an interpreter. Community, Work & Family 4(2), 151-171.
Mårtensson, J. (2002) The life situation of patients with heart failure in primary health care. An explorative and interventional study. (Dissertation). Department of Primary Health Care, Göteborg University.
Naeem, AG. (2003) The role of culture and religion in the management of diabetes: a study of Kashmiri men in Leeds. The Journal of The Royal Society for the Promotion of Health 123(2), 110-116.
Naithani, S., Gulliford, M. & Morgan, M. (2006) Patients’ perceptions and experiences of `continuity of care´ in diabetes. Health Expectations 9(2), 118-129.
National Board of Health and Welfare. (1999) National guidelines for care and treatment of diabetes mellitus. A version for health professionals. (In Swedish). Stockholm.
National Board of Health and Welfare. (2004) Equity in caring? A gender perspective on health care. (In Swedish). Stockholm.
Ngo-Metzger, Q., Massagli, MP., Clarridge, BR., Manocchia, M., Davis, RB., Lezzoni, LI. & Philips, RS. (2003) Linguistic and cultural barriers to care. Perspectives on Chinese and Vietnamese immigrants. Journal of General Internal Medicine 18(1), 44-52.
Niska, H. (2004) Community interpreting in Sweden. A short presentation. Received April 10, 2008 from http://transnordica.se/Skriften.swf
Nordström, S. (1993) Somalian immigrants. In: Swedish Integration Board. Somalis. Basic information, pp. 40-43. (In Swedish). Norrköping, Swedish Integration Board.
Northern Nurses´ Federation. (2003) Ethical guidelines for nursing research in the Nordic countries. Received August 30, 2008 from http://www.vardinorden.no/vard/index.html
Nthangeni, G., Steyn, NP., Alberts, M., Steyn, K., Levitt, NS., Laubscher, R., Bourne, L., Dick, J. & Temple, N. (2002) Dietary intake and barriers to dietary compliance in black type 2 diabetic patients attending primary health-care services. Public Health Nutrition 5(2), 329-338.
Papadopoulos, I. (2000) An exploration of health beliefs, lifestyle behaviours, and health needs of the London-based Greek Cypriot community. Journal of Transcultural Nursing 11(3), 182-190.

72
Papadopoulos, I. (2006) The Papadopoulos, Tilki and Taylor model of developing cultural competence. In: Papadopoulos, I. (Ed.), Transcultural health and social care. Development of culturally competent practitioners, pp. 7-24. Forewords by Cecil Helman and Larry Purnell. London, Chuchill Livingstone Elsevier.
Patton, MQ. (1990) Qualitative evaluation and research methods. Second Edition. Thousand Oaks, Sage Publication, Inc.
Patton, MQ. (2002) Qualitative Research & Evaluation Methods. Third Edition. Thousand Oaks: Sage Publications, Inc.
Peel, E., Parry, O., Douglas, M. & Lawton, J. (2004) Diagnosis of type 2 diabetes: qualitative analysis of patients´ emotional reactions and views about information provision. Patient Education and Counseling 53(3), 269-75.
Penckofer, S., Estwing Ferrans, C., Velsor-Friedrich, B. & Savoy, S. (2007) The psychological impact of living with diabetes. Women’s day-to-day experiences. The Diabetes Educator 33(4), 680-690.
Peters Harmel, A. & Mathur, R. (2004) Davidsons diabetes mellitus. Diagnosis and treatment. Fifth Edition. Philadelphia, Saunders.
Phelan, M. & Parkman, S. (1995) How to do it: Work with an interpreter. British Medical Journal 311, 555-557.
Polit, D. F. & Beck, C. T. (2004) Nursing Research. Principles and Method. Seventh Edition. Philadelphia, Lippincott Williams & Wilkins.
Pooley, CG., Gerrard, C., Hollis, S., Morton S. & Astbury, J. (2001) `Oh it’s a wonderful practice you can talk to them´: a qualitative study of patients´ and health professionals´ views on the management of type 2 diabetes. Health and Social Care in the Community 9 (5), 318-326.
Popoola, MM. (2005) Living with diabetes. The holistic experiences of Nigerians and African Americans. Holistic Nursing Practice 19(1), 10-16.
Purnell L.D. & Paulanka, B.J. (1998) Transcultural health care. A culturally competent approach. Philadelphia, F. A. Davis Company.
Qureshi, B. (2002) Diabetes in Ramadan. Journal of the Royal Society of Medicine 95(10), 489-490.
Renders, CM., Valk, GD., Griffin, S., Wagner, EH., van Eijk, JThM. & Assendelft, WJJ. (2000) Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. Cochrane Database of Systematic Reviews. Issue 4. Art. No.:CD001481.
Rhodes, P. & Nucon, A. (2003) A problem of communication? Diabetes care among Bangladeshi people in Bradford. Health and Social Care in the Community 11(1), 45-54.
Robinson, M. & Gilmartin, J. (2002) Barriers to communication between health practitioners and service users who are not fluent in English. Nurse Education Today 22 (6), 457-465.

73
Rosenberg, E., Seller, R. & Leanza, Y. (2008) Through interpreters´ eyes: Comparing roles of professional and family interpreters. Patient Education and Counseling 70 (1), 87-93.
Rosengren K.E. (1981) Advances in Scandinavian content analysis. An introduction. In: Rosengren, K.E. (ed.), Advances in content analysis, pp. 9-19. Beverly Hills, California, Sage Publications, Inc.
Rubin, R.R. & Peyrot, M. (2001) Psychological issues and treatment for people with diabetes. Journal of Clinical Psychology 57(4), 457-478.
Saleh Stattin, N. (2001) Immigrant patients with diabetes. How they understand, learn to manage and live with their diabetes. (Dissertation). Department of Public health and Caring Sciences, Health Services Research, Uppsala University, Sweden.
Salti, I., Bénard, E., Detournay, B., Bianchi-Biscay, M., Le Brigand, C., Voinet, C., Jabbar, A. on behalf of the EPIDIAR study group. (2004) A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries. Diabetes Care 27(19), 2306-2311.
Samarasinghe, K. & Arvidsson, B. (2002) ‘It is a different war to fight here in Sweden’ – the impact of involuntary migration on the health of refugee families in transition. Scandinavian Journal of Caring Sciences 16(3), 292-301.
Samuel-Hodge, CD., Headen, SW., Skelly, AH., Ingram, AF., Keyserling, TC., Jackson, EJ., Ammerman, AS. & Elasy, TA. (2000) Influences on Day-to-Day Self-Management of Type 2 Diabetes Among African-American Women. Diabetes Care 23(7), 928-933.
SCB. (n.d.-a) Asylum seekers during 2007 and 2006, after citizenship and sex. (In Swedish). Received September 15, 2008 from http://www.scb.se/templates/tableOrChart____82972.asp
SCB. (n.d.-b) Summary of the statistics of the population 1960-2007. (In Swedish) Received September 16, 2008 from http://www.scb.se/templates/tableOrChart___26040.asp
SCB. (2004) Postwar period of migration. (In Swedish). Örebro, Statistic Sweden.
SCB. (2007) Description of the population in Sweden 2006. Official statistics of Sweden. (In Swedish). Statistics Sweden 2007. Retrieved Dec ember 31, 2008 from http://www.scb.se/templates/PlanerPublicerat/ViewInfo.aspx?publobjid=4958&lang=SV
SCB. (2008) Tables on population in Sweden 2007. (In Swedish). Official statistics of Sweden. Statistics Sweden 2008. Retrieved December 31, 2008 from http://www.scb.se/templates/PlanerPublicerat/ViewInfo.aspx?publobjid=6636&lang=SV

74
Schröder, A. (2006) Quality of care in the psychiatric setting: perspectives of the patient, next of kin and care staff. (Dissertation). Department of Medicine and Care, Division of Nursing Science Faculty of Health Sciences, Linköping University, Sweden.
Scott, P. (1998) Lay beliefs and the management of disease amongst West Indians with diabetes. Health and Social Care in the Community 6(6), 407-419.
Scuglik, DL., Alarcón, RD., Lapeyre III, AC., Williams, MD. & Logan, KM. (2007) When the poetry no longer rhymes: Mental health issues among Somali Immigrants in the USA. Transcultural Psychiatry, 44(4), 581-595.
SFS. Aliens Act 2005:716. (In Swedish). Retrieved September 15, 2008 from http://www.riksdagen.se/Webbnav/index.aspx?nid=3910
Sjöström, B. & Dahlgren, LO. (2002) Applying phenomenography in nursing research. Journal of Advanced Nursing 40(3), 339-345.
Skärsäter, I. (2002) The importance of social support for men and women, suffering from major depression. (Dissertation). Faculty of Health and Caring Sciences, Institute of Nursing, Göteborg University, Sweden.
Smide, B. (2006) Diabetes in Tanzania – a developing country. In: Wikblad, K. (Ed.), Care with diabetes, pp. 323-333. (In Swedish). Lund, Studentlitteratur.
SOU 1999:137. Immigrants. Background, present situation and prognosis. In: Equity in health/the second step toward national goals for public health, pp. 242-251. (In Swedish). Interim report from the National Public Health Committee. Received September 8, 2008 from http/www.regeringen.se/sb/d/108/a/22547
Squires, A. (2008) Language barriers and qualitative nursing research: methodological considerations. International Nursing Review 55(3), 265-273.
Sulmani, RA., Famuyiwa, FO. & Laajam, MA. (1988) Diabetes Mellitus and Ramadan fasting: The need for a critical appraisal. Diabetic Medicine 5(6), 589-591.
Sundquist, J. (2001) Migration, equality and access to health care services. (Editorial). Journal of Epidemiological Community Health 55(10), 691-692
Svanberg, I. & Tydén, M. (1992) A thousand years of immigration. A Swedish cultural history. (In Swedish). Stockholm, Gidlunds Bokförlag.
Swedish Integration Board. (1999) Participation for integration – Stimulating the integration process for the Somali speaking population in Sweden.(In Swedish with an English summary). Norrköping, The Swedish Integration Board. Report 1999:4.
Swedish Integration Board. (2006) Pockets facts – Statistics on Integration. Norrköping

75
Swedish Migration Board (n.d.-a) History of the Swedish migration. Retrieved September 8, 2008, from http://www.migrationsverket.se/english.jsp
Swedish Migration Board. (2008a) Asylum seekers to Sweden during 1984-2006. Retrieved Sept 8, 2008 from http://www.migrationsverket.se/english.jsp
Swedish Migration Board. (2008b) Facts & Figures 2007. Retrieved Sept 8, 2008 from http://www.migrationsverket.se/english.jsp
Taylor, D. (2006) Migrants and refugees. In: Papadopoulos, I. (Ed.), Transcultural health and social care. Development of culturally component practitioners, pp. 45-64. Edinburgh, Churchill Livingstone.
Temple, B. & Young A. (2004) Qualitative research and translation dilemmas. Qualitative Research 4(2), 161-178.
Thomas, V & Dines, A. (1994) The health care needs of ethnic minority groups: are nurses and individuals playing their part? Journal of Advanced Nursing 20(5), 802-808.
Thyli, B., Athlin, E. & Hedelin, B. (2007) Challenges in community health nursing of old migrant patients in Norway – an exploratory study. International Journal of Older People Nursing 2(1), 45-51.
Tsai, JH-C., Choe, JH., Lim, JMC., Acorda, E., Chan, NL., Taylor, V. & Tu, S-P. (2004) Developing culturally competent health knowledge: Issues of data analysis of cross-cultural, cross-language qualitative research. International Journal of Qualitative Methods 3(4), Article 2. Retrieved 7 March 2005 from http://www.ualberta.ca/~iiqm/backissues/3_4/pdf/tsai.pdf
Twinn, S. (1997) An exploratory study examining the influence of translation on the validity and reliability of qualitative data in nursing research. Journal of Advanced Nursing 26(2), 418-423.
Twinn, S. (1998) An analysis of the effectiveness of focus groups as a method of qualitative data collection with Chinese populations in nursing research. Journal of Advanced Nursing 28(3), 654-61.
Van Dam, H.A., van der Horst, F., van der Borne, B., Ryckman, R. & Crebolder, H. (2003) Provider-patient interaction in diabetes care: effects on patient self-care and outcomes. A systematic review. Patient Education and Counseling 51(1), 17-28.
Vijan, S., Stuart, N.S., Fitzgerald, J.T., Ronis, D.L., Hayward, R.A., Slater, S. & Hofer, T.P. (2004) Barriers to following dietary recommendations in Type 2 diabetes. Diabetic Medicine 22(1), 32-38.
Wen, LK., Parchman, ML. & Shepherd, MD. (2004) Family support and diet barriers among older Hispanic adults with type 2 diabetes. Family Medicine 36(6), 423-430.

76
Wenestam, C-G. (2000) The phenomenographic method in health research. In: Fridlund, B. & Hildingh, C. (Eds.), Qualitative research methods in the service of health, pp. 97-115. Lund, Studentlitteratur.
Wenzel, J., Utz, SW., Steeves, R., Hinton, I. & Jones, RA. (2005) ‘Plenty of sickness.’ Description by African Americans living in rural areas with type 2 diabetes. Diabetes Educator 31(1), 98-107.
Westermeyer, J. (1990) Working with an interpreter in psychiatric assessment and treatment. Journal of Nervous and Mental Disease 178(12), 745-749.
WHO. (2006) Diabetes. Fact sheet No 312. Received September 18, 2008 from http://www.who.int/topics/diabetes_mellitus/en
Wikblad, K.F. (1991) Patient perspectives of diabetes care and education. Journal of Advanced Nursing 16 (7), 837-844.
Wild, S., Roglic, G., Green, A., Sicree, R. & King, H. (2004) Global prevalence of diabetes. Estimates for the year 2000 and projections for 2030. Diabetes Care 27(5), 1047-53.
Wiman, E. & Wikblad, K. (2004) Caring and uncaring encounters in nursing in an emergency department. Journal of Clinical Nursing 13(4), 422-429.
World Medical Association. (2004) World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Received Sept 2, 2008 from http:// www.wma.net/e/policy/b3.html
Wändell, PE. & Gåfvels, C. (2007) High prevalence of diabetes among immigrants from non-European countries in Sweden. Primary Care Diabetes 1(1), 13-16.
Wändell, PE., Hjörleifsdottir Steiner, K. & Johansson, SE. (2003) Diabetes mellitus in Turkish immigrants in Sweden. Diabetes & Metabolism 29(4 pt 1), 435-439.
Wändell, PE., Wajngot, A., De Faire, U. & Hellénius, ML. (2007) Increased prevalence of diabetes among immigrants from non-European countries in 60-years-old men and women in Sweden. Diabetes & Metabolism 33(1), 30-36.
Ypinazar, VA. & Margolis, SA. (2006) Delivering culturally sensitive care: The perceptions of older Arabian Gulf Arabs concerning religion, health, and disease. Qualitative Health Research 16(6), 773-787.
Zimmet, P. (1999) Diabetes epidemiology as a tool to trigger diabetes research and care. Diabetologia 42(5), 499-518.
Zimmet, P. (2000) Globalization, coca-colonization and the chronic disease epidemic: can the Doomsday scenario be averted? Journal of Internal Medicine 247(3), 301-310.
Zimmet, P., Alberti, K.G.M.M. & Shaw, J. (2001) Global and societal implications of the diabetic epidemic. Nature 414(6865), 782-787.
Zimmet, P.Z., McCarty, D.J. & de Courten, M.P. (1997) The global epidemiology of non-insulin dependent diabetes mellitus and metabolic syndrome. Journal of Diabetes and Its Complications 11 (2), 60-68.

Living with diabetes within the
framework of Swedish primary
health care:
Somalian and professional perspectives
Anne-Marie Wallin
SCHOOL OF HEALTH SCIENCES, JÖNKÖPING UNIVERSITYDISSERTATION SERIES NO. 6, 2009
f o r s k a r s k o l a n h ä l s a o c h v ä l f ä r d
Living with diabetes w
ithin the framew
ork of Swedish prim
ary health care: Somalian and professional perspectives A
nne-Marie W
allin
Anne-Marie Wallin
Anne-Marie Wallin is a Registered Nurse with a Master of Science degree in Public Health. She has many years of experience as a district nurse and as a public health worker in multicultural settings. She has been coor-dinator around immigrants issues in primary health care in Örebro County Council. Anne-Marie Wallin has developed and carried out projects focusing on spe-cific health needs among immigrants and participated in epidemiological studies specially focused on immi-
grants. She has also had lectures for SFI (Swedish for immigrants) classes regarding health care and lectures in training courses for local-government interpreters in Örebro municipality about the Swedish health care in general.
Owing to the increased immigration during the last twenty years or so means that a lot of health-care professionals within diabetes care will in the future be encounter-ing people with diabetes who are born in countries culturally remote from Sweden. To ensure a high quality of diabetes care for all patients there is a need to acquire deeper knowledge of immigrants experiences of living with the disease and their conceptions of the encounter in diabetes care within primary health care. Therefore the thesis includes both immigrants of Somalian origin and health-care profes-sionals. To the author’s knowledge is this the first published research in Sweden or elsewhere that focuses on immigrants from Somalia with diabetes mellitus.
The findings in the thesis showed that changing lifestyle was considered as a hard work by the patients and a number of barriers was mentioned especially when it comes to eating habits. There was also a variation how they managed the fasting month of Ramadan. Those who fasted did not see the diabetes as an obstacle, oth-ers did so and indicated that fasting was not compulsory for a sick person. Women used more supernatural beliefs than men when they described their experiences in connection with the diagnosis and their health beliefs. Most of the experiences of receiving the diagnosis consisted of ways of managing this information. The pa-tients conceived the diabetes care as being of high quality but they also conceived limitation with the care. They conceived unmet needs such as too long waiting times for appointments, not encountering the same physician every time, lack of contact with specialists and failure to culturally adapt dietary advice. Health-care professionals conceived cultural challenges in the encounter such as managing lan-guage barriers, illiteracy and different traditions such as fasting during Ramadan.
JÖNKÖPING, 2009
ISSN 1654-3602 ISBN 978-91-85835-05-8